Molecular Aspects and Treatment of Iron Deficiency in the Elderly

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Signs, Symptoms, and Outcomes
3. Pathophysiology
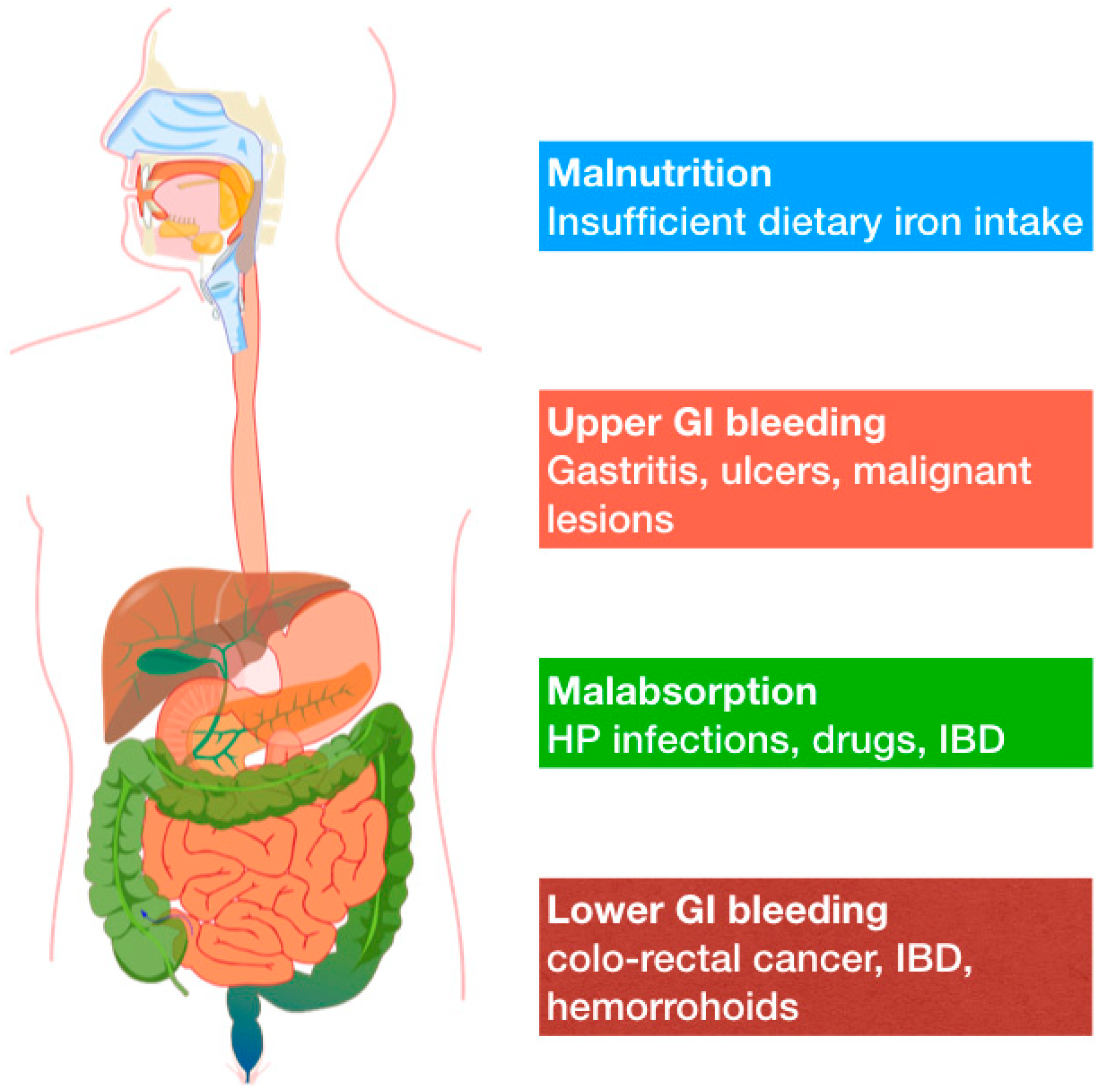
3.1. Etiology
3.2. Molecular Mechanisms
4. Diagnosis
5. Therapy
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Balducci, L.; Ershler, W.B.; Krantz, S. Anemia in the elderly—Clinical findings and impact on health. Crit. Rev. Oncol. Hematol. 2006, 58, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Busti, F.; Campostrini, N.; Martinelli, N.; Girelli, D. Iron deficiency in the elderly population, revisited in the hepcidin era. Front. Pharmacol. 2014, 5. [Google Scholar] [CrossRef]
- Umbreit, J. Iron deficiency: A concise review. Am. J. Hematol. 2005, 78, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Steensma, D.P.; Tefferi, A. Anemia in the Elderly: How Should We Define It, When Does It Matter, and What Can Be Done? Mayo Clin. Proc. 2007, 82, 958–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodnough, L.T.; Schrier, S.L. Evaluation and management of anemia in the elderly. Am. J. Hematol. 2014, 89, 88–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halawi, R.; Moukhadder, H.; Taher, A. Anemia in the elderly: A consequence of aging? Expert Rev. Hematol. 2017, 10, 327–335. [Google Scholar] [CrossRef]
- Stauder, R.; Valent, P.; Theurl, I. Anemia at older age: Etiologies, clinical implications, and management. Blood 2018, 131, 505–514. [Google Scholar] [CrossRef]
- Röhrig, G.; Gütgemann, I.; Kolb, G.; Leischker, A. Anemia in the aged is not ageing related: Position paper on anemia in the aged by the “working group anemia” of the German Geriatric Society (DGG). Eur. Geriatr. Med. 2018, 9, 395–397. [Google Scholar] [CrossRef]
- Van Puyvelde, K.; Cytryn, E.; Mets, T.; Beyer, I. Anaemia in the elderly. Acta Clin. Belg. 2009, 64, 292–302. [Google Scholar] [CrossRef] [Green Version]
- McLean, E.; Cogswell, M.; Egli, I.; Wojdyla, D.; de Benoist, B. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public Health Nutr. 2008, 12, 444. [Google Scholar] [CrossRef] [Green Version]
- Joosten, E. Iron deficiency anemia in older adults: A review. Geriatr. Gerontol. Int. 2017, 18, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Muhammad, A. Role of small bowel capsule endoscopy in the diagnosis and management of iron deficiency anemia in elderly: A comprehensive review of the current literature. World J. Gastroenterol. 2014, 20, 8416. [Google Scholar] [CrossRef] [PubMed]
- Villani, R.; Donatiello, I.; Barone, F.; Cavallone, F.; Fioravanti, G.; Di Cosimo, F.; Bellanti, F.; Sollitto, F.; Vendemiale, G.; Serviddio, G. Efficacy and safety of direct-acting antivirals in elderly with chronic hepatitis C: Results from a retrospective cohort study. J. Gerontol. Geriatr. 2018, 66, 46–55. [Google Scholar]
- Ludwig, H.; Fritz, E.; Leitgeb, C.; Pecherstorfer, M.; Samonigg, H.; Schuster, J. Prediction of response to erythropoietin treatment in chronic anemia of cancer. Blood 1994, 84, 1056–1063. [Google Scholar] [CrossRef] [Green Version]
- Fairweather-Tait, S.J.; Wawer, A.A.; Gillings, R.; Jennings, A.; Myint, P.K. Iron status in the elderly. Mech. Ageing Dev. 2014, 136–137, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Rohrig, G.; Gutgemann, I.; Leischker, A.; Kolb, G. Anemia in the aged—A geriatric syndrome?: Second position paper on anemia in the aged by the working group anemia of the German Geriatric Society. Z. Gerontol. Geriatr. 2018, 51, 921–923. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune-metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Bellanti, F.; Iannelli, G.; Blonda, M.; Tamborra, R.; Villani, R.; Romano, A.; Calcagnini, S.; Mazzoccoli, G.; Vinciguerra, M.; Gaetani, S.; et al. Alterations of Clock Gene RNA Expression in Brain Regions of a Triple Transgenic Model of Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 59, 615–631. [Google Scholar] [CrossRef] [Green Version]
- Gowanlock, Z.; Sriram, S.; Martin, A.; Xenocostas, A.; Lazo-Langner, A. Erythropoietin Levels in Elderly Patients with Anemia of Unknown Etiology. PLoS ONE 2016, 11, e0157279. [Google Scholar] [CrossRef] [Green Version]
- Bellanti, F.; Romano, A.D.; Lo Buglio, A.; Castriotta, V.; Guglielmi, G.; Greco, A.; Serviddio, G.; Vendemiale, G. Oxidative stress is increased in sarcopenia and associated with cardiovascular disease risk in sarcopenic obesity. Maturitas 2018, 109, 6–12. [Google Scholar] [CrossRef]
- Lane, D.; Jansson, P.; Richardson, D. Bonnie and Clyde: Vitamin C and iron are partners in crime in iron deficiency anaemia and its potential role in the elderly. Aging 2016, 8, 1150–1152. [Google Scholar] [CrossRef] [Green Version]
- Cui, Y.; Wu, Q.; Zhou, Y. Iron-refractory iron deficiency anemia: New molecular mechanisms. Kidney Int. 2009, 76, 1137–1141. [Google Scholar] [CrossRef] [Green Version]
- Andrews, N.C.; Schmidt, P.J. Iron homeostasis. Annu. Rev. Physiol. 2007, 69, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T. Hepcidin and its role in regulating systemic iron metabolism. ASH Educ. Program Book 2006. [Google Scholar] [CrossRef]
- Nicolas, G.; Bennoun, M.; Devaux, I.; Beaumont, C.; Grandchamp, B.; Kahn, A.; Vaulont, S. Lack of hepcidin gene expression and severe tissue iron overload in upstream stimulatory factor 2 (USF2) knockout mice. Proc. Natl. Acad. Sci. USA 2001, 98, 8780–8785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolas, G.; Bennoun, M.; Porteu, A.; Mativet, S.; Beaumont, C.; Grandchamp, B.; Sirito, M.; Sawadogo, M.; Kahn, A.; Vaulont, S. Severe iron deficiency anemia in transgenic mice expressing liver hepcidin. Proc. Natl. Acad. Sci. USA 2002, 99, 4596–4601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, D.A.; Roy, C.N.; Fleming, M.D.; Loda, M.F.; Wolfsdorf, J.I.; Andrews, N.C. Inappropriate expression of hepcidin is associated with iron refractory anemia: Implications for the anemia of chronic disease. Blood 2002, 100, 3776–3781. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, R.; Jung, C.L.; Gabayan, V.; Deng, J.C.; Ganz, T.; Nemeth, E.; Bulut, Y. Hepcidin induction by pathogens and pathogen-derived molecules is strongly dependent on interleukin-6. Infect. Immun. 2014, 82, 745–752. [Google Scholar] [CrossRef] [Green Version]
- Romano, A.D.; Greco, E.; Vendemiale, G.; Serviddio, G. Bioenergetics and mitochondrial dysfunction in aging: Recent insights for a therapeutical approach. Curr. Pharm. Des. 2014, 20, 2978–2992. [Google Scholar] [CrossRef]
- Keithi-Reddy, S.R.; Addabbo, F.; Patel, T.V.; Mittal, B.V.; Goligorsky, M.S.; Singh, A.K. Association of anemia and erythropoiesis stimulating agents with inflammatory biomarkers in chronic kidney disease. Kidney Int. 2008, 74, 782–790. [Google Scholar] [CrossRef] [Green Version]
- Besarab, A.; Hemmerich, S. Iron-Deficiency Anemia. In Management of Anemia; Springer: New York, NY, USA, 2017; pp. 11–29. [Google Scholar]
- Rangel, I.; Gonçalves, A.; de Sousa, C.; Leite, S.; Campelo, M.; Martins, E.; Amorim, S.; Moura, B.; Silva Cardoso, J.; Maciel, M.J. Iron Deficiency Status Irrespective of Anemia: A Predictor of Unfavorable Outcome in Chronic Heart Failure Patients. Cardiology 2014, 128, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Abitbol, V.; Borderie, D.; Polin, V.; Maksimovic, F.; Sarfati, G.; Esch, A.; Tabouret, T.; Dhooge, M.; Dreanic, J.; Perkins, G.; et al. Diagnosis of Iron Deficiency in Inflammatory Bowel Disease by Transferrin Receptor-Ferritin Index. Medicine 2015, 94, e1011. [Google Scholar] [CrossRef] [PubMed]
- Rashtak, S.; Murray, J.A. Celiac Disease in the Elderly. Gastroenterol. Clin. N. Am. 2009, 38, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Martín-Masot, R.; Nestares, M.T.; Diaz-Castro, J.; López-Aliaga, I.; Muñoz Alférez, M.J.; Moreno-Fernandez, J.; Maldonado, J. Multifactorial etiology of anemia in celiac disease and effect of gluten-free diet: A comprehensive review. Nutrients 2019, 11, 2557. [Google Scholar] [CrossRef] [Green Version]
- McNamee, T.; Hyland, T.; Harrington, J.; Cadogan, S.; Honari, B.; Perera, K.; Fitzgerald, A.P.; Perry, I.J.; Cahill, M.R. Haematinic deficiency and macrocytosis in middle-aged and older adults. PLoS ONE 2013, 8, e77743. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.L.; Shaw, N.S. Iron status of the Taiwanese elderly: The prevalence of iron deficiency and elevated iron stores. Asia Pac. J. Clin. Nutr. 2005, 14, 278–284. [Google Scholar]
- Andres, E.; Serraj, K.; Federici, L.; Vogel, T.; Kaltenbach, G. Anemia in elderly patients: New insight into an old disorder. Geriatr. Gerontol. Int. 2013, 13, 519–527. [Google Scholar] [CrossRef]
- Beyer, I.; Compté, N.; Busuioc, A.; Cappelle, S.; Lanoy, C.; Cytryn, E. Anemia and transfusions in geriatric patients: A time for evaluation. Hematology 2010, 15, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.D.; Serviddio, G.; de Matthaeis, A.; Bellanti, F.; Vendemiale, G. Oxidative stress and aging. J. Nephrol. 2010, 23, S29–S36. [Google Scholar]
- Casteleyn, I.; Joosten, E. Evaluation of Parenteral Iron Therapy in Ambulatory Older Adults with Iron Deficiency Anaemia. Acta Haematol. 2017, 138, 221–222. [Google Scholar] [CrossRef]
- Silverberg, D.S.; Mor, R.; Weu, M.T.; Schwartz, D.; Schwartz, I.F.; Chernin, G. Anemia and iron deficiency in COPD patients: Prevalence and the effects of correction of the anemia with erythropoiesis stimulating agents and intravenous iron. BMC Pulm. Med. 2014, 14, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, J.L.; Stanworth, S.J.; Roubinian, N.; Fergusson, D.A.; Triulzi, D.; Doree, C.; Hebert, P.C. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst. Rev. 2016, 10, CD002042. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drug | Elemental Iron Concentration | Dosing | |
|---|---|---|---|
| IV IRON PRODUCTS | |||
| Ferric carboxymaltose | 50 mg/mL | Weight ≥ 50 kg | 2 doses of 20 mg/kg given every 7 days |
| Weight ≤ 50 kg | 2 doses of 15 mg/kg given every 7 days | ||
| Ferric gluconate | 12.5 mg/mL | 125 to 187.5 mg IV infusion over 1 h | |
| Iron sucrose | 20 mg/mL | 100 to 200 mg IV infusion over 15 min | |
| ORAL IRON PRODUCTS | |||
| Ferrous gluconate | Various formulations | 50 to 250 mg/day | |
| Ferrous sulfate | Various formulations | 100 to 200 mg/day | |
| Iron sucrose | Various formulations | 30 mg/day | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romano, A.D.; Paglia, A.; Bellanti, F.; Villani, R.; Sangineto, M.; Vendemiale, G.; Serviddio, G. Molecular Aspects and Treatment of Iron Deficiency in the Elderly. Int. J. Mol. Sci. 2020, 21, 3821. https://doi.org/10.3390/ijms21113821
Romano AD, Paglia A, Bellanti F, Villani R, Sangineto M, Vendemiale G, Serviddio G. Molecular Aspects and Treatment of Iron Deficiency in the Elderly. International Journal of Molecular Sciences. 2020; 21(11):3821. https://doi.org/10.3390/ijms21113821
Chicago/Turabian StyleRomano, Antonino Davide, Annalisa Paglia, Francesco Bellanti, Rosanna Villani, Moris Sangineto, Gianluigi Vendemiale, and Gaetano Serviddio. 2020. "Molecular Aspects and Treatment of Iron Deficiency in the Elderly" International Journal of Molecular Sciences 21, no. 11: 3821. https://doi.org/10.3390/ijms21113821
APA StyleRomano, A. D., Paglia, A., Bellanti, F., Villani, R., Sangineto, M., Vendemiale, G., & Serviddio, G. (2020). Molecular Aspects and Treatment of Iron Deficiency in the Elderly. International Journal of Molecular Sciences, 21(11), 3821. https://doi.org/10.3390/ijms21113821