Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study

 and
and
Abstract
:1. Introduction
2. Results
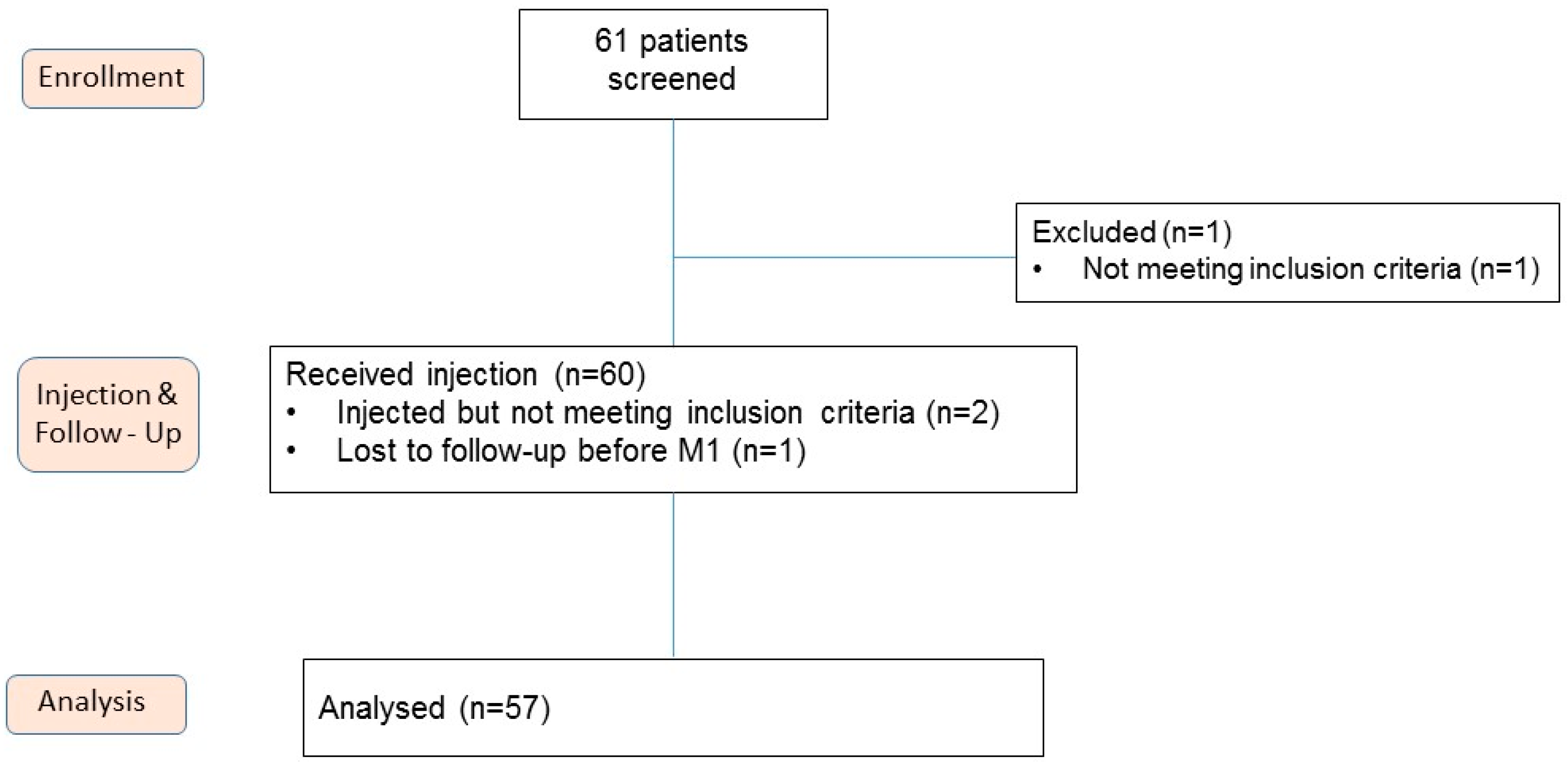
2.1. Characteristics of Patients
2.2. Biological Characteristics of PRP
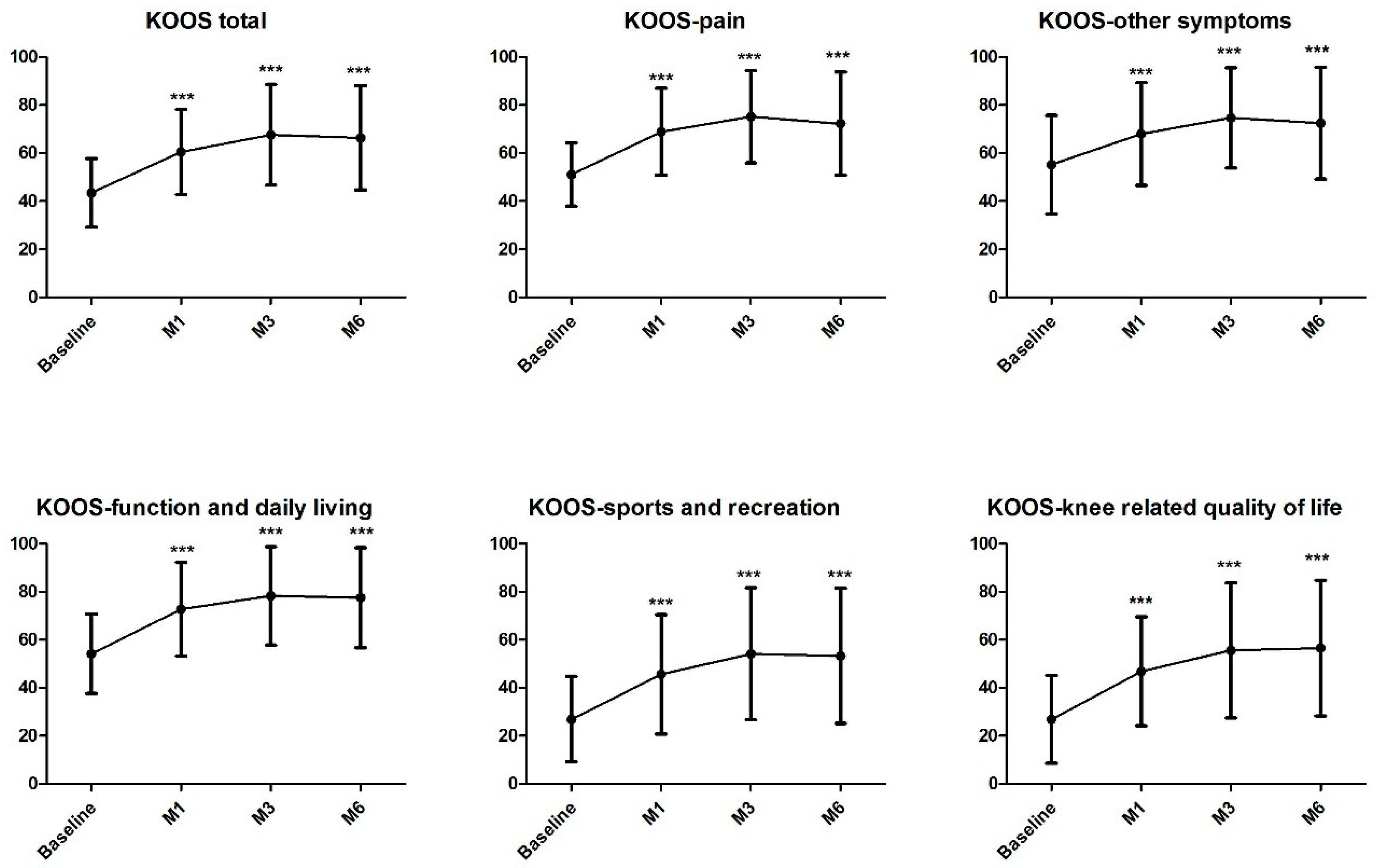
2.3. Effect of Single Autologous PRP Injection in Knee OA
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Study Design and Intervention
4.3. Autologous PRP Preparation Method
4.4. Injection
4.5. Evaluation Tools and Follow-Up
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lane, N.E.; Brandt, K.; Hawker, G.; Peeva, E.; Schreyer, E.; Tsuji, W.; Hochberg, M.C. OARSI-FDA initiative: Defining the disease state of osteoarthritis. Osteoarthr. Cartil. 2011, 19, 478–482. [Google Scholar] [CrossRef]
- Barbour, K.E.; Helmick, C.G.; Boring, M.; Zhang, X.; Lu, H.; Holt, J.B. Prevalence of Doctor-Diagnosed Arthritis at State and County Levels—United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T.; Zhang, Y.; Anthony, J.M.; Naimark, A.; Anderson, J.J. Weight loss reduces the risk for symptomatic knee osteoarthritis in woman. The Framingham Study. Ann. Intern. Med. 1992, 116, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Campbell, J.; Welch, V.; Gee, T.L.; Bourne, R.; Wells, G.A. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. 2006, 19, CD005328. [Google Scholar]
- Hepper, C.T.; Halvorson, J.J.; Duncan, S.T.; Gregory, A.J.; Dunn, W.R.; Spindler, K.P. The efficacy and duration of intra-articular corticosteroid injection for knee osteoarthritis: A systematic review of level I studies. J. Am. Acad. Orthop. Surg. 2009, 17, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Natov, N.S.; Obadan, I.E.; Price, L.L.; Schmid, C.H.; McAlindon, T.E. Therapeutic trajectory of hyaluronic acid versus corticosteroids in the treatment of knee osteoarthritis: A systematic review and meta-analysis. Arthritis Rheum. 2009, 61, 1704–1711. [Google Scholar] [CrossRef] [PubMed]
- Gregori, D.; Giacovelli, G.; Minto, C.; Barbetta, B.; Gualtieri, F.; Azzolina, D.; Vaghi, P.; Rovati, L.C. Association of Pharmacological Treatments with Long-term Pain Control in Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis. JAMA 2018, 320, 2564–2579. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.A. AAOS clinical practice guidelines. Treatment of osteoarthritis of the knee: Evidence-based guideline, 2ded. J. Am. Acad. Orthop. Surg. 2013, 21, 577–579. [Google Scholar] [PubMed]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.L.; Zhou, A.G.; Zhang, H.; Zhang, J. Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Trials. Arthroscopy 2017, 33, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Hunt, T.J. Editorial Commentary: The Time Has Come to Try Intra-articular Platelet-Rich Plasma Injections for Your Patients with Symptomatic Knee Osteoarthritis. Arthroscopy 2017, 33, 671–672. [Google Scholar] [CrossRef]
- Magalon, J.; Bausset, O.; Serratrice, N.; Giraudo, L.; Aboudou, H.; Veran, J.; Magalon, G.; Dignat-Georges, F.; Sabatier, F. Characterization and comparison of 5 Platelet-Rich Plasma preparations in a single donor model. Arthroscopy 2014, 30, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Castillo, T.N.; Pouliot, M.A.; Kim, H.J.; Dragoo, J.L. Comparion of growth factor and platelet concentration from commercial platelet-rich plasma separation systems. Am. J. Sports Med. 2011, 39, 266–271. [Google Scholar] [CrossRef]
- Riboh, J.C.; Saltzman, B.M.; Yanke, A.B.; Fortier, L.; Cole, B.J. Effect of leukocyte concentration on the efficacy of Platelet rich Plasma in the treatment of knee osteoarthritis. Am. J. Sports Med. 2016, 44, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, M.; Vílchez-Cavazos, J.F.; Peña-Martínez, V.M.; Said-Fernández, S.; Lara-Arias, J.; Martínez-Rodríguez, H.G. Leukocyte-poor platelet-rich plasma is more effective than the conventional therapy with acetaminophen for the treatment of early knee osteoarthritis. Arch. Orthop. Trauma Surg. 2016, 136, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.R.; Rodeo, S.; Bhutani, N.; Goodrich, L.R.; Huard, J.; Irrgang, J.; LaPrade, R.F.; Lattermann, C.; Lu, Y.; Mandelbaum, B.; et al. Optimizing Clinical Use of Biologics in Orthopaedic Surgery: Consensus Recommendations from the 2018 AAOS/NIH U-13 Conference. J. Am. Acad. Orthop. Surg. 2019, 27, e50–e63. [Google Scholar] [CrossRef] [PubMed]
- Magalon, J.; Chateau, A.L.; Bertrand, B.; Louis, M.L.; Silvestre, A.; Giraudo, L.; Veran, J.; Sabatier, F. DEPA classification: A proposal for standardising PRP use and a retrospective application of available devices. BMJ Open Sport Exerc. Med. 2016, 2, e000060. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.K.; Davis, K.W.; Ross, A.; Rosas, H.G. Fundamentals of Joint Injection. Am. J. Roentgenol. 2016, 207, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Louis, M.L.; Magalon, J.; Jouve, E.; Bornet, C.E.; Mattei, J.C.; Chagnaud, C.; Rochwerger, A.; Veran, J.; Sabatier, F. Growth Factors Levels Determine Efficacy of Platelets Rich Plasma Injection in Knee Osteoarthritis: A Randomized Double Blind Noninferiority Trial Compared with Viscosupplementation. Arthroscopy 2018, 34, 1530–1540. [Google Scholar] [CrossRef]
- Buendía-López, D.; Medina-Quirós, M.; Marín, M.Á. Clinical and radiographic comparison of a single LP-PRP injection, a single hyaluronic acid injection and daily NSAID administration with a 52-week follow-up: A randomized controlled trial. J. Orthop. Traumatol. 2018, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Lisi, C.; Perotti, C.; Scudeller, L.; Sammarchi, L.; Dametti, F.; Musella, V.; Di Natali, G. Treatment of knee osteoarthritis: Platelet-derived growth factors vs. hyaluronic acid. A randomized controlled trial. Clin. Rehabil. 2018, 32, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Woertler, K.; Buerger, H.; Moeller, J.; Rummeny, E.J. Patellar articular cartilage lesions: in vitro MR imaging evaluation after placement in gadopentetate dimeglumine solution. Radiology 2004, 230, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Robertson, J.; Jones, A.C.; Dieppe, P.A.; Doherty, M. The placebo effect and its determinants in osteoarthritis: Meta-analysis of randomised controlled trials. Ann. Rheum Dis. 2008, 67, 1716–1723. [Google Scholar] [CrossRef] [PubMed]
- Graiet, H.; Lokchine, A.; Francois, P.; Velier, M.; Grimaud, F.; Loyens, M.; Berda-Haddad, Y.; Veran, J.; Dignat-George, F.; Sabatier, F.; et al. Use of platelet-rich plasma in regenerative medicine: Technical tools for correct quality control. BMJ Open Sport Exerc. Med. 2018, 13, e000442. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex, male:female, n | 24:33 |
| Age, year, mean ± SD | 63.3 ± 9.6 |
| BMI, kg/m2, mean ± SD | 25.4 ± 3.9 |
| Symptom duration, mo, mean ± SD | 8.4 ± 9.9 |
| Kellgren Laurence Grade of knee OA grade 2: grade 3, n | 23:34 |
| Previous corticosteroids injection: HA injection, n | 6:42 |
| Flexion, °, mean ± SD | 124.1 ± 10.3 |
| Extension, °, mean ± SD | 15.0 ± 4.6 |
| KOOS total score, mean ± SD | 43.9 ± 14.6 |
| KOOS other symptoms score, mean ± SD | 56.0 ± 20.9 |
| KOOS pain score, mean ± SD | 51.3 ± 13.3 |
| KOOS function in daily living score, mean ± SD | 54.5 ± 17.1 |
| KOOS sport and recreation score, mean ± SD | 27.5 ± 19.0 |
| KOOS quality of life, mean ± SD | 30.3 ± 18.0 |
| Observed Pain on 50-foot walk test (0–100), mean ± SD | 38.6 ± 25.3 |
| Previous week VAS arthrosis activity (0–100) | 57.9 ± 18.4 |
| Previous week VAS damages caused by arthrosis (0–100) | 63.0 ± 19.3 |
| Previous week VAS global health (0–100) | 72.6 ± 16.2 |
| SF-36 PCS (0–100) | 37.1 ± 9.3 |
| SF-36 MCS (0–100) | 40.4 ± 8.9 |
| Mean ± Standard Deviation | |
|---|---|
| Blood | |
| Volume of whole blood collected, mL | 18.0 ± 0.0 |
| Red Blood Cells concentration, T/L | 4.22 ± 0.65 |
| Platelets concentration, G/L | 197 ± 37 |
| Leukocytes concentration, G/L | 5.71 ± 1.22 |
| PRP | |
| Volume of PRP injected, mL | 8.8 ± 1.1 |
| Red Blood Cells concentration, T/L | 0.01 ± 0.01 |
| Platelets concentration, G/L | 288 ± 95 |
| Leukocytes concentration, G/L | 0.22 ± 0.27 |
| Quantity of injected Red Blood Cells, millions | 92 ± 53 |
| Quantity of injected Red Blood Cells (%) | 3.7 ± 2.4 |
| Quantity of injected Platelets, millions | 2517 ± 812 |
| Quantity of injected Platelets (%) | 96.2 ± 2.5 |
| Quantity of injected Leukocytes, millions | 2 ± 2 |
| Quantity of injected Leukocytes (%) | 0.1 ± 0.1 |
| Recovery rate in platelets (%) | 68.3 ± 16.5 |
| Increase factor in platelets | 1.4 ± 0.4 |
| Increase factor in leukocytes | 0.1 ± 0.1 |
| DEPA Classification | CDA |
| Pre-Operative | 6 Months Post Injection | p | |
|---|---|---|---|
| Presence of edema (number of patients) | |||
| Grade 0 | 23 | 26 | p = 1 |
| Grade 1 | 18 | 13 | |
| Grade 2 | 6 | 10 | |
| Grade 3 | 2 | 8 | |
| Presence of joint effusion (number of patients) | p = 1 | ||
| Grade 0 | 14 | 14 | |
| Grade 1 | 17 | 16 | |
| Grade 2 | 14 | 13 | |
| Grade 3 | 4 | 6 | |
| Articular thickness (mm, mean ± SD) | |||
| IFT-F compartment | 1.16 ± 0.72 | 1.14 ± 0.77 | p = 0.72 |
| IFT-T compartment | 1.67 ± 0.85 | 1.64 ± 0.89 | p = 0.82 |
| LFT-F compartment | 1.60 ± 0.60 | 1.62 ± 0.60 | p = 0.75 |
| LFT-T compartment | 2.08 ± 0.91 | 2.14 ± 1.01 | p = 0.26 |
| IFP compartment | 2.27 ± 0.75 | 2.33 ± 0.77 | p = 0.22 |
| LFP compartment | 2.61 ± 1.03 | 2.68 ± 1.06 | p = 0.22 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guillibert, C.; Charpin, C.; Raffray, M.; Benmenni, A.; Dehaut, F.-X.; El Ghobeira, G.; Giorgi, R.; Magalon, J.; Arniaud, D. Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study. Int. J. Mol. Sci. 2019, 20, 1327. https://doi.org/10.3390/ijms20061327
Guillibert C, Charpin C, Raffray M, Benmenni A, Dehaut F-X, El Ghobeira G, Giorgi R, Magalon J, Arniaud D. Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study. International Journal of Molecular Sciences. 2019; 20(6):1327. https://doi.org/10.3390/ijms20061327
Chicago/Turabian StyleGuillibert, Caroline, Caroline Charpin, Marie Raffray, Annie Benmenni, Francois-Xavier Dehaut, Georges El Ghobeira, Roch Giorgi, Jeremy Magalon, and Denis Arniaud. 2019. "Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study" International Journal of Molecular Sciences 20, no. 6: 1327. https://doi.org/10.3390/ijms20061327
APA StyleGuillibert, C., Charpin, C., Raffray, M., Benmenni, A., Dehaut, F. -X., El Ghobeira, G., Giorgi, R., Magalon, J., & Arniaud, D. (2019). Single Injection of High Volume of Autologous Pure PRP Provides a Significant Improvement in Knee Osteoarthritis: A Prospective Routine Care Study. International Journal of Molecular Sciences, 20(6), 1327. https://doi.org/10.3390/ijms20061327