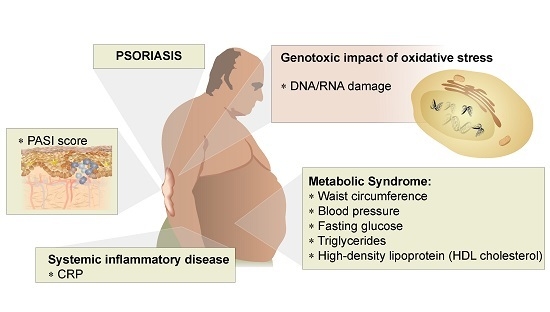
Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis

 , and
, and
Abstract
:
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Groups
4.2. Systemic Inflammation (CRP)
4.3. Oxidative Damage to Nucleic Acids
4.4. Metabolic Syndrome
4.5. Disease Status Determination
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Milic, M.; Frustaci, A.; del Bufalo, A.; Sanchez-Alarcon, J.; Valencia-Quintana, R.; Russo, P.; Bonassi, S. DNA damage in non-communicable diseases: A clinical and epidemiological perspective. Mutat. Res. 2015, 776, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Michalek, I.M.; Loring, B.; John, S.M. A systematic review of worldwide epidemiology of psoriasis. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Love, T.J.; Qureshi, A.A.; Karlson, E.W.; Gelfand, J.M.; Choi, H.K. Prevalence of the metabolic syndrome in psoriasis: Results from the National Health and Nutrition Examination Survey, 2003–2006. Arch. Dermatol. 2011, 147, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Vachatova, S.; Andrys, C.; Krejsek, J.; Salavec, M.; Ettler, K.; Rehacek, V.; Cermakova, E.; Malkova, A.; Fiala, Z.; Borska, L. Metabolic Syndrome and Selective Inflammatory Markers in Psoriatic Patients. J. Immunol. Res. 2016, 2016, 8. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Iinuma, S.; Honma, M.; Iizuka, H. Increased serum C-reactive protein level in Japanese patients of psoriasis with cardio- and cerebrovascular disease. J. Dermatol. 2014, 41, 981–985. [Google Scholar] [CrossRef] [PubMed]
- Vadakayil, A.R.; Dandekeri, S.; Kambil, S.M.; Ali, N.M. Role of C-reactive protein as a marker of disease severity and cardiovascular risk in patients with psoriasis. Indian Dermatol. Online J. 2015, 6, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Oliveira, H.; Reis, F.; Belo, L.; Rocha, S.; Quintanilha, A.; Figueiredo, A.; Teixeira, F.; Castro, E.; Rocha-Pereira, P.; et al. C-reactive protein and leucocyte activation in psoriasis vulgaris according to severity and therapy. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Beygi, S.; Lajevardi, V.; Abedini, R. C-reactive protein in psoriasis: A review of the literature. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Buring, J.E.; Cook, N.R.; Rifai, N. C-reactive protein, the metabolic syndrome, and risk of incident cardiovascular events: An 8-year follow-up of 14,719 initially healthy American women. Circulation 2003, 107, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.R.; Barton, M. GPER blockers as Nox downregulators: A new drug class to target chronic non-communicable diseases. J. Steroid Biochem. Mol. Biol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Rogulj, D.; El Aklouk, I.; Konjevoda, P.; Ljubic, S.; Pibernik Okanovic, M.; Barbir, A.; Luburic, M.; Radman, M.; Budinski, N.; Vucic Lovrencic, M. Age-dependent systemic DNA damage in early Type 2 Diabetes mellitus. Acta Biochim. Pol. 2017, 64, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Mantha, A.K.; Sarkar, B.; Tell, G. A short review on the implications of base excision repair pathway for neurons: Relevance to neurodegenerative diseases. Mitochondrion 2014, 16, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Nordholm, D.; Poulsen, H.E.; Hjorthoj, C.; Randers, L.; Nielsen, M.O.; Wulff, S.; Krakauer, K.; Norbak-Emig, H.; Henriksen, T.; Glenthoj, B.; et al. Systemic oxidative DNA and RNA damage are not increased during early phases of psychosis: A case control study. Psychiatry Res. 2016, 241, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Borska, L.; Andrys, C.; Krejsek, J.; Palicka, V.; Vorisek, V.; Hamakova, K.; Kremlacek, J.; Borsky, P.; Fiala, Z. Influence of dermal exposure to ultraviolet radiation and coal tar (polycyclic aromatic hydrocarbons) on the skin aging process. J. Dermatol. Sci. 2016, 81, 192–202. [Google Scholar] [CrossRef] [PubMed]
- Basavaraj, K.H.; Vasu Devaraju, P.; Rao, K.S. Studies on serum 8-hydroxy guanosine (8-OHdG) as reliable biomarker for psoriasis. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Kojanova, M.; Fialova, J.; Cetkovska, P.; Gkalpakiotis, S.; Jircikova, J.; Dolezal, T.; Arenberger, P. Characteristics and risk profile of psoriasis patients included in the Czech national registry BIOREP and a comparison with other registries. Int. J. Dermatol. 2017, 56, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Correa, M.M.; Thume, E.; De Oliveira, E.R.; Tomasi, E. Performance of the waist-to-height ratio in identifying obesity and predicting non-communicable diseases in the elderly population: A systematic literature review. Arch. Gerontol. Geriatr. 2016, 65, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Pirillo, I.; Tomassoni, D.; Sirignano, A.; Grappasonni, I. Metabolic syndrome, hypertension, and nervous system injury: Epidemiological correlates. Clin. Exp. Hypertens. 2017, 39, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Milcic, D.; Jankovic, S.; Vesic, S.; Milinkovic, M.; Marinkovic, J.; Cirkovic, A.; Jankovic, J. Prevalence of metabolic syndrome in patients with psoriasis: A hospital-based cross-sectional study. Anais Brasileiros de Dermatologia 2017, 92, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Sudhesan, A.; Rajappa, M.; Chandrashekar, L.; Ananthanarayanan, P.H.; Thappa, D.M.; Satheesh, S.; Chandrasekaran, A.; Devaraju, P. Association of C-Reactive Protein (rs1205) Gene Polymorphism with Susceptibility to Psoriasis in South Indian Tamils. J. Clin. Diagn. Res. 2016, 10, Gc01–Gc04. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. Psoriasis and metabolic syndrome: A systematic review and meta-analysis of observational studies. J. Am. Acad. Dermatol. 2013, 68, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Alsufyani, M.A.; Golant, A.K.; Lebwohl, M. Psoriasis and the metabolic syndrome. Dermatol. Ther. 2010, 23, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Seminara, N.M.; Shin, D.B.; Troxel, A.B.; Kimmel, S.E.; Mehta, N.N.; Margolis, D.J.; Gelfand, J.M. Prevalence of metabolic syndrome in patients with psoriasis: A population-based study in the United Kingdom. J. Investig. Dermatol. 2012, 132, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Miller, I.M.; Ellervik, C.; Zarchi, K.; Ibler, K.S.; Vinding, G.R.; Knudsen, K.M.; Jemec, G.B. The association of metabolic syndrome and psoriasis: A population- and hospital-based cross-sectional study. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Nappi, F.; Di Somma, C.; Savanelli, M.C.; Falco, A.; Balato, A.; Balato, N.; Savastano, S. Environmental Risk Factors in Psoriasis: The Point of View of the Nutritionist. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Neimann, A.L.; Shin, D.B.; Wang, X.; Margolis, D.J.; Troxel, A.B.; Gelfand, J.M. Prevalence of cardiovascular risk factors in patients with psoriasis. J. Am. Acad. Dermatol. 2006, 55, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Taheri Sarvtin, M.; Hedayati, M.T.; Shokohi, T.; HajHeydari, Z. Serum lipids and lipoproteins in patients with psoriasis. Arch. Iran. Med. 2014, 17, 343–346. [Google Scholar] [PubMed]
- Takahashi, H.; Iizuka, H. Psoriasis and metabolic syndrome. J. Dermatol. 2012, 39, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Akhyani, M.; Ehsani, A.H.; Robati, R.M.; Robati, A.M. The lipid profile in psoriasis: A controlled study. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 1330–1332. [Google Scholar] [CrossRef] [PubMed]
- Mallbris, L.; Granath, F.; Hamsten, A.; Stahle, M. Psoriasis is associated with lipid abnormalities at the onset of skin disease. J. Am. Acad. Dermatol. 2006, 54, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Huang, T. Oxidative stress in psoriasis and potential therapeutic use of antioxidants. Free Radic. Res. 2016, 50, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Borska, L.; Andrys, C.; Krejsek, J.; Palicka, V.; Chmelarova, M.; Hamakova, K.; Kremlacek, J.; Fiala, Z. Oxidative Damage to Nucleic Acids and Benzo(a)pyrene-7,8-diol-9,10-epoxide-DNA Adducts and Chromosomal Aberration in Children with Psoriasis Repeatedly Exposed to Crude Coal Tar Ointment and UV Radiation. Oxid. Med. Cell. Longev. 2014, 2014, 302528. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health; National Heart, Lung, and Blood Institute; National Cholesterol Education Program. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar]
- Salihbegovic, E.M.; Hadzigrahic, N.; Cickusic, A.J. Psoriasis and metabolic syndrome. Med. Arch. 2015, 69, 85–87. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; Version 3.4; R Foundation for Statistical Computing: Vienna, Austria, 2017; Available online: https://www.R-project.org/.
- Gross, J.; Ligges, U. Nortest: Tests for Normality, R Package Version 1.0-4; 2015. Available online: https://CRAN.R-project.org/package=nortest (accessed on 15 September 2017).
- Diedenhofen, B.; Musch, J. cocor: A comprehensive solution for the statistical comparison of correlations. PLoS ONE 2015, 10, e0121945. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients (n = 37) | Controls (n = 43) | p-Value |
|---|---|---|---|
| Age | 58 (53–62) | 56 (52–60) | 0.230 A |
| Gender (men/women) | 15/22 | 24/19 | - |
| PASI score | 15.8 (12.0–20.8) | - | - |
| With/without MetS | 23/14 | 18/25 | 0.078 C |
| Waist circumference (cm) | 97 (86–108) | 96 (87–102) | 0.200 B |
| Waist circumference men (cm) | 101 (90–119) | 100 (90–104) | 0.366 B |
| Waist circumference women (cm) | 97 (87–102) | 87 (84–99) | 0.161 B |
| Fasting glucose (mmol/L) | 5.7 (5.3–6.9) | 5.1 (4.7–6.3) | 0.007 A,** |
| TAG (mmol/L) | 1.6 (1.1–2.1) | 1.1 (0.8–1.7) | 0.040 A,* |
| HDL cholesterol (mmol/L) | 1.2 (1.1–1.5) | 1.0 (0.9–1.2) | <0.001 A,*** |
| HDL cholesterol, men (mmol/L) | 1.1 (1.0–1.4) | 1.0 (0.9–1.1) | 0.079 A |
| HDL cholesterol, women mmol/L) | 1.3 (1.2–1.6) | 1.2 (1.0–1.2) | 0.002 B,** |
| Systolic blood pressure (mmHg) | 135 (130–150) | 140 (128–150) | 0.463 B |
| Diastolic blood pressure (mmHg) | 90 (80–90) | 85 (80–90) | 0.210 A |
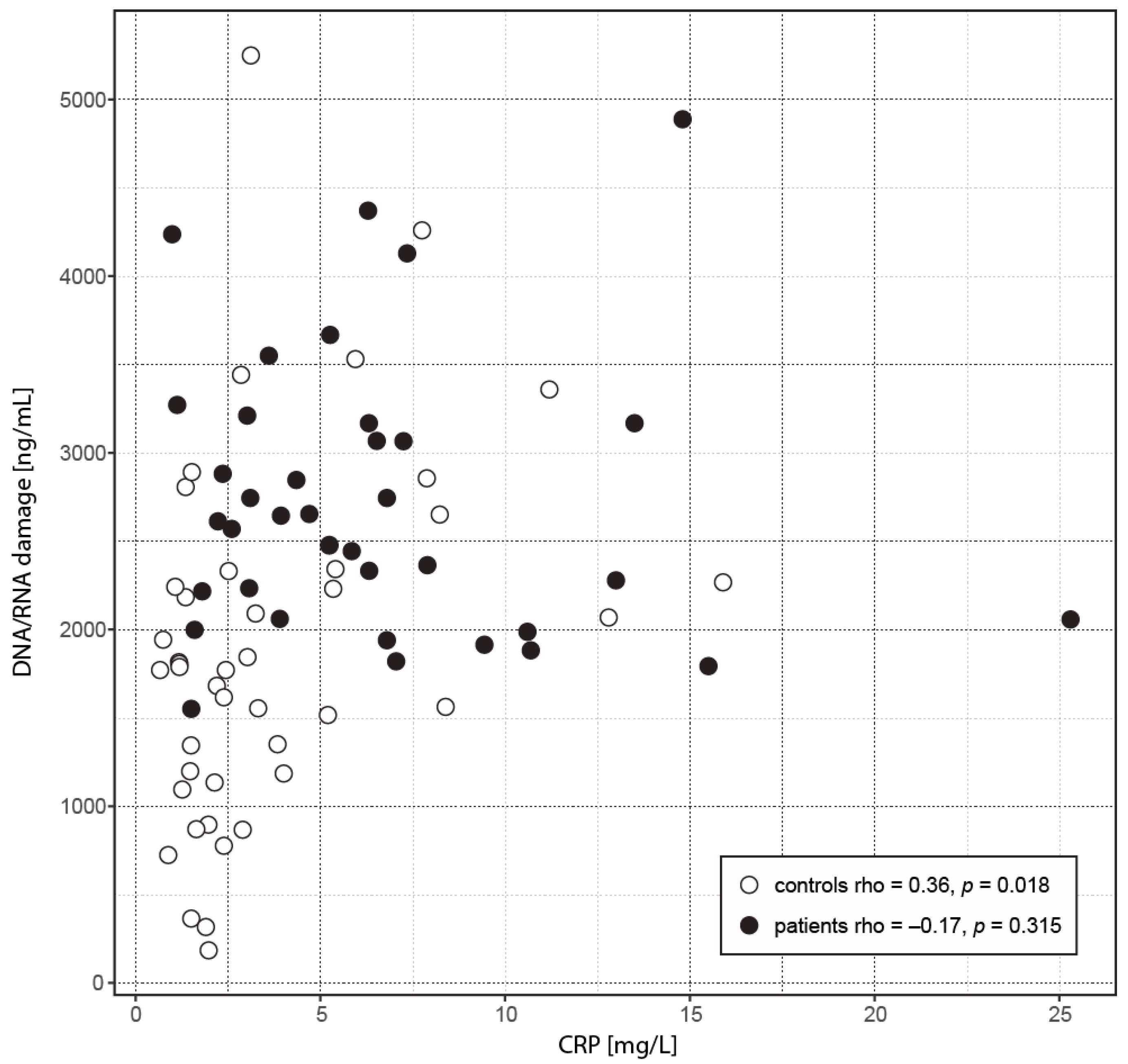
| CRP (mg/L) | 5.9 (3.1–7.4) | 2.4 (1.5–4.6) | <0.001 A,*** |
| DNA/RNA damage (pg/mL) | 2612 (2059–3168) | 1788 (1191–2298) | <0.001 A,*** |
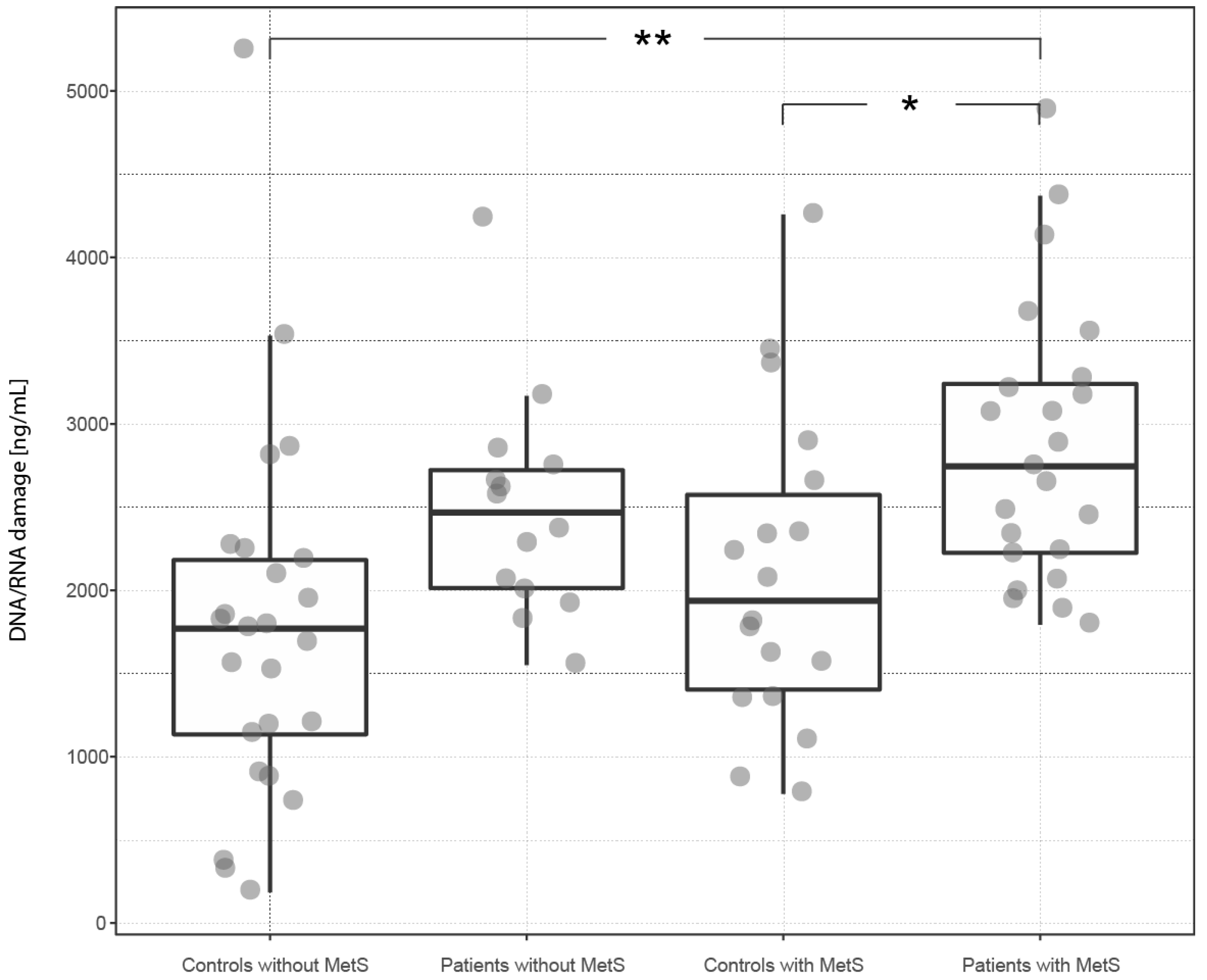
| Variable | Patients with MetS (n = 23) | Controls with MetS (n = 18) | p-Value |
| CRP (mg/L) | 6.3 (3.4–9.0) | 2.9 (2.4–7.2) | 0.108 A |
| DNA/RNA damage (pg/mL) | 2745 (2225–3241) | 1937 (1403–2573) | 0.049 * |
| Patients without MetS (n = 14) | Controls without MetS (n = 25) | ||
| CRP (mg/L) | 4.5 (2.3–7.0) | 2.0 (1.4–3.3) | 0.049 A,* |
| DNA/RNA damage (pg/mL) | 2467 (2013–2722) | 1770 (1134–2182) | 0.086 |
| Patients with MetS (n = 23) | Patients without MetS (n = 14) | ||
| CRP (mg/L) | 6.3 (3.4–9.0) | 4.5 (2.3–7.0) | 0.311 A |
| DNA/RNA damage (pg/mL) | 2745 (2225–3241) | 2467 (2013–2722) | 0.677 |
| Controls with MetS (n = 18) | Controls without MetS (n = 25) | ||
| CRP (mg/L) | 2.9 (2.4–7.2) | 2.0 (1.4–3.3) | 0.077 A |
| DNA/RNA damage (pg/mL) | 1937 (1403–2573) | 1770 (1134–2182) | 0.677 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borska, L.; Kremlacek, J.; Andrys, C.; Krejsek, J.; Hamakova, K.; Borsky, P.; Palicka, V.; Rehacek, V.; Malkova, A.; Fiala, Z. Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis. Int. J. Mol. Sci. 2017, 18, 2238. https://doi.org/10.3390/ijms18112238
Borska L, Kremlacek J, Andrys C, Krejsek J, Hamakova K, Borsky P, Palicka V, Rehacek V, Malkova A, Fiala Z. Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis. International Journal of Molecular Sciences. 2017; 18(11):2238. https://doi.org/10.3390/ijms18112238
Chicago/Turabian StyleBorska, Lenka, Jan Kremlacek, Ctirad Andrys, Jan Krejsek, Kvetoslava Hamakova, Pavel Borsky, Vladimir Palicka, Vit Rehacek, Andrea Malkova, and Zdenek Fiala. 2017. "Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis" International Journal of Molecular Sciences 18, no. 11: 2238. https://doi.org/10.3390/ijms18112238
APA StyleBorska, L., Kremlacek, J., Andrys, C., Krejsek, J., Hamakova, K., Borsky, P., Palicka, V., Rehacek, V., Malkova, A., & Fiala, Z. (2017). Systemic Inflammation, Oxidative Damage to Nucleic Acids, and Metabolic Syndrome in the Pathogenesis of Psoriasis. International Journal of Molecular Sciences, 18(11), 2238. https://doi.org/10.3390/ijms18112238