Monoclonal Antibodies and Airway Diseases

 , , and
, , and
Abstract
:1. Introduction
2. Monoclonal Antibodies
3. Chronic Inflammatory Airway Diseases
3.1. Asthma and Airway Allergy
3.2. CRS
3.3. Co-Morbid Asthma and CRS
3.4. Mechanisms behind Airway Diseases
4. The Role of Antibodies in Airway Diseases
4.1. IgE
4.2. Other Antibodies
5. Monoclonal Antibodies and Diagnostics of Airway Diseases
5.1. Measurement of Total and Specific IgE in Airway Diseases
5.2. Potential Biomarkers for Airway Diseases
6. Monoclonal Antibodies and Treatment of Airway Diseases
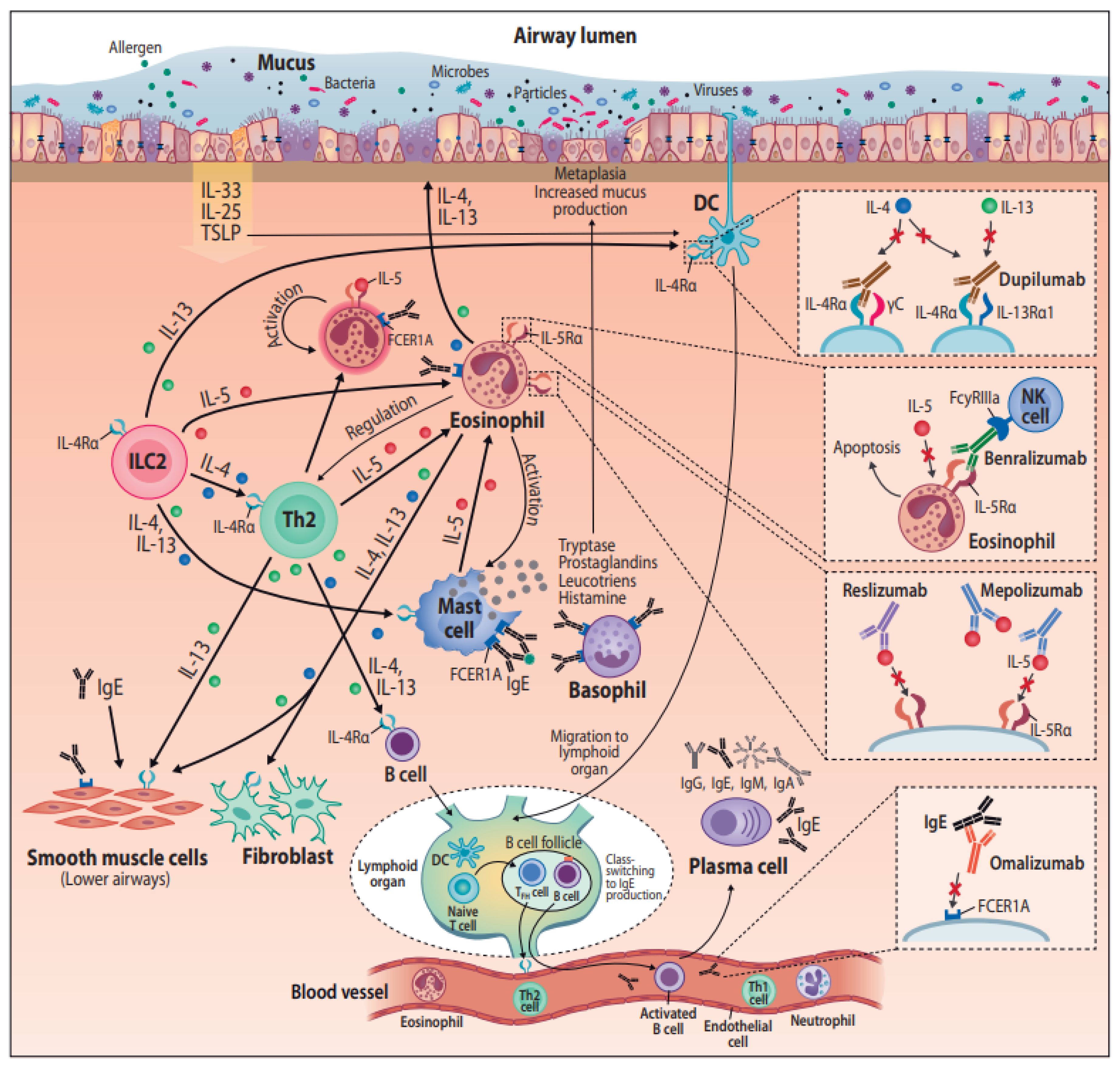
6.1. Commercially Available Monoclonal Antibodies and Their Mechanisms of Action
6.1.1. Omalizumab—Anti-IgE
6.1.2. Mepolizumab and Reslizumab—Anti-IL-5
6.1.3. Benralizumab—Anti-IL-5Ralpha
6.1.4. Dupilumab—Anti IL-4Ralpha
6.2. Monoclonal Antibodies in Asthma Treatment
6.3. Monoclonal Antibodies in CRS Treatment
6.4. Future Monoclonal Antibody Treatments for Airway Diseases
6.4.1. Anti-TSLP
6.4.2. Anti-TNF
6.4.3. Anti-IL-8
6.4.4. CRTH2 Antagonists
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CRS | Chronic rhinosinusitis |
| CRSwNP | Chronic rhinosinusitis with nasal polyps |
| N-ERD | NSAID-exacerbated respiratory disease |
| mAb | Monoclonal antibody |
| RCT | Randomized controlled trial |
References
- Dierick, B.J.; Van Der Molen, T.; Flokstra-de-Blok, B.M.J.; Muraro, A.; Postma, M.J.; Kocks, J.W.; Van Boven, J.F. Burden and socioeconomics of asthma, allergic rhinitis, atopic dermatitis and food allergy. Expert Rev. Pharm. Outcomes Res. 2020, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Hastan, D.; Fokkens, W.; Bachert, C.; Newson, R.B.; Bislimovska, J.; Bockelbrink, A.; Bousquet, P.J.; Brozek, G.; Bruno, A.; Dahlén, S.E.; et al. Chronic rhinosinusitis in Europe—An Underestimated Disease. A GA2LEN study. Allergy 2011, 66, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Settipane, R.A.; Kaliner, M. Nonallergic Rhinitis. Am. J. Rhinol. Allergy 2013, 27, S48–S51. [Google Scholar] [CrossRef] [PubMed]
- Toskala, E.; Kennedy, D.W. Asthma risk factors. Int. Forum Allergy Rhinol. 2015, 5, S11–S16. [Google Scholar] [CrossRef] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Global Strategy for Asthma Management and Prevention. Available online: www.ginasthma.org (accessed on 20 April 2020).
- Bousquet, J.; Anto, J.M.; Bachert, C.; Baiardini, I.; Bosnic-Anticevich, S.; Canonica, G.W.; Melen, E.; Palomares, O.; Scadding, G.K.; Togias, A.; et al. Allergic rhinitis. Nat. Rev. 2020, 6, 1–17. [Google Scholar]
- Barnes, P.J. Intrinsic asthma: Not so different from allergic asthma but driven by superantigens? Clin. Exp. Allergy 2009, 39, 1145–1151. [Google Scholar] [CrossRef]
- Panda, S.; Ding, J.L. Natural Antibodies Bridge Innate and Adaptive Immunity. J. Immunol. 2014, 194, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Marshall, J.S.; Warrington, R.; Watson, W.; Kim, H.L. An introduction to immunology and immunopathology. Allergy Asthma Clin. Immunol. 2018, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Köhler, G.; Milstein, C. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature 1975, 256, 495–497. [Google Scholar] [CrossRef]
- Vaisman-Mentesh, A.; Gutierrez-Gonzalez, M.; DeKosky, B.J.; Wine, Y. The Molecular Mechanisms That Underlie the Immune Biology of Anti-drug Antibody Formation Following Treatment with Monoclonal Antibodies. Front. Immunol. 2020, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.L.; Moshiri, A.S.; Novoa, R.; Simpson, C.L.; Takeshita, J.; Payne, A.S.; Chu, E.Y. Comparison of C3d immunohistochemical staining to enzyme-linked immunosorbent assay and immunofluorescence for diagnosis of bullous pemphigoid. J. Am. Acad. Dermatol. 2020, 83, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Black, C.A. A brief history of the discovery of the immunoglobulins and the origin of the modern immunoglobulin nomenclature. Immunol. Cell Biol. 1997, 75, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Platts-Mills, T.A.; Heymann, P.W.; Commins, S.P.; Woodfolk, J.A. The discovery of IgE 50 years later. Ann. Allergy Asthma Immunol. 2016, 116, 179–182. [Google Scholar] [CrossRef] [Green Version]
- McCracken, J.L.; Veeranki, S.P.; Ameredes, B.T.; Calhoun, W.J. Diagnosis and management of asthma in adults a review. JAMA—J. Am. Med. Assoc. 2017, 318, 279–290. [Google Scholar] [CrossRef]
- Porsbjerg, C.; Ulrik, C.; Skjold, T.; Backer, V.; Laerum, B.; Lehman, S.; Janson, C.; Sandstrøm, T.; Bjermer, L.; Dahlen, B.; et al. Nordic consensus statement on the systematic assessment and management of possible severe asthma in adults. Eur. Clin. Respir. J. 2018, 5, 1440868. [Google Scholar] [CrossRef]
- Kerkhof, M.; Tran, T.N.; Soriano, J.B.; Golam, S.; Gibson, D.; Hillyer, E.V.; Price, D. Healthcare resource use and costs of severe, uncontrolled eosinophilic asthma in the UK general population. Thorax 2017, 73, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Larsen, K.; Tos, M. The Estimated Incidence of Symptomatic Nasal Polyps. Acta Oto-Laryngol. 2002, 122, 179–182. [Google Scholar] [CrossRef]
- Johansson, L.; Åkerlund, A.; Melén, I.; Holmberg, K.; Bende, M. Prevalence of Nasal Polyps in Adults: The Skovde Population-Based Study. Ann. Otol. Rhinol. Laryngol. 2003, 112, 625–629. [Google Scholar] [CrossRef]
- McCormick, J.P.; Thompson, H.M.; Cho, D.-Y.; Woodworth, B.A.; Grayson, J.W. Phenotypes in Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyly, A.; Laulajainen-Hongisto, A.; Turpeinen, H.; Vento, S.I.; Myller, J.; Numminen, J.; Sillanpää, S.; Sahlman, J.; Kauppi, P.; Toppila-Salmi, S. Factors affecting upper airway control of NSAID-exacerbated respiratory disease: A real-world study of 167 patients. Immun. Inflamm. Dis. 2020, in press. [Google Scholar] [CrossRef]
- Jarvis, D.; Newson, R.; Lotvall, J.; Hastan, D.; Tomassen, P.; Keil, T.; Gjomarkaj, M.; Forsberg, B.; Gunnbjornsdottir, M.; Minov, J.; et al. Asthma in adults and its association with chronic rhinosinusitis: The GA2LEN survey in Europe. Allergy 2012, 67, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Bashiardes, S.; Zilberman-Schapira, G.; Elinav, E. Use of Metatranscriptomics in Microbiome Research. Bioinform. Biol. Insights 2016, 10, BBI.S34610–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laulajainen-Hongisto, A.; Toppila-Salmi, S.K.; Luukkainen, A.; Kern, R. Airway Epithelial Dynamics in Allergy and Related Chronic Inflammatory Airway Diseases. Front. Cell Dev. Biol. 2020, 8, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gause, W.C.; Rothlin, C.; Loke, P. Heterogeneity in the initiation, development and function of type 2 immunity. Nat. Rev. Immunol. 2020, 20, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Gough, H.; Grabenhenrich, L.; Reich, A.; Eckers, N.; Nitsche, O.; Schramm, D.; Beschorner, J.; Hoffmann, U.; Schuster, A.; Bauer, C.; et al. Allergic multimorbidity of asthma, rhinitis and eczema over 20 years in the German birth cohort MAS. Pediatric Allergy Immunol. 2015, 26, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Toppila-Salmi, S.; Chanoine, S.; Karjalainen, J.; Pekkanen, J.; Bousquet, J.; Siroux, V. Risk of adult-onset asthma increases with the number of allergic multimorbidities and decreases with age. Allergy 2019, 74, 2406–2416. [Google Scholar] [CrossRef] [Green Version]
- Willis-Owen, S.A.; Cookson, W.O.; Moffatt, M.F. The Genetics and Genomics of Asthma. Annu. Rev. Genom. Hum. Genet. 2018, 19, 223–246. [Google Scholar] [CrossRef]
- Stevenson, D.D.; Szczeklik, A. Clinical and pathologic perspectives on aspirin sensitivity and asthma. J. Allergy Clin. Immunol. 2006, 118, 773–786. [Google Scholar] [CrossRef]
- White, A.A.; Stevenson, D.D. Aspirin-Exacerbated Respiratory Disease. N. Engl. J. Med. 2018, 379, 1060–1070. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, M.L.; Agache, I.; Bavbek, S.; Bakirtas, A.; Blanca, M.; Bochenek, G.; Bonini, M.; Heffler, E.; Klimek, L.; Laidlaw, T.M.; et al. Diagnosis and Management of NSAID-Exacerbated Respiratory Disease (N-ERD)—A EAACI Position Paper. Allergy 2018, 74, 28–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascia, K.; Haselkorn, T.; Deniz, Y.M.; Miller, D.P.; Bleecker, E.R.; Borish, L. Aspirin sensitivity and severity of asthma: Evidence for irreversible airway obstruction in patients with severe or difficult-to-treat asthma. J. Allergy Clin. Immunol. 2005, 116, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Roca-Ferrer, J.; Perez-Gonzalez, M.; Garcia-Garcia, F.J.; Pereda, J.; Pujols, L.; Alobid, I.; Mullol, J.; Picado, C. Low prostaglandin E2and cyclooxygenase expression in nasal mucosa fibroblasts of aspirin-intolerant asthmatics. Respirology 2013, 18, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, J.R.; Teran, L.M. Aspirin-Intolerant Asthma: A Comprehensive Review of Biomarkers and Pathophysiology. Clin. Rev. Allergy Immunol. 2012, 45, 75–86. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinol. J. 2012, 50, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, D.D.; Simon, R.A.; Mathison, D.A. Aspirin-sensitive asthma: Tolerance to aspirin after positive oral aspirin challenges. J. Allergy Clin. Immunol. 1980, 66, 82–88. [Google Scholar] [CrossRef]
- Laulajainen-Hongisto, A.; Turpeinen, H.; Vento, S.I.; Numminen, J.; Sahlman, J.; Kauppi, P.; Virkkula, P.; Hytönen, M.; Toppila-Salmi, S. High Discontinuation Rates of Peroral ASA Treatment for CRSwNP: A Real-World Multicenter Study of 171 N-ERD Patients. J. Allergy Clin. Immunol. Pract. 2020, 8, 3565–3574. [Google Scholar] [CrossRef]
- Iqbal, I.Z.; Kao, S.S.; Ooi, E.H. The role of biologics in chronic rhinosinusitis: A systematic review. Int. Forum Allergy Rhinol. 2019, 10, 165–174. [Google Scholar] [CrossRef]
- Kim, C.; Han, J.; Wu, T.; Bachert, C.; Fokkens, W.; Hellings, P.; Hopkins, C.; Lee, S.; Mullol, J.; Lee, J.T. Role of Biologics in Chronic Rhinosinusitis with Nasal Polyposis: State of the Art Review. Otolaryngol. Neck Surg. 2020. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Buchheit, K.M. Biologics in chronic rhinosinusitis with nasal polyposis. Ann. Allergy Asthma Immunol. 2020, 124, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyerich, S.; Metz, M.; Bossios, A.; Eyerich, K. New biological treatments for asthma and skin allergies. Allergy 2020, 75, 546–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Licona-Limon, P.; Kim, L.K.; Palm, N.W.; Flavell, R. TH2, allergy and group 2 innate lymphoid cells. Nat. Immunol. 2013, 14, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Scadding, G. Cytokine profiles in allergic rhinitis topical collection on rhinitis. Curr. Allergy Asthma Rep. 2014, 14, 326–332. [Google Scholar] [CrossRef]
- Toppila-Salmi, S.; Van Drunen, C.M.; Fokkens, W.J.; Golebski, K.; Mattila, P.; Joenväärä, S.; Renkonen, J.; Renkonen, R. Molecular mechanisms of nasal epithelium in rhinitis and rhinosinusitis. Curr. Allergy Asthma Rep. 2015, 15, 495. [Google Scholar] [CrossRef] [Green Version]
- Cheng, G.; Arima, M.; Honda, K.; Hirata, H.; Eda, F.; Yoshida, N.; Fukushima, F.; Ishii, Y.; Fukuda, T. Anti–Interleukin-9 Antibody Treatment Inhibits Airway Inflammation and Hyperreactivity in Mouse Asthma Model. Am. J. Respir. Crit. Care Med. 2002, 166, 409–416. [Google Scholar] [CrossRef]
- Whitsett, J.A.; Alenghat, T. Respiratory epithelial cells orchestrate pulmonary innate immunity. Nat. Immunol. 2015, 16, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Athari, S.S. Targeting cell signaling in allergic asthma. Signal Transduct. Target. Ther. 2019, 4, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Cutting, G.R. Modifier Genetics: Cystic Fibrosis. Annu. Rev. Genom. Hum. Genet. 2005, 6, 237–260. [Google Scholar] [CrossRef]
- Gudis, D.; Zhao, K.-Q.; Cohen, N.A. Acquired Cilia Dysfunction in Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2012, 26, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ryu, G.; Kim, D.W. Th2 inflammatory responses in the development of nasal polyps and chronic rhinosinusitis. Curr. Opin. Allergy Clin. Immunol. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Stentzel, S.; Teufelberger, A.; Nordengrün, M.; Kolata, J.; Schmidt, F.; Van Crombruggen, K.; Michalik, S.; Kumpfmüller, J.; Tischer, S.; Schweder, T.; et al. Staphylococcal serine protease–like proteins are pacemakers of allergic airway reactions to Staphylococcus aureus. J. Allergy Clin. Immunol. 2017, 139, 492–500.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takabayashi, T.; Kato, A.; Peters, A.T.; Hulse, K.E.; Suh, L.A.; Carter, R.; Norton, J.; Grammer, L.C.; Cho, S.H.; Tan, B.K.; et al. Excessive Fibrin Deposition in Nasal Polyps Caused by Fibrinolytic Impairment through Reduction of Tissue Plasminogen Activator Expression. Am. J. Respir. Crit. Care Med. 2013, 187, 49–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siroux, V.; Ballardini, N.; Soler, M.; Lupinek, C.; Boudier, A.; Pin, I.; Just, J.; Nadif, R.; Antó, J.-M.; Melen, E.; et al. The asthma-rhinitis multimorbidity is associated with IgE polysensitization in adolescents and adults. Allergy 2018, 73, 1447–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachert, C.; Humbert, M.; Hanania, N.A.; Zhang, N.; Holgate, S.; Buhl, R.; Bröker, B.M. Staphylococcus aureus and its IgE-inducing enterotoxins in asthma: Current knowledge. Eur. Respir. J. 2020, 55, 1901592. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Zhang, N.; Holtappels, G.; De Lobel, L.; Van Cauwenberge, P.; Liu, S.; Lin, P.; Bousquet, J.; Van Steen, K. Presence of IL-5 protein and IgE antibodies to staphylococcal enterotoxins in nasal polyps is associated with comorbid asthma. J. Allergy Clin. Immunol. 2010, 126, 962–968.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomassen, P.; Jarvis, D.; Newson, R.; Van Ree, R.; Forsberg, B.; Howarth, P.; Janson, C.; Kowalski, M.L.; Krämer, U.; Matricardi, P.M.; et al. Staphylococcus aureus enterotoxin-specific IgE is associated with asthma in the general population: A GA(2)LEN study. Allergy 2013, 68, 1289–1297. [Google Scholar] [CrossRef]
- Bachert, C.; Marple, B.; Hosemann, W.; Cavaliere, C.; Wen, W.; Zhang, N. Endotypes of Chronic Rhinosinusitis with Nasal Polyps: Pathology and Possible Therapeutic Implications. J. Allergy Clin. Immunol. Pract. 2020, 8, 1514–1519. [Google Scholar] [CrossRef]
- Lan, F.; Zhang, N.; Holtappels, G.; De Ruyck, N.; Krysko, O.; Van Crombruggen, K.; Braun, H.; Johnston, S.L.; Papadopoulos, N.G.; Zhang, L.; et al. Staphylococcus aureusInduces a Mucosal Type 2 Immune Response via Epithelial Cell–derived Cytokines. Am. J. Respir. Crit. Care Med. 2018, 198, 452–463. [Google Scholar] [CrossRef]
- Bachert, C.; Holtappels, G.; Merabishvili, M.; Meyer, T.C.; Murr, A.; Zhang, N.; Van Crombruggen, K.; Gevaert, E.; Völker, U.; Bröker, B.M.; et al. Staphylococcus aureus controls interleukin-5 release in upper airway inflammation. J. Proteom. 2018, 180, 53–60. [Google Scholar] [CrossRef]
- Takeda, K.; Sakakibara, S.; Yamashita, K.; Motooka, D.; Nakamura, S.; El Hussien, M.A.; Katayama, J.; Maeda, Y.; Nakata, M.; Hamada, S.; et al. Allergic conversion of protective mucosal immunity against nasal bacteria in patients with chronic rhinosinusitis with nasal polyposis. J. Allergy Clin. Immunol. 2019, 143, 1163–1175.e15. [Google Scholar] [CrossRef] [PubMed]
- Cheng, K.-J.; Wang, S.-Q.; Xu, Y.-Y. Different roles of Staphylococcus aureus enterotoxin in different subtypes of nasal polyps. Exp. Ther. Med. 2016, 13, 321–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ba, L.; Zhang, N.; Meng, J.; Zhang, J.; Lin, P.; Zhou, P.; Liu, S.; Bachert, C. The association between bacterial colonization and inflammatory pattern in Chinese chronic rhinosinusitis patients with nasal polyps. Allergy 2011, 66, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Ocampo, C.J.; Peters, A.T. Antibody Deficiency in Chronic Rhinosinusitis: Epidemiology and Burden of Illness. Am. J. Rhinol. Allergy 2013, 27, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Cragg, M.S. Engineered antibodies to combat viral threats. Nature 2020. [Google Scholar] [CrossRef] [PubMed]
- Pelegrin, M.; Naranjo-Gomez, M.; Piechaczyk, M. Antiviral Monoclonal Antibodies: Can They Be More Than Simple Neutralizing Agents? Trends Microbiol. 2015, 23, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Verduyn, M.; Botto, G.; Jaubert, J.; Lier, C.; Flament, T.; Guilleminault, L. Serum IgG Concentrations in Adult Patients Experiencing Virus-Induced Severe Asthma Exacerbations. J. Allergy Clin. Immunol. Pract. 2019, 7, 1507–1513.e1. [Google Scholar] [CrossRef]
- Kim, H.; Ellis, A.K.; Fischer, D.A.; Noseworthy, M.; Olivenstein, R.; Chapman, K.R.; Lee, J. Asthma biomarkers in the age of biologics. Allergy Asthma Clin. Immunol. 2017, 13, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Fahy, J.V. Type 2 Inflammation in Asthma—Present in Most, Absent in Many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef]
- Robinson, D.; Humbert, M.; Buhl, R.; Cruz, A.A.; Inoue, H.; Korom, S.; Hanania, N.A.; Nair, P. Revisiting Type 2-high and Type 2-low airway inflammation in asthma: Current knowledge and therapeutic implications. Clin. Exp. Allergy 2017, 47, 161–175. [Google Scholar] [CrossRef]
- Barranco, P.; Phillips-Angles, E.; Dominguez-Ortega, J.; Quirce, S. Dupilumab in the management of moderate-to-severe asthma: The data so far. Ther. Clin. Risk Manag. 2017, 13, 1139–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Chen, D.; Zhou, H.; Zhang, W.; Xu, J.; Chen, L. The Role of Periostin in the Occurrence and Progression of Eosinophilic Chronic Sinusitis with Nasal Polyps. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Wang, X.; Zhang, N.; Wang, H.; Li, Y.; Fan, E.; Zhang, L.; Zhang, L.; Bachert, C. Association of periostin expression with eosinophilic inflammation in nasal polyps. J. Allergy Clin. Immunol. 2015, 136, 1700–1703.e9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebenezer, J.A.; Christensen, J.M.; Oliver, B.G.; Oliver, R.A.; Tjin, G.; Ho, J.; Habib, A.R.; Rimmer, J.; Sacks, R.; Harvey, R.J. Periostin as a marker of mucosal remodelling in chronic rhinosinusitis. Rhinol. J. 2017, 55, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Scioscia, G.; Lacedonia, D.; Soccio, P.; Lepore, G.; Saetta, M.; Barbaro, M.P.F.; Barnes, P.J. Looking for Airways Periostin in Severe Asthma: Could it Be Useful for Clustering Type 2 Endotype? Chest 2018, 154, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Ledger, K.S.; Agee, S.J.; Kasaian, M.T.; Forlow, S.B.; Durn, B.L.; Minyard, J.; Lu, Q.A.; Todd, J.; Vesterqvist, O.; Burczynski, M.E. Analytical validation of a highly sensitive microparticle-based immunoassay for the quantitation of IL-13 in human serum using the Erenna® immunoassay system. J. Immunol. Methods 2009, 350, 161–170. [Google Scholar] [CrossRef]
- Jeanblanc, N.M.; Hemken, P.M.; Datwyler, M.J.; Brophy, S.E.; Manetz, T.S.; Lee, R.; Liang, M.; Chowdhury, P.S.; Varkey, R.; Grant, E.P.; et al. Development of a new ARCHITECT automated periostin immunoassay. Clin. Chim. Acta 2017, 464, 228–235. [Google Scholar] [CrossRef]
- Schryver, E.D.; Derycke, L.; Calus, L.; Holtappels, G.; Hellings, P.W.; Van Zele, T.; Bachert, C.; Gevaert, P. The effect of systemic treatments on periostin expression reflects their interference with the eosinophilic inflammation in chronic rhinosinusitis with nasal polyps. Rhinology 2017, 55, 152–160. [Google Scholar] [CrossRef]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Kinch, M.S. An overview of FDA-approved biologics medicines. Drug Discov. Today 2015, 20, 393–398. [Google Scholar] [CrossRef]
- De Greve, G.; Hellings, P.; Fokkens, W.; Pugin, B.; Callebaut, I.; Seys, S.F. Endotype-driven treatment in chronic upper airway diseases. Clin. Transl. Allergy 2017, 7, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardell, L.; Stjärne, P.; Jonstam, K.; Bachert, C. Endotypes of chronic rhinosinusitis: Impact on management. J. Allergy Clin. Immunol. 2020, 145, 752–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manka, L.A.; Wechsler, M.E. Selecting the right biologic for your patients with severe asthma. Ann. Allergy Asthma Immunol. 2018, 121, 406–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geha, R.S.; Jabara, H.H.; Brodeur, S.R. The regulation of immunoglobulin E class-switch recombination. Nat. Rev. Immunol. 2003, 3, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Pelaia, C.; Calabrese, C.; Terracciano, R.; De Blasio, F.; Vatrella, A.; Pelaia, G. Omalizumab, the first available antibody for biological treatment of severe asthma: More than a decade of real-life effectiveness. Ther. Adv. Respir. Dis. 2018, 12, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, L.A.; Marcotte, G.V.; MacGlashan, D.M., Jr.; Togias, A.; Saini, S.S. Omalizumab-induced reductions in mast cell FcεRI expression and function. J. Allergy Clin. Immunol. 2004, 114, 527–530. [Google Scholar] [CrossRef] [PubMed]
- MacGlashan, D.W.; Bochner, B.S.; Adelman, D.C.; Jardieu, P.M.; Togias, A.; McKenzie-White, J.; Sterbinsky, S.A.; Hamilton, R.G.; Lichtenstein, L.M. Down-regulation of Fc(epsilon)RI expression on human basophils during in vivo treatment of atopic patients with anti-IgE antibody. J. Immunol. 1997, 158, 1438–1445. [Google Scholar]
- Novosad, J.; Krčmová, I. Evolution of our view on the IgE molecule role in bronchial asthma and the clinical effect of its modulation by omalizumab: Where do we stand today? Int. J. Immunopathol. Pharmacol. 2020, 34. [Google Scholar] [CrossRef]
- Bousquet, J.; Chanez, P.; Lacoste, J.Y.; Barnéon, G.; Ghavanian, N.; Enander, I.; Venge, P.; Ahlstedt, S.; Simony-Lafontaine, J.; Godard, P.; et al. Eosinophilic Inflammation in Asthma. N. Engl. J. Med. 1990, 323, 1033–1039. [Google Scholar] [CrossRef]
- Fulkerson, P.C.; Rothenberg, M.E. Targeting eosinophils in allergy, inflammation and beyond. Nat. Rev. Drug Discov. 2013, 12, 117–129. [Google Scholar] [CrossRef] [Green Version]
- Pelaia, C.; Paoletti, G.; Puggioni, F.; Racca, F.; Pelaia, G.; Canonica, G.W.; Heffler, E. Interleukin-5 in the Pathophysiology of Severe Asthma. Front. Physiol. 2019, 10, 1514. [Google Scholar] [CrossRef] [PubMed]
- Gnanakumaran, G.; Babu, K.S. Technology evaluation: Mepolizumab, GlaxoSmithKline. Curr. Opin. Mol. Ther. 2003, 5, 321–325. [Google Scholar] [PubMed]
- Fainardi, V.; Pisi, G.; Chetta, A. Mepolizumab in the treatment of severe eosinophilic asthma. Immunotherapy 2016, 8, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Kuvelkar, R.; Murgolo, N.J.; Taremi, S.S.; Chou, C.-C.; Wang, P.; Billah, M.M.; Egan, R.W. Mapping and characterization of the epitope(s) of Sch 55700, a humanized mAb, that inhibits human IL-5. Int. Immunol. 1999, 11, 1935–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolbeck, R.; Kozhich, A.; Koike, M.; Peng, L.; Andersson, C.K.; Damschroder, M.M.; Reed, J.L.; Woods, R.; Dall’Acqua, W.W.; Stephens, G.L.; et al. MEDI-563, a humanized anti–IL-5 receptor α mAb with enhanced antibody-dependent cell-mediated cytotoxicity function. J. Allergy Clin. Immunol. 2010, 125, 1344–1353.e2. [Google Scholar] [CrossRef]
- Ghazi, A.; Trikha, A.; Calhoun, W.J. Benralizumab—A Humanized Mab to IL-5rα with Enhanced Antibody-Dependent Cell-Mediated Cytotoxicity—A Novel Approach for the Treatment of Asthma. Expert Opin. Biol. Ther. 2012, 12, 113–118. [Google Scholar] [CrossRef]
- Lommatzsch, M.; Marchewski, H.; Schwefel, G.; Stoll, P.; Virchow, J.C.; Bratke, K. Benralizumab strongly reduces blood basophils in severe eosinophilic asthma. Clin. Exp. Allergy 2020, 50, 1267–1269. [Google Scholar] [CrossRef]
- Wenzel, S.E.; Ford, L.; Pearlman, D.; Spector, S.; Sher, L.; Skobieranda, F.; Wang, L.; Kirkesseli, S.; Rocklin, R.; Bock, B.; et al. Dupilumab in Persistent Asthma with Elevated Eosinophil Levels. N. Engl. J. Med. 2013, 368, 2455–2466. [Google Scholar] [CrossRef]
- Laporte, S.L.; Juo, Z.S.; Vaclavikova, J.; Colf, L.A.; Qi, X.; Heller, N.M.; Keegan, A.D.; Garcia, K.C. Molecular and Structural Basis of Cytokine Receptor Pleiotropy in the Interleukin-4/13 System. Cell 2008, 132, 259–272. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, N.A.; Bennett, B.L.; Graham, N.M.H.; Pirozzi, G.; Stahl, N.; Yancopoulos, G.D. Targeting key proximal drivers of type 2 inflammation in disease. Nat. Rev. Drug Discov. 2016, 15, 35–50. [Google Scholar] [CrossRef]
- Poulsen, L.K.; Hummelshoj, L. Triggers of IgE class switching and allergy development. Ann. Med. 2007, 39, 440–456. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.A. IL-13 effector functions. Annu. Rev. Immunol. 2003, 21, 425–456. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, H.F.; Phipps, S.; Foster, P.S. Eosinophil trafficking in allergy and asthma. J. Allergy Clin. Immunol. 2007, 119, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Le Floc’H, A.; Allinne, J.; Nagashima, K.; Scott, G.; Birchard, D.; Asrat, S.; Bai, Y.; Lim, W.K.; Martin, J.; Huang, T.; et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy 2020, 75, 1188–1204. [Google Scholar] [CrossRef] [PubMed]
- May, R.D.; Fung, M. Strategies targeting the IL-4/IL-13 axes in disease. Cytokine 2015, 75, 89–116. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2013, 43, 343–373. [Google Scholar] [CrossRef] [Green Version]
- Bousquet, J.J.; Brusselle, G.; Buhl, R.; Busse, W.W.; Cruz, A.A.; Djukanovic, R.; Domingo, C.; Hanania, N.A.; Humbert, M.; Gow, A.M.; et al. Care pathways for the selection of a biologic in severe asthma. Eur. Respir. J. 2017, 50, 1701782. [Google Scholar] [CrossRef] [Green Version]
- Boyman, O.; Kaegi, C.; Akdis, M.; Bavbek, S.; Bossios, A.; Chatzipetrou, A.; Eiwegger, T.; Firinu, D.; Harr, T.; Knol, E.F.; et al. EAACI IG Biologicals task force paper on the use of biologic agents in allergic disorders. Allergy 2015, 70, 727–754. [Google Scholar] [CrossRef] [Green Version]
- Kotisalmi, E.; Hakulinen, A.; Mäkelä, M.; Toppila-Salmi, S.; Kauppi, P. A Comparison of Biologicals in the Treatment of Adults with Severe Asthma—Real-Life Experiences. Asthma Res. Pract. 2020, 6, 1–11. [Google Scholar] [CrossRef]
- Normansell, R.; Walker, S.; Milan, S.J.; Walters, E.H.; Nair, P. Omalizumab for asthma in adults and children. Cochrane Database Syst. Rev. 2014, CD003559. [Google Scholar] [CrossRef]
- Humbert, M.; Taillé, C.; Mala, L.; Le Gros, V.; Just, J.; Molimard, M. Omalizumab effectiveness in patients with severe allergic asthma according to blood eosinophil count: The STELLAIR study. Eur. Respir. J. 2018, 51, 1702523. [Google Scholar] [CrossRef] [PubMed]
- Pavord, I.; Bleecker, E.R.; Buhl, R.; Chanez, P.; Bel, E.H.; Howarth, P.; Bratton, D.J.; Albers, F.C.; Yancey, S. Response to mepolizumab treatment is sustained across 4-weekly dosing periods. ERJ Open Res. 2020, 6, 00068–02020. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Zangrilli, J.; Wechsler, M.E.; Bateman, E.D.; Brusselle, G.; Bardin, P.; Murphy, K.; Maspero, J.F.; O’Brien, C.; Korn, S. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: Results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir. Med. 2015, 3, 355–366. [Google Scholar] [CrossRef]
- Bjermer, L.; Lemiere, C.; Maspero, J.; Weiss, S.; Zangrilli, J.; Germinaro, M. Reslizumab for Inadequately Controlled Asthma with Elevated Blood Eosinophil Levels: A Randomized Phase 3 Study. Chest 2016, 150, 789–798. [Google Scholar] [CrossRef] [Green Version]
- Bleecker, E.R.; Fitzgerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkström, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- Kavanagh, J.E.; Hearn, A.P.; Dhariwal, J.; D’Ancona, G.; Douiri, A.; Roxas, C.; Fernandes, M.; Green, L.; Thomson, L.; Nanzer, A.M.; et al. Real-World Effectiveness of Benralizumab in Severe Eosinophilic Asthma. Chest 2020. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef]
- Gevaert, P.; Calus, L.; Van Zele, T.; Blomme, K.; De Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; De Bacquer, D.; Van Cauwenberge, P.; et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e1. [Google Scholar] [CrossRef]
- Pinto, J.; Mehta, N.; DiTineo, M.; Wang, J.; Baroody, F.; Naclerio, R. A randomized, double-blind, placebo-controlled trial of anti-IgE for chronic rhinosinusitis. Rhinol. J. 2010, 48, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Forster-Ruhrmann, U.; Stergioudi, D.; Pierchalla, G.; Fluhr, J.; Bergmann, K.-C.; Olze, H. Omalizumab in patients with NSAIDs-exacerbated respiratory disease. Rhinology 2020, 58, 226–232. [Google Scholar] [CrossRef]
- Gevaert, P.; Omachi, T.A.; Corren, J.; Mullol, J.; Han, J.; Lee, S.E.; Kaufman, D.; Ligueros-Saylan, M.; Howard, M.; Zhu, R.; et al. Efficacy and safety of omalizumab in nasal polyposis: 2 randomized phase 3 trials. J. Allergy Clin. Immunol. 2020, 146, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Gevaert, P.; Lang-Loidolt, D.; Lackner, A.; Stammberger, H.; Staudinger, H.; Van Zele, T.; Holtappels, G.; Tavernier, J.; Van Cauwenberge, P.; Bachert, C. Nasal IL-5 levels determine the response to anti–IL-5 treatment in patients with nasal polyps. J. Allergy Clin. Immunol. 2006, 118, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Sousa, A.R.; Lund, V.J.; Scadding, G.; Gevaert, P.; Nasser, S.M.; Durham, S.R.; Cornet, M.E.; Kariyawasam, H.H.; Gilbert, J.; et al. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J. Allergy Clin. Immunol. 2017, 140, 1024–1031.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, P.; Van Bruaene, N.; Cattaert, T.; Van Steen, K.; Van Zele, T.; Acke, F.; De Ruyck, N.; Blomme, K.; Sousa, A.R.; Marshall, R.P.; et al. Mepolizumab, a humanized anti–IL-5 mAb, as a treatment option for severe nasal polyposis. J. Allergy Clin. Immunol. 2011, 128, 989–995.e8. [Google Scholar] [CrossRef] [Green Version]
- Chong, L.Y.; Piromchai, P.; Sharp, S.; Snidvongs, K.; Philpott, C.; Hopkins, C.; Burton, M.J. Biologics for chronic rhinosinusitis. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Hopkins, C.; Bachert, C.; Fokkens, W.; Desrosiers, M.; Wagenmann, M.; Lee, S.; Sousa, A.; Smith, S.; Martin, N.; Mayer, B.; et al. Late Breaking Abstract—Add-on mepolizumab for chronic rhinosinusitis with nasal polyps: SYNAPSE study. Eur. Respir. J. 2020, 56, 4616. [Google Scholar]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef] [Green Version]
- Akinlade, B.; Guttman-Yassky, E.; De Bruin-Weller, M.; Simpson, E.; Blauvelt, A.; Cork, M.; Prens, E.; Asbell, P.; Akpek, E.; Corren, J.; et al. Conjunctivitis in dupilumab clinical trials. Br. J. Dermatol. 2019, 181, 459–473. [Google Scholar] [CrossRef] [Green Version]
- Golebski, K.; Van Tongeren, J.; Van Egmond, D.; De Groot, E.J.; Fokkens, W.J.; Van Drunen, C.M. Specific Induction of TSLP by the Viral RNA Analogue Poly(I:C) in Primary Epithelial Cells Derived from Nasal Polyps. PLoS ONE 2016, 11, e0152808. [Google Scholar] [CrossRef]
- Gauvreau, G.M.; O’Byrne, P.M.; Boulet, L.-P.; Wang, Y.; Cockcroft, D.; Bigler, J.; Fitzgerald, J.M.; Boedigheimer, M.; Davis, B.E.; Dias, C.; et al. Effects of an Anti-TSLP Antibody on Allergen-Induced Asthmatic Responses. N. Engl. J. Med. 2014, 370, 2102–2110. [Google Scholar] [CrossRef]
- Catley, M.C.; Coote, J.; Bari, M.; Tomlinson, K.L. Monoclonal antibodies for the treatment of asthma. Pharmacol. Ther. 2011, 132, 333–351. [Google Scholar] [CrossRef] [PubMed]
- Baatjes, A.J.; Smith, S.G.; Dua, B.; Watson, R.; Gauvreau, G.M.; O’Byrne, P.M. Treatment with anti-OX40L or anti-TSLP does not alter the frequency of T regulatory cells in allergic asthmatics. Allergy 2015, 70, 1505–1508. [Google Scholar] [CrossRef] [PubMed]
- Corren, J.; Parnes, J.R.; Wang, L.; Mo, M.; Roseti, S.L.; Griffiths, J.M.; Van Der Merwe, R. Tezepelumab in Adults with Uncontrolled Asthma. N. Engl. J. Med. 2017, 377, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Michel, O.; Dinh, P.H.D.; Doyen, V.; Corazza, F. Anti-TNF inhibits the Airways neutrophilic inflammation induced by inhaled endotoxin in human. BMC Pharmacol. Toxicol. 2014, 15, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoniu, S.A.; Mihaltan, F.; Ulmeanu, R. Anti-TNF-α therapies in chronic obstructive pulmonary diseases. Expert Opin. Investig. Drugs 2008, 17, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Cazzola, M.; Polosa, R. Anti-TNF-α and Th1 cytokine-directed therapies for the treatment of asthma. Curr. Opin. Allergy Clin. Immunol. 2006, 6, 43–50. [Google Scholar] [CrossRef]
- Antoniu, S.A. Infliximab for chronic obstructive pulmonary disease: Towards a more specific inflammation targeting? Expert Opin. Investig. Drugs 2006, 15, 181–184. [Google Scholar] [CrossRef]
- Busse, W.W.; Holgate, S.; Kerwin, E.; Chon, Y.; Feng, J.; Lin, J.; Lin, S.-L. Randomized, Double-Blind, Placebo-controlled Study of Brodalumab, a Human Anti–IL-17 Receptor Monoclonal Antibody, in Moderate to Severe Asthma. Am. J. Respir. Crit. Care Med. 2013, 188, 1294–1302. [Google Scholar] [CrossRef]
- Nair, P.; Aziz-Ur-rehman, A.; Radford, K. Therapeutic implications of “neutrophilic asthma”. Curr. Opin. Pulm. Med. 2015, 21, 33–38. [Google Scholar] [CrossRef]
- Nair, P.; Gaga, M.; Zervas, E.; Alagha, K.; Hargreave, F.E.; O’Byrne, P.M.; Stryszak, P.; Gann, L.; Sadeh, J.; Chanez, P.; et al. Safety and efficacy of a CXCR2 antagonist in patients with severe asthma and sputum neutrophils: A randomized, placebo-controlled clinical trial. Clin. Exp. Allergy 2012, 42, 1097–1103. [Google Scholar] [CrossRef]
- O’Byrne, P.M.; Metev, H.; Puu, M.; Richter, K.; Keen, C.; Uddin, M.; Larsson, B.; Cullberg, M.; Nair, P. Efficacy and safety of a CXCR2 antagonist, AZD5069, in patients with uncontrolled persistent asthma: A randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2016, 4, 797–806. [Google Scholar] [CrossRef]
- Ricciotti, E.; Fitzgerald, G.A. Prostaglandins and Inflammation. Arter. Thromb. Vasc. Biol. 2011, 31, 986–1000. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin. Sci. 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mjösberg, J.; Trifari, S.; Crellin, N.K.; Peters, C.P.; Van Drunen, C.M.; Piet, B.; Fokkens, W.J.; Cupedo, T.; Spits, H. Human IL-25- and IL-33-responsive type 2 innate lymphoid cells are defined by expression of CRTH2 and CD161. Nat. Immunol. 2011, 12, 1055–1062. [Google Scholar] [CrossRef]
- Diamant, Z.; Aalders, W.; Parulekar, A.; Bjermer, L.; Hanania, N.A. Targeting lipid mediators in asthma: Time for reappraisal. Curr. Opin. Pulm. Med. 2019, 25, 121–127. [Google Scholar] [CrossRef]
- Roth-Walter, F.; Adcock, I.M.; Benito-Villalvilla, C.; Bianchini, R.; Bjermer, L.; Caramori, G.; Cari, L.; Chung, K.F.; Diamant, Z.; Eguiluz-Gracia, I.; et al. Comparing biologicals and small molecule drug therapies for chronic respiratory diseases: An EAACI Taskforce on Immunopharmacology position paper. Allergy 2019, 74, 432–448. [Google Scholar] [CrossRef]
- Ratner, P.; Andrews, C.P.; Hampel, F.C.; Martin, B.; Mohar, D.E.; Bourrelly, D.; Danaietash, P.; Mangialaio, S.; Dingemanse, J.; Hmissi, A.; et al. Efficacy and safety of setipiprant in seasonal allergic rhinitis: Results from Phase 2 and Phase 3 randomized, double-blind, placebo- and active-referenced studies. Allergy, Asthma Clin. Immunol. 2017, 13, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Diamant, Z.; Sidharta, P.N.; Singh, D.; O’Connor, B.J.; Zuiker, R.; Leaker, B.R.; Silkey, M.; Dingemanse, J. Setipiprant, a selective CRTH2 antagonist, reduces allergen-induced airway responses in allergic asthmatics. Clin. Exp. Allergy 2014, 44, 1044–1052. [Google Scholar] [CrossRef]
- Singh, D.; Cadden, P.; Hunter, M.; Collins, L.P.; Perkins, M.; Pettipher, R.; Townsend, E.; Vinall, S.; O’Connor, B. Inhibition of the asthmatic allergen challenge response by the CRTH2 antagonist OC000459. Eur. Respir. J. 2012, 41, 46–52. [Google Scholar] [CrossRef]
- Barnes, N.; Pavord, I.; Chuchalin, A.; Bell, J.; Hunter, M.; Lewis, T.; Parker, D.; Payton, M.; Collins, L.P.; Pettipher, R.; et al. A randomized, double-blind, placebo-controlled study of the CRTH2 antagonist OC000459 in moderate persistent asthma. Clin. Exp. Allergy 2012, 42, 38–48. [Google Scholar] [CrossRef]
- Hall, I.P.; Fowler, A.V.; Gupta, A.; Tetzlaff, K.; Nivens, M.C.; Sarno, M.; Finnigan, H.A.; Bateman, E.D.; Sutherland, E.R. Efficacy of BI 671800, an oral CRTH2 antagonist, in poorly controlled asthma as sole controller and in the presence of inhaled corticosteroid treatment. Pulm. Pharmacol. Ther. 2015, 32, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Erpenbeck, V.J.; Popov, T.A.; Miller, D.; Weinstein, S.F.; Spector, S.; Magnusson, B.; Osuntokun, W.; Goldsmith, P.; Weiss, H.M.; Beier, J. The oral CRTh2 antagonist QAW039 (fevipiprant): A phase II study in uncontrolled allergic asthma. Pulm. Pharmacol. Ther. 2016, 39, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Bateman, E.D.; Guerreros, A.G.; Brockhaus, F.; Holzhauer, B.; Pethe, A.; Kay, R.A.; Townley, R.G. Fevipiprant, an oral prostaglandin DP2receptor (CRTh2) antagonist, in allergic asthma uncontrolled on low-dose inhaled corticosteroids. Eur. Respir. J. 2017, 50, 1700670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, W.W.; Wenzel, S.E.; Meltzer, E.O.; Kerwin, E.M.; Liu, M.C.; Zhang, N.; Chon, Y.; Budelsky, A.L.; Lin, J.; Lin, S.-L. Safety and efficacy of the prostaglandin D2 receptor antagonist AMG 853 in asthmatic patients. J. Allergy Clin. Immunol. 2013, 131, 339–345. [Google Scholar] [CrossRef]
- Brightling, C.; Gaga, M.; Inoue, H.; Li, J.; Maspero, J.; Wenzel, S.; Maitra, S.; Lawrence, D.; Brockhaus, F.; Lehmann, T.; et al. Effectiveness of fevipiprant in reducing exacerbations in patients with severe asthma (LUSTER-1 and LUSTER-2): Two phase 3 randomised controlled trials. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Therapy (Target) | Asthma | CRSwNP | Dose | Response |
|---|---|---|---|---|
| Omalizumab (anti-IgE) | Severe allergic asthma with perennial allergy | Approved as add-on therapy for adults with severe CRSwNP by EMA in August 2020 | According to weight and total S-IgE value, every 2–4 weeks s.c. | Asthma: Reduction in exacerbations, improvement in symptoms, asthma related QoL↑, FEV1↑ |
| Pending FDA approval [41] | CRSwNP: Reduction in symptom score and nasal polyp score | |||
| Mepolizumab (anti-IL5) | Severe eosinophilic asthma with B-eos>300cells/ul | Ongoing studies for use in CRSwNP [41] | 100 or 300 mg s.c. every four weeks | Asthma: Reduction in exacerbations, improvement in symptoms, B-eos ↓, asthma related QoL↑, FEV1↑ |
| Reslizumab (anti-IL5) | Severe eosinophilic asthma with B-eos>400cells/ul | Ongoing studies | According to weight every four weeks i.v. | Asthma: Reduction in exacerbations, improvement in symptoms, B-eos↓, Asthma related QoL↑, FEV1↑ |
| Benralizumab (anti-IL5R) | Severe eosinophilic asthma with B-eos>300cells/ul | Ongoing studies for use in CRSwNP [41] | 30 mg every 4 weeks s.c. three times and then 30 mg every 8 weeks s.c. | Asthma: Reduction in exacerbations, improvement in symptoms, B-eos↓ |
| Dupilumab (anti-IL4Ralpha) | Severe eosinophilic asthma with B-eos>300cells/ul | Severe CRSwNP (approved by EMA and FDA) | First dose of 400 mg/600 mg s.c. according to weight, then 200 mg/300 mg every 2 weeks s.c. | Asthma: Reduction in exacerbations, improvement in symptoms, B-eos ↓, Asthma related QoL↑, FEV1↑ |
| CRSwNP: polyp size reduction, reduction in OCS and surgeries, improvement in symptom score |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lyly, A.; Laulajainen-Hongisto, A.; Gevaert, P.; Kauppi, P.; Toppila-Salmi, S. Monoclonal Antibodies and Airway Diseases. Int. J. Mol. Sci. 2020, 21, 9477. https://doi.org/10.3390/ijms21249477
Lyly A, Laulajainen-Hongisto A, Gevaert P, Kauppi P, Toppila-Salmi S. Monoclonal Antibodies and Airway Diseases. International Journal of Molecular Sciences. 2020; 21(24):9477. https://doi.org/10.3390/ijms21249477
Chicago/Turabian StyleLyly, Annina, Anu Laulajainen-Hongisto, Philippe Gevaert, Paula Kauppi, and Sanna Toppila-Salmi. 2020. "Monoclonal Antibodies and Airway Diseases" International Journal of Molecular Sciences 21, no. 24: 9477. https://doi.org/10.3390/ijms21249477
APA StyleLyly, A., Laulajainen-Hongisto, A., Gevaert, P., Kauppi, P., & Toppila-Salmi, S. (2020). Monoclonal Antibodies and Airway Diseases. International Journal of Molecular Sciences, 21(24), 9477. https://doi.org/10.3390/ijms21249477