
Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation


 ,
, 
Abstract
:1. Introduction
2. Results
2.1. The Clinical Characteristics of Patients Included in the Study
2.2. Pre-Transplant IL-6 and sgp130 Serum Levels Were Increased Prior to Conditioning Therapy Whereas the Levels of sIL-6R and Other IL-6 Family Members Did Not Differ from Healthy Controls
2.3. Preconditioning Levels of IL-6 Family Cytokines Did Not Differ between Patients with and without Later aGVHD
2.4. sIL-6R and sgp130 Levels Correlates with Time until Neutrophil Reconstitution but Not with Time Until Platelet Reconstitution
2.5. Pretransplant IL-6 Levels Correlated with Pretransplant CRP Levels
2.6. A Large Patient Subset Shows Early Weight Gain after Conditioning/Transplantation
2.7. The Risk of Steroid-Requiring aGVHD Was Only Associated with Maximum Weight Gain and Sibling vs. Non-Sibling Donor but Not with Preconditioning Levels of Cytokines/Receptors or CRP
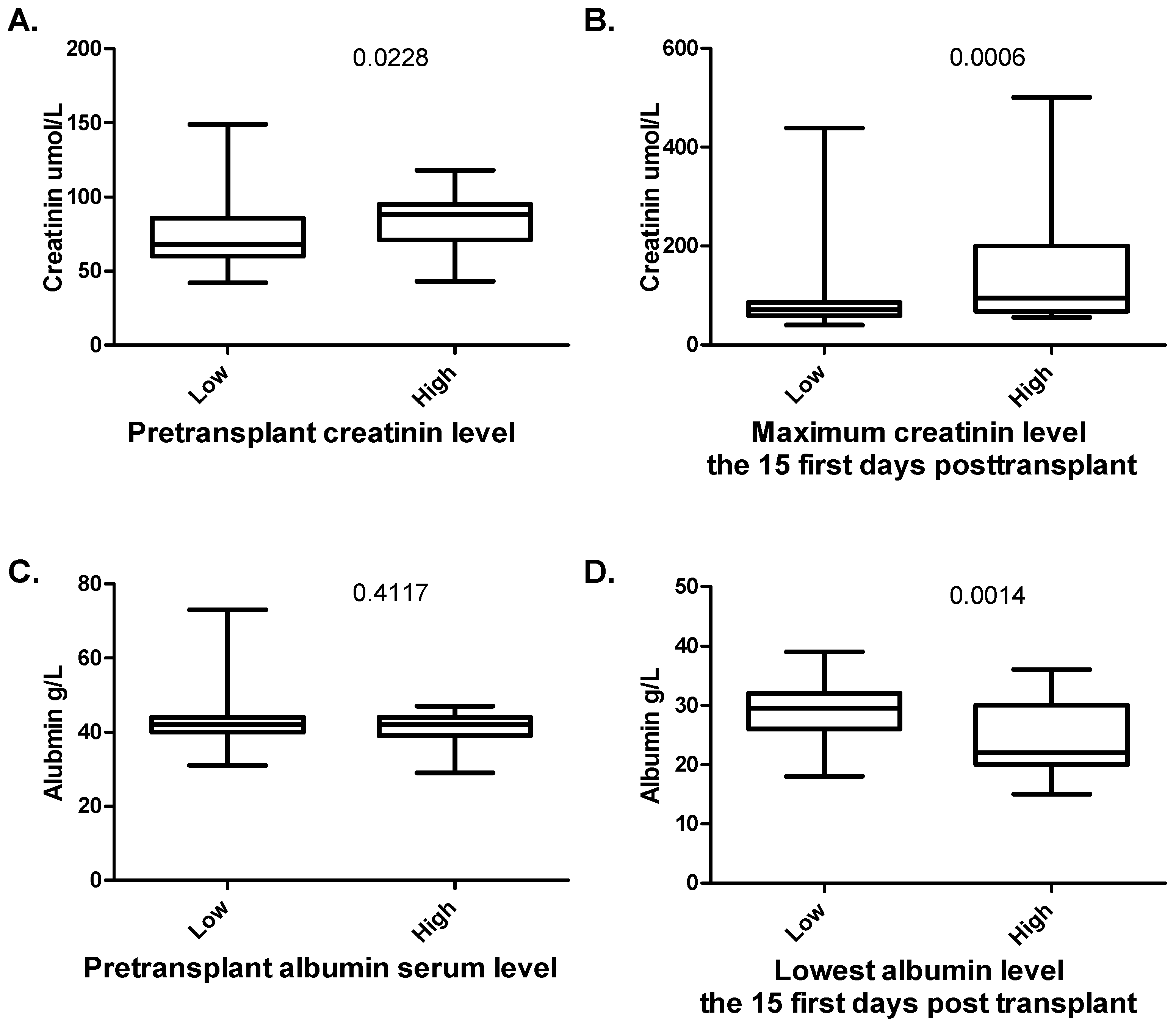
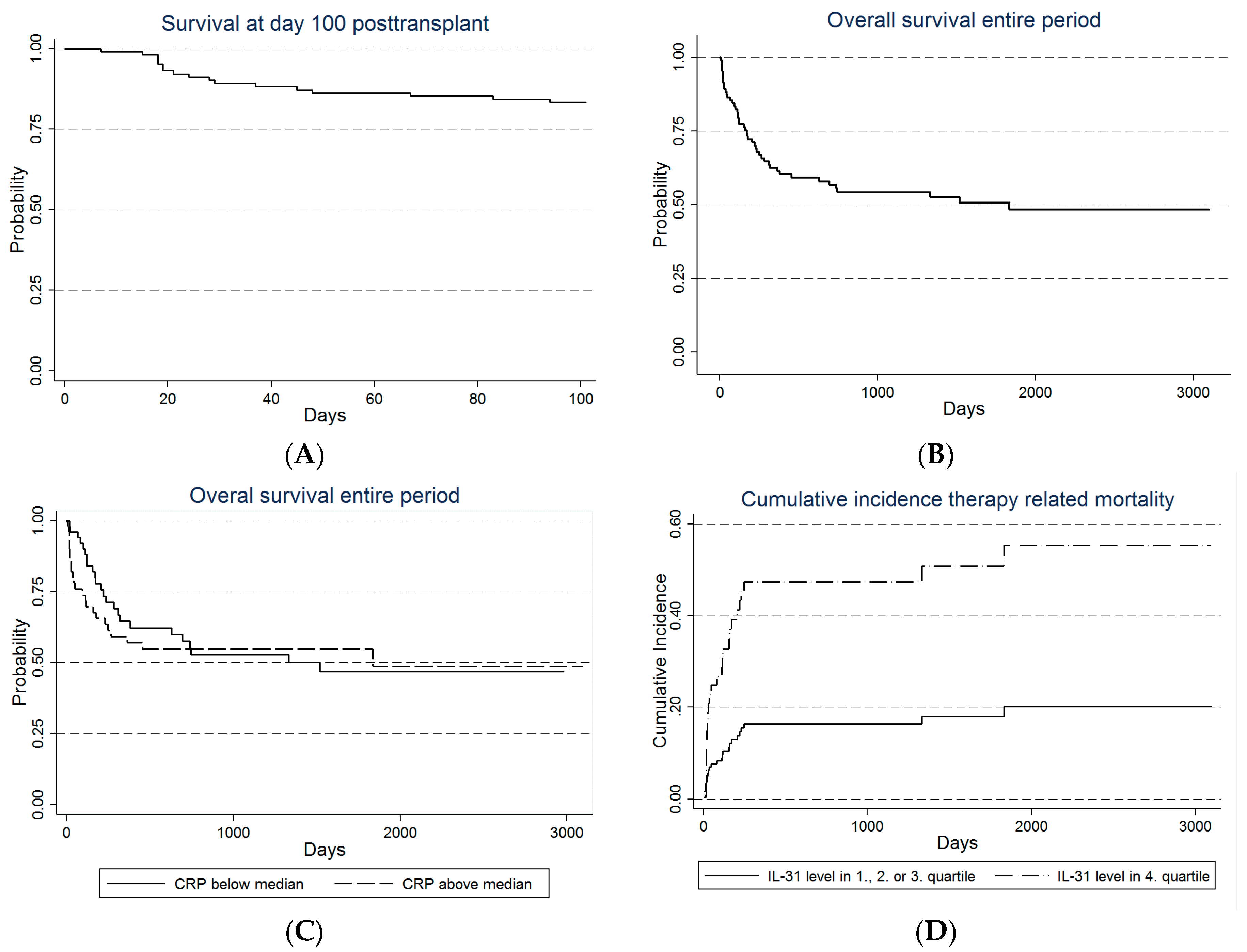
2.8. Transplant-Related Mortality before Day +100 Post-Transplant Was Only Associated with Maximum Weight Gain as Well as Preconditioning CRP and IL-31 Levels in Adjusted/Multivariate Analysis
2.9. Recipient Age, Maximum Weight Gain and Preconditioning IL-31 Levels Are Associated with Transplant-Related Mortality and Overall Survival after 2 Years in Multivariate Analysis
2.10. Only Maximum Weight Gain and Preconditioning Serum IL-31 Levels Are Associated with Transplant-Related Mortality and Overall Survival for the Entire Observation Period in Multivariate Analysis
3. Discussion
4. Material and Methods
4.1. Patients
4.2. Healthy Controls
4.3. Analysis of Soluble Mediator Levels in Serum Samples
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| aGVHD | Acute graft versus host disease |
| ALL | Acute lymphoblastic leukemia |
| AML | Acute myeloid leukemia |
| ASCT | Allogenic stem cell transplantation |
| BM | bone marrow |
| CD | Cluster of differentiation |
| cGVHD | Chronic graft versus host disease |
| CMV | Cytomegalovirus |
| CNTF | Ciliary neutrophilic factor |
| CRP | C-reactive protein |
| EBMT | European Society for Blood and Marrow Transplantation |
| G-CSF | granulocyte colony-stimulating factor |
| gp130 | Glycoprotein 130 |
| HCT-CI | Hematopoietic cell transplant comorbidity index |
| HLA | Human leucocyte antigen |
| IL | Interleukin |
| IL-6R | Interleukin-6 receptor |
| IQR | Interquartile range |
| LIF | Leukemia inhibitory factor |
| MAC | Myeloablativ conditioning |
| MDS | Myelodysplastic syndrome |
| MHC | Major histocompatibility complex |
| NR | Not reported |
| OS | Overall survival |
| OSM | Oncostatin M |
| PB | peripheral blood |
| PS | Performance status |
| RIC | Reduced intensity conditioning |
| sgp130 | Soluble glycoprotein 130 |
| sIL-6R | Soluble interleukin-6 receptor |
| SNP | Single nucleotide polymorphism |
| TRM | Transplant-related mortality |
References
- Jagasia, M.; Arora, M.; Flowers, M.E.; Chao, N.J.; McCarthy, P.L.; Cutler, C.S.; Urbano-Ispizua, A.; Pavletic, S.Z.; Haagenson, M.D.; Zhang, M.J.; et al. Risk factors for acute GVHD and survival after hematopoietic cell transplantation. Blood 2012, 119, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Cho, B.S.; Kim, J.H.; Yoon, J.H.; Shin, S.H.; Yahng, S.A.; Eom, K.S.; Kim, Y.J.; Kim, H.J.; Lee, S.; et al. Risk and prognostic factors for acute GVHD based on NIH consensus criteria. Bone Marrow Transplant. 2013, 48, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Melve, G.K.; Ersvssr, E.; Kittang, A.O.; Bruserud, O. The chemokine system in allogeneic stem-cell transplantation: A possible therapeutic target? Expert Rev. Hematol. 2011, 4, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.M.; Charron, D. Non-HLA immunogenetics in hematopoietic stem cell transplantation. Curr. Opin. Immunol. 2005, 17, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Artz, A.S.; Wickrema, A.; Dinner, S.; Godley, L.A.; Kocherginsky, M.; Odenike, O.; Rich, E.S.; Stock, W.; Ulaszek, J.; Larson, R.A.; et al. Pretreatment C-reactive protein is a predictor for outcomes after reduced-intensity allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplantat. 2008, 14, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Remberger, M.; Mattsson, J. C-reactive protein levels before reduced-intensity conditioning predict outcome after allogeneic stem cell transplantation. Int. J. Hematol. 2010, 92, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, S.; Kawabata, H.; Kanda, J.; Uchiyama, T.; Mizumoto, C.; Kondo, T.; Yamashita, K.; Ichinohe, T.; Ishikawa, T.; Kadowaki, N.; et al. Differing impacts of pretransplant serum ferritin and C-reactive protein levels on the incidence of chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Int. J. Hematol. 2013, 97, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Nakasone, H.; Oshima, K.; Ishihara, Y.; Wada, H.; Sakamoto, K.; Kawamura, K.; Ashizawa, M.; Machishima, T.; Terasako, K.; et al. Prediction of transplant-related complications by C-reactive protein levels before hematopoietic SCT. Bone Marrow Transplant. 2013, 48, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Aki, S.Z.; Suyani, E.; Bildaci, Y.; Cakar, M.K.; Baysal, N.A.; Sucak, G.T. Prognostic role of pre-transplantation serum C-reactive protein levels in patients with acute leukemia undergoing myeloablative allogeneic stem cell transplantation. Clin. Transplant. 2012, 26, E513–E521. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.K.; Christensen, I.J.; Heilmann, C.; Sengelov, H.; Muller, K.G. Pretransplant C-reactive protein as A prognostic marker in allogeneic stem cell transplantation. Scand. J. Immunol. 2014, 79, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Pavlu, J.; Kew, A.K.; Taylor-Roberts, B.; Auner, H.W.; Marin, D.; Olavarria, E.; Kanfer, E.J.; MacDonald, D.H.; Milojkovic, D.; Rahemtulla, A.; et al. Optimizing patient selection for myeloablative allogeneic hematopoietic cell transplantation in chronic myeloid leukemia in chronic phase. Blood 2010, 115, 4018–4020. [Google Scholar] [CrossRef] [PubMed]
- Scheller, J.; Garbers, C.; Rose-John, S. Interleukin-6: From basic biology to selective blockade of pro-inflammatory activities. Semin. Immunol. 2014, 26, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.S.; Hunter, C.A. gp130 at the nexus of inflammation, autoimmunity, and cancer. J. Leukoc. Biol. 2010, 88, 1145–1156. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, S.M. LIF in the regulation of T-cell fate and as a potential therapeutic. Genes Immun. 2011, 12, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, C.; Luscher-Firzlaff, J.; Baron, J.M.; Luscher, B. Signaling by IL-31 and functional consequences. Eur. J. Cell Biol. 2012, 91, 552–566. [Google Scholar] [CrossRef] [PubMed]
- Kopf, M.; Baumann, H.; Freer, G.; Freudenberg, M.; Lamers, M.; Kishimoto, T.; Zinkernagel, R.; Bluethmann, H.; Kohler, G. Impaired immune and acute-phase responses in interleukin-6-deficient mice. Nature 1994, 368, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Espat, N.J.; Auffenberg, T.; Rosenberg, J.J.; Rogy, M.; Martin, D.; Fang, C.H.; Hasselgren, P.O.; Copeland, E.M.; Moldawer, L.L. Ciliary neurotrophic factor is catabolic and shares with IL-6 the capacity to induce an acute phase response. Am. J. Physiol. 1996, 271, R185–R190. [Google Scholar] [PubMed]
- Varelias, A.; Gartlan, K.H.; Kreijveld, E.; Olver, S.D.; Lor, M.; Kuns, R.D.; Lineburg, K.E.; Teal, B.E.; Raffelt, N.C.; Cheong, M.; et al. Lung parenchyma-derived IL-6 promotes IL-17A-dependent acute lung injury after allogeneic stem cell transplantation. Blood 2015, 125, 2435–2444. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Das, R.; Komorowski, R.; Beres, A.; Hessner, M.J.; Mihara, M.; Drobyski, W.R. Blockade of interleukin-6 signaling augments regulatory T-cell reconstitution and attenuates the severity of graft-versus-host disease. Blood 2009, 114, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Tawara, I.; Koyama, M.; Liu, C.; Toubai, T.; Thomas, D.; Evers, R.; Chockley, P.; Nieves, E.; Sun, Y.; Lowler, K.P.; et al. Interleukin-6 modulates graft-versus-host responses after experimental allogeneic bone marrow transplantation. Clin. Cancer Res. 2011, 17, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Kimura, A.; Kishimoto, T. IL-6: Regulator of Treg/Th17 balance. Eur. J. Immunol. 2010, 40, 1830–1835. [Google Scholar] [CrossRef] [PubMed]
- Scheller, J.; Chalaris, A.; Schmidt-Arras, D.; Rose-John, S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim. Biophys. Acta 2011, 1813, 878–888. [Google Scholar] [CrossRef] [PubMed]
- Rose-John, S. IL-6 trans-signaling via the soluble IL-6 receptor: Importance for the pro-inflammatory activities of IL-6. Int. J. Biol. Sci. 2012, 8, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Rifai, N.; Hu, F.B. Interleukin-6 receptor gene, plasma C-reactive protein, and diabetes risk in women. Diabetes 2009, 58, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Revez, J.A.; Bain, L.; Chapman, B.; Powell, J.E.; Jansen, R.; Duffy, D.L.; Tung, J.Y.; Collaborators, A.; Penninx, B.W.; Visscher, P.M.; et al. A new regulatory variant in the interleukin-6 receptor gene associates with asthma risk. Genes Immun. 2013, 14, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, R.C.; Freitag, D.F.; Cutler, A.J.; Howson, J.M.; Rainbow, D.B.; Smyth, D.J.; Kaptoge, S.; Clarke, P.; Boreham, C.; Coulson, R.M.; et al. Functional IL6R 358Ala allele impairs classical IL-6 receptor signaling and influences risk of diverse inflammatory diseases. PLoS Genet. 2013, 9, e1003444. [Google Scholar] [CrossRef] [PubMed]
- Won, H.S.; Kim, Y.A.; Lee, J.S.; Jeon, E.K.; An, H.J.; Sun, D.S.; Ko, Y.H.; Kim, J.S. Soluble interleukin-6 receptor is a prognostic marker for relapse-free survival in estrogen receptor-positive breast cancer. Cancer Investig. 2013, 31, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Kruttgen, A.; Rose-John, S. Interleukin-6 in sepsis and capillary leakage syndrome. J. Interferon Cytokine Res. 2012, 32, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, P.V.; Garcia, R.; Waggie, K.S.; Anderson-Haley, M.; Nelson, A.; Hughes, S.D. Comparison of vascular leak syndrome in mice treated with IL21 or IL2. Comp. Med. 2013, 63, 13–21. [Google Scholar] [PubMed]
- Kai-Feng, W.; Hong-Ming, P.; Hai-Zhou, L.; Li-Rong, S.; Xi-Yan, Z. Interleukin-11-induced capillary leak syndrome in primary hepatic carcinoma patients with thrombocytopenia. BMC Cancer 2011, 11, 204. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chen, Q.; Corne, J.; Zhu, Z.; Lee, C.G.; Bhandari, V.; Homer, R.J.; Elias, J.A. Pulmonary expression of leukemia inhibitory factor induces B cell hyperplasia and confers protection in hyperoxia. J. Biol. Chem. 2003, 278, 31226–31232. [Google Scholar] [CrossRef] [PubMed]
- Burstein, S.A.; Mei, R.L.; Henthorn, J.; Friese, P.; Turner, K. Leukemia inhibitory factor and interleukin-11 promote maturation of murine and human megakaryocytes in vitro. J. Cell. Physiol. 1992, 153, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Broxmeyer, H.E.; Li, J.; Hangoc, G.; Cooper, S.; Tao, W.; Mantel, C.; Graham-Evans, B.; Ghilardi, N.; de Sauvage, F.J. Regulation of myeloid progenitor cell proliferation/survival by IL-31 receptor and IL-31. Exp. Hematol. 2007, 35, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Patchen, M.L.; MacVittie, T.J.; Williams, J.L.; Schwartz, G.N.; Souza, L.M. Administration of interleukin-6 stimulates multilineage hematopoiesis and accelerates recovery from radiation-induced hematopoietic depression. Blood 1991, 77, 472–480. [Google Scholar] [PubMed]
- Miyajima, A.; Kinoshita, T.; Tanaka, M.; Kamiya, A.; Mukouyama, Y.; Hara, T. Role of Oncostatin M in hematopoiesis and liver development. Cytokine Growth Factor Rev. 2000, 11, 177–183. [Google Scholar] [CrossRef]
- Maccio, A.; Madeddu, C.; Massa, D.; Mudu, M.C.; Lusso, M.R.; Gramignano, G.; Serpe, R.; Melis, G.B.; Mantovani, G. Hemoglobin levels correlate with interleukin-6 levels in patients with advanced untreated epithelial ovarian cancer: Role of inflammation in cancer-related anemia. Blood 2005, 106, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Reikvam, H.; Hatfield, K.J.; Fredly, H.; Nepstad, I.; Mosevoll, K.A.; Bruserud, O. The angioregulatory cytokine network in human acute myeloid leukemia—From leukemogenesis via remission induction to stem cell transplantation. Eur. Cytokine Netw. 2012, 23, 140–153. [Google Scholar] [PubMed]
- Costa-Lima, C.; Martins Miranda, E.C.; Colella, M.P.; Penteado Aranha, F.J.; Antonio de Souza, C.; Vigorito, A.C.; de Paula, E.V. Pretransplant β-microglobulin is associated with the risk of acute graft-versus-host-disease after allogeneic hematopoietic cell transplant. Biol. Blood Marrow Transplant. 2016, 22, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- Ganter, U.; Arcone, R.; Toniatti, C.; Morrone, G.; Ciliberto, G. Dual control of C-reactive protein gene expression by interleukin-1 and interleukin-6. EMBO J. 1989, 8, 3773–3779. [Google Scholar] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Schafer, Z.T.; Brugge, J.S. IL-6 involvement in epithelial cancers. J. Clin. Investig. 2007, 117, 3660–3663. [Google Scholar] [CrossRef] [PubMed]
- Treon, S.P.; Anderson, K.C. Interleukin-6 in multiple myeloma and related plasma cell dyscrasias. Curr. Opin. Hematol. 1998, 5, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Salgado, R.; Junius, S.; Benoy, I.; van Dam, P.; Vermeulen, P.; van Marck, E.; Huget, P.; Dirix, L.Y. Circulating interleukin-6 predicts survival in patients with metastatic breast cancer. Int. J. Cancer 2003, 103, 642–646. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, J.; Tachibana, M.; Horiguchi, Y.; Oya, M.; Ohigashi, T.; Asakura, H.; Murai, M. Serum interleukin 6 as a prognostic factor in patients with prostate cancer. Clin. Cancer Res. 2000, 6, 2702–2706. [Google Scholar]
- Seymour, J.F.; Talpaz, M.; Cabanillas, F.; Wetzler, M.; Kurzrock, R. Serum interleukin-6 levels correlate with prognosis in diffuse large-cell lymphoma. J. Clin. Oncol. 1995, 13, 575–582. [Google Scholar]
- Lucchini, G.; Willasch, A.M.; Daniel, J.; Soerensen, J.; Jarisch, A.; Bakhtiar, S.; Rettinger, E.; Brandt, J.; Klingebiel, T.; Bader, P. Epidemiology, risk factors, and prognosis of capillary leak syndrome in pediatric recipients of stem cell transplants: A retrospective single-center cohort study. Pediatr. Transplant. 2016. [Google Scholar] [CrossRef] [PubMed]
- Reikvam, H.; Gronningsaeter, I.S.; Ahmed, A.B.; Hatfield, K.; Bruserud, O. Metabolic serum profiles for patients receiving allogeneic stem cell transplantation: the pretransplant profile differs for patients with and without posttransplant capillary leak syndrome. Dis. Mark. 2015, 2015, 943430. [Google Scholar] [CrossRef] [PubMed]
- Lindas, R.; Tvedt, T.H.; Hatfield, K.J.; Reikvam, H.; Bruserud, O. Preconditioning serum levels of endothelial cell-derived molecules and the risk of posttransplant complications in patients treated with allogeneic stem cell transplantation. J. Transplant. 2014, 2014, 404096. [Google Scholar] [CrossRef] [PubMed]
- Carreras, E. Early complications after HSCT. In The EBMT Handbook on Haematopoietic Stem Cell Transplantation; Apperley, J., Carreras, E., Gluckman, E., Masszi, T., Eds.; EMBT: Geneva, Switzerland, 2012; p. 184. [Google Scholar]
- Slevin, M.; Krupinski, J. A role for monomeric C-reactive protein in regulation of angiogenesis, endothelial cell inflammation and thrombus formation in cardiovascular/cerebrovascular disease? Histol. Histopathol. 2009, 24, 1473–1478. [Google Scholar] [PubMed]
- Fordjour, P.A.; Wang, Y.; Shi, Y.; Agyemang, K.; Akinyi, M.; Zhang, Q.; Fan, G. Possible mechanisms of C-reactive protein mediated acute myocardial infarction. Eur. J. Pharmacol. 2015, 760, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, G.A.; Varelias, A.; Vuckovic, S.; Le Texier, L.; Gartlan, K.H.; Zhang, P.; Thomas, G.; Anderson, L.; Boyle, G.; Cloonan, N.; et al. Addition of interleukin-6 inhibition with tocilizumab to standard graft-versus-host disease prophylaxis after allogeneic stem-cell transplantation: A phase 1/2 trial. Lancet Oncol. 2014, 15, 1451–1459. [Google Scholar] [CrossRef]
- Dambacher, J.; Beigel, F.; Seiderer, J.; Haller, D.; Goke, B.; Auernhammer, C.J.; Brand, S. Interleukin 31 mediates MAP kinase and STAT1/3 activation in intestinal epithelial cells and its expression is upregulated in inflammatory bowel disease. Gut 2007, 56, 1257–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagi, Y.; Andoh, A.; Nishida, A.; Shioya, M.; Nishimura, T.; Hashimoto, T.; Tsujikawa, T.; Saito, Y.; Fujiyama, Y. Interleukin-31 stimulates production of inflammatory mediators from human colonic subepithelial myofibroblasts. Int. J. Mol. Med. 2007, 19, 941–946. [Google Scholar] [CrossRef] [PubMed]
- Ip, W.K.; Wong, C.K.; Li, M.L.; Li, P.W.; Cheung, P.F.; Lam, C.W. Interleukin-31 induces cytokine and chemokine production from human bronchial epithelial cells through activation of mitogen-activated protein kinase signalling pathways: Implications for the allergic response. Immunology 2007, 122, 532–541. [Google Scholar] [CrossRef] [PubMed]
- Perrigoue, J.G.; Li, J.; Zaph, C.; Goldschmidt, M.; Scott, P.; de Sauvage, F.J.; Pearce, E.J.; Ghilardi, N.; Artis, D. IL-31-IL-31R interactions negatively regulate type 2 inflammation in the lung. J. Exp. Med. 2007, 204, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ishii, T.; Zhang, W.; Sozer, S.; Dai, Y.; Mascarenhas, J.; Najfeld, V.; Zhao, Z.J.; Hoffman, R.; Wisch, N.; et al. Involvement of mast cells by the malignant process in patients with Philadelphia chromosome negative myeloproliferative neoplasms. Leukemia 2009, 23, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Reikvam, H.; Mosevoll, K.A.; Melve, G.K.; Gunther, C.C.; Sjo, M.; Bentsen, P.T.; Bruserud, O. The pretransplantation serum cytokine profile in allogeneic stem cell recipients differs from healthy individuals, and various profiles are associated with different risks of posttransplantation complications. Biol. Blood Marrow Transplant. 2012, 18, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Ruutu, T.; Juvonen, E.; Remberger, M.; Remes, K.; Volin, L.; Mattsson, J.; Nihtinen, A.; Hagglund, H.; Ringden, O.; Nordic Group for Blood and Marrow Transplantation. Improved survival with ursodeoxycholic acid prophylaxis in allogeneic stem cell transplantation: Long-term follow-up of a randomized study. Biol. Blood Marrow Transplant. 2014, 20, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999, 94, 680–687. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age, Median and Range (Years) | 47.5 (15–70) |
|---|---|
| Caucasian/non-Caucasian (number) | 95/5 |
| Diagnosis (number) | |
| AML | 43 |
| MDS-AML | 16 |
| Myelodysplastic syndrome (MDS), high-risk | 4 |
| Acute lymphoblastic leukemia | 20 |
| Chronic myeloid leukemia | 2 |
| Myelofibrosis | 4 |
| Chronic myelomonocytic leukemia | 2 |
| Myeloproliferative neoplasia, unspecified | 2 |
| Aplastic anemia | 4 |
| Chronic lymphocytic leukemia | 2 |
| Hodgkin’s lymphoma | 1 |
| Remission at transplantation (number) | 99 |
| aGVHD requiring high dose steroid treatment (number) 1 | 46 |
| Conditioning regimes (number) | |
| Busulfan + cyclophosphamide (myeloablative condition) | 74 |
| Fludarabine + busulfan (reduced intensity conditioning) | 17 |
| Antithymocyte globulin + cyclophosphamide | 4 |
| Others | 5 |
| GVHD prophylaxis (number) | |
| Cyclosporine A + methotrexate | 97 |
| Cyclosporine A + mycophenolate mofetil | 1 |
| Cyclosporine A + methotrexate + antithymocyte globulin | 2 |
| Donor (number) | |
| Related | 100 |
| Sibling | 93 |
| Parent | 6 |
| Other related | 1 |
| Female/male donor | 39/61 |
| Female donor to male recipient | 21 |
| CMV pos. recipient | 65 |
| CMV pos. donor to neg. recipient | 18 |
| Stem cell source (number) | |
| Bone marrow grafts | 5 |
| G-CSF mobilized peripheral blood stem cell grafts | 95 |
| CRP mg/L (median and range; lower limit of detection being 1.0 mg/L) | 5 (<1–120) |
| Maximum weight gain kg (median, range) | 5.0 (0–16.1) |
| Mediator | All Allotransplant Patients | Healthy Controls | p-Value | LLOD | ||||
|---|---|---|---|---|---|---|---|---|
| Median | Range | IQR | Median | Range | IQR | |||
| OSM | 6.7 | (6.7–89.3) | 2.6 | 7.3 | (6.7–111.9) | 25.4 | 0.13 | 6.7 |
| CNTF | 701 | (127–15,464) | 1874 | 502 | (127–11,819) | 0.67 | 127 | |
| IL-6 | 12.6 | (0.92–581) | 19.6 | 3.0 | (0.9–7.2) | 4.2 | <0.01 | 0.9 |
| sIL-6R | 11,580 | (609–42,666) | 10,722 | 8427 | (4936–22,594) | 10,541 | 0.09 | 18.7 |
| sgp130 | 54,808 | (8286–226,166) | 60,005 | 39,776 | (32,525–134,172) | 67,302 | 0.049 | 81.0 |
| sgp130-sIL-6R difference | 4306 | (−20,977–206,959) | 48,710 | 32,283 | (27,387–1,114,152) | 58,499 | 0.10 | NR |
| IL-31 | 7.12 | (2.59–130.80) | 7.52 | 8.70 | (2.59–25.51) | 8.62 | 0.1856 | 2.59 |
| Preconditioning Peripheral Blood Cell Counts | ||
| Peripheral Blood Parameter | IL-6 Family Cytokine | Correlation |
| Hemoglobin level | IL-6 | −0.40 |
| Total leukocyte count | OSM | 0.27 |
| Hematopoietic Reconstitution after Allotransplantation | ||
| Mediator | Neutrophils above 0.2 × 109/L | Platelets above 20 × 109/L |
| IL-6 | 0.12 | 0.19 |
| sIL-6R | 0.283 | 0.12 |
| sgp130 | 0.238 | 0.05 |
| Diff | 0.215 | 0.02 |
| CNTF | 0.19 | 0.01 |
| OSM | 0.01 | −0.06 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tvedt, T.H.; Lie, S.A.; Reikvam, H.; Rye, K.P.; Lindås, R.; Gedde-Dahl, T.; Ahmed, A.B.; Bruserud, Ø. Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation. Int. J. Mol. Sci. 2016, 17, 1823. https://doi.org/10.3390/ijms17111823
Tvedt TH, Lie SA, Reikvam H, Rye KP, Lindås R, Gedde-Dahl T, Ahmed AB, Bruserud Ø. Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation. International Journal of Molecular Sciences. 2016; 17(11):1823. https://doi.org/10.3390/ijms17111823
Chicago/Turabian StyleTvedt, Tor Henrik, Stein Atle Lie, Håkon Reikvam, Kristin Paulsen Rye, Roald Lindås, Tobias Gedde-Dahl, Aymen Bushra Ahmed, and Øystein Bruserud. 2016. "Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation" International Journal of Molecular Sciences 17, no. 11: 1823. https://doi.org/10.3390/ijms17111823
APA StyleTvedt, T. H., Lie, S. A., Reikvam, H., Rye, K. P., Lindås, R., Gedde-Dahl, T., Ahmed, A. B., & Bruserud, Ø. (2016). Pretransplant Levels of CRP and Interleukin-6 Family Cytokines; Effects on Outcome after Allogeneic Stem Cell Transplantation. International Journal of Molecular Sciences, 17(11), 1823. https://doi.org/10.3390/ijms17111823