
The Systemic Profile of Soluble Immune Mediators in Patients with Myelodysplastic Syndromes


Abstract
:1. Introduction
2. Results
2.1. The Serum Levels of Single Mediators Show a Wide Variation between Myelodysplastic Syndromes (MDS) Patients
- The patient P-selectin levels were significantly lower than the corresponding levels in the healthy controls (median control levels 83,100 pg/mL, range 43,800–112,000 pg/mL; p = 0.001), whereas the patient levels of intercellular adhesion molecule 1 (ICAM-1) (median control level 146,000 pg/mL, range 76,100–329,000 pg/mL, p < 0.001) and vascular cell adhesion molecule 1 (VCAM-1) (median control level 652,000 pg/L, range 342,000–1,580,000, p < 0.001) were increased. Furthermore, the patient levels did not show any significant correlation with age for any of these soluble adhesion molecules.
- The patient levels were significantly lower than corresponding levels in healthy controls for MMP-2 (median control level 180,000 pg/mL, range 54,400–248,000 pg/mL, p < 0.001), MMP-3 (median control level 39,500 pg/mL, range 4600–160,000 pg/mL, p < 0.001), MMP-8 (median control level 6380 pg/mL, range 1708–12,100 pg/mL, p = 0.039), and MMP-9 (median control level 115,000 pg/mL, range 42,900–333,000 pg/mL, p < 0.001). In contrast, the patients showed increased MMP-7 levels compared with the controls (median control level 2060 pg/mL, range 944–8930 pg/mL, p < 0.001). Only MMP-3 showed a correlation with age for the MDS patient group.
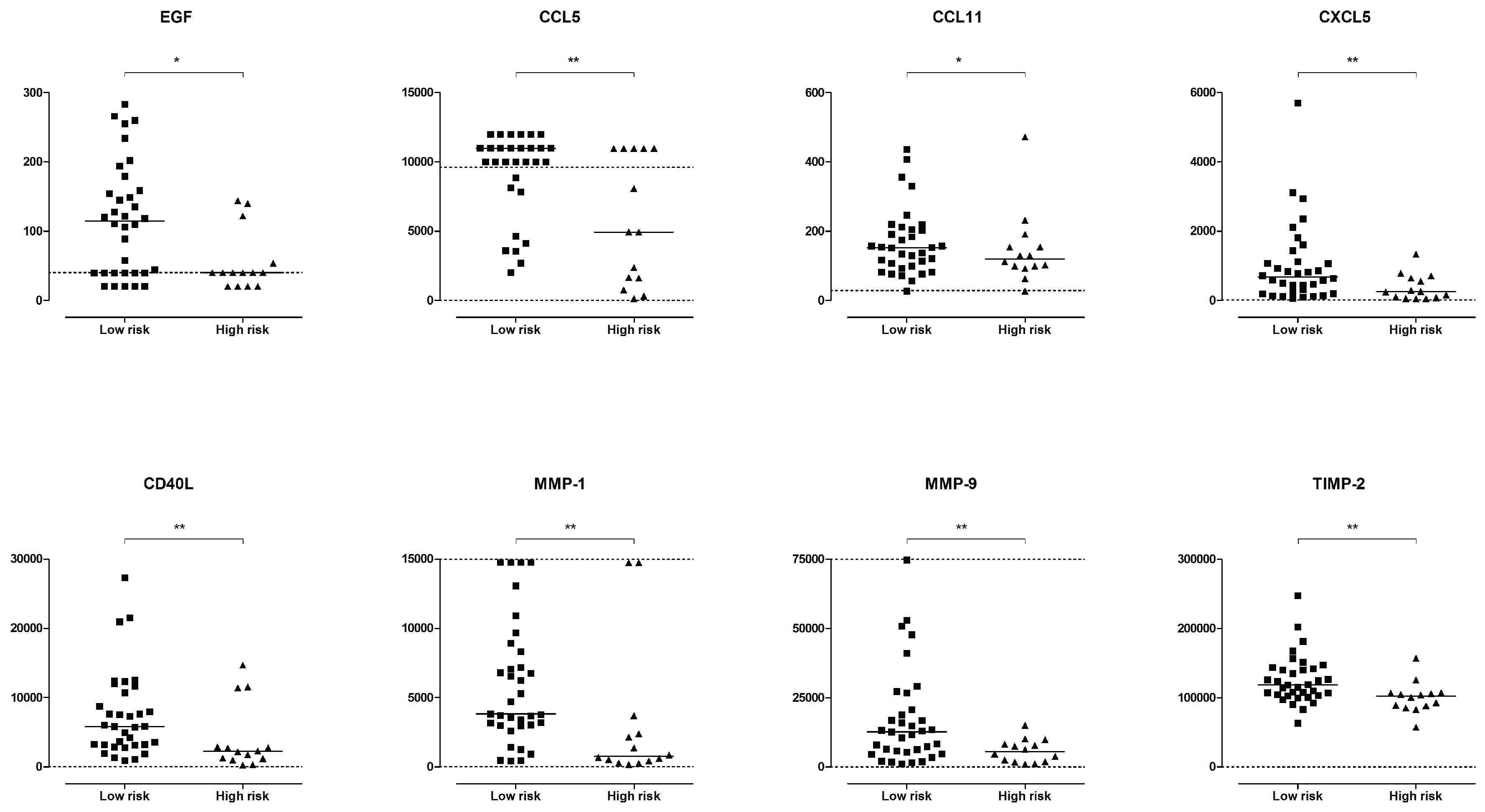
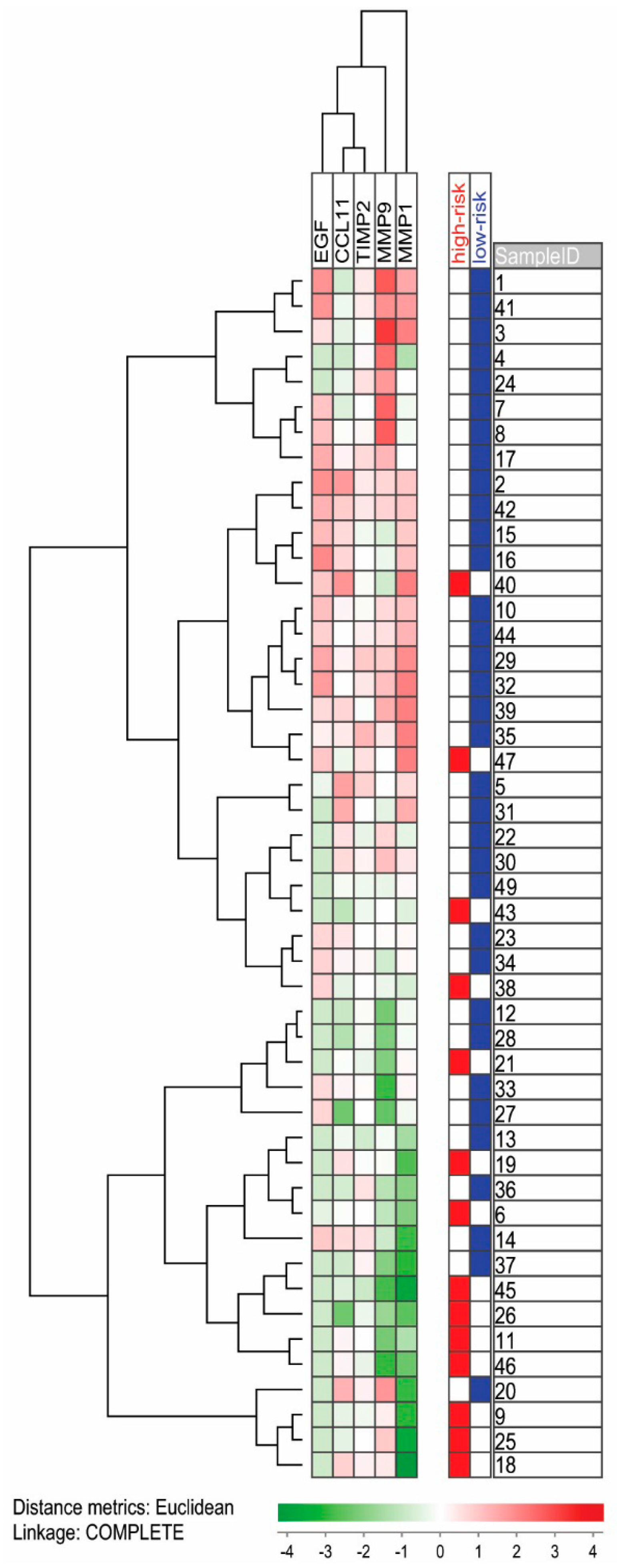
2.1.1. Serum Mediator Profiles Differ Slightly between High- and Low-Risk MDS Patients
2.1.2. Platelet Counts, Platelet-Derived Mediators and Serum Levels
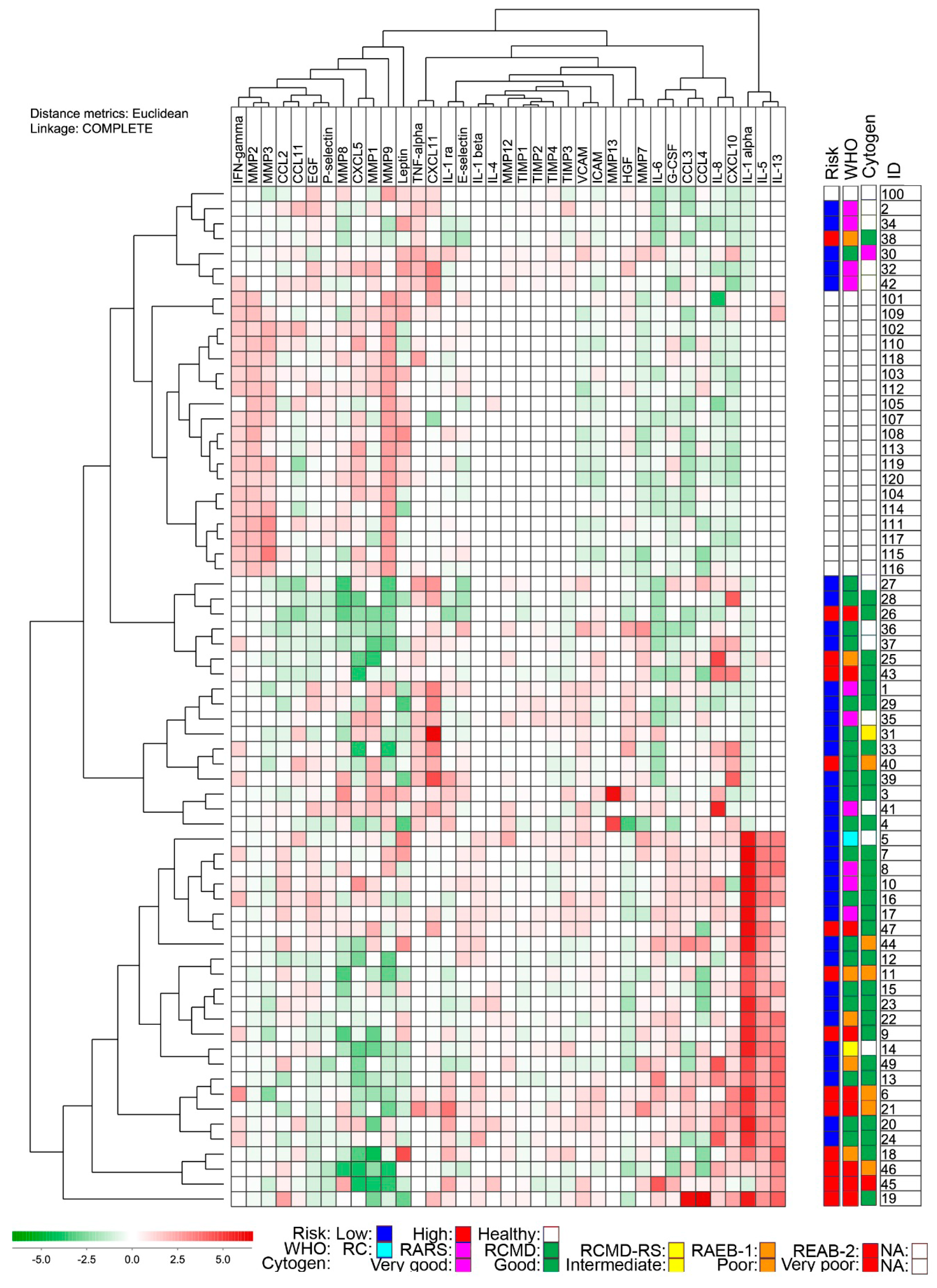
2.1.3. The Overall Serum Mediator Profile Shows a Wide Variation in MDS Patients and Cannot Distinguish between Low- and High-Risk Patients
2.1.4. Systemic Mediator Profiles Show Only Minor Variation over Time
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Sample Preparation and Analysis
4.3. Statistical and Bioinformatical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Corey, S.J.; Minden, M.D.; Barber, D.L.; Kantarjian, H.; Wang, J.C.; Schimmer, A.D. Myelodysplastic syndromes: The complexity of stem-cell diseases. Nat. Rev. Cancer 2007, 7, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Nimer, S.D. Myelodysplastic syndromes. Blood 2008, 111, 4841–4851. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.; Cox, C.; LeBeau, M.M.; Fenaux, P.; Morel, P.; Sanz, G.; Sanz, M.; Vallespi, T.; Hamblin, T.; Oscier, D.; et al. International scoring system for evaluating prognosis in myelodysplastic syndromes. Blood 1997, 89, 2079–2088. [Google Scholar] [PubMed]
- Sloand, E.M.; Mainwaring, L.; Fuhrer, M.; Ramkissoon, S.; Risitano, A.M.; Keyvanafar, K.; Lu, J.; Basu, A.; Barrett, A.J.; Young, N.S. Preferential suppression of trisomy 8 compared with normal hematopoietic cell growth by autologous lymphocytes in patients with trisomy 8 myelodysplastic syndrome. Blood 2005, 106, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Kordasti, S.Y.; Afzali, B.; Lim, Z.; Ingram, W.; Hayden, J.; Barber, L.; Matthews, K.; Chelliah, R.; Guinn, B.; Lombardi, G.; et al. IL-17-producing CD4+ T cells, pro-inflammatory cytokines and apoptosis are increased in low risk myelodysplastic syndrome. Br. J. Haematol. 2009, 145, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Qianqiao, Z.; Qi, H.; Feng, X.; Chunkang, C.; Xiao, L. In vitro deprivation of CD8+CD57+ T cells promotes the malignant growth of bone marrow colony cells in patients with lower-risk myelodysplastic syndrome. Exp. Hematol. 2010, 38, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Eksioglu, E.A.; Zhou, J.; Zhang, L.; Djeu, J.; Fortenbery, N.; Epling-Burnette, P.; van Bijnen, S.; Dolstra, H.; Cannon, J.; et al. Induction of myelodysplasia by myeloid-derived suppressor cells. J. Clin. Investig. 2013, 123, 4595–4611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kordasti, S.Y.; Ingram, W.; Hayden, J.; Darling, D.; Barber, L.; Afzali, B.; Lombardi, G.; Wlodarski, M.W.; Maciejewski, J.P.; Farzaneh, F.; et al. CD4+CD25high Foxp3+ regulatory T cells in myelodysplastic syndrome (MDS). Blood 2007, 110, 847–850. [Google Scholar] [CrossRef] [PubMed]
- Kittang, A.O.; Kordasti, S.; Sand, K.E.; Costantini, B.; Kramer, A.M.; Perezabellan, P.; Seidl, T.; Rye, K.P.; Hagen, K.M.; Kulasekararaj, A.; et al. Expansion of myeloid derived suppressor cells correlates with number of t regulatory cells and disease progression in myelodysplastic syndrome. Oncoimmunology 2016, 5, e1062208. [Google Scholar] [CrossRef] [PubMed]
- Verfaillie, C.M. Adhesion receptors as regulators of the hematopoietic process. Blood 1998, 92, 2609–2612. [Google Scholar] [PubMed]
- Kornblau, S.M.; Cohen, A.C.; Soper, D.; Huang, Y.W.; Cesano, A. Age-related changes of healthy bone marrow cell signaling in response to growth factors provide insight into low risk mds. Cytom. B Clin. Cytom. 2014, 86, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Kornblau, S.M.; McCue, D.; Singh, N.; Chen, W.; Estrov, Z.; Coombes, K.R. Recurrent expression signatures of cytokines and chemokines are present and are independently prognostic in acute myelogenous leukemia and myelodysplasia. Blood 2010, 116, 4251–4261. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Scheinberg, P.; Wu, C.O.; Samsel, L.; Nunez, O.; Prince, C.; Ganetzky, R.D.; McCoy, J.P., Jr.; Maciejewski, J.P.; Young, N.S. Cytokine signature profiles in acquired aplastic anemia and myelodysplastic syndromes. Haematologica 2011, 96, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Pardanani, A.; Finke, C.; Lasho, T.L.; Al-Kali, A.; Begna, K.H.; Hanson, C.A.; Tefferi, A. IPSS-independent prognostic value of plasma CXCL10, IL-7 AND IL-6 levels in myelodysplastic syndromes. Leukemia 2012, 26, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.O.; Kim, H.S.; Youn, J.C.; Shin, E.C.; Park, S. Serum cytokine profiles in healthy young and elderly population assessed using multiplexed bead-based immunoassays. J. Transl. Med. 2011, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Olsnes, A.M.; Motorin, D.; Ryningen, A.; Zaritskey, A.Y.; Bruserud, O. T lymphocyte chemotactic chemokines in acute myelogenous leukemia (AML): Local release by native human aml blasts and systemic levels of CXCL10 (IP-10), CCL5 (rantes) and CCL17 (TARC). Cancer Immunol. Immunother. 2006, 55, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Koike, M.; Ishiyama, T.; Tomoyasu, S.; Tsuruoka, N. Spontaneous cytokine overproduction by peripheral blood mononuclear cells from patients with myelodysplastic syndromes and aplastic anemia. Leuk. Res. 1995, 19, 639–644. [Google Scholar] [CrossRef]
- Wu, L.; Li, X.; Chang, C.; Ying, S.; He, Q.; Pu, Q. Deviation of type I and type II T cells and its negative effect on hematopoiesis in myelodysplastic syndrome. Int. J. Lab. Hematol. 2008, 30, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Tvedt, T.H.; Rye, K.P.; Reikvam, H.; Brenner, A.K.; Bruserud, O. The importance of sample collection when using single cytokine levels and systemic cytokine profiles as biomarkers—A comparative study of serum versus plasma samples. J. Immunol. Methods 2015, 418, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Bruserud, O.; Halstensen, A.; Peen, E.; Solberg, C.O. Serum levels of adhesion molecules and cytokines in patients with acute leukaemia. Leuk. Lymphoma 1996, 23, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Hatfield, K.J.; Reikvam, H.; Bruserud, O. The crosstalk between the matrix metalloprotease system and the chemokine network in acute myeloid leukemia. Curr. Med. Chem. 2010, 17, 4448–4461. [Google Scholar] [CrossRef] [PubMed]
- Bruserud, O. Bidirectional crosstalk between platelets and monocytes initiated by toll-like receptor: An important step in the early defense against fungal infections? Platelets 2013, 24, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Ries, C.; Loher, F.; Zang, C.; Ismair, M.G.; Petrides, P.E. Matrix metalloproteinase production by bone marrow mononuclear cells from normal individuals and patients with acute and chronic myeloid leukemia or myelodysplastic syndromes. Clin. Cancer Res. 1999, 5, 1115–1124. [Google Scholar] [PubMed]
- Iwata, M.; Pillai, M.; Ramakrishnan, A.; Hackman, R.C.; Deeg, H.J.; Opdenakker, G.; Torok-Storb, B. Reduced expression of inducible gelatinase B/matrix metalloproteinase-9 in monocytes from patients with myelodysplastic syndrome: Correlation of inducible levels with the percentage of cytogenetically marked cells and with marrow cellularity. Blood 2007, 109, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Travaglino, E.; Benatti, C.; Malcovati, L.; Della Porta, M.G.; Galli, A.; Bonetti, E.; Rosti, V.; Cazzola, M.; Invernizzi, R. Biological and clinical relevance of matrix metalloproteinases 2 and 9 in acute myeloid leukaemias and myelodysplastic syndromes. Eur. J. Haematol. 2008, 80, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Messingerova, L.; Jonasova, A.; Barancik, M.; Polekova, L.; Seres, M.; Gibalova, L.; Breier, A.; Sulova, Z. Lenalidomide treatment induced the normalization of marker protein levels in blood plasma of patients with 5q-myelodysplastic syndrome. Gen. Physiol. Biophys. 2015, 34, 399–406. [Google Scholar] [PubMed]
- Mitsiades, N.; Yu, W.H.; Poulaki, V.; Tsokos, M.; Stamenkovic, I. Matrix metalloproteinase-7-mediated cleavage of fas ligand protects tumor cells from chemotherapeutic drug cytotoxicity. Cancer Res. 2001, 61, 577–581. [Google Scholar] [PubMed]
- Sudhoff, T.; Germing, U.; Aul, C. Levels of circulating endothelial adhesion molecules in patients with myelodysplastic syndromes. Int. J. Oncol. 2002, 20, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Passam, F.H.; Tsirakis, G.; Boula, A.; Fragou, A.; Consolas, I.; Alegakis, A.; Kyriakou, D.S.; Alexandrakis, M.G. Levels of soluble forms of ICAM and VCAM in patients with myelodysplastic syndromes and their prognostic significance. Clin. Lab. Haematol. 2004, 26, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Waugh, D.J.; Wilson, C. The interleukin-8 pathway in cancer. Clin. Cancer Res. 2008, 14, 6735–6741. [Google Scholar] [CrossRef] [PubMed]
- Glenjen, N.; Hovland, R.; Wergeland, L.; Wendelbo, O.; Ernst, P.; Bruserud, O. The angioregulatory phenotype of native human acute myelogenous leukemia cells: Influence of karyotype, Flt3 abnormalities and differentiation status. Eur. J. Haematol. 2003, 71, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Schinke, C.; Giricz, O.; Li, W.; Shastri, A.; Gordon, S.; Barreyro, L.; Bhagat, T.; Bhattacharyya, S.; Ramachandra, N.; Bartenstein, M.; et al. IL8-CXCR2 pathway inhibition as a therapeutic strategy against mds and aml stem cells. Blood 2015, 125, 3144–3152. [Google Scholar] [CrossRef] [PubMed]
- Bruserud, O.; Ryningen, A.; Wergeland, L.; Glenjen, N.I.; Gjertsen, B.T. Osteoblasts increase proliferation and release of pro-angiogenic interleukin 8 by native human acute myelogenous leukemia blasts. Haematologica 2004, 89, 391–402. [Google Scholar] [PubMed]
- Appay, V.; van Lier, R.A.; Sallusto, F.; Roederer, M. Phenotype and function of human T lymphocyte subsets: Consensus and issues. Cytom. A 2008, 73, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Bonecchi, R.; Bianchi, G.; Bordignon, P.P.; D’Ambrosio, D.; Lang, R.; Borsatti, A.; Sozzani, S.; Allavena, P.; Gray, P.A.; Mantovani, A.; et al. Differential expression of chemokine receptors and chemotactic responsiveness of type 1T helper cells (Th1s) and Th2s. J. Exp. Med. 1998, 187, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Sallusto, F.; Lenig, D.; Mackay, C.R.; Lanzavecchia, A. Flexible programs of chemokine receptor expression on human polarized T helper 1 and 2 lymphocytes. J. Exp. Med. 1998, 187, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Strieter, R.M.; Kunkel, S.L.; Arenberg, D.A.; Burdick, M.D.; Polverini, P.J. Interferon γ-inducible Protein 10 (IP-10), a member of the C-X-C chemokine family, is an inhibitor of angiogenesis. Biochem. Biophys. Res. Commun. 1995, 210, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Guo, S.; Stiles, J.K. The emerging role of CXCL10 in cancer (review). Oncol. Lett. 2011, 2, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Ge, M.; Zheng, Y.; Li, X.; Lu, S.; Li, H.; Chen, F.; Chen, D.; Shao, Y.; Shi, J.; Feng, S. Differential expression profile of Th1/Th17/Th2-related chemokines and their receptors in patients with acquired bone marrow failure syndromes. Hum. Immunol. 2013, 74, 176–180. [Google Scholar] [CrossRef] [PubMed]
- Stavrum, A.K.; Petersen, K.; Jonassen, I.; Dysvik, B. Analysis of gene-expression data using J-Express. Curr. Protoc. Bioinform. 2008. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mediator | MDS Patients | Healthy Individuals | p-Value |
|---|---|---|---|
| Cytokines | |||
| IL-1ra | 761 (182–10,311) | 852 (503–1700) | <0.001 |
| IL-1α | 5.04 (bd–241) | n/a | n/a |
| IL-1β * | bd (bd–6.99) | n/a | n/a |
| IL-4 | bd (bd–51.4) | bd (bd–29.5) | ns |
| IL-5 | 4.17 (bd–16.3) | bd (bd–1.57) | <0.001 |
| IL-6 * | 5.85 (bd–88.7) | 3.47 (bd–5.23) | 0.013 |
| IL-10 * | bd (bd–22.8) | 3.87 (2.62–5.33) | <0.001 |
| IL-13 | bd (bd–362) | bd (bd–66.7) | 0.001 |
| Chemokines | |||
| CCL2 * | 276 (bd–1570) | 268 (146–632) | ns |
| CCL3 | 113 (bd–6370) | 55.2 (bd–137) | <0.001 |
| CCL4 * | 66.0 (bd–6320) | 64.7 (14.0–150) | ns |
| CCL5 | ad (134–ad) | ad (5060–ad) | 0.010 |
| CCL11 | 136 (bd–283) | 114 (30.4–500) | ns |
| CXCL5 | 566 (bd–5700) | 1 590 (425–4200) | <0.001 |
| CXCL8 * | 41.0 (8.10–1220) | 14.5 (1.69–37.8) | <0.001 |
| CXCL10 * | 59.0 (7.00–590) | 17.1 (9.16–57.6) | <0.001 |
| CXCL11 * | 40.5 (bd–2690) | bd (bd–167) | ns |
| Immunomodulatory cytokines | |||
| TNFα | 2.01 (bd–24.9) | 3.17 (bd–17.8) | ns |
| IFNγ * | bd (bd–6.97) | 2.94 (bd–3.57) | <0.001 |
| CD40L * | 3940 (264–27,300) | 7560 (4470–22,600) | 0.013 |
| Growth factors | |||
| EGF * | 73.4 (bd–283) | 80.1 (40.2–222) | ns |
| VEGF * | 86.5 (bd–275) | 84.2 (10.4–264) | ns |
| TPO | 467 (110–2058) | 779 (174–1057) | <0.001 |
| HGF | 275 (31.0–1605) | 385 (175–545) | ns |
| G-CSF * | 33.9 (bd–140) | 25.6 (bd–71.3) | ns |
| Leptin | 4750 (622–148,000) | 10,500 (1400–46,600) | ns |
| Adhesion molecules; serum levels in MDS patients | |||
| E-Selectin | 28,400 (6770–107,000) | ICAM-1 | 272,000 (84,100–589,000) |
| P-Selectin | 56,200 (18,100–126,000) | VCAM-1 | 1,220,000 (552,000–4,540,000) |
| Matrix metalloproteinases and inhibitors; serum levels in MDS patients | |||
| MMP-1 | 3570 (184–14,800) | MMP-12 | 8.50 (bd–38.3) |
| MMP-2 | 45,800 (36,000–62,500) | TIMP-1 | 166,000 (91,000–257,000) |
| MMP-3 | 12,500 (2720–17,800) | TIMP-2 | 108,000 (57,400–248,000) |
| MMP-7 | 4810 (993–31,100) | TIMP-3 | 27,400 (bd–77,400) |
| MMP-8 | 4260 (350–35,600) | TIMP-4 | 2080 (1110–4170) |
| MMP-9 | 8110 (1040–74,700) | ||
| Mediator | Low-Risk MDS | High-Risk MDS | p-Value |
|---|---|---|---|
| Cytokines | |||
| IL-1ra | 665 (318–4610) | 1032 (182–10,300) | ns |
| IL-1α | 2.75 (bd–241) | 23.9 (bd–203) | ns |
| IL-1β | bd (bd–6.99) | 0.87 (bd–4.04) | ns |
| IL-4 | bd (bd–46.0) | bd (bd–51.4) | ns |
| IL-5 | bd (bd–16.3) | 4.55 (bd–16.1) | ns |
| IL-6 | 5.55 (bd–39.2) | 5.85 (bd–88.7) | ns |
| IL-13 | bd (bd–292) | 103 (bd–362) | ns |
| Chemokines | |||
| CCL2 | 276 (bd–1570) | 268 (146–632) | ns |
| CCL3 | 113 (bd–6370) | 55.2 (bd–137) | ns |
| CCL4 | 66.0 (bd–6320) | 64.7 (14.0–150) | ns |
| CCL5 | ad (2010–ad) | ad (134–ad) | 0.001 |
| CCL11 | 136 (bd–283) | 114 (30.4–500) | 0.012 |
| CXCL5 | 566 (bd–5700) | 1590 (425–4200) | 0.004 |
| CXCL8 | 41.0 (8.1–1220) | 14.5 (1.69–37.8) | ns |
| CXCL10 | 59.0 (7.0–590) | 17.1 (9.16–57.6) | ns |
| CXCL11 | 40.5 (bd–2690) | bd (bd–167) | ns |
| Immunomodulatory cytokines | |||
| TNFα | 4.02 (bd–17.8) | bd (bd–24.9) | ns |
| IFNγ | bd (bd–3.35) | bd (bd–6.97) | ns |
| CD40L | 5830 (918–27,300) | 2260 (264–14,700) | 0.006 |
| Growth factors | |||
| EGF | 115 (bd–283) | bd (bd–144) | 0.011 |
| VEGF | 91.1 (17.1–191) | 69.1 (bd–275) | ns |
| TPO | 497 (110–1770) | 439 (154–2060) | ns |
| HGF | 290 (31.0–1610) | 273 (91.7–634) | ns |
| G-CSF | 32.4 (bd–89.0) | 38.7 (bd–140) | ns |
| Leptin | 4560 (622–54,700) | 4750 (786–148,000) | ns |
| Adhesion molecules | |||
| E-Selectin | 28,600 (6770–107,000) | 24,700 (8310–59,700) | ns |
| P-Selectin | 57,200 (18,100–126,000) | 54,800 (21,400–94,800) | ns |
| ICAM-1 | 239,000 (84,100–503,000) | 303,000 (118,000–589,000) | ns |
| VCAM-1 | 1,180,000 (553,000–4,540,000) | 1,380,000 (870,000–2,770,000) | ns |
| Matrix metalloproteinases and inhibitors | |||
| MMP-1 | 3820 (425–ad) | 777 (184–ad) | 0.003 |
| MMP-2 | 45,900 (37,300–62,500) | 44,700 (36,000–62,200) | ns |
| MMP-3 | 12,500 (5240–ad) | 12,100 (2720–ad) | ns |
| MMP-7 | 4710 (993–28,400) | 6100 (1640–31,100) | ns |
| MMP-8 | 4260 (438–35,600) | 4100 (350–24,100) | ns |
| MMP-9 | 12,500 (1070–74,700) | 5510 (1040–15,100) | 0.010 |
| MMP-12 | 8.20 (bd–38.3) | 8.50 (bd–16.2) | ns |
| TIMP-1 | 167,000 (98,400–257,000) | 135,000 (91,000–245,000) | ns |
| TIMP-2 | 119,000 (62,700–248,000) | 102,000 (57,400–158,000) | 0.006 |
| TIMP-3 | 34,300 (bd–77,400) | 9180 (bd–77,300) | ns |
| TIMP-4 | 2120 (1110–3500) | 1880 (1280–4170) | ns |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kittang, A.O.; Sand, K.; Brenner, A.K.; Rye, K.P.; Bruserud, Ø. The Systemic Profile of Soluble Immune Mediators in Patients with Myelodysplastic Syndromes. Int. J. Mol. Sci. 2016, 17, 1080. https://doi.org/10.3390/ijms17071080
Kittang AO, Sand K, Brenner AK, Rye KP, Bruserud Ø. The Systemic Profile of Soluble Immune Mediators in Patients with Myelodysplastic Syndromes. International Journal of Molecular Sciences. 2016; 17(7):1080. https://doi.org/10.3390/ijms17071080
Chicago/Turabian StyleKittang, Astrid Olsnes, Kristoffer Sand, Annette Katharina Brenner, Kristin Paulsen Rye, and Øystein Bruserud. 2016. "The Systemic Profile of Soluble Immune Mediators in Patients with Myelodysplastic Syndromes" International Journal of Molecular Sciences 17, no. 7: 1080. https://doi.org/10.3390/ijms17071080
APA StyleKittang, A. O., Sand, K., Brenner, A. K., Rye, K. P., & Bruserud, Ø. (2016). The Systemic Profile of Soluble Immune Mediators in Patients with Myelodysplastic Syndromes. International Journal of Molecular Sciences, 17(7), 1080. https://doi.org/10.3390/ijms17071080