L/N-Type Calcium Channel Blocker Cilnidipine Added to Renin-Angiotensin Inhibition Improves Ambulatory Blood Pressure Profile and Suppresses Cardiac Hypertrophy in Hypertension with Chronic Kidney Disease

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Effects of Cilnidipine on Ambulatory BP Profile
2.3. Effects of Cilnidipine Substitution on Renal Function, Renin-Angiotensin System, Systemic Sympathetic Nerve Activity, Inflammation and Oxidative Stress
2.4. Effects of Cilnidipine on Power Spectral Analyses of Low-Frequency (LF) and High-Frequency (HF) Activity
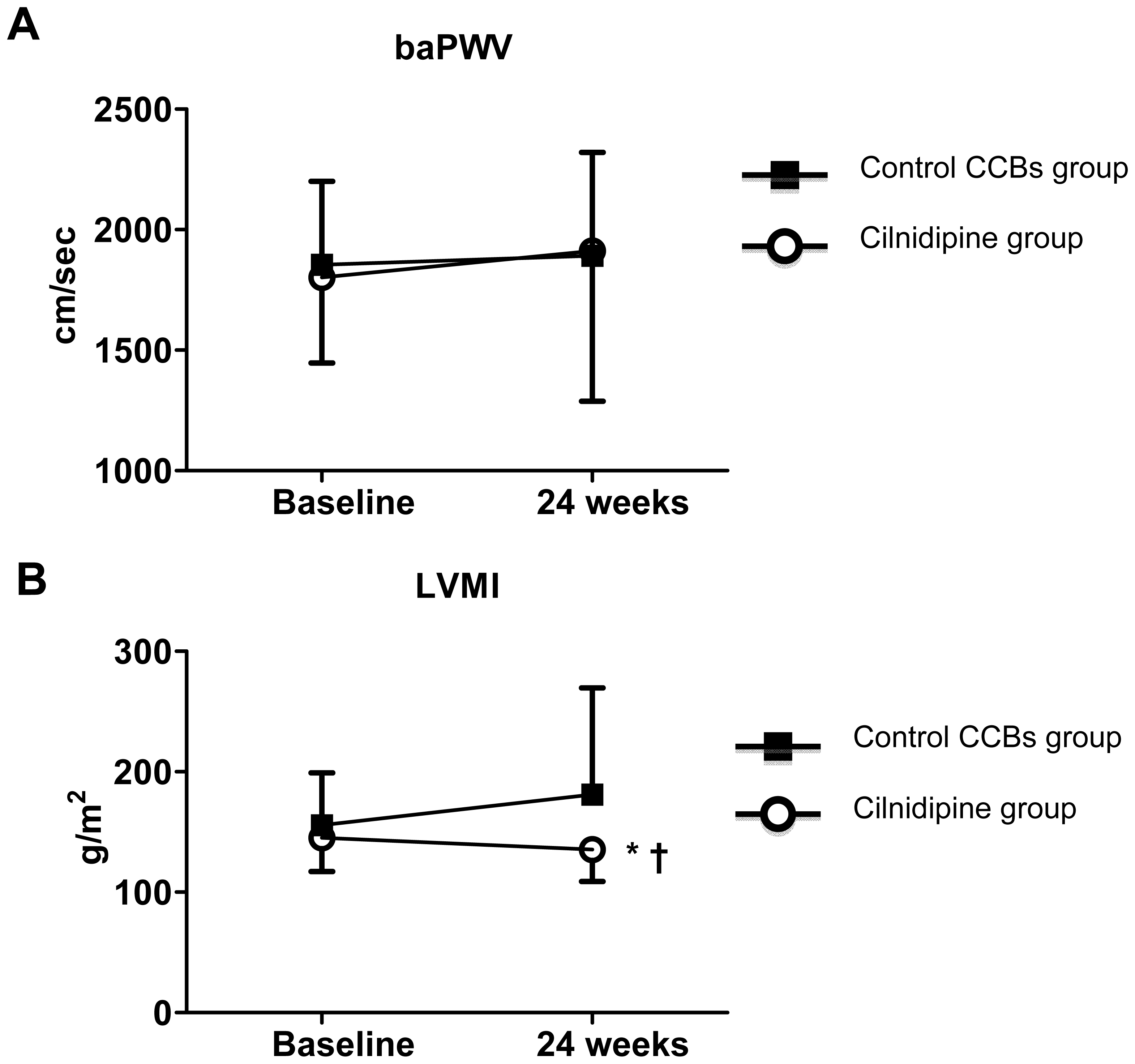
2.5. Effects of Cilnidipine on Parameters of Cardiovascular Function
2.6. Multivariate Regression Analysis for Assessment of Factors Contributing to Regression of Cardiac Hypertrophy
3. Discussion
4. Experimental Section
4.1. Study Design
4.2. Study Participants
4.3. Study Treatment
4.4. Clinical BP Measurement and Ambulatory BP Monitoring
4.5. Power Spectral Analysis of R-R Intervals for Assessment of Cardiac Sympathetic Nerve Activity
4.6. Echocardiography and Brachial-Ankle Pulse Wave Velocity (baPWV)
4.7. Laboratory Measurements
4.8. Statistical Analysis
5. Conclusions
Acknowledgments
Disclosures
Conflicts of Interest
References
- Hodgkinson, J.; Mant, J.; Martin, U.; Guo, B.; Hobbs, F.D.; Deeks, J.J.; Heneghan, C.; Roberts, N.; McManus, R.J. Relative effectiveness of clinic and home blood pressure monitoring compared with ambulatory blood pressure monitoring in diagnosis of hypertension: Systematic review. Br. Med. J 2011, 342, d3621. [Google Scholar]
- Lovibond, K.; Jowett, S.; Barton, P.; Caulfield, M.; Heneghan, C.; Hobbs, F.D.; Hodgkinson, J.; Mant, J.; Martin, U.; Williams, B.; et al. Cost-effectiveness of options for the diagnosis of high blood pressure in primary care: A modelling study. Lancet 2011, 378, 1219–1230. [Google Scholar]
- Kikuya, M.; Hozawa, A.; Ohokubo, T.; Tsuji, I.; Michimata, M.; Matsubara, M.; Ota, M.; Nagai, K.; Araki, T.; Satoh, H.; et al. Prognostic significance of blood pressure and heart rate variabilities: The Ohasama study. Hypertension 2000, 36, 901–906. [Google Scholar]
- Tamura, K.; Kanaoka, T.; Ohsawa, M.; Haku, S.; Azushima, K.; Maeda, A.; Dejima, T.; Wakui, H.; Ozawa, M.; Shigenaga, A.; et al. Emerging concept of anti-hypertensive therapy based on ambulatory blood pressure profile in chronic kidney disease. Am. J. Cardiovasc. Dis 2011, 1, 236–243. [Google Scholar]
- Minutolo, R.; Agarwal, R.; Borrelli, S.; Chiodini, P.; Bellizzi, V.; Nappi, F.; Cianciaruso, B.; Zamboli, P.; Conte, G.; Gabbai, F.B.; et al. Prognostic role of ambulatory blood pressure measurement in patients with nondialysis chronic kidney disease. Arch. Intern. Med 2011, 171, 1090–1098. [Google Scholar]
- Spallone, V.; Bernardi, L.; Ricordi, L.; Solda, P.; Maiello, M.R.; Calciati, A.; Gambardella, S.; Fratino, P.; Menzinger, G. Relationship between the circadian rhythms of blood pressure and sympathovagal balance in diabetic autonomic neuropathy. Diabetes 1993, 42, 1745–1752. [Google Scholar]
- Yanagi, M.; Tamura, K.; Fujikawa, T.; Wakui, H.; Kanaoka, T.; Ohsawa, M.; Azushima, K.; Maeda, A.; Kobori, H.; Umemura, S. The angiotensin II type 1 receptor blocker olmesartan preferentially improves nocturnal hypertension and proteinuria in chronic kidney disease. Hypertens. Res 2013, 36, 262–269. [Google Scholar]
- Orth, S.R.; Amann, K.; Strojek, K.; Ritz, E. Sympathetic overactivity and arterial hypertension in renal failure. Nephrol. Dial. Transplant 2001, 16, 67–69. [Google Scholar]
- Neumann, J.; Ligtenberg, G.; Klein, I.I.; Koomans, H.A.; Blankestijn, P.J. Sympathetic hyperactivity in chronic kidney disease: Pathogenesis, clinical relevance, and treatment. Kidney Int 2004, 65, 1568–1576. [Google Scholar]
- Masuo, K.; Lambert, G.W.; Esler, M.D.; Rakugi, H.; Ogihara, T.; Schlaich, M.P. The role of sympathetic nervous activity in renal injury and end-stage renal disease. Hypertens. Res 2010, 33, 521–528. [Google Scholar]
- Vink, E.E.; de Jager, R.L.; Blankestijn, P.J. Sympathetic hyperactivity in chronic kidney disease: Pathophysiology and (new) treatment options. Curr. Hypertens. Rep 2013, 15, 95–101. [Google Scholar]
- Sakata, K.; Shirotani, M.; Yoshida, H.; Nawada, R.; Obayashi, K.; Togi, K.; Miho, N. Effects of amlodipine and cilnidipine on cardiac sympathetic nervous system and neurohormonal status in essential hypertension. Hypertension 1999, 33, 1447–1452. [Google Scholar]
- Minami, J.; Kawano, Y.; Makino, Y.; Matsuoka, H.; Takishita, S. Effects of cilnidipine, a novel dihydropyridine calcium antagonist, on autonomic function, ambulatory blood pressure and heart rate in patients with essential hypertension. Br. J. Clin. Pharmacol 2000, 50, 615–620. [Google Scholar]
- Takahara, A.; Koganei, H.; Takeda, T.; Iwata, S. Antisympathetic and hemodynamic property of a dual L/N-type Ca(2+) channel blocker cilnidipine in rats. Eur. J. Pharmacol 2002, 434, 43–47. [Google Scholar]
- Minami, J.; Ishimitsu, T.; Higashi, T.; Numabe, A.; Matsuoka, H. Comparison between cilnidipine and nisoldipine with respect to effects on blood pressure and heart rate in hypertensive patients. Hypertens. Res 1998, 21, 215–219. [Google Scholar]
- Hoshide, S.; Kario, K.; Ishikawa, J.; Eguchi, K.; Shimada, K. Comparison of the effects of cilnidipine and amlodipine on ambulatory blood pressure. Hypertens. Res 2005, 28, 1003–1008. [Google Scholar]
- Fujita, T.; Ando, K.; Nishimura, H.; Ideura, T.; Yasuda, G.; Isshiki, M.; Takahashi, K. Antiproteinuric effect of the calcium channel blocker cilnidipine added to renin-angiotensin inhibition in hypertensive patients with chronic renal disease. Kidney Int 2007, 72, 1543–1549. [Google Scholar]
- Konoshita, T.; Makino, Y.; Kimura, T.; Fujii, M.; Wakahara, S.; Arakawa, K.; Inoki, I.; Nakamura, H.; Miyamori, I. A new-generation N/L-type calcium channel blocker leads to less activation of the renin-angiotensin system compared with conventional L type calcium channel blocker. J. Hypertens 2010, 28, 2156–2160. [Google Scholar]
- Kario, K.; Ando, S.I.; Kido, H.; Nariyama, J.; Takiuchi, S.; Yagi, T.; Shimizu, T.; Eguchi, K.; Ohno, M.; Kinoshita, O.; et al. The effects of the L/N-type calcium channel blocker (cilnidipine) on sympathetic hyperactive morning hypertension: results from ACHIEVE-ONE. J. Clin. Hypertens 2013, 15, 133–142. [Google Scholar]
- Fukuda, M.; Masuda, T.; Ogura, M.N.; Moriya, T.; Tanaka, K.; Yamamoto, K.; Ishii, A.; Yonezawa, R.; Noda, C.; Izumi, T. Influence of nifedipine coat-core and amlodipine on systemic arterial stiffness modulated by sympathetic and parasympathetic activity in hypertensive patients. Hypertens. Res 2009, 32, 392–398. [Google Scholar]
- Toal, C.B.; Meredith, P.A.; Elliott, H.L. Long-acting dihydropyridine calcium-channel blockers and sympathetic nervous system activity in hypertension: A literature review comparing amlodipine and nifedipine GITS. Blood Press 2012, 21, 3–10. [Google Scholar]
- Fukumoto, S.; Ishimura, E.; Motoyama, K.; Morioka, T.; Kimoto, E.; Wakikawa, K.; Shoji, S.; Koyama, H.; Shoji, T.; Emoto, M.; et al. Antialbuminuric advantage of cilnidipine compared with L-type calcium channel blockers in type 2 diabetic patients with normoalbuminuria and microalbuminuria. Diabetes Res. Clin. Pract 2012, 97, 91–98. [Google Scholar]
- Abe, M.; Okada, K.; Maruyama, N.; Matsumoto, S.; Maruyama, T.; Fujita, T.; Matsumoto, K.; Soma, M. Benidipine reduces albuminuria and plasma aldosterone in mild-to-moderate stage chronic kidney disease with albuminuria. Hypertens. Res 2011, 34, 268–273. [Google Scholar]
- Takenaka, T.; Seto, T.; Okayama, M.; Kojima, E.; Nodaira, Y.; Sueyoshi, K.; Kikuta, T.; Watanabe, Y.; Inoue, T.; Takane, H.; et al. Long-term effects of calcium antagonists on augmentation index in hypertensive patients with chronic kidney disease: A randomized controlled study. Am. J. Nephrol 2012, 35, 416–423. [Google Scholar]
- Ohmori, S.; Matsumura, K.; Kajioka, T.; Fukuhara, M.; Abe, I.; Fujishima, M. Left ventricular mass predicted by a single reading of ambulatory blood pressure in essential hypertension. Hypertens. Res 2000, 23, 311–316. [Google Scholar]
- Oikawa, K.; Ishihara, R.; Maeda, T.; Yamaguchi, K.; Koike, A.; Kawaguchi, H.; Tabata, Y.; Murotani, N.; Itoh, H. Prognostic value of heart rate variability in patients with renal failure on hemodialysis. Int. J. Cardiol 2009, 131, 370–377. [Google Scholar]
- Pop-Busui, R.; Evans, G.W.; Gerstein, H.C.; Fonseca, V.; Fleg, J.L.; Hoogwerf, B.J.; Genuth, S.; Grimm, R.H.; Corson, M.A.; Prineas, R. Effects of cardiac autonomic dysfunction on mortality risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Diabetes Care 2010, 33, 1578–1584. [Google Scholar]
- Chandra, P.; Sands, R.L.; Gillespie, B.W.; Levin, N.W.; Kotanko, P.; Kiser, M.; Finkelstein, F.; Hinderliter, A.; Pop-Busui, R.; Rajagopalan, S.; et al. Predictors of heart rate variability and its prognostic significance in chronic kidney disease. Nephrol. Dial. Transplant 2012, 27, 700–709. [Google Scholar]
- Kingwell, B.A.; Thompson, J.M.; Kaye, D.M.; McPherson, G.A.; Jennings, G.L.; Esler, M.D. Heart rate spectral analysis, cardiac norepinephrine spillover, and muscle sympathetic nerve activity during human sympathetic nervous activation and failure. Circulation 1994, 90, 234–240. [Google Scholar]
- Watson, A.M.; Hood, S.G.; Ramchandra, R.; McAllen, R.M.; May, C.N. Increased cardiac sympathetic nerve activity in heart failure is not due to desensitization of the arterial baroreflex. Am. J. Physiol. Heart Circ. Physiol 2007, 293, H798–H804. [Google Scholar]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis 2009, 53, 982–992. [Google Scholar]
- Mitsuhashi, H.; Tamura, K.; Yamauchi, J.; Ozawa, M.; Yanagi, M.; Dejima, T.; Wakui, H.; Masuda, S.; Azuma, K.; Kanaoka, T.; et al. Effect of losartan on ambulatory short-term blood pressure variability and cardiovascular remodeling in hypertensive patients on hemodialysis. Atherosclerosis 2009, 207, 186–190. [Google Scholar]
- Masuda, S.; Tamura, K.; Wakui, H.; Kanaoka, T.; Ohsawa, M.; Maeda, A.; Dejima, T.; Yanagi, M.; Azuma, K.; Umemura, S. Effects of angiotensin II type 1 receptor blocker on ambulatory blood pressure variability in hypertensive patients with overt diabetic nephropathy. Hypertens. Res 2009, 32, 950–955. [Google Scholar]
- Kanaoka, T.; Tamura, K.; Ohsawa, M.; Wakui, H.; Maeda, A.; Dejima, T.; Azushima, K.; Haku, S.; Mitsuhashi, H.; Yanagi, M.; et al. Effects of aliskiren-based therapy on ambulatory blood pressure profile, central hemodynamics, and arterial stiffness in nondiabetic mild to moderate hypertensive patients. J. Clin. Hypertens 2012, 14, 522–529. [Google Scholar]
- Shigenaga, A.; Tamura, K.; Dejima, T.; Ozawa, M.; Wakui, H.; Masuda, S.; Azuma, K.; Tsurumi-Ikeya, Y.; Mitsuhashi, H.; Okano, Y.; et al. Effects of angiotensin II type 1 receptor blocker on blood pressure variability and cardiovascular remodeling in hypertensive patients on chronic peritoneal dialysis. Nephron. Clin. Pract 2009, 112, c31–c40. [Google Scholar]
- Kanaoka, T.; Tamura, K.; Moriya, T.; Tanaka, K.; Konno, Y.; Kondoh, S.; Toyoda, M.; Umezono, T.; Fujikawa, T.; Ohsawa, M.; et al. Effects of multiple factorial intervention on ambulatory BP profile and renal function in hypertensive Type 2 diabetic patients with overt nephropathy—A pilot study. Clin. Exp. Hypertens 2011, 33, 255–263. [Google Scholar]
- Okano, Y.; Tochikubo, O.; Umemura, S. Relationship between base blood pressure during sleep and health-related quality of life in healthy adults. J. Hum. Hypertens 2007, 21, 135–140. [Google Scholar]
- Yamashina, A.; Tomiyama, H.; Takeda, K.; Tsuda, H.; Arai, T.; Hirose, K.; Koji, Y.; Hori, S.; Yamamoto, Y. Validity, reproducibility, and clinical significance of noninvasive brachial-ankle pulse wave velocity measurement. Hypertens. Res 2002, 25, 359–364. [Google Scholar]


{kind=link}
| Variables | Control CCBs group | Cilnidipine group | p |
|---|---|---|---|
| n = 24 | n = 21 | ||
| Age (years) | 70.3 ± 11.0 | 69.5 ± 9.9 | NS |
| Male (%) | 54.2 | 76.2 | NS |
| BMI (kg/m2) | 24.2 ± 5.0 | 24.9 ± 4.3 | NS |
| Smoking (%) | 45.8 | 61.9 | |
| Diabetes (%) | 37.5 | 38.1 | NS |
| Dyslipidemia (%) | 54.2 | 42.9 | NS |
| Coronary artery disease (%) | 0.0 | 4.8 | NS |
| Cerebral vascular disease (%) | 16.7 | 19.0 | NS |
| Cause of CKD (n (%)) | |||
| Nephrosclerosis | 14 (58) | 15 (71) | NS |
| Diabetic nephropathy | 5 (21) | 5 (24) | NS |
| Chronic glomerulonephritis | 3 (13) | 1 (5) | NS |
| Polycystic kidney disease | 1 (4) | 0 (0) | NS |
| Chronic pyelonephritis | 0 (0) | 1 (5) | NS |
| Medication (%) | |||
| ARBs | 91.7 | 100 | NS |
| ACEIs | 20.8 | 19.0 | NS |
| DRI | 4.2 | 0.0 | NS |
| α blockers | 29.2 | 38.1 | NS |
| β blockers | 33.3 | 14.3 | NS |
| Diuretics | NS | ||
| Thiazide diuretics | 25.0 | 23.8 | NS |
| Loop diuretics | 16.7 | 4.8 | NS |
| CNS acting drugs | 4.2 | 0.0 | NS |
| Clinic BP | Control CCBs group (n = 24) | Cilnidipine group (n = 21) | ||||
|---|---|---|---|---|---|---|
| Baseline | 24 weeks | Δ | Baseline | 24 weeks | Δ | |
| SBP (mmHg) | 142 ± 16 | 138 ± 16 | −3 ± 18 | 139 ± 16 | 132 ± 13 | −6 ± 14 |
| DBP (mmHg) | 81 ± 9 | 79 ± 7 | −1 ± 10 | 78 ± 13 | 78 ± 13 | 0 ± 11 |
| HR (beats/min) | 70 ± 10 | 70 ± 9 | −1 ± 9 | 69 ± 10 | 69 ± 9 | 0 ± 11 |
| Ambulatory BP | Control CCBs group (n = 24) | Cilnidipine group (n = 21) | ||||
|---|---|---|---|---|---|---|
| Baseline | 24 weeks | Δ | Baseline | 24 weeks | Δ | |
| 24-h | ||||||
| SBP (mmHg) | 133 ± 13 | 137 ± 15 | 3 ± 11 | 131 ± 12 | 127 ± 9 † | −3 ± 9 |
| DBP (mmHg) | 75 ± 8 | 76 ± 9 | 1 ± 6 | 75 ± 8 | 72 ± 7 | −2 ± 6 |
| HR (beats/min) | 65 ± 9 | 68 ± 9 | 2 ± 5 | 68 ± 9 | 64 ± 7 * | −5 ± 9 † |
| SBPV (%) | 12.5 ± 2.7 | 13.8 ± 2.9 | 1.3 ± 2.9 | 14.3 ± 2.7 † | 13.5 ± 2.9 | −1.3 ± 3.1 † |
| DBPV (%) | 13.7 ± 2.5 | 14.7 ± 2.8 | 0.9 ± 2.8 | 14.4 ± 3.6 | 15.0 ± 2.9 | −0.1 ± 4.4 |
| Daytime | ||||||
| SBP (mmHg) | 136 ± 13 | 140 ± 15 | 3 ± 12 | 134 ± 11 | 130 ± 10 † | −3 ± 11 |
| DBP (mmHg) | 77 ± 9 | 79 ± 9 | 2 ± 7 | 77 ± 8 | 75 ± 8 * | −2 ± 8 |
| HR (beats/min) | 68 ± 15 | 71 ± 10 | 3 ± 12 | 70 ± 7 | 67 ± 8 | −4 ± 6 † |
| SBPV (%) | 12.0 ± 2.6 | 13.5 ± 3.2 | 1.3 ± 3.1 | 13.2 ± 2.9 | 12.5 ± 2.9 | −1.0 ± 3.5 |
| DBPV (%) | 13.1 ± 3.0 | 14.1 ± 3.3 | 0.7 ± 3.0 | 13.4 ± 4.0 | 13.2 ± 3.4 | −0.7 ± 4.6 |
| Nighttime | ||||||
| SBP (mmHg) | 126 ± 16 | 128 ± 18 | 0 ± 13 | 122 ± 18 | 120 ± 11 | −2 ± 13 |
| DBP (mmHg) | 71 ± 8 | 71 ± 9 | 1 ± 8 | 69 ± 9 | 67 ± 6 | 0 ± 7 |
| HR (beats/min) | 59 ± 8 | 62 ± 9 | 3 ± 6 | 59 ± 10 | 58 ± 8 | −1 ± 5 † |
| SBPV (%) | 9.4 ± 1.8 | 9.9 ± 2.2 | 0.7 ± 2.5 | 9.7 ± 2.5 | 11.1 ± 3.4 | 1.1 ± 4.7 |
| DBPV (%) | 10.7 ± 3.3 | 11.6 ± 4.1 | 1.2 ± 3.8 | 11.6 ± 3.2 | 13.7 ± 3.6 | 1.3 ± 4.4 |
| Variables | Control CCBs group (n = 24) | Cilnidipine group (n = 21) | ||||
|---|---|---|---|---|---|---|
| Baseline | 24 weeks | Δ | Baseline | 24 weeks | Δ | |
| Renal function | ||||||
| s-Cr (mg/dL) | 1.8 ± 1.0 | 2.0 ± 1.3 | 0.1 ± 0.5 | 2.0 ± 1.2 | 2.1 ± 1.6 | 0.2 ± 0.6 |
| eGFR (mL/min/1.7 m2) | 34.9 ± 17.3 | 34.1 ± 19.3 | −0.5 ± 5.4 | 35.1 ± 17.3 | 35.0 ± 19.0 | −1.1 ± 3.1 |
| UPCR (g/g-Cr) | 1.0 ± 1.2 | 1.1 ± 1.4 | 0.1 ± 0.9 | 1.4 ± 2.6 | 1.1 ± 1.8 | −0.2 ± 1.1 |
| Urinary type IV collagen (g/g-Cr) | 6.8 ± 3.6 | 9.2 ± 8.0 | 2.3 ± 6.1 | 9.5 ± 11.9 | 8.4 ± 7.9 | −1.1 ± 9.0 |
| Endocrine function | ||||||
| PRA (ng/mL/h) | 2.1 ± 2.4 | 3.1 ± 4.4 | 0.9 ± 3.1 | 2.7 ± 4.3 | 2.8 ± 3.7 | 1.0 ± 3.5 |
| PAC (pg/mL) | 69.3 ± 44.2 | 70.7 ± 47.9 | −3.9 ± 25.8 | 66.8 ± 40.6 | 76.1 ± 55.6 | 3.6 ± 46.9 |
| Noradrenaline (μg/mL) | 393 ± 237 | 484 ± 275 * | 87 ± 168 | 276 ± 136 | 364 ± 239 | 82 ± 272 |
| Inflammation and oxidative stress | ||||||
| hs-CRP (mg/dL) | 0.3 ± 0.6 | 0.2 ± 0.2 | −0.1 ± 0.3 | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.0 ± 0.1 |
| Pentosidine (μg/L) | 41.2 ± 25.8 | 41.0 ± 24.6 | −0.8 ± 19.5 | 41.6 ± 23.0 | 46.1 ± 27.6 | −0.2 ± 18.4 |
| Urinary 8-OHdG (ng/mg-Cr) | 4.7 ± 3.5 | 4.1 ± 2.6 | −0.7 ± 3.9 | 4.1 ± 2.3 | 4.1 ± 2.3 | 0.0 ± 3.0 |
| MDA-LDL (u/L) | 110.9 ± 51.5 | 105.0 ± 44.7 | −5.9 ± 46.1 | 93.9 ± 53.7 | 93.9 ± 42.2 | 0.0 ± 54.8 |
| ADMA (μmol/L) | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.0 ± 0.1 | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.0 ± 0.1 |
| Variables | Control CCBs group (n = 24) | Cilnidipine group (n = 21) | ||||
|---|---|---|---|---|---|---|
| Baseline | 24 weeks | Δ | Baseline | 24 weeks | Δ | |
| 24-h LF/HF | 1.3 ± 0.4 | 1.5 ± 0.5 * | 0.2 ± 0.4 | 1.5 ± 0.4 | 1.4 ± 0.4 | −0.1 ± 0.3 † |
| Daytime LF/HF | 1.4 ± 0.4 | 1.6 ± 0.5 * | 0.2 ± 0.4 | 1.5 ± 0.4 | 1.4 ± 0.4 | −0.1 ± 0.4 † |
| Nighttime LF/HF | 1.3 ± 0.5 | 1.4 ± 0.6 | 0.1 ± 0.4 | 1.5 ± 0.6 | 1.3 ± 0.7 | −0.2 ± 0.7 † |
| Variables | Coefficient | 95% interval | p | |
|---|---|---|---|---|
| Lower | Upper | |||
| Age | −0.241 | −2.555 | 0.559 | 0.200 |
| Gender (Male 1, Female 0) | 0.447 | 9.914 | 78.272 | 0.013 * |
| Treatment group | −0.397 | −86.145 | −4.755 | 0.030 * |
| Changes in 24-h SBP | 0.128 | −0.095 | 0.128 | 0.500 |
| Changes in 24-h DBP | −0.293 | −8.390 | 0.983 | 0.117 |
| Changes in 24-h HR | 0.152 | −1.463 | 3.393 | 0.422 |
| Changes in 24-h SBPV | −0.302 | 0.117 | −0.302 | 0.105 |
| Changes in 24-h LF/HF | 0.407 | 7.409 | 105.041 | 0.026 * |
© 2013 by the authors; licensee MDPI, Basel, Switzerland This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kanaoka, T.; Tamura, K.; Wakui, H.; Ohsawa, M.; Azushima, K.; Uneda, K.; Kobayashi, R.; Fujikawa, T.; Tsurumi-Ikeya, Y.; Maeda, A.; et al. L/N-Type Calcium Channel Blocker Cilnidipine Added to Renin-Angiotensin Inhibition Improves Ambulatory Blood Pressure Profile and Suppresses Cardiac Hypertrophy in Hypertension with Chronic Kidney Disease. Int. J. Mol. Sci. 2013, 14, 16866-16881. https://doi.org/10.3390/ijms140816866
Kanaoka T, Tamura K, Wakui H, Ohsawa M, Azushima K, Uneda K, Kobayashi R, Fujikawa T, Tsurumi-Ikeya Y, Maeda A, et al. L/N-Type Calcium Channel Blocker Cilnidipine Added to Renin-Angiotensin Inhibition Improves Ambulatory Blood Pressure Profile and Suppresses Cardiac Hypertrophy in Hypertension with Chronic Kidney Disease. International Journal of Molecular Sciences. 2013; 14(8):16866-16881. https://doi.org/10.3390/ijms140816866
Chicago/Turabian StyleKanaoka, Tomohiko, Kouichi Tamura, Hiromichi Wakui, Masato Ohsawa, Kengo Azushima, Kazushi Uneda, Ryu Kobayashi, Tetsuya Fujikawa, Yuko Tsurumi-Ikeya, Akinobu Maeda, and et al. 2013. "L/N-Type Calcium Channel Blocker Cilnidipine Added to Renin-Angiotensin Inhibition Improves Ambulatory Blood Pressure Profile and Suppresses Cardiac Hypertrophy in Hypertension with Chronic Kidney Disease" International Journal of Molecular Sciences 14, no. 8: 16866-16881. https://doi.org/10.3390/ijms140816866
APA StyleKanaoka, T., Tamura, K., Wakui, H., Ohsawa, M., Azushima, K., Uneda, K., Kobayashi, R., Fujikawa, T., Tsurumi-Ikeya, Y., Maeda, A., Yanagi, M., Toya, Y., & Umemura, S. (2013). L/N-Type Calcium Channel Blocker Cilnidipine Added to Renin-Angiotensin Inhibition Improves Ambulatory Blood Pressure Profile and Suppresses Cardiac Hypertrophy in Hypertension with Chronic Kidney Disease. International Journal of Molecular Sciences, 14(8), 16866-16881. https://doi.org/10.3390/ijms140816866