Expression of Partitioning Defective 3 (Par-3) for Predicting Extrahepatic Metastasis and Survival with Hepatocellular Carcinoma

Abstract
:1. Introduction
2. Results
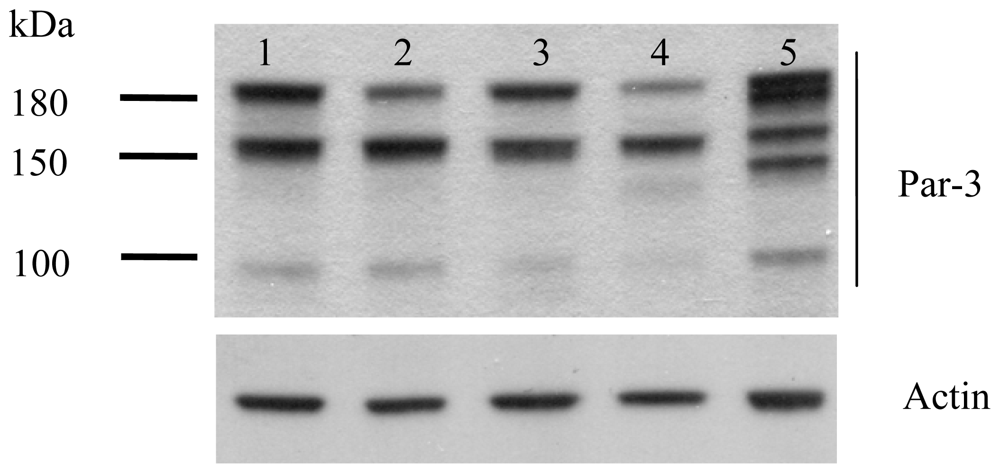
2.1. Protein Expression of Par-3 in HCC Cell Lines
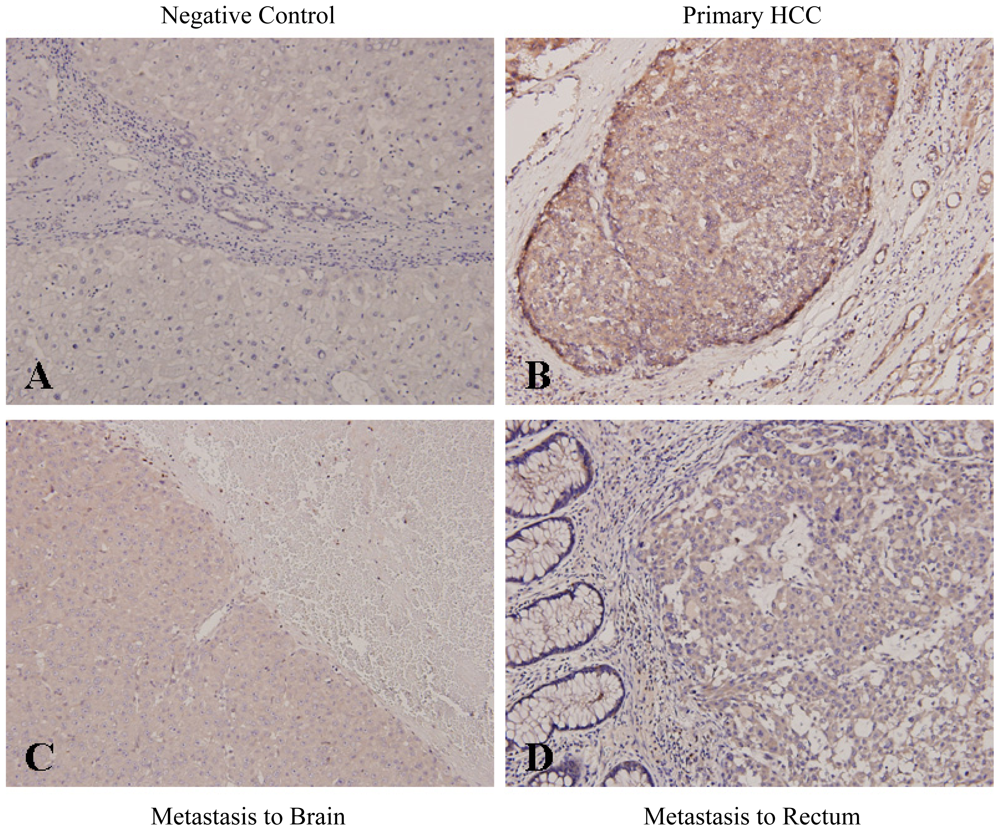
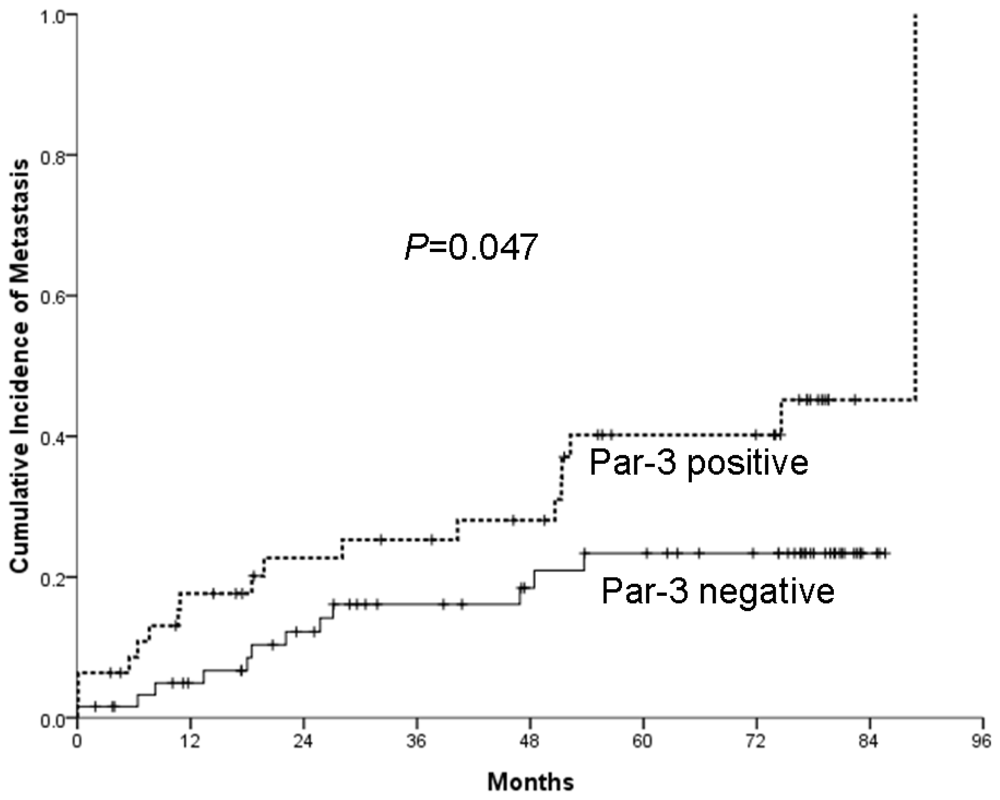
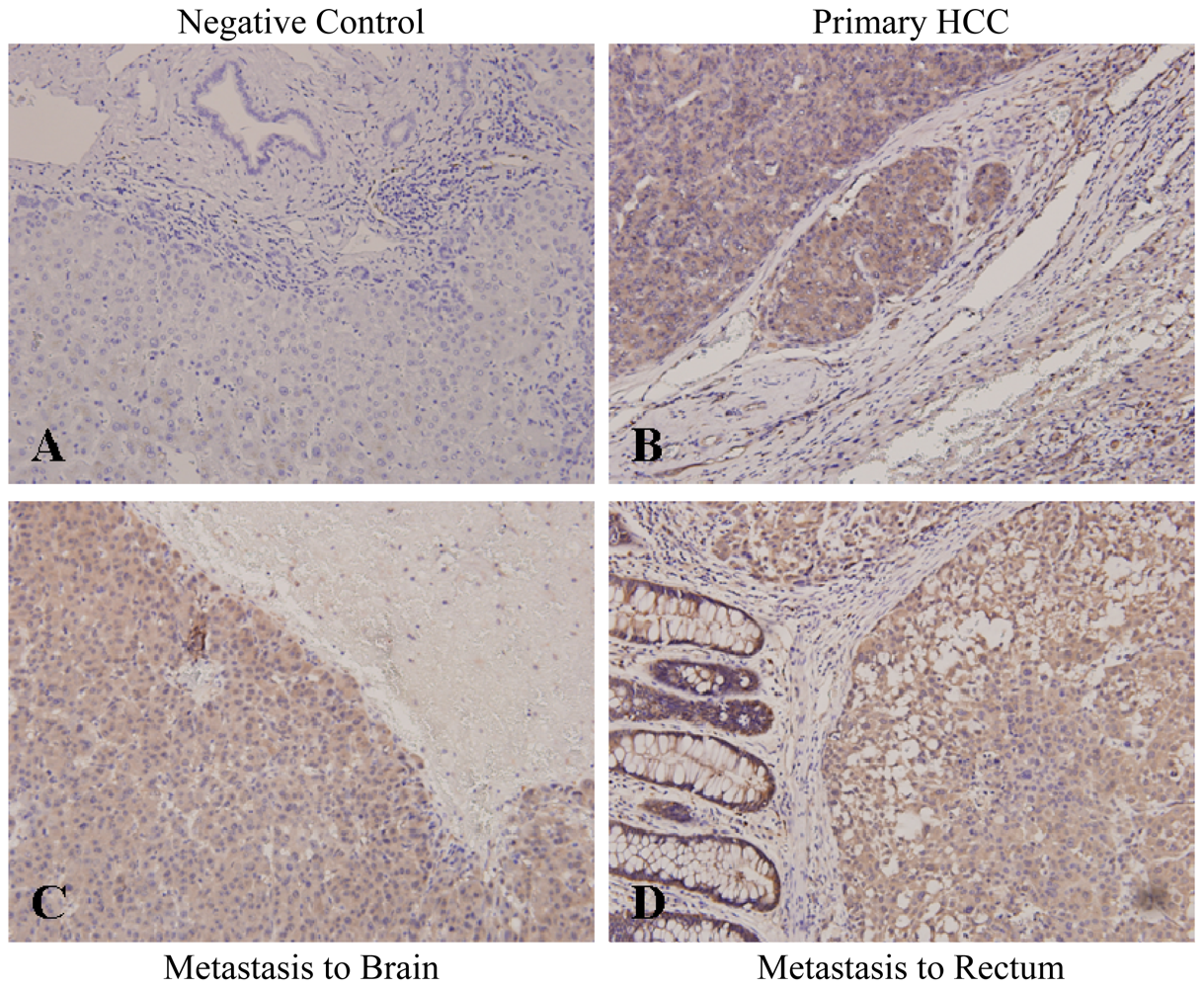
2.2. Increased Par-3 Protein Expression in Primary and Metastatic HCC Tissues and Association with HCC Extrahepatic Metastasis
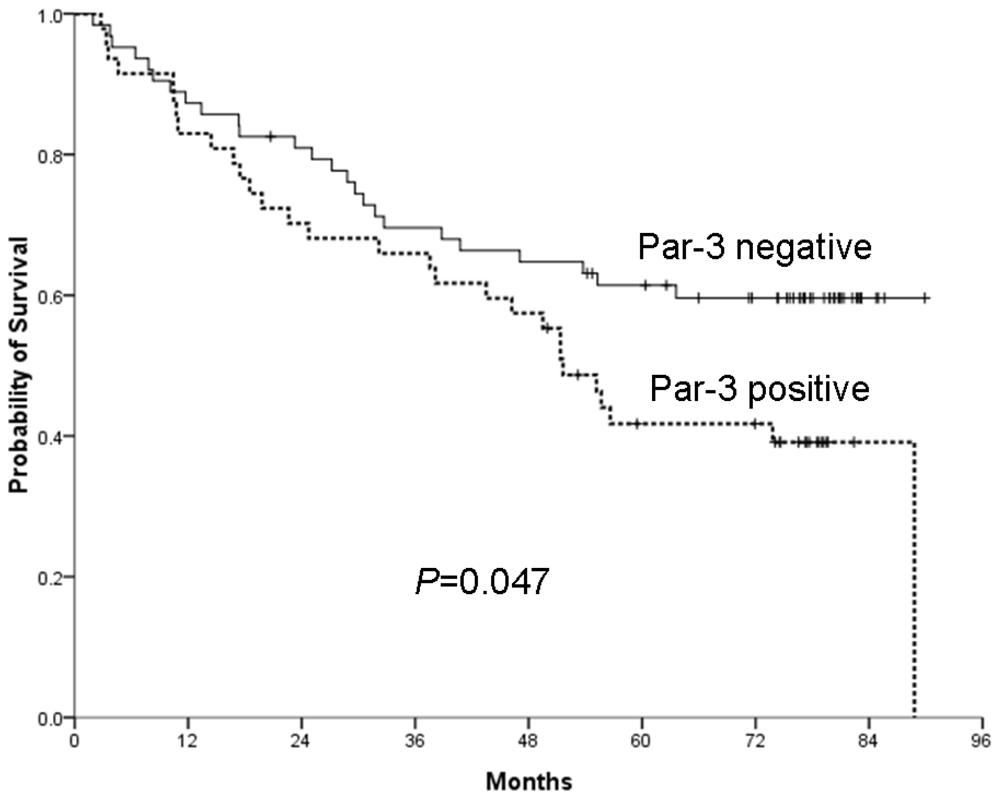
2.3. Overexpression of Par-3 and HCC Patient Survival
2.4. Correlation of Par-3 Expression with 14-3-3ɛ
3. Discussion
4. Materials and Methods
4.1. Patients and Clinical Specimens
4.2. Immunohistochemical Analysis
4.3. Cell Culture and Western Blot Analysis
4.4. Statistical Analysis
5. Conclusions
Acknowledgments
- Conflict of InterestThe authors declare no conflict of interest.
References
- Sherman, M. Hepatocellular carcinoma: Epidemiology, surveillance, and diagnosis. Semin. Liver Dis 2010, 30, 3–16. [Google Scholar]
- Rampone, B.; Schiavone, B.; Martino, A.; Viviano, C.; Confuorto, G. Current management strategy of hepatocellular carcinoma. World J. Gastroenterol 2009, 15, 3210–3216. [Google Scholar]
- Natsuizaka, M.; Omura, T.; Akaike, T.; Kuwata, Y.; Yamazaki, K.; Sato, T.; Karino, Y.; Toyota, J.; Suga, T.; Asaka, M. Clinical features of hepatocellular carcinoma with extrahepatic metastases. J. Gastroenterol. Hepatol 2005, 20, 1781–1787. [Google Scholar]
- Hasegawa, K.; Kokudo, N. Surgical treatment of hepatocellular carcinoma. Surg. Today 2009, 39, 833–843. [Google Scholar]
- Sawada, N.; Murata, M.; Kikuchi, K.; Osanai, M.; Tobioka, H.; Kojima, T.; Chiba, H. Tight junctions and human diseases. Med. Electron Microsc 2003, 36, 147–156. [Google Scholar]
- Lin, D.; Edwards, A.S.; Fawcett, J.P.; Mbamalu, G.; Scott, J.D.; Pawson, T. A mammalian PAR-3-PAR-6 complex implicated in Cdc42/Rac1 and aPKC signalling and cell polarity. Nat. Cell Biol 2000, 2, 540–547. [Google Scholar]
- Ooshio, T.; Fujita, N.; Yamada, A.; Sato, T.; Kitagawa, Y.; Okamoto, R.; Nakata, S.; Miki, A.; Irie, K.; Takai, Y. Cooperative roles of Par-3 and afadin in the formation of adherens and tight junctions. J. Cell Sci 2007, 120, 2352–2365. [Google Scholar]
- Chen, X.; Macara, I.G. Par-3 controls tight junction assembly through the Rac exchange factor Tiam1. Nat. Cell Biol 2005, 7, 262–269. [Google Scholar]
- Suzuki, A.; Ohno, S. The PAR-aPKC system: Lessons in polarity. J. Cell Sci 2006, 119, 979–987. [Google Scholar]
- Humbert, P.O.; Dow, L.E.; Russell, S.M. The Scribble and Par complexes in polarity and migration: friends or foes? Trends Cell Biol 2006, 16, 622–630. [Google Scholar]
- Hutterer, A.; Betschinger, J.; Petronczki, M.; Knoblich, J.A. Sequential roles of Cdc42, Par-6, aPKC, and Lgl in the establishment of epithelial polarity during Drosophila embryogenesis. Dev. Cell 2004, 6, 845–854. [Google Scholar]
- Shin, K.; Fogg, V.C.; Margolis, B. Tight junctions and cell polarity. Annu. Rev. Cell Dev. Biol 2006, 22, 207–235. [Google Scholar]
- Ozdamar, B.; Bose, R.; Barrios-Rodiles, M.; Wang, H.R.; Zhang, Y.; Wrana, J.L. Regulation of the polarity protein Par6 by TGFbeta receptors controls epithelial cell plasticity. Science 2005, 307, 1603–1609. [Google Scholar]
- Nolan, M.E.; Aranda, V.; Lee, S.; Lakshmi, B.; Basu, S.; Allred, D.C.; Muthuswamy, S.K. The polarity protein Par6 induces cell proliferation and is overexpressed in breast cancer. Cancer Res 2008, 68, 8201–8209. [Google Scholar]
- Eder, A.M.; Sui, X.; Rosen, D.G.; Nolden, L.K.; Cheng, K.W.; Lahad, J.P.; Kango-Singh, M.; Lu, K.H.; Warneke, C.L.; Atkinson, E.N.; et al. Atypical PKCiota contributes to poor prognosis through loss of apical-basal polarity and cyclin E overexpression in ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 12519–12524. [Google Scholar]
- Regala, R.P.; Weems, C.; Jamieson, L.; Copland, J.A.; Thompson, E.A.; Fields, A.P. Atypical protein kinase Ciota plays a critical role in human lung cancer cell growth and tumorigenicity. J. Biol. Chem 2005, 280, 31109–31115. [Google Scholar]
- Kunnev, D.; Ivanov, I.; Ionov, Y. Par-3 partitioning defective 3 homolog (C. elegans) and androgen-induced prostate proliferative shutoff associated protein genes are mutationally inactivated in prostate cancer cells. BMC Cancer 2009, 9, 318. [Google Scholar]
- Zen, K.; Yasui, K.; Gen, Y.; Dohi, O.; Wakabayashi, N.; Mitsufuji, S.; Itoh, Y.; Zen, Y.; Nakanuma, Y.; Taniwaki, M.; et al. Defective expression of polarity protein PAR-3 gene (PARD3) in esophageal squamous cell carcinoma. Oncogene 2009, 28, 2910–2918. [Google Scholar]
- Zitzelsberger, H.; Hieber, L.; Richter, H.; Unger, K.; Briscoe, C.V.; Peddie, C.; Riches, A. Gene amplification of atypical PKC-binding PARD3 in radiation-transformed neoplastic retinal pigment epithelial cell lines. Genes Chromosomes Cancer 2004, 40, 55–59. [Google Scholar]
- Fang, C.M.; Xu, Y.H. Down-Regulated expression of atypical PKC-binding domain deleted asip isoforms in human hepatocellular carcinomas. Cell Res 2001, 11, 223–229. [Google Scholar]
- Gao, L.; Macara, I.G.; Joberty, G. Multiple splice variants of Par3 and of a novel related gene, Par3L, produce proteins with different binding properties. Gene 2002, 294, 99–107. [Google Scholar]
- Kohjima, M.; Noda, Y.; Takeya, R.; Saito, N.; Takeuchi, K.; Sumimoto, H. PAR3beta, a novel homologue of the cell polarity protein PAR3, localizes to tight junctions. Biochem. Biophys. Res. Commun 2002, 299, 641–646. [Google Scholar]
- Yoshii, T.; Mizuno, K.; Hirose, T.; Nakajima, A.; Sekihara, H.; Ohno, S. sPAR-3, a splicing variant of PAR-3, shows cellular localization and an expression pattern different from that of PAR-3 during enterocyte polarization. Am. J. Physiol. Gastrointest. Liver Physiol 2005, 288, G564–G570. [Google Scholar]
- Wang, Y.; Du, D.; Fang, L.; Yang, G.; Zhang, C.; Zeng, R.; Ullrich, A.; Lottspeich, F.; Chen, Z. Tyrosine phosphorylated Par3 regulates epithelial tight junction assembly promoted by EGFR signaling. EMBO J 2006, 25, 5058–5070. [Google Scholar]
- Wang, X.; Nie, J.; Zhou, Q.; Liu, W.; Zhu, F.; Chen, W.; Mao, H.; Luo, N.; Dong, X.; Yu, X. Downregulation of Par-3 expression and disruption of Par complex integrity by TGF-beta during the process of epithelial to mesenchymal transition in rat proximal epithelial cells. Biochim. Biophys. Acta 2008, 1782, 51–59. [Google Scholar]
- Mishima, A.; Suzuki, A.; Enaka, M.; Hirose, T.; Mizuno, K.; Ohnishi, T.; Mohri, H.; Ishigatsubo, Y.; Ohno, S. Over-Expression of PAR-3 suppresses contact-mediated inhibition of cell migration in MDCK cells. Genes Cells 2002, 7, 581–596. [Google Scholar]
- Izaki, T.; Kamakura, S.; Kohjima, M.; Sumimoto, H. Phosphorylation-Dependent binding of 14-3-3 to Par3beta, a human Par3-related cell polarity protein. Biochem. Biophys. Res. Commun 2005, 329, 211–218. [Google Scholar]
- Ko, B.S.; Chang, T.C.; Hsu, C.; Chen, Y.C.; Shen, T.L.; Chen, S.C.; Wang, J.; Wu, K.K.; Jan, Y.J.; Liou, J.Y. Overexpression of 14-3-3epsilon predicts tumour metastasis and poor survival in hepatocellular carcinoma. Histopathology 2011, 58, 705–711. [Google Scholar]
- Ko, B.S.; Lai, I.R.; Chang, T.C.; Liu, T.A.; Chen, S.C.; Wang, J.; Jan, Y.J.; Liou, J.Y. Involvement of 14-3-3gamma overexpression in extrahepatic metastasis of hepatocellular carcinoma. Hum. Pathol 2011, 42, 129–135. [Google Scholar]
- Liu, T.A.; Jan, Y.J.; Ko, B.S.; Chen, S.C.; Liang, S.M.; Hung, Y.L.; Hsu, C.; Shen, T.L.; Lee, Y.M.; Chen, P.F.; et al. Increased expression of 14-3-3beta promotes tumor progression and predicts extrahepatic metastasis and worse survival in hepatocellular carcinoma. Am. J. Pathol 2011, 179, 2698–2708. [Google Scholar]
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis 1999, 19, 329–338. [Google Scholar]
- Barnes, D.M.; Harris, W.H.; Smith, P.; Millis, R.R.; Rubens, R.D. Immunohistochemical determination of oestrogen receptor: Comparison of different methods of assessment of staining and correlation with clinical outcome of breast cancer patients. Br. J. Cancer 1996, 74, 1445–1451. [Google Scholar]
- Chang, G.C.; Liu, K.J.; Hsieh, C.L.; Hu, T.S.; Charoenfuprasert, S.; Liu, H.K.; Luh, K.T.; Hsu, L.H.; Wu, C.W.; Ting, C.C.; et al. Identification of alpha-enolase as an autoantigen in lung cancer: Its overexpression is associated with clinical outcomes. Clin. Cancer Res 2006, 12, 5746–5754. [Google Scholar]
- Jan, Y.J.; Ko, B.S.; Hsu, C.; Chang, T.C.; Chen, S.C.; Wang, J.; Liou, J.Y. Overexpressed focal adhesion kinase predicts a higher incidence of extrahepatic metastasis and worse survival in hepatocellular carcinoma. Hum. Pathol 2009, 40, 1384–1390. [Google Scholar]
- Lai, I.R.; Chu, P.Y.; Lin, H.S.; Liou, J.Y.; Jan, Y.J.; Lee, J.C.; Shen, T.L. Phosphorylation of focal adhesion kinase at Tyr397 in gastric carcinomas and its clinical significance. Am. J. Pathol 2010, 177, 1629–1637. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Par-3 positivity (Q-score ≥ 2)% (n) | p-Value |
|---|---|---|
| Overall (n = 111) | 42.3% (47) | |
| Age | ||
| ≥60 years (n = 55) | 40.0% (22) | NS |
| <60 years (n = 56) | 44.6% (25) | |
| Gender | ||
| Male (n = 84) | 42.9% (36) | NS |
| Female (n = 27) | 40.7% (11) | |
| Histology grade | ||
| 1 (n = 7) | 42.9% (3) | NS |
| 2 (n = 79) | 41.8% (33) | |
| 3 (n = 25) | 44.0% (11) | |
| Types of surgery | ||
| Wedge resection (n = 39) | 38.5% (15) | NS |
| Segmentectomy (n = 54) | 38.9% (21) | |
| Lobectomy (n = 18) | 61.1% (11) | |
| Surgical margin | ||
| Free (n = 84) | 42.9% (36) | NS |
| Involved (n = 27) | 40.7% (11) | |
| BCLC staging | ||
| Not available (n = 5) | ||
| Early (stage A1 to A4) (n = 56) | 44.6% (25) | NS |
| Intermediate (stage B) (n = 49) | 40.8% (20) | |
| Advanced (stage C) (n = 1) | 100.0% (1) | |
| Tumor size | ||
| ≥5.0 cm (n = 36) | 50.0% (18) | NS |
| <5.0 cm (n = 75) | 38.7% (29) | |
| Tumor multiplicity | ||
| Single (n = 86) | 50.0% (43) | 0.002 * |
| Multiple (n = 25) | 16.0% (4) | |
| Capsular formation | ||
| Not available (n = 8) | NS | |
| Yes (n = 60) | 41.7% (25) | |
| No (n = 43) | 39.5% (17) | |
| Micro-vascular thrombi | ||
| Yes (n = 48) | 45.8% (22) | NS |
| No (n = 63) | 39.7% (25) | |
| Liver cirrhosis | ||
| Not available (n = 3) | NS | |
| Yes (n = 56) | 48.2% (27) | |
| No (n = 52) | 38.5% (20) | |
| Viral hepatitis | ||
| Not available (n = 7) | ||
| Hepatitis B (n = 56) | 41.1% (23) | NS |
| Hepatitis C (n = 30) | 43.3% (13) | |
| Both (n = 15) | 40.0% (6) | |
| None (n = 3) | 66.7% (2) | |
| Alpha-fetoprotein level | ||
| Not available (n = 12) | 0.046 * | |
| ≥80 ng/mL (n = 36) | 55.6% (20) | |
| <80 ng/mL (n = 63) | 34.9% (22) | |
| Subsequent extrahepatic metastasis | ||
| Yes (n = 31) | 58.1% (18) | 0.037 * |
| No (n = 80) | 36.3% (29) | |
| 14-3-3ɛ expression | ||
| Yes (n = 68) | 51.5% (35) | 0.014 * |
| No (n = 43) | 27.9% (12) |
| Variables | p-Value |
|---|---|
| Histology grade (1 + 2 : 3) | NS |
| Presence of liver cirrhosis (No : Yes) | NS |
| Par-3 expression (negative : positive) | 0.037 * |
| Bulky tumor (≥5.0 cm : <5.0 cm) | NS |
| Surgical margin (free : involved) | NS |
| Capsule formation (no : yes) | NS |
| Vascular thrombi (no : yes) | NS |
| BCLC staging (Stage A : B to C) | NS |
| Variables | Overall survival | Progression-free survival | ||
|---|---|---|---|---|
| Hazard ratio (95% CI) | p-Value | Hazard ratio (95% CI) | p-Value | |
| Par-3 expression (negative : positive) | 2.049 (1.082–3.884) | 0.028 * | 1.486 (0.886–2.490) | 0.133 |
| Types of operation (wedge : wider resection) | 0.719 (0.269–1.922) | 0.510 | 0.756 (0.431–1.325) | 0.329 |
| Surgical margin (free : involved) | 1.510 (0.763–2.988) | 0.237 | 1.061 (0.580–1.941) | 0.847 |
| Capsular formation (no : yes) | 1.357 (0.723–2.547) | 0.342 | 1.543 (0.915–2.602) | 0.104 |
| Alpha-fetoprotein level (low : high) | 1.824 (0.986–3.412) | 0.059 # | 1.757 (1.064–2.898) | 0.028 * |
| Liver cirrhosis (no : yes) | 1.294 (0.651–2.571) | 0.463 | 1.059 (0.598–1.875) | 0.845 |
| BCLC stage (A : B and C) | 1.861 (0.902–3.838) | 0.093 # | 1.555 (0.872–2.775) | 0.135 |
© 2013 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Jan, Y.-J.; Ko, B.-S.; Liu, T.-A.; Wu, Y.-M.; Liang, S.-M.; Chen, S.-C.; Wang, J.; Liou, J.-Y. Expression of Partitioning Defective 3 (Par-3) for Predicting Extrahepatic Metastasis and Survival with Hepatocellular Carcinoma. Int. J. Mol. Sci. 2013, 14, 1684-1697. https://doi.org/10.3390/ijms14011684
Jan Y-J, Ko B-S, Liu T-A, Wu Y-M, Liang S-M, Chen S-C, Wang J, Liou J-Y. Expression of Partitioning Defective 3 (Par-3) for Predicting Extrahepatic Metastasis and Survival with Hepatocellular Carcinoma. International Journal of Molecular Sciences. 2013; 14(1):1684-1697. https://doi.org/10.3390/ijms14011684
Chicago/Turabian StyleJan, Yee-Jee, Bor-Sheng Ko, Tzu-An Liu, Yao-Ming Wu, Shu-Man Liang, Shyh-Chang Chen, John Wang, and Jun-Yang Liou. 2013. "Expression of Partitioning Defective 3 (Par-3) for Predicting Extrahepatic Metastasis and Survival with Hepatocellular Carcinoma" International Journal of Molecular Sciences 14, no. 1: 1684-1697. https://doi.org/10.3390/ijms14011684
APA StyleJan, Y. -J., Ko, B. -S., Liu, T. -A., Wu, Y. -M., Liang, S. -M., Chen, S. -C., Wang, J., & Liou, J. -Y. (2013). Expression of Partitioning Defective 3 (Par-3) for Predicting Extrahepatic Metastasis and Survival with Hepatocellular Carcinoma. International Journal of Molecular Sciences, 14(1), 1684-1697. https://doi.org/10.3390/ijms14011684