The Role of Toll-Like Receptors and Vitamin D in Cardiovascular Diseases—A Review


Abstract
:
{kind=link}
{kind=link}
1. Toll-Like Receptors
1.1. Toll-Like Receptors and Cardiovascular Diseases
1.2. Coronary and Cerebrovascular Atherosclerosis
1.3. Acute Coronary Syndrome
1.4. Stroke
1.5. Thrombosis
1.6. Heart Failure
1.7. Valvular Heart Disease
1.8. Arrhythmias
1.9. Hypertension
1.10. Cardiac Involvement in Infectious Diseases
2. Vitamin D
2.1. Vitamin D and Cardiovascular Diseases
2.2. Coronary and Cerebrovascular Atherosclerosis
2.3. Acute Coronary Syndrome
2.4. Stroke
2.5. Thrombosis
2.6. Heart Failure
2.7. Valvular Heart Disease
2.8. Arrhythmias
2.9. Hypertension
2.10. Cardiac Involvement in Infectious Diseases
3. Toll-Like Receptors and Vitamin D
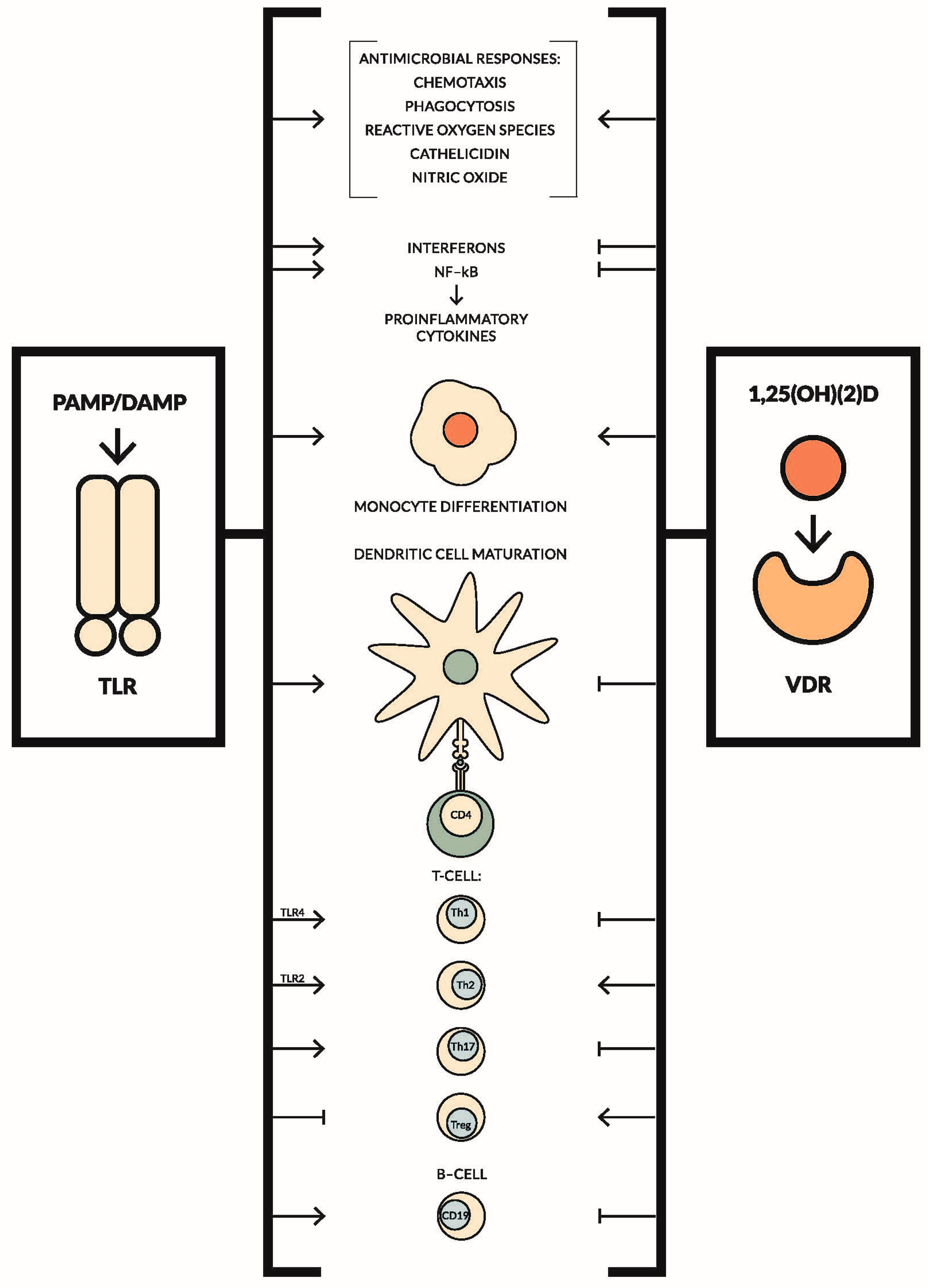
3.1. The Interplay between TLRs and Vitamin D in Relation to Innate and Adaptive Immune System
3.2. Toll-Like Receptors and Vitamin D in Cardiovascular Diseases
3.3. Emerging Role of Vitamin K2 in Cardiovascular Diseases and Its Relationship with TLRs and Vitamin D
3.4. Summary
Acknowledgments
Conflicts of Interest
Abbreviations
| TLRs | toll-like receptors |
| PRR | pattern-recognition receptor |
| PAMP | pathogen-associated molecular patterns |
| DAMP | danger-associated molecular patterns |
| TRIF | TIR-domain-containing adaptor inducing interferon-β |
| TIRAP | TIR domain-containing adaptor protein |
| TRAM | TRIF-related adaptor molecule |
| NF-κB | nuclear factor κ-light-chain-enhancer of activated B cells |
| HMGB1 | high-mobility group box 1 |
| CD | cluster of differentiation |
| Treg | T regulatory cell |
| DC | dendritic cell |
| Teff | T effector cell |
| MCP-1 | monocyte chemotactic protein-1 |
| TGF-β | transforming growth factor β |
| ApoE−/− mice | apolipoprotein E knockout mice |
| iNOS | inducible nitric oxide synthase |
| ROS | reactive oxygen species |
| BMP-2 | bone morphogenetic protein-2 |
| Runx2 | Runt-related transcription factor 2 |
| TNF-α | tumor necrosis factor alpha |
| IL-6 | interleukin 6 |
| Ito | potassium current |
| IFN3 | interferon regulatory factor 3 |
| SHR | spontaneously hypertensive rat |
| IRAK1 | interleukin-1 receptor-associated kinase 1 |
| LPS | Lipopolysaccharide |
| TNF | tumor necrosis factor |
| IL-1β | interleukin 1β |
| NO | nitric oxide |
| NOS2 | nitric oxide synthase 2 |
| EMCV | encephalomyocarditis virus |
| CVB3 | coxsackievirus group B serotype 3 |
| UVB radiation | ultraviolet B radiation |
| 25(OH)D | 25-hydroxyvitamin D, calcidiol |
| 1,25(OH)(2)D | 1,25-dihydroxyvitamin D, calcitriol |
| VDR | vitamin D receptor |
| HREs | hormone response elements |
| NHANES | national health and nutrition examination survey |
| RAAS | renin-angiotensin system |
| NADPH | reduced nicotinamide adenine dinucleotide phosphate |
| eNOS | nitric oxide synthase |
| RANTES | regulated on activation, normal T cell expressed, and secreted |
| ICAM-1 | intercellular adhesion molecule-1 |
| PECAM-1 | platelet-endothelial cell adhesion molecule-1 |
| VCAM-1 | vascular cell adhesion molecule-1 |
| RAGE | receptor of advanced glycation end products |
| COX-2 | cyclooxygenase-2 |
| 15PGDH | 15-hydroxyprostaglandin dehydrogenase |
| EDCFs | endothelium-derived contracting factors |
| COX-1 | cyclooxygenase-1 |
| STEMI | ST-elevation myocardial infarction |
| NSTEMI | non-ST-elevation myocardial infarction |
| CHF | congestive heart failure |
| iPTH | intact parathyroid hormone |
| AF | atrial fibrillation |
| CABG | coronary artery bypass surgery |
| POAF | postoperative atrial fibrillation |
| PVC | premature ventricular complex |
| PTH | parathyroid hormone |
| DBP | vitamin D binding-protein |
| PBMC | peripheral blood mononuclear cell |
References
- Majewska, M.; Szczepanik, M. The role of toll-like receptors (TLR) in innate and adaptive immune responses and their function in immune response regulation. Postep. Hig. Med. Doswiadczalnej 2006, 60, 52–63. [Google Scholar] [PubMed]
- Schnare, M.; Rollinghoff, M.; Qureshi, S. Toll-like receptors: Sentinels of host defence against bacterial infection. Int. Arch. Allergy Immunol. 2006, 139, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Kawai, T.; Akira, S. Toll-like receptors and innate immunity. Biochem. Biophys. Res. Commun. 2009, 388, 621–625. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.L. The emerging role of innate immunity in the heart and vascular system: For whom the cell tolls. Circ. Res. 2011, 108, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Akira, S.; Takeda, K.; Kaisho, T. Toll-like receptors: Critical proteins linking innate and acquired immunity. Nat. Immunol. 2001, 2, 675–680. [Google Scholar] [CrossRef] [PubMed]
- West, A.P.; Koblansky, A.A.; Ghosh, S. Recognition and signaling by toll-like receptors. Annu. Rev. Cell Dev. Biol. 2006, 22, 409–437. [Google Scholar] [CrossRef] [PubMed]
- Cook, D.N.; Pisetsky, D.S.; Schwartz, D.A. Toll-like receptors in the pathogenesis of human disease. Nat. Immunol. 2004, 5, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, T.; Kawai, T. Toll-like receptor signaling pathways. Front. Immunol. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Kang, R.; Coyne, C.B.; Zeh, H.J.; Lotze, M.T. PAMPs and DAMPs: Signal 0 s that spur autophagy and immunity. Immunol. Rev. 2012, 249, 158–175. [Google Scholar] [CrossRef] [PubMed]
- Gazzinelli, R.T.; Denkers, E.Y. Protozoan encounters with toll-like receptor signalling pathways: Implications for host parasitism. Nat. Rev. Immunol. 2006, 6, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Goulopoulou, S.; McCarthy, C.G.; Webb, R.C. Toll-like receptors in the vascular system: Sensing the dangers within. Pharmacol. Rev. 2015, 68, 142–167. [Google Scholar] [CrossRef] [PubMed]
- Jezierska, A.; Kolosova, I.A.; Verin, A.D. Toll like receptors signaling pathways as a target for therapeutic interventions. Curr. Signal Transduct. Ther. 2011, 6, 428–440. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, L.A.J.; Bryant, C.E.; Doyle, S.L. Therapeutic targeting of toll-like receptors for infectious and inflammatory diseases and cancer. Pharmacol. Rev. 2009, 61, 177–197. [Google Scholar] [CrossRef] [PubMed]
- Frantz, S.; Ertl, G.; Bauersachs, J. Mechanisms of disease: Toll-like receptors in cardiovascular disease. Nat. Clin. Pract. Cardiovasc. Med. 2007, 4, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, J.G. Role of toll-like receptors in cardiovascular diseases. Clin. Sci. 2011, 121, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Salvador, B.; Arranz, A.; Francisco, S.; Córdoba, L.; Punzón, C.; Llamas, M.Á.; Fresno, M. Modulation of endothelial function by toll like receptors. Pharmacol. Res. 2016, 108, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, M.; Naito, S. Tissue-specific mRNA expression profiles of human toll-like receptors and related genes. Biol. Pharm. Bull. 2005, 28, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Dekleijn, D.; Pasterkamp, G. Toll-like receptors in cardiovascular diseases. Cardiovasc. Res. 2003, 60, 58–67. [Google Scholar] [CrossRef]
- Lin, E.; Freedman, J.E.; Beaulieu, L.M. Innate immunity and toll-like receptor antagonists: A potential role in the treatment of cardiovascular diseases. Cardiovasc. Ther. 2009, 27, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Spirig, R.; Tsui, J.; Shaw, S. The emerging role of TLR and innate immunity in cardiovascular disease. Cardiol. Res. Pract. 2012, 2012, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; Ahmadi, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Libby, P.; Okamoto, Y.; Rocha, V.Z.; Folco, E. Inflammation in atherosclerosis: Transition from theory to practice. Circ. J. Off. J. Jpn. Circ. Soc. 2010, 74, 213–220. [Google Scholar] [CrossRef]
- Edfeldt, K.; Swedenborg, J.; Hansson, G.K.; Yan, Z. Expression of toll-like receptors in human atherosclerotic lesions: A possible pathway for plaque activation. Circulation 2002, 105, 1158–1161. [Google Scholar] [PubMed]
- Holloway, J.W.; Yang, I.A.; Ye, S. Variation in the toll-like receptor 4 gene and susceptibility to myocardial infarction. Pharmacogenet. Genom. 2005, 15, 15–21. [Google Scholar] [CrossRef]
- Doherty, T.M.; Fisher, E.A.; Arditi, M. TLR signaling and trapped vascular dendritic cells in the development of atherosclerosis. Trends Immunol. 2006, 27, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Kakkar, V.; Lu, X. Essential roles of toll-like receptors in atherosclerosis. Curr. Med. Chem. 2016, 23, 431–454. [Google Scholar] [CrossRef] [PubMed]
- Higashimori, M.; Tatro, J.B.; Moore, K.J.; Mendelsohn, M.E.; Galper, J.B.; Beasley, D. Role of toll-like receptor 4 in intimal foam cell accumulation in apolipoprotein E-deficient mice. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Quillard, T.; Araújo, H.A.; Franck, G.; Shvartz, E.; Sukhova, G.; Libby, P. TLR2 and neutrophils potentiate endothelial stress, apoptosis and detachment: Implications for superficial erosion. Eur. Heart J. 2015, 36, 1394–1404. [Google Scholar] [CrossRef] [PubMed]
- Crea, F.; Libby, P. Acute coronary syndromes: The way forward from mechanisms to precision treatment. Circulation 2017, 136, 1155–1166. [Google Scholar] [CrossRef] [PubMed]
- Falck-Hansen, M.; Kassiteridi, C.; Monaco, C. Toll-like receptors in atherosclerosis. Int. J. Mol. Sci. 2013, 14, 14008–14823. [Google Scholar] [CrossRef] [PubMed]
- Björkbacka, H.; Kunjathoor, V.V.; Moore, K.J.; Koehn, S.; Ordija, C.M.; Lee, M.A.; Means, T.; Halmen, K.; Luster, A.D.; Golenbock, D.T.; et al. Reduced atherosclerosis in MyD88-null mice links elevated serum cholesterol levels to activation of innate immunity signaling pathways. Nat. Med. 2004, 10, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Michelsen, K.S.; Wong, M.H.; Shah, P.K.; Zhang, W.; Yano, J.; Doherty, T.M.; Akira, S.; Rajavashisth, T.B.; Arditi, M. Lack of toll-like receptor 4 or myeloid differentiation factor 88 reduces atherosclerosis and alters plaque phenotype in mice deficient in apolipoprotein E. Proc. Natl. Acad. Sci. USA 2004, 101, 10679–10684. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, M.; Thorp, E.; Hansson, G.K.; Tabas, I. Treg-mediated suppression of atherosclerosis requires MYD88 signaling in DCs. J. Clin. Investig. 2013, 123, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Kalekar, L.A.; Schmiel, S.E.; Nandiwada, S.L.; Lam, W.Y.; Barsness, L.O.; Zhang, N.; Stritesky, G.L.; Malhotra, D.; Pauken, K.E.; Linehan, J.L.; et al. CD4+ T cell anergy prevents autoimmunity and generates regulatory T cell precursors. Nat. Immunol. 2016, 17, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Schenten, D.; Nish, S.A.; Yu, S.; Yan, X.; Lee, H.K.; Brodsky, I.; Pasman, L.; Yordy, B.; Wunderlich, F.T.; Brüning, J.C.; et al. Signaling through the adaptor molecule MyD88 in CD4+ T cells is required to overcome suppression by regulatory T cells. Immunity 2014, 40, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Pastrana, J.L. Regulatory T cells and atherosclerosis. J. Clin. Exp. Cardiol. 2013. [Google Scholar] [CrossRef] [PubMed]
- Cole, J.E.; Navin, T.J.; Cross, A.J.; Goddard, M.E.; Alexopoulou, L.; Mitra, A.T.; Davies, A.H.; Flavell, R.A.; Feldmann, M.; Monaco, C. Unexpected protective role for Toll-like receptor 3 in the arterial wall. Proc. Natl. Acad. Sci. USA 2011, 108, 2372–2377. [Google Scholar] [CrossRef] [PubMed]
- Baiersdörfer, M.; Schwarz, M.; Seehafer, K.; Lehmann, C.; Heit, A.; Wagner, H.; Kirschning, C.J.; Koch-Brandt, C. Toll-like receptor 3 mediates expression of clusterin/apolipoprotein J in vascular smooth muscle cells stimulated with RNA released from necrotic cells. Exp. Cell Res. 2010, 316, 3489–3500. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Inflammation in atherosclerosis. J. Am. Coll. Cardiol. 2009, 54, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Gurses, K.M.; Kocyigit, D.; Yalcin, M.U.; Canpinar, H.; Oto, M.A.; Ozer, N.; Tokgozoglu, L.; Guc, D.; Aytemir, K. Enhanced platelet toll-like receptor 2 and 4 expression in acute coronary syndrome and stable angina pectoris. Am. J. Cardiol. 2015, 116, 1666–1671. [Google Scholar] [CrossRef] [PubMed]
- Satoh, S.; Yada, R.; Inoue, H.; Omura, S.; Ejima, E.; Mori, T.; Takenaka, K.; Kawamura, N.; Numaguchi, K.; Mori, E.; et al. Toll-like receptor-4 is upregulated in plaque debris of patients with acute coronary syndrome more than toll-like receptor-2. Heart Vessels 2016, 31, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Arslan, F.; Smeets, M.B.; O’Neill, L.A.J.; Keogh, B.; McGuirk, P.; Timmers, L.; Tersteeg, C.; Hoefer, I.E.; Doevendans, P.A.; Pasterkamp, G.; et al. Myocardial ischemia/reperfusion injury is mediated by Leukocytic toll-like receptor-2 and reduced by systemic administration of a novel anti-toll-like receptor-2 antibody. Circulation 2010, 121, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Shimamoto, A.; Chong, A.J.; Yada, M.; Shomura, S.; Takayama, H.; Fleisig, A.J.; Agnew, M.L.; Hampton, C.R.; Rothnie, C.L.; Spring, D.J.; et al. Inhibition of toll-like receptor 4 with eritoran attenuates myocardial ischemia-reperfusion injury. Circulation 2006, 114, I270–I274. [Google Scholar] [CrossRef] [PubMed]
- Oyama, J.-I. Reduced myocardial ischemia-reperfusion injury in toll-like receptor 4-deficient mice. Circulation 2004, 109, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.; Feng, Y.; Zhang, M.; Zou, L.; Li, Y.; Buys, E.S.; Huang, P.; Brouckaert, P.; Chao, W. Toll-like receptor 4 signaling confers cardiac protection against ischemic injury via inducible nitric oxide synthase- and soluble guanylate cyclase-dependent mechanisms. Anesthesiology 2011, 114, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Shichita, T.; Ito, M.; Yoshimura, A. Post-ischemic inflammation regulates neural damage and protection. Front. Cell. Neurosci. 2014, 8. [Google Scholar] [CrossRef] [PubMed]
- Downes, C.E.; Crack, P.J. Neural injury following stroke: Are toll-like receptors the link between the immune system and the CNS? Neural injury and the immune system. Br. J. Pharmacol. 2010, 160, 1872–1888. [Google Scholar] [CrossRef] [PubMed]
- Fadakar, K.; Dadkhahfar, S.; Esmaeili, A.; Rezaei, N. The role of toll-like receptors (TLRs) in stroke. Rev. Neurosci. 2014, 25. [Google Scholar] [CrossRef] [PubMed]
- Qiao, H.; Zhang, X.; Zhu, C.; Dong, L.; Wang, L.; Zhang, X.; Xing, Y.; Wang, C.; Ji, Y.; Cao, X. Luteolin downregulates TLR4, TLR5, NF-κB and p-p38MAPK expression, upregulates the p-ERK expression, and protects rat brains against focal ischemia. Brain Res. 2012, 1448, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ha, T.; Lu, C.; Lam, F.; Liu, L.; Schweitzer, J.; Kalbfleisch, J.; Kao, R.L.; Williams, D.L.; Li, C. Poly (I:C) therapy decreases cerebral ischaemia/reperfusion injury via TLR3-mediated prevention of Fas/FADD interaction. J. Cell. Mol. Med. 2015, 19, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Brea, D.; Sobrino, T.; Rodríguez-Yáñez, M.; Ramos-Cabrer, P.; Agulla, J.; Rodríguez-González, R.; Campos, F.; Blanco, M.; Castillo, J. Toll-like receptors 7 and 8 expression is associated with poor outcome and greater inflammatory response in acute ischemic stroke. Clin. Immunol. 2011, 139, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Fu, B.; Zhang, X.; Chen, L.; Zhang, L.; Zhao, X.; Bai, X.; Zhu, C.; Cui, L.; Wang, L. Neuroprotective effect of bicyclol in rat ischemic stroke: Down-regulates TLR4, TLR9, TRAF6, NF-κB, MMP-9 and up-regulates claudin-5 expression. Brain Res. 2013, 1528, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Zhou, Y.; Pan, J.; Li, X.; Wang, H.; Wang, Y. Temporal pattern of toll-like receptor 9 upregulation in neurons and glial cells following cerebral ischemia reperfusion in mice. Int. J. Neurosci. 2016, 126, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.L.; Ciesielski, T.M.; Marsh, B.J.; Yang, T.; Homen, D.S.; Boule, J.-L.; Lessov, N.S.; Simon, R.P.; Stenzel-Poore, M.P. Toll-Like receptor 9: A new target of ischemic preconditioning in the brain. J. Cereb. Blood Flow Metab. 2008, 28, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.-C.; Arumugam, T.V.; Xu, X.; Cheng, A.; Mughal, M.R.; Jo, D.G.; Lathia, J.D.; Siler, D.A.; Chigurupati, S.; Ouyang, X.; et al. Pivotal role for neuronal toll-like receptors in ischemic brain injury and functional deficits. Proc. Natl. Acad. Sci. USA 2007, 104, 13798–13803. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Yang, Q.; Lv, F.; Cui, J.; Fu, H.; Wang, J. Reduced cerebral ischemia-reperfusion injury in toll-like receptor 4 deficient mice. Biochem. Biophys. Res. Commun. 2007, 353, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Hua, F.; Ma, J.; Ha, T.; Kelley, J.; Williams, D.L.; Kao, R.L.; Kalbfleisch, J.H.; Browder, I.W.; Li, C. Preconditioning with a TLR2 specific ligand increases resistance to cerebral ischemia/reperfusion injury. J. Neuroimmunol. 2008, 199, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Liu, L.; Chen, Y.; Ha, T.; Kelley, J.; Schweitzer, J.; Kalbfleisch, J.H.; Kao, R.L.; Williams, D.L.; Li, C. TLR2 ligand induces protection against cerebral ischemia/reperfusion injury via activation of phosphoinositide 3-Kinase/Akt signaling. J. Immunol. 2011, 187, 1458–1466. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the global burden of disease study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Pradillo, J.M.; Fernández-López, D.; García-Yébenes, I.; Sobrado, M.; Hurtado, O.; Moro, M.A.; Lizasoain, I. Toll-like receptor 4 is involved in neuroprotection afforded by ischemic preconditioning. J. Neurochem. 2009, 109, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Moraga, A.; Pradillo, J.M.; Cuartero, M.I.; Hernandez-Jimenez, M.; Oses, M.; Moro, M.A.; Lizasoain, I. Toll-like receptor 4 modulates cell migration and cortical neurogenesis after focal cerebral ischemia. FASEB J. 2014, 28, 4710–4718. [Google Scholar] [CrossRef] [PubMed]
- D’Atri, L.P.; Schattner, M. Platelet toll-like receptors in thromboinflammation. Front. Biosci. Landmark Ed. 2017, 22, 1867–1883. [Google Scholar] [PubMed]
- Blair, P.; Rex, S.; Vitseva, O.; Beaulieu, L.; Tanriverdi, K.; Chakrabarti, S.; Hayashi, C.; Genco, C.A.; Iafrati, M.; Freedman, J.E. Stimulation of toll-like receptor 2 in human platelets induces a thromboinflammatory response through activation of phosphoinositide 3-kinase. Circ. Res. 2009, 104, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Birks, E.J.; Felkin, L.E.; Banner, N.R.; Khaghani, A.; Barton, P.J.R.; Yacoub, M.H. Increased toll-like receptor 4 in the myocardium of patients requiring left ventricular assist devices. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2004, 23, 228–235. [Google Scholar] [CrossRef]
- Frantz, S.; Kobzik, L.; Kim, Y.D.; Fukazawa, R.; Medzhitov, R.; Lee, R.T.; Kelly, R.A. Toll4 (TLR4) expression in cardiac myocytes in normal and failing myocardium. J. Clin. Investig. 1999, 104, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Boyd, J.H.; Mathur, S.; Wang, Y.; Bateman, R.M.; Walley, K.R. Toll-like receptor stimulation in cardiomyoctes decreases contractility and initiates an NF-κB dependent inflammatory response. Cardiovasc. Res. 2006, 72, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Knuefermann, P.; Schwederski, M.; Velten, M.; Krings, P.; Ehrentraut, H.; Rudiger, M.; Boehm, O.; Fink, K.; Dreiner, U.; Grohe, C.; et al. Bacterial DNA induces myocardial inflammation and reduces cardiomyocyte contractility: Role of toll-like receptor 9. Cardiovasc. Res. 2008, 78, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Timmers, L.; Sluijter, J.P.G.; van Keulen, J.K.; Hoefer, I.E.; Nederhoff, M.G.J.; Goumans, M.-J.; Doevendans, P.A.; van Echteld, C.J.A.; Joles, J.A.; Quax, P.H.; et al. Toll-like receptor 4 mediates maladaptive left ventricular remodeling and impairs cardiac function after myocardial infarction. Circ. Res. 2008, 102, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Babu, A.N.; Meng, X.; Zou, N.; Yang, X.; Wang, M.; Song, Y.; Cleveland, J.C.; Weyant, M.; Banerjee, A.; Fullerton, D.A. Lipopolysaccharide stimulation of human aortic valve interstitial cells activates inflammation and osteogenesis. Ann. Thorac. Surg. 2008, 86, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; Ao, L.; Song, Y.; Babu, A.; Yang, X.; Wang, M.; Weyant, M.J.; Dinarello, C.A.; Cleveland, J.C.; Fullerton, D.A. Expression of functional toll-like receptors 2 and 4 in human aortic valve interstitial cells: Potential roles in aortic valve inflammation and stenosis. Am. J. Physiol. Cell Physiol. 2008, 294, C29–C35. [Google Scholar] [CrossRef] [PubMed]
- Toli, K.; Paraskevas, K.I.; Poulakou, M.V.; Agrogiannis, G.; Kavantzas, N.; Xanthopoulos, V.; Iliopoulos, D.G.; Mantas, I.; Papachristodoulou, A.; Patsouris, E.; et al. Association between plasma levels and immunolocalization of cytokines in heart valve lesions: A possible target for treatment? Expert Opin. Ther. Targets 2008, 12, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Monnerat-Cahli, G.; Alonso, H.; Gallego, M.; Alarcón, M.L.; Bassani, R.A.; Casis, O.; Medei, E. Toll-like receptor 4 activation promotes cardiac arrhythmias by decreasing the transient outward potassium current (Ito) through an IRF3-dependent and MyD88-independent pathway. J. Mol. Cell. Cardiol. 2014, 76, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Mersmann, J.; Koch, A.; Tran, N.; Zimmermann, R.; Granja, T.F.; Larmann, J.; Herzog, C.; Theilmeier, G.; Bornstein, S.R.; Kirschning, C.J.; et al. Toll-like receptor 2 signaling triggers fatal arrhythmias upon myocardial ischemia-reperfusion. Crit. Care Med. 2010, 38, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.G.; Goulopoulou, S.; Wenceslau, C.F.; Spitler, K.; Matsumoto, T.; Webb, R.C. Toll-like receptors and damage-associated molecular patterns: Novel links between inflammation and hypertension. AJP Heart Circ. Physiol. 2014, 306, H184–H196. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.V.; Abboud, F.M. Toll-like receptors and hypertension. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R501–R504. [Google Scholar] [CrossRef] [PubMed]
- Bomfim, G.F.; Echem, C.; Martins, C.B.; Costa, T.J.; Sartoretto, S.M.; Dos Santos, R.A.; Oliveira, M.A.; Akamine, E.H.; Fortes, Z.B.; Tostes, R.C.; et al. Toll-like receptor 4 inhibition reduces vascular inflammation in spontaneously hypertensive rats. Life Sci. 2015, 122, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Hernanz, R.; Martínez-Revelles, S.; Palacios, R.; Martín, A.; Cachofeiro, V.; Aguado, A.; García-Redondo, L.; Barrús, M.T.; de Batista, P.R.; Briones, A.M.; et al. Toll-like receptor 4 contributes to vascular remodelling and endothelial dysfunction in angiotensin II-induced hypertension: TLR4 and vascular damage in hypertension. Br. J. Pharmacol. 2015, 172, 3159–3176. [Google Scholar] [CrossRef] [PubMed]
- Erridge, C. Endogenous ligands of TLR2 and TLR4: Agonists or assistants? J. Leukoc. Biol. 2010, 87, 989–999. [Google Scholar] [CrossRef] [PubMed]
- Harwani, S.C.; Chapleau, M.W.; Legge, K.L.; Ballas, Z.K.; Abboud, F.M. Neurohormonal modulation of the innate immune system is proinflammatory in the prehypertensive spontaneously hypertensive rat, a genetic model of essential hypertension. Circ. Res. 2012, 111, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Dange, R.B.; Agarwal, D.; Masson, G.S.; Vila, J.; Wilson, B.; Nair, A.; Francis, J. Central blockade of TLR4 improves cardiac function and attenuates myocardial inflammation in angiotensin II-induced hypertension. Cardiovasc. Res. 2014, 103, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Dange, R.B.; Agarwal, D.; Teruyama, R.; Francis, J. Toll-like receptor 4 inhibition within the paraventricular nucleus attenuates blood pressure and inflammatory response in a genetic model of hypertension. J. Neuroinflamm. 2015, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Vijay-Kumar, M.; Aitken, J.D.; Carvalho, F.A.; Cullender, T.C.; Mwangi, S.; Srinivasan, S.; Sitaraman, S.V.; Knight, R.; Ley, R.E.; Gewirtz, A.T. Metabolic syndrome and altered gut microbiota in mice lacking toll-like receptor 5. Science 2010, 328, 228–231. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, C.G.; Wenceslau, C.F.; Goulopoulou, S.; Ogbi, S.; Baban, B.; Sullivan, J.C.; Matsumoto, T.; Webb, R.C. Circulating mitochondrial DNA and toll-like receptor 9 are associated with vascular dysfunction in spontaneously hypertensive rats. Cardiovasc. Res. 2015, 107, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.L.; Silva, L.E.V.; Hott, S.C.; Bomfim, G.F.; da Silva, C.A.A.; Fazan, R.; Resstel, L.B.M.; Tostes, R.C.; Carneiro, F.S. Toll-like receptor 9 plays a key role in the autonomic cardiac and baroreflex control of arterial pressure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 308, R714–R723. [Google Scholar] [CrossRef] [PubMed]
- Nemoto, S.; Vallejo, J.G.; Knuefermann, P.; Misra, A.; Defreitas, G.; Carabello, B.A.; Mann, D.L. Escherichia coli LPS-induced LV dysfunction: Role of toll-like receptor-4 in the adult heart. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, H2316–H2323. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.A.; Haudek, S.B.; Koroglu, T.; Tsen, M.F.; Bryant, D.D.; White, D.J.; Kusewitt, D.F.; Horton, J.W.; Giroir, B.P. IRAK1 deletion disrupts cardiac Toll/IL-1 signaling and protects against contractile dysfunction. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H597–H606. [Google Scholar] [CrossRef] [PubMed]
- Baumgarten, G.; Knuefermann, P.; Schuhmacher, G.; Vervölgyi, V.; von Rappard, J.; Dreiner, U.; Fink, K.; Djoufack, C.; Hoeft, A.; Grohé, C.; et al. Toll-like receptor 4, nitric oxide, and myocardial depression in endotoxemia. Shock Augusta Ga 2006, 25, 43–49. [Google Scholar] [CrossRef]
- Knuefermann, P.; Sakata, Y.; Baker, J.S.; Huang, C.-H.; Sekiguchi, K.; Hardarson, H.S.; Takeuchi, O.; Akira, S.; Vallejo, J.G. Toll-like receptor 2 mediates Staphylococcus aureus-induced myocardial dysfunction and cytokine production in the heart. Circulation 2004, 110, 3693–3698. [Google Scholar] [CrossRef] [PubMed]
- Hardarson, H.S.; Baker, J.S.; Yang, Z.; Purevjav, E.; Huang, C.-H.; Alexopoulou, L.; Li, N.; Flavell, R.A.; Bowles, N.E.; Vallejo, J.G. Toll-like receptor 3 is an essential component of the innate stress response in virus-induced cardiac injury. Am. J. Physiol. Heart Circ. Physiol. 2007, 292, H251–H258. [Google Scholar] [CrossRef] [PubMed]
- Negishi, H.; Osawa, T.; Ogami, K.; Ouyang, X.; Sakaguchi, S.; Koshiba, R.; Yanai, H.; Seko, Y.; Shitara, H.; Bishop, K.; et al. A critical link between toll-like receptor 3 and type II interferon signaling pathways in antiviral innate immunity. Proc. Natl. Acad. Sci. USA 2008, 105, 20446–20451. [Google Scholar] [CrossRef] [PubMed]
- Pagni, P.P.; Traub, S.; Demaria, O.; Chasson, L.; Alexopoulou, L. Contribution of TLR7 and TLR9 signaling to the susceptibility of MyD88-deficient mice to myocarditis. Autoimmunity 2010, 43, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Fuse, K.; Chan, G.; Liu, Y.; Gudgeon, P.; Husain, M.; Chen, M.; Yeh, W.-C.; Akira, S.; Liu, P.P. Myeloid differentiation factor-88 plays a crucial role in the pathogenesis of Coxsackievirus B3-induced myocarditis and influences type I interferon production. Circulation 2005, 112, 2276–2285. [Google Scholar] [CrossRef] [PubMed]
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [Google Scholar] [PubMed]
- Dusso, A.S.; Brown, A.J.; Slatopolsky, E. Vitamin D. Am. J. Physiol. Renal Physiol. 2005, 289, F8–F28. [Google Scholar] [CrossRef] [PubMed]
- Lowe, K.E.; Maiyar, A.C.; Norman, A.W. Vitamin D-mediated gene expression. Crit. Rev. Eukaryot. Gene Expr. 1992, 2, 65–109. [Google Scholar] [PubMed]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and human health: Lessons from vitamin D receptor null mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Veugelers, P.J.; Pham, T.-M.; Ekwaru, J.P. Optimal vitamin D supplementation doses that minimize the risk for both low and high serum 25-hydroxyvitamin D concentrations in the general population. Nutrients 2015, 7, 10189–10208. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B.; Heaney, R.P.; Holick, M.F.; Lips, P.; Meunier, P.J.; Vieth, R. Estimates of optimal vitamin D status. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2005, 16, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.A.; Cooper, C.; Ebeling, P.R.; Eggersdorfer, M.; Hilger, J.; Hoffmann, K.; Josse, R.; Kanis, J.A.; Mithal, A.; Pierroz, D.D.; et al. A global representation of vitamin D status in healthy populations. Arch. Osteoporos. 2012, 7, 155–172. [Google Scholar] [CrossRef] [PubMed]
- Forrest, K.Y.Z.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D: Extraskeletal Health. Rheum. Dis. Clin. N. Am. 2012, 38, 141–160. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M. Vitamin D—Effects on skeletal and extraskeletal health and the need for supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D. A review of vitamin D status and CVD. Proc. Nutr. Soc. 2014, 73, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Giovannucci, E. 25-Hydroxyvitamin D and Risk of Myocardial Infarction in MenA Prospective Study. Arch. Intern. Med. 2008, 168, 1174. [Google Scholar] [CrossRef] [PubMed]
- Kendrick, J.; Targher, G.; Smits, G.; Chonchol, M. 25-Hydroxyvitamin D deficiency is independently associated with cardiovascular disease in the third national health and nutrition examination survey. Atherosclerosis 2009, 205, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Pichiri, I.; Lippi, G. Vitamin D, thrombosis, and hemostasis: More than skin deep. Semin. Thromb. Hemost. 2012, 38, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Mousa, A.; Naderpoor, N.; de Courten, M.P.J.; Scragg, R.; de Courten, B. 25-hydroxyvitamin D is associated with adiposity and cardiometabolic risk factors in a predominantly vitamin D-deficient and overweight/obese but otherwise healthy cohort. J. Steroid Biochem. Mol. Biol. 2017, 173, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Meehan, M.; Penckofer, S. The role of vitamin D in the aging adult. J. Aging Gerontol. 2014, 2, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Gouni-Berthold, I.; Krone, W.; Berthold, H.K. Vitamin D and cardiovascular disease. Curr. Vasc. Pharmacol. 2009, 7, 414–422. [Google Scholar] [CrossRef] [PubMed]
- Rejnmark, L.; Bislev, L.S.; Cashman, K.D.; Eiríksdottir, G.; Gaksch, M.; Grübler, M.; Grimnes, G.; Gudnason, V.; Lips, P.; Pilz, S.; et al. Non-skeletal health effects of vitamin D supplementation: A systematic review on findings from meta-analyses summarizing trial data. PLoS ONE 2017, 12, e0180512. [Google Scholar] [CrossRef] [PubMed]
- Sokol, S.I.; Tsang, P.; Aggarwal, V.; Melamed, M.L.; Srinivas, V.S. Vitamin D status and risk of cardiovascular events: Lessons learned via systematic review and meta-analysis. Cardiol. Rev. 2011, 19, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Brewer, L.C.; Michos, E.D.; Reis, J.P. Vitamin D in atherosclerosis, vascular disease, and endothelial function. Curr. Drug Targets 2011, 12, 54–60. [Google Scholar] [CrossRef] [PubMed]
- García-Canton, C.; Bosch, E.; Ramírez, A.; Gonzalez, Y.; Auyanet, I.; Guerra, R.; Perez, M.A.; Fernández, E.; Toledo, A.; Lago, M.; et al. Vascular calcification and 25-hydroxyvitamin D levels in non-dialysis patients with chronic kidney disease stages 4 and 5. Nephrol. Dial. Transplant. Off. Publ. Eur. Dial. Transpl. Assoc. Eur. Ren. Assoc. 2011, 26, 2250–2256. [Google Scholar] [CrossRef] [PubMed]
- Kassi, E.; Adamopoulos, C.; Basdra, E.K.; Papavassiliou, A.G. Role of Vitamin D in Atherosclerosis. Circulation 2013, 128, 2517–2531. [Google Scholar] [CrossRef] [PubMed]
- Merke, J.; Milde, P.; Lewicka, S.; Hügel, U.; Klaus, G.; Mangelsdorf, D.J.; Haussler, M.R.; Rauterberg, E.W.; Ritz, E. Identification and regulation of 1,25-dihydroxyvitamin D3 receptor activity and biosynthesis of 1,25-dihydroxyvitamin D3. Studies in cultured bovine aortic endothelial cells and human dermal capillaries. J. Clin. Investig. 1989, 83, 1903–1915. [Google Scholar] [CrossRef] [PubMed]
- Zehnder, D.; Bland, R.; Chana, R.S.; Wheeler, D.C.; Howie, A.J.; Williams, M.C.; Stewart, P.M.; Hewison, M. Synthesis of 1,25-dihydroxyvitamin D3 by human endothelial cells is regulated by inflammatory cytokines: A novel autocrine determinant of vascular cell adhesion. J. Am. Soc. Nephrol. JASN 2002, 13, 621–629. [Google Scholar] [PubMed]
- Molinari, C.; Uberti, F.; Grossini, E.; Vacca, G.; Carda, S.; Invernizzi, M.; Cisari, C. 1α,25-dihydroxycholecalciferol induces nitric oxide production in cultured endothelial cells. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2011, 27, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Queen, L.R.; Ji, Y.; Xu, B.; Young, L.; Yao, K.; Wyatt, A.W.; Rowlands, D.J.; Siow, R.C.M.; Mann, G.E.; Ferro, A. Mechanisms underlying β2-adrenoceptor-mediated nitric oxide generation by human umbilical vein endothelial cells: Endothelial β-adrenoceptors and nitric oxide. J. Physiol. 2006, 576, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Hirata, M.; Serizawa, K.; Aizawa, K.; Yogo, K.; Tashiro, Y.; Takeda, S.; Moriguchi, Y.; Endo, K.; Fukagawa, M. 22-Oxacalcitriol prevents progression of endothelial dysfunction through antioxidative effects in rats with type 2 diabetes and early-stage nephropathy. Nephrol. Dial. Transplant. 2013, 28, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Andrukhova, O.; Slavic, S.; Zeitz, U.; Riesen, S.C.; Heppelmann, M.S.; Ambrisko, T.D.; Markovic, M.; Kuebler, W.M.; Erben, R.G. Vitamin D is a regulator of endothelial nitric oxide synthase and arterial stiffness in mice. Mol. Endocrinol. 2014, 28, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Equils, O.; Naiki, Y.; Shapiro, A.M.; Michelsen, K.; Lu, D.; Adams, J.; Jordan, S. 1,25-Dihydroxyvitamin D inhibits lipopolysaccharide-induced immune activation in human endothelial cells. Clin. Exp. Immunol. 2006, 143, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Martinesi, M.; Bruni, S.; Stio, M.; Treves, C. 1,25-Dihydroxyvitamin D3 inhibits tumor necrosis factor-alpha-induced adhesion molecule expression in endothelial cells. Cell Biol. Int. 2006, 30, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Collins, T.; Read, M.A.; Neish, A.S.; Whitley, M.Z.; Thanos, D.; Maniatis, T. Transcriptional regulation of endothelial cell adhesion molecules: NF-κ B and cytokine-inducible enhancers. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 1995, 9, 899–909. [Google Scholar]
- Talmor, Y.; Bernheim, J.; Klein, O.; Green, J.; Rashid, G. Calcitriol blunts pro-atherosclerotic parameters through NF-κB and p38 in vitro. Eur. J. Clin. Investig. 2008, 38, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Stach, K.; Kälsch, A.-I.; Nguyen, X.D.; Elmas, E.; Kralev, S.; Lang, S.; Weiss, C.; Borggrefe, M.; Kälsch, T. 1α,25-Dihydroxyvitamin D3 Attenuates Platelet Activation and the Expression of VCAM-1 and MT1-MMP in Human Endothelial Cells. Cardiology 2011, 118, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.V.; Feldman, D. Molecular pathways mediating the anti-inflammatory effects of calcitriol: Implications for prostate cancer chemoprevention and treatment. Endocr. Relat. Cancer 2010, 17, R19–R38. [Google Scholar] [CrossRef] [PubMed]
- Chenevard, R. Selective COX-2 inhibition improves endothelial function in coronary artery disease. Circulation 2003, 107, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Feletou, M.; Taddei, S. Endothelium-dependent contractions in hypertension. Br. J. Pharmacol. 2005, 144, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.S.K.; Man, R.Y.K.; Vanhoutte, P.M. Calcium-independent phospholipase A2 plays a key role in the endothelium-dependent contractions to acetylcholine in the aorta of the spontaneously hypertensive rat. AJP Heart Circ. Physiol. 2010, 298, H1260–H1266. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.S.K.; Delansorne, R.; Man, R.Y.K.; Vanhoutte, P.M. Vitamin D derivatives acutely reduce endothelium-dependent contractions in the aorta of the spontaneously hypertensive rat. AJP Heart Circ. Physiol. 2008, 295, H289–H296. [Google Scholar] [CrossRef] [PubMed]
- Takeda, M.; Yamashita, T.; Sasaki, N.; Nakajima, K.; Kita, T.; Shinohara, M.; Ishida, T.; Hirata, K. Oral administration of an active form of vitamin D3 (calcitriol) decreases atherosclerosis in mice by inducing regulatory T cells and immature dendritic cells with tolerogenic functions. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2495–2503. [Google Scholar] [CrossRef] [PubMed]
- Bobryshev, Y.V. Vitamin D3 suppresses immune reactions in atherosclerosis, affecting regulatory T cells and dendritic cell function. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2317–2319. [Google Scholar] [CrossRef] [PubMed]
- Mangge, H.; Weghuber, D.; Prassl, R.; Haara, A.; Schnedl, W.; Postolache, T.T.; Fuchs, D. The role of vitamin D in atherosclerosis inflammation revisited: More a bystander than a player? Curr. Vasc. Pharmacol. 2015, 13, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Nunes, J.P.L. Troponin I, but not BNP, is associated with phosphorus, calcium and vitamin D in stable coronary artery disease. Kidney Blood Press. Res. 2013, 37, 43–47. [Google Scholar] [CrossRef] [PubMed]
- De Metrio, M.; Milazzo, V.; Rubino, M.; Cabiati, A.; Moltrasio, M.; Marana, I.; Campodonico, J.; Cosentino, N.; Veglia, F.; Bonomi, A.; et al. Vitamin D plasma levels and in-hospital and 1-year outcomes in acute coronary syndromes: A prospective study. Medicine (Baltimore) 2015, 94, e857. [Google Scholar] [CrossRef] [PubMed]
- Naesgaard, P.A.; Pönitz, V.; Aarsetoey, H.; Brügger-Andersen, T.; Grundt, H.; Harris, W.S.; Staines, H.; Nilsen, D.W.T. Prognostic utility of vitamin D in acute coronary syndrome patients in coastal norway. Dis. Markers 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Saxena, P. To evaluate the role of plasma vitamin D level as a prognostic marker and its relation to in-hospital complications in patients with acute coronary syndrome. Int. J. Adv. Med. 2016, 976–981. [Google Scholar] [CrossRef]
- Gondim, F.; Caribé, A.; Vasconcelos, K.; Segundo, A.; Bandeira, F. Vitamin D deficiency is associated with severity of acute coronary syndrome in patients with type 2 diabetes and high rates of sun exposure. Clin. Med. Insights Endocrinol. Diabetes 2016, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Tomaschitz, A.; Drechsler, C.; Zittermann, A.; Dekker, J.M.; März, W. Vitamin D supplementation: A promising approach for the prevention and treatment of strokes. Curr. Drug Targets 2011, 12, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, S. Role of vitamin D in the outcome of ischemic stroke- A randomized controlled trial. J. Clin. Diagn. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, Y.; Khademvatani, K.; Seyyed-Mohammadzad, M.H.; Akbari, M.; Eskandari, R.; Rostamzadeh, A. The relationship between vitamin D status and idiopathic lower-extremity deep vein thrombosis. Int. J. Gen. Med. 2014, 7, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Entezari-Maleki, T.; Hajhossein Talasaz, A.; Salarifar, M.; Hadjibabaie, M.; Javadi, M.R.; Bozorgi, A.; Jenab, Y.; Boroumand, M.A.; Gholami, K. Plasma vitamin D status and its correlation with risk factors of thrombosis, P-selectin and HS-CRP level in patients with venous thromboembolism; the first study of iranian population. Iran. J. Pharm. Res. IJPR 2014, 13, 319–327. [Google Scholar] [PubMed]
- Brilla, C.G. The cardiac structure-function relationship and the renin-angiotensin-aldosterone system in hypertension and heart failure. Curr. Opin. Cardiol. 1994, 9 (Suppl. 1), S2–S10; discussion S10–S11. [Google Scholar] [CrossRef] [PubMed]
- Sigurdsson, A.; Swedberg, K. Neurohormonal activation and congestive heart failure: Today’s experience with ACE inhibitors and rationale for their use. Eur. Heart J. 1995, 16 (Suppl. N), 65–72. [Google Scholar] [CrossRef] [PubMed]
- Sackner-Bernstein, J.D.; Mancini, D.M. Rationale for treatment of patients with chronic heart failure with adrenergic blockade. JAMA 1995, 274, 1462–1467. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A.; Schleithoff, S.S.; Koerfer, R. Vitamin D insufficiency in congestive heart failure: Why and what to do about it? Heart Fail. Rev. 2006, 11, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Rizvi, A.A. Vitamin D deficiency in patients with congestive heart failure: Mechanisms, manifestations, and management. South. Med. J. 2011, 104, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Andersson, P.; Rydberg, E.; Willenheimer, R. Primary hyperparathyroidism and heart disease—A review. Eur. Heart J. 2004, 25, 1776–1787. [Google Scholar] [CrossRef] [PubMed]
- Meredith, A.; Boroomand, S.; Carthy, J.; Luo, Z.; McManus, B. 1,25 Dihydroxyvitamin D3 inhibits TGFβ1-mediated primary human cardiac myofibroblast activation. PLoS ONE 2015, 10, e0128655. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Singh, S.S.; Yu, H.; Lee, J.Y.; Cho, B.R.; Kang, P.M. Vitamin D signaling pathway plays an important role in the development of heart failure after myocardial infarction. J. Appl. Physiol. 2013, 114, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Mihos, C.G.; De La Cruz, J.A.; Hernandez, A.; Santana, O. Vitamin D Deficiency and supplementation in cardiovascular disorders. Cardiol. Rev. 2017, 25, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Schleithoff, S.S.; Zittermann, A.; Tenderich, G.; Berthold, H.K.; Stehle, P.; Koerfer, R. Vitamin D supplementation improves cytokine profiles in patients with congestive heart failure: A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2006, 83, 754–759. [Google Scholar] [PubMed]
- Camici, M.; Galetta, F.; Franzoni, F.; Carpi, A.; Zangeneh, F. Vitamin D and heart. Intern. Emerg. Med. 2013, 8 (Suppl. 1), S5–S9. [Google Scholar] [CrossRef] [PubMed]
- Ameri, P.; Canepa, M.; Milaneschi, Y.; Spallarossa, P.; Leoncini, G.; Giallauria, F.; Strait, J.B.; Lakatta, E.G.; Brunelli, C.; Murialdo, G.; et al. Relationship between vitamin D status and left ventricular geometry in a healthy population: Results from the baltimore longitudinal study of aging. J. Intern. Med. 2013, 273, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Czarny, M.J.; Resar, J.R. Diagnosis and management of valvular aortic stenosis. Clin. Med. Insights Cardiol. 2014, 8 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Manning, W.J. Asymptomatic aortic stenosis in the elderly: A clinical review. JAMA 2013, 310, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Lind, B.K.; Kitzman, D.W.; Gersh, B.J.; Siscovick, D.S. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N. Engl. J. Med. 1999, 341, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Hekimian, G.; Boutten, A.; Flamant, M.; Duval, X.; Dehoux, M.; Benessiano, J.; Huart, V.; Dupré, T.; Berjeb, N.; Tubach, F.; et al. Progression of aortic valve stenosis is associated with bone remodelling and secondary hyperparathyroidism in elderly patients—The COFRASA study. Eur. Heart J. 2013, 34, 1915–1922. [Google Scholar] [CrossRef] [PubMed]
- Linhartová, K.; Veselka, J.; Sterbáková, G.; Racek, J.; Topolcan, O.; Cerbák, R. Parathyroid hormone and vitamin D levels are independently associated with calcific aortic stenosis. Circ. J. Off. J. Jpn. Circ. Soc. 2008, 72, 245–250. [Google Scholar] [CrossRef]
- Eren, E.; Ellidag, H.Y.; Cekin, Y.; Ayoglu, R.U.; Sekercioglu, A.O.; Yılmaz, N. Heart valve disease: The role of calcidiol deficiency, elevated parathyroid hormone levels and oxidative stress in mitral and aortic valve insufficiency. Redox Rep. Commun. Free Radic. Res. 2014, 19, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Vitezova, A.; Cartolano, N.S.; Heeringa, J.; Zillikens, M.C.; Hofman, A.; Franco, O.H.; Kiefte-de Jong, J.C. Vitamin D and the risk of atrial fibrillation—The rotterdam study. PLoS ONE 2015, 10, e0125161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, A.; Misialek, J.R.; Michos, E.D.; Eckfeldt, J.; Selvin, E.; Soliman, E.Z.; Chen, L.Y.; Gross, M.D.; Lutsey, P.L. Serum 25-hydroxyvitamin D and the incidence of atrial fibrillation: The atherosclerosis risk in communities (ARIC) STUDY. Europace 2016, 18, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Yang, Y.; Ng, C.Y.; Wang, D.; Wang, J.; Li, G.; Liu, T. Meta-analysis of vitamin D deficiency and risk of atrial fibrillation: Vitamin D deficiency and risk of AF. Clin. Cardiol. 2016, 39, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Gode, S.; Aksu, T.; Demirel, A.; Sunbul, M.; Gul, M.; Bakır, I.; Yeniterzi, M. Effect of vitamin D deficiency on the development of postoperative atrial fibrillation in coronary artery bypass patients. J. Cardiovasc. Thorac. Res. 2016, 8, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Cerit, L.; Kemal, H.; Gulsen, K.; Ozcem, B.; Cerit, Z.; Duygu, H. Relationship between vitamin D and the development of atrial fibrillation after on-pump coronary artery bypass graft surgery. Cardiovasc. J. Afr. 2017, 28, 104–107. [Google Scholar] [CrossRef] [PubMed]
- Belen, E.; Aykan, A.C.; Kalaycioglu, E.; Sungur, M.A.; Sungur, A.; Cetin, M. Low-level vitamin D is associated with atrial fibrillation in patients with chronic heart failure. Adv. Clin. Exp. Med. 2016, 25, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Kiuchi, M.G.; Ramalho e Silva, G.; Paz, L.M.R.; Chen, S.; Hoye, N.A.; Souto, G.L.L. Influence of vitamin D levels on the treatment of premature ventricular complexes in patients with chronic kidney disease. IJC Metab. Endocr. 2017, 14, 53–58. [Google Scholar] [CrossRef]
- Pilz, S.; Tomaschitz, A. Role of vitamin D in arterial hypertension. Expert Rev. Cardiovasc. Ther. 2010, 8, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Resnick, L.M.; Müller, F.B.; Laragh, J.H. Calcium-regulating hormones in essential hypertension. Relation to plasma renin activity and sodium metabolism. Ann. Intern. Med. 1986, 105, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Carrara, D.; Bernini, M.; Bacca, A.; Rugani, I.; Duranti, E.; Virdis, A.; Ghiadoni, L.; Taddei, S.; Bernini, G. Cholecalciferol administration blunts the systemic renin-angiotensin system in essential hypertensives with hypovitaminosis D. J. Renin-Angiotensin-Aldosterone Syst. JRAAS 2014, 15, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, A.; Forman, J.P.; Williams, J.S. Vitamin D and the vascular sensitivity to angiotensin II in obese Caucasians with hypertension. J. Hum. Hypertens. 2011, 25, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Xiang, W.; Kong, J.; Chen, S.; Cao, L.-P.; Qiao, G.; Zheng, W.; Liu, W.; Li, X.; Gardner, D.G.; Li, Y.C. Cardiac hypertrophy in vitamin D receptor knockout mice: Role of the systemic and cardiac renin-angiotensin systems. Am. J. Physiol. Endocrinol. Metab. 2005, 288, E125–E132. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Hänni, A.; Lithell, H.; Hvarfner, A.; Sörensen, O.H.; Ljunghall, S. Vitamin D is related to blood pressure and other cardiovascular risk factors in middle-aged men. Am. J. Hypertens. 1995, 8, 894–901. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Apekey, T.A.; Steur, M. Vitamin D and risk of future hypertension: Meta-analysis of 283,537 participants. Eur. J. Epidemiol. 2013, 28, 205–221. [Google Scholar] [CrossRef] [PubMed]
- Scragg, R.; Sowers, M.; Bell, C. Serum 25-hydroxyvitamin D, ethnicity, and blood pressure in the third national health and nutrition examination survey. Am. J. Hypertens. 2007, 20, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Curhan, G.C.; Taylor, E.N. Plasma 25-hydroxyvitamin D levels and risk of incident hypertension among young women. Hypertension 2008, 52, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Margolis, K.L.; Ray, R.M.; van Horn, L.; Manson, J.E.; Allison, M.A.; Black, H.R.; Beresford, S.A.A.; Connelly, S.A.; Curb, J.D.; Grimm, R.H.; et al. Women’s health initiative investigators effect of calcium and vitamin D supplementation on blood pressure: The women’s health Initiative randomized Trial. Hypertension 2008, 52, 847–855. [Google Scholar] [CrossRef]
- Van Ballegooijen, A.J.; Kestenbaum, B.; Sachs, M.C.; de Boer, I.H.; Siscovick, D.S.; Hoofnagle, A.N.; Ix, J.H.; Visser, M.; Brouwer, I.A. Association of 25-hydroxyvitamin D and parathyroid hormone with incident hypertension. J. Am. Coll. Cardiol. 2014, 63, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Braun, A.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Liu, Y.; Giovannucci, E.; Christopher, K.B. Association of low serum 25-hydroxyvitamin D levels and mortality in the critically ill. Crit. Care Med. 2011, 39, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Christopher, K.B. Vitamin D supplementation in the ICU patient. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Watkins, H.; Ashrafian, H.; Redwood, C. Inherited cardiomyopathies. N. Engl. J. Med. 2011, 364, 1643–1656. [Google Scholar] [CrossRef] [PubMed]
- Fang, L.-H.; Fan, X.-C. Expression of Vitamin D receptor in the myocardium of mice with viral myocarditis. Zhongguo Dang Dai Er Ke Za Zhi/Chin. J. Contemp. Pediatr. 2015, 17, 1007–1012. [Google Scholar]
- Biragyn, A.; Ruffini, P.A.; Leifer, C.A.; Klyushnenkova, E.; Shakhov, A.; Chertov, O.; Shirakawa, A.K.; Farber, J.M.; Segal, D.M.; Oppenheim, J.J.; et al. Toll-like receptor 4-dependent activation of dendritic cells by β-defensin 2. Science 2002, 298, 1025–1029. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.D.; Lutz, W.H.; Phan, V.A.; Bachman, L.A.; McKean, D.J.; Kumar, R. Potent inhibition of dendritic cell differentiation and maturation by vitamin D analogs. Biochem. Biophys. Res. Commun. 2000, 270, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Kabelitz, D. Expression and function of toll-like receptors in T lymphocytes. Curr. Opin. Immunol. 2007, 19, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Provvedini, D.M.; Tsoukas, C.D.; Deftos, L.J.; Manolagas, S.C. 1,25-dihydroxyvitamin D3 receptors in human leukocytes. Science 1983, 221, 1181–1183. [Google Scholar] [CrossRef] [PubMed]
- Rigby, W.F.; Stacy, T.; Fanger, M.W. Inhibition of T lymphocyte mitogenesis by 1,25-dihydroxyvitamin D3 (calcitriol). J. Clin. Investig. 1984, 74, 1451–1455. [Google Scholar] [CrossRef] [PubMed]
- Peng, G.; Guo, Z.; Kiniwa, Y.; Voo, K.S.; Peng, W.; Fu, T.; Wang, D.Y.; Li, Y.; Wang, H.Y.; Wang, R.-F. Toll-like receptor 8-mediated reversal of CD4+ regulatory T cell function. Science 2005, 309, 1380–1384. [Google Scholar] [CrossRef] [PubMed]
- Adorini, L.; Penna, G.; Giarratana, N.; Uskokovic, M. Tolerogenic dendritic cells induced by vitamin D receptor ligands enhance regulatory T cells inhibiting allograft rejection and autoimmune diseases. J. Cell. Biochem. 2003, 88, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Rozkova, D.; Horvath, R.; Bartunkova, J.; Spisek, R. Glucocorticoids severely impair differentiation and antigen presenting function of dendritic cells despite upregulation of toll-like receptors. Clin. Immunol. Orlando FL 2006, 120, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Ding, C.; Wilding, J.P.H.; Bing, C. 1,25-dihydroxyvitamin D3 protects against macrophage-induced activation of NF-κB and MAPK signalling and chemokine release in human adipocytes. PLoS ONE 2013, 8, e61707. [Google Scholar] [CrossRef]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; van der Meer, J.W.M.; Sutmuller, R.P.; Adema, G.J.; Kullberg, B.-J. From the Th1/Th2 paradigm towards a toll-like receptor/T-Helper bias. Antimicrob. Agents Chemother. 2005, 49, 3991–3996. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Cader, M.S.; Amarasinghe, A.; Abdul-Careem, M.F. Activation of toll-like receptor signaling pathways leading to nitric oxide-mediated antiviral responses. Arch. Virol. 2016, 161, 2075–2086. [Google Scholar] [CrossRef] [PubMed]
- Do, J.E.; Kwon, S.Y.; Park, S.; Lee, E.-S. Effects of vitamin D on expression of toll-like receptors of monocytes from patients with Behcet’s disease. Rheumatol. Oxf. Engl. 2008, 47, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, S.; Yun, J.-M.; Duncan-Staley, C.R.; Jialal, I. Low vitamin D levels correlate with the proinflammatory state in type 1 diabetic subjects with and without microvascular complications. Am. J. Clin. Pathol. 2011, 135, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Rodriguez, L.; Lopez-Hoyos, M.; Garcia-Unzueta, M.; Amado, J.A.; Cacho, P.M.; Martinez-Taboada, V.M. Age and low levels of circulating vitamin D are associated with impaired innate immune function. J. Leukoc. Biol. 2012, 91, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Ojaimi, S.; Skinner, N.A.; Strauss, B.J.; Sundararajan, V.; Woolley, I.; Visvanathan, K. Vitamin D deficiency impacts on expression of toll-like receptor-2 and cytokine profile: A pilot study. J. Transl. Med. 2013, 11, 176. [Google Scholar] [CrossRef] [PubMed]
- Du, T.; Zhou, Z.-G.; You, S.; Huang, G.; Lin, J.; Yang, L.; Li, X.; Zhou, W.-D.; Chao, C. Modulation of monocyte hyperresponsiveness to TLR ligands by 1,25-dihydroxy-vitamin D3 from LADA and T2DM. Diabetes Res. Clin. Pract. 2009, 83, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.; Wang, H.; Wu, F.; Li, M.; Chen, W.; Lv, L. Vitamin D3 alters toll-like receptor 4 signaling in monocytes of pregnant women at risk for preeclampsia. Int. J. Clin. Exp. Med. 2015, 8, 18041–18049. [Google Scholar] [PubMed]
- Dickie, L.J.; Church, L.D.; Coulthard, L.R.; Mathews, R.J.; Emery, P.; McDermott, M.F. Vitamin D3 down-regulates intracellular toll-like receptor 9 expression and toll-like receptor 9-induced IL-6 production in human monocytes. Rheumatology 2010, 49, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Földes, G.; von Haehling, S.; Okonko, D.O.; Jankowska, E.A.; Poole-Wilson, P.A.; Anker, S.D. Fluvastatin reduces increased blood monocyte toll-like receptor 4 expression in whole blood from patients with chronic heart failure. Int. J. Cardiol. 2008, 124, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Hodgkinson, C.P.; Ye, S. Statins inhibit toll-like receptor 4-mediated lipopolysaccharide signaling and cytokine expression. Pharmacogenet. Genom. 2008, 18, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lemus, E.; Murakami, Y.; Larrayoz-Roldan, I.M.; Moughamian, A.J.; Pavel, J.; Nishioku, T.; Saavedra, J.M. Angiotensin II AT1 receptor blockade decreases lipopolysaccharide-induced inflammation in the rat adrenal gland. Endocrinology 2008, 149, 5177–5188. [Google Scholar] [CrossRef] [PubMed]
- Dasu, M.R.; Riosvelasco, A.C.; Jialal, I. Candesartan inhibits toll-like receptor expression and activity both in vitro and in vivo. Atherosclerosis 2009, 202, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Zittermann, A. The biphasic effect of vitamin D on the musculoskeletal and cardiovascular system. Int. J. Endocrinol. 2017, 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hartley, L.; Clar, C.; Ghannam, O.; Flowers, N.; Stranges, S.; Rees, K. Vitamin K for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Gast, G.C.M.; de Roos, N.M.; Sluijs, I.; Bots, M.L.; Beulens, J.W.J.; Geleijnse, J.M.; Witteman, J.C.; Grobbee, D.E.; Peeters, P.H.M.; van der Schouw, Y.T. A high menaquinone intake reduces the incidence of coronary heart disease. Nutr. Metab. Cardiovasc. Dis. NMCD 2009, 19, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Cranenburg, E.C.M.; Schurgers, L.J.; Vermeer, C. Vitamin K: The coagulation vitamin that became omnipotent. Thromb. Haemost. 2007, 98, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Erkkilä, A.T.; Booth, S.L.; Hu, F.B.; Jacques, P.F.; Manson, J.E.; Rexrode, K.M.; Stampfer, M.J.; Lichtenstein, A.H. Phylloquinone intake as a marker for coronary heart disease risk but not stroke in women. Eur. J. Clin. Nutr. 2005, 59, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Erkkilä, A.T.; Booth, S.L.; Hu, F.B.; Jacques, P.F.; Lichtenstein, A.H. Phylloquinone intake and risk of cardiovascular diseases in men. Nutr. Metab. Cardiovasc. Dis. NMCD 2007, 17, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Erkkilä, A.T.; Booth, S.L. Vitamin K intake and atherosclerosis. Curr. Opin. Lipidol. 2008, 19, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Geleijnse, J.M.; Vermeer, C.; Grobbee, D.E.; Schurgers, L.J.; Knapen, M.H.J.; van der Meer, I.M.; Hofman, A.; Witteman, J.C.M. Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: The rotterdam study. J. Nutr. 2004, 134, 3100–3105. [Google Scholar] [PubMed]
- Van Ballegooijen, A.J.; Pilz, S.; Tomaschitz, A.; Grübler, M.R.; Verheyen, N. The synergistic interplay between vitamins D and K for bone and cardiovascular health: A narrative review. Int. J. Endocrinol. 2017, 2017, 1–12. [Google Scholar] [CrossRef]
- Braam, L.A.J.L.M.; Hoeks, A.P.G.; Brouns, F.; Hamulyák, K.; Gerichhausen, M.J.W.; Vermeer, C. Beneficial effects of vitamins D and K on the elastic properties of the vessel wall in postmenopausal women: A follow-up study. Thromb. Haemost. 2004. [Google Scholar] [CrossRef] [PubMed]
- Shea, M.K.; O’Donnell, C.J.; Hoffmann, U.; Dallal, G.E.; Dawson-Hughes, B.; Ordovas, J.M.; Price, P.A.; Williamson, M.K.; Booth, S.L. Vitamin K supplementation and progression of coronary artery calcium in older men and women. Am. J. Clin. Nutr. 2009, 89, 1799–1807. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Z.; Zhu, J.; Long, X.; Yan, J. Vitamin K2 can suppress the expression of toll-like receptor 2 (TLR2) and TLR4, and inhibit calcification of aortic intima in ApoE−/− mice as well as smooth muscle cells. Vascular 2017. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.-H.; Maresz, K.; Lee, P.-S.; Wu, J.-C.; Ho, C.-T.; Popko, J.; Mehta, D.S.; Stohs, S.J.; Badmaev, V. Inhibition of TNF-α, IL-1α, and IL-1β by Pretreatment of Human Monocyte-Derived Macrophages with Menaquinone-7 and Cell Activation with TLR Agonists In Vitro. J. Med. Food 2016, 19, 663–669. [Google Scholar] [CrossRef] [PubMed]

© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamczak, D.M. The Role of Toll-Like Receptors and Vitamin D in Cardiovascular Diseases—A Review. Int. J. Mol. Sci. 2017, 18, 2252. https://doi.org/10.3390/ijms18112252
Adamczak DM. The Role of Toll-Like Receptors and Vitamin D in Cardiovascular Diseases—A Review. International Journal of Molecular Sciences. 2017; 18(11):2252. https://doi.org/10.3390/ijms18112252
Chicago/Turabian StyleAdamczak, Daria M. 2017. "The Role of Toll-Like Receptors and Vitamin D in Cardiovascular Diseases—A Review" International Journal of Molecular Sciences 18, no. 11: 2252. https://doi.org/10.3390/ijms18112252
APA StyleAdamczak, D. M. (2017). The Role of Toll-Like Receptors and Vitamin D in Cardiovascular Diseases—A Review. International Journal of Molecular Sciences, 18(11), 2252. https://doi.org/10.3390/ijms18112252