Antibacterial Surface Treatment for Orthopaedic Implants



Abstract
:1. Introduction
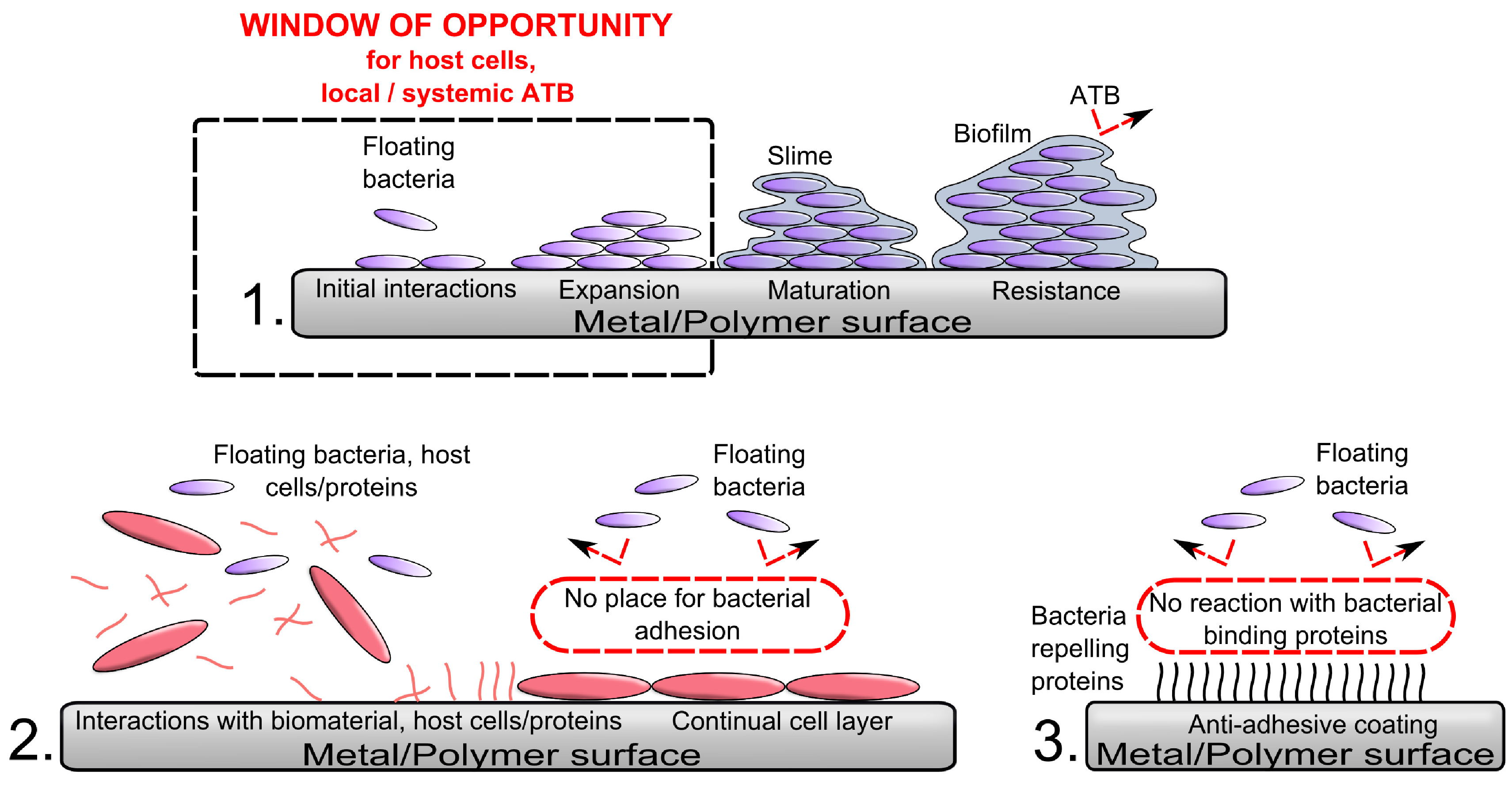
1.1. How to Win the Race for the Surface?

1.2. Brief Overview of Basic Concepts of PJI Prevention
1.3. Indications for Implants with Antibacterial Surface Treatment
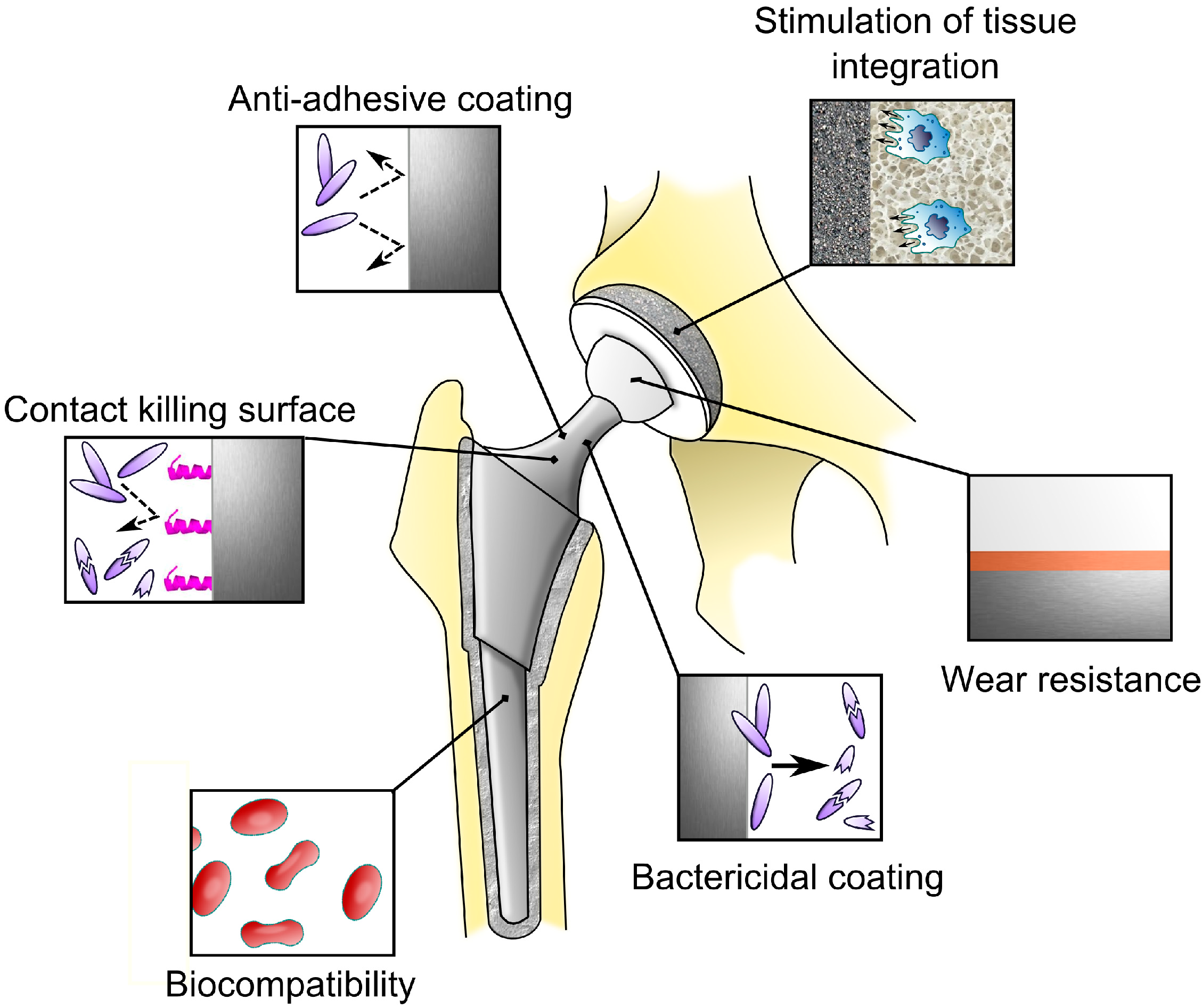
1.4. Rules for Construction of Implants with Anti-Infective Coating

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strategy | Features | Examples | References |
|---|---|---|---|
| Prevention in adhesion and adsorption | Anti-adhesive polymers | [68,69,70,71] | |
| Albumin | [72] | ||
| Super-hydrophobic surfaces | [73,74,75] | ||
| Nano-patterned surface | [76,77,78,79] | ||
| Hydrogels | [80,81,82,83] | ||
| Methods to kill bacteria | Inorganic | Silver nanoparticles | [84,85,86,87,88,89,90] |
| Titanium dioxide | [91,92,93] | ||
| Selenium ion | [94,95,96] | ||
| Copper ion | [97,98] | ||
| Zinc ion | [99,100] | ||
| Organic | Coated or covalently linked antibiotics | [101,102,103,104,105] | |
| Chitosan derivatives | [106,107,108,109] | ||
| Signaling, inhibiting and antimicrobial peptides | [110,111,112,113,114,115] | ||
| Cytokines | [116] | ||
| Enzymes | [117,118] | ||
| Other | Non-antibiotic bactericidal substances | [119] | |
| Combined | Multilayer coating | [120,121,122,123,124] | |
| Synergy material intensification | [125] | ||
| Positively charged polymers | [126] | ||
| Multi-functional and smart coating | Passive | Nanostructured “smart” material | [71,127,128] |
| Active | Concept: sensors conjoined to nanocontainers | [129,130,131,132,133] | |
| Alternative approach | Lytic bacteriophages | [134] |
1.5. General Principles of Thin Surface Modifications
1.6. Remarks on the Testing of Antibacterial Coatings
2. Basic Concepts of Antibacterial Coating

2.1. Anti-Adhesive Approaches

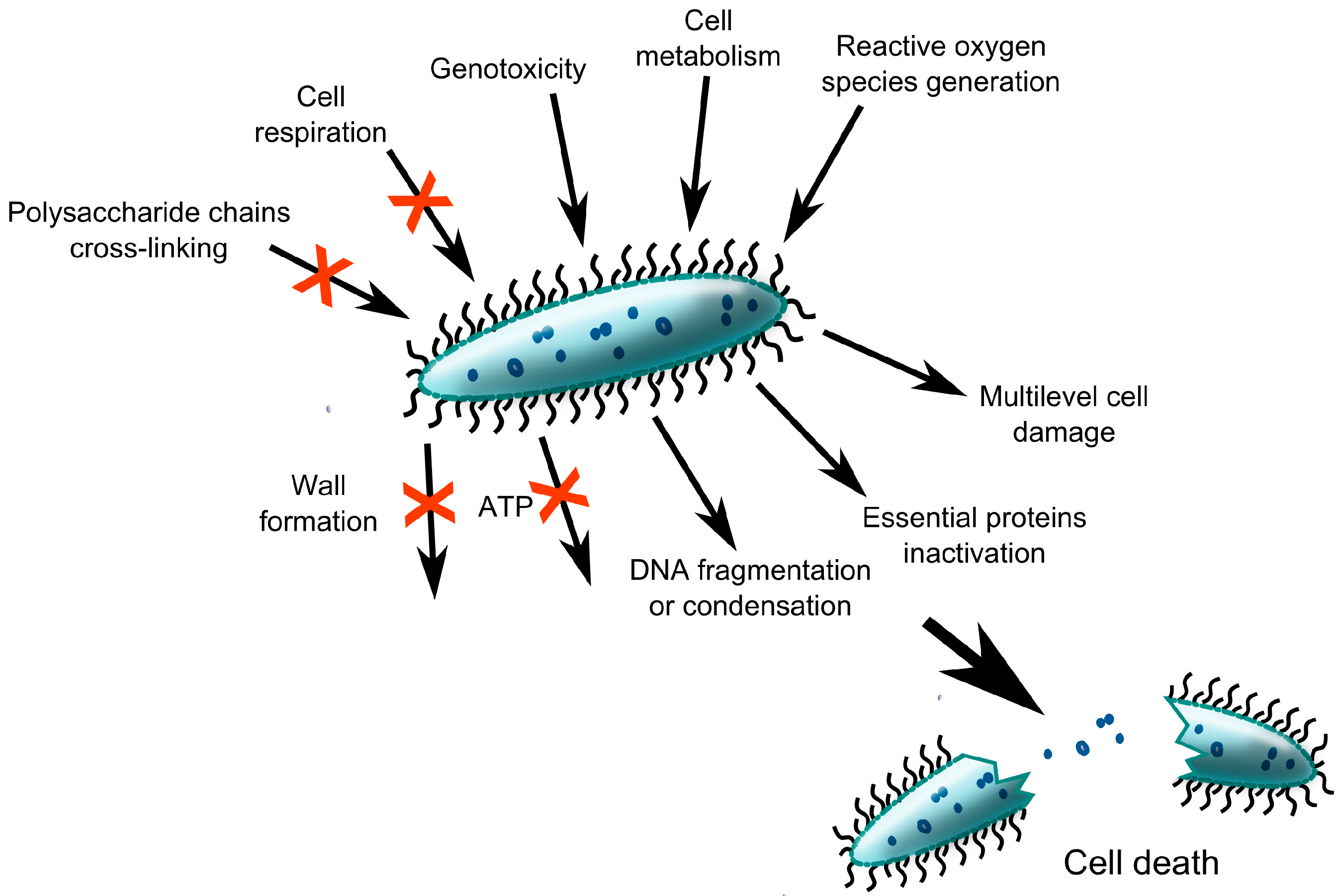
2.2. Surfaces with Intrinsically Antibacterial Properties

2.2.1. Coating of Implant Surface by Anti-Infective Metals
2.2.2. Non-Metal Elements with Antibacterial Properties for Implant Surface Treatment
2.2.3. Antibacterial Coatings of Organic Origin

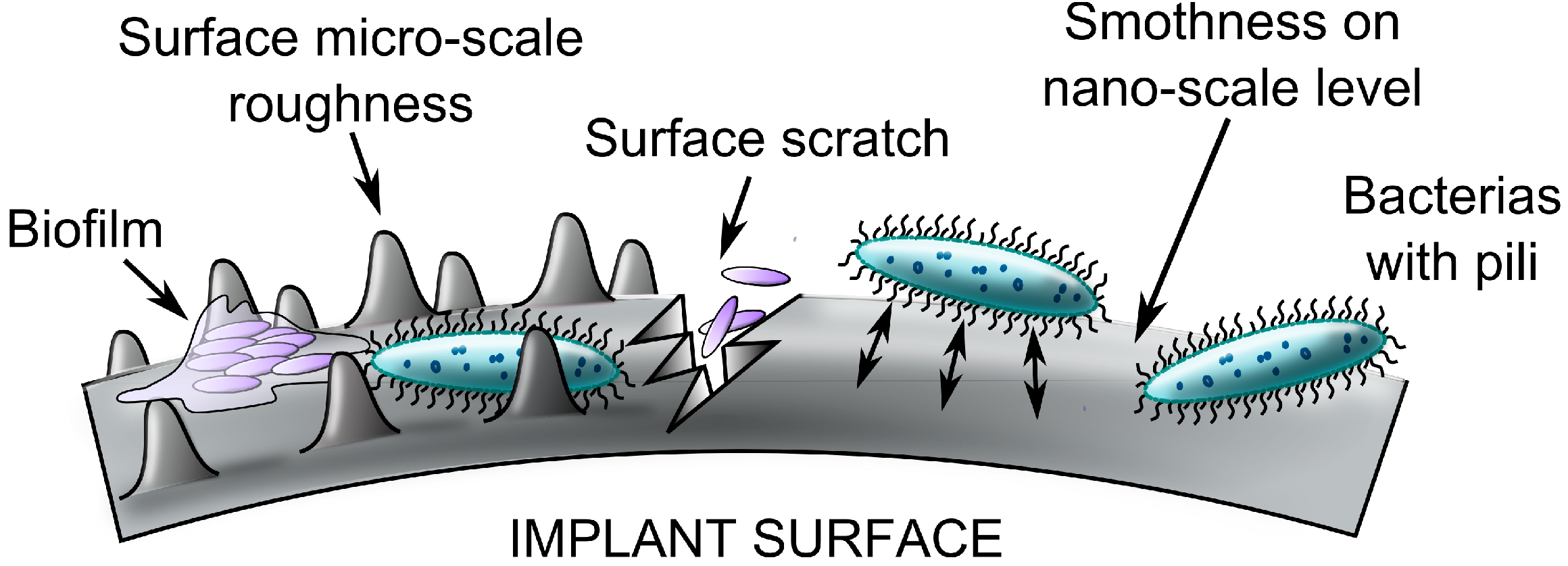
2.2.4. Nanostructured Surfaces and Coatings

3. Multifunctional and Smart Coatings

4. Translation of Anti-Infective Coatings into the Clinical Practice
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cats-Baril, W.; Gehrke, T.; Huff, K.; Kendoff, D.; Maltenfort, M.; Parvizi, J. International consensus on periprosthetic joint infection: Description of the consensus process. Clin. Orthop. Relat. Res. 2013, 471, 4065–4075. [Google Scholar] [CrossRef]
- Lentino, J.R. Prosthetic joint infections: Bane of orthopedists, challenge for infectious disease specialists. Clin. Infect. Dis. 2003, 36, 1157–1161. [Google Scholar]
- Dale, H.; Hallan, G.; Hallan, G.; Espehaug, B.; Havelin, L.I.; Engesaeter, L.B. Increasing risk of revision due to deep infection after hip arthroplasty. Acta Orthop. 2009, 80, 639–645. [Google Scholar]
- Aggarwal, V.K.; Bakhshi, H.; Ecker, N.U.; Parvizi, J.; Gehrke, T.; Kendoff, D. Organism profile in periprosthetic joint infection: Pathogens differ at two arthroplasty infection referral centers in Europe and in the United States. J. Knee Surg. 2014, 10. [Google Scholar] [CrossRef]
- Zmistowski, B.; Karam, J.A.; Durinka, J.B.; Casper, D.S.; Parvizi, J. Periprosthetic joint infection increases the risk of one-year mortality. J. Bone Jt. Surg. Am. 2013, 95, 2177–2184. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the United States. J. Arthroplast. 2012, 27, 61–65. [Google Scholar]
- Illingworth, K.D.; Mihalko, W.M.; Parvizi, J.; Sculco, T.; McArthur, B.; el Bitar, Y.; Saleh, K.J. How to minimize infection and thereby maximize patient outcomes in total joint arthroplasty: A multicenter approach: AAOS exhibit selection. J. Bone Jt. Surg. Am. 2013, 95, e50. [Google Scholar]
- An, Y.H.; Friedman, R.J. Prevention of sepsis in total joint arthroplasty. J. Hosp. Infect. 1996, 33, 93–108. [Google Scholar] [CrossRef]
- Humphreys, H. Surgical site infection, ultraclean ventilated operating theatres and prosthetic joint surgery: Where now? J. Hosp. Infect. 2012, 81, 71–72. [Google Scholar]
- Zhang, S.Y.; Herman, M.; Ciancanelli, M.J.; de Diego, P.R.; Sancho-Shimizu, V.; Abel, L.; Casanova, J.L. TLR3 immunity to infection in mice and humans. Curr. Opin. Immunol. 2013, 25, 19–33. [Google Scholar]
- Ziakas, P.D.; Prodromou, M.L.; el Khoury, J.; Zintzaras, E.; Mylonakis, E. The role of TLR4 896 A>G and 1196 C>T in susceptibility to infections: A review and meta-analysis of genetic association studies. PLoS One 2013, 8, e81047. [Google Scholar]
- Navratilova, Z.; Gallo, J.; Mrazek, F.; Lostak, J.; Petrek, M. MBL2 gene variation affecting serum MBL is associated with prosthetic joint infection in Czech patients after total joint arthroplasty. Tissue Antigens 2012, 80, 444–451. [Google Scholar]
- Malik, M.H.; Bayat, A.; Jury, F.; Kay, P.R.; Ollier, W.E. Genetic susceptibility to total hip arthroplasty failure—Positive association with mannose-binding lectin. J. Arthroplast. 2007, 22, 265–270. [Google Scholar] [CrossRef]
- Pruzansky, J.S.; Bronson, M.J.; Grelsamer, R.P.; Strauss, E.; Moucha, C.S. Prevalence of modifiable surgical site infection risk factors in hip and knee joint arthroplasty patients at an urban academic hospital. J. Arthroplast. 2014, 29, 272–276. [Google Scholar] [CrossRef]
- Aggarwal, V.K.; Tischler, E.H.; Lautenbach, C.; Williams, G.R., Jr.; Abboud, J.A.; Altena, M.; Bradbury, T.L.; Calhoun, J.H.; Dennis, D.A.; del Gaizo, D.J.; et al. Mitigation and education. J. Arthroplast. 2014, 29, 19–25. [Google Scholar] [CrossRef]
- Gristina, A.G.; Naylor, P.; Myrvik, Q. Infections from biomaterials and implants: A race for the surface. Med. Prog. Technol. 1988, 14, 205–224. [Google Scholar]
- Busscher, H.J.; van der Mei, H.C. How do bacteria know they are on a surface and regulate their response to an adhering state? PLoS Pathog. 2012, 8, e1002440. [Google Scholar] [CrossRef]
- Costerton, W.; Veeh, R.; Shirtliff, M.; Pasmore, M.; Post, C.; Ehrlich, G. The application of biofilm science to the study and control of chronic bacterial infections. J. Clin. Investig. 2003, 112, 1466–1477. [Google Scholar] [CrossRef]
- Chen, Y.; Busscher, H.J.; van der Mei, H.C.; Norde, W. Statistical analysis of long- and short-range forces involved in bacterial adhesion to substratum surfaces as measured using atomic force microscopy. Appl. Environ. Microbiol. 2011, 77, 5065–5070. [Google Scholar] [CrossRef]
- Wang, Y.; Subbiahdoss, G.; de Vries, J.; Libera, M.; van der Mei, H.C.; Busscher, H.J. Effect of adsorbed fibronectin on the differential adhesion of osteoblast-like cells and Staphylococcus aureus with and without fibronectin-binding proteins. Biofouling 2012, 28, 1011–1021. [Google Scholar] [CrossRef]
- Wagner, C.; Aytac, S.; Hansch, G.M. Biofilm growth on implants: Bacteria prefer plasma coats. Int. J. Artif. Organs 2011, 34, 811–817. [Google Scholar] [CrossRef]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of orthopedic implants with emphasis on bacterial adhesion process and techniques used in studying bacterial-material interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef]
- Chagnot, C.; Zorgani, M.A.; Astruc, T.; Desvaux, M. Proteinaceous determinants of surface colonization in bacteria: Bacterial adhesion and biofilm formation from a protein secretion perspective. Front. Microbiol. 2013, 4. [Google Scholar] [CrossRef]
- Jenney, C.R.; Anderson, J.M. Adsorbed serum proteins responsible for surface dependent human macrophage behavior. J. Biomed. Mater. Res. 2000, 49, 435–447. [Google Scholar] [CrossRef]
- Thevenot, P.; Hu, W.; Tang, L. Surface chemistry influences implant biocompatibility. Curr. Top. Med. Chem. 2008, 8, 270–280. [Google Scholar] [CrossRef]
- Roach, P.; Eglin, D.; Rohde, K.; Perry, C.C. Modern biomaterials: A review—Bulk properties and implications of surface modifications. J. Mater. Sci. Mater. Med. 2007, 18, 1263–1277. [Google Scholar] [CrossRef]
- Wilson, C.J.; Clegg, R.E.; Leavesley, D.I.; Pearcy, M.J. Mediation of biomaterial-cell interactions by adsorbed proteins: A review. Tissue Eng. 2005, 11, 1–18. [Google Scholar] [CrossRef]
- Stoodley, P.; Ehrlich, G.D.; Sedghizadeh, P.P.; Hall-Stoodley, L.; Baratz, M.E.; Altman, D.T.; Sotereanos, N.G. Orthopaedic biofilm infections. Curr. Orthop. Pract. 2011, 22, 558–563. [Google Scholar] [CrossRef]
- Costerton, J.W.; Stewart, P.S.; Greenberg, E.P. Bacterial biofilms: A common cause of persistent infections. Science 1999, 284, 1318–1322. [Google Scholar] [CrossRef]
- Laverty, G.; Gorman, S.P.; Gilmore, B.F. Biomolecular mechanisms of staphylococcal biofilm formation. Future Microbiol. 2013, 8, 509–524. [Google Scholar] [CrossRef] [Green Version]
- Foster, T.J.; Geoghegan, J.A.; Ganesh, V.K.; Hook, M. Adhesion, invasion and evasion: The many functions of the surface proteins of Staphylococcus aureus. Nat. Rev. Microbiol. 2014, 12, 49–62. [Google Scholar]
- Fux, C.A.; Costerton, J.W.; Stewart, P.S.; Stoodley, P. Survival strategies of infectious biofilms. Trends Microbiol. 2005, 13, 34–40. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef]
- Gardner, A.B.; Lee, S.K.; Woods, E.C.; Acharya, A.P. Biomaterials-based modulation of the immune system. Biomed. Res. Int. 2013, 2013. [Google Scholar] [CrossRef]
- Harvey, A.G.; Hill, E.W.; Bayat, A. Designing implant surface topography for improved biocompatibility. Expert Rev. Med. Devices 2013, 10, 257–267. [Google Scholar]
- Cohen, H.C.; Joyce, E.J.; Kao, W.J. Biomaterials selectively modulate interactions between human blood-derived polymorphonuclear leukocytes and monocytes. Am. J. Pathol. 2013, 182, 2180–2190. [Google Scholar] [CrossRef]
- Busscher, H.J.; van der Mei, H.C.; Subbiahdoss, G.; Jutte, P.C.; van den Dungen, J.J.; Zaat, S.A.; Schultz, M.J.; Grainger, D.W. Biomaterial-associated infection: Locating the finish line in the race for the surface. Sci. Transl. Med. 2012, 4, 153rv10. [Google Scholar]
- Nish, S.; Medzhitov, R. Host defense pathways: Role of redundancy and compensation in infectious disease phenotypes. Immunity 2011, 34, 629–636. [Google Scholar] [CrossRef]
- Zimmerli, W.; Lew, P.D.; Waldvogel, F.A. Pathogenesis of foreign body infection. Evidence for a local granulocyte defect. J. Clin. Investig. 1984, 73, 1191–1200. [Google Scholar] [CrossRef]
- Higgins, D.M.; Basaraba, R.J.; Hohnbaum, A.C.; Lee, E.J.; Grainger, D.W.; Gonzalez-Juarrero, M. Localized immunosuppressive environment in the foreign body response to implanted biomaterials. Am. J. Pathol. 2009, 175, 161–170. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Pathogenesis of implant-associated infection: The role of the host. Semin. Immunopathol. 2011, 33, 295–306. [Google Scholar] [CrossRef]
- Berbari, E.F.; Osmon, D.R.; Lahr, B.; Eckel-Passow, J.E.; Tsaras, G.; Hanssen, A.D.; Mabry, T.; Steckelberg, J.; Thompson, R. The Mayo prosthetic joint infection risk score: Implication for surgicalsite infection reporting and risk stratification. Infect. Control Hosp. Epidemiol. 2012, 33, 774–781. [Google Scholar] [CrossRef]
- Engelsman, A.F.; Saldarriaga-Fernandez, I.C.; Nejadnik, M.R.; van Dam, G.M.; Francis, K.P.; Ploeg, R.J.; Busscher, H.J.; van der Mer, H.C. The risk of biomaterial-associated infection after revision surgery due to an experimental primary implant infection. Biofouling 2010, 26, 761–767. [Google Scholar] [CrossRef]
- Gastmeier, P.; Breier, A.C.; Brandt, C. Influence of laminar airflow on prosthetic joint infections: A systematic review. J. Hosp. Infect. 2012, 81, 73–78. [Google Scholar] [CrossRef]
- Merollini, K.M.; Zheng, H.; Graves, N. Most relevant strategies for preventing surgical site infection after total hip arthroplasty: Guideline recommendations and expert opinion. Am. J. Infect. Control 2013, 41, 221–226. [Google Scholar] [CrossRef]
- Cristina, M.L.; Spagnolo, A.M.; Sartini, M.; Panatto, D.; Gasparini, R.; Orlando, P.; Ottria, G.; Perdelli, F. Can particulate air sampling predict microbial load in operating theatres for arthroplasty? PLoS One 2012, 7, e52809. [Google Scholar] [CrossRef]
- Breier, A.C.; Brandt, C.; Sohr, D.; Geffers, C.; Gastmeier, P. Laminar airflow ceiling size: No impact on infection rates following hip and knee prosthesis. Infect. Control Hosp. Epidemiol. 2011, 32, 1097–1102. [Google Scholar] [CrossRef]
- Engesaeter, L.B.; Lie, S.A.; Espehaug, B.; Furnes, O.; Vollset, S.E.; Havelin, L.I. Antibiotic prophylaxis in total hip arthroplasty: Effects of antibiotic prophylaxis systemically and in bone cement on the revision rate of 22,170 primary hip replacements followed 0–14 years in the Norwegian Arthroplasty Register. Acta Orthop. Scand. 2003, 74, 644–651. [Google Scholar] [CrossRef]
- Hawn, M.T.; Richman, J.S.; Vick, C.C.; Deierhoi, R.J.; Graham, L.A.; Henderson, W.G.; Itani, K.M. Timing of surgical antibiotic prophylaxis and the risk of surgical site infection. JAMA Surg. 2013, 148, 649–657. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, C.; Cheng, T.; Peng, X.; Zhang, W.; Qin, H.; Zhang, X. A systematic review and meta-analysis of antibiotic-impregnated bone cement use in primary total hip or knee arthroplasty. PLoS One 2013, 8, e82745. [Google Scholar]
- Andersson, A.E.; Bergh, I.; Karlsson, J.; Eriksson, B.I.; Nilsson, K. Traffic flow in the operating room: An explorative and descriptive study on air quality during orthopedic trauma implant surgery. Am. J. Infect. Control 2012, 40, 750–755. [Google Scholar] [CrossRef]
- Clyburn, T.A.; Evans, R.P.; Moucha, C.S.; Prokuski, L. Surgical site infection prevention: The operating room environment. Instr. Course Lect. 2011, 60, 565–574. [Google Scholar]
- Hester, R.A.; Nelson, C.L.; Harrison, S. Control of contamination of the operative team in total joint arthroplasty. J. Arthroplast. 1992, 7, 267–269. [Google Scholar] [CrossRef]
- Hey, J.D.; Patel, M.S. Prevention and cure? Or: Is an ounce of prevention worth a pound of cure? J. Health Econ. 1983, 2, 119–138. [Google Scholar] [CrossRef]
- Corvec, S.; Portillo, M.E.; Pasticci, B.M.; Borens, O.; Trampuz, A. Epidemiology and new developments in the diagnosis of prosthetic joint infection. Int. J. Artif. Organs 2012, 35, 923–934. [Google Scholar]
- Cataldo, M.A.; Petrosillo, N.; Cipriani, M.; Cauda, R.; Tacconelli, E. Prosthetic joint infection: Recent developments in diagnosis and management. J. Infect. 2010, 61, 443–448. [Google Scholar] [CrossRef]
- Tsaras, G.; Osmon, D.R.; Mabry, T.; Lahr, B.; St Sauveur, J.; Yawn, B.; Kurland, R.; Berbari, E.F. Incidence, secular trends, and outcomes of prosthetic joint infection: A population-based study, olmsted county, Minnesota, 1969–2007. Infect. Control Hosp. Epidemiol. 2012, 33, 1207–1212. [Google Scholar] [CrossRef]
- Dale, H.; Fenstad, A.M.; Hallan, G.; Havelin, L.I.; Furnes, O.; Overgaard, S.; Pedersen, A.B.; Kärrholm, J.; Garellick, G.; Pulkkinen, P.; et al. Increasing risk of prosthetic joint infection after total hip arthroplasty. Acta Orthop. 2012, 83, 449–458. [Google Scholar] [CrossRef]
- Rasouli, M.R.; Maltenfort, M.G.; Purtill, J.J.; Hozack, W.J.; Parvizi, J. Has the rate of in-hospital infections after total joint arthroplasty decreased? Clin. Orthop. Relat. Res. 2013, 471, 3102–3111. [Google Scholar] [CrossRef]
- Bozic, K.J.; Ward, D.T.; Lau, E.C.; Chan, V.; Wetters, N.G.; Naziri, Q.; Odum, S.; Fehring, T.K.; Mont, M.A.; Gioe, T.J.; et al. Risk factors for periprosthetic joint infection following primary total hip arthroplasty: A case control study. J. Arthroplast. 2014, 29, 154–156. [Google Scholar] [CrossRef]
- Namba, R.S.; Inacio, M.C.; Paxton, E.W. Risk factors associated with deep surgical site infections after primary total knee arthroplasty: An analysis of 56,216 knees. J. Bone Jt. Surg. Am. 2013, 95, 775–782. [Google Scholar] [CrossRef]
- Everhart, J.S.; Altneu, E.; Calhoun, J.H. Medical comorbidities are independent preoperative risk factors for surgical infection after total joint arthroplasty. Clin. Orthop. Relat. Res. 2013, 471, 3112–3119. [Google Scholar] [CrossRef]
- Jamsen, E.; Nevalainen, P.; Eskelinen, A.; Huotari, K.; Kalliovalkama, J.; Moilanen, T. Obesity, diabetes, and preoperative hyperglycemia as predictors of periprosthetic joint infection: A single-center analysis of 7181 primary hip and knee replacements for osteoarthritis. J. Bone Jt. Surg. Am. 2012, 94, e101. [Google Scholar] [CrossRef]
- Van de Vosse, E.; van Dissel, J.T.; Ottenhoff, T.H. Genetic deficiencies of innate immune signalling in human infectious disease. Lancet Infect. Dis. 2009, 9, 688–698. [Google Scholar] [CrossRef]
- Kause, A.; Odegard, J. The genetic analysis of tolerance to infections: A review. Front. Genet. 2012, 3, 262. [Google Scholar]
- Stahelova, A.; Mrazek, F.; Smizansky, M.; Petrek, M.; Gallo, J. Variation in the IL1B, TNF and IL6 genes and individual susceptibility to prosthetic joint infection. BMC Immunol. 2012, 13, 25. [Google Scholar] [CrossRef]
- Ratner, B.D.; Schoen, F.J. The concept and assessment of biocompatibility. In Biomaterials Science: An Introduction to Materials in Medicine1, 3rd ed.; Ratner, B.D., Hoffman, A.S., Schoen, F.J., Lemons, J.E., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 588–592. [Google Scholar]
- Bernthal, N.M.; Stavrakis, A.I.; Billi, F.; Cho, J.S.; Kremen, T.J.; Simon, S.I.; Cheung, A.L.; Finerman, G.A.; Lieberman, J.R.; Adams, J.S.; et al. A mouse model of post-arthroplasty Staphylococcus aureus joint infection to evaluate in vivo the efficacy of antimicrobial implant coatings. PLoS One 2010, 5, e12580. [Google Scholar] [CrossRef]
- Follmann, H.D.; Martins, A.F.; Gerola, A.P.; Burgo, T.A.; Nakamura, C.V.; Rubira, A.F.; Muniz, E.C. Antiadhesive and antibacterial multilayer films via layer-by-layer assembly of TMC/heparin complexes. Biomacromolecules 2012, 13, 3711–3722. [Google Scholar] [CrossRef]
- Neoh, K.G.; Kang, E.T. Combating bacterial colonization on metals via polymer coatings: Relevance to marine and medical applications. ACS Appl. Mater. Interfaces 2011, 3, 2808–2819. [Google Scholar] [CrossRef]
- Muszanska, A.K.; Rochford, E.T.; Gruszka, A.; Bastian, A.A.; Busscher, H.J.; Norde, W.; van der Mei, H.C.; Herrmann, A. Antiadhesive polymer brush coating functionalized with antimicrobial and rgd peptides to reduce biofilm formation and enhance tissue integration. Biomacromolecules 2014, 15, 2019–2026. [Google Scholar] [CrossRef]
- An, Y.H.; Stuart, G.W.; McDowell, S.J.; McDaniel, S.E.; Kang, Q.; Friedman, R.J. Prevention of bacterial adherence to implant surfaces with a crosslinked albumin coating in vitro. J. Orthop. Res. 1996, 14, 846–849. [Google Scholar] [CrossRef]
- Zhu, H.; Guo, Z.; Liu, W. Adhesion behaviors on superhydrophobic surfaces. Chem. Commun. (Camb.) 2014, 18, 3900–3913. [Google Scholar]
- Stallard, C.P.; McDonnell, K.A.; Onayemi, O.D.; O’Gara, J.P.; Dowling, D.P. Evaluation of protein adsorption on atmospheric plasma deposited coatings exhibiting superhydrophilic to superhydrophobic properties. Biointerphases 2012, 7, 31. [Google Scholar]
- Poncin-Epaillard, F.; Herry, J.M.; Marmey, P.; Legeay, G.; Debarnot, D.; Bellon-Fontaine, M.N. Elaboration of highly hydrophobic polymeric surface—A potential strategy to reduce the adhesion of pathogenic bacteria? Mater. Sci. Eng. C 2013, 33, 1152–1161. [Google Scholar] [CrossRef]
- Shida, T.; Koseki, H.; Yoda, I.; Horiuchi, H.; Sakoda, H.; Osaki, M. Adherence ability of Staphylococcus epidermidis on prosthetic biomaterials: An in vitro study. Int. J. Nanomed. 2013, 8, 3955–3961. [Google Scholar]
- Singh, A.V.; Vyas, V.; Patil, R.; Sharma, V.; Scopelliti, P.E.; Bongiorno, G.; Podestà, A.; Lenardi, C.; Gade, W.N.; Milani, P. Quantitative characterization of the influence of the nanoscale morphology of nanostructured surfaces on bacterial adhesion and biofilm formation. PLoS One 2011, 6, e25029. [Google Scholar] [CrossRef]
- Ivanova, E.P.; Truong, V.K.; Wang, J.Y.; Berndt, C.C.; Jones, R.T.; Yusuf, I.I.; Peake, I.; Schmidt, H.W.; Fluke, C.; Barnes, D.; et al. Impact of nanoscale roughness of titanium thin film surfaces on bacterial retention. Langmuir 2010, 26, 1973–1982. [Google Scholar] [CrossRef]
- Truong, V.K.; Lapovok, R.; Estrin, Y.S.; Rundell, S.; Wang, J.Y.; Fluke, C.J.; Crawford, R.J.; Ivanova, E.P. The influence of nano-scale surface roughness on bacterial adhesion to ultrafine-grained titanium. Biomaterials 2010, 31, 3674–3683. [Google Scholar] [CrossRef]
- Pandit, V.; Zuidema, J.M.; Venuto, K.N.; Macione, J.; Dai, G.; Gilbert, R.J.; Kotha, S.P. Evaluation of multifunctional polysaccharide hydrogels with varying stiffness for bone tissue engineering. Tissue Eng. A 2013, 19, 2452–2463. [Google Scholar] [CrossRef]
- Zhao, C.; Li, X.; Li, L.; Cheng, G.; Gong, X.; Zheng, J. Dual functionality of antimicrobial and antifouling of poly(N-hydroxyethylacrylamide)/salicylate hydrogels. Langmuir 2013, 29, 1517–1524. [Google Scholar] [CrossRef]
- Zan, X.; Kozlov, M.; McCarthy, T.J.; Su, Z. Covalently attached, silver-doped poly(vinyl alcohol) hydrogel films on poly(l-lactic acid). Biomacromolecules 2010, 11, 1082–1088. [Google Scholar] [CrossRef]
- Drago, L.; Boot, W.; Dimas, K.; Malizos, K.; Hansch, G.M.; Stuyck, J.; Gawlitta, D.; Romanò, C.L. Does implant coating with antibacterial-loaded hydrogel reduce bacterial colonization and biofilm formation in vitro? Clin. Orthop. Relat. Res. 2014. [Google Scholar] [CrossRef]
- Cheng, H.; Li, Y.; Huo, K.; Gao, B.; Xiong, W. Long-lasting in vivo and in vitro antibacterial ability of nanostructured titania coating incorporated with silver nanoparticles. J. Biomed. Mater. Res. A 2013. [Google Scholar] [CrossRef]
- Gao, A.; Hang, R.; Huang, X.; Zhao, L.; Zhang, X.; Wang, L.; Tang, B.; Ma, S.; Chu, P.K. The effects of titania nanotubes with embedded silver oxide nanoparticles on bacteria and osteoblasts. Biomaterials 2014, 35, 4223–4235. [Google Scholar] [CrossRef]
- Mei, S.; Wang, H.; Wang, W.; Tong, L.; Pan, H.; Ruan, C.; Ma, Q.; Liu, M.; Yang, H.; Zhang, L.; et al. Antibacterial effects and biocompatibility of titanium surfaces with graded silver incorporation in titania nanotubes. Biomaterials 2014, 35, 4255–4265. [Google Scholar] [CrossRef]
- Dong, W.; Zhu, Y.; Zhang, J.; Lu, L.; Zhao, C.; Qin, L.; Li, Y. Investigation on the antibacterial micro-porous titanium with silver nano-particles. J. Nanosci. Nanotechnol. 2013, 13, 6782–6786. [Google Scholar] [CrossRef]
- Panacek, A.; Balzerova, A.; Prucek, R.; Ranc, V.; Vecerova, R.; Husickova, V.; Pechoušek, J.; Filip, J.; Zbořil, R.; Kvítek, L. Preparation, characterization and antimicrobial efficiency of Ag/PDDA-diatomite nanocomposite. Colloids Surf. B Biointerfaces 2013, 110, 191–198. [Google Scholar] [CrossRef]
- Kvitek, L.; Panacek, A.; Soukupova, J.; Kolar, M.; Vecerova, R.; Prucek, R.; Holecová, M.; Zbořil, R. Effect of surfactants and polymers on stability and antibacterial activity of silver nanoparticles (NPs). J. Phys. Chem. C 2008, 112, 5825–5834. [Google Scholar] [CrossRef]
- Knetsch, M.L.W.; Koole, L.H. New strategies in the development of antimicrobial coatings: The example of increasing usage of silver and silver nanoparticles. Polymers 2011, 3, 340–366. [Google Scholar] [CrossRef]
- Koseki, H.; Asahara, T.; Shida, T.; Yoda, I.; Horiuchi, H.; Baba, K.; Osaki, M. Clinical and histomorphometrical study on titanium dioxide-coated external fixation pins. Int. J. Nanomed. 2013, 8, 593–599. [Google Scholar]
- Haenle, M.; Fritsche, A.; Zietz, C.; Bader, R.; Heidenau, F.; Mittelmeier, W.; Gollwitzer, H. An extended spectrum bactericidal titanium dioxide (TiO2) coating for metallic implants: In vitro effectiveness against MRSA and mechanical properties. J. Mater. Sci. Mater. Med. 2011, 22, 381–387. [Google Scholar] [CrossRef]
- Yue, C.; Kuijer, R.; Kaper, H.J.; van der Mei, H.C.; Busscher, H.J. Simultaneous interaction of bacteria and tissue cells with photocatalytically activated, anodized titanium surfaces. Biomaterials 2014, 35, 2580–2587. [Google Scholar] [CrossRef]
- Holinka, J.; Pilz, M.; Kubista, B.; Presterl, E.; Windhager, R. Effects of selenium coating of orthopaedic implant surfaces on bacterial adherence and osteoblastic cell growth. Bone Jt. J. 2013, 95, 678–682. [Google Scholar] [CrossRef]
- Tran, P.A.; Webster, T.J. Selenium nanoparticles inhibit Staphylococcus aureus growth. Int. J. Nanomed. 2011, 6, 1553–1558. [Google Scholar]
- Rodriguez-Valencia, C.; Lopez-Alvarez, M.; Cochon-Cores, B.; Pereiro, I.; Serra, J.; Gonzalez, P. Novel selenium-doped hydroxyapatite coatings for biomedical applications. J. Biomed. Mater. Res. A 2013, 101, 853–861. [Google Scholar]
- Hans, M.; Erbe, A.; Mathews, S.; Chen, Y.; Solioz, M.; Mucklich, F. Role of copper oxides in contact killing of bacteria. Langmuir 2013, 29, 16160–16166. [Google Scholar] [CrossRef]
- Hoene, A.; Prinz, C.; Walschus, U.; Lucke, S.; Patrzyk, M.; Wilhelm, L.; Neumann, H.G.; Schlosser, M. In vivo evaluation of copper release and acute local tissue reactions after implantation of copper-coated titanium implants in rats. Biomed. Mater. 2013, 8. [Google Scholar] [CrossRef]
- Elizabeth, E.; Baranwal, G.; Krishnan, A.G.; Menon, D.; Nair, M. ZnO nanoparticle incorporated nanostructured metallic titanium for increased mesenchymal stem cell response and antibacterial activity. Nanotechnology 2014, 25. [Google Scholar] [CrossRef]
- Hu, H.; Zhang, W.; Qiao, Y.; Jiang, X.; Liu, X.; Ding, C. Antibacterial activity and increased bone marrow stem cell functions of Zn-incorporated TiO2 coatings on titanium. Acta Biomater. 2012, 8, 904–915. [Google Scholar] [CrossRef]
- Antoci, V., Jr.; Adams, C.S.; Parvizi, J.; Ducheyne, P.; Shapiro, I.M.; Hickok, N.J. Covalently attached vancomycin provides a nanoscale antibacterial surface. Clin. Orthop. Relat. Res. 2007, 461, 81–87. [Google Scholar]
- Antoci, V., Jr.; King, S.B.; Jose, B.; Parvizi, J.; Zeiger, A.R.; Wickstrom, E.; Freeman, T.A.; Composto, R.J.; Ducheyne, P.; Shapiro, I.M.; et al. Vancomycin covalently bonded to titanium alloy prevents bacterial colonization. J. Orthop. Res. 2007, 25, 858–866. [Google Scholar] [CrossRef]
- Walter, M.S.; Frank, M.J.; Satue, M.; Monjo, M.; Ronold, H.J.; Lyngstadaas, S.P.; Haugen, H.J. Bioactive implant surface with electrochemically bound doxycycline promotes bone formation markers in vitro and in vivo. Dent. Mater. 2014, 30, 200–214. [Google Scholar] [CrossRef]
- Chennell, P.; Feschet-Chassot, E.; Devers, T.; Awitor, K.O.; Descamps, S.; Sautou, V. In vitro evaluation of TiO2 nanotubes as cefuroxime carriers on orthopaedic implants for the prevention of periprosthetic joint infections. Int. J. Pharm. 2013, 455, 298–305. [Google Scholar] [CrossRef]
- Hickok, N.J.; Shapiro, I.M. Immobilized antibiotics to prevent orthopaedic implant infections. Adv. Drug Deliv. Rev. 2012, 64, 1165–1176. [Google Scholar] [CrossRef]
- Norowski, P.A.; Courtney, H.S.; Babu, J.; Haggard, W.O.; Bumgardner, J.D. Chitosan coatings deliver antimicrobials from titanium implants: A preliminary study. Implant Dent. 2011, 20, 56–67. [Google Scholar] [CrossRef]
- Chen, X.N.; Gu, Y.X.; Lee, J.H.; Lee, W.Y.; Wang, H.J. Multifunctional surfaces with biomimetic nanofibres and drug-eluting micro-patterns for infection control and bone tissue formation. Eur. Cells Mater. 2012, 24, 237–248. [Google Scholar]
- Renoud, P.; Toury, B.; Benayoun, S.; Attik, G.; Grosgogeat, B. Functionalization of titanium with chitosan via silanation: Evaluation of biological and mechanical performances. PLoS One 2012, 7, e39367. [Google Scholar]
- Tan, H.; Ma, R.; Lin, C.; Liu, Z.; Tang, T. Quaternized chitosan as an antimicrobial agent: Antimicrobial activity, mechanism of action and biomedical applications in orthopedics. Int. J. Mol. Sci. 2013, 14, 1854–1869. [Google Scholar] [CrossRef]
- Rapsch, K.; Bier, F.F.; Tadros, M.; von Nickisch-Rosenegk, M. Identification of antimicrobial peptides and immobilization strategy suitable for a covalent surface coating with biocompatible properties. Bioconjug. Chem. 2014, 25, 308–319. [Google Scholar] [CrossRef]
- Costa, F.; Carvalho, I.F.; Montelaro, R.C.; Gomes, P.; Martins, M.C. Covalent immobilization of antimicrobial peptides (AMPs) onto biomaterial surfaces. Acta Biomater. 2011, 7, 1431–1440. [Google Scholar] [CrossRef]
- Zheng, D.; Neoh, K.G.; Shi, Z.; Kang, E.T. Assessment of stability of surface anchors for antibacterial coatings and immobilized growth factors on titanium. J. Colloid Interface Sci. 2013, 406, 238–246. [Google Scholar] [CrossRef]
- Lopez-Leban, F.; Kiran, M.D.; Wolcott, R.; Balaban, N. Molecular mechanisms of RIP, an effective inhibitor of chronic infections. Int. J. Artif. Organs 2010, 33, 582–589. [Google Scholar]
- Chen, F.; Gao, Y.; Chen, X.; Yu, Z.; Li, X. Quorum quenching enzymes and their application in degrading signal molecules to block quorum sensing-dependent infection. Int. J. Mol. Sci. 2013, 14, 17477–17500. [Google Scholar] [CrossRef]
- Bouchet, A.M.; Iannucci, N.B.; Pastrian, M.B.; Cascone, O.; Santos, N.C.; Disalvo, E.A.; Hollmann, A. Biological activity of antibacterial peptides matches synergism between electrostatic and non electrostatic forces. Colloids Surf. B 2014, 114, 363–371. [Google Scholar] [CrossRef]
- Li, B.; McKeague, A.L. Emerging ideas: Interleukin-12 nanocoatings prevent open fracture-associated infections. Clin. Orthop. Relat. Res. 2011, 469, 3262–3265. [Google Scholar] [CrossRef]
- Thallinger, B.; Prasetyo, E.N.; Nyanhongo, G.S.; Guebitz, G.M. Antimicrobial enzymes: An emerging strategy to fight microbes and microbial biofilms. Biotechnol. J. 2013, 8, 97–109. [Google Scholar] [CrossRef]
- Chua, P.H.; Neoh, K.G.; Kang, E.T.; Wang, W. Surface functionalization of titanium with hyaluronic acid/chitosan polyelectrolyte multilayers and RGD for promoting osteoblast functions and inhibiting bacterial adhesion. Biomaterials 2008, 29, 1412–1421. [Google Scholar] [CrossRef]
- Glinel, K.; Thebault, P.; Humblot, V.; Pradier, C.M.; Jouenne, T. Antibacterial surfaces developed from bio-inspired approaches. Acta Biomater. 2012, 8, 1670–1684. [Google Scholar] [CrossRef]
- He, T.; Chan, V. Covalent layer-by-layer assembly of polyethyleneimine multilayer for antibacterial applications. J. Biomed. Mater. Res. A 2010, 95, 454–464. [Google Scholar]
- Fu, J.; Ji, J.; Fan, D.; Shen, J. Construction of antibacterial multilayer films containing nanosilver via layer-by-layer assembly of heparin and chitosan-silver ions complex. J. Biomed. Mater. Res. A 2006, 79, 665–674. [Google Scholar]
- Zhou, B.; Li, Y.; Deng, H.; Hu, Y.; Li, B. Antibacterial multilayer films fabricated by layer-by-layer immobilizing lysozyme and gold nanoparticles on nanofibers. Colloids Surf. B 2014, 116, 432–438. [Google Scholar] [CrossRef]
- Huang, W.; Li, X.; Xue, Y.; Huang, R.; Deng, H.; Ma, Z. Antibacterial multilayer films fabricated by LBL immobilizing lysozyme and HTCC on nanofibrous mats. Int. J. Biol. Macromol. 2013, 53, 26–31. [Google Scholar] [CrossRef]
- Min, J.; Braatz, R.D.; Hammond, P.T. Tunable staged release of therapeutics from layer-by-layer coatings with clay interlayer barrier. Biomaterials 2014, 35, 2507–2517. [Google Scholar] [CrossRef]
- Rizzello, L.; Pompa, P.P. Nanosilver-based antibacterial drugs and devices: Mechanisms, methodological drawbacks, and guidelines. Chem. Soc. Rev. 2013, 7, 1501–1518. [Google Scholar]
- Gottenbos, B.; van der Mei, H.C.; Klatter, F.; Grijpma, D.W.; Feijen, J.; Nieuwenhuis, P.; Busscher, H.J. Positively charged biomaterials exert antimicrobial effects on gram-negative bacilli in rats. Biomaterials 2003, 24, 2707–2710. [Google Scholar] [CrossRef]
- Yu, Q.; Cho, J.; Shivapooja, P.; Ista, L.K.; Lopez, G.P. Nanopatterned smart polymer surfaces for controlled attachment, killing, and release of bacteria. ACS Appl. Mater. Interfaces 2013, 5, 9295–9304. [Google Scholar] [CrossRef]
- Holzapfel, B.M.; Reichert, J.C.; Schantz, J.T.; Gbureck, U.; Rackwitz, L.; Nöth, U.; Jakob, F.; Rudert, M.; Groll, J.; Hutmacher, D.W. How smart do biomaterials need to be? A translational science and clinical point of view. Adv. Drug Deliv. Rev. 2013, 65, 581–603. [Google Scholar]
- Parvizi, J.; Antoci, V., Jr.; Hickok, N.J.; Shapiro, I.M. Selfprotective smart orthopedic implants. Expert Rev. Med. Devices 2007, 4, 55–64. [Google Scholar] [CrossRef]
- Mastronardi, E.; Foster, A.; Zhang, X.; Derosa, M.C. Smart materials based on DNA aptamers: Taking aptasensing to the next level. Sensors 2014, 14, 3156–3171. [Google Scholar] [CrossRef]
- Ehrlich, G.D.; Stoodley, P.; Kathju, S.; Zhao, Y.; McLeod, B.R.; Balaban, N.; Hu, F.Z.; Sotereanos, N.G.; Costerton, J.W.; Stewart, P.S.; et al. Engineering approaches for the detection and control of orthopaedic biofilm infections. Clin. Orthop. Relat. Res. 2005, 437, 59–66. [Google Scholar]
- Shchukin, D.G.; Mohwald, H. Self-repairing coatings containing active nanoreservoirs. Small 2007, 3, 926–943. [Google Scholar] [CrossRef]
- Shchukin, D.; Mohwald, H. Materials science. A coat of many functions. Science 2013, 341, 1458–1459. [Google Scholar] [CrossRef]
- Yilmaz, C.; Colak, M.; Yilmaz, B.C.; Ersoz, G.; Kutateladze, M.; Gozlugol, M. Bacteriophage therapy in implant-related infections: An experimental study. J. Bone Jt. Surg. Am. 2013, 95, 117–125. [Google Scholar] [CrossRef]
- Ratner, B.D.; Hoffman, A.S. Physicochemical surface modifications of materials used in medicine. In Biomaterials Science: An Introduction to Materials in Medicine; Ratner, B.D., Hoffman, A.S., Schoen, F.J., Lemons, J.E., Eds.; Academic Press (Elsevier): Waltham, MA, USA, 2013; pp. 259–276. [Google Scholar]
- Daghighi, S.; Sjollema, J.; van der Mei, H.C.; Busscher, H.J.; Rochford, E.T. Infection resistance of degradable versus non-degradable biomaterials: An assessment of the potential mechanisms. Biomaterials 2013, 34, 8013–8017. [Google Scholar] [CrossRef]
- Campoccia, D.; Cangini, I.; Selan, L.; Vercellino, M.; Montanaro, L.; Visai, L.; Arciola, C.R. An overview of the methodological approach to the in vitro study of anti-infective biomaterials. Int. J. Artif. Organs 2012, 35, 800–816. [Google Scholar]
- Stoodley, P.; Hall-Stoodley, L.; Costerton, B.; DeMeo, P.; Shirtliff, M.; Gawalt, E.; Kathju, S. Biofilms, biomaterials, and device-related infections. In Biomaterials Science: An Introduction to Materials in Medicine; Ratner, B.D., Hoffman, A.S., Schoen, F.J., Lemons, J.E., Eds.; Academic Press (Elsevier): Waltham, MA, USA, 2013; pp. 565–583. [Google Scholar]
- Barros, J.; Grenho, L.; Manuel, C.M.; Ferreira, C.; Melo, L.F.; Nunes, O.C.; Monteiro, F.J.; Ferraz, M.P. .A modular reactor to simulate biofilm development in orthopedic materials. Int. Microbiol. 2013, 16, 191–198. [Google Scholar]
- Ludecke, C.; Jandt, K.D.; Siegismund, D.; Kujau, M.J.; Zang, E.; Rettenmayr, M.; Bossert, J.; Roth, M. Reproducible biofilm cultivation of chemostat-grown Escherichia coli and investigation of bacterial adhesion on biomaterials using a non-constant-depth film fermenter. PLoS One 2014, 9, e84837. [Google Scholar] [CrossRef]
- Zaborowska, M.; Welch, K.; Branemark, R.; Khalilpour, P.; Engqvist, H.; Thomsen, P.; Trobos, M. Bacteria-material surface interactions: Methodological development for the assessment of implant surface induced antibacterial effects. J. Biomed. Mater. Res. B Appl. Biomater. 2014. [Google Scholar] [CrossRef]
- Campoccia, D.; Montanaro, L.; Arciola, C.R. A review of the biomaterials technologies for infection-resistant surfaces. Biomaterials 2013, 34, 8533–8554. [Google Scholar] [CrossRef]
- Rojo, L.; Barcenilla, J.M.; Vazquez, B.; Gonzalez, R.; San Roman, J. Intrinsically antibacterial materials based on polymeric derivatives of eugenol for biomedical applications. Biomacromolecules 2008, 9, 2530–2535. [Google Scholar] [CrossRef]
- Song, C.; Zheng, Y. Wetting-controlled strategies: From theories to bio-inspiration. J. Colloid Interface Sci. 2013. [Google Scholar] [CrossRef]
- MacCallum, J.L.; Tieleman, D.P. Hydrophobicity scales: A thermodynamic looking glass into lipid-protein interactions. Trends Biochem. Sci. 2011, 36, 653–662. [Google Scholar]
- Bieser, A.M.; Tiller, J.C. Mechanistic considerations on contact-active antimicrobial surfaces with controlled functional group densities. Macromol. Biosci. 2011, 11, 526–534. [Google Scholar] [CrossRef]
- Braem, A.; van Mellaert, L.; Mattheys, T.; Hofmans, D.; de Waelheyns, E.; Geris, L.; Anné, J.; Schrooten, J.; Vleugels, J. Staphylococcal biofilm growth on smooth and porous titanium coatings for biomedical applications. J. Biomed. Mater. Res. A 2013. [Google Scholar] [CrossRef]
- Vadillo-Rodriguez, V.; Pacha-Olivenza, M.A.; Gonzalez-Martin, M.L.; Bruque, J.M.; Gallardo-Moreno, A.M. Adsorption behavior of human plasma fibronectin on hydrophobic and hydrophilic Ti6Al4V substrata and its influence on bacterial adhesion and detachment. J. Biomed. Mater. Res. A 2013, 101, 1397–1404. [Google Scholar]
- Yeo, I.S.; Kim, H.Y.; Lim, K.S.; Han, J.S. Implant surface factors and bacterial adhesion: A review of the literature. Int. J. Artif. Organs 2012, 35, 762–772. [Google Scholar] [CrossRef]
- Lu, T.; Qiao, Y.; Liu, X. Surface modification of biomaterials using plasma immersion ion implantation and deposition. Interface Focus 2012, 2, 325–336. [Google Scholar] [CrossRef]
- Bacakova, L.; Filova, E.; Parizek, M.; Ruml, T.; Svorcik, V. Modulation of cell adhesion, proliferation and differentiation on materials designed for body implants. Biotechnol. Adv. 2011, 29, 739–767. [Google Scholar] [CrossRef]
- Badihi Hauslich, L.; Sela, M.N.; Steinberg, D.; Rosen, G.; Kohavi, D. The adhesion of oral bacteria to modified titanium surfaces: Role of plasma proteins and electrostatic forces. Clin. Oral Implants Res. 2013, 24, 49–56. [Google Scholar] [CrossRef]
- Dale, H.; Skramm, I.; Lower, H.L.; Eriksen, H.M.; Espehaug, B.; Furnes, O.; Skjeldestad, F.E.; Havelin, L.I.; Engesaeter, L.B. Infection after primary hip arthroplasty: A comparison of 3 Norwegian health registers. Acta Orthop. 2011, 82, 646–654. [Google Scholar] [CrossRef]
- Engesaeter, L.B.; Espehaug, B.; Lie, S.A.; Furnes, O.; Havelin, L.I. Does cement increase the risk of infection in primary total hip arthroplasty? Revision rates in 56,275 cemented and uncemented primary THAs followed for 0–16 years in the Norwegian Arthroplasty Register. Acta Orthop. 2006, 77, 351–358. [Google Scholar] [CrossRef]
- Anselme, K.; Davidson, P.; Popa, A.M.; Giazzon, M.; Liley, M.; Ploux, L. The interaction of cells and bacteria with surfaces structured at the nanometre scale. Acta Biomater. 2010, 6, 3824–3846. [Google Scholar] [CrossRef]
- Puckett, S.D.; Taylor, E.; Raimondo, T.; Webster, T.J. The relationship between the nanostructure of titanium surfaces and bacterial attachment. Biomaterials 2010, 31, 706–713. [Google Scholar] [CrossRef]
- Mitik-Dineva, N.; Wang, J.; Mocanasu, R.C.; Stoddart, P.R.; Crawford, R.J.; Ivanova, E.P. Impact of nano-topography on bacterial attachment. Biotechnol. J. 2008, 3, 536–544. [Google Scholar] [CrossRef]
- Mitik-Dineva, N.; Wang, J.; Truong, V.K.; Stoddart, P.; Malherbe, F.; Crawford, R.J.; Ivanova, E.P. Escherichia coli, Pseudomonas aeruginosa, and Staphylococcus aureus attachment patterns on glass surfaces with nanoscale roughness. Curr. Microbiol. 2009, 58, 268–273. [Google Scholar] [CrossRef]
- An, Y.H.; Bradley, J.; Powers, D.L.; Friedman, R.J. The prevention of prosthetic infection using a cross-linked albumin coating in a rabbit model. J. Bone Jt. Surg. Br. 1997, 79, 816–819. [Google Scholar] [CrossRef]
- Harris, L.G.; Tosatti, S.; Wieland, M.; Textor, M.; Richards, R.G. Staphylococcus aureus adhesion to titanium oxide surfaces coated with non-functionalized and peptide-functionalized poly(l-lysine)-grafted-poly(ethylene glycol) copolymers. Biomaterials 2004, 25, 4135–4148. [Google Scholar] [CrossRef]
- Foka, A.; Katsikogianni, M.G.; Anastassiou, E.D.; Spiliopoulou, I.; Missirlis, Y.F. The combined effect of surface chemistry and flow conditions on Staphylococcus epidermidis adhesion and ica operon expression. Eur. Cells Mater. 2012, 24, 386–402. [Google Scholar]
- Leisner, M.; Kuhr, J.T.; Radler, J.O.; Frey, E.; Maier, B. Kinetics of genetic switching into the state of bacterial competence. Biophys. J. 2009, 96, 1178–1188. [Google Scholar] [CrossRef]
- Norman, T.M.; Lord, N.D.; Paulsson, J.; Losick, R. Memory and modularity in cell-fate decision making. Nature 2013, 503, 481–486. [Google Scholar] [CrossRef]
- Decuzzi, P.; Ferrari, M. Modulating cellular adhesion through nanotopography. Biomaterials 2010, 31, 173–179. [Google Scholar] [CrossRef]
- Carson, L.; Gorman, S.P.; Gilmore, B.F. The use of lytic bacteriophages in the prevention and eradication of biofilms of Proteus mirabilis and Escherichia coli. FEMS Immunol. Med. Microbiol. 2010, 59, 447–455. [Google Scholar]
- Siddiq, D.M.; Darouiche, R.O. New strategies to prevent catheter-associated urinary tract infections. Nat. Rev. Urol. 2012, 9, 305–314. [Google Scholar] [CrossRef]
- Borovicka, J.; Metheringham, W.J.; Madden, L.A.; Walton, C.D.; Stoyanov, S.D.; Paunov, V.N. Photothermal colloid antibodies for shape-selective recognition and killing of microorganisms. J. Am. Chem. Soc. 2013, 135, 5282–5285. [Google Scholar] [CrossRef]
- Gomes, J.; Grunau, A.; Lawrence, A.K.; Eberl, L.; Gademann, K. Bioinspired surfaces against bacterial infections. Chimia 2013, 67, 275–278. [Google Scholar] [CrossRef] [Green Version]
- Lemire, J.A.; Harrison, J.J.; Turner, R.J. Antimicrobial activity of metals: Mechanisms, molecular targets and applications. Nat. Rev. Microbiol. 2013, 11, 371–384. [Google Scholar] [CrossRef]
- Visai, L.; de Nardo, L.; Punta, C.; Melone, L.; Cigada, A.; Imbriani, M.; Arciola, C.R. Titanium oxide antibacterial surfaces in biomedical devices. Int. J. Artif. Organs 2011, 34, 929–946. [Google Scholar] [CrossRef]
- Moseke, C.; Gbureck, U.; Elter, P.; Drechsler, P.; Zoll, A.; Thull, R.; Ewald, A. Hard implant coatings with antimicrobial properties. J. Mater. Sci.-Mater. Med. 2011, 22, 2711–2720. [Google Scholar] [CrossRef]
- Chernousova, S.; Epple, M. Silver as antibacterial agent: Ion, nanoparticle, and metal. Angew. Chem. Int. Ed. Engl. 2013, 52, 1636–1653. [Google Scholar] [CrossRef]
- Mijnendonckx, K.; Leys, N.; Mahillon, J.; Silver, S.; van Houdt, R. Antimicrobial silver: Uses, toxicity and potential for resistance. Biometals 2013, 26, 609–621. [Google Scholar] [CrossRef]
- Fielding, G.A.; Roy, M.; Bandyopadhyay, A.; Bose, S. Antibacterial and biological characteristics of silver containing and strontium doped plasma sprayed hydroxyapatite coatings. Acta Biomater. 2012, 8, 3144–3152. [Google Scholar] [CrossRef]
- Noda, I.; Miyaji, F.; Ando, Y.; Miyamoto, H.; Shimazaki, T.; Yonekura, Y.; Miyazaki, M.; Mawatari, M.; Hotokebuchi, T. Development of novel thermal sprayed antibacterial coating and evaluation of release properties of silver ions. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 89, 456–465. [Google Scholar]
- Panacek, A.; Kolar, M.; Vecerova, R.; Prucek, R.; Soukupova, J.; Krystof, V.; Hamal, P.; Zboril, R.; Kvítek, L. Antifungal activity of silver nanoparticles against Candida spp. Biomaterials 2009, 30, 6333–6340. [Google Scholar] [CrossRef]
- Grass, G.; Rensing, C.; Solioz, M. Metallic copper as an antimicrobial surface. Appl. Environ. Microbiol. 2011, 77, 1541–1547. [Google Scholar] [CrossRef]
- Petrini, P.; Arciola, C.R.; Pezzali, I.; Bozzini, S.; Montanaro, L.; Tanzi, M.C.; Speziale, P.; Visai, L. Antibacterial activity of zinc modified titanium oxide surface. Int. J. Artif. Organs 2006, 29, 434–442. [Google Scholar]
- Elguindi, J.; Wagner, J.; Rensing, C. Genes involved in copper resistance influence survival of Pseudomonas aeruginosa on copper surfaces. J. Appl. Microbiol. 2009, 106, 1448–1455. [Google Scholar]
- Hodgkinson, V.; Petris, M.J. Copper homeostasis at the host-pathogen interface. J. Biol. Chem. 2012, 287, 13549–13555. [Google Scholar] [CrossRef]
- Pelgrift, R.Y.; Friedman, A.J. Nanotechnology as a therapeutic tool to combat microbial resistance. Adv. Drug Deliv. Rev. 2013, 65, 1803–1815. [Google Scholar] [CrossRef]
- Vargas-Reus, M.A.; Memarzadeh, K.; Huang, J.; Ren, G.G.; Allaker, R.P. Antimicrobial activity of nanoparticulate metal oxides against peri-implantitis pathogens. Int. J. Antimicrob. Agents 2012, 40, 135–139. [Google Scholar] [CrossRef]
- Zhao, L.; Chu, P.K.; Zhang, Y.; Wu, Z. Antibacterial coatings on titanium implants. J. Biomed. Mater. Res. B 2009, 91, 470–480. [Google Scholar] [CrossRef]
- Finke, B.; Polak, M.; Hempel, F.; Rebl, H.; Zietz, C.; Stranak, V.; Lukowski, G.; Hippler, R.; Bader, R.; Nebe, J.B.; et al. Antimicrobial potential of copper-containing titanium surfaces generated by ion implantation and dual high power impulse magnetron sputtering. Adv. Eng. Mater. 2012, 14, B224–B230. [Google Scholar]
- Arenas, M.A.; Perez-Jorge, C.; Conde, A.; Matykina, E.; Hernandez-Lopez, J.M.; Perez-Tanoira, R.; de Damborenea, J.J.; Gómez-Barrena, E.; Esteba, J. Doped TiO2 anodic layers of enhanced antibacterial properties. Colloids Surf. B Biointerfaces 2013, 105, 106–112. [Google Scholar] [CrossRef]
- Xia, W.; Grandfield, K.; Hoess, A.; Ballo, A.; Cai, Y.; Engqvist, H. Mesoporous titanium dioxide coating for metallic implants. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 82–93. [Google Scholar]
- Uhm, S.H.; Song, D.H.; Kwon, J.S.; Lee, S.B.; Han, J.G.; Kim, K.N. Tailoring of antibacterial Ag nanostructures on TiO2 nanotube layers by magnetron sputtering. J. Biomed. Mater. Res. B 2014, 102, 592–603. [Google Scholar] [CrossRef]
- Masse, A.; Bruno, A.; Bosetti, M.; Biasibetti, A.; Cannas, M.; Gallinaro, P. Prevention of pin track infection in external fixation with silver coated pins: Clinical and microbiological results. J. Biomed. Mater. Res. 2000, 53, 600–604. [Google Scholar] [CrossRef]
- Kakinuma, H.; Ishii, K.; Ishihama, H.; Honda, M.; Toyama, Y.; Matsumoto, M.; Aizawa, M. Antibacterial polyetheretherketone implants immobilized with silver ions based on chelate-bonding ability of inositol phosphate: Processing, material characterization, cytotoxicity, and antibacterial properties. J. Biomed. Mater. Res. A 2014. [CrossRef]
- Wang, Q.; Webster, T.J. Nanostructured selenium for preventing biofilm formation on polycarbonate medical devices. J. Biomed. Mater. Res. A 2012, 100, 3205–3210. [Google Scholar] [CrossRef]
- Martynkova, G.S.; Valaskova, M. Antimicrobial nanocomposites based on natural modified materials: A review of carbons and clays. J. Nanosci. Nanotechnol. 2014, 14, 673–693. [Google Scholar] [CrossRef]
- Alt, V.; Bitschnau, A.; Osterling, J.; Sewing, A.; Meyer, C.; Kraus, R.; Meissner, S.A.; Wenisch, S.; Domann, E.; Schnettler, R. The effects of combined gentamicin-hydroxyapatite coating for cementless joint prostheses on the reduction of infection rates in a rabbit infection prophylaxis model. Biomaterials 2006, 27, 4627–4634. [Google Scholar] [CrossRef]
- Schmidmaier, G.; Lucke, M.; Wildemann, B.; Haas, N.P.; Raschke, M. Prophylaxis and treatmentof implant-related infections by antibiotic-coated implants: A review. Injury 2006, 37, S105–S112. [Google Scholar] [CrossRef]
- Fei, J.; Liu, G.D.; Pan, C.J.; Chen, J.Y.; Zhou, Y.G.; Xiao, S.H.; Wang, Y.; Yu, H.J. Preparation, release profiles and antibacterial properties of vancomycin-loaded Ca-P coating titanium alloy plate. J. Mater. Sci. Mater. Med. 2011, 22, 989–995. [Google Scholar] [CrossRef]
- Neut, D.; Dijkstra, R.J.; Thompson, J.I.; van der Mei, H.C.; Busscher, H.J. A gentamicin-releasing coating for cementless hip prostheses-Longitudinal evaluation of efficacy using in vitro bio-optical imaging and its wide-spectrum antibacterial efficacy. J. Biomed. Mater. Res. A 2012, 100, 3220–3226. [Google Scholar]
- Shi, X.; Wu, H.; Li, Y.; Wei, X.; Du, Y. Electrical signals guided entrapment and controlled release of antibiotics on titanium surface. J. Biomed. Mater. Res. A 2013, 101, 1373–1378. [Google Scholar]
- Salwiczek, M.; Qu, Y.; Gardiner, J.; Strugnell, R.A.; Lithgow, T.; McLean, K.M.; Thissen, H. Emerging rules for effective antimicrobial coatings. Trends Biotechnol. 2013, 32, 82–90. [Google Scholar]
- Friedman, A.; Friedman, J. New biomaterials for the sustained release of nitric oxide: Past, present and future. Expert Opin. Drug Deliv. 2009, 6, 1113–1122. [Google Scholar] [CrossRef]
- Yount, N.Y.; Yeaman, M.R. Emerging themes and therapeutic prospects for anti-infective peptides. Annu. Rev. Pharmacol. Toxicol. 2012, 52, 337–360. [Google Scholar] [CrossRef]
- Guilhelmelli, F.; Vilela, N.; Albuquerque, P.; Derengowski, L.D.; Silva-Pereira, I.; Kyaw, C.M. Antibiotic development challenges: The various mechanisms of action of antimicrobial peptides and of bacterial resistance. Front. Microbiol. 2013, 4, 353. [Google Scholar]
- Haney, E.F.; Hancock, R.E. Peptide design for antimicrobial and immunomodulatory applications. Biopolymers 2013, 100, 572–583. [Google Scholar] [CrossRef]
- Dobson, A.J.; Purves, J.; Kamysz, W.; Rolff, J. Comparing selection on S. aureus between antimicrobial peptides and common antibiotics. PLoS One 2013, 8, e76521. [Google Scholar]
- Kazemzadeh-Narbat, M.; Lai, B.F.; Ding, C.; Kizhakkedathu, J.N.; Hancock, R.E.; Wang, R. Multilayered coating on titanium for controlled release of antimicrobial peptides for the prevention of implant-associated infections. Biomaterials 2013, 34, 5969–5977. [Google Scholar] [CrossRef]
- Kazemzadeh-Narbat, M.; Kindrachuk, J.; Duan, K.; Jenssen, H.; Hancock, R.E.; Wang, R. Antimicrobial peptides on calcium phosphate-coated titanium for the prevention of implant-associated infections. Biomaterials 2010, 31, 9519–9526. [Google Scholar] [CrossRef]
- Forbes, S.; McBain, A.J.; Felton-Smith, S.; Jowitt, T.A.; Birchenough, H.L.; Dobson, C.B. Comparative surface antimicrobial properties of synthetic biocides and novel human apolipoprotein E derived antimicrobial peptides. Biomaterials 2013, 34, 5453–5464. [Google Scholar] [CrossRef]
- Holmberg, K.V.; Abdolhosseini, M.; Li, Y.; Chen, X.; Gorr, S.U.; Aparicio, C. Bio-inspired stable antimicrobial peptide coatings for dental applications. Acta Biomater. 2013, 9, 8224–8231. [Google Scholar] [CrossRef]
- Gao, G.; Lange, D.; Hilpert, K.; Kindrachuk, J.; Zou, Y.; Cheng, J.T.; Kazemzadeh-Narbat, M.; Yu, K.; Wang, R.; Straus, S.K.; et al. The biocompatibility and biofilm resistance of implant coatings based on hydrophilic polymer brushes conjugated with antimicrobial peptides. Biomaterials 2011, 32, 3899–3909. [Google Scholar] [CrossRef]
- Li, B.; Jiang, B.; Boyce, B.M.; Lindsey, B.A. Multilayer polypeptide nanoscale coatings incorporating IL-12 for the prevention of biomedical device-associated infections. Biomaterials 2009, 30, 2552–2558. [Google Scholar] [CrossRef]
- Pereira, C.S.; Thompson, J.A.; Xavier, K.B. AI-2-mediated signalling in bacteria. FEMS Microbiol. Rev. 2013, 37, 156–181. [Google Scholar]
- Lui, L.T.; Xue, X.; Sui, C.; Brown, A.; Pritchard, D.I.; Halliday, N.; Winzer, K.; Howdle, S.M.; Fernandez-Trillo, F.; Krasnogor, N.; et al. Bacteria clustering by polymers induces the expression of quorum-sensing-controlled phenotypes. Nat. Chem. 2013, 5, 1058–1065. [Google Scholar] [CrossRef]
- Gomes, J.; Grunau, A.; Lawrence, A.K.; Eberl, L.; Gademann, K. Bioinspired, releasable quorum sensing modulators. Chem. Commun. (Camb.) 2013, 49, 155–157. [Google Scholar] [CrossRef]
- Brooks, J.L.; Jefferson, K.K. Staphylococcal biofilms: Quest for the magic bullet. Adv. Appl. Microbiol. 2012, 81, 63–87. [Google Scholar]
- Kiran, M.D.; Giacometti, A.; Cirioni, O.; Balaban, N. Suppression of biofilm related, device-associated infections by staphylococcal quorum sensing inhibitors. Int. J. Artif. Organs 2008, 31, 761–770. [Google Scholar]
- Chen, G.; Swem, L.R.; Swem, D.L.; Stauff, D.L.; O’Loughlin, C.T.; Jeffrey, P.D.; Bassler, B.L.; Hughson, F.M. A strategy for antagonizing quorum sensing. Mol. Cell 2011, 42, 199–209. [Google Scholar] [CrossRef]
- Ho, K.K.; Chen, R.; Willcox, M.D.; Rice, S.A.; Cole, N.; Iskander, G.; Kumar, N. Quorum sensing inhibitory activities of surface immobilized antibacterial dihydropyrrolones via click chemistry. Biomaterials 2013, 35, 2336–2345. [Google Scholar]
- Bottcher, T.; Kolodkin-Gal, I.; Kolter, R.; Losick, R.; Clardy, J. Synthesis and activity of biomimetic biofilm disruptors. J. Am. Chem. Soc. 2013, 135, 2927–2930. [Google Scholar] [CrossRef]
- Gu, Y.; Zhang, W.; Wang, H.; Lee, W.Y. Chitosan surface enhances the mobility, cytoplasm spreading, and phagocytosis of macrophage. Colloids Surf. B Biointerfaces 2014, 117, 42–50. [Google Scholar] [CrossRef]
- Peng, Z.X.; Tu, B.; Shen, Y.; Du, L.; Wang, L.; Guo, S.R.; Tang, T.T. Quaternized chitosan inhibits icaA transcription and biofilm formation by Staphylococcus on a titanium surface. Antimicrob. Agents Chemother. 2011, 55, 860–866. [Google Scholar] [CrossRef]
- Tan, H.; Peng, Z.; Li, Q.; Xu, X.; Guo, S.; Tang, T. The use of quaternised chitosan-loaded PMMA to inhibit biofilm formation and downregulate the virulence-associated gene expression of antibiotic-resistant staphylococcus. Biomaterials 2012, 33, 365–377. [Google Scholar] [CrossRef]
- Yang, C.C.; Lin, C.C.; Liao, J.W.; Yen, S.K. Vancomycin-chitosan composite deposited on post porous hydroxyapatite coated Ti6Al4V implant for drug controlled release. Mater. Sci. Eng. C 2013, 33, 2203–2212. [Google Scholar] [CrossRef]
- Banerjee, M.; Mallick, S.; Paul, A.; Chattopadhyay, A.; Ghosh, S.S. Heightened reactive oxygen species generation in the antimicrobial activity of a three component iodinated chitosan-silver nanoparticle composite. Langmuir 2010, 26, 5901–5908. [Google Scholar] [CrossRef]
- Costa, F.; Maia, S.; Gomes, P.; Martins, M.C. Characterization of hLF1-11 immobilization onto chitosan ultrathin films, and its effects on antimicrobial activity. Acta Biomater. 2014. [Google Scholar] [CrossRef]
- Jennison, T.; McNally, M.; Pandit, H. Prevention of infection in external fixator pin sites. Acta Biomater. 2014, 10, 595–603. [Google Scholar] [CrossRef]
- Shi, Z.; Neoh, K.G.; Kang, E.T.; Wang, W. Antibacterial and mechanical properties of bone cement impregnated with chitosan nanoparticles. Biomaterials 2006, 27, 2440–2449. [Google Scholar] [CrossRef]
- Rizzello, L.; Cingolani, R.; Pompa, P.P. Nanotechnology tools for antibacterial materials. Nanomedicine (Lond.) 2013, 8, 807–821. [Google Scholar] [CrossRef]
- Taylor, E.; Webster, T.J. Reducing infections through nanotechnology and nanoparticles. Int. J. Nanomed. 2011, 6, 1463–1473. [Google Scholar] [CrossRef]
- Nair, L.S.; Laurencin, C.T. Nanofibers and nanoparticles for orthopaedic surgery applications. J. Bone Jt. Surg. Am. 2008, 90, 128–131. [Google Scholar] [CrossRef]
- Campoccia, D.; Montanaro, L.; Agheli, H.; Sutherland, D.S.; Pirini, V.; Donati, M.E.; Arciola, C.R. Study of Staphylococcus aureus adhesion on a novel nanostructured surface by chemiluminometry. Int. J. Artif. Organs 2006, 29, 622–629. [Google Scholar]
- Lee, F.P.; Wang, D.J.; Chen, L.K.; Kung, C.M.; Wu, Y.C.; Ou, K.L.; Yu, C.H. Antibacterial nanostructured composite films for biomedical applications: Microstructural characteristics, biocompatibility, and antibacterial mechanisms. Biofouling 2013, 29, 295–305. [Google Scholar] [CrossRef]
- Montanaro, L.; Campoccia, D.; Arciola, C.R. Nanostructured materials for inhibition of bacterial adhesion in orthopedic implants: A minireview. Int. J. Artif. Organs 2008, 31, 771–776. [Google Scholar]
- Wang, H.; Cheng, M.; Hu, J.; Wang, C.; Xu, S.; Han, C.C. Preparation and optimization of silver nanoparticles embedded electrospun membrane for implant associated infections prevention. ACS Appl. Mater. Interfaces 2013, 5, 11014–11021. [Google Scholar] [CrossRef]
- Lischer, S.; Korner, E.; Balazs, D.J.; Shen, D.; Wick, P.; Grieder, K.; Haas, D.; Heuberger, M.; Hegemann, D. Antibacterial burst-release from minimal Ag-containing plasma polymer coatings. J. R. Soc. Interface 2011, 8, 1019–1030. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Z.; Yuan, X.; Cui, Z.; Bao, H.; Li, X.; Liu, Y.; Yang, X. Cytotoxicity and antibacterial property of titanium alloy coated with silver nanoparticle-containing polyelectrolyte multilayer. Mater. Sci. Eng. C 2013, 33, 2816–2820. [Google Scholar] [CrossRef]
- Song, J.; Jang, J. Antimicrobial polymer nanostructures: Synthetic route, mechanism of action and perspective. Adv. Colloid Interface Sci. 2014, 203, 37–50. [Google Scholar] [CrossRef]
- Marková, Z.; Šišková, K.; Filip, J.; Šafářová, K.; Prucek, R.; Panáček, A.; Kolář, M.; Zbořil, R. Chitosan-based synthesis of magnetically-driven nanocomposites with biogenic magnetite core, controlled silver size, and high antimicrobial activity. Green Chem. 2012, 14, 2550–2558. [Google Scholar] [CrossRef]
- Prucek, R.; Tucek, J.; Kilianova, M.; Panacek, A.; Kvitek, L.; Filip, J.; Kolář, M.; Tománková, K.; Zbořil, R. The targeted antibacterial and antifungal properties of magnetic nanocomposite of iron oxide and silver nanoparticles. Biomaterials 2011, 32, 4704–4713. [Google Scholar] [CrossRef]
- Panacek, A.; Kvitek, L.; Prucek, R.; Kolar, M.; Vecerova, R.; Pizurova, N.; Sharma, V.K.; Nevecna, T.; Zboril, R. Silver colloid nanoparticles: Synthesis, characterization, and their antibacterial activity. J. Phys. Chem. B 2006, 110, 16248–16253. [Google Scholar]
- Bondarenko, O.; Ivask, A.; Kakinen, A.; Kurvet, I.; Kahru, A. Particle-cell contact enhances antibacterial activity of silver nanoparticles. PLoS One 2013, 8, e64060. [Google Scholar]
- Agnihotri, S.; Mukherji, S.; Mukherji, S. Immobilized silver nanoparticles enhance contact killing and show highest efficacy: Elucidation of the mechanism of bactericidal action of silver. Nanoscale 2013, 5, 7328–7340. [Google Scholar] [CrossRef]
- Martinez-Gutierrez, F.; Boegli, L.; Agostinho, A.; Sanchez, E.M.; Bach, H.; Ruiz, F.; James, G. Anti-biofilm activity of silver nanoparticles against different microorganisms. Biofouling 2013, 29, 651–660. [Google Scholar] [CrossRef]
- Kose, N.; Otuzbir, A.; Peksen, C.; Kiremitci, A.; Dogan, A. A silver ion-doped calcium phosphate-based ceramic nanopowder-coated prosthesis increased infection resistance. Clin. Orthop. Relat. Res. 2013, 471, 2532–2539. [Google Scholar] [CrossRef]
- Della Valle, C.; Visai, L.; Santin, M.; Cigada, A.; Candiani, G.; Pezzoli, D.; Arciola, C.R.; Imbriani, M.; Chiesa, R. A novel antibacterial modification treatment of titanium capable to improve osseointegration. Int. J. Artif. Organs 2012, 35, 864–875. [Google Scholar]
- Liu, Y.; Zheng, Z.; Zara, J.N.; Hsu, C.; Soofer, D.E.; Lee, K.S.; Siu, R.K.; Miller, L.S.; Zhang, X.; Carpenter, D.; et al. The antimicrobial and osteoinductive properties of silver nanoparticle/poly (dl-lactic-co-glycolic acid)-coated stainless steel. Biomaterials 2012, 33, 8745–8756. [Google Scholar] [CrossRef]
- Lan, M.Y.; Liu, C.P.; Huang, H.H.; Lee, S.W. Both enhanced biocompatibility and antibacterial activity in Ag-decorated TiO2 nanotubes. PLoS One 2013, 8, e75364. [Google Scholar]
- Seil, J.T.; Webster, T.J. Antibacterial effect of zinc oxide nanoparticles combined with ultrasound. Nanotechnology 2012, 23, 495101. [Google Scholar] [CrossRef]
- Vishwakarma, V.; Josephine, J.; George, R.P.; Krishnan, R.; Dash, S.; Kamruddin, M.; Kalavathi, S.; Manoharan, N.; Tyagi, A.K.; Dayal, R.K. Antibacterial copper-nickel bilayers and multilayer coatings by pulsed laser deposition on titanium. Biofouling 2009, 25, 705–710. [Google Scholar] [CrossRef]
- Jan, T.; Iqbal, J.; Ismail, M.; Zakaullah, M.; Naqvi, S.H.; Badshah, N. Sn doping induced enhancement in the activity of ZnO nanostructures against antibiotic resistant S. aureus bacteria. Int. J. Nanomed. 2013, 8, 3679–3687. [Google Scholar]
- Campoccia, D.; Montanaro, L.; Arciola, C.R. A review of the clinical implications of anti-infective biomaterials and infection-resistant surfaces. Biomaterials 2013, 34, 8018–8029. [Google Scholar] [CrossRef]
- Shirwaiker, R.A.; Samberg, M.E.; Cohen, P.H.; Wysk, R.A.; Monteiro-Riviere, N.A. Nanomaterialsand synergistic low-intensity direct current (LIDC) stimulation technology for orthopedic implantable medical devices. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2013, 5, 191–204. [Google Scholar] [CrossRef]
- Wang, J.; Zhu, Y.; Bawa, H.K.; Ng, G.; Wu, Y.; Libera, M.; van der Mei, H.C.; Busscher, H.J.; Yu, X. Oxygen-generating nanofiber cell scaffolds with antimicrobial properties. ACS Appl. Mater. Interfaces 2011, 3, 67–73. [Google Scholar] [CrossRef]
- Gallo, P.M.; Gallucci, S. The dendritic cell response to classic, emerging, and homeostatic danger signals. Implications for autoimmunity. Front. Immunol. 2013, 4, 138. [Google Scholar]
- Shtansky, D.V.; Gloushankova, N.A.; Bashkova, I.A.; Kharitonova, M.A.; Moizhess, T.G.; Sheveiko, A.N.; Kiryukhantsev-Korneev, F.V.; Petrzhik, M.I.; Levashov, E.A. Multifunctional Ti-(Ca,Zr)-(C,N,O,P) films for load-bearing implants. Biomaterials 2006, 27, 3519–3531. [Google Scholar]
- Hardes, J.; von Eiff, C.; Streitbuerger, A.; Balke, M.; Budny, T.; Henrichs, M.P.; Hauschild, G.; Ahrens, H. Reduction of periprosthetic infection with silver-coated megaprostheses in patients with bone sarcoma. J. Surg. Oncol. 2010, 101, 389–395. [Google Scholar]
- Hussmann, B.; Johann, I.; Kauther, M.D.; Landgraeber, S.; Jager, M.; Lendemans, S. Measurement of the silver ion concentration in wound fluids after implantation of silver-coated megaprostheses: Correlation with the clinical outcome. BioMed Res. Int. 2013, 2013, 763096. [Google Scholar]
- Tran, P.A.; Sarin, L.; Hurt, R.H.; Webster, T.J. Titanium surfaces with adherent selenium nanoclusters as a novel anticancer orthopedic material. J. Biomed. Mater. Res. A 2010, 93, 1417–1428. [Google Scholar]
- Pishbin, F.; Mourino, V.; Flor, S.; Kreppel, S.; Salih, V.; Ryan, M.P.; Boccaccini, A.R. Electrophoretic deposition of gentamicin-loaded bioactive glass/chitosan composite coatings for orthopaedic implants. ACS Appl. Mater. Interfaces 2014, 6, 8796–8806. [Google Scholar] [CrossRef]
- Zhuang, J.; Gordon, M.R.; Ventura, J.; Li, L.; Thayumanavan, S. Multi-stimuli responsive macromolecules and their assemblies. Chem. Soc. Rev. 2013, 42, 7421–7435. [Google Scholar] [CrossRef]
- Furth, M.E.; Atala, A.; van Dyke, M.E. Smart biomaterials design for tissue engineering and regenerative medicine. Biomaterials 2007, 28, 5068–5073. [Google Scholar] [CrossRef]
- Schneider, G.F.; Decher, G. From “nano-bags” to “micro-pouches”. Understanding and tweaking flocculation-based processes for the preparation of new nanoparticle-composites. Nano Lett. 2008, 8, 3598–3604. [Google Scholar] [CrossRef]
- Zhao, X.; Meng, G.; Han, F.; Li, X.; Chen, B.; Xu, Q.; Zhu, X.; Chu, Z.; Kong, M.; Huang, Q. Nanocontainers made of various materials with tunable shape and size. Sci. Rep. 2013, 3, 2238. [Google Scholar]
- Grainger, D.W.; van der Mei, H.C.; Jutte, P.C.; van den Dungen, J.J.; Schultz, M.J.; van der Laan, B.F.; Zaat, S.A.; Busscher, H.J. Critical factors in the translation of improved antimicrobial strategies for medical implants and devices. Biomaterials 2013, 34, 9237–9243. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Gallo, J.; Holinka, M.; Moucha, C.S. Antibacterial Surface Treatment for Orthopaedic Implants. Int. J. Mol. Sci. 2014, 15, 13849-13880. https://doi.org/10.3390/ijms150813849
Gallo J, Holinka M, Moucha CS. Antibacterial Surface Treatment for Orthopaedic Implants. International Journal of Molecular Sciences. 2014; 15(8):13849-13880. https://doi.org/10.3390/ijms150813849
Chicago/Turabian StyleGallo, Jiri, Martin Holinka, and Calin S. Moucha. 2014. "Antibacterial Surface Treatment for Orthopaedic Implants" International Journal of Molecular Sciences 15, no. 8: 13849-13880. https://doi.org/10.3390/ijms150813849
APA StyleGallo, J., Holinka, M., & Moucha, C. S. (2014). Antibacterial Surface Treatment for Orthopaedic Implants. International Journal of Molecular Sciences, 15(8), 13849-13880. https://doi.org/10.3390/ijms150813849