Oversecretion and Overexpression of Nicotinamide Phosphoribosyltransferase/Pre-B Colony-Enhancing Factor/Visfatin in Inflammatory Bowel Disease Reflects the Disease Activity, Severity of Inflammatory Response and Hypoxia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Circulating Nampt
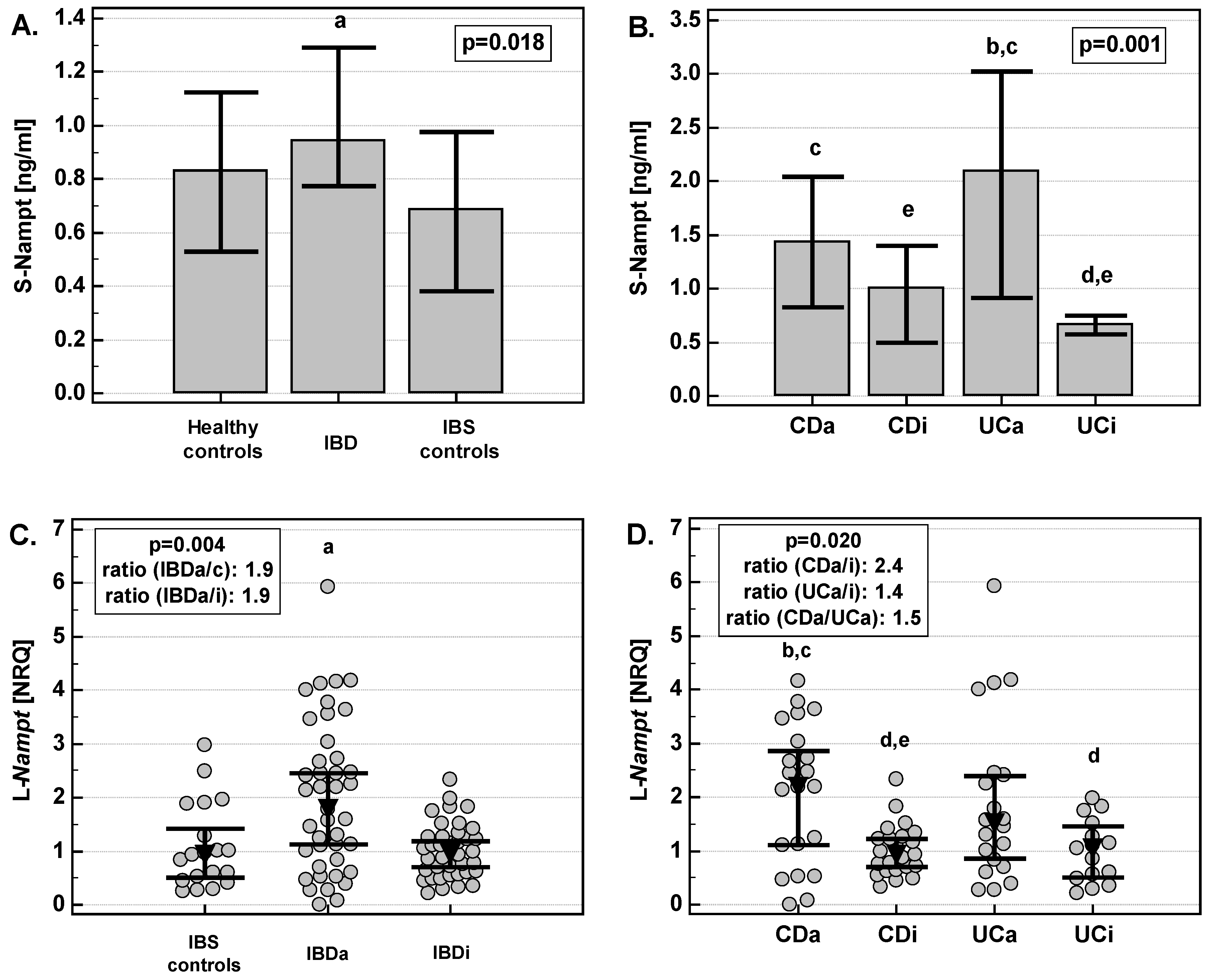
2.1.1. Serum-Nampt (S-Nampt) in IBD
2.1.2. S-Nampt Correlates with Nutritional and Inflammatory Markers
2.1.3. S-Nampt Was More Elevated in UC Patients with Active Disease Treated with Azathioprine (AZA)
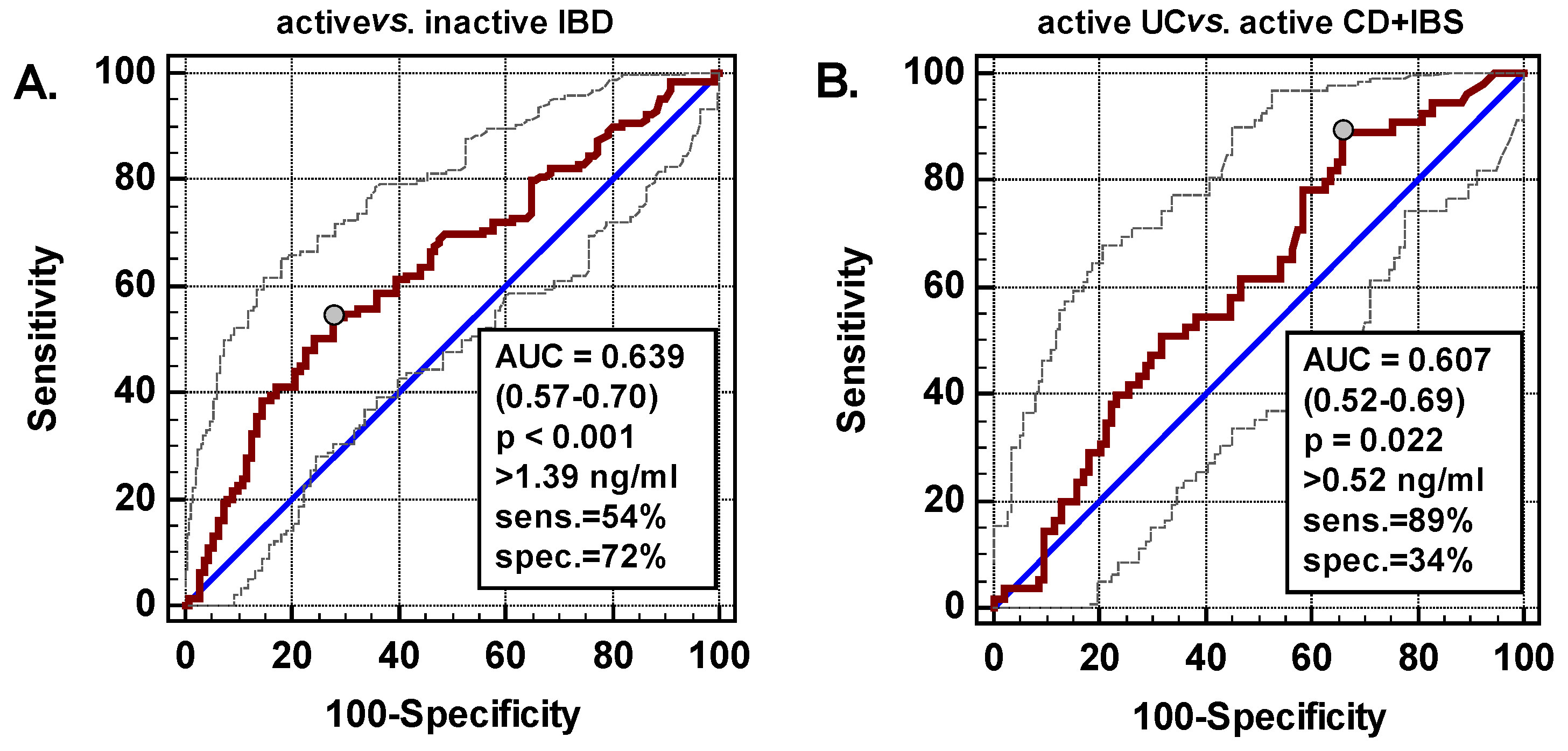
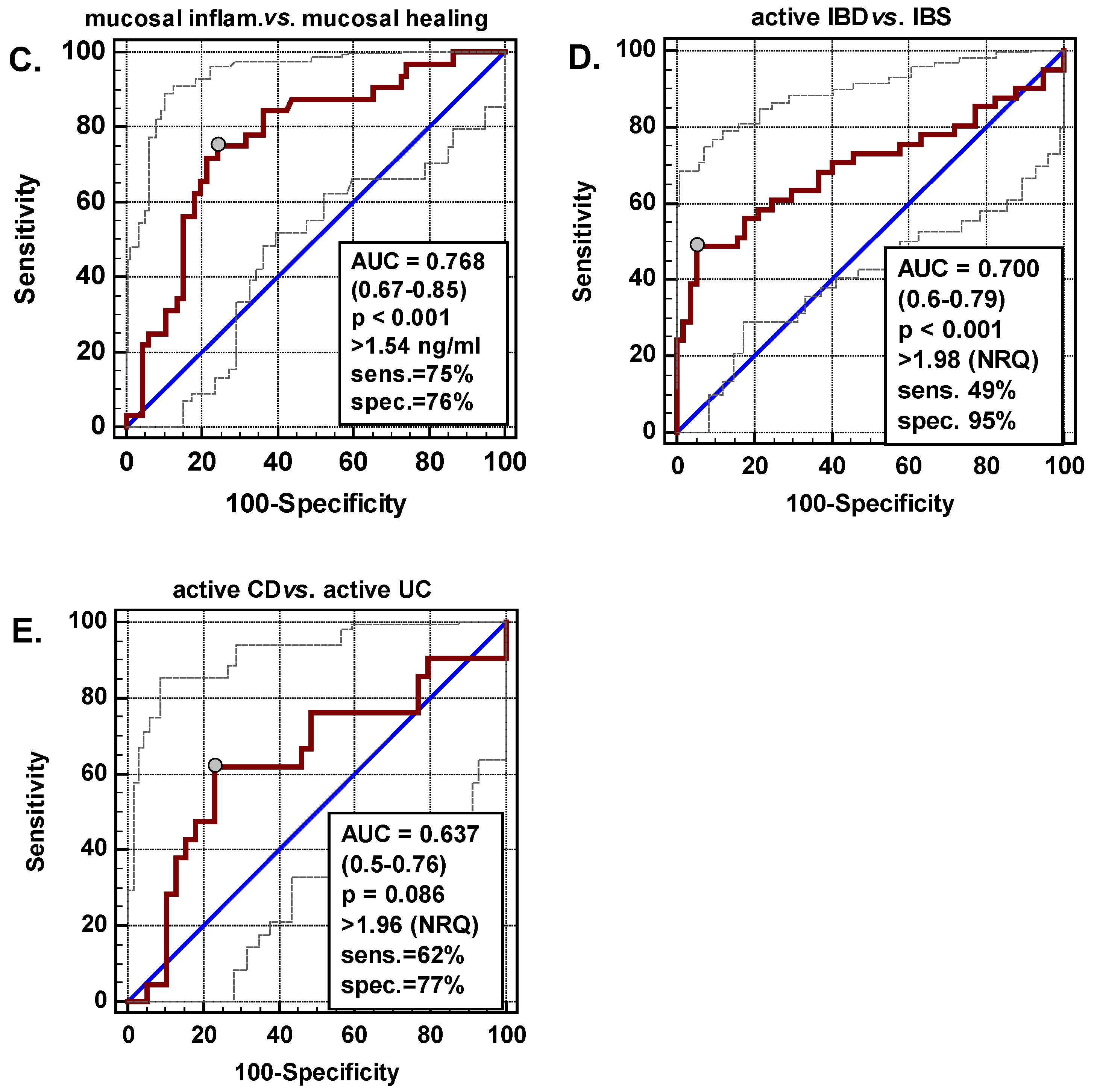
2.1.4. S-Nampt as a Biomarker in IBD
2.2. Leukocyte Expression of Nampt
2.2.1. Leukocyte Nampt (L-Nampt) Expression Is Up-Regulated in Active IBD
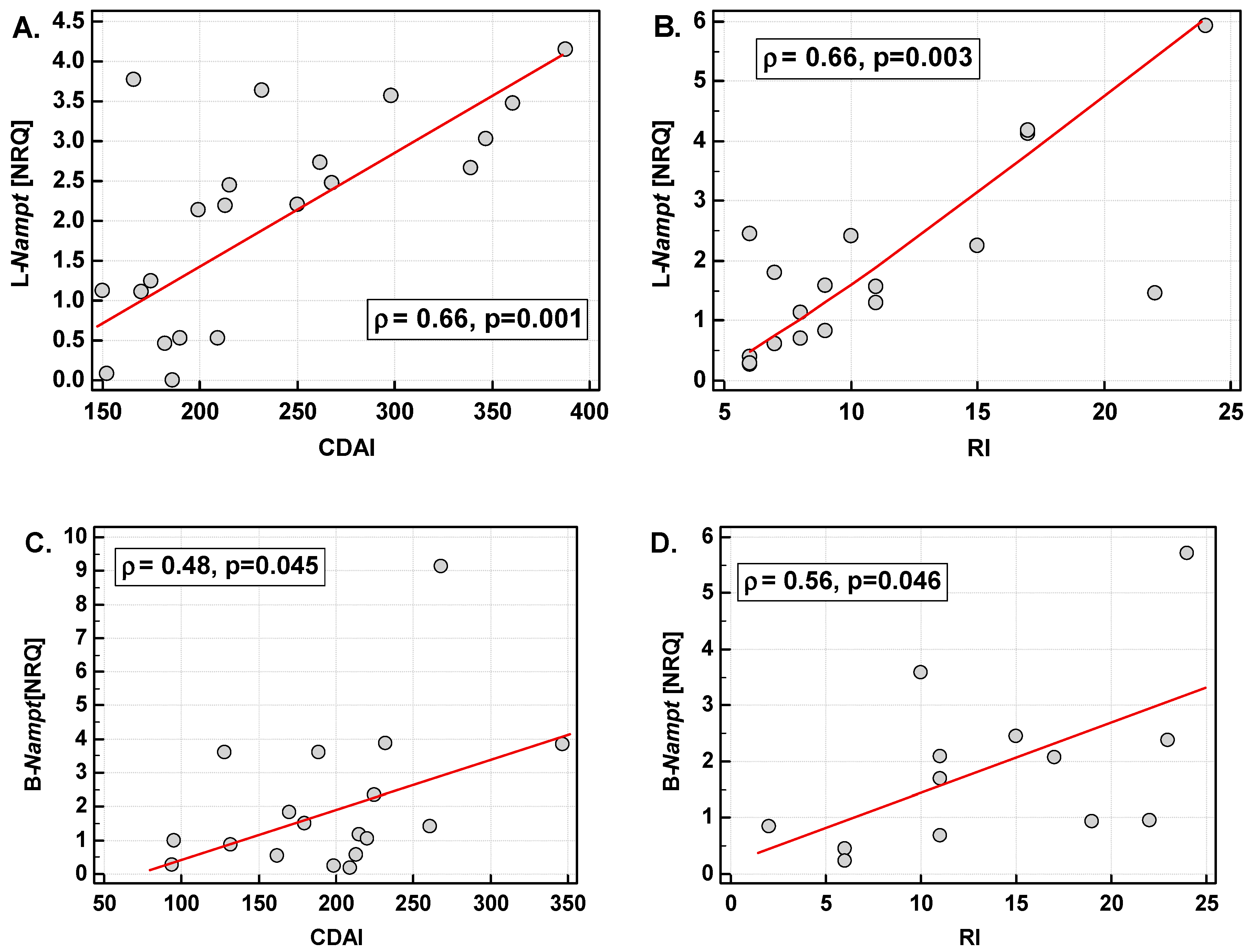
2.2.2. L-Nampt Expression Correlates with Systemic Inflammatory and Nutritional Indices
2.2.3. L-Nampt Expression Is Up-Regulated in IBD Patients Treated with CS or AZA but the Effect Is Mediated by the Disease Activity
2.2.4. L-Nampt as a Biomarker in IBD
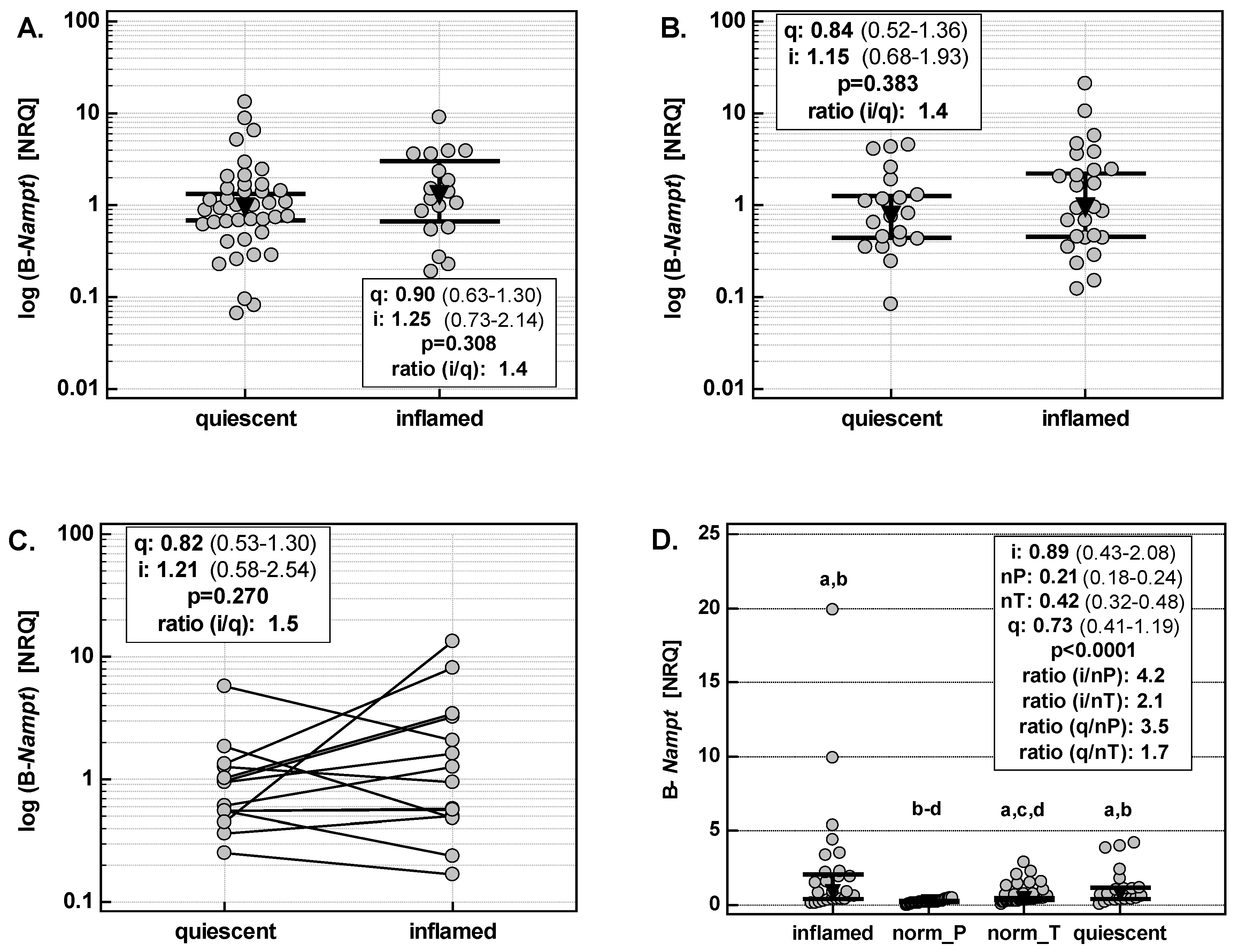
2.3. Bowel Expression of Nampt
2.3.1. Bowel Nampt (B-Nampt) Expression Is Up-Regulated Both in Inflamed and Quiescent Colon
2.3.2. B-Nampt Expression Is Independently Associated with IL1B and HIF1A in Inflamed but with FGF2 in Quiescent Bowel
3. Discussion
4. Materials and Methods
4.1. Study Population
4.1.1. Circulating Nampt
4.1.2. Leukocyte Nampt (L-Nampt)
4.1.3. Bowel Nampt (B-Nampt)
4.1.4. Ethical Considerations
4.2. Analytical Methods
4.2.1. Circulating Nampt
4.2.2. Nampt Expression in Leukocytes
4.2.3. Nampt Expression in Bowel Tissue
4.2.4. Reverse Transcription (RT)
4.2.5. Quantitative (Real-Time) PCR (qPCR)
4.2.6. Normalization Strategy, Calculation of Expression Level
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| Nampt | Nicotinamide phosphoribosyltransferase |
| PBEF | pre-B-cell colony enhancing factor 1 |
| IBD | inflammatory bowel disease |
| UC | ulcerative colitis |
| CD | Crohn’s disease |
| IBS | irritable bowel syndrome |
| CDAI | Crohn’s Disease Activity Index |
| RI | Rachmilewitz Index |
| CS | corticosteroids |
| AZA | azathioprine |
| hsCRP | high-sensitive C-reactive protein |
| CRC | colorectal adenocarcinoma |
| ROC | Receiver operating characteristic curve analysis |
| AUC | area under ROC curve |
| MH | mucosal healing |
References
- Burisch, J.; Munkholm, P. The epidemiology of inflammatory bowel disease. Scand. J. Gastroenterol. 2015, 50, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Fiocchi, C. Inflammatory bowel disease pathogenesis: Where are we? J. Gastroenterol. Hepatol. 2015, 30 (Suppl. 1), 12–18. [Google Scholar] [CrossRef] [Green Version]
- Colombel, J.F.; Mahadevan, U. Inflammatory bowel disease 2017: Innovations and changing paradigms. Gastroenterology 2017, 152, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Rogler, G.; Biedermann, L. Clinical utility of biomarkers in IBD. Curr. Gastroenterol. Rep. 2015, 17, 26. [Google Scholar] [CrossRef]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M.; Halawi, H.; Oduyebo, I. Biomarkers as a diagnostic tool for irritable bowel syndrome: Where are we? Expert Rev. Gastroenterol. Hepatol. 2017, 11, 303–316. [Google Scholar] [CrossRef]
- Pereira, S.; Pereira-Castro, I.; Neto, C.; Teixeiro da Costa, L.; Amorim, A.; Silva, R.M. Extensive regulation of nicotinate phosphoribosyltransferase (NAPRT) expression in human tissues and tumors. Oncotarget 2016, 7, 1973–1983. [Google Scholar] [CrossRef]
- Zhang, J.; Heruth, D.P.; Ye, S.Q. Nicotinamide phosphoribosyltransferase in human diseases. Bioanal. Biomed. 2011, 3, 13–25. [Google Scholar] [CrossRef]
- Carbone, F.; Liberal, L.; Bonaventura, A.; Vecchie, A.; Casula, A.; Cea, M.; Monacelli, F.; Caffa, I.; Bruzzone, S.; Montecucco, F.; et al. Regulation and function of extracellular nicotinamide phosphoribosyltransferase/visfatin. Compr. Physiol. 2017, 7, 603–621. [Google Scholar] [CrossRef]
- Grolla, A.A.; Travelli, C.; Genazzani, A.A.; Sethi, J.K. Extracellular nicotinamide phosphoribosyltransferase, a new cancer metabokine. Br. J. Pharmacol. 2016, 173, 2182–2194. [Google Scholar] [CrossRef]
- Espindola-Netto, J.M.; Chini, C.S.; Tarragó, M.; Wang, E.; Dutta, S.; Pal, K.; Mukhopadhyay, D.; Sola-Penna, M.; Chini, E.H. Preclinical efficacy of the novel competitive NAMPT inhibitor STF-118804 in pancreatic cancer. Oncotarget 2017, 8, 85054–85067. [Google Scholar] [CrossRef] [PubMed]
- Peterse, E.F.P.; van den Akker, B.E.W.M.; Niessen, B.; Oosting, J.; Suijker, J.; de Jong, Y.; Danen, E.H.J.; Cleton-Jansen, A.M.; Bovée, J.V.M.G. NAD synthesis pathway interference is a viable therapeutic strategy for chondrosarcoma. Mol. Cancer Res. 2017, 15, 1714–1721. [Google Scholar] [CrossRef] [PubMed]
- Gerner, R.R.; Klepsch, V.; Macheiner, S.; Arnhard, K.; Adolph, T.E.; Grander, C.; Wieser, V.; Pfister, A.; Moser, P.; Hermann-Kleiter, N.; et al. NAD metabolism fuels human and mouse intestinal inflammation. Gut 2018, 67, 1813–1823. [Google Scholar] [CrossRef] [PubMed]
- Mesco, B.; Poliska, S.; Szegedi, A.; Szekanecz, Z.; Palatka, K.; Papp, M.; Nagy, L. Peripheral blood gene expression patterns discriminate among chronic inflammatory diseases and healthy controls and identify novel targets. BMC Med. Genom. 2010, 3, 15. [Google Scholar] [CrossRef] [PubMed]
- Gesing, J.; Scheuermann, K.; Wagner, I.V.; Löffler, D.; Friebe, D.; Kiess, W.; Schuster, V.; Körner, A. NAMPT serum levels are selectively elevated in acute infectious disease and in acute relapse of chronic inflammatory diseases in children. PLoS ONE 2017, 12, e0183027. [Google Scholar] [CrossRef] [PubMed]
- Star, A.; Deeke, S.A.; Ning, Z.; Chiang, C.-K.; Zhang, X.; Mottawea, W.; Singleton, R.; Benchimol, E.I.; Wen, M.; Mack, D.R.; et al. Proteomic analysis of ascending colon biopsies from a paediatric inflammatory bowel disease inception cohort identifies protein biomarkers that differentiate Crohn’s disease from UC. Gut 2017, 66, 1573–1583. [Google Scholar] [CrossRef]
- Moschen, A.R.; Kaser, A.; Enrich, B.; Mosheimer, B.; Theurl, M.; Niederegger, H.; Tilg, H. Visfatin, an adipocytokine with proinflammatory and immunomodulating properties. J. Immunol. 2007, 178, 1748–1758. [Google Scholar] [CrossRef]
- Trejo-Vazquez, F.; Garza-Veloz, I.; Villela-Ramirez, G.A.; Ortiz-Castro, Y.; Mauricio-Saucedo, P.; Cardenas-Vargas, E.; Diaz-Baez, M.; Cid-Baez, M.A.; Castañeda-Miranda, R.; Ortiz-Rodriguez, J.M.; et al. Positive association between leptin serum levels and disease activity on endoscopy in inflammatory bowel disease: A case-control study. Exp. Ther. Med. 2018, 15, 3336–3344. [Google Scholar] [CrossRef] [Green Version]
- Terzoudis, S.; Malliaraki, N.; Damilakis, J.; Dimitriadou, D.A.; Zavos, C.; Koutroubakis, I.E. Chemerin, visfatin, and vaspin serum levels in relation to bone mineral density in patients with inflammatory bowel disease. Eur. J. Gastroenterol. Hepatol. 2016, 28, 814–819. [Google Scholar] [CrossRef]
- Waluga, M.; Hartleb, M.; Boryczka, G.; Kukla, M.; Zwirska-Korczala, K. Serum adipokines in inflammatory bowel disease. World J. Gastroenterol. 2014, 20, 6912–6917. [Google Scholar] [CrossRef]
- Valentini, L.; Wirth, E.K.; Schweizer, U.; Hengstermann, S.; Schaper, L.; Koernicke, T.; Dietz, E.; Norman, K.; Buning, C.; Winklhofer-Roob, B.M.; et al. Circulating adipokines and the protective effects of hyperinsulinemia in inflammatory bowel disease. Nutrition 2009, 25, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Ogjanovic, S.; Bao, S.; Yamamoto, S.Y.; Garibay-Tupas, J.; Samal, B.; Bryant-Greenwood, G.D. Genomic organization of the gene coding for human pre-B-cell colony enhancing factor and expression in human fetal membranes. J. Mol. Endocrinol. 2001, 26, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Sayed, E.H.; Brakat, M.S.; Diab, W.M.; Abd Elmaged, M.H.; Tayel, M.Y.; Ramadan, R.A. Study of the Role of Nicotinamide Phosphoribosyl Transferase/Visfatin in Egyptian Patients with Systemic Lupus Erythematous and Lupus Nephritis. Am. J. Int. Med. 2016, 4, 18–23. [Google Scholar] [CrossRef]
- Daperno, M.; Castiglione, F.; de Ridder, L.; Dotan, I.; Färkkilä, M.; Florholmen, J.; Fraser, G.; Fries, W.; Hebuterne, X.; Lakatos, P.L.; et al. Measures and markers of prediction to achieve, detect, and monitor intestinal healing in inflammatory bowel disease. J. Crohn’s Colitis 2011, 5, 484–498. [Google Scholar] [CrossRef]
- Neurath, M.F.; Travis, S.P.L. Mucosal healing in inflammatory bowel diseases: A systematic review. Gut 2012, 61, 1619–1635. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, K.; Misa, I.; Diakowska, D.; Kapturkiewicz, B.; Gamian, A.; Krzystek-Korpacka, M. Nampt/PBEF/visfatin upregulation in colorectal tumors, mirrored in normal tissue and whole blood of colorectal cancer patients, is associated with metastasis, hypoxia, IL1β, and anemia. Biomed. Res. Int. 2015, 2015, 523930. [Google Scholar] [CrossRef] [PubMed]
- Garten, A.; Schuster, S.; Penke, M.; Gorski, T.; de Giorgis, T.; Kiess, W. Physiological and pathological role of NAMPT and NAD metabolism. Nat. Rev. Endocrinol. 2015, 11, 535–546. [Google Scholar] [CrossRef]
- Maddaluno, L.; Urwyler, C.; Werner, S. Fibroblast growth factors: Key players in regeneration and tissue repair. Development 2017, 144, 4047–4060. [Google Scholar] [CrossRef]
- Bae, Y.H.; Bae, M.K.; Kim, S.R.; Lee, J.H.; Wee, H.J.; Bae, S.K. Upregulation of fibroblast growth factor-2 by visfatin that promotes endothelial angiogenesis. Biochem. Biophys. Res. Commun. 2009, 379, 206–211. [Google Scholar] [CrossRef]
- Stone, R.C.; Pastar, I.; Ojeh, N.; Chen, V.; Liu, S.; Garzon, K.I.; Tomic-Canic, M. Epithelial-mesenchymal transition in tissue repair and fibrosis. Cell Tissue Res. 2016, 365, 495–506. [Google Scholar] [CrossRef] [Green Version]
- Curciarello, R.; Docena, G.H.; MacDonald, T.T. The role of cytokines in the fibrotic responses in Crohn’s disease. Front. Med. 2017, 4, 126. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.F.; Diegelmann, R.F.; Elson, C.O.; Lindblad, W.J.; Gotschalk, N.; Gay, S.; Gay, R. Collagen content ant type in the intestinal stricture in Crohn’s disease. Gastroenterology 1988, 94, 257–265. [Google Scholar] [CrossRef]
- Pillai, V.B.; Sundaresan, N.R.; Kim, G.; Samant, S.; Moreno-Vinasco, L.; Garcia, J.G.N.; Gupta, M.P. Nampt secreted from cardiomyocytes promotes development of cardiac hypertrophy and adverse ventricular remodeling. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, H415–H426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roche, J. The Epithelial-to-Mesenchymal Transition in Cancer. Cancers 2018, 10, E52. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.K.; Kim, S.R.; Kim, J.G.; Kim, J.Y.; Koo, T.H.; Jang, H.O.; Yun, I.; Yoo, M.A.; Bae, M.K. Hypoxic induction of human visfatin gene is directly mediated by hypoxia-inducible factor-1. FEBS Lett. 2006, 580, 4105–4113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kralisch, S.; Klein, J.; Lossner, U.; Bluher, M.; Paschke, R.; Stumvoll, M.; Fasshauer, M. Hormonal regulation of the novel adipocytokine visfatin in 3T3-L1 adipocytes. J. Endocrinol. 2005, 185, R1–R8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Seidel, E.R. Estrogens induce visfatin expression in 3T3-L1 cells. Peptides 2010, 31, 271–274. [Google Scholar] [CrossRef]
- Annie, L.; Gurusubramanian, G.; Roy, V.K. Estrogen and progesterone dependent expression of visfatin/NAMPT regulates proliferation and apoptosis in mice uterus during estrous cycle. J. Steroid Biochem. Mol. Biol. 2018, 185, 225–236. [Google Scholar] [CrossRef]
- Celichowski, P.; Jopek, K.; Milecka, P.; Szyszka, M.; Tyczewska, M.; Malendowicz, L.K.; Ruciński, M. Nicotinamide phosphoribosyltransferase and the hypothalamic-pituitary-adrenal axis of the rat. Mol. Med. Rep. 2018, 17, 6163–6173. [Google Scholar] [CrossRef]
- Leivo-Korpela, S.; Lehtimaki, L.; Hamalainen, M.; Vuolteenaho, K.; Koobi, L.; Jarvenpaa, R.; Kankaanranta, H.; Saarelainen, S.; Moilanen, E. Adipokines NUCB2/nesfatin-1 and visfatin as novel inflammatory factors in chronic obstructive pulmonary disease. Med. Inflamm. 2014, 2014, 232167. [Google Scholar] [CrossRef]
- Waljee, A.K.; Wiitala, W.L.; Govani, S.; Stidham, R.; Saini, S.; Hou, J.; Feagins, L.A.; Khan, N.; Good, C.B.; Vijan, S.; et al. Corticosteroid Use and Complications in a US Inflammatory Bowel Disease Cohort. PLoS ONE 2016, 11, e0158017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschen, A.R.; Geiger, S.; Gerner, R.; Tilg, H. Pre-B cell colony enhancing factor/NAMPT/visfatin and its role in inflammation-related bone disease. Mutat. Res. 2010, 690, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, K.W.; Tremaine, W.J.; Ilstrup, D.M. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis: A randomized study. N. Engl. J. Med. 1987, 317, 1625–1629. [Google Scholar] [CrossRef] [PubMed]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, RESEARCH0034. [Google Scholar] [CrossRef] [Green Version]
- Krzystek-Korpacka, M.; Diakowska, D.; Bania, J.; Gamian, A. Expression stability of common housekeeping genes is differently affected by bowel inflammation and cancer: Implications for finding suitable normalizers for inflammatory bowel disease studies. Inflamm. Bowel. Dis. 2014, 20, 1147–1156. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-IBD Controls | IBD | ||
|---|---|---|---|---|
| Healthy Individuals | IBS | CD | UC | |
| BMI (kg/m2) | −0.44, p = 0.200 | −0.34, p = 0.276 | −0.08, p = 0.559 | 0.0, p = 0.940 |
| Hb (g/L) | na | 0.38, p = 0.226 | 0.01, p = 0.903 | −0.17, p = 0.068 |
| Iron (μM) | −0.29, p = 0.086 | 0.13, p = 0.681 | −0.34, p = 0.003 | −0.30, p = 0.006 |
| Tf (mg/dL) | −0.02, p = 0.915 | −0.02, p = 0.957 | −0.28, p = 0.018 | −0.34, p = 0.001 |
| Alb (g/dL) | −0.20, p = 0.212 | −0.14, p = 0.636 | −0.35, p = 0.001 | −0.28, p = 0.006 |
| PLT (×109/L) | na | −0.54, p = 0.089 | 0.14, p = 0.175 | 0.20, p = 0.030 |
| WBC (×109/L) | na | −0.39, p = 0.217 | 0.27, p = 0.009 | 0.18, p = 0.044 |
| ESR (mm/h) | na | −0.20, p = 0.526 | 0.13, p = 0.219 | 0.41, p < 0.001 |
| hsCRP (mg/L) | −0.10, p = 0.521 | 0.12, p = 0.744 | 0.35, p = 0.013 | 0.37, p = 0.002 |
| Parameter | Non-IBD Controls (IBS) | IBD | |
|---|---|---|---|
| CD | UC | ||
| Hb (g/L) | ρ= −0.46, p = 0.047 | ρ= −0.34, p = 0.025 | ρ= −0.36, p = 0.032 |
| PLT (×109/L) | ρ= −0.08, p = 0.753 | ρ = 0.34, p = 0.024 | ρ = 0.32, p = 0.061 |
| WBC (×109/L) | ρ = 0.21, p = 0.387 | ρ = 0.45, p = 0.003 | ρ = 0.38, p = 0.025 |
| ESR (mm/h) | ρ= −0.02, p = 0.926 | ρ = 0.08, p = 0.821 | ρ = 0.19, p = 0.511 |
| hsCRP (mg/L) | ρ = 0.28, p = 0.334 | ρ = 0.33, p = 0.054 | ρ = 0.66, p < 0.001 |
| IL1B (NRQ) | ρ = 0.33, p = 0.163 | ρ= −0.09, p = 0.566 | ρ = 0, p = 0.977 |
| TNFA (NRQ) | ρ = 0.26, p = 0.286 | ρ = 0.17, p = 0.271 | ρ = 0.28, p = 0.102 |
| IL8 (NRQ) | ρ = 0.52, p = 0.023 | ρ = 0.13, p = 0.384 | ρ= −0.14, p = 0.429 |
| VEGFA (NRQ) | ρ = 0.14, p = 0.567 | ρ = 0.63, p < 0.0001 | ρ = 0.48, p = 0.003 |
| Parameter | Non-IBD Controls | IBD | p | ||
|---|---|---|---|---|---|
| Healthy Individuals | IBS | CD | UC | ||
| N | 40 | 20 | 113 | 127 | - |
| Age, median (yrs.) | 35 (25–44) | 37.5 (23–50) | 36 (28–47.25) | 38 (28–52) | 0.463 6 |
| Sex (F/M), n | 20/20 | 12/8 | 58/55 | 55/72 | 0.419 7 |
| BMI, median (kg/m2) | 25.3 (22.5–26.4) 2 | 26.2 (22.5–28.4) 2 | 22.2 (21.5–22.8) 1,3,4 | 23.9(22.9–24.8) 2 | 0.002 6 |
| Active disease, n (%) | - | - | 74 (65.5) | 55 (43.3) | <0.001 7 |
| Hb, median (g/dL) | na | 13.3 (12.5–14.6) 2 | 12.3 (11.9–12.7) 1 | 12.7 (12.2–13.3) | 0.048 6 |
| Iron, median (μM) | 18.6 (16.4–21.6) 2,3 | 18.7 (12–24.8) 2 | 10.9 (8.7–11.8) 1,3,4 | 14.3 (12.3–16.3) 2,4 | <0.001 6 |
| Tf, median (mg/dL) | 276 (267–293) 2 | 284 (255–304) 2 | 236 (223–258) 1,3,4 | 263 (250–282) 2 | 0.009 6 |
| Alb, median (g/dL) | 4.82 (4.7–4.9) 2,3 | 4.72 (4.6–4.9) 2,3 | 4.36 (4.2–4.4) 1,3,4 | 4.54 (4.4–4.6) 1,2,4 | <0.001 6 |
| PLT, median (×109/L) | na | 261 (223–307) | 343 (292–376) | 293 (282–315) | 0.094 6 |
| WBC, median (×109/L) | na | 6.55 (4.9–7.1) | 7.0 (6.2–7.9) | 6.87 (6.1–7.4) | 0.773 6 |
| ESR, median (mm/h) | na | 10 (5.5–24) 2 | 20 (18–26) 1,3 | 14 (11–20) 2 | 0.011 6 |
| hsCRP, median (mg/L) | 2.21 (0.6–5.3) 2,3 | 1.47 (0–24) 2,3 | 16.6 (7.3–25.5) 1,4 | 5 (2–7) 1,4 | <0.001 6 |
| IL-1β, median (pg/mL) | 0.79 (0.39–2.04) | 0.17 (0–1.28) | 0.79 (0.47–1.25) | 0.88 (0.70–1.43) | 0.161 6 |
| IL-6, median (pg/mL) | 0.68 (0.58–0.87) 2,3 | 1.11 (0.65–2.33) 2 | 2.74 (1.9–4) 1,3,4 | 1.98 (1.33–2.87) 2,4 | <0.001 6 |
| TNFα, median (pg/mL) | 1 (0.35–1.59) | 0.62 (0–2) | 0.77 (0.22–1) | 0.49 (0.33–0.83) | 0.780 6 |
| CS, n (%) 5 | - | - | 38 (53%) | 34 (47%) | 0.283 8 |
| AZA, n (%) | - | - | 47 (42%) | 30 (24%) | 0.004 8 |
| Parameter | IBS-controls | IBD | p | |
|---|---|---|---|---|
| CD | UC | |||
| N | 19 | 44 | 35 | - |
| Age, mean (yrs.) | 37.4 (30.7–45.6) | 34.1 (31.2–37.3) | 38.8 (34.5–43.6) | 0.225 5 |
| Sex (F/M), n | 7/12 | 18/26 | 15/20 | 0.912 6 |
| Active disease, n (%) | - | 21 (48%) | 20 (57%) | 0.429 6 |
| Hb, mean (g/dL) | 14.4 (13.7–15.1) 1,2 | 13 (12.3–13.6) 3 | 12.9 (12.1–13.8) 3 | 0.029 5 |
| PLT, median (×109/L) | 256 (212–294) 1,2 | 306 (244–337) 3 | 326 (280–367) 3 | 0.013 7 |
| WBC, median (×109/L) | 6.11 (5.53–6.97) | 7.32 (5.38–8.95) | 8.44 (7.29–9.5) | 0.145 7 |
| ESR, median (mm/h) | 7 (6–9) 1,2 | 23 (12–55) 3 | 21 (8–26) 3 | <0.001 7 |
| hsCRP, mean (mg/L) | 2 (0.8–5.2) | 7.7 (3.9–15.2) | 6.4 (2.9–14.3) | 0.082 5 |
| CS, n (%) 4 | - | 7 (33%) | 10 (50%) | 0.285 8 |
| AZA, n (%) | - | 18 (41%) | 6 (18%) | 0.047 8 |
| Symbol | Gene Name | Accession No. | Primer Sequence 5’→3’ | Amp. Size (bp) | E (%) Leuko | E (%) Tissue |
|---|---|---|---|---|---|---|
| SDHA | Succinate dehydrogenase subunit A | NM_004168.2 | F: agaggcacggaaggagtcac R: caccacatcttgtctcatcagtagg | 267 | 94.8 | - |
| TBP | TATA-box-binding protein | NM_003194.4 | F: tataatcccaagcggtttgctg R: ctggctcataactactaaattgttg | 283 | 109.7 | - |
| IL1B 1 | Interleukin (IL)-1β | NM_000576.2 | F: ccacagaccttccaggagaatg R: gtgcagttcagtgatcgtacagg | 131 | 100.1 | 94.7 |
| TNFA 1 | Tumor necrosis factor α | NM_000594.3 | F: ctcttctgcctgctgcactttg R: atgggctacaggcttgtcactc | 135 | 100.1 | 98.2 |
| IL8 | Interleukin 8 | NM_000584.3 | F: caacacagaaattattgtaaagc R: aagtgttgaagtagatttgc | 191 | - | 96.7 |
| VEGFA 1 | Vascular endothelial growth factor A | NM_001025366.2 | F: ttgccttgctgctctacctcca R: gatggcagtagctgcgctgata | 126 | 94.5 | 96.1 |
| HIF1A | Hypoxia-inducible factor 1α | NM_001530.3 | F: ctgccaccactgatgaatta R: gtatgtgggtaggagatgga | 90 | - | 104.7 |
| Nampt | Nicotinamide phosphoribosyltransferase | NM_005746.2 | F: cacaggcaccactaataatcagac R: ctccaccagaaccgaaggc | 243 | 108.8 | 104 |
| RPS23 1 | Ribosomal protein S23 | NM_001025.4 | F: aggaagtgtgtaagggtccagc R: caccaacagcatgacctttgcg | 142 | - | 102.9 |
| PPIA 1 | Peptidylprolyl isomerase A | NM_021130.3 | F: ggcaaatgctggacccaacaca R: tgctggtcttgccattcctgga | 161 | - | 99.7 |
| RPLP0 1 | Ribosomal protein, large, P0 | NM_001002.3 | F: tcacaacaagcataccaagaagc R: gtatccgatgtccacaatgtcaag | 263 | 102.1 | |
| FGF2 | Basic fibroblast growth factor | NM_002006.5 | F: tctatcaaaggagtgtgtgctaac R: tgcccagttcgtttcagtgc | 179 | - | 100.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neubauer, K.; Bednarz-Misa, I.; Walecka-Zacharska, E.; Wierzbicki, J.; Agrawal, A.; Gamian, A.; Krzystek-Korpacka, M. Oversecretion and Overexpression of Nicotinamide Phosphoribosyltransferase/Pre-B Colony-Enhancing Factor/Visfatin in Inflammatory Bowel Disease Reflects the Disease Activity, Severity of Inflammatory Response and Hypoxia. Int. J. Mol. Sci. 2019, 20, 166. https://doi.org/10.3390/ijms20010166
Neubauer K, Bednarz-Misa I, Walecka-Zacharska E, Wierzbicki J, Agrawal A, Gamian A, Krzystek-Korpacka M. Oversecretion and Overexpression of Nicotinamide Phosphoribosyltransferase/Pre-B Colony-Enhancing Factor/Visfatin in Inflammatory Bowel Disease Reflects the Disease Activity, Severity of Inflammatory Response and Hypoxia. International Journal of Molecular Sciences. 2019; 20(1):166. https://doi.org/10.3390/ijms20010166
Chicago/Turabian StyleNeubauer, Katarzyna, Iwona Bednarz-Misa, Ewa Walecka-Zacharska, Jaroslaw Wierzbicki, Anil Agrawal, Andrzej Gamian, and Malgorzata Krzystek-Korpacka. 2019. "Oversecretion and Overexpression of Nicotinamide Phosphoribosyltransferase/Pre-B Colony-Enhancing Factor/Visfatin in Inflammatory Bowel Disease Reflects the Disease Activity, Severity of Inflammatory Response and Hypoxia" International Journal of Molecular Sciences 20, no. 1: 166. https://doi.org/10.3390/ijms20010166
APA StyleNeubauer, K., Bednarz-Misa, I., Walecka-Zacharska, E., Wierzbicki, J., Agrawal, A., Gamian, A., & Krzystek-Korpacka, M. (2019). Oversecretion and Overexpression of Nicotinamide Phosphoribosyltransferase/Pre-B Colony-Enhancing Factor/Visfatin in Inflammatory Bowel Disease Reflects the Disease Activity, Severity of Inflammatory Response and Hypoxia. International Journal of Molecular Sciences, 20(1), 166. https://doi.org/10.3390/ijms20010166