Combined Gastric and Colorectal Cancer Screening—A New Strategy

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. General Characteristics of the Study Population
2.2. Histopathological Results of Endoscopic Gastric Biopsies
2.3. Helicobacter Pylori Infection Status
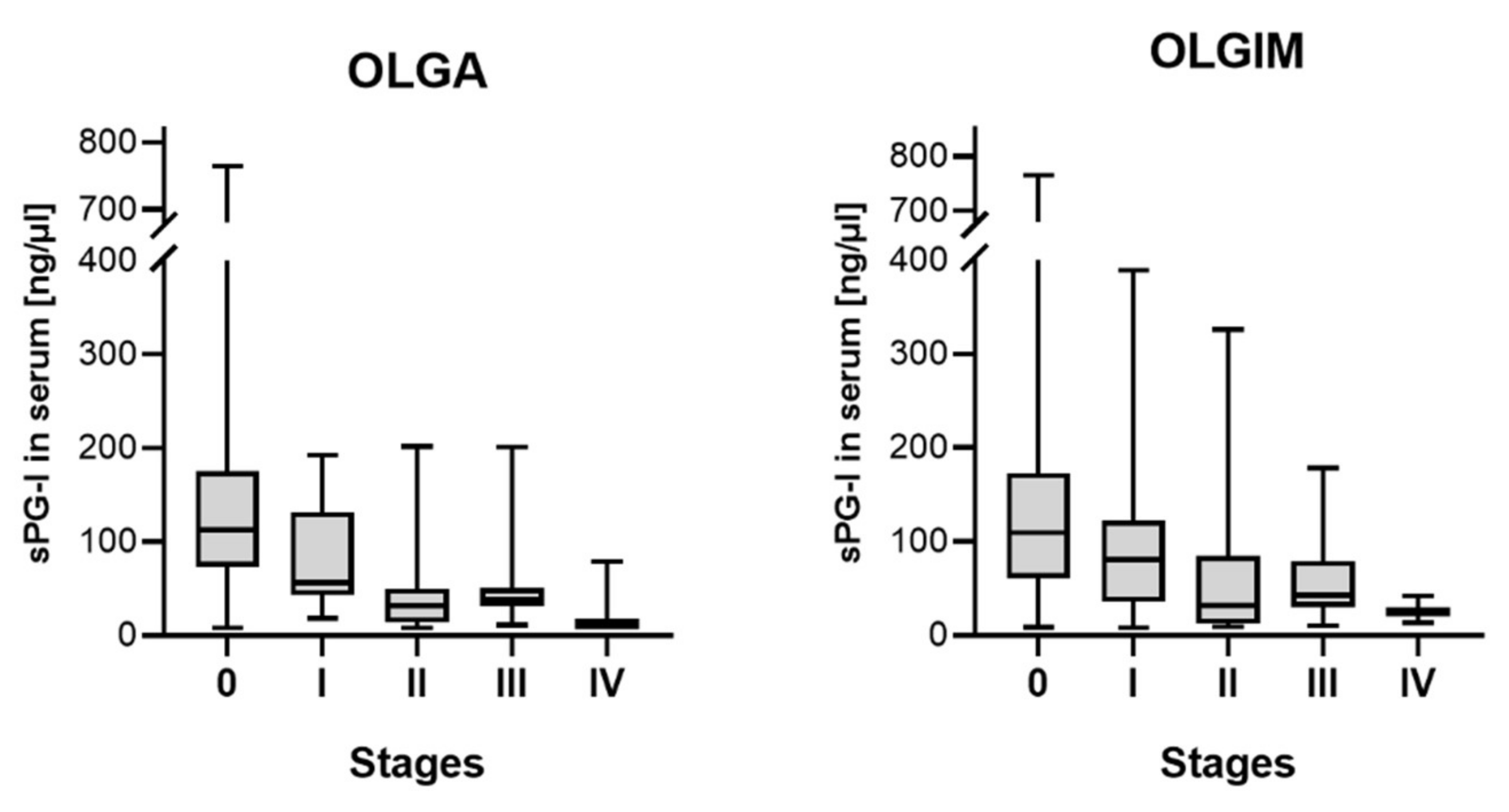
2.4. Serum Pepsinogen I and Histopathological Alterations
2.5. Combination with Other Serum Parameters
2.6. Risk Stratification
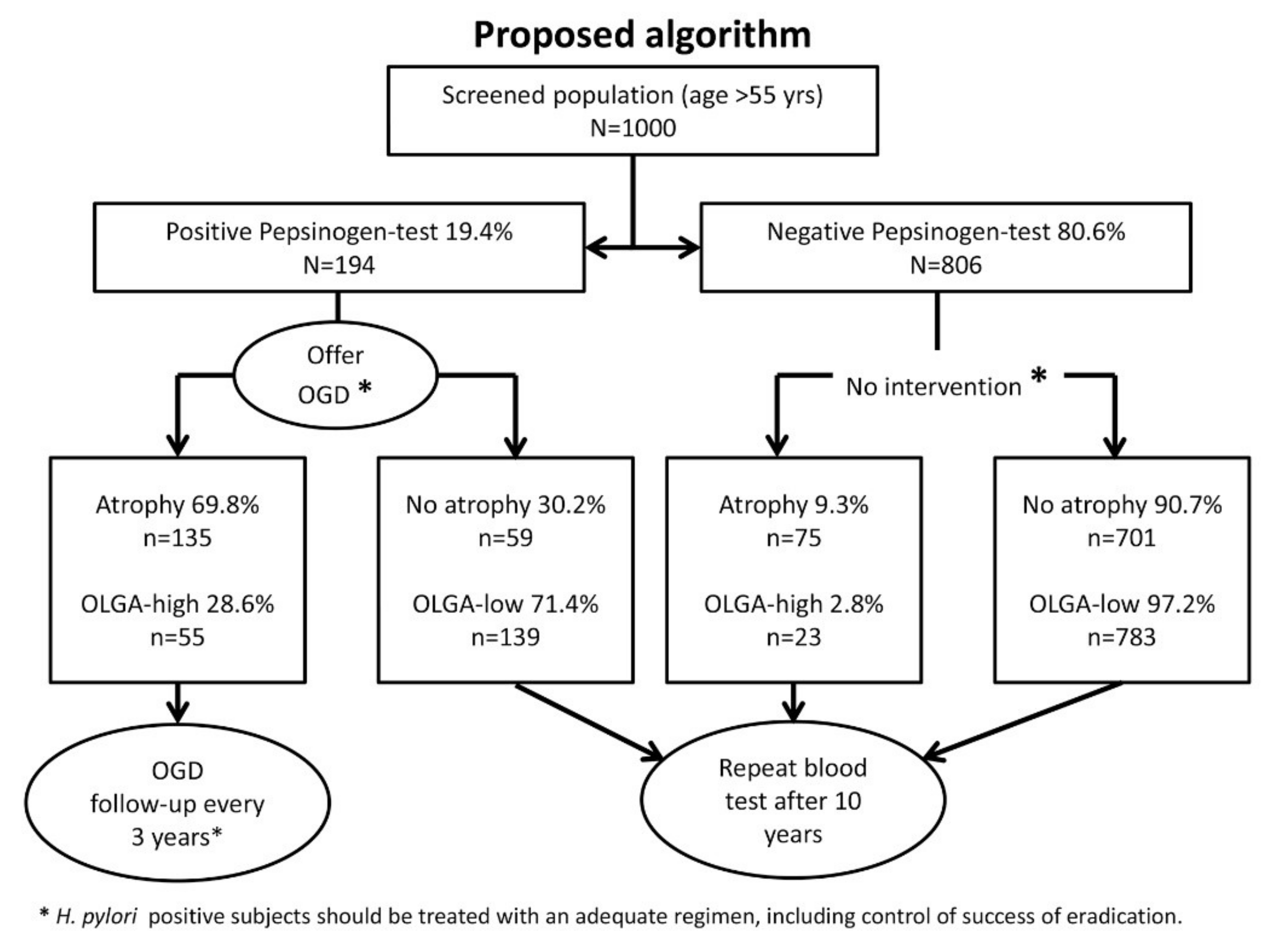
2.7. Proposal
3. Discussion
4. Material and Methods
4.1. Study Cohort
4.2. Assessment of Serum Parameters
4.3. Histopathological Assessment
4.4. Statistical Analysis
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Basu, P.; Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Vale, D.B.; Segnan, N.; Tomatis, M.; Soerjomataram, I.; Primic Žakelj, M.; et al. Status of implementation and organization of cancer screening in The European Union Member States-Summary results from the second European screening report. Int. J. Cancer 2018, 142, 44–56. [Google Scholar] [CrossRef]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef]
- Brenner, H.; Chang-Claude, J.; Jansen, L.; Knebel, P.; Stock, C.; Hoffmeister, M. Reduced risk of colorectal cancer up to 10 years after screening, surveillance, or diagnostic colonoscopy. Gastroenterology 2014, 146, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Nishihara, R.; Wu, K.; Lochhead, P.; Morikawa, T.; Liao, X.; Qian, Z.R.; Inamura, K.; Kim, S.A.; Kuchiba, A.; Yamauchi, M.; et al. Long-term colorectal-cancer incidence and mortality after lower endoscopy. The N. Engl. J. Med. 2013, 369, 1095–1105. [Google Scholar] [CrossRef]
- Brenner, H.; Hoffmeister, M.; Brenner, G.; Altenhofen, L.; Haug, U. Expected reduction of colorectal cancer incidence within 8 years after introduction of the German screening colonoscopy programme: Estimates based on 1,875,708 screening colonoscopies. Eur. J. Cancer 2009, 45, 2027–2033. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Shan, Y.-S.; Hu, H.-M.; Price, T.J.; Sirohi, B.; Yeh, K.-H.; Yang, Y.-H.; Sano, T.; Yang, H.-K.; Zhang, X.; et al. Management of gastric cancer in Asia: Resource-stratified guidelines. Lancet Oncol. 2013, 14, e535–e547. [Google Scholar] [CrossRef]
- Jun, J.K.; Choi, K.S.; Lee, H.-Y.; Suh, M.; Park, B.; Song, S.H.; Jung, K.W.; Lee, C.W.; Choi, I.J.; Park, E.-C.; et al. Effectiveness of the Korean National Cancer Screening Program in Reducing Gastric Cancer Mortality. Gastroenterology 2017, 152. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA-A Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends—An Update. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 16–27. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Link, A.; Selgrad, M. Helicobacter pylori: Perspectives and time trends. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 628–638. [Google Scholar] [CrossRef]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable to pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Herrero, R.; Park, J.Y.; Forman, D. The fight against gastric cancer—The IARC Working Group report. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 1107–1114. [Google Scholar] [CrossRef]
- Ford, A.C.; Forman, D.; Hunt, R.H.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer in healthy asymptomatic infected individuals: Systematic review and meta-analysis of randomised controlled trials. BMJ 2014, 348, g3174. [Google Scholar] [CrossRef]
- Ford, A.C.; Forman, D.; Hunt, R.; Yuan, Y.; Moayyedi, P. Helicobacter pylori eradication for the prevention of gastric neoplasia. In Cochrane Database of Systematic Reviews; Moayyedi, P., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2015. [Google Scholar]
- Bornschein, J.; Malfertheiner, P. Helicobacter pylori and gastric cancer. Dig. Dis. 2014, 32, 249–264. [Google Scholar] [CrossRef]
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef]
- Dinis-Ribeiro, M.; Areia, M.; de Vries, A.C.; Marcos-Pinto, R.; Monteiro-Soares, M.; O’Connor, A.; Pereira, C.; Pimentel-Nunes, P.; Correia, R.; Ensari, A.; et al. Management of precancerous conditions and lesions in the stomach (MAPS): Guideline from the European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter Study Group (EHSG), European Society of Pathology (ESP), and the Sociedade Portuguesa. Endoscopy 2012, 44, 74–94. [Google Scholar] [CrossRef]
- Yanaoka, K.; Oka, M.; Ohata, H.; Yoshimura, N.; Deguchi, H.; Mukoubayashi, C.; Enomoto, S.; Inoue, I.; Iguchi, M.; Maekita, T.; et al. Eradication of Helicobacter pylori prevents cancer development in subjects with mild gastric atrophy identified by serum pepsinogen levels. Int. J. Cancer 2009, 125, 2697–2703. [Google Scholar] [CrossRef]
- Leja, M.; Park, J.Y.; Murillo, R.; Liepniece-Karele, I.; Isajevs, S.; Kikuste, I.; Rudzite, D.; Krike, P.; Parshutin, S.; Polaka, I.; et al. Multicentric randomised study of Helicobacter pylori eradication and pepsinogen testing for prevention of gastric cancer mortality: The GISTAR study. BMJ Open 2017, 7, e016999. [Google Scholar] [CrossRef]
- Watabe, H.; Mitsushima, T.; Yamaji, Y.; Okamoto, M.; Wada, R.; Kokubo, T.; Doi, H.; Yoshida, H.; Kawabe, T.; Omata, M. Predicting the development of gastric cancer from combining Helicobacter pylori antibodies and serum pepsinogen status: A prospective endoscopic cohort study. Gut 2005, 54, 764–768. [Google Scholar] [CrossRef]
- Terasawa, T.; Nishida, H.; Kato, K.; Miyashiro, I.; Yoshikawa, T.; Takaku, R.; Hamashima, C. Prediction of gastric cancer development by serum pepsinogen test and Helicobacter pylori seropositivity in Eastern Asians: A systematic review and meta-analysis. PLoS ONE 2014, 9, e109783. [Google Scholar] [CrossRef]
- Tashiro, A.; Sano, M.; Kinameri, K.; Fujita, K.; Takeuchi, Y. Comparing mass screening techniques for gastric cancer in Japan. World J. Gastroenterol. 2006, 12, 4873–4874. [Google Scholar]
- Paterson, H.M.; McCole, D.; Auld, C.D. Impact of open-access endoscopy on detection of early oesophageal and gastric cancer 1994–2003: Population-based study. Endoscopy 2006, 38, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. European Helicobacter and Microbiota Study Group and Consensus panel Management of Helicobacter pylori infection—The Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed]
- Marques-Silva, L.; Areia, M.; Elvas, L.; Dinis-Ribeiro, M. Prevalence of gastric precancerous conditions. Eur. J. Gastroenterol. Hepatol. 2014, 26, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Areia, M.; Spaander, M.C.; Kuipers, E.J.; Dinis-Ribeiro, M. Endoscopic screening for gastric cancer: A cost-utility analysis for countries with an intermediate gastric cancer risk. United Eur. Gastroenterol. J. 2018, 6, 192–202. [Google Scholar] [CrossRef]
- Sasazuki, S. The ABC Method and Gastric Cancer: Evidence From Prospective Studies. J. Epidemiol. 2016, 26, 611–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tepes, B.; Seruga, M.; Vujasinovic, M.; Urlep, D.; Ljepovic, L.; Brglez, J.N.; Forte, A.; Anita Kek, L.; Skvarc, M. Premalignant Gastric Lesions in Patients Included in National Colorectal Cancer Screening. Radiol. Oncol. 2018, 52, 7–13. [Google Scholar] [CrossRef]
- Goni, E.; Venerito, M.; Schulz, C.; Weigt, J.; Langner, C.; Link, A.; Malfertheiner, P. Influence of laboratory-related and endoscopy-related factors on the assessment of serum pepsinogens and gastrin-17. Eur. J. Gastroenterol. Hepatol. 2017, 29, 1340–1345. [Google Scholar] [CrossRef]
- Zagari, R.M.; Rabitti, S.; Greenwood, D.C.; Eusebi, L.H.; Vestito, A.; Bazzoli, F. Systematic review with meta-analysis: Diagnostic performance of the combination of pepsinogen, gastrin-17 and anti-Helicobacter pylori antibodies serum assays for the diagnosis of atrophic gastritis. Aliment. Pharmacol. Therapeut. 2017, 46, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P. Editorial: The non-invasive diagnosis of atrophic gastritis. Aliment. Pharmacol. Therapeut. 2017, 46, 1112–1113. [Google Scholar] [CrossRef]
- De Re, V.; Orzes, E.; Canzonieri, V.; Maiero, S.; Fornasarig, M.; Alessandrini, L.; Cervo, S.; Steffan, A.; Zanette, G.; Mazzo, C.; et al. Pepsinogens to Distinguish Patients With Gastric Intestinal Metaplasia and Helicobacter pylori Infection Among Populations at Risk for Gastric Cancer. Clin. Transl. Gastroenterol. 2016, 7, e183. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Moore, S.P.; Hassler, S.; Ellison-Loschmann, L.; Forman, D.; Bray, F. The burden of stomach cancer in indigenous populations: A systematic review and global assessment. Gut 2013, 63, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Wong, B.C.-Y.; Lam, S.K.; Wong, W.M.; Chen, J.S.; Zheng, T.T.; Feng, R.E.; Lai, K.C.; Hu, W.H.C.; Yuen, S.T.; Leung, S.Y.; et al. Helicobacter pylori eradication to prevent gastric cancer in a high-risk region of China: A randomized controlled trial. JAMA 2004, 291, 187–194. [Google Scholar] [CrossRef]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef]
- Yoon, S.B.; Park, J.M.; Lim, C.-H.; Cho, Y.K.; Choi, M.-G. Effect of Helicobacter pylori eradication on metachronous gastric cancer after endoscopic resection of gastric tumors: A meta-analysis. Helicobacter 2014, 19, 243–248. [Google Scholar] [CrossRef]
- Han, S.J.; Kim, S.G.; Lim, J.H.; Choi, J.M.; Oh, S.; Park, J.Y.; Kim, J.; Kim, J.S.; Jung, H.C. Long-Term Effects of Helicobacter pylori Eradication on Metachronous Gastric Cancer Development. Gut Liver 2018, 12, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G.M.; Warren, J.R.; Glaser, M.E.; Cullen, D.J.; Marshall, B.J.; Collins, B.J. Long-term follow-up of gastric histology after Helicobacter pylori eradication. J. Gastroenterol. Hepatol. 1996, 11, 670–673. [Google Scholar] [CrossRef] [PubMed]
- Annibale, B.; Aprile, M.R.; D’ambra, G.; Caruana, P.; Bordi, C.; Delle Fave, G. Cure of Helicobacter pylori infection in atrophic body gastritis patients does not improve mucosal atrophy but reduces hypergastrinemia and its related effects on body ECL-cell hyperplasia. Aliment. Pharmacol. Therapeut. 2000, 14, 625–634. [Google Scholar] [CrossRef]
- Watanabe, H.; Yamaguchi, N.; Kuwayama, H.; Sekine, C.; Uemura, N.; Kaise, M.; Nakamura, T.; Kubo, M.; Yoshida, S.; Haruma, K.; et al. Improvement in gastric histology following Helicobacter pylori eradication therapy in Japanese peptic ulcer patients. J. Int. Med. Res. 2003, 31, 362–369. [Google Scholar] [CrossRef]
- Ito, M.; Haruma, K.; Kamada, T.; Mihara, M.; Kim, S.; Kitadai, Y.; Sumii, M.; Tanaka, S.; Yoshihara, M.; Chayama, K. Helicobacter pylori eradication therapy improves atrophic gastritis and intestinal metaplasia: A 5-year prospective study of patients with atrophic gastritis. Aliment. Pharmacol. Therapeut. 2002, 16, 1449–1456. [Google Scholar] [CrossRef]
- Xiao, S.; Li, S.; Zhou, L.; Jiang, W.; Liu, J. Helicobacter pylori status and risks of metachronous recurrence after endoscopic resection of early gastric cancer: A systematic review and meta-analysis. J. Gastroenterol. 2018. [Google Scholar] [CrossRef]
- Choi, I.J.; Kook, M.-C.; Kim, Y.-I.; Cho, S.-J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.-H. Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef]
- Malfertheiner, P. Helicobacter pylori Treatment for Gastric Cancer Prevention. N. Engl. J. Med. 2018, 378, 1154–1156. [Google Scholar] [CrossRef]
- Yeh, J.M.; Hur, C.; Ward, Z.; Schrag, D.; Goldie, S.J. Gastric adenocarcinoma screening and prevention in the era of new biomarker and endoscopic technologies: A cost-effectiveness analysis. Gut 2016, 65, 563–574. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Lin, J.-T.; Wu, H.-M.; Liu, T.-Y.; Yen, M.-F.; Chiu, H.-M.; Wang, H.-P.; Wu, M.-S.; Hsiu-Hsi Chen, T. Cost-effectiveness analysis between primary and secondary preventive strategies for gastric cancer. Cancer Epidemiol. Biomarkers Prev. 2007, 16, 875–885. [Google Scholar] [CrossRef]
- Lomba-Viana, R.; Dinis-Ribeiro, M.; Fonseca, F.; Vieira, A.S.; Bento, M.J.B.; Lomba-Viana, H. Serum pepsinogen test for early detection of gastric cancer in a European country. Eur. J. Gastroenterol. Hepatol. 2012, 24, 37–41. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- Capelle, L.G.; de Vries, A.C.; Haringsma, J.; Ter Borg, F.; de Vries, R.A.; Bruno, M.J.; van Dekken, H.; Meijer, J.; van Grieken, N.C.T.; Kuipers, E.J. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest. Endosc. 2010, 71, 1150–1158. [Google Scholar] [CrossRef]
- Rugge, M.; Correa, P.; Di Mario, F.; El-Omar, E.; Fiocca, R.; Geboes, K.; Genta, R.M.; Graham, D.Y.; Hattori, T.; Malfertheiner, P.; et al. OLGA staging for gastritis: A tutorial. Dig. Liver Dis. 2008, 40, 650–658. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Item | PG*-Positive (n = 63) | PG-Negative (n = 216) | Total (n = 279) | p-Value | |
|---|---|---|---|---|---|
| Age | median (range) | 64 (50–93) | 67 (50–94) | 67 (50–94) | 0.931 |
| Sex | male (%) | 37 (58.7%) | 121 (56.0%) | 158 (56.6%) | 0.773 |
| H. pylori | positive (%) | 21 (33.3%) | 64 (29.6%) | 85 (30.5%) | 0.641 |
| Atrophy | positive (%) | 44 (69.8%) | 20 (9.3%) | 64 (23.1%) | <0.001 |
| IM * | positive (%) | 30 (47.6%) | 29 (13.6%) | 59 (21.3%) | <0.001 |
| OLGA * | Stage 0 | 17 (27.0%) | 194 (90.7%) | 211 (76.2%) | <0.001 |
| Stage I | 11 (17.5%) | 9 (4.2%) | 20 (7.2%) | ||
| Stage II | 17 (27.0%) | 5 (2.3%) | 22 (7.9%) | ||
| Stage III | 16 (25.4%) | 5 (2.3%) | 21 (7.6%) | ||
| Stage IV | 2 (3.2%) | 1 (0.5%) | 3 (1.1%) | ||
| OLGIM * | Stage 0 | 33 (27.0%) | 185 (86.4%) | 218 (78.7%) | <0.001 |
| Stage I | 9 (17.5%) | 19 (6.9%) | 28 (10.1%) | ||
| Stage II | 10 (27.0%) | 7 (3.3%) | 17 (6.1%) | ||
| Stage III | 8 (25.4%) | 3 (1.4%) | 11 (4.0%) | ||
| Stage IV | 3 (3.2%) | 0 (0.0%) | 3 (1.1%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selgrad, M.; Bornschein, J.; Kandulski, A.; Weigt, J.; Roessner, A.; Wex, T.; Malfertheiner, P. Combined Gastric and Colorectal Cancer Screening—A New Strategy. Int. J. Mol. Sci. 2018, 19, 3854. https://doi.org/10.3390/ijms19123854
Selgrad M, Bornschein J, Kandulski A, Weigt J, Roessner A, Wex T, Malfertheiner P. Combined Gastric and Colorectal Cancer Screening—A New Strategy. International Journal of Molecular Sciences. 2018; 19(12):3854. https://doi.org/10.3390/ijms19123854
Chicago/Turabian StyleSelgrad, Michael, Jan Bornschein, Arne Kandulski, Jochen Weigt, Albert Roessner, Thomas Wex, and Peter Malfertheiner. 2018. "Combined Gastric and Colorectal Cancer Screening—A New Strategy" International Journal of Molecular Sciences 19, no. 12: 3854. https://doi.org/10.3390/ijms19123854
APA StyleSelgrad, M., Bornschein, J., Kandulski, A., Weigt, J., Roessner, A., Wex, T., & Malfertheiner, P. (2018). Combined Gastric and Colorectal Cancer Screening—A New Strategy. International Journal of Molecular Sciences, 19(12), 3854. https://doi.org/10.3390/ijms19123854