The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias


 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Concordance between the Q-LAMP Assay and the Standard BIOMED-1 Method on p210 and p190 BCR-ABL1 Isoforms
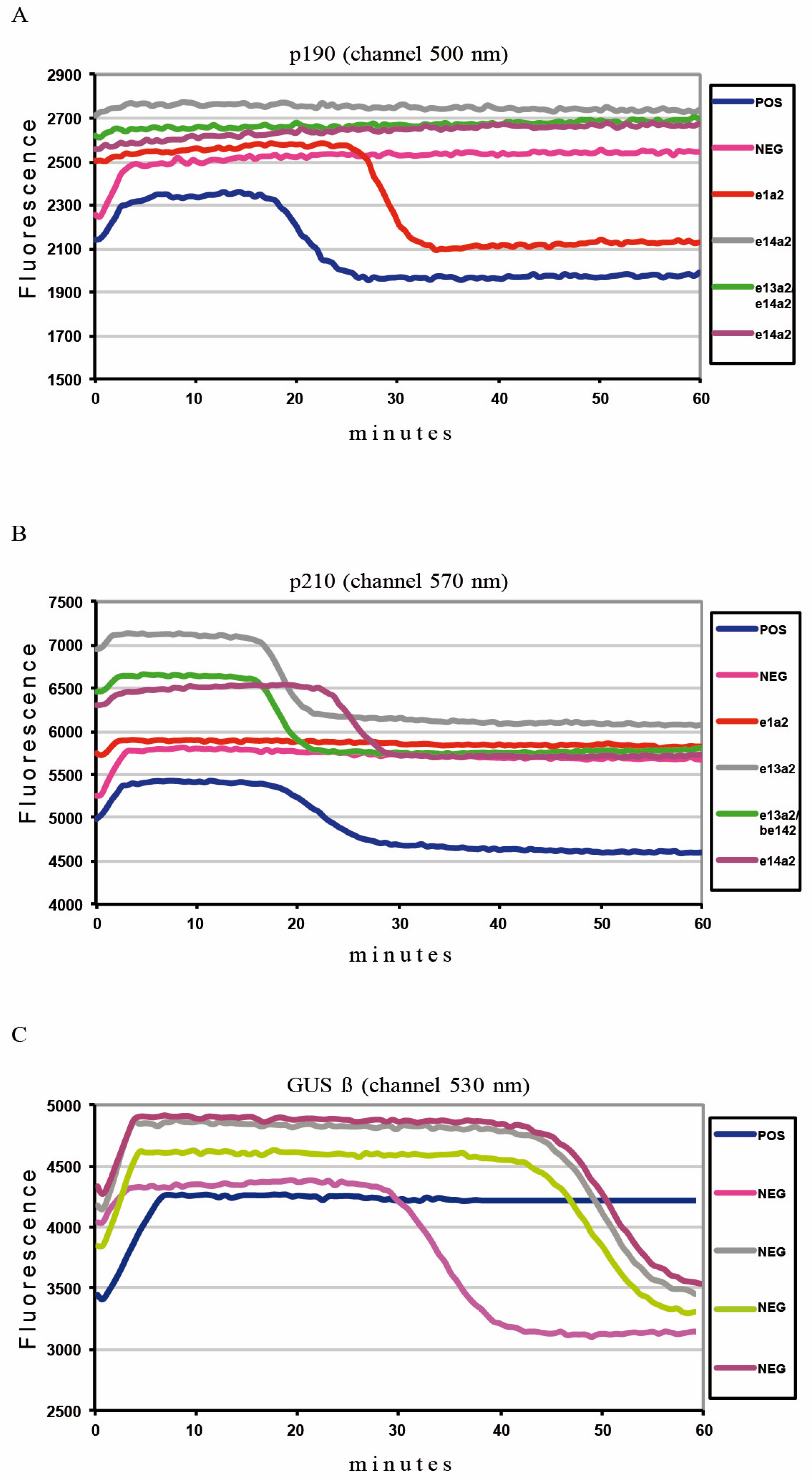
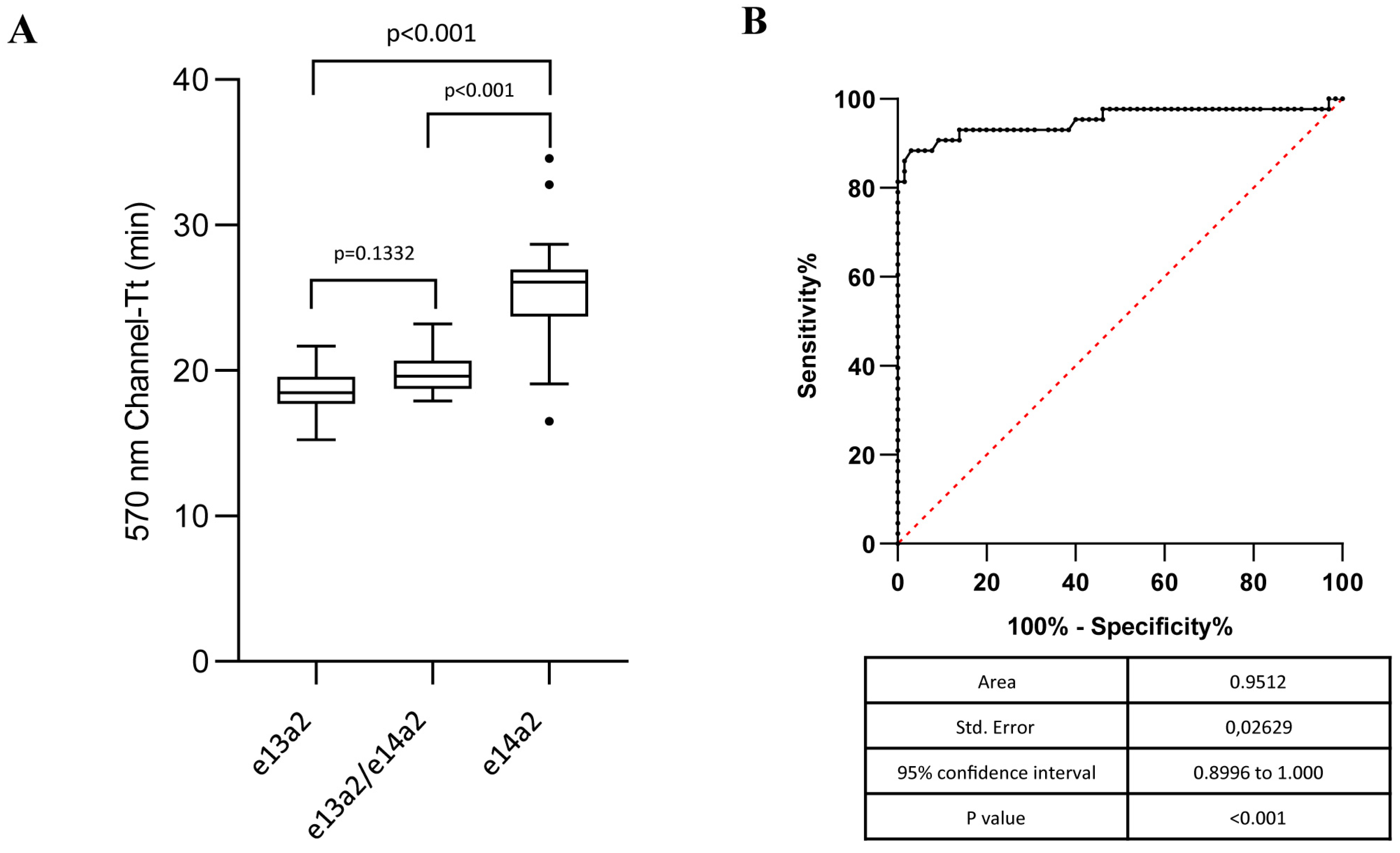
2.2. Q-LAMP Performance on Common BCR-ABL1 p210 Isoforms
2.3. Concordance between the Q-LAMP Assay and the Standard BIOMED-1 Method on Rare p210 and p190 BCR-ABL1 Isoforms
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. RNA Extraction
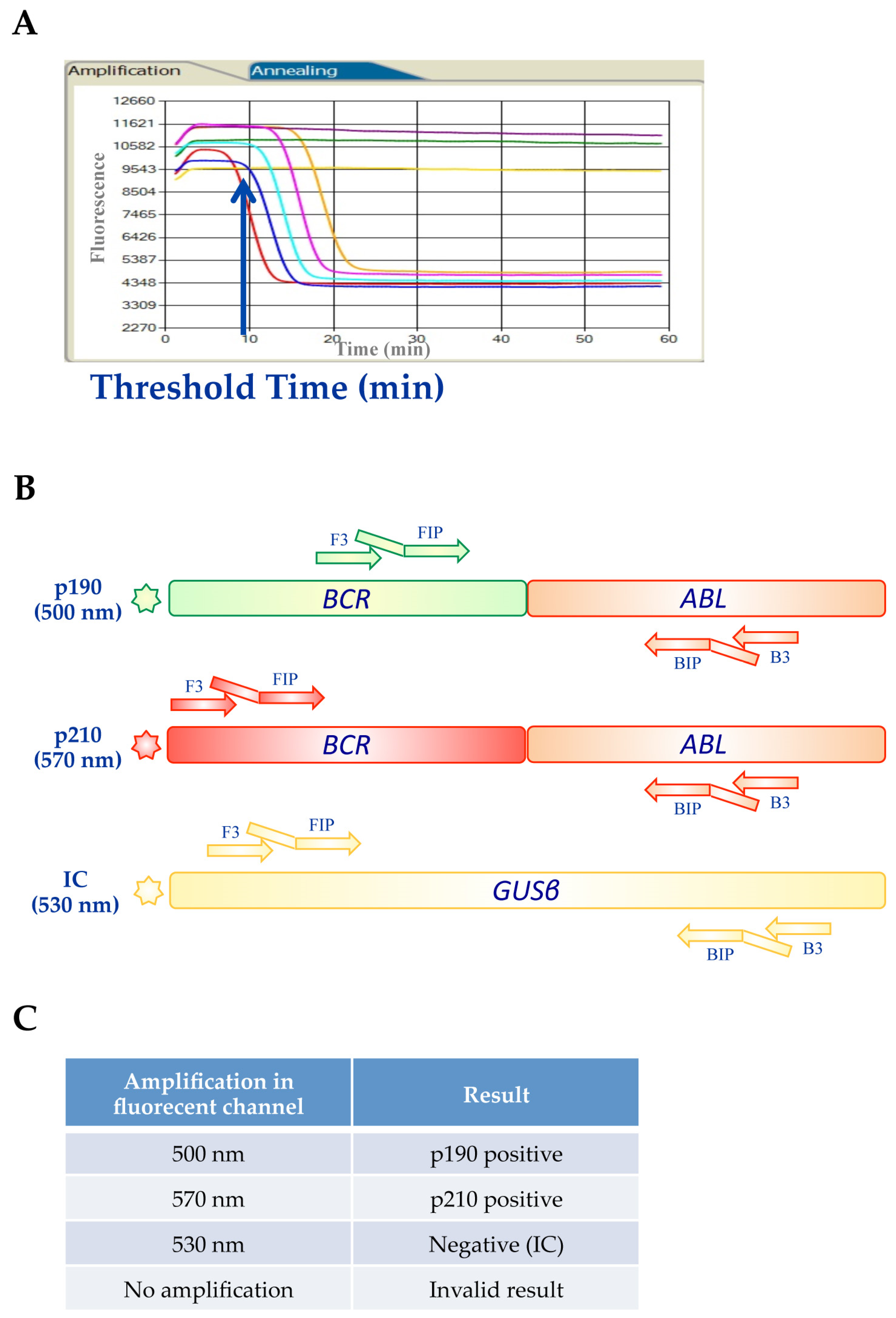
4.3. BCR-ABL1 Q-LAMP Assay
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ABL1 | Abelson murine leukemia |
| ALL | acute lymphoblastic leukemia |
| BCR | breakpoint cluster region |
| CML | chronic myeloid leukemia |
| GUSβ | β-glucuronidase |
| LAMP | loop-mediated isothermal amplification |
| ROC | receiver operating characteristic |
| TK | tyrosine kinase |
| TKI | tyrosine kinase inhibitor |
| TFR | treatment-free remission |
References
- Foroni, L.; Wilson, G.; Gerrard, G.; Mason, J.; Grimwade, D.; White, H.E.; De Castro, D.G.; Austin, S.; Awan, A.; Burt, E.; et al. Guidelines for the measurement of BCR-ABL1 transcripts in chronic myeloid leukaemia. Br. J. Haematol. 2011, 153, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, C.A.; Hooberman, A.L.; Spino, C.; Dodge, R.K.; Larson, R.A.; Davey, F.; Wurster-Hill, D.H.; Sobol, R.E.; Schiffer, C.; Bloomfield, C.D. Clinical significance of the BCR-ABL fusion gene in adult acute lymphoblastic leukemia: A Cancer and Leukemia Group B Study (8762). Blood 1992, 80, 2983–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimaki, K.; Hattori, Y.; Nakajima, H. 10-year complete remission in a Philadelphia chromosome-positive acute lymphoblastic leukemia patient using imatinib without high-intensity chemotherapy or allogeneic stem cell transplantation. Int. J. Hematol. 2018, 107, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Apperley, J.F. Chronic myeloid leukaemia. Lancet 2015, 385, 1447–1459. [Google Scholar] [CrossRef]
- Stagno, F.; Stella, S.; Spitaleri, A.; Pennisi, M.S.; Di Raimondo, F.; Vigneri, P. Imatinib mesylate in chronic myeloid leukemia: Frontline treatment and long-term outcomes. Expert Rev. Anticancer Ther. 2016, 16, 273–278. [Google Scholar] [CrossRef]
- Quintas-Cardama, A.; Cortes, J. Molecular biology of bcr-abl1-positive chronic myeloid leukemia. Blood 2009, 113, 1619–1630. [Google Scholar] [CrossRef] [Green Version]
- Giallongo, C.; Parrinello, N.; Tibullo, D.; La Cava, P.; Romano, A.; Chiarenza, A.; Barbagallo, I.; Palumbo, G.A.; Stagno, F.; Vigneri, P.; et al. Myeloid derived suppressor cells (MDSCs) are increased and exert immunosuppressive activity together with polymorphonuclear leukocytes (PMNs) in chronic myeloid leukemia patients. PLoS ONE 2014, 9, e101848. [Google Scholar] [CrossRef] [Green Version]
- Preyer, M.; Vigneri, P.; Wang, J.Y. Interplay between kinase domain autophosphorylation and F-actin binding domain in regulating imatinib sensitivity and nuclear import of BCR-ABL. PLoS ONE 2011, 6, e17020. [Google Scholar] [CrossRef]
- Manzella, L.; Tirro, E.; Pennisi, M.S.; Massimino, M.; Stella, S.; Romano, C.; Vitale, S.R.; Vigneri, P. Roles of Interferon Regulatory Factors in Chronic Myeloid Leukemia. Curr. Cancer Drug Targ. 2016, 16, 594–605. [Google Scholar] [CrossRef]
- Jain, P.; Kantarjian, H.; Patel, K.P.; Gonzalez, G.N.; Luthra, R.; Kanagal Shamanna, R.; Sasaki, K.; Jabbour, E.; Romo, C.G.; Kadia, T.M.; et al. Impact of BCR-ABL transcript type on outcome in patients with chronic-phase CML treated with tyrosine kinase inhibitors. Blood 2016, 127, 1269–1275. [Google Scholar] [CrossRef]
- Jinawath, N.; Norris-Kirby, A.; Smith, B.D.; Gocke, C.D.; Batista, D.A.; Griffin, C.A.; Murphy, K.M. A rare e14a3 (b3a3) BCR-ABL fusion transcript in chronic myeloid leukemia: Diagnostic challenges in clinical laboratory practice. J. Mol. Diagn. JMD 2009, 11, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Fujisawa, S.; Nakamura, S.; Naito, K.; Kobayashi, M.; Ohnishi, K. A variant transcript, e1a3, of the minor BCR-ABL fusion gene in acute lymphoblastic leukemia: Case report and review of the literature. Int. J. Hematol. 2008, 87, 184–188. [Google Scholar] [CrossRef]
- Massimino, M.; Stella, S.; Tirro, E.; Consoli, M.L.; Pennisi, M.S.; Puma, A.; Vitale, S.R.; Romano, C.; Zammit, V.; Stagno, F.; et al. Efficacy of Dasatinib in a Very Elderly CML Patient Expressing a Rare E13a3 Bcr-Abl1 Fusion Transcript: A Case Report. Anticancer Res. 2019, 39, 3949–3954. [Google Scholar] [CrossRef]
- Massimino, M.; Stella, S.; Tirro, E.; Consoli, M.L.; Pennisi, M.S.; Puma, A.; Vitale, S.R.; Romano, C.; Zammit, V.; Stagno, F.; et al. Rapid decline of Philadelphia-positive metaphases after nilotinib treatment in a CML patient expressing a rare e14a3 BCR-ABL1 fusion transcript: A case report. Oncol. Lett. 2019, 18, 2648–2653. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.M.; Harris, R.J.; Giannoudis, A.; Davies, A.; Knight, K.; Watmough, S.J.; Wang, L.; Clark, R.E. Chronic myeloid leukemia patients with the e13a2 BCR-ABL fusion transcript have inferior responses to imatinib compared to patients with the e14a2 transcript. Haematologica 2009, 94, 1362–1367. [Google Scholar] [CrossRef] [Green Version]
- Hanfstein, B.; Lauseker, M.; Hehlmann, R.; Saussele, S.; Erben, P.; Dietz, C.; Fabarius, A.; Proetel, U.; Schnittger, S.; Haferlach, C.; et al. Distinct characteristics of e13a2 versus e14a2 BCR-ABL1 driven chronic myeloid leukemia under first-line therapy with imatinib. Haematologica 2014, 99, 1441–1447. [Google Scholar] [CrossRef]
- Bonifacio, M.S.; Binotto, G.; De Marchi, F.; Maino, E.; Calistri, E.; Bonalumi, A.; Frison, L.; Marin, L.; Medeot, M.; De Matteis, G.; et al. Predictive Factors of Stable Deep Molecular Response in Chronic Myeloid Leukemia Patients Treated with Imatinib Standard Dose: A Study from the Gruppo Triveneto LMC. Blood 2015, 126, 597. [Google Scholar] [CrossRef]
- Vigneri, P.; Stagno, F.; Stella, S.; Cupri, A.; Forte, S.; Massimino, M.; Antolino, A.; Siragusa, S.; Mannina, D.; Impera, S.S.; et al. High BCR-ABL/GUS(IS) Levels at Diagnosis of Chronic Phase CML Are Associated with Unfavorable Responses to Standard-Dose Imatinib. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 7189–7198. [Google Scholar] [CrossRef] [Green Version]
- Castagnetti, F.; Gugliotta, G.; Breccia, M.; Iurlo, A.; Levato, L.; Albano, F.; Vigneri, P.; Abruzzese, E.; Rossi, G.; Rupoli, S.; et al. The BCR-ABL1 transcript type influences response and outcome in Philadelphia chromosome-positive chronic myeloid leukemia patients treated frontline with imatinib. Am. J. Hematol. 2017, 92, 797–805. [Google Scholar] [CrossRef] [Green Version]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef]
- Bassan, R.; Rossi, G.; Pogliani, E.M.; Di Bona, E.; Angelucci, E.; Cavattoni, I.; Lambertenghi-Deliliers, G.; Mannelli, F.; Levis, A.; Ciceri, F.; et al. Chemotherapy-phased imatinib pulses improve long-term outcome of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: Northern Italy Leukemia Group protocol 09/00. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 3644–3652. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, E.; Kantarjian, H.; Ravandi, F.; Thomas, D.; Huang, X.; Faderl, S.; Pemmaraju, N.; Daver, N.; Garcia-Manero, G.; Sasaki, K.; et al. Combination of hyper-CVAD with ponatinib as first-line therapy for patients with Philadelphia chromosome-positive acute lymphoblastic leukaemia: A single-centre, phase 2 study. Lancet. Oncol. 2015, 16, 1547–1555. [Google Scholar] [CrossRef] [Green Version]
- Pirosa, M.C.; Leotta, S.; Cupri, A.; Stella, S.; Martino, E.A.; Scalise, L.; Sapienza, G.; Calafiore, V.; Mauro, E.; Spadaro, A.; et al. Long-Term Molecular Remission Achieved by Antibody Anti-CD22 and Ponatinib in a Patient Affected by Ph’+ Acute Lymphoblastic Leukemia Relapsed after Second Allogeneic Hematopoietic Stem Cell Transplantation: A Case Report. Chemotherapy 2018, 63, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Stella, S.; Massimino, M.; Tirro, E.; Vitale, S.R.; Scalise, L.; Leotta, S.; Pennisi, M.S.; Puma, A.; Romano, C.; Stagno, F.; et al. B-ALL Relapses After Autologous Stem Cell Transplantation Associated With a Shift from e1a2 to e14a2 BCR-ABL Transcripts: A Case Report. Anticancer Res. 2019, 39, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Van Dongen, J.J.; Macintyre, E.A.; Gabert, J.A.; Delabesse, E.; Rossi, V.; Saglio, G.; Gottardi, E.; Rambaldi, A.; Dotti, G.; Griesinger, F.; et al. Standardized RT-PCR analysis of fusion gene transcripts from chromosome aberrations in acute leukemia for detection of minimal residual disease. Report of the BIOMED-1 Concerted Action: Investigation of minimal residual disease in acute leukemia. Leukemia 1999, 13, 1901–1928. [Google Scholar] [CrossRef]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, e63. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Qu, G.; Guo, S.; Ma, L.; Zhang, N.; Zhang, S.; Gao, S.; Shen, Z. Applications of loop-mediated isothermal DNA amplification. Appl. Biochem. Biotechnol. 2011, 163, 845–850. [Google Scholar] [CrossRef]
- Nakao, R.; Stromdahl, E.Y.; Magona, J.W.; Faburay, B.; Namangala, B.; Malele, I.; Inoue, N.; Geysen, D.; Kajino, K.; Jongejan, F.; et al. Development of loop-mediated isothermal amplification (LAMP) assays for rapid detection of Ehrlichia ruminantium. BMC Microbiol. 2010, 10, 296. [Google Scholar] [CrossRef] [Green Version]
- Soleimani, M.; Shams, S.; Majidzadeh, A.K. Developing a real-time quantitative loop-mediated isothermal amplification assay as a rapid and accurate method for detection of Brucellosis. J. Appl. Microbiol. 2013, 115, 828–834. [Google Scholar] [CrossRef]
- Spinelli, O.; Rambaldi, A.; Rigo, F.; Zanghi, P.; D’Agostini, E.; Amicarelli, G.; Colotta, F.; Divona, M.; Ciardi, C.; Coco, F.L.; et al. Simple, rapid and accurate molecular diagnosis of acute promyelocytic leukemia by loop mediated amplification technology. Oncoscience 2015, 2, 50–58. [Google Scholar] [CrossRef]
- Minnucci, G.; Amicarelli, G.; Salmoiraghi, S.; Spinelli, O.; Guinea Montalvo, M.L.; Giussani, U.; Adlerstein, D.; Rambaldi, A. A novel, highly sensitive and rapid allele-specific loop-mediated amplification assay for the detection of the JAK2V617F mutation in chronic myeloproliferative neoplasms. Haematologica 2012, 97, 1394–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmoiraghi, S.; Montalvo, M.L.; D’Agostini, E.; Amicarelli, G.; Minnucci, G.; Spinelli, O.; Rambaldi, A. Mutations and chromosomal rearrangements of JAK2: Not only a myeloid issue. Expert Rev. Hematol. 2013, 6, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Salmoiraghi, S.; Minnucci, G.; Amicarelli, G.; Zanghi, P.; Elidi, L.; Montalvo, M.L.G.; Rigo, F.; D’Agostini, E.; Tettamanzi, V.; Giachelia, M.; et al. Development of new tools for molecular diagnosis of hematologic malignancies. Biochim. Clin. 2016, 40, 234–243. [Google Scholar]
- Hochhaus, A.; Larson, R.A.; Guilhot, F.; Radich, J.P.; Branford, S.; Hughes, T.P.; Baccarani, M.; Deininger, M.W.; Cervantes, F.; Fujihara, S.; et al. Long-Term Outcomes of Imatinib Treatment for Chronic Myeloid Leukemia. N. Engl. J. Med. 2017, 376, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Maino, E.; Sancetta, R.; Viero, P.; Imbergamo, S.; Scattolin, A.M.; Vespignani, M.; Bassan, R. Current and future management of Ph/BCR-ABL positive ALL. Expert Rev. Anticancer Ther. 2014, 14, 723–740. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.E.; Polydoros, F.; Apperley, J.F.; Milojkovic, D.; Pocock, C.; Smith, G.; Byrne, J.L.; De Lavallade, H.; O’Brien, S.G.; Coffey, T.; et al. De-escalation of tyrosine kinase inhibitor dose in patients with chronic myeloid leukaemia with stable major molecular response (DESTINY): An interim analysis of a non-randomised, phase 2 trial. Lancet. Haematol. 2017, 4, e310–e316. [Google Scholar] [CrossRef] [Green Version]
- D’Adda, M.; Farina, M.; Schieppati, F.; Borlenghi, E.; Bottelli, C.; Cerqui, E.; Ferrari, S.; Gramegna, D.; Pagani, C.; Passi, A.; et al. The e13a2 BCR-ABL transcript negatively affects sustained deep molecular response and the achievement of treatment-free remission in patients with chronic myeloid leukemia who receive tyrosine kinase inhibitors. Cancer 2019, 125, 1674–1682. [Google Scholar] [CrossRef]
- Baccarani, M.; Castagnetti, F.; Gugliotta, G.; Rosti, G.; Soverini, S.; Albeer, A.; Pfirrmann, M.; International BCR-ABL Study Group. The proportion of different BCR-ABL1 transcript types in chronic myeloid leukemia. An international overview. Leukemia 2019, 33, 1173–1183. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Results by Conventional RT-PCR (BIOMED-1) | |||||
|---|---|---|---|---|---|
| p190 | p210 | Negative | Total | ||
| Q-LAMP Assay | p190 | 14 | / | / | 14 |
| p210 | / | 108 | / | 107 | |
| Negative | / | / | 50 | 50 | |
| Total | 14 | 108 | 50 | 172 | |
| Isoform (N Sample) | Mean Tt * (st. dev) | Median Tt * (Range) | CV |
|---|---|---|---|
| e1a2 | 27.03 | 26.70 | 0.07 |
| (14) | (1.87) | (24.45–31.80) | / |
| e13a2 | 18.64 | 18.48 | 0.08 |
| (44) | (1.41) | (15.25–21.67) | / |
| e14a2 | 25.46 | 26.08 | 0.13 |
| (43) | (3.29) | (16.53–34.57) | / |
| e13a2/e14a2 | 19.84 | 19.63 | 0.06 |
| (21) | (1.29) | (17.93–23.20) | / |
| Results by conventional RT-PCR (BIOMED-1) | ||||||
|---|---|---|---|---|---|---|
| e1a3 | e13a3 (b2a3) | e14a2 (b3a3) | e19a2 | Total | ||
| Q-LAMP Assay | e1a3 | 5 | / | / | / | 5 |
| e13a2 (b2a3) | / | 9 | / | / | 9 | |
| e14a2 (b3a3) | / | / | 3 | / | 3 | |
| e19a2 | / | / | / | 3 | 3 | |
| Total | 5 | 9 | 3 | 3 | 20 | |
| Q-LAMP Assay | BIOMED-1 Method | |
|---|---|---|
| Nucleic acid input (RNA ng/sample) | RNA (500) | cDNA (1000) |
| Number of steps | 1 | ≥3 |
| Reaction setup | Easy | Moderately complex (RT-PCR is required) |
| Detection of rare BCR-ABL1 isoforms | Possible | Possible |
| Time to results (minutes) | <60 | >300 |
| Mark | CE/IVD | LDT |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stella, S.; Gottardi, E.M.; Favout, V.; Barragan Gonzalez, E.; Errichiello, S.; Vitale, S.R.; Fava, C.; Luciano, L.; Stagno, F.; Grimaldi, F.; et al. The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias. Int. J. Mol. Sci. 2019, 20, 6106. https://doi.org/10.3390/ijms20246106
Stella S, Gottardi EM, Favout V, Barragan Gonzalez E, Errichiello S, Vitale SR, Fava C, Luciano L, Stagno F, Grimaldi F, et al. The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias. International Journal of Molecular Sciences. 2019; 20(24):6106. https://doi.org/10.3390/ijms20246106
Chicago/Turabian StyleStella, Stefania, Enrico Marco Gottardi, Valeria Favout, Eva Barragan Gonzalez, Santa Errichiello, Silvia Rita Vitale, Carmen Fava, Luigia Luciano, Fabio Stagno, Francesco Grimaldi, and et al. 2019. "The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias" International Journal of Molecular Sciences 20, no. 24: 6106. https://doi.org/10.3390/ijms20246106
APA StyleStella, S., Gottardi, E. M., Favout, V., Barragan Gonzalez, E., Errichiello, S., Vitale, S. R., Fava, C., Luciano, L., Stagno, F., Grimaldi, F., Pironi, L., Sargas Simarro, C., Vigneri, P., & Izzo, B. (2019). The Q-LAMP Method Represents a Valid and Rapid Alternative for the Detection of the BCR-ABL1 Rearrangement in Philadelphia-Positive Leukemias. International Journal of Molecular Sciences, 20(24), 6106. https://doi.org/10.3390/ijms20246106