Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis

 , and
, and 
Abstract
:1. Background
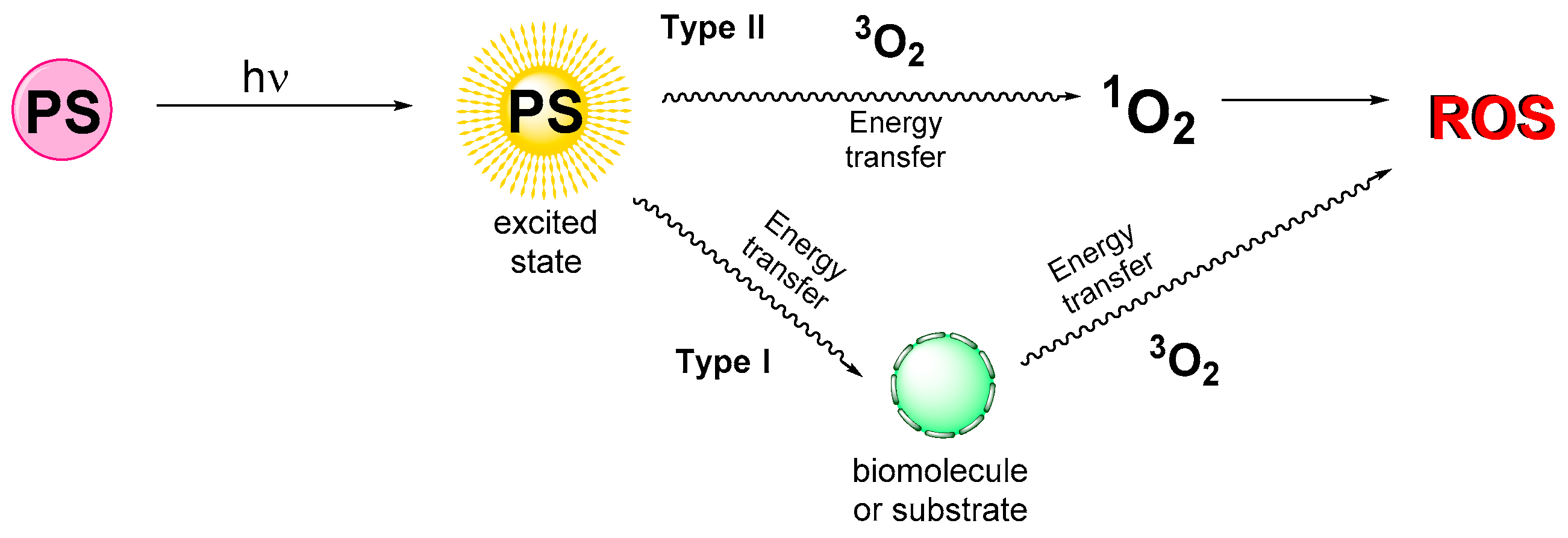
1.1. Photodynamic Therapy Principle
1.2. Rheumatoid Arthritis
2. Photosensitizers Used to Treat Rheumatoid Arthritis
2.1. First Generation of Photosensitizers
2.2. Second Generation of Photosensitizers
2.3. Other Photosensitizers
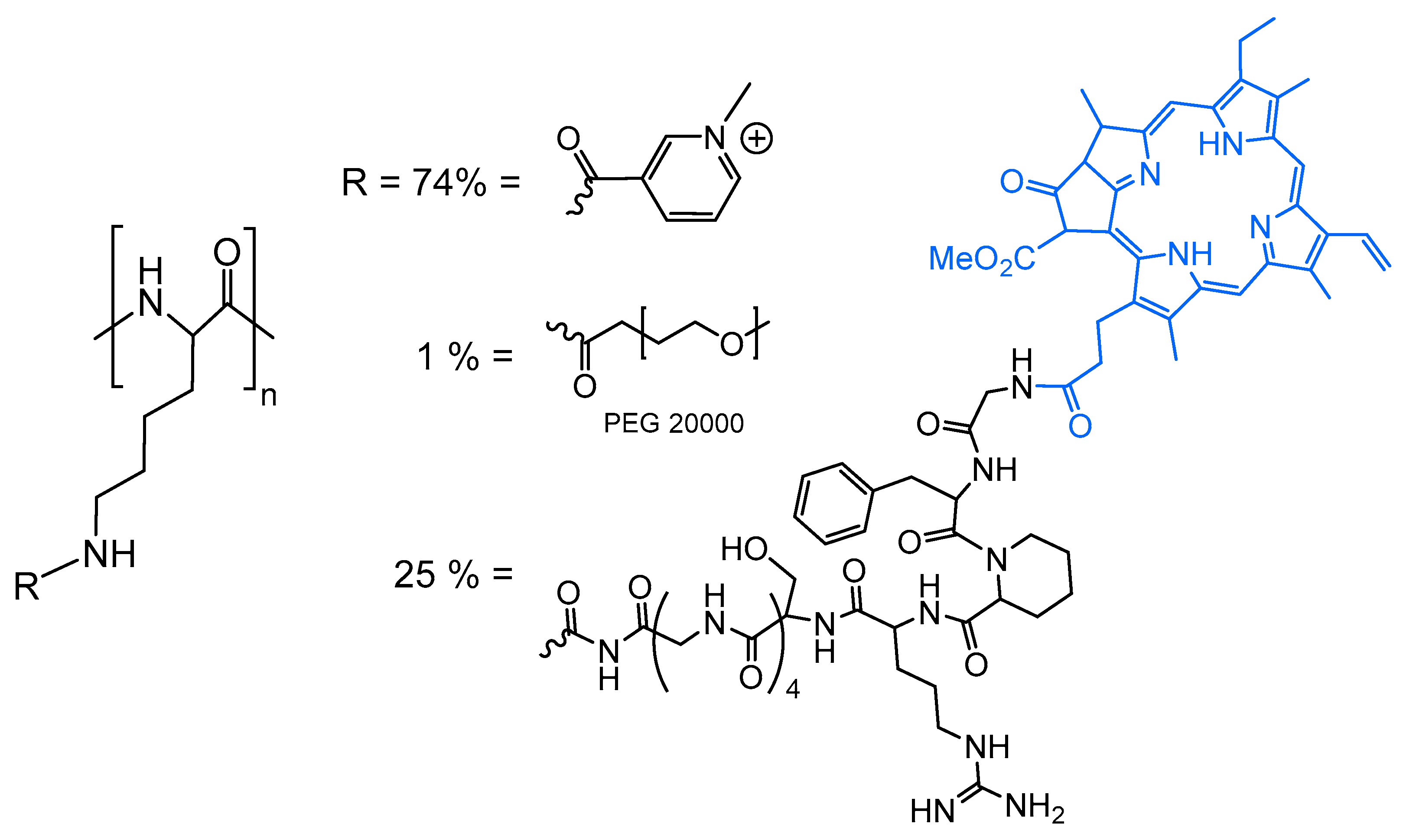
2.4. Encapsulation of Photosensitizers
2.5. Summary
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BPD-MA | benzoporphyrin derivative monoacid ring a |
| Ce6 | Chlorin e6 |
| DMARDs | disease-modifying antirheumatic drugs |
| FCA | Freund’s complete adjuvant |
| FDA | food and drug administration |
| FLS | fibroblast-like synoviocytes |
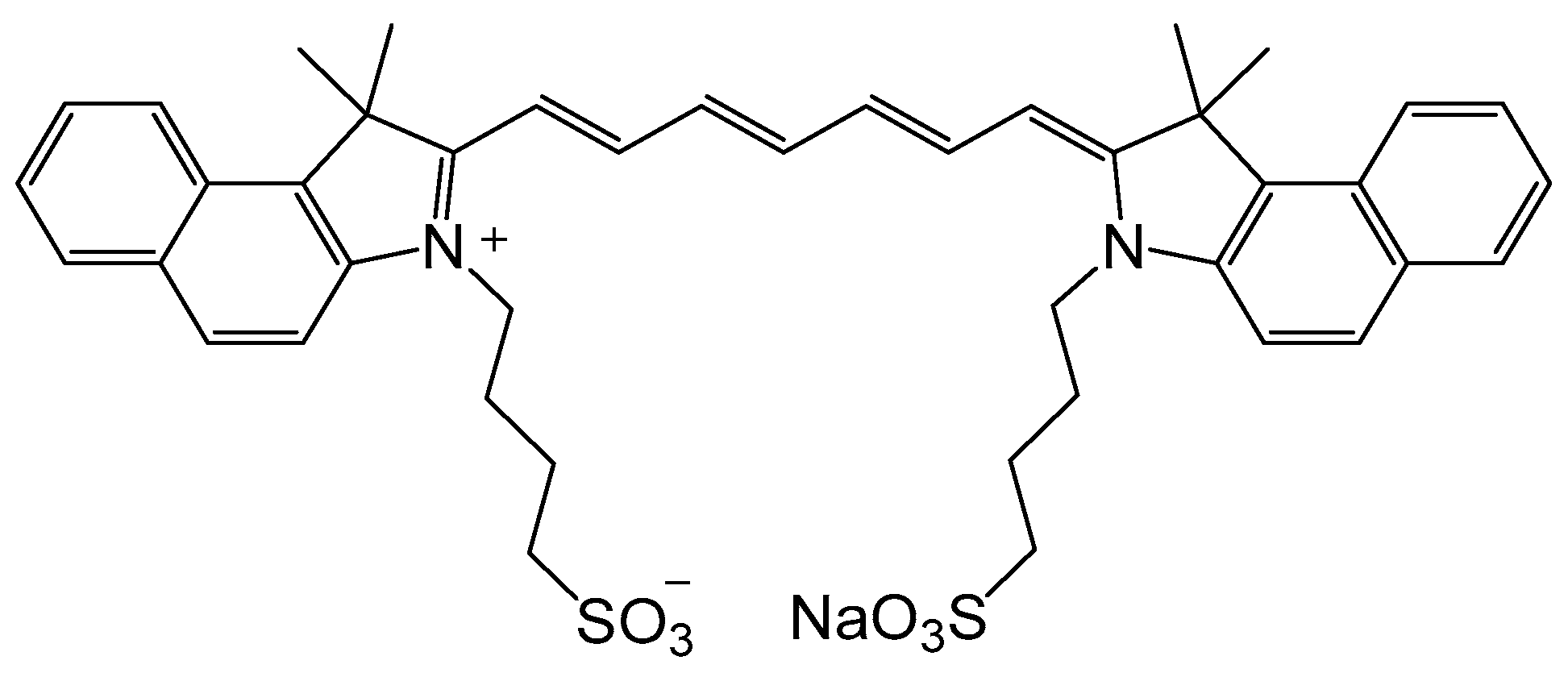
| ICG | indocyanine green |
| IL-17 | interleukin-17 |
| IR | infrared |
| LiD | light dose |
| LD50 | 50% of cell mortality after light activation |
| LED | light-emitting diode |
| lpr | lymphoproliferation |
| MRL | Murphy Roths Large |
| m-THPC | meso-tetra(hydroxyphenyl)chlorin |
| MTT | 3-(4,5-dimethythiazol-2-yl)-2,5-diphenyl tetrazolium bromide |
| NA | not applicable |
| ND | not determined |
| NIR | near infrared |
| NZW | New Zealand white |
| PDT | photodynamic therapy |
| PEG | polyethylene glycol |
| PFP | perfluoro-n-pentane |
| PLGA | poly(DL-lactide-co-glycolic acid) |
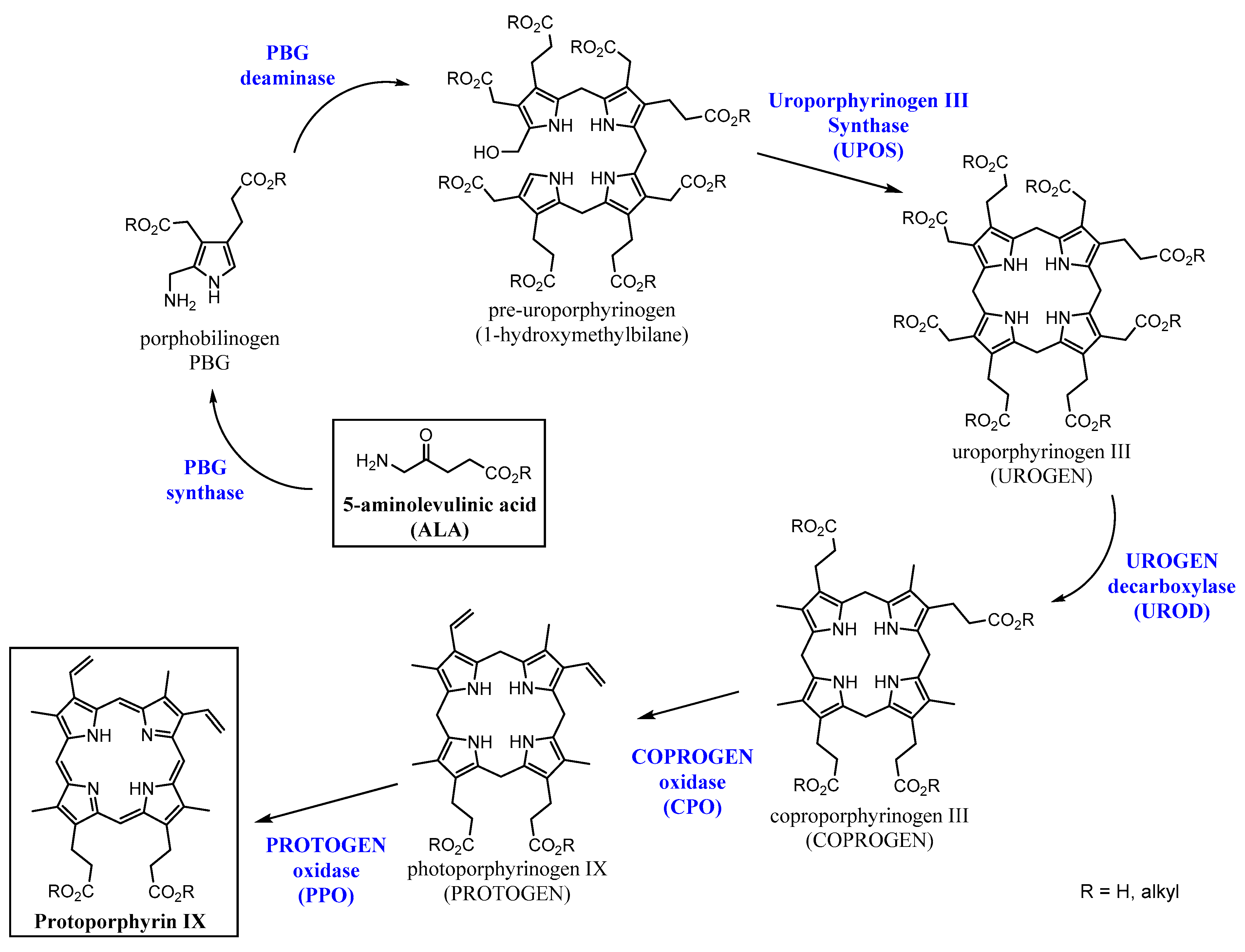
| PpIX | protoporphyrin IX |
| PS | photosensitizer |
| RA | rheumatoid arthritis |
| ROS | radical oxygen species |
| SAA | serum amyloid A |
| SCID | severe combined immunodeficiency |
| TNF | tumor necrosis factor |
| THPC | tetra(hydroxyphenyl)chlorin |
| TPCC | tetra(4-carboxyphenyl)chlorin |
| TPPS2a | meso-tetraphenylporphyrin disulfonate with two sulfonate groups on adjacent phenyl rings |
| TSPP | tetra(4-sulfonatophenyl)porphine |
| WBI | whole body irradiation |
References
- Stacey, O.J.; Pope, S.J.A. New avenues in the design and potential application of metal complexes for photodynamic therapy. RSC Adv. 2013, 3, 25550–25564. [Google Scholar] [CrossRef]
- Dolmans, D.E.J.G.J.; Fukumura, D.; Jain, R.K. Photodynamic Therapy for Cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.A.; Evans, D.H.; Abrahamse, H. Photodynamic therapy (PDT): A short review on cellular mechanisms and cancer research applications for PDT. J. Photochem. Photobiol. B Biol. 2009, 96, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.B.; Brown, E.A.; Walker, I. The present and future role of photodynamic therapy in cancer treatment. Lancet 2004, 5, 497–508. [Google Scholar] [CrossRef]
- Shi, X.; Zhang, C.Y.; Gao, J.; Wang, Z. Recent advances in photodynamic therapy for cancer and infectious diseases. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2019, e1560. [Google Scholar] [CrossRef] [PubMed]
- Aniogo, E.C.; George, B.P.A.; Abrahamse, H. The role of photodynamic therapy on multidrug resistant breast cancer. Cancer Cell Int. 2019, 19, 91. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Shin, H.; Han, J.; Na, K. Combination of photodynamic therapy (PDT) and anti-tumor immunity in cancer therapy. J. Pharm. Investig. 2018, 48, 143–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed]
- Croia, C.; Bursi, R.; Sutera, D.; Petrelli, F.; Alunno, A.; Puxeddu, I. One year in review 2019: Pathogenesis of rheumatoid arthritis. Clin. Exp. Rheumatol. 2019, 37, 347–357. [Google Scholar]
- Deane, K.D.; Holers, V.M. The Natural History of Rheumatoid Arthritis. Clin. Ther. 2019, in press. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. Diagnosis and management of rheumatoid arthritis: A review. JAMA 2018, 320, 1360–1372. [Google Scholar] [CrossRef] [PubMed]
- Silvagni, E.; Di Battista, M.; Bonifacio, A.F.; Zucchi, D.; Governato, G.; Scirè, C.A. One year in review 2019: Novelties in the treatment of rheumatoid arthritis. Clin. Exp. Rheumatol. 2019, 37, 519–534. [Google Scholar] [PubMed]
- Seymour, H.E.; Worsley, A.; Smith, J.M.; Thomas, S.H.L. Anti-TNF agents for rheumatoid arthritis. Br. J. Clin. Pharmacol. 2001, 51, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kremer, J.M.; Bloom, B.J.; Breedveld, F.C.; Coombs, J.H.; Fletcher, M.P.; Gruben, D.; Krishnaswami, S.; Burgos-Vargas, R.; Wilkinson, B.; Zerbini, C.A.F.; et al. The safety and efficacy of a JAK inhibitor in patients with active rheumatoid arthritis: Results of a double-blind, placebo-controlled phase IIa trial of three dosage levels of CP-690,550 versus placebo. Arthritis Rheum. 2009, 60, 1895–1905. [Google Scholar] [CrossRef] [PubMed]
- Allison, B.A.; Pritchard, P.H.; Richter, A.M.; Levy, J.G. The plasma distribution of benzoporphyrin derivative and the effects of plasma lipoproteins on its biodistribution. Photochem. Photobiol. 1990, 52, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Ratkay, L.G.; Chowdhary, R.K.; Neyndorff, H.C.; Tonzetich, J.; Waterfield, J.D.; Levy, J.G. Photodynamic therapy; a comparison with other immunomodulatory treatments of adjuvant-enhanced arthritis in MRL-lpr mice. J. Clin. Exp. Immunol. 1994, 95, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.M.; Jam, A.K.; Canaan, A.J.; Meadows, H.; Levy, J.G. Skin photosensitivity as a model in photodynamic therapy. Proc. SPIE Int. Soc. Opt. Eng. 1996, 2625, 194–205. [Google Scholar] [CrossRef]
- Chowdhary, R.K.; Ratkay, L.G.; Canaan, A.J.; Waterfield, J.D.; Richter, A.M.; Levy, J.G. Uptake of Verteporfin® by articular tissues following systemic and intra-articular administration. Biopharm. Drug Dispos. 1998, 19, 395–400. [Google Scholar] [CrossRef]
- Chowdhary, R.K.; Neyndorff, H.C.; Waterfield, J.D.; Levy, J.G.; Keystone, E.C.; Iamaroon, A.; Ratkay, L.G.; Richter, A.M. Amelioration of antigen-induced arthritis in rabbits by induction of apoptosis of inflammatory-cells with local application of transdermal photodynamic therapy. Arthritis Rheum. 1998, 41, 525–534. [Google Scholar] [CrossRef]
- Trauner, K.B.; Gandour-Edwards, R.; Bamberg, M.; Shortkroff, S.; Sledge, C.; Hasan, T. Photodynamic Synovectomy Using Benzoporphyrin Derivative in an Antigen-induced Arthritis Model for Rheumatoid Arthritis. Photochem. Photobiol. 1998, 67, 133–139. [Google Scholar] [CrossRef]
- Richter, A.M.; Kelly, B.; Chow, J.; Liu, D.J.; Towers, G.H.; Dolphin, D.; Levy, J.G. Preliminary studies on a more effective phototoxic agent than hematoporphyrin. J. Natl. Cancer Inst. 1987, 79, 1327–1332. [Google Scholar] [PubMed]
- Waterfield, J.D.; Fairhurst, M.; Waterfield, E.M.; Norbury, K.C. Evaluation of the immunotoxicity of benzoporphyrin derivative (BPD-MA) in mice. Immunopharmacol. Immunotoxicol. 1997, 19, 89–103. [Google Scholar] [CrossRef] [PubMed]
- Hendrich, C.; Hüttmann, G.; Vispo-Seara, J.L.; Houserek, S.; Siebert, W.E. Experimental photodynamic laser therapy for rheumatoid arthritis with a second generation photosensitizer. Knee Surg. Sports Traumatol. Arthrosc. 2000, 8, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Pernot, M.; Bastogne, T.; Barry, N.P.E.; Therrien, B.; Koellensperger, G.; Hann, S.; Reshetov, V.; Barberi-Heyob, M. Systems biology approach for in vivo photodynamic therapy optimization of ruthenium-porphyrin compounds. J. Photochem. Photobiol. B Biol. 2012, 117, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Jalili, A.; Makowski, M.; Świtaj, T.; Nowis, D.; Wilczyński, G.M.; Wilczek, E.; Chorązy-Massalska, M.; Radzikowska, A.; Maśliński, W.; Białly, Ł.; et al. Effective photoimmunotherapy of murine colon carcinoma induced by the combination of photodynamic therapy and dendritic cells. Clin. Cancer Res. 2004, 10, 4498–4508. [Google Scholar] [CrossRef] [PubMed]
- Peng, Q.; Warloe, T.; Moan, J.; Godal, A.; Apricena, F.; Giercksky, K.E.; Nesland, J.M. Antitumor effect of 5-aminolevulinic acid-mediated photodynamic therapy can be enhanced by the use of a low dose of photofrin in human tumor xenografts. Cancer Res. 2001, 61, 5824–5832. [Google Scholar] [PubMed]
- Firczuk, M.; Gabrysiak, M.; Barankiewicz, J.; Domagala, A.; Nowis, D.; Kujawa, M.; Jankowska-Steifer, E.; Wachowska, M.; Glodkowska-Mrowka, E.; Korsak, B.; et al. GRP78-targeting subtilase cytotoxin sensitizes cancer cells to photodynamic therapy. Cell Death Dis. 2013, 4, e741. [Google Scholar] [CrossRef] [PubMed]
- Schuitmaker, J.J.; Baas, P.; van Leengoed, H.L.L.M.; van der Meulen, F.W.; Star, W.M.; van Zandwijk, N. Photodynamic therapy: A promising new modality for the treatment of cancer. J. Photochem. Photobiol. B Biol. 1996, 34, 3–12. [Google Scholar] [CrossRef]
- Sutedja, T.; Baas, P.; Stewart, F.; van Zandwijk, N. A pilot study of photodynamic therapy in patients with inoperable non-small cell lung cancer. Eur. J. Cancer 1992, 28, 1370–1373. [Google Scholar] [CrossRef]
- Nseyo, U.O.; DeHaven, J.; Dougherty, T.J.; Potter, W.R.; Merrill, D.L.; Lundahl, S.L.; Lamm, D.L. Photodynamic Therapy (PDT) in the Treatment of Patients with Resistant Superficial Bladder Cancer: A Long Term Experience. J. Clin. Laser Med. Surg. 1998, 16, 61–68. [Google Scholar] [CrossRef]
- Abdel Gaber, S.A. Photodynamic Diagnosis and Therapy for Oral Potentially Malignant Disorders and Cancers. In Development of Oral Cancer: Risk Factors and Prevention Strategies; Al Moustafa, A.-E., Ed.; Springer: Cham, Switzerland, 2017; Chapter 10; pp. 147–175. [Google Scholar] [CrossRef]
- Trauner, K.; Gandour-Edwards, R.; Bamberg, M.; Nishioka, N.S.; Flotte, T.; Autry, S.; Hasan, T. Influence of light delivery on photodynamic synovectomy in an antigen- induced arthritis model for rheumatoid arthritis. Lasers Surg. Med. 1998, 22, 147–156. [Google Scholar] [CrossRef]
- Koren, H.; Alth, G. Photodynamic therapy in gynaecologic cancer. J. Photochem. Photobiol. B Biol. 1996, 36, 189–191. [Google Scholar] [CrossRef]
- Feyh, J. Photodynamic treatment for cancers of the head and neck. J. Photochem. Photobiol. B Biol. 1996, 36, 175–177. [Google Scholar] [CrossRef]
- Gupta, S.; Dwarakanath, B.S.; Muralidhar, K.; Jain, V. Cellular uptake, localization and photodynamic effects of haematoporphyrin derivative in human glioma and squamous carcinoma cell lines. J. Photochem. Photobiol. B Biol. 2003, 69, 107–120. [Google Scholar] [CrossRef]
- Yu, Z.; Li, H.; Zhang, L.-M.; Zhu, Z.; Yang, L. Enhancement of phototoxicity against human pancreatic cancer cells with photosensitizer-encapsulated amphiphilic sodium alginate derivative nanoparticles. Int. J. Pharm. 2014, 473, 501–509. [Google Scholar] [CrossRef]
- Burmester, G.R.; Locher, P.; Koch, B.; Winchester, R.J.; Dimitriu-Bona, A.; Kalden, J.R.; Mohr, W. The tissue architecture of synovial membranes in inflammatory and non-inflammatory joint diseases. Rheumatol. Int. 1983, 3, 173–181. [Google Scholar] [CrossRef]
- Hendrich, C.; Diddens, H.; Nosir, H.; Siebert, W.E. Treatment of Rheumatoid Arthritis using Photodynamic Therapy? Proc. SPIE Int. Soc. Opt. Eng. 1995, 2371, 592–595. [Google Scholar] [CrossRef]
- Hendrich, C.; Hüttmann, G.; Lehnert, C.; Diddens, H.; Siebert, W.E. Photodynamic laser therapy for rheumatoid arthritis cell culture studies and animal experiments. Knee Surg. Sports Traumatol. Arthrosc. 1997, 5, 58–63. [Google Scholar] [CrossRef]
- Fidanzi-Dugas, C.; Liagre, B.; Chemin, G.; Perraud, A.; Carrion, C.; Couquet, C.-Y.; Granet, R.; Sol, V.; Léger, D.Y. Analysis of the in vitro and in vivo effects of photodynamic therapy on prostate cancer by using new photosensitizers, protoporphyrin IX-polyamine derivatives. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1676–1690. [Google Scholar] [CrossRef]
- Leeper, F.J. The biosynthesis of porphyrins, chlorophylls, and vitamin B12. Nat. Prod. Rep. 1989, 6, 171–203. [Google Scholar] [CrossRef]
- Layer, G.; Reichelt, J.; Jahn, D.; Heinz, D.W. Structure and function of enzymes in heme biosynthesis. Protein Sci. 2010, 19, 1137–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, D.G.; Golub, A.L.; Marcus, S.L.; Carroll, R.L.; Sobel, R.S.; Lundahl, S. Photodynamic Therapy (PDT) and Photodiagnosis (PD) Using Endogenous Photosensitization Induced by 5-Aminolevulinic Acid (ALA): Current Clinical and Development Status. J. Clin. Laser Med. Surg. 1996, 14, 59–66. [Google Scholar] [CrossRef]
- Uehlinger, P.; Zellweger, M.; Wagnières, G.; Juillerat-Jeanneret, L.; Van Den Bergh, H.; Lange, N. 5-Aminolevulinic acid and its derivatives: Physical chemical properties and protoporphyrin IX formation in cultured cells. J. Photochem. Photobiol. B Biol. 2000, 54, 72–80. [Google Scholar] [CrossRef]
- Kirdaite, G.; Lange, N.; Busso, N.; Van Den Bergh, H.; Kucera, P.; So, A. Protoporphyrin IX photodynamic therapy for synovitis. Arthritis Rheum. 2002, 46, 1371–1378. [Google Scholar] [CrossRef] [PubMed]
- Bagdonas, S.; Kirdaite, G.; Streckyte, G.; Graziene, V.; Leonaviciene, L.; Bradunaite, R.; Venalis, A.; Rotomskis, R. Spectroscopic study of ALA-induced endogenous porphyrins in arthritic knee tissues: Targeting rheumatoid arthritis PDT. Photochem. Photobiol. Sci. 2005, 4, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Miyazawa, S.; Nishida, K.; Komiyama, T.; Nakae, Y.; Takeda, K.; Yorimitsu, M.; Kitamura, A.; Kunisada, T.; Ohtsuka, A.; Inoue, H. Novel transdermal photodynamic therapy using ATX-S10·Na(II) induces apoptosis of synovial fibroblasts and ameliorates collagen antibody-induced arthritis in mice. Rheumatol. Int. 2006, 26, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Torikai, E.; Kageyama, Y.; Kohno, E.; Hirano, T.; Koide, Y.; Terakawa, S.; Nagano, A. Photodynamic therapy using talaporfin sodium for synovial membrane from rheumatoid arthritis patients and collagen-induced arthritis rats. Clin. Rheumatol. 2008, 27, 751–761. [Google Scholar] [CrossRef]
- Hansch, A.; Frey, O.; Gajda, M.; Susanna, G.; Boettcher, J.; Bräuer, R.; Kaiser, W.A. Photodynamic treatment as a novel approach in the therapy of arthritic joints. Lasers Surg. Med. 2008, 40, 265–272. [Google Scholar] [CrossRef]
- Dietze, A.; Engesæter, B.; Berg, K. Transgene delivery and gelonin cytotoxicity enhanced by photochemical internalization in fibroblast-like synoviocytes (FLS) from rheumatoid arthritis patients. Photochem. Photobiol. Sci. 2005, 4, 341–347. [Google Scholar] [CrossRef]
- Berg, K.; Moan, J. Lysosomes as photochemical targets. Int. J. Cancer 1994, 59, 814–822. [Google Scholar] [CrossRef]
- Selbo, P.K.; Weyergang, A.; Høgset, A.; Norum, O.J.; Berstad, M.B.; Vikdal, M.; Berg, K. Photochemical internalization provides time- and space-controlled endolysosomal escape of therapeutic molecules. J. Control. Release 2010, 148, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Selbo, P.K.; Prasmickaite, L.; Tjelle, T.E.; Sandvig, K.; Moan, J.; Gaudernack, G.; Fodstad, Ø.; Kjølsrud, S.; Anholt, H.; et al. Photochemical internalization: A novel technology for delivery of macromolecules into cytosol. Cancer Res. 1999, 59, 1180–1183. [Google Scholar] [PubMed]
- Keller, P.; Sowinska, M.; Tassetti, V.; Heisel, F.; Hajri, A.; Evrard, S.; Miehe, J.A.; Marescaux, J.; Aprahamian, M. Photodynamic imaging of a rat pancreatic cancer with pheophorbide a. Photochem. Photobiol. 1996, 63, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.D.; Xu, C.B.; Lam, H.M.; Wong, F.-L.; Leung, A.W.N.; Leong, M.M.L.; Cho, W.C.S.; Hoeven, R.; Lv, Q.; Rong, R. Proteomic analysis reveals that pheophorbide a-mediated photodynamic treatment inhibits prostate cancer growth by hampering GDP-GTP exchange of ras-family proteins. Photodiagn. Photodyn. Ther. 2018, 23, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Gheewala, T.; Skwor, T.; Munirathinam, G. Photodynamic therapy using pheophorbide and 670nm LEDs exhibits anti-cancer effects in-vitro in androgen dependent prostate cancer. Photodiagn. Photodyn. Ther. 2018, 21, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Kim, D.K.; Kim, J. Apoptosis-related microRNA-145-5p enhances the effects of pheophorbide a-based photodynamic therapy in oral cancer. Oncotarget 2017, 8, 35184–35192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Zhang, J.; Shi, G.; Song, H.; Shi, S.; Zhang, X.; Huang, P.; Wang, Z.; Wang, W.; Wang, C.; et al. A Light Responsive Nanoparticle-Based Delivery System Using Pheophorbide a Graft Polyethylenimine for Dendritic Cell-Based Cancer Immunotherapy. Mol. Pharm. 2017, 14, 1760–1770. [Google Scholar] [CrossRef]
- You, H.; Yoon, H.-E.; Jeong, P.-H.; Ko, H.; Yoon, J.-H.; Kim, Y.-C. Pheophorbide-a conjugates with cancer-targeting moieties for targeted photodynamic cancer therapy. Bioorg. Med. Chem. 2015, 23, 1453–1462. [Google Scholar] [CrossRef]
- Gabriel, D.; Lange, N.; Chobaz-Peclat, V.; Zuluaga, M.F.; Gurny, R.; Van Den Bergh, H.; Busso, N. Thrombin-sensitive dual fluorescence imaging and therapeutic agent for detection and treatment of synovial inflammation in murine rheumatoid arthritis. J. Control. Release 2012, 163, 178–186. [Google Scholar] [CrossRef]
- Hendrich, C.; Siebert, W.E. Photodynamic therapy for rheumatoid arthritis? Lasers Surg. Med. 1997, 21, 359–364. [Google Scholar] [CrossRef]
- Loeb, F.; Clark, W.M.; Coatney, G.R.; Coggeshall, L.T.; Dieuaide, F.R.; Dochez, A.R.; Hakansson, E.G.; Marshall, E.K., Jr.; Marvel, C.S.; et al. Activity of a new antimalarial agent, chloroquine (SN 7618): Statement approved by the Board for coordination of malarial studies. JAMA 1946, 130, 1069–1070. [Google Scholar] [CrossRef]
- Vergne, P.; Liagre, B.; Bertin, P.; Cook-Moreau, J.; Treves, R.; Beneytout, J.L.; Rigaud, M. Methotrexate and cyclooxygenase metabolism in cultured human rheumatoid synoviocytes. J. Rheumatol. 1998, 25, 433–440. [Google Scholar] [PubMed]
- Biemond, P.; Swaak, A.J.G.; Penders, J.M.A.; Beindorff, C.M.; Koster, J.F. Superoxide production by polymorphonuclear leucocytes in rheumatoid arthritis and osteoarthritis: In vivo inhibition by the antirheumatic drug piroxicam due to interference with the activation of the NADPH-oxidase. Ann. Rheum. Dis. 1986, 45, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Brogden, R.N.; Heel, R.C.; Speight, T.M.; Avery, G.S. Piroxicam. A reappraisal of its pharmacology and therapeutic efficacy. Drugs 1984, 28, 292–323. [Google Scholar] [CrossRef] [PubMed]
- Abu Dayyeh, B.K.; Jirapinyo, P.; Weitzner, Z.; Barker, C.; Flicker, M.S.; Lautz, D.B.; Thompson, C.C. Endoscopic sclerotherapy for the treatment of weight regain after Roux-en-Y gastric bypass: Outcomes, complications, and predictors of response in 575 procedures. Gastrointest. Endosc. 2012, 76, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Neupane, J.; Ghimire, S.; Shakya, S.; Chaudhary, L.; Shrivastava, V.P. Effect of light emitting diodes in the photodynamic therapy of rheumatoid arthritis. Photodiagn. Photodyn. Ther. 2010, 7, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Butterweck, V.; Petereit, F.; Winterhoff, H.; Nahrstedtl, A. Solubilized Hypericin and Pseudohypericin from Hypericum perforatum Exert Antidepressant Activity in the Forced Swimming Test. Planta Med. 1998, 64, 291–294. [Google Scholar] [CrossRef]
- García, I.; Ballesta, S.; Gilaberte, Y.; Rezusta, A.; Pascual, Á. Antimicrobial photodynamic activity of hypericin against methicillin-susceptible and resistant Staphylococcus aureus biofilms. Future Microbiol. 2015, 10, 347–356. [Google Scholar] [CrossRef]
- Assefa, Z.; Vantieghem, A.; Declercq, W.; Vandenabeele, P.; Vandenheede, J.R.; Merlevede, W.; de Witte, P.; Agostinis, P. The activation of the c-Jun N-terminal kinase and p38 mitogen-activated protein kinase signaling pathways protects HeLa cells from apoptosis following photodynamic therapy with hypericin. J. Biol. Chem. 1999, 274, 8788–8796. [Google Scholar] [CrossRef]
- Vantieghem, A.; Xu, Y.; Declercq, W.; Vandenabeele, P.; Denecker, G.; Vandenheede, J.R.; Merlevede, W.; De Witte, P.A.; Agostinis, P. Different Pathways Mediate Cytochrome c Release After Photodynamic Therapy with Hypericin. Photochem. Photobiol. 2001, 74, 133–142. [Google Scholar] [CrossRef]
- Hendrickx, N.; Volanti, C.; Moens, U.; Seternes, O.M.; de Witte, P.; Vandenheede, J.R.; Piette, J.; Agostinis, P. Up-regulation of cyclooxygenase-2 and apoptosis resistance by p38 MAPK in hypericin-mediated photodynamic therapy of human cancer cells. J. Biol. Chem. 2003, 278, 52231–52239. [Google Scholar] [CrossRef] [PubMed]
- Mikeš, J.; Koval’, J.; Jendželovský, R.; Sačková, V.; Uhrinová, I.; Kello, M.; Kuliková, L.; Fedoročko, P. The role of p53 in the efficiency of photodynamic therapy with hypericin and subsequent long-term survival of colon cancer cells. Photochem. Photobiol. Sci. 2009, 8, 1558–1567. [Google Scholar] [CrossRef] [PubMed]
- Ferenc, P.; Solár, P.; Kleban, J.; Mikeš, J.; Fedoročko, P. Down-regulation of Bcl-2 and Akt induced by combination of photoactivated hypericin and genistein in human breast cancer cells. J. Photochem. Photobiol. B Biol. 2010, 98, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Kovaľ, J.; Mikeš, J.; Jendželovský, R.; Kello, M.; Solár, P.; Fedoročko, P. Degradation of HER2 Receptor Through Hypericin-mediated Photodynamic Therapy. Photochem. Photobiol. 2010, 86, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Karioti, A.; Bilia, A.R. Hypericins as Potential Leads for New Therapeutics. Int. J. Mol. Sci. 2010, 11, 562–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, K.; Gao, S.; Guo, J.; Ni, G.; Chen, Z.; Li, F.; Zhu, X.; Wen, Y.; Guo, Y. Hypericin-photodynamic therapy inhibits proliferation and induces apoptosis in human rheumatoid arthritis fibroblast-like synoviocytes cell line MH7A. Iran. J. Basic Med. Sci. 2018, 21, 130–137. [Google Scholar] [CrossRef]
- Schmitt, F.; Lagopoulos, L.; Käuper, P.; Rossi, N.; Busso, N.; Barge, J.; Wagnières, G.; Laue, C.; Wandrey, C.; Juillerat-Jeanneret, L. Chitosan-based nanogels for selective delivery of photosensitizers to macrophages and improved retention in and therapy of articular joints. J. Control. Release 2010, 144, 242–250. [Google Scholar] [CrossRef] [Green Version]
- Tang, Q.; Cui, J.; Tian, Z.; Sun, J.; Wang, Z.; Chang, S.; Zhu, S. Oxygen and indocyanine green loaded phase-transition nanoparticle-mediated photo-sonodynamic cytotoxic effects on rheumatoid arthritis fibroblast-like synoviocytes. Int. J. Nanomed. 2017, 12, 381–393. [Google Scholar] [CrossRef]
- Zhao, C.; Rehman, F.U.; Jiang, H.; Selke, M.; Wang, X.; Liu, C.Y. Titanium dioxide-tetra sulphonatophenyl porphyrin nanocomposites for target cellular bio-imaging and treatment of rheumatoid arthritis. Sci. China Chem. 2016, 59, 637–642. [Google Scholar] [CrossRef]
- Dougherty, T.J.; Gomer, C.J.; Henderson, B.W.; Jori, G.; Kessel, D.; Korbelik, M.; Moan, J.; Peng, Q. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [Google Scholar] [CrossRef]
- Rehman, F.U.; Zhao, C.; Wu, C.; Li, X.; Jiang, H.; Selke, M.; Wang, X. Synergy and translation of allogenic bone marrow stem cells after photodynamic treatment of rheumatoid arthritis with tetra sulfonatophenyl porphyrin and TiO2 nanowhiskers. Nano Res. 2016, 9, 3305–3321. [Google Scholar] [CrossRef]
- Lu, Y.; Li, L.; Lin, Z.; Wang, L.; Lin, L.; Li, M.; Zhang, Y.; Yin, Q.; Li, Q.; Xia, H. A New Treatment Modality for Rheumatoid Arthritis: Combined Photothermal and Photodynamic Therapy Using Cu7.2S4 Nanoparticles. Adv. Healthc. Mater. 2018, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Alexeree, S.M.; Sliem, M.A.; El-Balshy, R.M.; Amin, R.M.; Harith, M.A. Exploiting biosynthetic gold nanoparticles for improving the aqueous solubility of metal-free phthalocyanine as biocompatible PDT agent. Mater. Sci. Eng. C 2017, 76, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.R.; Khodadadi, A.; Hadizadeh, M. A nanoporous photosensitizing hydrogel based on chitosan cross-linked by zinc phthalocyanine: An injectable and pH-stimuli responsive system for effective cancer therapy. RSC Adv. 2016, 6, 91445–91452. [Google Scholar] [CrossRef]
- Tian, N.; Sun, W.; Guo, X.; Lu, J.; Li, C.; Hou, Y.; Wang, X.; Zhou, Q. Mitochondria targeted and NADH triggered photodynamic activity of chloromethyl modified Ru(II) complexes under hypoxic conditions. Chem. Commun. 2019, 55, 2676–2679. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.; Freudenreich, J.; Barry, N.P.; Juillerat-Jeanneret, L.; Süss-Fink, G.; Therrien, B. Organometallic cages as vehicles for intracellular release of photosensitizers. J. Am. Chem. Soc. 2012, 134, 754–757. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PS | Activation Wavelength (nm) | Type of Administration | Irradiation Mode | Target/Model | Ref. |
|---|---|---|---|---|---|
| [Na][ATX-S10] | 670 | intravenous | trans-cutaneous | FLS/mice | [44] |
| BPD-MA | 690 | intravenous | trans-cutaneous | MRL-lpr mice (FCA) | [14] |
| BPD-MA | 690 | intravenous | intra-anticular | rabbit | [18] |
| BPD-MA lyposomal | 690 | intravenous/intra-articular | trans-cutaneous/intra-articular | NZW rabbit (FCA) | [16] |
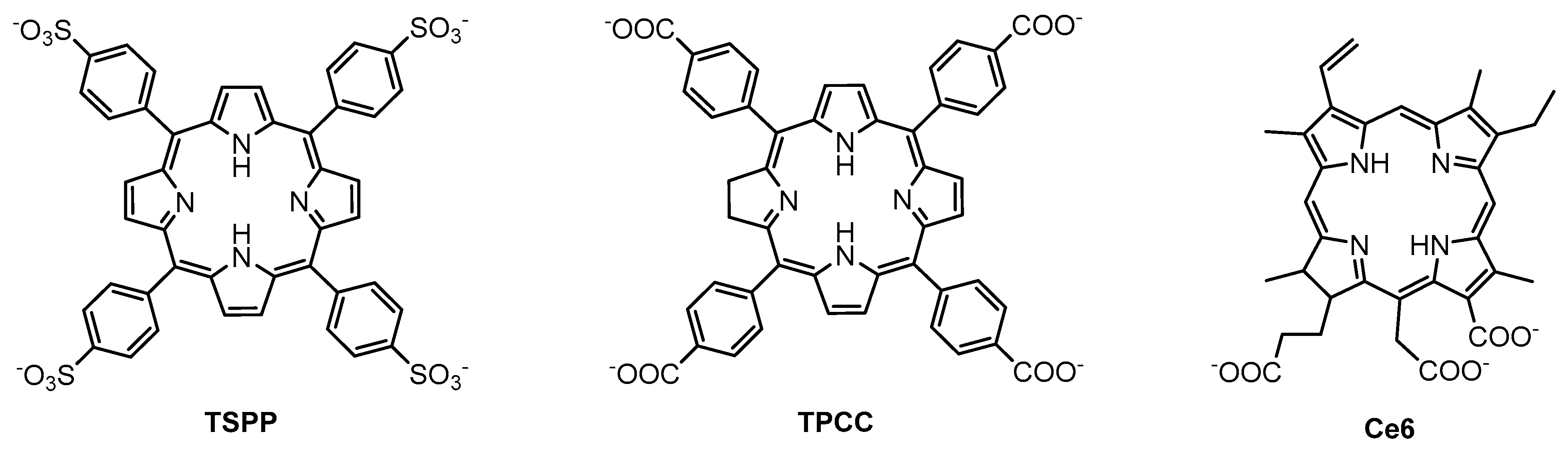
| Ce6 | 652 | intra-articular | intra-anticular | human THP-1 and murine RAW 264.7 macrophages/mice | [76] |
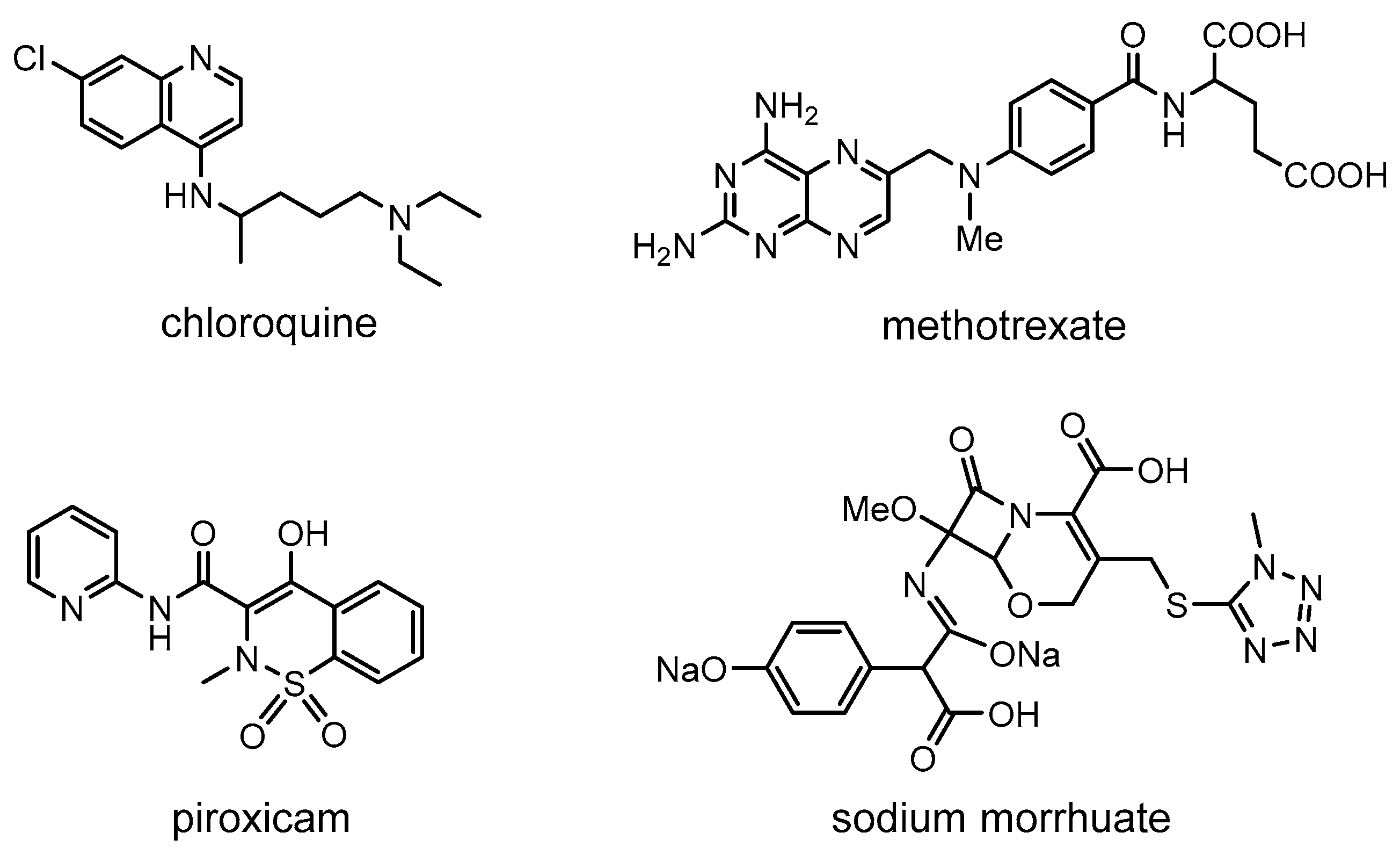
| Chloroquine | 351 | NA | ND | FLS | [58] |
| Cu7.2S4 nanoparticles | 808 | intra-articular | trans-cutaneous | FLS/murine | [80] |
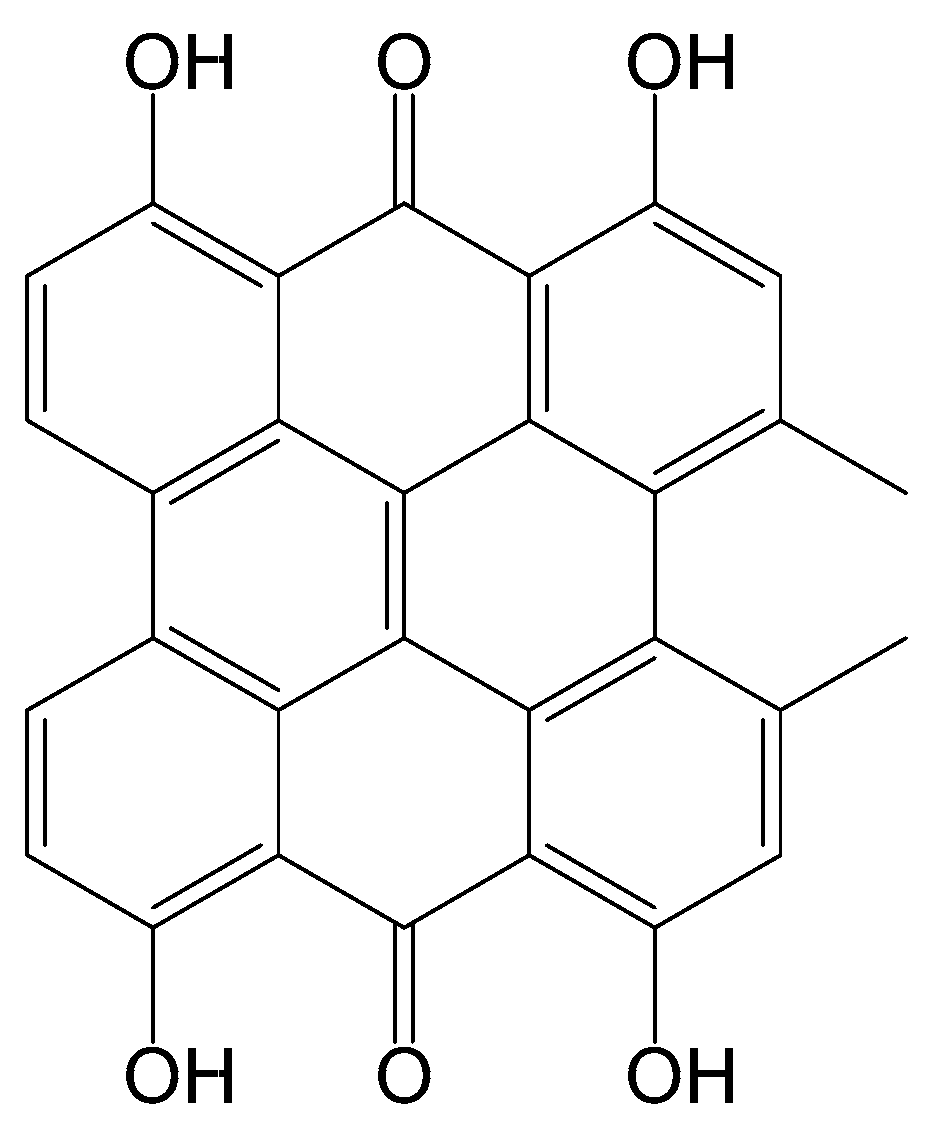
| Hypericin | 593 | NA | ND | FLS | [75] |
| ICG | 780 | NA | ND | FLS | [65] |
| Methotrexate | 450, 550, 590, 660, and 850 | intra-articular | trans-cutaneous | goat/chicken | [64] |
| Methotrexate | 351 | NA | ND | FLS | [58] |
| m-THPC | 652 | intravenous | trans-cutaneous | mice | [46] |
| Pheophorbide A (T-PS) | 665 | intravenous | trans-cutaneous | murine | [57] |
| Photofrin | 630 | intravenous | intra-anticular | NZW rabbit | [29] |
| Photosan-3 | 630 | intravenous/intra-articular | intra-anticular | FLS/rabbit | [34,36] |
| Piroxicam | 351 | NA | ND | FLS | [58] |
| PpIX | 635 | intra-articular | trans-cutaneous | FLS/mice | [42] |
| PpIX | 635 | intra-articular | trans-cutaneous | rabbit | [43] |
| Sodium morrhuate | 351 | NA | ND | FLS | [58] |
| Talaporfin | 664 | intra-articular | intra-articular | FLS/mice/rat | [45] |
| TPCC | 652 | intra-articular | intra-articular | human THP-1 and murine RAW 264.7 macrophages/mice | [76] |
| TPPS2A | 435 | NA | ND | FLS | [47] |
| TSPP | 652 | intra-articular | intra-articular | human THP-1 and murine RAW 264.7 macrophages/mice | [76] |
| TSPP-TiO2 nanoparticle | 490 | NA | ND | FLS/bone marrow stromal cells | [77,79] |
| TSPP-TiO2 nanoparticle | 500–550 | intravenous | trans-cutaneous | murine | [77] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallardo-Villagrán, M.; Leger, D.Y.; Liagre, B.; Therrien, B. Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis. Int. J. Mol. Sci. 2019, 20, 3339. https://doi.org/10.3390/ijms20133339
Gallardo-Villagrán M, Leger DY, Liagre B, Therrien B. Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis. International Journal of Molecular Sciences. 2019; 20(13):3339. https://doi.org/10.3390/ijms20133339
Chicago/Turabian StyleGallardo-Villagrán, Manuel, David Yannick Leger, Bertrand Liagre, and Bruno Therrien. 2019. "Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis" International Journal of Molecular Sciences 20, no. 13: 3339. https://doi.org/10.3390/ijms20133339
APA StyleGallardo-Villagrán, M., Leger, D. Y., Liagre, B., & Therrien, B. (2019). Photosensitizers Used in the Photodynamic Therapy of Rheumatoid Arthritis. International Journal of Molecular Sciences, 20(13), 3339. https://doi.org/10.3390/ijms20133339