
A Novel Inflammation-Based Stage (I Stage) Predicts Overall Survival of Patients with Nasopharyngeal Carcinoma

Abstract
:
1. Introduction
2. Results
2.1. Patient Characteristics
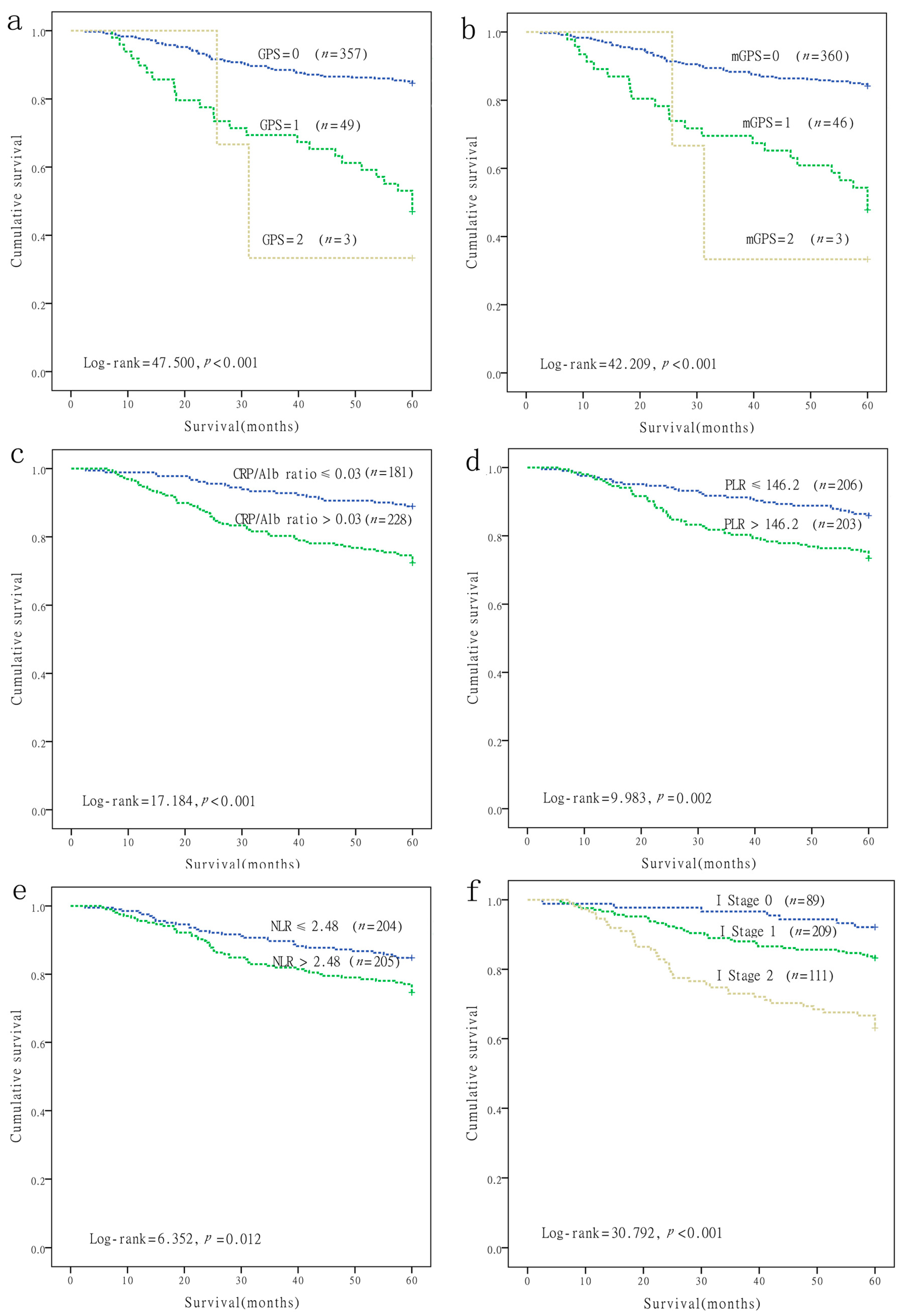
2.2. Prognostic Value of Inflammation-Based Prognostic Scores in Nasopharyngeal Carcinoma (NPC)
2.3. A Novel Inflammation-Based Stage (I Stage) Was Constructed by Combining Independent Risk Factors
2.4. The Relationship between I Stage and Clinicopathological Characteristics
2.5. Comparison of the AUCs for the Inflammation-Based Prognostic Scores
3. Discussion
4. Materials and Methods
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lee, A.W.; Ng, W.; Chan, Y.; Sze, H.; Chan, C.; Lam, T. The battle against nasopharyngeal cancer. Radiother. Oncol. 2012, 104, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Adami, H.-O. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [PubMed]
- Xu, F.-H.; Xiong, D.; Xu, Y.-F.; Cao, S.-M.; Xue, W.-Q.; Qin, H.-D.; Liu, W.-S.; Cao, J.-Y.; Zhang, Y.; Feng, Q.-S.; et al. An epidemiological and molecular study of the relationship between smoking, risk of nasopharyngeal carcinoma, and Epstein–Barr virus activation. J. Natl. Cancer Inst. 2012, 104, 1396–1410. [Google Scholar] [CrossRef] [PubMed]
- Young, L.S.; Dawson, C.W. Epstein-Barr virus and nasopharyngeal carcinoma. Chin. J. Cancer 2014, 33, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Ng, W.; Chan, L.; Chan, O.S.; Hung, W.; Chan, C.; Cheng, P.T.; Sze, H.; Lam, T.; Yau, T. The strength/weakness of the AJCC/UICC staging system for nasopharyngeal cancer and suggestions for future improvement. Oral Oncol. 2012, 48, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Muliawati, Y.; Haroen, H.; Rotty, L. Cancer anorexia-cachexia syndrome. Pathogenesis 2012, 5, 5. [Google Scholar]
- McMillan, D.C. Systemic inflammation, nutritional status and survival in patients with cancer. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed]
- Bromberg, J.; Wang, T.C. Inflammation and cancer: IL-6 and STAT3 complete the link. Cancer Cell 2009, 15, 79–80. [Google Scholar] [CrossRef] [PubMed]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Huang, D. The value of the systematic inflammation-based Glasgow Prognostic Score in patients with gastric cancer: A literature review. J. Cancer Res. Ther. 2014, 10, 799. [Google Scholar] [CrossRef] [PubMed]
- Hirashima, K.; Watanabe, M.; Shigaki, H.; Imamura, Y.; Ida, S.; Iwatsuki, M.; Ishimoto, T.; Iwagami, S.; Baba, Y.; Baba, H. Prognostic significance of the modified Glasgow Prognostic Score in elderly patients with gastric cancer. J. Gastroenterol. 2014, 49, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.-F.; Huang, Y.; Chen, Q.-X. Preoperative platelet lymphocyte ratio (PLR) is superior to neutrophil lymphocyte ratio (NLR) as a predictive factor in patients with esophageal squamous cell carcinoma. World J. Surg. Oncol. 2014, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhou, G.-Q.; Liu, X.; Chen, L.; Li, W.-F.; Tang, L.-L.; Liu, Q.; Sun, Y.; Ma, J. Exploration and validation of C-reactive protein/albumin ratio as a novel inflammation-based prognostic marker in nasopharyngeal carcinoma. J. Cancer Prev. 2016, 7, 1406. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc. Nutr. Soc. 2008, 67, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, E.; Cairns, E.; Hamilton, J.; Kelly, C. Evaluation of a modified early warning system for acute medical admissions and comparison with C-reactive protein/albumin ratio as a predictor of patient outcome. Clin. Med. 2009, 9, 30–33. [Google Scholar] [CrossRef]
- Pinato, D.; Shiner, R.; Seckl, M.; Stebbing, J.; Sharma, R.; Mauri, F. Prognostic performance of inflammation-based prognostic indices in primary operable non-small cell lung cancer. Br. J. Cancer 2014, 110, 1930–1935. [Google Scholar] [CrossRef] [PubMed]
- Dutta, S.; Al-Mrabt, N.M.; Fullarton, G.M.; Horgan, P.G.; McMillan, D.C. A comparison of POSSUM and GPS models in the prediction of post-operative outcome in patients undergoing oesophago-gastric cancer resection. Ann. Surg. Oncol. 2011, 18, 2808–2817. [Google Scholar] [CrossRef] [PubMed]
- Lindenmann, J.; Fink-Neuboeck, N.; Koesslbacher, M.; Pichler, M.; Stojakovic, T.; Roller, R.E.; Maier, A.; Anegg, U.; Smolle, J.; Smolle-Juettner, F.M. The influence of elevated levels of C-reactive protein and hypoalbuminemia on survival in patients with advanced inoperable esophageal cancer undergoing palliative treatment. J. Surg. Oncol. 2014, 110, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Ishizuka, M.; Kubota, K.; Kita, J.; Shimoda, M.; Kato, M.; Sawada, T. Impact of an inflammation-based prognostic system on patients undergoing surgery for hepatocellular carcinoma: A retrospective study of 398 Japanese patients. Am. J. Surg. 2012, 203, 101–106. [Google Scholar] [CrossRef]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M.; et al. The Glasgow Prognostic Score, an inflammation based prognostic score, predicts survival in patients with hepatocellular carcinoma. BMC Cancer 2013, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.W. Tumour-educated macrophages promote tumour progression and metastasis. Nat. Rev. Cancer 2004, 4, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Schreiber, R.D.; Old, L.J.; Smyth, M.J. Cancer immunoediting: Integrating immunity’s roles in cancer suppression and promotion. Science 2011, 331, 1565–1570. [Google Scholar] [CrossRef] [PubMed]
- Kusumanto, Y.H.; Dam, W.A.; Hospers, G.A.; Meijer, C.; Mulder, N.H. Platelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular endothelial growth factor. Angiogenesis 2003, 6, 283–287. [Google Scholar] [CrossRef] [PubMed]
- El-Hag, A.; Clark, R.A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system. J. Immunol. 1987, 139, 2406–2413. [Google Scholar] [PubMed]
- Germano, G.; Allavena, P.; Mantovani, A. Cytokines as a key component of cancer-related inflammation. Cytokine 2008, 43, 374–379. [Google Scholar] [CrossRef]
- Xia, W.-X.; Ye, Y.-F.; Lu, X.; Wang, L.; Ke, L.-R.; Zhang, H.-B.; Roycik, M.D.; Yang, J.; Shi, J.-L.; Cao, K.-J.; et al. The impact of baseline serum C-reactive protein and C-reactive protein kinetics on the prognosis of metastatic nasopharyngeal carcinoma patients treated with palliative chemotherapy. PLoS ONE 2013, 8, e76958. [Google Scholar] [CrossRef] [PubMed]
- Osugi, J.; Muto, S.; Matsumura, Y.; Higuchi, M.; Suzuki, H.; Gotoh, M. Prognostic impact of the high-sensitivity modified Glasgow Prognostic Score in patients with resectable non-small cell lung cancer. J. Cancer Res. Ther. 2016, 12, 945–951. [Google Scholar] [PubMed]
- Yamada, S.; Fujii, T.; Yabusaki, N.; Murotani, K.; Iwata, N.; Kanda, M.; Tanaka, C.; Nakayama, G.; Sugimoto, H.; Koike, M.; et al. Clinical implication of inflammation-based prognostic score in pancreatic cancer: Glasgow Prognostic Score is the most reliable parameter. Medicine 2016, 95, e3582. [Google Scholar] [CrossRef] [PubMed]
- Kimura, J.; Kunisaki, C.; Makino, H.; Oshima, T.; Ota, M.; Oba, M.; Takagawa, R.; Kosaka, T.; Ono, H.A.; Akiyama, H.; et al. Evaluation of the Glasgow Prognostic Score in patients receiving chemoradiotherapy for stage III and IV esophageal cancer. Dis. Esophagus 2015. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.C.; Yi, Y.; Fu, Y.P.; He, H.W.; Cai, X.Y.; Wang, J.X.; Zhou, J.; Cheng, Y.F.; Jin, J.J.; Fan, J.; et al. Prognostic value of the modified Glasgow Prognostic Score in patients undergoing radical surgery for hepatocellular carcinoma. Medicine 2015, 94, e1486. [Google Scholar] [CrossRef] [PubMed]
- Mcmillan, D.C.; Crozier, J.E.; Canna, K.; Angerson, W.J.; Mcardle, C.S. Evaluation of an inflammation-based prognostic score (GPS) in patients undergoing resection for colon and rectal cancer. Int. J. Colorectal Dis. 2007, 22, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Torre, M.L.; Nigri, G.; Cavallini, M.; Mercantini, P.; Ziparo, V.; Ramacciato, G. The Glasgow Prognostic Score as a predictor of survival in patients with potentially resectable pancreatic adenocarcinoma. Ann. Surg. Oncol. 2012, 19, 2917–2923. [Google Scholar] [CrossRef] [PubMed]
- Shafique, K.; Proctor, M.J.; Mcmillan, D.C.; Leung, H.; Smith, K.; Sloan, B.; Morrison, D.S. The modified Glasgow Prognostic Score in prostate cancer: Results from a retrospective clinical series of 744 patients. BMC Cancer 2013, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Talwar, D.; Balmar, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; Morrison, D.S.; Mcmillan, D.C. The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow inflammation outcome study. Br. J. Cancer 2011, 103, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Tanaka, K.; Fushiya, N.; Koike, K.; Nishino, H.; Matsushima, M. The C-reactive protein/albumin ratio, a novel inflammation-based prognostic score, predicts outcomes in patients with hepatocellular carcinoma. Ann. Surg. Oncol. 2015, 22, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.-L.; Wang, F.-H.; Zhang, D.-S.; Qiu, M.-Z.; Ren, C.; Jin, Y.; Zhou, Y.-X.; Wang, D.-S.; He, M.-M.; Bai, L.; et al. A novel inflammation-based prognostic score in esophageal squamous cell carcinoma: The C-reactive protein/albumin ratio. BMC Cancer 2015, 15, 1. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Zhang, L.; Luo, M.; Hu, G.; Mei, Q.; Liu, D.; Long, G.; Hu, G. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: Neutrophil-lymphocyte ratio and platelet-lymphocyte ratio. Head Neck 2015, 38, E1332–E1340. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Chen, L.; Zhang, Y.; Guo, R.; Li, W.F.; Mao, Y.P.; Tan, L.L.; Sun, Y.; Zhang, F.; Liu, L.Z.; et al. Survival analysis of patients with advanced-stage nasopharyngeal carcinoma according to the Epstein-Barr virus status. Oncotarget 2016, 7, 24208–24216. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Wei, S.; Su, L.; Lv, W.; Hong, J. Prognostic significance of pretreated serum lactate dehydrogenase level in nasopharyngeal carcinoma among Chinese population: A meta-analysis. Medicine 2016, 95, e4494. [Google Scholar] [CrossRef] [PubMed]
- Gu, A.D.; Zeng, M.S.; Qian, C.N. The criteria to confirm the role of Epstein-Barr virus in nasopharyngeal carcinoma initiation. Int. J. Mol. Sci. 2012, 13, 13737–13747. [Google Scholar] [CrossRef] [PubMed]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.; Farid, S.; Malik, H.; Young, A.; Toogood, G.; Lodge, J.; Prasad, K. Preoperative neutrophil-to-lymphocyte ratio as a prognostic predictor after curative resection for hepatocellular carcinoma. World J. Surg. 2008, 32, 1757–1762. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | No. of Patients (%) | S.T. (Month) Mean (95%, CI) | Five-year OS (%) Mean ± SD | p-Value |
|---|---|---|---|---|
| Gender | 0.004 | |||
| Male | 288 (70.4%) | 52.4 (50.6–54.2) | 76.0 ± 2.5 | |
| Female | 121 (29.6%) | 56.9 (55.1–58.7) | 88.4 ± 2.9 | |
| Age (years) | 0.002 | |||
| ≤45 | 216 (52.8%) | 55.0 (53.2–56.8) | 85.6 ± 2.4 | |
| >45 | 193 (47.2%) | 52.3 (50.1–54.5) | 73.1 ± 3.2 | |
| Tumor stage | 0.006 | |||
| T1 | 38 (9.3%) | 57.4 (55.1–59.8) | 86.8 ± 5.5 | |
| T2 | 109 (26.7%) | 55.8 (53.3–58.2) | 88.1 ± 3.1 | |
| T3 | 161 (39.4%) | 53.1 (50.7–55.5) | 78.9 ± 3.2 | |
| T4 | 101 (24.7%) | 51.2 (48.1–54.3) | 69.3 ± 4.6 | |
| Node stage | <0.001 | |||
| N0 | 75 (18.3%) | 55.5 (52.7–58.3) | 82.7 ± 4.4 | |
| N1 | 140 (34.2%) | 57.5 (56.1–58.9) | 87.9 ± 2.8 | |
| N2 | 149 (36.4%) | 52.6 (50.0–55.2) | 79.2 ± 3.3 | |
| N3 | 45 (11.0%) | 42.9 (37.0–48.8) | 51.1 ± 7.5 | |
| TNM stage | 0.001 | |||
| I–II | 77 (18.8%) | 58.9 (57.5–60.3) | 93.5 ± 2.8 | |
| III–IV | 332 (81.2%) | 52.5 (50.9–54.2) | 76.5 ± 2.3 | |
| Distant metastases | <0.001 | |||
| Yes | 64 (15.6%) | 34.2 (29.9–38.5) | 18.8 ± 4.9 | |
| No | 345 (84.4%) | 57.4 (56.3–58.5) | 91.0 ± 1.5 | |
| Treatment | 0.047 | |||
| Radiotherapy | 74 (18.1%) | 57.8 (55.8–59.8) | 87.8 ± 3.8 | |
| Chemoradiotherapy | 335 (81.9%) | 52.9 (51.2–54.5) | 77.9 ± 2.3 | |
| GPS | <0.001 | |||
| 0 | 357 (87.3%) | 55.0 (53.7–56.4) | 84.6 ± 1.9 | |
| 1 | 49 (12.0%) | 45.2 (39.7–50.7) | 46.9 ± 7.1 | |
| 2 | 3 (0.7%) | 39.0 (22.0–56.0) | 33.3 ± 27.2 | |
| mGPS | <0.001 | |||
| 0 | 360 (88.0%) | 55.0 (53.5–56.3) | 84.2 ± 1.9 | |
| 1 | 46 (11.3%) | 45.4 (39.7–51.2) | 47.8 ± 7.4 | |
| 2 | 3 (0.7%) | 39.0 (22.0–56.0) | 33.3 ± 27.2 | |
| CRP/Alb ratio | <0.001 | |||
| ≤0.03 | 181 (44.3%) | 56.8 (55.2–58.3) | 89.0 ± 2.3 | |
| >0.03 | 228 (55.7%) | 51.3 (49.2–53.5) | 72.4 ± 3.0 | |
| PLR | 0.002 | |||
| ≤146.2 | 206 (50.4%) | 55.8 (54.1–57.5) | 85.9 ± 2.4 | |
| >146.2 | 203 (49.6%) | 51.6 (49.4–53.9) | 73.4 ± 3.1 | |
| NLR | 0.012 | |||
| ≤2.48 | 204 (49.9%) | 55.2 (53.4–57.0) | 84.8 ± 2.5 | |
| >2.48 | 205 (50.1%) | 52.3 (50.1–54.4) | 74.6 ± 3.0 |
| Prognostic Factor | Coefficient | SE | p-Value | RR | 95.0% CI for RR |
|---|---|---|---|---|---|
| GPS | 1.404 | 0.727 | 0.053 | 4.070 | 0.980–16.908 |
| mGPS | −0.382 | 0.741 | 0.606 | 0.682 | 0.160–2.9149 |
| CRP/Alb ratio | 0.739 | 0.275 | 0.007 | 2.093 | 1.222–3.587 |
| PLR | 0.695 | 0.271 | 0.010 | 2.003 | 1.177–3.410 |
| NLR | 0.140 | 0.266 | 0.598 | 1.150 | 0.683–1.938 |
| Patient Characteristics | I Stage 0 | I Stage 1 | I Stage 2 | p-Value |
|---|---|---|---|---|
| n = (89), No. (%) | n = (209), No. (%) | n = (111), No. (%) | ||
| Gender | 0.402 | |||
| Male | 66 (74.2%) | 141 (67.5%) | 81 (73.0%) | |
| Female | 23 (25.8%) | 68 (32.5%) | 30 (27.0%) | |
| Age (years) | 0.487 | |||
| ≤45 | 52 (58.4%) | 107 (51.2%) | 57 (51.4%) | |
| >45 | 37 (41.6%) | 102 (48.8%) | 54 (48.6%) | |
| Tumor stage | 0.038 | |||
| T1 | 4 (4.5%) | 28 (13.4%) | 6 (5.4%) | |
| T2 | 31 (34.8%) | 53 (25.4%) | 25 (22.5%) | |
| T3 | 33 (37.1%) | 82 (39.2%) | 46 (41.4%) | |
| T4 | 21 (23.6%) | 46 (22.0%) | 34 (30.6%) | |
| Node stage | <0.001 | |||
| N0 | 15 (16.9%) | 43 (20.6%) | 17 (15.3%) | |
| N1 | 40 (44.9%) | 76 (36.4%) | 24 (21.6%) | |
| N2 | 31 (34.8%) | 74 (35.4%) | 44 (39.6%) | |
| N3 | 3 (3.4%) | 16 (7.7%) | 26 (23.4%) | |
| TNM stage | 0.014 | |||
| I–II | 22 (24.7%) | 44 (21.1%) | 11 (9.9%) | |
| III–IV | 67 (75.3%) | 165 (78.9%) | 100 (90.1%) | |
| Distant metastases | <0.001 | |||
| Yes | 5 (5.6%) | 29 (13.9%) | 30 (27.0%) | |
| No | 84 (94.4%) | 180 (86.1%) | 81 (73.0%) | |
| Treatment | 0.831 | |||
| Radiotherapy | 17 (19.1%) | 39 (18.7%) | 18 (16.2%) | |
| Chemoradiotherapy | 72 (80.9%) | 170 (81.3%) | 93 (83.8%) |
| Scores | AUC | 95% CI | p-Value |
|---|---|---|---|
| GPS | 0.632 | (0.559–0.706) | <0.001 |
| mGPS | 0.622 | (0.548–0.695) | 0.001 |
| CRP/Alb ratio (categorical) | 0.626 | (0.562–0.691) | <0.001 |
| PLR (categorical) | 0.597 | (0.529–0.664) | 0.006 |
| NLR (categorical) | 0.579 | (0.510–0.647) | 0.027 |
| I Stage (categorical) | 0.670 | (0.606–0.735) | <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.-P.; Chen, S.-L.; Liu, X.-M.; He, X.; Xing, S.; Liu, Y.-J.; Lin, Y.-H.; Liu, W.-L. A Novel Inflammation-Based Stage (I Stage) Predicts Overall Survival of Patients with Nasopharyngeal Carcinoma. Int. J. Mol. Sci. 2016, 17, 1900. https://doi.org/10.3390/ijms17111900
Li J-P, Chen S-L, Liu X-M, He X, Xing S, Liu Y-J, Lin Y-H, Liu W-L. A Novel Inflammation-Based Stage (I Stage) Predicts Overall Survival of Patients with Nasopharyngeal Carcinoma. International Journal of Molecular Sciences. 2016; 17(11):1900. https://doi.org/10.3390/ijms17111900
Chicago/Turabian StyleLi, Jian-Pei, Shu-Lin Chen, Xiao-Min Liu, Xia He, Shan Xing, Yi-Jun Liu, Yue-Hao Lin, and Wan-Li Liu. 2016. "A Novel Inflammation-Based Stage (I Stage) Predicts Overall Survival of Patients with Nasopharyngeal Carcinoma" International Journal of Molecular Sciences 17, no. 11: 1900. https://doi.org/10.3390/ijms17111900
APA StyleLi, J. -P., Chen, S. -L., Liu, X. -M., He, X., Xing, S., Liu, Y. -J., Lin, Y. -H., & Liu, W. -L. (2016). A Novel Inflammation-Based Stage (I Stage) Predicts Overall Survival of Patients with Nasopharyngeal Carcinoma. International Journal of Molecular Sciences, 17(11), 1900. https://doi.org/10.3390/ijms17111900