Toxicology and Analysis of Psychoactive Tryptamines



Abstract
:1. Introduction
2. Results
2.1. Tryptamines of Natural Origin
2.2. Tryptamines of Synthetic Origin
2.2.1. Ring Unsubstituted Tryptamines
2.2.2. 4-Substituted Tryptamines
2.2.3. 5-Substituted Tryptamines
2.3. Analytical Methods to Determine Tryptamines and/or Metabolites in Conventional and Non-Conventional Biological Matrices
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 2-MTHβC | 2-Methyl-1,2,3,4-tetrahydro-beta-carboline |
| 4-AcO-DALT | 4-Acetoxy-N, N-diallyltryptamine |
| 4-AcO-DET | 4-Acetoxy-N,N-diethyltryptamine |
| 4-AcO-DiPT | 4-Acetoxy-N, N- diisopropyltryptamine |
| 4-AcO-DMT | 4-Acetoxy-N,N-dimethyltryptamine |
| 4-AcO-DPT | 4-Acetoxy-N, N-dipropyltryptamine |
| 4-AcO-MET | 4-Acetoxy-N-methyl-N-ethyltryptamine |
| 4-HIAA | 4-Hydroxyindole acetic acid |
| 4-MeO-DMT | 4-Methoxy-N,N-dimethyltryptamine |
| 4-MeO-MiPT | 4-Methoxy-N-methyl-N-isopropyltryptamine |
| 4-OH-DET | 4-Hydroxy-diethyl-tryptamine |
| 4-OH-DMT | 4-Hydroxy-NN-dimethyltryptamine |
| 4-OH-DPT | 4-Hydroxy-N,N-dipropyltryptamine |
| 4-OH-MET | 4-Hydroxy-N-methyl-N-ethyltriptamine |
| 4-OH-MiPT | 4-Hydroxy-N-methyl-N-isopropyltryptamine |
| 4-OH-MPT | 4-Hydroxy-N-methyl-N-propyltryptamine |
| 4-OH-pyr-T | 4-Hydroxy-N,N-tetramethylenetryptamine |
| 5-HT | 5-Hydroxytryptamine |
| 5-MeO-DALT | 5-Methoxy-N,N-diallyltryptamine |
| 5-MeO-DET | 5-Methoxy-N,N-diethyltryptamine |
| 5-MeO-DiPT | 5-Methoxy-diisopropyltryptamine |
| 5-MeO-DMT | 5-Methoxy-N,N-dimethyltryptamine |
| 5-MeO-DPT | 5-Methoxy-N, N-dipropyltryptamine |
| 5-MeO-MET | 5-Methoxy-N-methyl-N-ethyltryptamine |
| 5-MeO-MiPT | 5-Methoxy-N-methyl-N-isopropyltryptamine |
| 5-MeO-MiPT-N-oxide | 5-Methoxy-N-methyl-N-isopropyltrypt-amine-N-oxide |
| 5-MeO-NiPT | 5-Methoxy-N-isopropyltryptamine |
| 5-MeO-TMT | 5-Methoxy-N,N-trimethyltryptamine |
| 5-MeO-α-MT | 5-Methoxy-alpha-methyltryptamine |
| 5-OH-DiPT | 5-Hydroxy-N,N-diisopropyltryptamine |
| 5-OH-DMT | 5-Hydroxy-N,N-dimethyltryptamine |
| 5-OH-MiPT | 5-Hydroxy-N-methyl-N-isopropyltryptamine |
| CNS | Central nervous system |
| DBS | Dried blood spots |
| DDA | Data dependent acquisition |
| DEA | Drug Enforcement Administration |
| DET | N,N-diethyltryptamine |
| DiPT | N,N-diisopropyltryptamine |
| DLLME | Dispersive liquid-liquid microextraction |
| DMT | N,N-dimethyltryptamine |
| DMT-NO | Dimethyltryptamine-N-oxide |
| DPT | N,N-dipropyltryptamine |
| ED | Emergency department |
| EMCDDA | European Monitoring Centre for Drugs and Drug Addiction |
| FDA | Food and Drug Administration |
| GC | Gas chromatography |
| GC-EI-TOF | Gas chromatography time-of-flight detection with electron impact ionization |
| GC-MS | Gas chromatography-mass spectrometry |
| GDS | Global Drug Survey |
| HPLC | High-performance liquid chromatography |
| HPLC-MS | High-performance liquid chromatography coupled with mass spectrometry |
| IAA | Indole-3-Acetic Acid |
| IM | Intramuscular |
| IV | Intravenous |
| LC | Liquid chromatography |
| LC–HRMS/MS | Liquid chromatography–high-resolution mass spectrometry |
| LC-MS/MS | Liquid chromatography coupled with mass spectrometry in |
| LLE | Liquid-liquid extraction |
| LOD | Limit of detection |
| LSD | Lysergic acid diethylamide |
| MAO | Monoamine oxidase |
| MAOI | Monoamine oxidase inhibitor |
| MDMA | 3,4-Methylenedioxymethamphetamine |
| MET | N-methyl-N-ethyltryptamine |
| MRM | Multiple reaction monitoring |
| NMT | N-methyltryptamine |
| NPS | New psychoactive substances |
| OH-5-MeO- MiPT | hydroxy-5-methoxy-N-methyl-N-isopropyl-tryptamine |
| PDA | Photodiode array acquisition |
| SIM | Single ion monitoring |
| SPE | Solid phase extraction |
| STAI | Speilberg State-Trait Anxiety Inventory |
| TOF | Time of flight |
| UHPLC-HRMS/MS | Ultra-performance liquid chromatography-high resolution mass spectrometry |
| UNODC | United Nations Office on Drugs and Crime |
| WHO | World Health Organization |
| α-ET | Alpha-ethyltryptamine |
| α-MT | Alpha-methyltryptamine |
References
- World Drug Report 2019 (United Nations Publication, Sales No E.19.XI.8). United Nations Office on Drugs and Crime (UNODC) Cannabis and Hallucinogens. Available online: https://wdr.unodc.org/wdr2019/prelaunch/WDR19_Booklet_5_CANNABIS_HALLUCINOGENS.pdf (accessed on 22 July 2020).
- Glennon, R.A.; Titeler, M.; McKenney, J.D. Evidence for 5-HT2 involvement in the mechanism of action of hallucinogenic agents. Life Sci. 1984, 35, 2505–2511. [Google Scholar] [CrossRef]
- Nichols, D.E. Hallucinogens. Pharmacol. Ther. 2004, 101, 131–181. [Google Scholar] [CrossRef] [PubMed]
- Titeler, M.; Lyon, R.A.; Glennon, R.A. Radio ligand binding evidence implicates the brain 5-HT2 receptor as a site of action for LSD and phenylisopropylamine hallucinogens. Psychopharmacology 1988, 94, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Vollenweider, F.X.; Vollenweider-Scherpenhuyzen, M.F.; Babler, A.; Vogel, H.; Hell, D. Psilocybin induces schizophrenia-like psychosis in humans via a serotonin-2 agonist action. NeuroReport 1998, 9, 3897–3902. [Google Scholar] [CrossRef] [Green Version]
- Rickli, A.; Moning, O.D.; Hoener, M.C.; Liechti, M.E. Receptor interaction profiles of novel psychoactive tryptamines compared with classic hallucinogens. Eur. Neuropsychopharmacol. 2016, 26, 1327–1337. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, D.; Barnes, G.; Giaroli, G.; Tracy, D. Classical hallucinogens as antidepressants? A review of pharmacodynamics and putative clinical roles. Ther. Adv. Psychopharmacol. 2014, 4, 156–169. [Google Scholar] [CrossRef] [Green Version]
- Bunzow, J.R.; Sonders, M.S.; Arttamangkul, S.; Harrison, L.M.; Zhang, G.; Quigley, D.I.; Darland, T.; Suchland, K.L.; Pasumamula, S.; Kennedy, J.L.; et al. Amphetamine, 3,4-methylenedioxy methamphetamine, lysergic acid diethylamide, and metabolites of the catecholamine neurotransmitters are agonists of a rat trace amine receptor. Mol. Pharm. 2001, 60, 1181–1188. [Google Scholar] [CrossRef]
- Cozzi, N.V.; Gopalakrishnan, A.; Anderson, L.L.; Feih, J.T.; Shulgin, A.T.; Daley, P.F.; Ruoho, A.E. Dimethyltryptamine and other hallucinogenic tryptamines exhibit substrate behavior at the serotonin uptake transporter and the vesicle monoamine transporter. J. Neuraltransm. 2009, 116, 1591–1599. [Google Scholar] [CrossRef]
- Fantegrossi, W.E.; Harrington, A.W.; Kiessel, C.L.; Eckler, J.R.; Rabin, R.A.; Winter, J.C.; Coop, A.; Rice, K.C.; Woods, J.H. Hallucinogen-like actions of 5-methoxy-N,N-diisopropyl-tryptamine in mice and rats. Pharmacol. Biochem. Behav. 2006, 83, 122–129. [Google Scholar] [CrossRef]
- McKenna, D.J.; Repke, D.B.; Lo, L.; Peroutka, S.J. Differential interactions of indolealkylamines with 5-hydroxytryptamine receptor subtypes. Neuropharmacology 1990, 29, 193–198. [Google Scholar] [CrossRef]
- Luethi, D.; Liechti, M.E. Monoamine transporter and receptor interaction profiles in vitro predict reported human doses of novel psychoactive stimulants and psychedelics. Int. J. Neuropsychopharmacol. 2018, 21, 926–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, R.G.; Hallak, J.E.C. Therapeutic use of serotoninergic hallucinogens: A review of the evidence and of the biological and psychological mechanisms. Neurosci. Biobehav. Rev. 2020, 108, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Ray, T.S. Psychedelics and the human receptorome. PLoS ONE 2010, 5, e9019. [Google Scholar] [CrossRef]
- Global Drug Survey (GDS). Available online: https://www.globaldrugsurvey.com/wp-content/themes/globaldrugsurvey/results/GDS2019-Exec-Summary.pdf (accessed on 22 July 2020).
- Winstock, A.; Barratt, M.; Maier, L.; Ferris, J. Global Drug Survey (GDS). Available online: https://www.globaldrugsurvey.com/gds-2019/ (accessed on 22 July 2020).
- Marchei, E.; Paci, R.; Mannocchi, G.; Marinelli, E.; Pichini, S.; Paolo, F. Trends in Analytical Chemistry New synthetic opioids in biological and non-biological matrices: A review of current analytical methods. Trends Anal. Chem. 2018, 102, 1–15. [Google Scholar] [CrossRef]
- Lo Faro, A.F.; Di Trana, A.; La Maida, N.; Tagliabracci, A.; Giorgetti, R.; Busardò, F.P. Biomedical analysis of New Psychoactive Substances (NPS) of natural origin. J. Pharm. Biomed. Anal. 2020, 179, 112945. [Google Scholar] [CrossRef]
- Giorgetti, A.; Busardò, F.P.; Tittarelli, R.; Auwärter, V. Post-Mortem Toxicology: A Systematic Review of Death Cases Involving Synthetic Cannabinoid Receptor Agonists. Front. Psychiatry 2020, 11, 1–22. [Google Scholar] [CrossRef]
- Wilde, M.; Pichini, S.; Pacifici, R.; Tagliabracci, A.; Busardò, F.P.; Auwärter, V.; Solimini, R. Metabolic Pathways and Potencies of New Fentanyl Analogs Procedures for Assessment of Metabolic. Front. Pharm. 2019, 10, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Busardò, F.P.; Carlier, J.; Giorgetti, R.; Tagliabracci, A.; Pacifici, R.; Gottardi, M.; Pichini, S. Ultra-High-Performance Liquid Chromatography-Tandem Mass Spectrometry Assay for Quantifying Fentanyl and 22 Analogs and Metabolites in Whole Blood, Urine, and Hair. Front. Chem. 2019, 7, 1–13. [Google Scholar] [CrossRef]
- Tittarelli, R.; Mannocchi, G.; Pantano, F.; Romolo, F. Recreational Use, Analysis and Toxicity of Tryptamines. Curr. Neuropharmacol. 2014, 13, 26–46. [Google Scholar] [CrossRef] [Green Version]
- Araújo, A.M.; Carvalho, R.; Bastos, M.L.; Pinho, P.G.; Carvalho, M. The hallucinogenic world of tryptamines: An updated review. Arch. Toxicol. 2015, 89, 1151–1173. [Google Scholar] [CrossRef]
- Murch, S.J.; Campbell, K.B.; Saxena, P.K. The role of serotonin and melatonin in plant morphogenesis: Regulation of auxin-induced root organogenesis in in vitro-cultured explants of St. John’s wort (hypericum perforatum L.). Vitr. Cell. Dev. Biol. Plant 2001, 37, 786–793. [Google Scholar] [CrossRef]
- McKenna, D.; Riba, J. New World Tryptamine Hallucinogens and the Neuroscience of Ayahuasca. Brain Imaging Behav. Neurosci. 2018, 36, 283–311. [Google Scholar] [CrossRef]
- Szára, S. DMT at fifty. Neuropsychopharmacol. Hung. 2007, 9, 201–205. [Google Scholar]
- Strassman, R.J.; Qualls, C.R. Dose-response Study of N,N-dimethyltryptamine in Humans. I. Neuroendocrine, autonomic, and cardiovascular effects. Arch. Gen. Psychiatry 1994, 51, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Erspamer, V. Observations on the fate of indolealkylamines in the organism. J. Physiol. 1954, 127, 118–133. [Google Scholar] [CrossRef] [Green Version]
- Pichini, S.; Marchei, E.; Palmi, I.; Pellegrini, M.; Pacifici, R.; Zuccaro, P. Smart Drugs. Available online: http://old.iss.it/binary/drog/cont/SD_COMPLETO_ridotto.pdf (accessed on 13 May 2020).
- Tupper, K.W.; Wood, E.; Yensen, R.; Johnson, M.W. Psychedelic medicine: A re-emerging therapeutic paradigm. Can. Med Assoc. J. 2015, 187, 1054–1059. [Google Scholar] [CrossRef] [Green Version]
- Słonina, G.; Janczura, K. New psychoactive substances in Poland: An overview of psychodysleptics (lysergamides and tryptamines). World Sci. News 2018, 109, 245–262. [Google Scholar]
- Constantino, M.T.D.; Repke, D.B. Anadenanthera: Visionary Plant of Ancient South. America, 2nd ed.; Routledge: New York, NY, USA, 2006; pp. 143–187. [Google Scholar] [CrossRef]
- Paterson, N.E.; Darby, W.C.; Sandhu, P.S. N,N-Dimethyltryptamine-Induced Psychosis. Clin. Neuropharmacol. 2015, 38, 141–143. [Google Scholar] [CrossRef]
- Bilhimer, M.H.; Schult, R.F.; Higgs, K.V.; Wiegand, T.J.; Gorodetsky, R.M.; Acquisto, N.M. Acute Intoxication following Dimethyltryptamine Ingestion. Case Rep. Emerg. Med. 2018, 2018, 1–3. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Hallucinogenic Mushrooms Drug Profile. Available online: http://www.emcdda.europa.eu/publications/drug-profiles/hallucinogenic-mushrooms_en (accessed on 8 May 2020).
- Hofmann, A.; Heim, R.; Brack, A.; Kobel, H. Psilocybin, a Psychotropic Substance from the Mexican Mushroom Psilicybe Mexicana Heim. Experientia 1958, 14, 107–109. [Google Scholar] [CrossRef]
- Pellegrini, M.; Rotolo, M.C.; Marchei, E.; Pacifici, R.; Saggio, F.; Pichini, S. Magic truffles or Philosopher’s stones: A legal way to sell psilocybin? Drug Test. Anal. 2013, 5, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Nichols, D.E.; Johnson, M.W.; Nichols, C.D. Psychedelics as Medicines: An emerging new paradigm. Clin. Pharm. 2017, 101, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Cameron, L.P.; Nazarian, A.; Olson, D.E. Psychedelic Microdosing: Prevalence and Subjective Effects. J. Psychoact. Drugs 2020, 52, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Honyiglo, E.; Franchi, A.; Cartiser, N.; Bottinelli, C.; Advenier, A.S.; Bévalot, F.; Fanton, L. Unpredictable Behavior Under the Influence of “Magic Mushrooms”: A Case Report and Review of the Literature. J. Forensic Sci. 2019, 64, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R.L.; Bolstridge, M.; Rucker, J.; Day, C.M.J.; Erritzoe, D.; Kaelen, M.; Bloomfield, M.; Rickard, J.A.; Forbes, B.; Feilding, A.; et al. Psilocybin with psychological support for treatment-resistant depression: An open-label feasibility study. Lancet Psychiatry 2016, 3, 619–627. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, R.R.; Johnson, M.W.; Carducci, M.A.; Umbricht, A.; Richards, W.A.; Richards, B.D.; Cosimano, M.P.; Klinedinst, M.A. Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer: A randomized double-blind trial. J. Psychopharmacol. 2016, 30, 1181–1197. [Google Scholar] [CrossRef]
- Grob, C.S.; Danforth, A.L.; Chopra, G.S.; Hagerty, M.; McKay, C.R.; Halberstad, A.L.; Greer, G.R. Pilot study of psilocybin treatment for anxiety in patients with advanced-stage cancer. Arch. Gen. Psychiatry 2011, 68, 71–78. [Google Scholar] [CrossRef]
- Ross, S.; Bossis, A.; Guss, J.; Agin-Liebes, G.; Malone, T.; Cohen, B.; Mennenga, S.E.; Belser, A.; Kalliontzi, K.; Babb, J.; et al. Rapid and sustained symptom reduction following psilocybin treatment for anxiety and depression in patients with life-threatening cancer: A randomized controlled trial. J. Psychopharmacol. 2016, 30, 1165–1180. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.W.J.; Garcia-Romeu, A.; Cosimano, M.P.; Griffiths, R.R. Pilot Study of the 5-HT2A R Agonist Psilocybin in the Treatment of Tobacco Addiction. J. Psychopharmacol. 2014, 28, 983–992. [Google Scholar] [CrossRef] [Green Version]
- Bogenschutz, M.P.; Forcehimes, A.A.; Pommy, J.A.; Wilcox, C.E.; Barbosa, P.; Strassman, R.J. Psilocybin-assisted treatment for alcohol dependence: A proof-of-concept study. J. Psychopharmacol. 2015, 29, 289–299. [Google Scholar] [CrossRef]
- Davis, A.; Barsuglia, J.P.; Lancelotta, R.; Grant, R.M.; Renn, E. The epidemiology of 5-methoxy-N, N-dimethyltryptamine (5-MeO-DMT) use: Benefits, consequences, patterns of use, subjective effects, and reasons for consumption. J. Psychopharmacol. 2018, 32, 779–792. [Google Scholar] [CrossRef] [PubMed]
- Psychedelic Times. Exploring the Sacred Power of 5-MeO-DMT and the Psychedelic Toad: Podcast with Dr. Gerardo Sandoval. Available online: https://psychedelictimes.com/podcasts/exploring-the- sacred-power-of-5-meo-dmt-podcast-with-dr-gerardo-sandoval/ (accessed on 22 July 2020).
- Shen, H.W.; Jiang, X.-L.; Winter, J.C.; Yu, A.M. Psychedelic 5-Methoxy-N,N-Dimethyltryptamine: Metabolism, Pharmacokinetics, Drug Interactions, and Pharmacological Actions. Curr. Drug Metab. 2011, 11, 659–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitaram, B.R.; McLeod, W.R. Observations on the metabolism of the psychotomimetic indolealkylamines: Implications for future clinical studies. Biol. Psychiatry 1990, 28, 841–848. [Google Scholar] [CrossRef]
- Sitaram, B.R.; Lockett, L.; Blackman, G.L.; McLeod, W.R. Urinary excretion of 5-methoxy-N,N-dimethyltryptamine, N,N-dimethyltryptamine and their N-oxides in the rat. Biochem. Pharmacol. 1987, 36, 2235–2237. [Google Scholar] [CrossRef]
- Brush, D.E.; Bird, S.B.; Boyer, E.W. Monoamine oxidase inhibitor poisoning resulting from Internet misinformation on illicit substances. J. Toxicol. Clin. Toxicol. 2004, 42, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Sklerov, J.; Levine, B.; Moore, K.A.; King, T.; Fowler, D. A fatal intoxication following the ingestion of 5-methoxy-N,N-dimethyltryptamine in an Ayahuasca preparation. J. Anal. Toxicol. 2005, 29, 838–841. [Google Scholar] [CrossRef] [Green Version]
- Dipartimento per le Politiche Antidroga. Available online: http://www.politicheantidroga.gov.it/media/1286/36_triptamine.pdf (accessed on 20 May 2020).
- Rusterholz, D.B.; Long, J.P.; Nichols, D.E. Effect of alpha-Methyltryptamine on Spontaneous Activity in mice. Pharm. Biochem. Behav. 1979, 10, 223–227. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Alpha-methyltryptamine (AMT). Available online: https://legal-high-inhaltsstoffe.de/sites/default/files/uploads/amt.pdf. (accessed on 20 July 2020).
- Wilcox, J. Psychoactive properties of alpha-methyltryptamine: Analysis from self-reports of users. J. Psychoact. Drugs 2012, 44, 274–276. [Google Scholar] [CrossRef]
- Holstege, C.P.; Baer, A.B.; Kirk, M.A. Prolonged hallucinations following ingestion of alpha-methyl-tryptamine. J. Toxicol. Clin. Toxicol. 2003, 41, 641–752. [Google Scholar] [CrossRef]
- Long, H.; Nelson, L.S.; Hoffman, R.S. Alpha-methyltryptamine Revisited via Easy Internet Access. Vet. Hum. Toxicol. 2003, 45, 149. [Google Scholar]
- Boland, D.M.; Andollo, W.; Hime, G.W.; Hearn, W.L. Fatality due to acute α-methyltryptamine intoxication. J. Anal. Toxicol. 2005, 29, 394–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanamori, T.; Kuwayama, K.; Tsujikawa, K.; Miyaguchi, H.; Iwata, Y.T.; Inoue, H. In vivo metabolism of α-methyltryptamine in rats: Identification of urinary metabolites. Xenobiotica 2008, 38, 1476–1486. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) European Drug Report 2018: Trends and Developments. Available online: https://www.emcdda.europa.eu/system/files/publications/8585/20181816_TDAT18001ENN_PDF.pdf (accessed on 20 July 2020).
- Glennon, R.A.; Bondareva, T.; Young, R. α-Ethyltryptamine (α-ET) as a discriminative stimulus in rats. Pharm. Biochem. Behav. 2006, 85, 448–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daldrup, T.; Heller, C.; Matthiensen, U.; Honus, S.; Bresges, A.; Haarhoff, K. Etryptamine, a new designer drug with a fatal effect. Int. J. Legal Med. 1986, 97, 61–68. [Google Scholar] [CrossRef]
- Drug Enforcement Administration (DEA), U.S.; Department of Justice. Drugs of Abuse: A DEA Resource Guide 2017. Available online: https://www.dea.gov/sites/default/files/drug_of_abuse.pdf (accessed on 10 June 2020).
- Huang, X.; Johnson, M.P.; Nichols, D.E. Reduction in brain serotonin markers by a-ethyltryptamine (Monase). Eur. J. Pharmacol. 1991, 200, 187–190. [Google Scholar] [CrossRef]
- Massaro, E.J. Handbook of Neurotoxicology, 1st ed.; Humana Press: Totowa, NJ, USA, 2002. [Google Scholar] [CrossRef]
- Krebs, K.M.; Geyer, M.A. Behavioral characterization of a-ethyltryptamine, a tryptamine derivative with MDMA-like properties in rats. Psychopharmacology 1993, 113, 284–287. [Google Scholar] [CrossRef]
- Morano, R.; Spies, C.; Walker, F.; Plank, S. Fatal Intoxication Involving Etryptamine. J. Forensic Sci. 1993, 38, 721–725. [Google Scholar] [CrossRef]
- Chemeurope Search Results for Diethyltryptamine. Available online: https://www.chemeurope.com/en/encyclopedia/Diethyltryptamine.html (accessed on 7 May 2020).
- DrugBank Search Results for Diethyltryptamine. Available online: https://www.drugbank.ca/drugs/DB01460 (accessed on 8 May 2020).
- Szára, S.; Rockland, L.H.; Rosenthal, D.; Handlon, J.H. Psychological Effects and Metabolism of N,N-diethyltryptamine in Man. Arch. Gen. Psychiatry 1966, 15, 320–329. [Google Scholar] [CrossRef]
- Laing, R.R. Hallucinogens: A Forensic Drug Handbook, 1st ed.; Academic Press: London, UK, 2003; pp. 50–53. [Google Scholar]
- Barker, S.A.; Borjigin, J.; Lomnicka, I.; Strassman, R. LC/MS/MS analysis of the endogenous dimethyltryptamine hallucinogens, their precursors, and major metabolites in rat pineal gland microdialysate. Biomed. Chromatogr. 2013, 27, 1690–1700. [Google Scholar] [CrossRef] [Green Version]
- Gardner, D.; Riet-Correa, F.; Lemos, D.; Welch, K.; Pfister, J.; Panter, K. Teratogenic effects of Mimosa tenuiflora in a rat model and possible role of N-methyl- and N,N-dimethyltryptamine. J. Agric. Food Chem. 2014, 62, 7398–7401. [Google Scholar] [CrossRef]
- Grof, S.; Soskin, R.A.; Richards, W.A.; Kurland, A.A. DPT as an Adjunct in Psychotherapy of Alcoholics. Int. Pharm. 1973, 115, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Erowid Search Results for DPT. Available online: https://www.erowid.org/search.php?exclude=&q=DPT&x=0&y=0 (accessed on 8 May 2020).
- Thiagaraj, H.V.; Russo, E.B.; Burnett, A.; Goldstein, E.; Thompson, C.M.; Parker, K.K. Binding Properties of Dipropyltryptamine at the Human 5-HT1a Receptor. Pharmacology 2005, 1552, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Fantegrossi, W.E.; Reissig, C.J.; Katz, E.B.; Yarosh, H.L.; Rice, K.C.; Winter, J.C. Hallucinogen-like effects of N,N-dipropyltryptamine (DPT): Possible mediation by serotonin 5-HT1A and 5-HT2A receptors in rodents. Pharm. Biochem. Behav. 2008, 88, 358–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dailey, R.M.; Nelson, L.D.; Scaglione, J.M. Tachycardia and rhabdomyolysis after intentional ingestion of N,N-Dipropyltryptamine. J. Toxicol. Clin. Toxicol. 2003, 41, 742–743. [Google Scholar]
- Gatch, M.B.; Forster, M.J.; Janowsky, A.; Eshleman, A.J. Abuse Liability Profile of Three Substituted Tryptamines. J. Pharmacol. Exp. Ther. 2011, 338, 280–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulgin, A.; Shulgin, A. Tryptamines that I Have Known and Loved (TiHKAL): The Continuation, 1st ed.; Transform Press: Berkeley, CA, 1997; pp. 433–557. [Google Scholar]
- Repke, D.B.; Ferguson, W.J.; Bates, D.K. Psilocin Analogs II. Synthesis of 3-[2-(Dialky1amino)ethyl-, 3-[2-(N-Methyl-N-alkylamino)ethyl], and 3-[2-(Cycloalkylamino)ethyl]indol-4-ol. J. Heterocycl. Chem. 1981, 5, 1–5. [Google Scholar] [CrossRef]
- Erowid A Report on 6-Carbon Tryptamines. Available online: https://erowid.org/experiences/exp.php?ID=101510 (accessed on 16 June 2020).
- Eurowid. A Mirror to the Mind. Available online: https://erowid.org/experiences/exp.php?ID=94380 (accessed on 16 June 2020).
- Sciani, J.M.; Angeli, C.B.; Antoniazzi, M.M.; Jared, C.; Pimenta, D.C. Differences and Similarities among Parotoid Macrogland Secretions in South American Toads: A Preliminary Biochemical Delineation. Sci. World J. 2013, 2013, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Britannica. Bufotenine Drug. Available online: https://www.britannica.com/science/bufotenine (accessed on 20 July 2020).
- Dobbs, M. Clinical Neurotoxicology Syndromes, Substances, Environments, 1st ed.; Saunders: Philadelphia, PA, USA, 2009; p. 331. [Google Scholar]
- Keomany, S.; Mayxay, M.; Souvannasing, P.; Vilayhong, C.; Stuart, B.L.; Srour, L.; Newton, P.N. Toad poisoning in Laos. Am. J. Trop. Med. Hyg. 2007, 77, 850–853. [Google Scholar] [CrossRef]
- Weil, A.T.; Davis, W. Bufo alvarius: A potent hallucinogen of animal origin. J. Ethnopharmacol. 1994, 41, 1–8. [Google Scholar] [CrossRef]
- Ott, J. Pharmañopo—Psychonautics: Human intranasal, sublingual, intrarectal, pulmonary and oral pharmacology of bufotenine. J. Psychoact. Drugs 2001, 33, 273–281. [Google Scholar] [CrossRef]
- Postma, T.L. Neurotoxic animal poisons and venoms. Clin. Neurotoxicol. Syndr. Subst. Env. 2009, 463–489. [Google Scholar] [CrossRef]
- Drug Enforcement Administration (DEA). 5-Methoxy-N,N-Diisopropyttryptamine (Street Names: Foxy, or Foxy Methoxy). Available online: http://www.deadiversion.usdoj.gov/drug_chem_info/5meodipt.pdf (accessed on 26 June 2020).
- Noworyta-Sokołowska, K.; Kamińska, K.; Kreiner, G.; Rogóż, Z.; Gołembiowska, K. Neurotoxic Effects of 5-MeO-DIPT: A Psychoactive Tryptamine Derivative in Rats. Neurotox. Res. 2016, 30, 606–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulgin, A.T.; Carter, M.F. N,N-Diisopropyltryptamine (DIPT) and 5-methoxy-N,N-diisopropyltryptamine (5-MeO-DIPT). Two Orally Active Tryptamine Analogs With CNS Activity. Commun. Psychopharmacol. 1980, 4, 363–369. [Google Scholar] [PubMed]
- Shen, H.W.; Jiang, X.L.; Yu, A.M. Nonlinear pharmacokinetics of 5-methoxy-N,N-dimethyltryptamine in mice. Drug Metab. Dispos. 2011, 39, 1227–1234. [Google Scholar] [CrossRef] [Green Version]
- Kamata, T.; Katagi, M.; Kamata, H.T.; Miki, A.; Shima, N.; Zaitsu, K.; Nishikawa, M.; Tanaka, E.; Honda, K.; Tsuchihashi, H. Metabolism of the psychotomimetic tryptamine derivative 5-methoxy-N,N-diiso- propyltryptamine in humans: Identification and quantification of its urinary metabolites. Drug Metab. Dispos. 2006, 34, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.; McGeorge, F.; Smolinske, S.; Meatherall, R. A “Foxy” intoxication. Forensic Sci. Int. 2005, 148, 31–36. [Google Scholar] [CrossRef]
- Smolinske, S.C.; Rastogi, R.; Schenkel, S. Foxy methoxy: A new drug of abuse. J. Med. Toxicol. 2005, 1, 23–25. [Google Scholar] [CrossRef] [Green Version]
- Meatherall, R.; Sharma, P. Foxy, a designer tryptamine hallucinogen. J. Anal. Toxicol. 2003, 27, 313–317. [Google Scholar] [CrossRef] [Green Version]
- Corkery, J.M.; Durkin, E.; Elliott, S.; Schifano, F.; Ghodse, A.H. The recreational tryptamine 5-MeO-DALT (N,N-diallyl-5-methoxytryptamine): A brief review. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2012, 39, 259–262. [Google Scholar] [CrossRef] [Green Version]
- Michely, J.A.; Helfer, A.G.; Brandt, S.D.; Meyer, M.R.; Maurer, H.H. Metabolism of the new psychoactive substances N,N-diallyltryptamine (DALT) and 5-methoxy-DALT and their detectability in urine by GC–MS, LC–MSn, and LC–HR–MS–MS. Anal. Bioanal. Chem. 2015, 407, 7831–7842. [Google Scholar] [CrossRef] [Green Version]
- Eurowid Search Results for 5-MeO-MiPT. Available online: https://www.erowid.org/chemicals/5meo_mipt/5meo_mipt_dose.shtml (accessed on 25 May 2020).
- Repke, D.B.; Grotjahn, D.B.; Shulgin, A.T. Psychotomimetic N-Methyl-N-isopropyltryptamines. Effects of Variation of Aromatic Oxygen Substituents. J. Med. Chem. 1985, 28, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Cayman Chemical. Product Information for 5-Methoxy DET (5-MeO DET, 5-methoxy-N,N-Diethyltryptamine). Available online: https://www.caymanchem.com/pdfs/17300.pdf (accessed on 20 July 2020).
- Grafinger, K.E.; Hädener, M.; König, S.; Weinmann, W. Study of the in vitro and in vivo metabolism of the tryptamine 5-MeO-MiPT using human liver microsomes and real case samples. Drug Test. Anal. 2018, 10, 562–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, E.; Watanabe, H.; Kojima, T.; Hagiwara, H.; Fujisaki, M.; Miyatake, R.; Hashimoto, K.; Iyo, M. Combined intoxication with methylone and 5-MeO-MIPT. Prog. Neuro Psychopharmacol. Biol. Psychiatry 2007, 31, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Drugs Forum Search for 5-MeO-MET. Available online: https://drugs-forum.com/threads/5-meo-met.40412/ (accessed on 12 June 2020).
- Wohlfarth, A.; Weinmann, W.; Dresen, S. LC-MS/MS screening method for designer amphetamines, tryptamines, and piperazines in serum. Anal. Bioanal. Chem. 2010, 396, 2403–2414. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.D.; Okai, G.G.; da Costa, J.L.; de Almeida, R.M.; Oliveira-Silva, D.; Yonamine, M. Determination of dimethyltryptamine and β-carbolines (ayahuasca alkaloids) in plasma samples by LC-MS/MS. Bioanalysis 2012, 4, 1731–1738. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Schürenkamp, J.; Pfeiffer, H.; Köhler, H. A validated method for quantitation of psilocin in plasma by LC-MS/MS and study of stability. Int. J. Legal Med. 2012, 126, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Schürenkamp, J.; Gasse, A.; Pfeiffer, H.; Köhler, H. Determination of psilocin, bufotenine, LSD and its metabolites in serum, plasma and urine by SPE-LC-MS/MS. Int. J. Leg. Med. 2013, 127, 593–601. [Google Scholar] [CrossRef]
- Ambach, L.; Redondo, A.H.; König, S.; Weinmann, W. Rapid and simple LC-MS/MS screening of 64 novel psychoactive substances using dried blood spots. Drug Test. Anal. 2014, 6, 367–375. [Google Scholar] [CrossRef]
- Ambach, L.; Redondo, A.H.; König, S.; Angerer, V.; Schürch, S.; Weinmann, W. Detection and quantification of 56 new psychoactive substances in whole blood and urine by LC–MS/MS. Bioanalysis 2015, 7, 1119–1136. [Google Scholar] [CrossRef]
- Odoardi, S.; Fisichella, M.; Romolo, F.S.; Strano-Rossi, S. High-throughput screening for new psychoactive substances (NPS) in whole blood by DLLME extraction and UHPLC-MS/MS analysis. J. Chromatogr. B. Anal. Technol. Biomed. Life Sci. 2015, 1000. [Google Scholar] [CrossRef]
- Martin, R.; Schürenkamp, J.; Gasse, A.; Pfeiffer, H.; Köhler, H. Analysis of psilocin, bufotenine and LSD in hair. J. Anal. Toxicol. 2015, 39, 126–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamowicz, P.; Tokarczyk, B. Simple and rapid screening procedure for 143 new psychoactive substances by liquid chromatography-tandem mass spectrometry. Drug Test. Anal. 2016, 8, 652–667. [Google Scholar] [CrossRef] [PubMed]
- Brandt, S.D.; Kavanagh, P.V.; Dowling, G.; Talbot, B.; Westphal, F.; Meyer, M.R.; Maurer, H.H.; Halberstadt, A.L.; Sciences, B.; Bureau, S. Analytical characterization of N,N-diallyltryptamine (DALT) and 16 ring-substituted derivatives. Drug Test. Anal. 2016, 9, 115–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaiano, F.; Busardò, F.P.; Palumbo, D.; Kyriakou, C.; Fioravanti, A.; Catalani, V.; Mari, F.; Bertol, E. A novel screening method for 64 new psychoactive substances and 5 amphetamines in blood by LC–MS/MS and application to real cases. J. Pharm. Biomed. Anal. 2016, 129, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, H.; Nordfjærn, T.; Bretteville-Jensen, A.L.; Edland-Gryt, M.; Furuhaugen, H.; Karinen, R.; Øiestad, E.L. Comparison of drugs used by nightclub patrons and criminal offenders in Oslo, Norway. Forensic Sci Int. 2016, 265, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Fabregat-Safont, D.; Barneo-Muñoz, M.; Martinez-Garcia, F.; Sancho, J.V.; Hernández, F.; Ibáñez, M. Proposal of 5-methoxy-N-methyl-N-isopropyltryptamine consumption biomarkers through identification of in vivo metabolites from mice. J. Chromatogr. A 2017, 1508, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Michely, J.A.; Brandt, S.D.; Meyer, M.R.; Maurer, H.H. Biotransformation and detectability of the new psychoactive substances N,N-diallyltryptamine (DALT) derivatives 5-fluoro-DALT, 7-methyl-DALT, and 5,6-methylenedioxy-DALT in urine using GC-MS, LC-MSn, and LC-HR-MS/MS. Anal. Bioanal. Chem. 2017, 409, 1681–1695. [Google Scholar] [CrossRef] [Green Version]
- Fagiola, M.; Hahn, T.; Avella, J. Screening of Novel Psychoactive Substances in Postmortem Matrices by Liquid Chromatography-Tandem Mass Spectrometry (LC-MS-MS). J. Anal. Toxicol. 2018, 42, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Roujia, W.; Ping, X.; Zhiguo, Y.; Yan, S. Application of hair analysis to document illegal 5-methoxy-N,N-diisopropyltryptamine (5-MeO-DiPT) use. Forensic Sci. Int. 2019, 304, 109972. [Google Scholar] [CrossRef]
- Pope, J.D.; Choy, K.W.; Drummer, O.H.; Schneider, H.G. Harmala Alkaloids Identify Ayahuasca Intoxication in a Urine Drug Screen. J. Anal. Toxicol. 2019, 43, e23–e27. [Google Scholar] [CrossRef]
- Yan, X.; Xiang, P.; Zhao, Y.; Yu, Z.; Yan, H. Determination of 5-MeO-DIPT in human urine using gas chromatography coupled with high resolution Orbitrap mass spectrometry. J. Anal. Toxicol. 2020, 44, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Varì, M.R.; Pichini, S.; Giorgetti, R.; Busardò, F.P. NPS—Synthetic stimulants. Forensic Sci. 2018, e1197. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). Available online: https://www.emcdda.europa.eu/emcdda-home-page_en (accessed on 26 June 2020).
- United Nations Office on Drugs and Crime (UNODC). Available online: https://www.unodc.org/ (accessed on 26 June 2020).
- World Health Organization (WHO). Available online: https://www.who.int/ (accessed on 26 June 2020).


{kind=link}
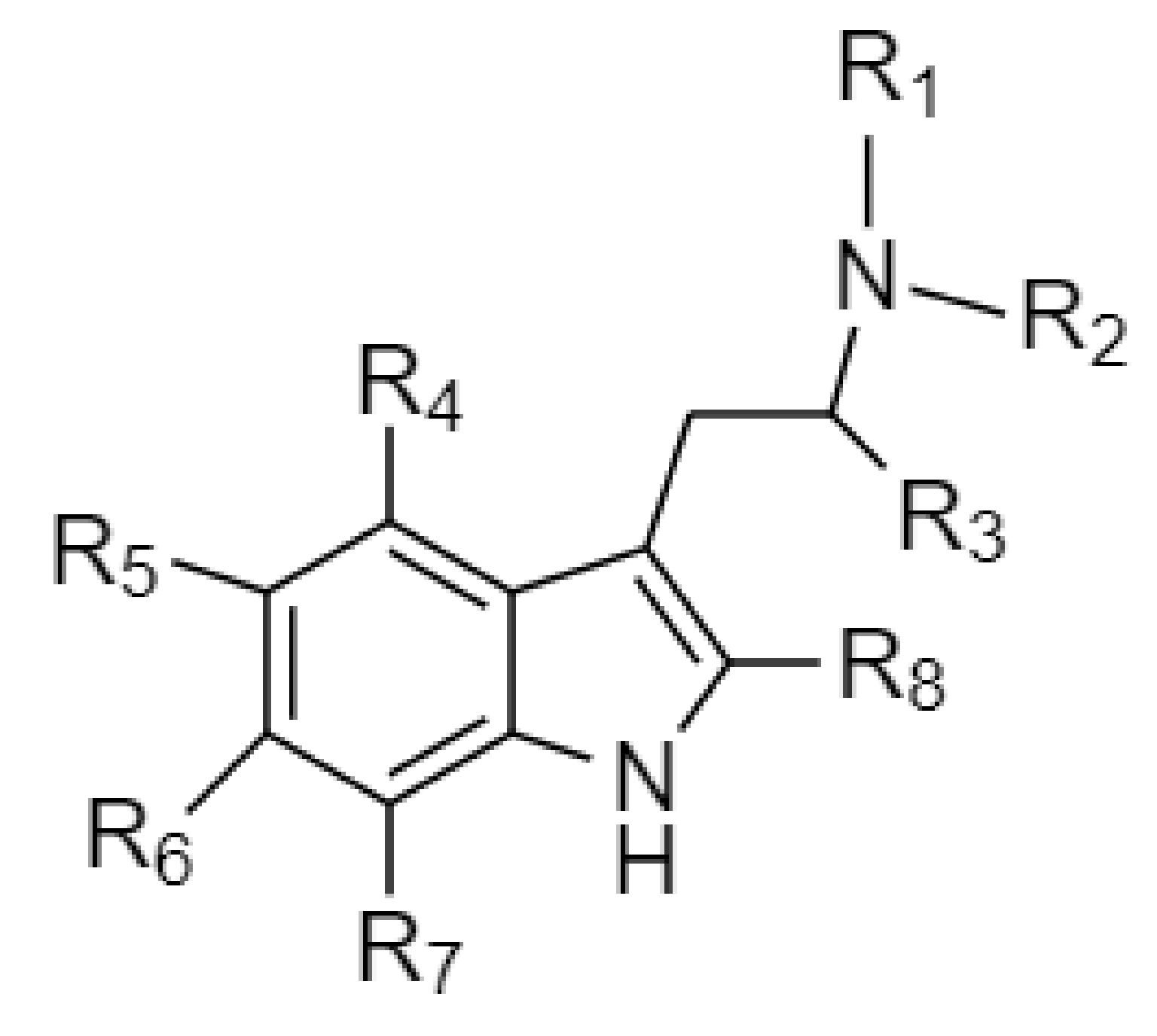
| Abbreviation | Chemical Name | Molecular Formula | Chemical Structure | Molecular Weight (g/mol) | R1 | R2 | R3 | R4 | R5 | R6 | R7 | R8 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tryptamine | Tryptamine | C10H12N2 |  | 160.2 | H | H | H | H | H | H | H | H |
| Ring unsubstituted tryptamines | ||||||||||||
| α-MT | α-methyltryptamine | C11H14N2 |  | 174.2 | H | H | CH3 | H | H | H | H | H |
| α-ET | α-ethyltryptamine | C12H16N2 |  | 188.3 | H | H | CH2CH3 | H | H | H | H | H |
| DMT | N,N-dimethyltryptamine | C12H16N2 |  | 188.3 | CH3 | CH3 | H | H | H | H | H | H |
| DET | N,N-diethyltryptamine | C14H20N2 |  | 216.3 | CH2CH3 | CH2CH3 | H | H | H | H | H | H |
| MET | N-methyl-N-ethyltryptamine | C13H18N2 |  | 202.3 | CH3 | CH2CH3 | H | H | H | H | H | H |
| NMT | N-methyltryptamine | C11H14N2 |  | 174.2 | H | CH3 | H | H | H | H | H | H |
| DPT | N,N-dipropyltryptamine | C16H24N2 |  | 244.4 | CH2CH2CH3 | CH2CH2CH3 | H | H | H | H | H | H |
| DiPT | N,N-diisopropyltryptamine | C16H24N2 |  | 244.4 | CH(CH3)2 | CH(CH3)2 | H | H | H | H | H | H |
| 4-Substituted tryptamines | ||||||||||||
| Psilocin | 4-Hydroxy-N,N-dimethyltryptamine | C12H16N2O |  | 204.3 | CH3 | CH3 | H | OH | H | H | H | H |
| Psilocybin | 4-Phosphoryloxy-N,N-dimethyltryptamine | C12H17N2O4P |  | 284.3 | CH3 | CH3 | H | OPO3H2 | H | H | H | H |
| 4-OH-MET | 4-Hydroxy-N-methyl-N-ethyltryptamine | C13H18N2O |  | 218.3 | CH3 | CH2CH3 | H | OH | H | H | H | H |
| 4-OH-DPT | 4-Hydroxy-N,N-dipropyltryptamine | C16H24N2O |  | 260.4 | CH2CH2CH3 | CH2CH2CH3 | H | OH | H | H | H | H |
| 4-OH-DET | 4-Hydroxy-N,N-diethyltryptamine | C14H20N2O |  | 232.3 | CH2CH3 | CH2CH3 | H | OH | H | H | H | H |
| 4-OH-MiPT | 4-Hydroxy-N-methyl-N-isopropyltryptamine | C14H20N2O |  | 232.3 | CH3 | CH(CH3)2 | H | OH | H | H | H | H |
| 4-OH-DiPT | 4-Hydroxy-N,N-diisopropyltryptamine | C16H24N2O |  | 260.4 | CH(CH3)2 | CH(CH3)2 | H | OH | H | H | H | H |
| 4-OH-DALT | 4-Hydroxy-N,N-diallyltryptamine | C16H20N2O |  | 256.3 | CH2CHCH2 | CH2CHCH2 | H | OH | H | H | H | H |
| 4-AcO-MET | 4-Acetoxy-N-methyl-N-ethyltryptamine | C15H20N2O2 |  | 260.3 | CH3 | CH2CH3 | H | OCOCH3 | H | H | H | H |
| 4-AcO-DPT | 4-Acetoxy-N,N-dipropyltryptamine | C18H26N2O2 |  | 302.4 | CH2CH2CH3 | CH2CH2CH3 | H | OCOCH3 | H | H | H | H |
| 4-AcO-DALT | 4-Acetoxy-N,N-diallyltryptamine | C18H22N2O2 |  | 298.4 | CH2CHCH2 | CH2CHCH2 | H | OCOCH3 | H | H | H | H |
| 5-Substituted tryptamines | ||||||||||||
| Bufotenine | 5-Hydroxy-N,N-dimethyltryptamine | C12H16N2O |  | 204.3 | CH3 | CH3 | H | H | OH | H | H | H |
| 5-OH-DiPT | 5-Hydroxy-N,N-diisopropyltryptamine | C16H24N2O |  | 260.4 | CH(CH3)2 | CH(CH3)2 | H | H | OH | H | H | H |
| 5-MeO-α-MT | 5-Methoxy-alpha-methyltryptamine | C12H16N2O |  | 204.3 | H | H | CH3 | H | OCH3 | H | H | H |
| 5-MeO-DMT | 5-Methoxy-N,N-dimethyltryptamine | C13H18N2O |  | 218.3 | CH3 | CH3 | H | H | OCH3 | H | H | H |
| 5-MeO-DPT | 5-Methoxy-N,N-dipropyltryptamine | C17H26N2O |  | 274.4 | CH2CH2CH3 | CH2CH2CH3 | H | H | OCH3 | H | H | H |
| 5-MeO-DiPT | 5-Methoxy-N,N-diisopropyltryptamine | C17H26N2O |  | 274.4 | CH(CH3)2 | CH(CH3)2 | H | H | OCH3 | H | H | H |
| 5-MeO-MiPT | 5-Methoxy-N-methyl-N-isopropyltryptamine | C15H22N2O |  | 246.4 | CH3 | CH(CH3)2 | H | H | OCH3 | H | H | H |
| 5-MeO-IPT | 5-Methoxy-N-isopropyltryptamine | C14H20N2O |  | 232.3 | H | CH(CH3)2 | H | H | OCH3 | H | H | H |
| 5-MeO-MET | 5-Methoxy-N-methyl-N-ethyltryptamine | C14H20N2O |  | 232.3 | CH3 | CH2CH3 | H | H | OCH3 | H | H | H |
| 5-MeO-DET | 5-Methoxy-N,N-diethyltryptamine | C15H22N2O |  | 246.4 | CH2CH3 | CH2CH3 | H | H | OCH3 | H | H | H |
| 5-MeO-DALT | 5-Methoxy-N,N- diallyltryptamine | C17H22N2O |  | 270.4 | CH2CHCH2 | CH2CHCH2 | H | H | OCH3 | H | H | H |
| 5-Me-DALT | 5-Methyl-N,N-diallyltryptamine | C17H22N2 |  | 254.4 | CH2CHCH2 | CH2CHCH2 | H | H | CH3 | H | H | H |
| 5-F-DALT | 5-Fluoro-N,N-diallyltryptamine | C16H19N2F |  | 258.3 | CH2CHCH2 | CH2CHCH2 | H | H | F | H | H | H |
| 5-Cl-DALT | 5-Chloro-N,N-diallyltryptamine | C16H19N2Cl |  | 274.8 | CH2CHCH2 | CH2CHCH2 | H | H | Cl | H | H | H |
| 5-Br-DALT | 5-Bromo-N,N-diallyltryptamine | C16H19N2Br |  | 319.2 | CH2CHCH2 | CH2CHCH2 | H | H | Br | H | H | H |
| 5-MeO-2-Me-DALT | 5-Methoxy-2-methyl-N,N-diallyltryptamine | C18H24N2O |  | 284.4 | CH2CHCH2 | CH2CHCH2 | H | H | OCH3 | H | H | CH3 |
| 5-EtO-DALT | 5-Ethoxy-N,N-diallyltryptamine | C18H24N2O |  | 284.4 | CH2CHCH2 | CH2CHCH2 | H | H | OCH2CH3 | H | H | H |
| Others | ||||||||||||
| 5,6-MD-DALT | 5,6-Methylenedioxy-N,N-diallyltryptamine | C17H20N2O2 |  | 284.4 | CH2CH | CH2CH | H | H | OCH2O * | H | H | |
| 7-Et-DALT | 7-Ethyl-N,N-diallyltryptamine | C18H24N2 |  | 268.4 | CH2CHCH2 | CH2CHCH2 | H | H | H | H | CH2CH3 | H |
| 7-Me-DALT | 7-Methyl-N,N-diallyltryptamine | C17H22N2 |  | 254.4 | CH2CHCH2 | CH2CHCH2 | H | H | H | H | CH3 | H |
| Analytes | Sample (µL) | Sample Preparation | Method | Mobile Phase | Linear Range (ng/mL) | LOD (ng/mL) | LOQ (ng/mL) | Recovery (%) | Accuracy (%) | Intraday Precision (%) | Interday Precision (%) | Concentration (ng/mL) | References |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 5-MeO-DMT α-MT DiPT DMT DPT MiPT | P: 1000 | Dilute; SPE; Evaporate; Resuspend | LC-MS/MS (positive ESI; MRM) | A: 1mM AmFo with 0.1% FA; B: MeOH with 0.1% FA | NA | 1.0 2.5 1.0 2.5 1.0 2.5 | NA | NA | NA | NA | NA | NA | Wohlfarth, 2010 [109] |
| DMT | B: 1000 | Dilute; SPE; Evaporate; Resuspend | LC-QTrap/MS (positive ESI; MRM) | A: 5 mM AmFo with 0.1% FA; B:MeOH with 0.1% FA | NA | 0.1 | 0.2 | 94.0–102.9 | 83.2–95.1 | 3.7–9.3 | 2.5–14.1 | 1.2–19.8 | Oliveira, 2012 [110] |
| Psilocin | P: 500 | Dilute; Centrifuge; SPE; Evaporate; Resuspend | LC-MS/MS (positive EI; MRM) | A: MeOH with 0.1% FA; B: 2 mM AmAc with 0.1% FA | 2–100 | 0.1 | 0.3 | 86 | −8.8–4.1 | 1.5–2.7 | 2.4–4.3 | NA | Martin, 2012 [111] |
| Psilocin Bufotenine | S: 1000 | Dilute; Centrifuge | LC-MS/MS (positive EI; MRM) | A: ACN with 0.1% FA; B: 2 mM AmAc buffer with 0.1% FA (pH3) | 1–17.5 | 0.05 0.05 | 0.17 0.1 | 95 91.6 | −2.9–−1.1 −3.1–−0.6 | 1.16–1.68 3–4.3 | 2.27–4.5 5.43–6.52 | 0.2–0.5 0.5 | Martin, 2013 [112] |
| Psilocin Bufotenine | P: 1000 | Dilute; Centrifuge | LC-MS/MS (positive EI; MRM) | A: ACN with 0.1% FA; B: 2 mM AmAc buffer with 0.1% FA (pH3) | 1–17.5 | 0.05 0.07 | 0.15 0.27 | 93.5 91.3 | −2.9–−1.1 −3.1–−0.6 | 1.16–1.68 3–4.3 | 2.27–4.5 5.43–6.52 | NA | Martin, 2013 [112] |
| Psilocin Bufotenine | U: 500 | Enzymatic hydrolysis; Centrifuge; SPE;Evaporate; Resuspend | LC-MS/MS (positive EI; MRM) | A: ACN with 0.1% FA; B: 2 mM AmAc buffer with 0.1% FA (pH3) | 1–17.5 | 0.2 0.1 | 0.2 0.14 | 91.8 88.8 | −2.9–−1.1 −3.1–−0.6 | 1.16–1.68 3–4.3 | 2.27–4.5 5.43–6.52 | 11–13 1.6–5.9 | Martin, 2013 [112] |
| 5-MeO-DALT 5-MeO-DMT α-MT DiPT DMT DPT | B: 10 | Dilute; DBS; Evaporate; Resuspend. | LC-MS/MS (positive ESI; MRM) | A: water with 0.1% FA; B: ACN with 0.1% FA; | NA | 1.0 1.0 2.5 1.0 1.0 1.0 | NA | NA | NA | NA | NA | NA | Ambach, 2014 [113] |
| 5-MeO-DALT 5-MeO-DMT α-MT DiPT DMT DPT | B: 500 | Dilute; Centrifuge; SPE; Wash; Evaporate; Resuspend. | LC-MS/MS (positive ESI; sMRM) | A: 10 mM AmFo with 0.1% FA; B: MeOH with 0.1% FA | 2.5–1000 | NA | 2.5 2.5 2.5 2.5 52.5 | NA | NA | NA | NA | NA | Ambach, 2015 [114] |
| 5-MeO-DALT 5-MeO-DMT α-MT DiPT DMT DPT | U: 250 | LLE: Dilute; Centrifuge; Organic phase: evaporated; Residue: resuspended. | LC-MS/MS (positive ESI; sMRM) | A: 10 mM AmFo with 0.1% FA; B: MeOH with 0.1% FA | 1 1 2.5 1 2.5 1 | NA | NA | NA | NA | NA | Ambach, 2015 [114] | ||
| 5-MeO-DALT | B: 500 | Protein precipitation; DLLME; Centrifuge; Resuspend | LC–MS/MS (positive ESI; sMRM) | A:5mM AmFo with 0.1% AF; B: MeOH with 0.1% FA | 2–1000 | 0.2–2 | NA | 5–110 | NA | NA | NA | NA | Odoardi, 2015 [115] |
| Psilocin Bufotenine | H: 50 mg | Wash; Centrifuge; Resuspend | LC-MS/MS (positive EI; MRM) | A: ACN with 0.1% FA; B: 2 mM AmAc buffer with 0.1% FA | 0.04–2 | 10 pg/mg | 16 pg/mg 22 pg/mg | NA | −2.5–−0. 54–8.8 | 0.8–2.47 4.8–8.3 | 1.78–2.91 6.7–9.6 | 0.14–1.45 | Martin, 2015 [116] |
| DALT 5-MeO-DALT | U:100 | Dilute; Centrifuge; Evaporate; Resuspend | LC-HR-MS/MS (positive ionization; full scan & DDA) | A: 2 mM AmFo with 0.1% FA; B: 2 mM AmFo : ACN:MeOH (50:50, v/v; 1% water) with 0.1% FA | NA | 1 | NA | NA | NA | NA | NA | NA | Michely, 2015 [102] |
| DALT 5-MeO-DALT | U: 5000 | Acid hydrolysis | GC–MS SUSA (positive EI; full scan) | helium | NA | 10 50 | NA | NA | NA | NA | NA | NA | Michely, 2015 [102] |
| 4-OH-DET 4-OH-DIPT 4-OH-MET 4-OH-MIPT 4-MeO-DMT 4-AcO-DiPT 5-MeO-α-MT 5-Meo-DALT 5-MeO-DiPT 5-MeO-DMT 5-MeO-MiPT α-MT DiPT DMT DPT MET NMT DET | B: 200 | Dilute; Protein precipitation; Centrifuge; Evaporate; Resuspend | LC-MS/MS (positive ESI; dMRM) | A: ACN with 0.1% FA; B: water with 0.1% FA | 1–100 | 0.06 1.05 NA NA 2.98 0.99 0.11 1.11 0.15 2.61 NA 2.61 0.88 0.08 0.30 NA 1.50 0.72 | NA | 17.1 | DMT:111 | DMT:7 | DMT: 10.3 | DMT:11.1 | Adamowicz, 2016 [117] |
| DALT 2-Ph-DALT 4-AcO-DALT 4-OH-DALT 5-Me-DALT 5-MeO-DALT 5-MeO-2-Me-DALT 5-EtO-DALT 5-F-DALT 5-F-2-Me-DALT 5-Cl-DALT 5-Br-DALT 6-F-DALT 7-Me-DALT 7-Et-DALT | B, P, U: NA | Dilute and shoot | GC-MS; sIR; (positive ESI; full scan & PDA) | helium | NA | NA | NA | NA | NA | NA | NA | NA | Brandt, 2016 [118] |
| DALT 2-Ph-DALT 4-AcO-DALT 4-OH-DALT 5-Me-DALT 5-MeO-DALT 5-MeO-2-Me-DALT 5-EtO-DALT 5-F-DALT 5-F-2-Me-DALT 5-Cl-DALT 5-Br-DALT 6-F-DALT 7-Me-DALT 7-Et-DALT | B, P, U: NA | Dilute and shoot | LC-MS; sIR; (positive HESI; full scan & DDA) | A: water with 0.1% FA; B: ACN with 0.1% FA | NA | NA | NA | NA | NA | NA | NA | NA | Brandt, 2016 [118] |
| 5-MeO-DiPT 4-OH-DiPT | B: 200 | Protein precipitation; Centrifuge; Evaporate; Resuspend | LC-MS/MS (positive ESI; MRM; full scan & DDA) | A: 5 mM FA B: ACN | 1–100 | 0.1 | 0.3 | 84 91 | −13.3–6.3 7.7–14.7 | −9.9–14.9 2.2–15.7 | 9.7–14.6 6.9–14.1 | NA | Vaiano, 2016 [119] |
| DMT 5-MeO-DMT α-MT | OF: 500 | Dilution; LLE; Centrifuge; Evaporate; Resuspend | UHPLC-MS/MS (positive ESI; MRM) | A:10mM AmFo B: meOH | NA | NA | NA | NA | NA | NA | NA | NA | Gjerde, 2016 [120] |
| 5-MeO-MiPT | S: 100 | Dilute; Centrifuge; Evaporate; Resuspend | UHPLC-HRMS XEVO G2 QTOFMS (positive ESI) | A: water with 0.01% FA; B:MeOH with 0.01% FA | NA | NA | NA | NA | NA | NA | NA | NA | Fabregat-Safont, 2017 [121] |
| 5-MeO-MiPT | U: 200 | Enzymatic hydrolysis; Protein precipitation; Centrifuge | UHPLC-HRMS interfaced to a XEVO G2 QTOF MS(positive ESI) | A: water with 0.01% FA; B:MeOH with 0.01% FA | NA | NA | NA | NA | NA | NA | NA | NA | Fabregat-Safont, 2017 [121] |
| 5-MeO-MiPT | U: 100 | Protein precipitation; Centrifuge | UHPLC-HRMS interfaced to a XEVO G2 QTOF MS (positive ESI) | A: water with 0.01% FA; B:MeOH with 0.01% FA | NA | NA | NA | NA | NA | NA | NA | NA | Fabregat-Safont, 2017 [121] |
| 5-F-DALT 7-Me-DALT 6-MD-DALT | U: 100 | Dilute; Centrifuge; Evaporate; Resuspend | LC-HRMS/MS (positive HESI; full scan & DDA | A: 2 mM aqueous AmFo with 0.1% FA (pH 3); B: 2 mM aqueous AmFo with ACN:MeOH (1:1, v/v; 1% water) with 0.1% FA | NA | NA | NA | NA | NA | NA | NA | NA | Michely, 2017 [122] |
| 5-F-DALT 7-Me-DALT 5,6-MD-DALT | U: 2500 | Acid hydrolysis | GC-MS SUSA (positive ESI; full scan) | helium | NA | NA | NA | NA | NA | NA | NA | NA | Michely, 2017 [122] |
| Psilocin DMT 5-MeO-DMT | B: 1000 | Centrifuge; Evaporate; Resuspend | LC-MS/MS (positive ESI; dMRM) | A: 5mM AmFo in water with 0.01% FA; B: ACN with 0.01% FA | NA | 2.50 | NA | NA | NA | NA | NA | NA | Fagiola, 2018 [123] |
| Psilocin DMT 5-MeO-DMT | U: 1000 | Centrifuge; Evaporate; Resuspend | LC-MS/MS (positive ESI; dMRM) | A: 5mM AmFo in water with 0.01% FA; B: ACN with 0.01% FA | NA | 2.50 | NA | NA | NA | NA | NA | NA | Fagiola, 2018 [123] |
| 5-MeO-DiPT | H: 30 mg | Wash; Pulverize; Centrifuge | LC-MS/MS (positive ESI; MRM) | A: 20 mM AmAc, 5% ACN and water with 0.1% FA; B: ACN with 0.1% FA | 0.1–100 pg/mg | NA | 0.1 pg/mg | 91.1–112 | 92.1–106 | <13 | 12.1–17.0 | 0.2–7533 pg/mg | Roujia, 2019 [124] |
| DMT Psilocybin | U: NA | Dilute | LC-QTOF (positive ESI) | A: 5 mM AmFo (pH 3) B: ACN with 0.1% AF | NA | 1–2 | NA | NA | NA | NA | NA | NA | Pope, 2019 [125] |
| 5-MeO-DiPT 5-OH-DiPT 5-MeO-IPT | U:1000 | Centrifuge; Resuspend | GC- Orbitrap- MS (positive EI; full scan) | helium | 2–300 | 1 | 2 | 92.4–98.4 | 93–108.7 | 3.1–7.2 | 7.2–10.3 | 2–2.8 | Yan, 2020 [126] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malaca, S.; Lo Faro, A.F.; Tamborra, A.; Pichini, S.; Busardò, F.P.; Huestis, M.A. Toxicology and Analysis of Psychoactive Tryptamines. Int. J. Mol. Sci. 2020, 21, 9279. https://doi.org/10.3390/ijms21239279
Malaca S, Lo Faro AF, Tamborra A, Pichini S, Busardò FP, Huestis MA. Toxicology and Analysis of Psychoactive Tryptamines. International Journal of Molecular Sciences. 2020; 21(23):9279. https://doi.org/10.3390/ijms21239279
Chicago/Turabian StyleMalaca, Sara, Alfredo Fabrizio Lo Faro, Alice Tamborra, Simona Pichini, Francesco Paolo Busardò, and Marilyn A. Huestis. 2020. "Toxicology and Analysis of Psychoactive Tryptamines" International Journal of Molecular Sciences 21, no. 23: 9279. https://doi.org/10.3390/ijms21239279
APA StyleMalaca, S., Lo Faro, A. F., Tamborra, A., Pichini, S., Busardò, F. P., & Huestis, M. A. (2020). Toxicology and Analysis of Psychoactive Tryptamines. International Journal of Molecular Sciences, 21(23), 9279. https://doi.org/10.3390/ijms21239279