The Efficacy of Buprenorphine in Major Depression, Treatment-Resistant Depression and Suicidal Behavior: A Systematic Review

 ,
, 
 ,
,  ,
,
Abstract
:1. Introduction
1.1. The Impact of Major Depression and Treatment Resistant Depression Worldwide
1.2. Psychoacvtive Treatments for Major Affective Disorders: A Brief Overview
1.3. The Potential of Buprenorphine
2. Results
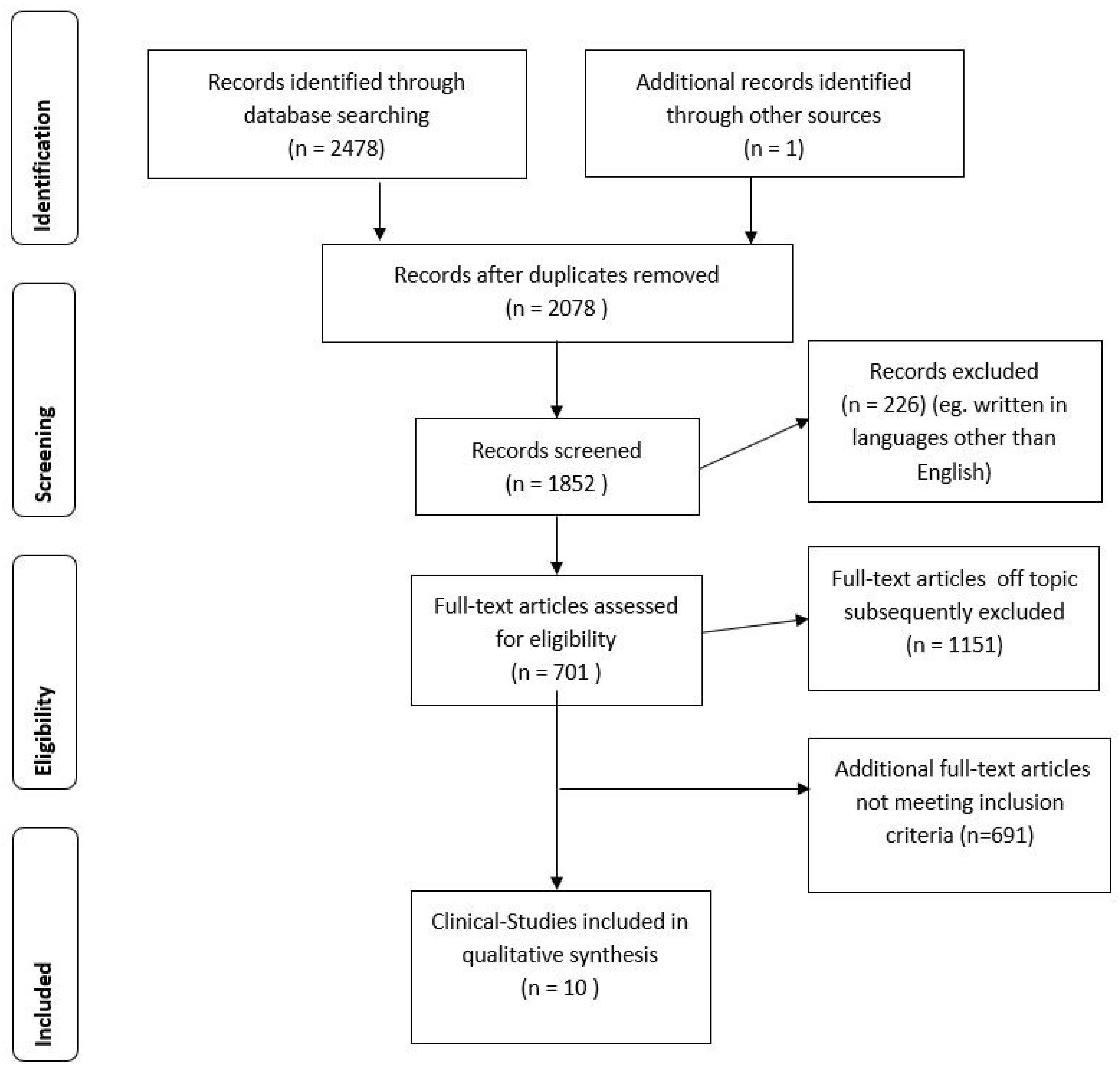
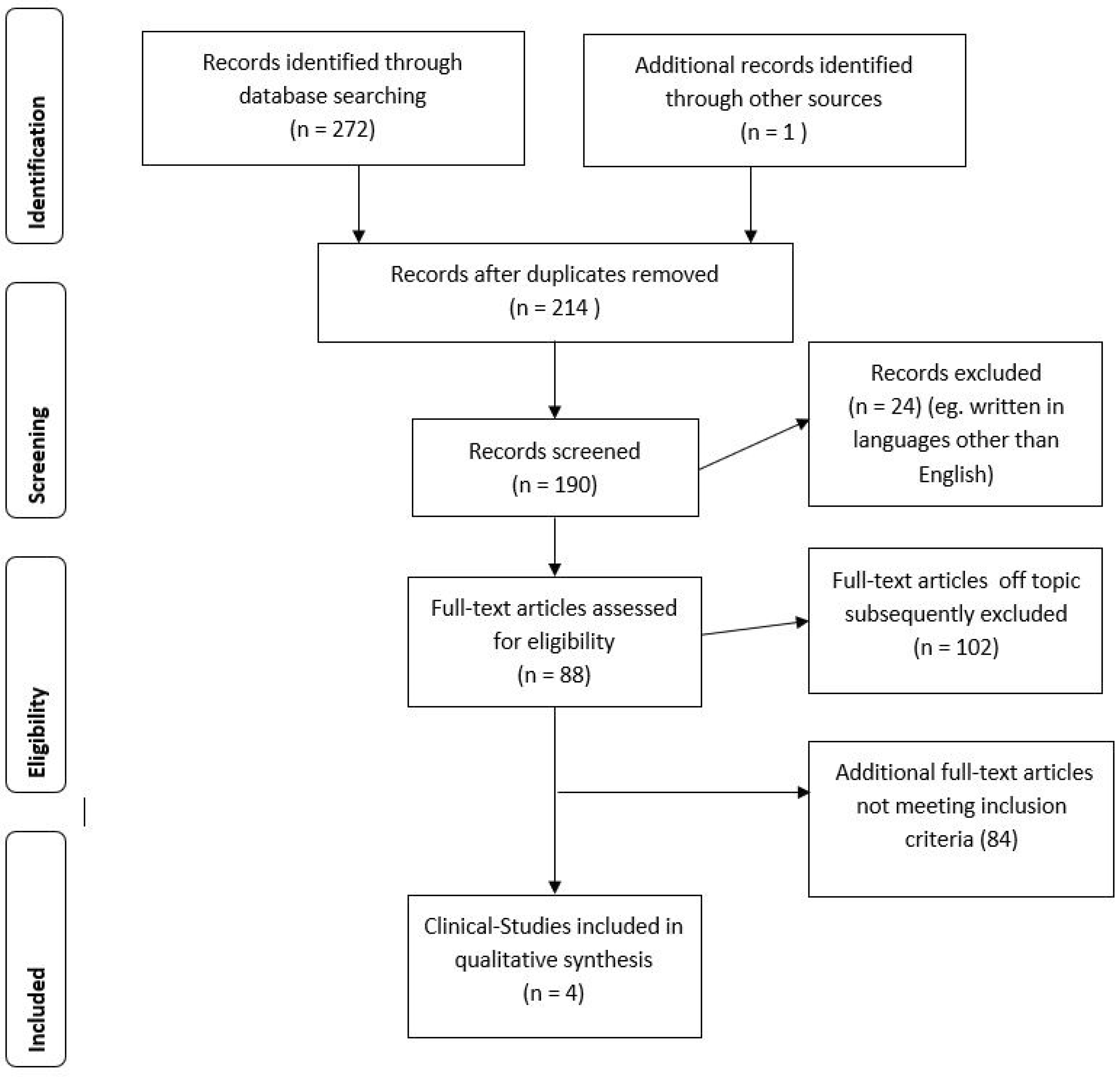
2.1. Study Sample
2.2. Study Types and Sample Characteristics
2.3. Study Quality Assessment
2.4. Studies Description
3. Discussion
3.1. Summary of Main Findings
3.2. Main Shortcomings/Limitations
4. Materials and Methods
4.1. Eligibility Criteria
4.2. Information Sources
4.3. Search Terms
4.4. Selection of Studies
4.5. Data Collection Process
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2015 disease and injury incidence and prevalence collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Fava, M.; Davidson, K.G. Definition and epidemiology of treatment-resistant depression. Psychiatr. Clin. N. Am. 1996, 19, 179–200. [Google Scholar] [CrossRef]
- Valenstein, M. Keeping our eyes on STAR*D. Am. J. Psychiatry 2006, 163, 1484–1486. [Google Scholar] [CrossRef] [PubMed]
- Dunner, D.L.; Rush, A.J.; Russell, J.M.; Burke, M.; Woodard, S.; Wingard, P.; Allen, J. Prospective, long-term, multicenter study of the naturalistic outcomes of patients with treatment-resistant depression. J. Clin. Psychiatry 2006, 67, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Nebbia, J.; Cipriani, N.; Conigliaro, C.; Erbuto, D.; Pompili, M.; Amore, M. Number of illness episodes as predictor of residual symptoms in major depressive disorder. Psychiatry Res. 2018, 262, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Howland, R.H.; Rovedi, F.; Girardi, P.; Amore, M. The role of ketamine in treatment-resistant depression: A systematic review. Curr. Neuropharmacol. 2014, 12, 444–461. [Google Scholar] [CrossRef] [PubMed]
- Sibille, E.; French, B. Biological substrates underpinning diagnosis of major depression. Int. J. Neuropsychopharmacol. 2013, 16, 1893–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fekadu, A.; Wooderson, S.C.; Rane, L.J.; Markopoulou, K.; Poon, L.; Cleare, A.J. Long-term impact of residual symptoms in treatment-resistant depression. Can. J. Psychiatry 2011, 56, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Thase, M.E. Achieving remission and managing relapse in depression. J. Clin. Psychiatry 2003, 64, 3–7. [Google Scholar] [PubMed]
- Harris, E.C.; Barraclough, B. Suicide as an outcome for mental disorders. A meta-analysis. Br. J. Psychiatry 1997, 170, 205–228. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Nonsuicidal self-injury. In American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013; pp. 783–808. [Google Scholar]
- Moscicki, E.K.; Carroll, P.; Rae, D.S.; Locke, B.Z.; Roy, A.; Regier, D.A. Suicide attempts in the epidemiologic catchment area study. Yale J. Biol. Med. 1988, 61, 259–268. [Google Scholar] [PubMed]
- Jacobson, C.M.; Gould, M. The epidemiology and phenomenology of non-suicidal self-injurious behavior among adolescents: A critical review of the literature. Arch. Suicide Res. 2007, 11, 129–147. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.S.; Ostroff, R.B.; Hoffman, R.E. Naltrexone as a treatment for repetitive self-injurious behaviour: An open-label trial. J. Clin. Psychiatry 1996, 57, 233–237. [Google Scholar] [PubMed]
- Tenore, P.L. Psychotherapeutic benefits of opioid agonist therapy. J. Addict. Dis. 2008, 27, 49–65. [Google Scholar] [CrossRef] [PubMed]
- Badiani, A. Encyclopedia of Psychopharmacology; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Anderson, I.M.; Ferrier, I.N.; Baldwin, R.C.; Cowen, P.J.; Howard, L.; Lewis, G.; Matthews, K.; McCallister-Williams, R.H.; Peveler, R.C.; Scott, J.; et al. Evidence-based guidelines for treating depressive disorders with antidepressants: A revision of the 2000 British association for psychopharmacology guidelines. J. Psychopharmacol. 2008, 22, 343–396. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence (NICE). Depression in Adults: Recognition and Management; CG90; NICE: London, UK, 2009. [Google Scholar]
- Trivedi, M.H.; Rush, A.J.; Wisniewski, S.R.; Nierenberg, A.A.; Warden, D.; Ritz, L.; Norquist, G.; Howland, R.H.; Lebowitz, B.; McGrath, P.J. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: Implications for clinical practice. Am. J. Psychiatry 2006, 163, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Jordan, M.R.; Morrisonponce, D. Naloxone. In Treasure Island (FL): Stat Pearls; U.S. National Library of Medicine: Bethesda, MD, USA, 2018. [Google Scholar]
- Turncliff, R.; Di Petrillo, L.; Silverman, B.; Ehrich, E. Single- and multiple-dose pharmacokinetics of samidorphan, a novel opioid antagonist, in healthy volunteers. Clin. Ther. 2015, 37, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Bodnar, R.J. Endogenous opiates and behavior: 2010. Peptides 2011, 32, 2522–2552. [Google Scholar] [CrossRef] [PubMed]
- Knoll, A.T.; Carlezon, W.A., Jr. Dynorphin, stress, and depression. Brain Res. 2010, 1314, 56–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherrer, J.F.; Svrakic, D.M.; Freedland, K.E.; Chrusciel, T.; Balasubramanian, S.; Bucholz, K.K.; Lawler, E.V.; Lustman, P.J. Prescription opioid analgesics increase the risk of depression. J. Gen. Intern. Med. 2014, 29, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Le Merrer, J.; Becker, J.A.; Befort, K.; Kieffer, B.L. Reward processing by the opioid system in the brain. Physiol. Rev. 2009, 89, 1379–1412. [Google Scholar] [CrossRef] [PubMed]
- Berrocoso, E.; Sánchez-Blázquez, P.; Garzón, J.; Mico, J.A. Opiates as antidepressants. Curr. Pharm. Des. 2009, 15, 1612–1622. [Google Scholar] [CrossRef] [PubMed]
- Eisch, A.J.; Harburg, G.C. Opiates, psychostimulants, and adult hippocampal neurogenesis: Inshights for addiction and stem cell biology. Hippocampus 2006, 16, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Lutz, P.E.; Kieffer, B.L. Opioid receptors: Distinct roles in mood disorders. Trends Neurosci. 2013, 36, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Tao, R.; Auerbach, S.B. Involvement of the dorsal raphe but not median raphe nucleus in morphine-induced increases in serotonin release in the rat forebrain. Neuroscience 1995, 68, 553–561. [Google Scholar] [CrossRef]
- Delfs, J.M.; Zhu, Y.; Druhan, J.P.; Aston-Jones, G. Noradrenaline in the ventral forebrain is critical for opiate withdrawal-induced aversion. Nature 2000, 403, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Filliol, D.; Ghozland, S.; Chluba, J.; Martin, M.; Matthes, H.W.; Simonin, F.; Befort, K.; Gavériaux-Ruff, C.; Dierich, A.; LeMeur, M.; et al. Mice deficient for delta- and mu-opioid receptors exhibit opposing alterations of emotional responses. Nat. Genet. 2000, 25, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.A.; Befort, K.; Nozaki, C.; Gavériaux-Ruff, C.; Kieffer, B.L. The delta opioid receptor: An evolving target for the treatment of brain disorders. Trends Pharmacol. Sci. 2011, 32, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Wee, S.; Koob, G.F. The role of the dynorphin-κ opioid system in the reinforcing effects of drugs of abuse. Psychopharmacology 2010, 210, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Khroyan, T.V.; Wu, J.; Polgar, W.E.; Cami-Kobeci, G.; Fotaki, N.; Husbands, S.M.; Toll, L. BU08073 a buprenorphine analogue with partial agonist activity at μ-receptors in vitro but long-lasting opioid antagonist activity in vivo in mice. Br. J. Pharmacol. 2015, 172, 668–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlman, J.J., Jr.; Lalani, S.; Magluilo, J., Jr.; Levine, B.; Darwin, W.D. Human pharmacokinetics of intravenous, sublingual, and buccal buprenorphine. J. Anal. Toxicol. 1996, 20, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Elkader, A.; Sproule, B. Buprenorphine: Clinical pharmacokinetics in the treatment of opioid dependence. Clin. Pharmacokinect. 2005, 44, 661–680. [Google Scholar] [CrossRef] [PubMed]
- Picard, N.; Cresteil, T.; Djebli, N.; Marquet, P. In vitro metabolism study of buprenorphine: Evidence for new metabolic pathways. Drug Metab. Dispos. 2005, 33, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Cone, E.J.; Gorodetzky, C.W.; Yousefnejad, D.; Buchwald, W.F.; Johnson, R.E. The metabolism and excretion of buprenorphine in humans. Drug Metab. Dispos. 1984, 12, 577–581. [Google Scholar] [PubMed]
- Sher, L. Buprenorphine and the treatment of depression, anxiety, non-suicidal self-injury, and suicidality. Acta Psychiatr. Scand. 2016, 134, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Emrich, H.M.; Vogt, P.; Her, A. Possible antidepressive effects of opioids: Action of buprenorphine. Ann. N. Y. Acad. Sci. 1982, 398, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Bodkin, J.A.; Zornberg, G.L.; Scott, L.E.; Cole, J.O. Buprenorphine treatment of refractory depression. J. Clin. Psychopharmacol. 1995, 15, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Karp, J.F.; Butters, M.A.; Begley, A.; Miller, M.D.; Lenze, E.J.; Blumberger, D.; Mulsant, B.; Reynolds, C.F., III. Safety, tolerability, and clinical effect of low-dose buprenorphine for treatment-resistant depression in mid-life and older adults. J. Clin. Psychiatry 2014, 75, e785–e793. [Google Scholar] [CrossRef] [PubMed]
- Ehrich, E.; Turncliff, R.; Du, Y.; Leigh-Pemberton, R.; Fernandez, E.; Jones, R.; Fava, M. Evaluation of opioid modulation in major depressive disorder. Neuropsychopharmacology 2015, 40, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Fava, M.; Memisoglu, A.; Thase, M.E.; Bodkin, J.A.; Trivedi, M.H.; de Somer, M.; Du, Y.; Leigh-Pemberton, R.; DiPetrillo, L.; Silverman, B.; et al. Opioid modulation with buprenorphine/samidorphan as adjunctive treatment for inadequate response to antidepressants: A randomized double-blind placebo-controlled trial. Am. J. Psychiatry 2016, 173, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Nyhuis, P.W.; Gastpar, M.; Scherbaum, N. Opiate treatment in depression refractory to antidepressants and electroconvulsive therapy. J. Clin. Psychopharmacol. 2008, 28, 593–595. [Google Scholar] [CrossRef] [PubMed]
- Striebel, J.M.; Kalapatapu, R.K. The anti-suicidal potential of buprenorphine: A case report. Int. J. Psychiatry Med. 2014, 47, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Kosten, T.R.; Morgan, C.; Kosten, T.A. Depressive symptoms during buprenorphine treatment of opioid abusers. J. Subst. Abuse Treat. 1990, 7, 51–54. [Google Scholar] [CrossRef]
- Dean, A.J.; Bell, J.; Christie, M.J.; Mattick, R.P. Depressive symptoms during buprenorphine vs. methadone maintenance: Findings from a randomised, controlled trial in opioid dependence. Eur. Psychiatry 2004, 19, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Gerra, G.; Fantoma, A.; Zaimovic, A. Naltrexone and buprenorphine combination in the treatment of opioid dependence. J. Psychopharmacol. 2006, 20, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Yovell, Y.; Bar, G.; Mashiah, M.; Baruch, Y.; Briskman, I.; Asherov, J.; Lotan, A.; Rigbi, A.; Panksepp, J. Ultra-low-dose buprenorphine as a time-limited treatment for severe suicidal ideation: A randomized controlled trial. Am. J. Psychiatry 2016, 173, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, J.; Abtahi, S. Eight-milligram single dose of buprenorphine as an expeditious treatment for severe suicidal ideation: A case report. Iran. Red Crescent Med. J. 2017, 19. [Google Scholar] [CrossRef]
- Norelli, L.J.; Smith, H.S.; Sher, L.; Blackwood, T.A. Buprenorphine in the treatment of non-suicidal self-injury: A case series and discussion of the literature. Int. J. Adolesc. Med. Health 2013, 25, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Gabilondo, A.M.; Meana, J.J.; Garcia-Sevilla, J.A. Increased density of m-opioid receptors in the postmortem brain of suicide victims. Brain Res. 1995, 682, 245–250. [Google Scholar] [CrossRef]
- Dilsaver, S.C. The pathophysiologies of substance abuse and affective disorders: An integrative model? J. Clin. Psychopharmacol. 1987, 7, 1–10. [Google Scholar] [PubMed]
- Leander, J.D. Buprenorphine has potent kappa opioid receptor antagonist activity. Neuropharmacology 1987, 26, 1445–1447. [Google Scholar] [CrossRef]
- Panksepp, J.; Watt, D. Why does depression hurt? Ancestral primary process separation-distress (PANIC/GRIEF) and diminished brain reward (SEEKING) processes in the genesis of depressive affect. Psychiatry 2011, 74, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Ballard, E.D.; Ionescu, D.F.; Vande Voort, J.L.; Niciu, M.J.; Richards, E.M.; Luckenbaugh, D.A.; Brutsché, N.E.; Ameli, R.; Furey, M.L.; Zarate, C.A., Jr. Improvement in suicidal ideation after ketamine infusion: Relationship to reductions in depression and anxiety. J. Psychiatr. Res. 2014, 58, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belenky, G.L.; Holaday, J.W. The opiate antagonist naloxone modifies the effects of electroconvulsive shock (ECS) on respiration, blood pressure and heart rate. Brain Res. 1979, 177, 414–417. [Google Scholar] [CrossRef]
- Raskin, J.; Wiltse, C.G.; Siegal, A.; Sheikh, J.; Xu, J.; Dinkel, J.J.; Rotz, B.T.; Mohs, R.C. Efficacy of duloxetine on cognition, depression, and pain in elderly patients with major depressive disorder: An 8-week, double-blind, placebo-controlled trial. Am. J. Psychiatry 2007, 164, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.L.; Byas-Smith, M.G.; Reed, B.A. Effects of intermediate- and long-term use of opioids on cognition in patients with chronic pain. Clin. J. Pain 2002, 18, S83–S90. [Google Scholar] [CrossRef] [PubMed]
- Dagtekin, O.; Gerbershagen, H.J.; Wagner, W.; Petzke, F.; Radbruch, L.; Sabatowski, R. Assessing cognitive and psychomotor performance under long-term treatment with transdermal buprenorphine in chronic noncancer pain patients. Anesth. Analg. 2007, 105, 1442–1448. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Control Group | Diagnosis | Study Design | Sample | Treatment | Psychometric Instruments | Inter-Reliability Test | Limitations | Main Conclusions | Statistical Analyses | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Norelli et al., 2013 [53] | No | Treatment resistant NSSI | Case-report | 6 adults | Personalized doses of buprenorphine. | No instruments were used for different amounts of time | No | Short duration of the clinical study; small number of the evaluated subjects; lack of control group; exiguity of the experimental group; lack of exclusion criteria. | Five patients had a significant reduction in total incidents, seclusion and restraint episodes, NSSI and improved mood states. One patient had not statistically significant changes. | A comparison was made between the mean monthly number of overall incidents, NSSI episodes, and S/R episodes without buprenorphine treatment, and the average number with buprenorphine treatment. A t-test comparison was used to determine the significance of the differences between these two data sets. A t-value was calculated for the overall combined data from all patients, and each individual patient in the study. A t-value was calculated by dividing the overall increase or decrease from the baseline over the standard deviation of post-treatment data divided by the square root of the number of post-treatment data points. | I = 0; II = 0 III = 2; IV = 0 V = 0; VI = 0 Total score = 2 |
| Striebel and Kalapatapu, 2014 [47] | No | Chronic suicidal ideation; TRD; Chronic back pain; Opioid dependence | Case-report | 1 adult | 16/4 mg of buprenorphine/naloxone; 3 month. | No instruments were used | No | Small number of the evaluated subjects; lack of control group; lack of exclusion criteria; lack of standardized measures. | The patient showed a reduction and cessation of suicidal thoughts and depression and a decrease of pain. | - | I = 0; II = 0 III = 1; IV = 0 V = 0; VI = 0 Total score = 1 |
| Ahmadi et al., 2017 [52] | No | Chronic suicidal ideation due to substance-induced depressive disorder | Case-report | 25-year old man | 8-mg single dose of sublingual buprenorphine; 10 days. | BSIS; BDI | No | Short duration of the clinical study; small number of the evaluated subjects; lack of control group; exiguity of the experimental group; lack of exclusion criteria. | The patient had a rapid reduction and cessation of suicidal thoughts and depression. | - | I = 0; II = 0 III = 1; IV = 2 V = 0; VI = 0 Total score = 3 |
| Reference | Control Group | Diagnosis | Study Design | Sample | Treatment | Psychometric Instruments | Inter-Reliability Test | Limitations | Main Conclusions | Statistical Analyses | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kosten et al., 1990 [48] | No | Opioid addiction | Observational prospective study | 40 adults | Buprenorphine 3.2 mg, with a range from 2 to 8 mg; 1 month. | BDI; SDS | No | Short duration of the clinical study; lack of control group; exiguity of the experimental group; diagnostic heterogeneity of the study population. Depression was not a primary outcome; self-report measures; lack of control group; short duration of the clinical study. | Depressive patients had a significant reduction in depressive symptoms at the end of the first week; this reduction continued over the second week. Depressive symptoms steadily declined during the month. | ANOVA | I = 2; II = 0 III = 1; IV = 1 V = 0; VI = 0 Total score = 2 |
| Gerra et al., 2006 [50] | Yes | Opioid dependence | Controlled observational prospective study | 60 adults | 30 patients: naltrexone alone; 30 patients: naltrexone (50 mg oral dose) plus buprenorphine (4 mg sublingual); 12 weeks. | SCL-90; VAS for craving scores | No | Lack of randomization; lack of placebo buprenorphine control; diagnostic heterogeneity of the study population; lack of psychiatric evaluation at baseline; depression not as the primary outcome; SCL-90 is not specific for depression; lack of exclusion criteria; for psychopathological evaluations only self-report instruments were used; short duration of the clinical study. | Patients in the naltrexone plus buprenorphine group showed a greater reduction in irritability, depression, tiredness, psychosomatic symptoms and craving scores than patients in the naltrexone group. Patients of both groups showed a significant decrease of irritability, depression, tiredness and psychosomatic symptoms scores. | ANOVA; Kaplan-Meier; chi-square test. | I = 2; II = 1 III = 1; IV = 1 V = 0; VI = 0 Total score = 5 |
| Nyhuis et al., 2008 [46] | No | TRD | Observational prospective study | 6 adults | Buprenorphine ranging from 0.8 to 2.0 mg; 7 days. | HAM-D; BDI | No | Short duration of the clinical study; lack of control group; exiguity of the experimental group; lack of exclusion criteria. | All six depressive patients improved over one week; five patients reached a complete remission | - | I = 1; II = 0 III = 1; IV = 2 V = 0; VI = 0 Total score = 4 |
| Reference | Control Group | Diagnosis | Study Design | Sample | Treatment | Psychometric Instruments | Inter-Reliability Test | Limitations | Main Conclusions | Statistical Analyses | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bodkin et al., 1994 [42] | No | TRD | Open label clinical trial, case report | 10 adults | Buprenorphine. Dosage was titrated according to tolerance and clinical benefit, with a maximum daily dosage of 1.8 mg; 4-6 weeks. | HAM-D; ADDS; POMS; GAS | No | Short duration of the clinical study; small number of the evaluated subjects; lack of control group, exiguity of the experimental group. | Patients showed a clinically striking improvement in both subjective and objective measures of depression. Four patients achieved a complete remission of symptoms, two were moderately improved, and one deteriorated. | Paired t-tests. | I = 1; II = 0 III = 1; IV = 2 V = 0; VI = 0 Total score = 4 |
| Karp et al., 2014 [43] | No | TRD | Open label clinical trial | 15 adults aged 50 and older | Buprenorphine (from 0.2 mg to 1.6 mg/day). The average daily dose was 0.40 mg/day; 8 weeks. | MADRS; SCID; BSI-anxiety; the Positive and Negative Affect Scales; SSI; Choice Reaction Time Task Congruous vs. Incongruous Conditions Reaction Time Task; HVLT-R; UKU; FIBSER; SF-26; PSQI; COWS; MMSE | No | Lack of control group; exiguity of the experimental group; lack of randomization; short duration of the clinical study. | Patients exhibited a sharp decline in depression severity during the first 3 weeks, in particular in pessimism and sadness scores. Executive function and learning improved from pre- to post-treatment. | Descriptive analysis; Exact Wilcoxon tests. | I = 1; II = 0 III = 1; IV = 2 V = 0; VI = 0 Total score = 4 |
| Reference | Control Group | Diagnosis | Study Design | Sample | Treatment | Psychometric Instruments | Inter-Reliability Test | Limitations | Main Conclusions | Statistical Analyses | Quality Assessment |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Emrich et al., 1982 [41] | Yes | TRD | Double-blind, placebo-controlled clinical trial | 10 adults | Buprenorphine 2 mg per day; 4–8 days. | HAM-D; IMPS; VBS | No | Short duration of the clinical study; lack of control group; exiguity of the experimental group. | Overall, four patients showed more than 50% reduction in depression, two patients showed a moderate response, and four, a slight reduction. | Wilcoxon-test. | I = 1; II = 1 III = 1; IV = 2 V = 0; VI = 0 Total score = 5 |
| Dean et al., 2004 [49] | Yes | Heroin-dependence | Randomized, double-blind, placebo controlled clinical trial | 147 adults | 68 patients: buprenorphine sublingual tablets and placebo methadone syrup; 79 patients: methadone syrup and placebo buprenorphine tablet. Dosing was initiated at 30 mg methadone or 4 mg buprenorphine; doses were individually titrated to optimize response; 3 months. | BDI | No | Diagnostic heterogeneity of the study population; self-scored questionnaires; lack of psychiatric evaluation at baseline; depression not as the primary outcome; lack of exclusion criteria. | Depressive symptoms improved in all subjects, with no difference between methadone and buprenorphine groups. | t-tests; chi-square tests. Treatment effects data were analyzed using a two-way fixed effects analysis of variance. Outcome predictors were examined using regression analyses. | I = 2; II = 2 III = 1; IV = 1 V = 0; VI = 0 Total score = 6 |
| Ehrich et al., 2015 [44] | Yes | MDD and inadequate response to standard antidepressant therapy (TRD) | Randomized, double-blind, placebo controlled clinical trial | 32 adults | 14 patients: buprenorphine: samidorphan 8:1 dose-ratio; 14 patients: buprenorphine: samidorphan 1:1 dose-ratio; 4 patients: placebo; 1 week. | HAM-D; MADRS; VAS | No | Short duration of the clinical study; small number of the evaluated subjects; VAS not validated in this population; for psychopathological evaluations only self-report instruments were used. | Patients in the 1:1 ratio group in seven days exhibited statistically significant improvement in depressive symptoms; antidepressant effects were greatest in this group. | Descriptive statistics about safety, t-test; Bonferroni adjustment; Exact Wilcoxon tests. | I = 1; II = 1 III = 1; IV = 1 V = 0; VI = 0 Total score = 4 |
| Yovell et al., 2016 [51] | Yes | Clinically significant suicidal ideation | Randomized, double blind, placebo-controlled clinical trial | 88 adults | 57 patients: buprenorphine (0.1 or 0.2 mg/day. Once a week, the daily dose could be raised of 0.1–0.2 mg increments); 31 patients: placebo; 4 weeks. | BSSI; BDI; SPS | No | Self-scored questionnaires; diagnostic heterogeneity of the study population. | Patients in the buprenorphine group had a greater reduction in suicidal ideation, suicide probability and depression scores than patients in placebo group. | Two-sided t tests for continuous variables and Pearson’s chi-square test or Fisher’s exact test, as appropriate, for categorical variables. Correlations were calculated using Pearson’sr. Fisher’s r-to-z transformation was used for testing the difference between correlations. | I = 2; II = 1 III = 1; IV = 1; V = 0; VI = 0 Total score = 5 |
| Fava et al., 2016 [45] | Yes | MDD adults who had an inadequate response to one or two courses of antidepressant treatment (TRD) | Randomized, double-blind, placebo-controlled trial | 142 adults | Buprenorphine/samidorphan 2 mg/2 mg; buprenorphine/samidorphan 8 mg/8 mg; placebo; 4 weeks. | HAM-D; MADRS; CGI-S | Yes | Short duration of the clinical study. | Patients in the 2:2 ratio group, compared with patients in the placebo group, showed significantly greater improvements. There was also evidence of improvement in the 8:8 ratio group although it did not achieve statistical significance. | The primary efficacy endpoint, was evaluated using the weighted combination of statistics from the stage-specific mixed models for repeated measures (MMRM); Kenward-Roger approximation was used to adjust the denominator degrees of freedom. Combined inference was conducted using the weighted linear combination of stage-wise test statistics. | I = 2; II = 2 III = 1; IV = 2 V = 2; VI = 2 Total score = 11 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serafini, G.; Adavastro, G.; Canepa, G.; De Berardis, D.; Valchera, A.; Pompili, M.; Nasrallah, H.; Amore, M. The Efficacy of Buprenorphine in Major Depression, Treatment-Resistant Depression and Suicidal Behavior: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 2410. https://doi.org/10.3390/ijms19082410
Serafini G, Adavastro G, Canepa G, De Berardis D, Valchera A, Pompili M, Nasrallah H, Amore M. The Efficacy of Buprenorphine in Major Depression, Treatment-Resistant Depression and Suicidal Behavior: A Systematic Review. International Journal of Molecular Sciences. 2018; 19(8):2410. https://doi.org/10.3390/ijms19082410
Chicago/Turabian StyleSerafini, Gianluca, Giulia Adavastro, Giovanna Canepa, Domenico De Berardis, Alessandro Valchera, Maurizio Pompili, Henry Nasrallah, and Mario Amore. 2018. "The Efficacy of Buprenorphine in Major Depression, Treatment-Resistant Depression and Suicidal Behavior: A Systematic Review" International Journal of Molecular Sciences 19, no. 8: 2410. https://doi.org/10.3390/ijms19082410
APA StyleSerafini, G., Adavastro, G., Canepa, G., De Berardis, D., Valchera, A., Pompili, M., Nasrallah, H., & Amore, M. (2018). The Efficacy of Buprenorphine in Major Depression, Treatment-Resistant Depression and Suicidal Behavior: A Systematic Review. International Journal of Molecular Sciences, 19(8), 2410. https://doi.org/10.3390/ijms19082410