The Role of Genetic Polymorphisms in Chronic Pain Patients

 ,
, 
Abstract
:
1. Introduction
2. Genetic Polymorphisms Influence on Chronic Pain Conditions
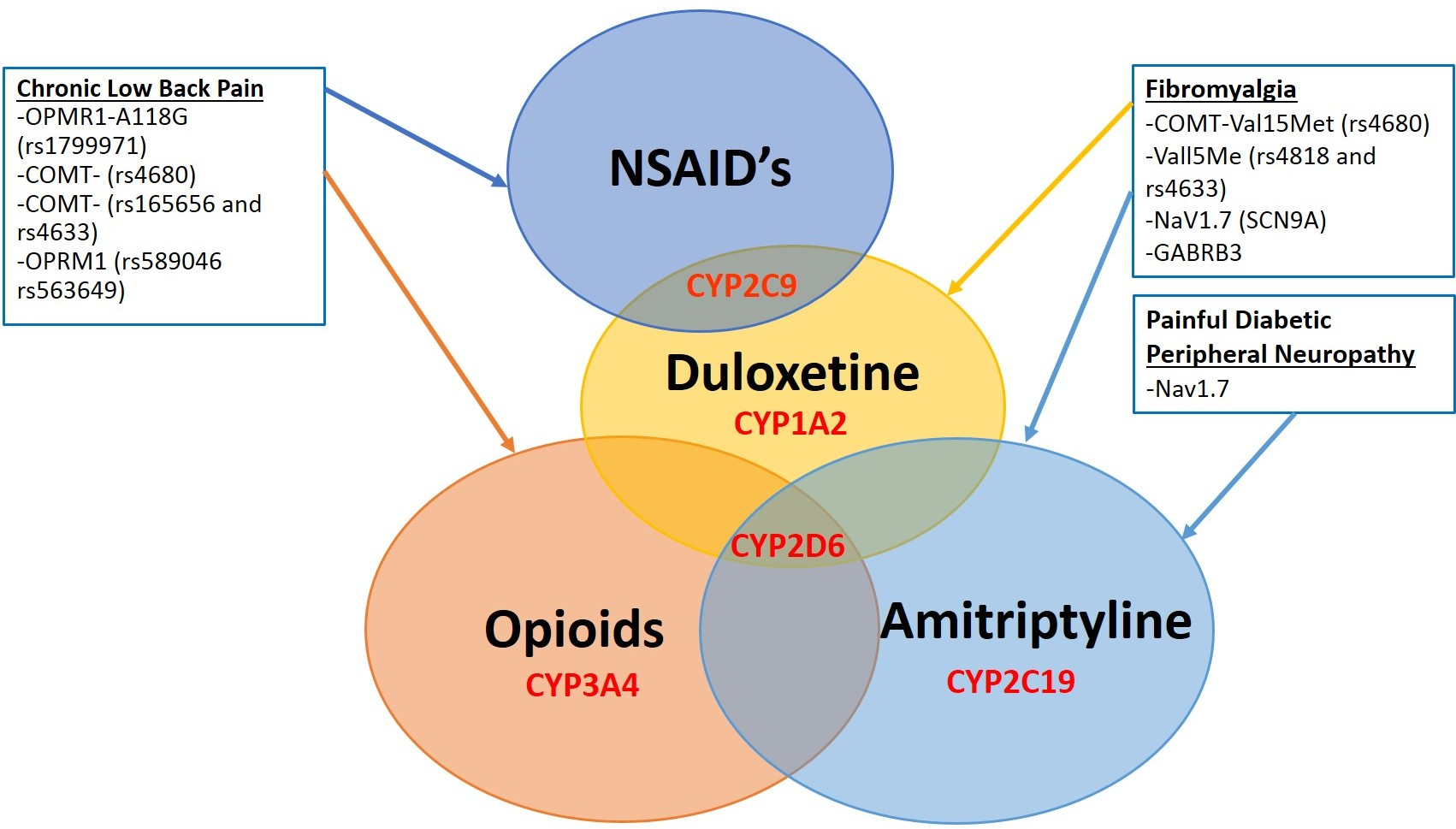
2.1. Fibromyalgia
2.2. Chronic Low Back Pain
2.3. Migraine Headaches
2.4. Painful Diabetic Peripheral Neuropathy
2.5. Trigeminal Neuralgia
3. Genetic Polymorphisms and Gene Products Influence on Pain Medications
3.1. Duloxetine
3.2. Amitriptyline
3.3. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
3.4. Opioids
3.5. Prophylactic Drugs Treatment for Migraine
4. Clinical Applications of Pharmacogenetics
4.1. Pain Perception Assessment
4.2. CYP450 2D6 Genotyping
4.3. Methadone Initiation Assessment
4.4. Opioid Addiction Genotyping
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| DEA | Drug Enforcement Administration |
| FM | fibromyalgia |
| SLC6A4 | serotonin transporter gene |
| TRPV2 | transient receptor potential vanilloid 2 genes |
| CSF | cerebrospinal fluid |
| (5-HT) | 5-hydroxytriptamine |
| (5-HTT) | serotonin transporter |
| COMT | Catechol-O-methyltransferase |
| SNP | short nucleotide polymorphisms |
| DRD4 | dopamine receptor D4 |
| MAO | A-monoamine oxidase |
| GTPCH | guanosine triphosphate cyclohydrolase |
| GABRB3 | GABA receptor beta 3 subunit |
| APOE | apolipoprotein MYT1L myelin transcription factor 1 |
| CLBP | chronic low back pain |
| OPRM1 | opioid receptor µ 1 |
| LDD | lumbar disk disease |
| GDF5 | growth differentiation factor 5 |
| COMT | catecholaminergic enzyme |
| VNTR | variable nucleotide tandem repeat |
| NSAIDs | (nonsteroidal anti-inflammatory drugs) |
| ACAN | chondroitin sulfate-1 encoding domain of the aggrecan gene |
| EDNRA | encoding endothelin type A receptor |
| MTHFR | encoding methylenetetrahydrofolate reductase |
| NOS3 | encoding endothelial nitric oxide synthase |
| ACE | encoding angiotensin-1 converting enzyme |
| TGFB2 | encoding β-2 transforming growth factor |
| TGFBR2 | encoding β-2 transforming growth factor receptor |
| VEGF | vascular endothelial growth factor |
| NOTCH3 | neurogenic locus notch homolog protein 3 |
| ESR1 | estrogen receptor 1 |
| MTHFR | methylenetetrahydrofolate reductase |
| DPN | painful diabetic peripheral neuropathy |
| 5-HTTLPR | 5-hydroxytriptamine transporter-linked polymorphic region |
| TN | trigeminal neuralgia |
| CYP450 | cytochrome P450 |
| TCA | tricyclic antidepressant |
| DPWG | Dutch Pharmacogenetics Working Group |
| CPIC | Clinical Pharmacogenetics Implementation Consortium |
| SSRIs | selective serotonin reuptake inhibitors |
| NSRIs | non-selective reuptake inhibitors |
| IM | intermediate-metabolizer |
| EM | extensive metabolizer |
| DDIs | drug-drug interactions |
| DGIs | drug-gene interactions |
| DDGIs | drug-drug-gene interactions |
| DOA | deceased patients with opioid addiction |
| LOA | living patients with opioid addiction |
| ABCB1 | ATP-binding cassette sub-family B member 1 |
References
- Manchikanti, L.; Atluri, S.; Candido, K.D.; Boswell, M.V.; Simopoulos, T.T.; Grider, J.S.; Falco, F.J.; Hirsch, J.A. Zohydro approval by food and drug administration: Controversial or frightening? Pain Physician 2014, 17, E437–E450. [Google Scholar] [PubMed]
- Gaskin, D.J.; Richard, P. The economic costs of pain in the United States. J. Pain 2012, 13, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.A.; Seth, P.; David, F.; Scholl, L. Increases in Drug and Opioid-Involved Overdose Deaths—United States, 2010–2015. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Kolodny, A.; Courtwright, D.T.; Hwang, C.S.; Kreiner, P.; Eadie, J.L.; Clark, T.W.; Alexander, G.C. The prescription opioid and heroin crisis: A public health approach to an epidemic of addiction. Annu. Rev. Public Health 2015, 36, 559–574. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Lee, S.S. New insights into the genetics of fibromyalgia. Korean J. Intern. Med. 2017, 32, 984–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diatchenko, L.; Fillingim, R.B.; Smith, S.B.; Maixner, W. The phenotypic and genetic signatures of common musculoskeletal pain conditions. Nat. Rev. Rheumatol. 2013, 9, 340–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, L.M.; Fan, J.; Russell, I.J.; Yunus, M.B.; Khan, M.A.; Kushner, I.; Olson, J.M.; Iyengar, S.K. The fibromyalgia family study: A genome-wide linkage scan study. Arthritis Rheumatol. 2013, 65, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Kim, S.H.; Nah, S.S.; Lee, J.H.; Kim, S.K.; Lee, Y.A.; Hong, S.J.; Kim, H.S.; Lee, H.S.; Kim, H.A.; et al. Polymorphisms of the TRPV2 and TRPV3 genes associated with fibromyalgia in a Korean population. Rheumatology 2016, 55, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- Tour, J.; Lofgren, M.; Mannerkorpi, K.; Gerdle, B.; Larsson, A.; Palstam, A.; Bileviciute-Ljungar, I.; Bjersing, J.; Martin, I.; Ernberg, M.; et al. Gene-to-gene interactions regulate endogenous pain modulation in fibromyalgia patients and healthy controls-antagonistic effects between opioid and serotonin-related genes. Pain 2017, 158, 1194–1203. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Jauand, M.; Sitges, C.; Rodriguez, V.; Picornell, A.; Ramon, M.; Buskila, D.; Montoya, P. Pain sensitivity in fibromyalgia is associated with catechol-O-methyltransferase (COMT) gene. Eur. J. Pain 2013, 17, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Park, D.J.; Kang, J.H.; Yim, Y.R.; Kim, J.E.; Lee, J.W.; Lee, K.E.; Wen, L.; Kim, T.J.; Park, Y.W.; Lee, S.S. Exploring Genetic Susceptibility to Fibromyalgia. Chonnam Med. J. 2015, 51, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Zorina-Lichtenwalter, K.; Meloto, C.B.; Khoury, S.; Diatchenko, L. Genetic predictors of human chronic pain conditions. Neuroscience 2016, 338, 36–62. [Google Scholar] [CrossRef] [PubMed]
- Inanir, A.; Yigit, S.; Tekcan, A.; Pinarli, F.A.; Inanir, S.; Karakus, N. Angiotensin converting enzyme and methylenetetrahydrofolate reductase gene variations in fibromyalgia syndrome. Gene 2015, 564, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, J.B.; Barbosa, F.R.; Morel, L.J.; Franca Sde, C.; Zingaretti, S.M.; da Silva, L.M.; Pereira, A.M.; Marins, M.; Fachin, A.L. Serotonin receptor (5-HT 2A) and catechol-O-methyltransferase (COMT) gene polymorphisms: Triggers of fibromyalgia? Rev. Bras. Reumatol. 2010, 50, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.Y.; Yang, L.C.; Lu, H.F.; Ko, J.Y.; Wang, C.H.; Lin, S.H.; Lee, T.H.; Concejero, A.; Hsu, C.J. Association of mu-opioid receptor gene polymorphism (A118G) with variations in morphine consumption for analgesia after total knee arthroplasty. Acta Anaesthesiol. Scand. 2006, 50, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.B.; Jacobsen, L.M.; Schistad, E.I.; Pedersen, L.M.; Rygh, L.J.; Roe, C.; Gjerstad, J. Pain intensity the first year after lumbar disc herniation is associated with the A118G polymorphism in the opioid receptor mu 1 gene: Evidence of a sex and genotype interaction. J. Neurosci. 2012, 32, 9831–9834. [Google Scholar] [CrossRef] [PubMed]
- Paassilta, P.; Lohiniva, J.; Goring, H.H.; Perala, M.; Raina, S.S.; Karppinen, J.; Hakala, M.; Palm, T.; Kroger, H.; Kaitila, I.; et al. Identification of a novel common genetic risk factor for lumbar disk disease. JAMA 2001, 285, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Higashino, K.; Matsui, Y.; Yagi, S.; Takata, Y.; Goto, T.; Sakai, T.; Katoh, S.; Yasui, N. The alpha2 type IX collagen tryptophan polymorphism is associated with the severity of disc degeneration in younger patients with herniated nucleus pulposus of the lumbar spine. Int. Orthop. 2007, 31, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, L.M.; Schistad, E.I.; Storesund, A.; Pedersen, L.M.; Rygh, L.J.; Roe, C.; Gjerstad, J. The COMT rs4680 Met allele contributes to long-lasting low back pain, sciatica and disability after lumbar disc herniation. Eur. J. Pain 2012, 16, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Gruber, H.E.; Sha, W.; Brouwer, C.R.; Steuerwald, N.; Hoelscher, G.L.; Hanley, E.N., Jr. A novel catechol-O-methyltransferase variant associated with human disc degeneration. Int. J. Med. Sci. 2014, 11, 748–753. [Google Scholar] [CrossRef] [PubMed]
- Gasparini, C.F.; Sutherland, H.G.; Griffiths, L.R. Studies on the pathophysiology and genetic basis of migraine. Curr. Genomics 2013, 14, 300–315. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, R.; Dong, Z.; Wang, X.; Yu, S. Impact of ESR1 Gene Polymorphisms on Migraine Susceptibility: A Meta-Analysis. Medicine 2015, 94, e0976. [Google Scholar] [CrossRef] [PubMed]
- Shao, E.; Hughes, J.; Eley, R. The presenting and prescribing patterns of migraine in an Australian emergency department: A descriptive exploratory study. World J. Emerg. Med. 2017, 8, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, CSD, sensitization and modulation of pain. Pain 2013, 154, S44–S53. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A.; Salomone, S.; Caraci, F.; Pizza, V.; Bernardini, R.; D’Amato, C.C. Role of magnesium, coenzyme Q10, riboflavin, and vitamin B12 in migraine prophylaxis. Vitam. Horm. 2004, 69, 297–312. [Google Scholar] [PubMed]
- Christensen, A.F.; Esserlind, A.L.; Werge, T.; Stefansson, H.; Stefansson, K.; Olesen, J. The influence of genetic constitution on migraine drug responses. Cephalalgia 2016, 36, 624–639. [Google Scholar] [CrossRef] [PubMed]
- Takigawa, H.; Kowa, H.; Nakashima, K. No associations between five polymorphisms in COMT gene and migraine. Acta Neurol. Scand. 2017, 135, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Blesneac, I.; Themistocleous, A.C.; Fratter, C.; Conrad, L.J.; Ramirez, J.D.; Cox, J.J.; Tesfaye, S.; Shillo, P.R.; Rice, A.S.C.; Tucker, S.J.; et al. Rare NaV1.7 variants associated with painful diabetic peripheral neuropathy. Pain 2018, 159, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Deshmukh, H.A.; Donnelly, L.A.; Torrance, N.; Colhoun, H.M.; Palmer, C.N.; Smith, B.H. A Genome-wide Association Study Provides Evidence of Sex-specific Involvement of Chr1p35.1 (ZSCAN20-TLR12P) and Chr8p23.1 (HMGB1P46) With Diabetic Neuropathic Pain. EBioMedicine 2015, 2, 1386–1393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monastiriotis, C.; Papanas, N.; Veletza, S.; Maltezos, E. APOE gene polymorphisms and diabetic peripheral neuropathy. Arch. Med. Sci. 2012, 8, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Clair, C.; Cohen, M.J.; Eichler, F.; Selby, K.J.; Rigotti, N.A. The Effect of Cigarette Smoking on Diabetic Peripheral Neuropathy: A Systematic Review and Meta-Analysis. J. Gen. Intern. Med. 2015, 30, 1193–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martirosyan, N.L.; Patel, A.A.; Carotenuto, A.; Kalani, M.Y.; Belykh, E.; Walker, C.T.; Preul, M.C.; Theodore, N. Genetic Alterations in Intervertebral Disc Disease. Front. Surg. 2016, 3, 59. [Google Scholar] [CrossRef] [PubMed]
- Uttara, B.; Singh, A.V.; Zamboni, P.; Mahajan, R.T. Oxidative stress and neurodegenerative diseases: A review of upstream and downstream antioxidant therapeutic options. Curr. Neuropharmacol. 2009, 7, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Meng, W.; Adams, M.J.; Hebert, H.L.; Deary, I.J.; McIntosh, A.M.; Smith, B.H. A Genome-Wide Association Study Finds Genetic Associations with Broadly-Defined Headache in UK Biobank (N=223,773). EBioMedicine 2018, 28, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Sadosky, A.; Schaefer, C.; Mann, R.; Bergstrom, F.; Baik, R.; Parsons, B.; Nalamachu, S.; Nieshoff, E.; Stacey, B.R.; Anschel, A.; et al. Burden of illness associated with painful diabetic peripheral neuropathy among adults seeking treatment in the US: Results from a retrospective chart review and cross-sectional survey. Diabetes Metab. Syndr. Obes. 2013, 6, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Yu, X.; Zhang, H. The serotonin transporter gene polymorphism is associated with the susceptibility and the pain severity in idiopathic trigeminal neuralgia patients. J. Headache Pain 2014, 15, 42. [Google Scholar] [CrossRef] [PubMed]
- Hocum, B.T.; White, J.R., Jr.; Heck, J.W.; Thirumaran, R.K.; Moyer, N.; Newman, R.; Ashcraft, K. Cytochrome P-450 gene and drug interaction analysis in patients referred for pharmacogenetic testing. Am. J. Health Syst. Pharm. 2016, 73, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Samer, C.F.; Daali, Y.; Wagner, M.; Hopfgartner, G.; Eap, C.B.; Rebsamen, M.C.; Rossier, M.F.; Hochstrasser, D.; Dayer, P.; Desmeules, J.A. Genetic polymorphisms and drug interactions modulating CYP2D6 and CYP3A activities have a major effect on oxycodone analgesic efficacy and safety. Br. J. Pharmacol. 2010, 160, 919–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knadler, M.P.; Lobo, E.; Chappell, J.; Bergstrom, R. Duloxetine: Clinical pharmacokinetics and drug interactions. Clin. Pharmacokinet. 2011, 50, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Bajwa, Z.H.; Simopoulos, T.T.; Pal, J.; Kraemer, J.J.; Chopra, P.; Nagda, J.V.; Najib, U.; Celestin, J.; Sial, K.; Ahmad, B.; et al. Low and therapeutic doses of antidepressants are associated with similar response in the context of multimodal treatment of pain. Pain Physician 2009, 12, 893–900. [Google Scholar] [PubMed]
- Kapur, B.M.; Lala, P.K.; Shaw, J.L. Pharmacogenetics of chronic pain management. Clin. Biochem. 2014, 47, 1169–1187. [Google Scholar] [CrossRef] [PubMed]
- Prior, T.I.; Baker, G.B. Interactions between the cytochrome P450 system and the second-generation antipsychotics. J. Psychiatry Neurosci. 2003, 28, 99–112. [Google Scholar] [PubMed]
- Ryu, S.; Park, S.; Lee, J.H.; Kim, Y.R.; Na, H.S.; Lim, H.S.; Choi, H.Y.; Hwang, I.Y.; Lee, J.G.; Park, Z.W.; et al. A Study on CYP2C19 and CYP2D6 Polymorphic Effects on Pharmacokinetics and Pharmacodynamics of Amitriptyline in Healthy Koreans. Clin. Transl. Sci. 2017, 10, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Arellano, A.L.; Martin-Subero, M.; Monerris, M.; A, L.; Farre, M.; Montane, E. Multiple adverse drug reactions and genetic polymorphism testing: A case report with negative result. Medicine 2017, 96, e8505. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, A.; Franceschi, M.; Vitale, D.F.; Zaninelli, A.; Masotti, G.; Rengo, F.; F.I.R.I (Fondazione Italiana Ricerca Sull’Invecchiamento); Sofia Project Investigators. Upper gastrointestinal symptoms and therapies in elderly out-patients, users of non-selective NSAIDs or coxibs. Aliment. Pharmacol. Ther. 2005, 22, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olesen, A.E.; Sato, H.; Nielsen, L.M.; Staahl, C.; Droney, J.; Gretton, S.; Branford, R.; Drewes, A.M.; Arendt-Nielsen, L.; Riley, J.; et al. The genetic influences on oxycodone response characteristics in human experimental pain. Fundam. Clin. Pharmacol. 2015, 29, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Smith, H.S. The metabolism of opioid agents and the clinical impact of their active metabolites. Clin. J. Pain 2011, 27, 824–838. [Google Scholar] [CrossRef] [PubMed]
- Tverdohleb, T.; Dinc, B.; Knezevic, I.; Candido, K.D.; Knezevic, N.N. The role of cytochrome P450 pharmacogenomics in chronic non-cancer pain patients. Expert Opin. Drug Metab. Toxicol. 2016, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gudin, J. Opioid therapies and cytochrome p450 interactions. J. Pain Symptom Manag. 2012, 44, S4–S14. [Google Scholar] [CrossRef] [PubMed]
- Mura, E.; Govoni, S.; Racchi, M.; Carossa, V.; Ranzani, G.N.; Allegri, M.; van Schaik, R.H. Consequences of the 118A>G polymorphism in the OPRM1 gene: Translation from bench to bedside? J. Pain Res. 2013, 6, 331–353. [Google Scholar] [CrossRef] [PubMed]
- Al-Quliti, K.W.; Assaedi, E.S. New advances in prevention of migraine. Review of current practice and recent advances. Neurosciences 2016, 21, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Eising, E.; de Vries, B.; Vijfhuizen, L.S.; International Headache Genetics Consortium; Anttila, V.; Winsvold, B.S.; Kurth, T.; Stefansson, H.; Kallela, M.; et al. Gene-based pleiotropy across migraine with aura and migraine without aura patient groups. Cephalalgia 2016, 36, 648–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedin-Do, A.; Pouriamanesh, S.; Kamaliyan, Z.; Mirfakhraie, R. Angiotensin-converting enzyme gene rs4343 polymorphism increases susceptibility to migraine. CNS Neurosci. Ther. 2017, 23, 698–699. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Kantorovich, S.; Lee, C.; Anand, N.; Blanchard, J.; Fung, E.T.; Meshkin, B.; Brenton, A.; Richeimer, S. An observational study of the impact of genetic testing for pain perception in the clinical management of chronic non-cancer pain. J. Psychiatr. Res. 2017, 89, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Tong, J.; Hu, J.; Zhang, H.; Ouyang, W.; Huang, D.; Tang, Q.; Liao, Q. COMT gene haplotypes are closely associated with postoperative fentanyl dose in patients. Anesth. Analg. 2015, 120, 933–940. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, K.K.; McNally, B.A.; Linder, M.W. Clinical Utility and Economic Impact of CYP2D6 Genotyping. Clin. Lab. Med. 2016, 36, 525–542. [Google Scholar] [CrossRef] [PubMed]
- Bank, P.C.D.; Caudle, K.E.; Swen, J.J.; Gammal, R.S.; Whirl-Carrillo, M.; Klein, T.E.; Relling, M.V.; Guchelaar, H.J. Comparison of the Guidelines of the Clinical Pharmacogenetics Implementation Consortium and the Dutch Pharmacogenetics Working Group. Clin. Pharmacol. Ther. 2018, 103, 599–618. [Google Scholar] [CrossRef] [PubMed]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Perrot, S.; Javier, R.M.; Marty, M.; Le Jeunne, C.; Laroche, F.; CEDR (Cercle d’Etude de la Douleur en Rhumatologie France), French Rheumatological Society, Pain Study Section. Is there any evidence to support the use of anti-depressants in painful rheumatological conditions? Systematic review of pharmacological and clinical studies. Rheumatology 2008, 47, 1117–1123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, L. Propafenone Therapy and CYP2D6 Genotype. In Medical Genetics Summaries; Pratt, V., McLeod, H., Dean, L., Malheiro, A., Rubinstein, W., Eds.; National Center for Biotechnology Information (US): Bethesda, MD, USA, 2012. [Google Scholar]
- Gardiner, S.J.; Begg, E.J. Pharmacogenetics, drug-metabolizing enzymes, and clinical practice. Pharmacol. Rev. 2006, 58, 521–590. [Google Scholar] [CrossRef] [PubMed]
- Gillman, P.K. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br. J. Pharmacol. 2007, 151, 737–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuilleumier, P.H.; Stamer, U.M.; Landau, R. Pharmacogenomic considerations in opioid analgesia. Pharmgenom. Pers. Med. 2012, 5, 73–87. [Google Scholar]
- Yang, Y.; Botton, M.R.; Scott, E.R.; Scott, S.A. Sequencing the CYP2D6 gene: From variant allele discovery to clinical pharmacogenetic testing. Pharmacogenomics 2017, 18, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Elliott, L.S.; Henderson, J.C.; Neradilek, M.B.; Moyer, N.A.; Ashcraft, K.C.; Thirumaran, R.K. Clinical impact of pharmacogenetic profiling with a clinical decision support tool in polypharmacy home health patients: A prospective pilot randomized controlled trial. PLoS ONE 2017, 12, e0170905. [Google Scholar] [CrossRef] [PubMed]
- Seth, P.; Rudd, R.A.; Noonan, R.K.; Haegerich, T.M. Quantifying the Epidemic of Prescription Opioid Overdose Deaths. Am. J. Public Health 2018, 108, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Zanger, U.M.; Klein, K. Pharmacogenetics of cytochrome P450 2B6 (CYP2B6): Advances on polymorphisms, mechanisms, and clinical relevance. Front. Genet. 2013, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Kharasch, E.D.; Regina, K.J.; Blood, J.; Friedel, C. Methadone Pharmacogenetics: CYP2B6 Polymorphisms Determine Plasma Concentrations, Clearance, and Metabolism. Anesthesiology 2015, 123, 1142–1153. [Google Scholar] [CrossRef] [PubMed]
- Christoffersen, D.J.; Damkier, P.; Feddersen, S.; Moller, S.; Thomsen, J.L.; Brasch-Andersen, C.; Brosen, K. The ABCB1, rs9282564, AG and TT Genotypes and the COMT, rs4680, AA Genotype are Less Frequent in Deceased Patients with Opioid Addiction than in Living Patients with Opioid Addiction. Basic Clin. Pharmacol. Toxicol. 2016, 119, 381–388. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Chronic Pain Type | References | Receptors and Mediator Channels Involved in Disease Susceptibility | Pharmacogenomics of Pain Medications | Possible Clinical Implications | Associated Population |
|---|---|---|---|---|---|
| Fibromyalgia | [8,9,10,13,14] | - COMT-Val15Met (rs4680) - COMT-Vall5Met (rs4818) and (rs4633) - DRD4 - MAO-A - β-2 adrenergic receptor - GTPCH (GABA) A receptor, - GABRB3 - Sodium channel NaV1.7 (SCN9A) - APOE - MYT1L - NRXN3 - MTHFR C677T | - Duloxetine metabolism through CYP2D6, CYP2C9, and predominantly CYP1A2 - Amitriptyline metabolism into nortriptyline (through CYP2C19), and hydroxyl (through CYP2D6) | - Avoid co-administration of duloxetine with a CYP2D6 substrate (e.g., risperidone, aripiprazole, metoprolol, etc.) due to potential increases in toxic levels of the substrates | - Brazilian, Spanish, Turkish, and Israeli Val15Met (rs4680) - Korean (COMT–SNP rs4818 and rs4633) |
| Chronic Low Back Pain | [15,16,17,18,19,20] | - OPMR1-SNPs A118G (rs1799971) - Gln326 to Trp - Arg103 to Trp - COMT SNPs rs4680 - COMT-CG for rs165656 and CT for rs4633 - CASP9 - Elevated levels of GDF5 - VNTR in the chondroitin sulfate-1 encoding domain of the ACAN - Matrix metalloproteinase SNPs | - NSAIDs metabolism through CYP2C9 (increased risk for adverse effects) - Opioids metabolism through CYP2D6 and CYP3A4 (an increased risk for adverse effects in UM, and decreased analgesic efficacy in PM) - Poor Oxycodone analgesic in OPRM1 rs589046, and OPRM1 rs563649 | - Pain perception assessment - CYP2D6 genotyping based on scores for level of evidence and clinical relevance - Genotyping for Methadone treatment initiation - Genotyping for at risk for addiction population | - Finish (Gln326 to Trp) |
| Migraine | [21,22,23,24,25,26,27] | - EDNRA - encoding MTHFR - encoding NOS3 - encoding ACE - encoding TGFB2 - encoding TGFBR2 - NOTCH3 - ESR1 rs1801132 (325C>G) - ESR1 rs2228480 (594G>A) - ESR1 rs2234693 - 5,10-MTHFR C677T (rs1801133), A1298C (rs1801131) - NNMT | - Rs2274316-nominally lower effect of β-blocker in migraine only (MO) - Angiotensin II receptor-antagonists—lower effect for migraine typical aura (MTA) ± migraine without aura (MO) patients with rs11172113 | - Individualized prophylactic treatment | - Spanish (ESR1 rs1801132 (325C>G) - Australian (ESR1 rs2228480 (594G>A) - Chinese (ESR1 rs2234693) |
| Diabetic Painful Peripheral Neuropathy | [28,29,30] | Genetic variants of Nav1.7 | - Duloxetine metabolism through CYP2D6, CYP2C9, and predominantly CYP1A2 - Amitriptyline metabolism through nortriptyline (CYP2C19), and hydroxyl (CYP2D6) | - Correction of modifiable risk factors - Management of hyperglycemia - Avoid co-administration of duloxetine with a CYP2D6 substrate (e.g., risperidone, aripiprazole, metoprolol, etc.) due to potential increase to toxic levels of the substrates | - Males (Chr8p23.1 at rs6986153) - Females (rs71647933) - DPN-males—30% more compared to Females |
| Trigeminal Neuralgia | [31] | Serotonin transporter gene (5-HTT)-linked polymorphic Region (5-HTTLPR) | Association between poor carbamazepine response and 5-HTTLPR polymorphisms | - Reassess poor carbamazepine therapeutic response | - Chinese (5-HTTLPR) |
| Condition | Reference | Number of the Evaluated SNPs and Pathway | Aim | Significant SNPs |
|---|---|---|---|---|
| Fibromyalgia | [8] | TRPV2 gene 3 positions [rs3813768 (C>G), rs8121 (C>T), rs1129235 (C>A)] TRPV3 gene 2 positions [rs7216486 (G>A) and rs395357 (C>T)] | Polymorphisms of the TRPV2 and TRPV3 genes associated with fibromyalgia in a Korean population. | Rs395357 associated with symptom severity |
| Fibromyalgia | [10] | 4 SNPs: rs6269, rs4633, rs4818 and rs4680 or Val158Met identified haplotypes designated as low (LPS), average (APS) and high pain sensitivity (HPS) | Pain sensitivity in fibromyalgia is associated with catechol-O-methyltransferase (COMT) gene | Met/Met genotype (Val158Met SNP)-increased pain sensitivity |
| Low Back Pain | [15] | A118G on the OPRM1 gene | Association of mu-opioid receptor gene polymorphisms (A118G) with variations in morphine consumption for analgesia after total knee arthroplasty. | G118 (GG) associated with significant morphine consumption |
| Low Back Pain | [19] | COMT Val158Met SNP | The COMT rs4680 Met allele contributes to long-lasting low back pain, sciatica and disability after lumbar disc herniation. | Met/Met genotype (Val158Met) was associated with significantly more pain compared to Val/Met and Val/Val |
| Pain perception assessment | [52] | rs6269, rs4633, rs4818, rs4680 | COMT gene haplotypes are closely associated with postoperative fentanyl dose in patients. | COMT gene haplotype ACCG associated with significant fentanyl consumption |
| Methadone initiative assessment | [65] | CYP2B6*1/*1 (n = 21), CYP2B6*1/*6 (n = 20), CYP2B6*6/*6 (n = 17), CYP2B6*1/*4 (n = 1), CYP2B6*4/*6 (n = 3), CYP2B6*5/*5 (n = 2) | Methadone Pharmacogenetics: CYP2B6 Polymorphisms determine plasma concentrations, clearance and metabolism. | CYP2B6*6-decreased metabolism and clearance in African-Americans |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knezevic, N.N.; Tverdohleb, T.; Knezevic, I.; Candido, K.D. The Role of Genetic Polymorphisms in Chronic Pain Patients. Int. J. Mol. Sci. 2018, 19, 1707. https://doi.org/10.3390/ijms19061707
Knezevic NN, Tverdohleb T, Knezevic I, Candido KD. The Role of Genetic Polymorphisms in Chronic Pain Patients. International Journal of Molecular Sciences. 2018; 19(6):1707. https://doi.org/10.3390/ijms19061707
Chicago/Turabian StyleKnezevic, Nebojsa Nick, Tatiana Tverdohleb, Ivana Knezevic, and Kenneth D. Candido. 2018. "The Role of Genetic Polymorphisms in Chronic Pain Patients" International Journal of Molecular Sciences 19, no. 6: 1707. https://doi.org/10.3390/ijms19061707
APA StyleKnezevic, N. N., Tverdohleb, T., Knezevic, I., & Candido, K. D. (2018). The Role of Genetic Polymorphisms in Chronic Pain Patients. International Journal of Molecular Sciences, 19(6), 1707. https://doi.org/10.3390/ijms19061707