Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Measure of Success According to POSEIDON Concept
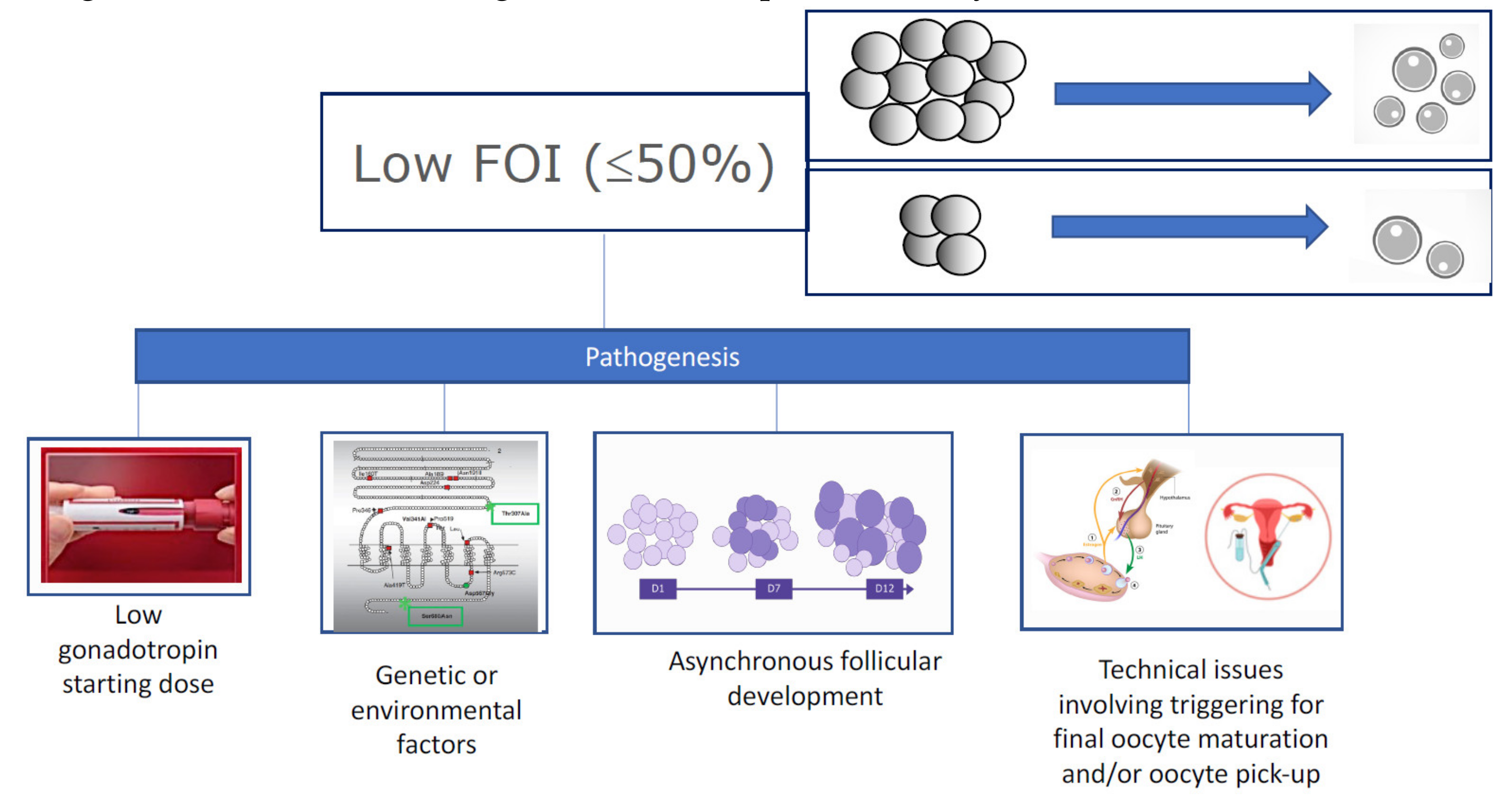
2.1. Follicle-to-Oocyte Index (FOI)
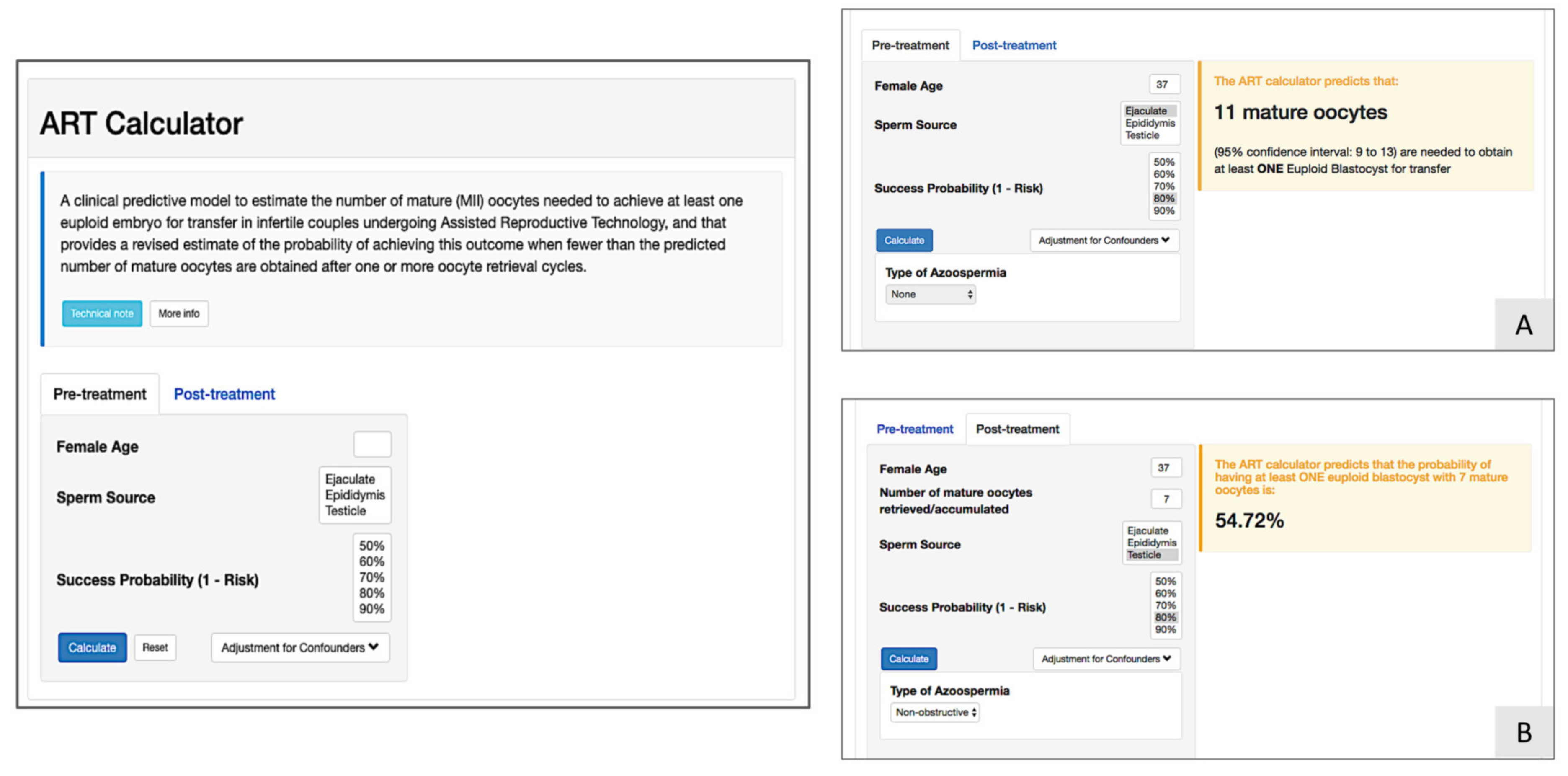
2.2. The ART Calculator
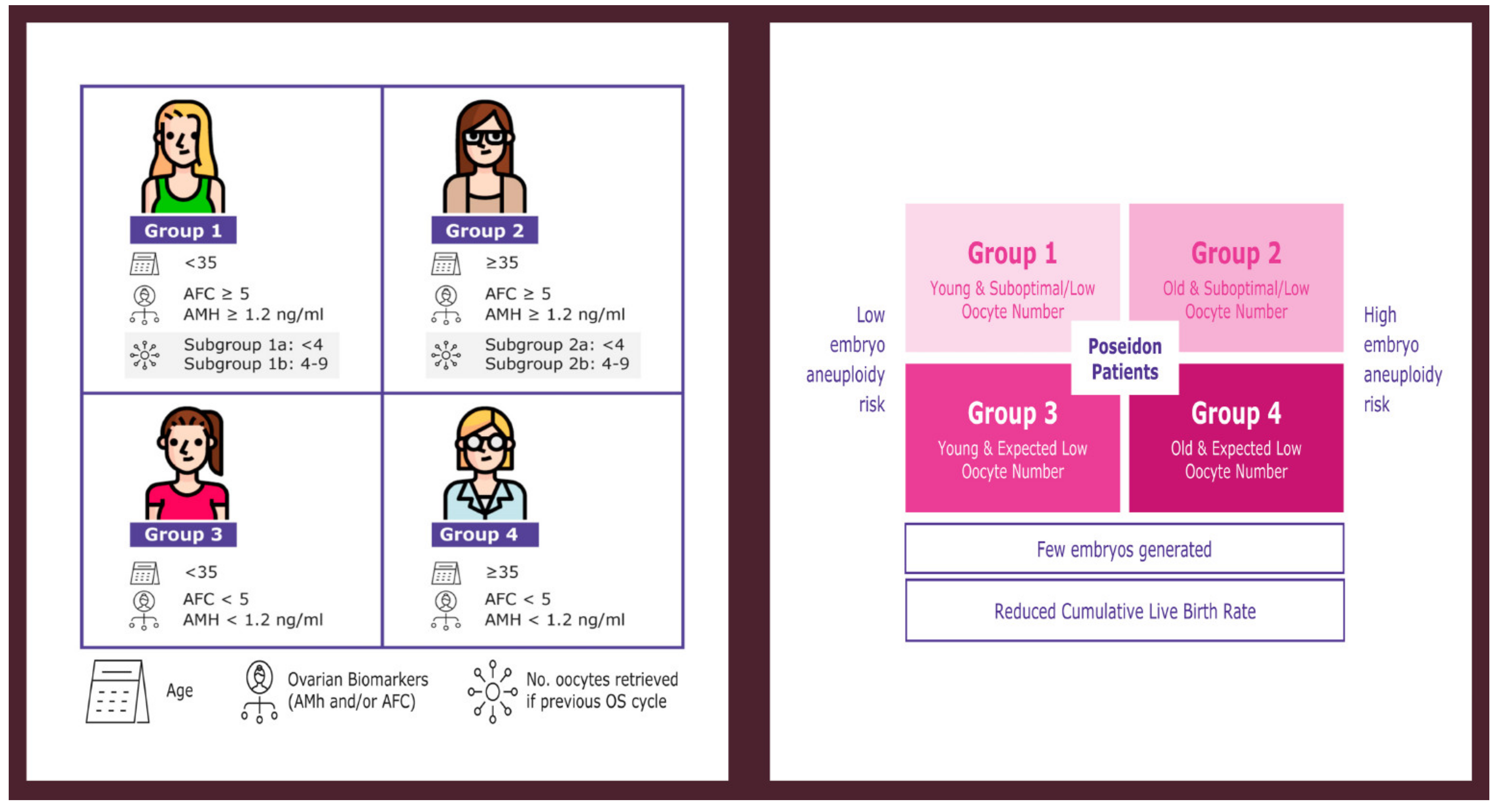
3. POSEIDON Groups 1 and 2
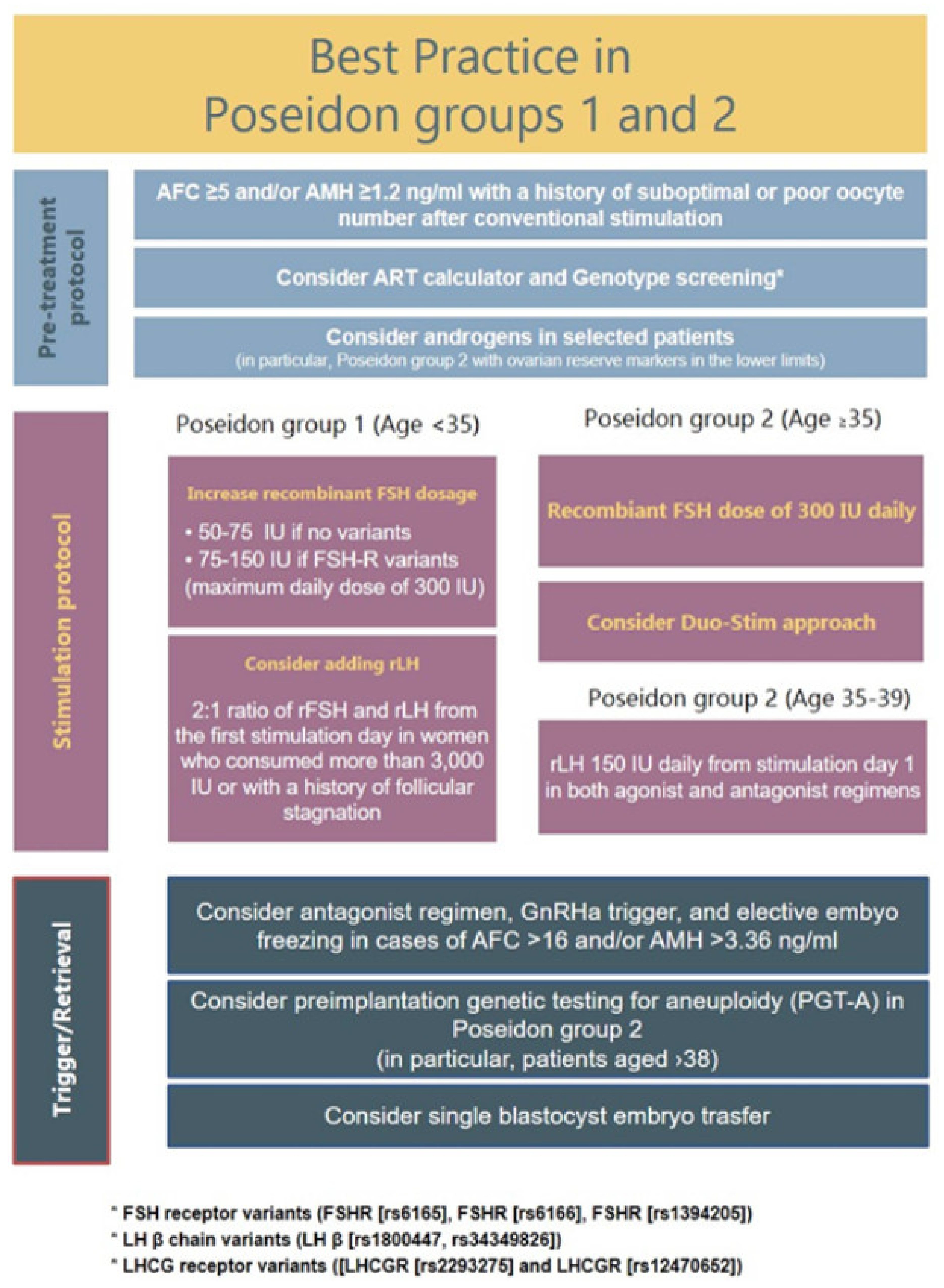
3.1. Clinical Management of POSEIDON Groups 1 and 2 Patients
3.2. Use of rFSH
3.3. FSH Dose Increase
3.4. rLH Supplementation
3.5. Dehydroepiandrosterone Supplementation
3.6. Double Stimulation
3.7. Conclusions: Clinical Management POSEIDON Groups 1 and 2
3.8. Future Research
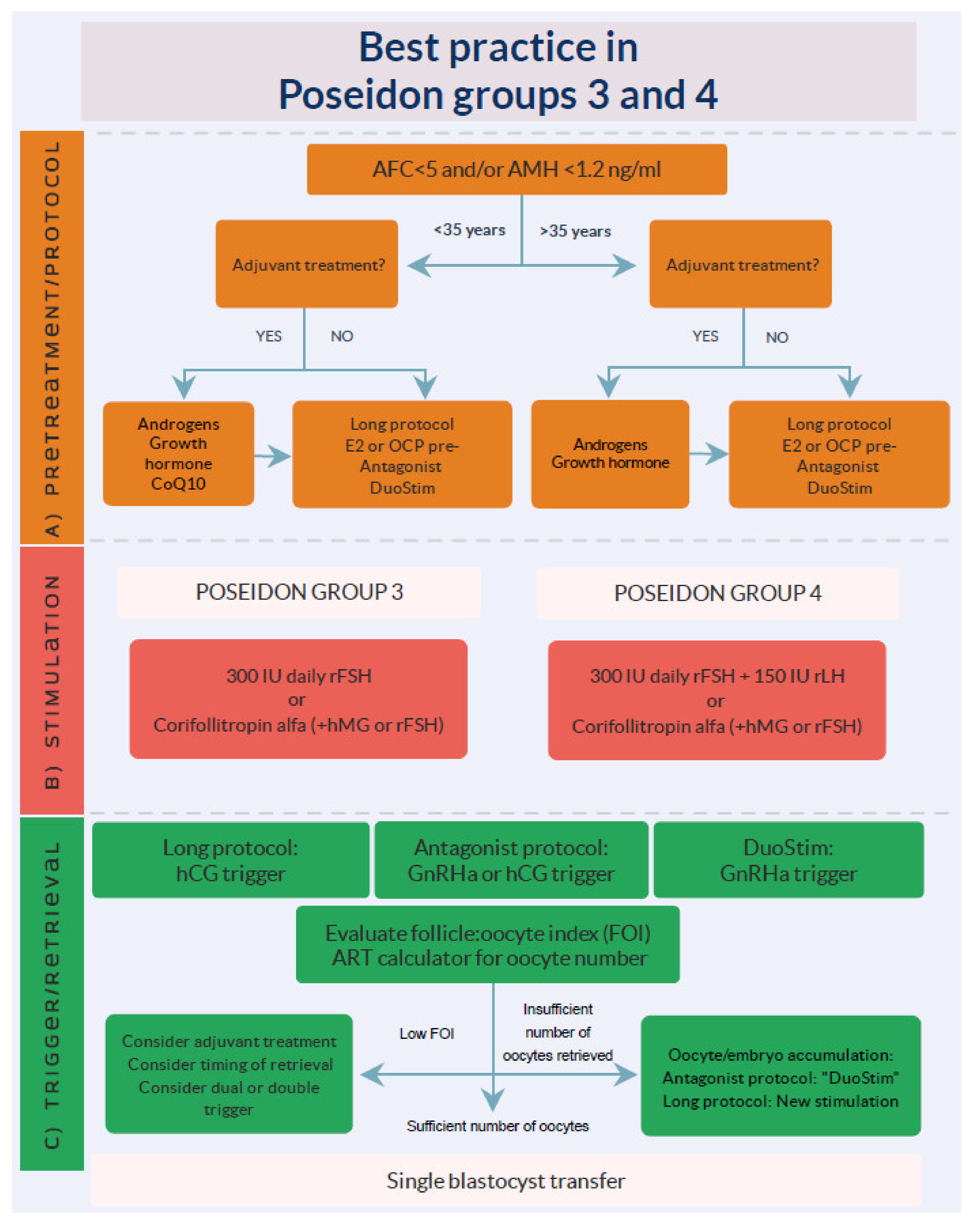
4. POSEIDON Groups 3 and 4
4.1. Stimulation Protocols
4.2. Ovulation Trigger
4.3. Adjuvants
4.3.1. Androgens
4.3.2. Growth Hormone
4.3.3. Coenzyme Q 10
4.4. Conclusions: Clinical Management POSEIDON Groups 3 and 4
4.5. Future Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sunkara, S.K.; Rittenberg, V.; Raine-Fenning, N.; Bhattacharya, S.; Zamora, J.; Coomarasamy, A. Association between the number of eggs and live birth in IVF treatment: An analysis of 400 135 treatment cycles. Hum. Reprod. Oxf. Engl. 2011, 26, 1768–1774. [Google Scholar] [CrossRef] [Green Version]
- Drakopoulos, P.; Blockeel, C.; Stoop, D.; Camus, M.; de Vos, M.; Tournaye, H.; Polyzos, N.P. Conventional ovarian stimulation and single embryo transfer for IVF/ICSI. How many oocytes do we need to maximize cumulative live birth rates after utilization of all fresh and frozen embryos? Hum. Reprod. 2016, 31, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Patrizio, P.; Vaiarelli, A.; Setti, L.; Tobler, K.J.; Shoham, G.; Leong, M.; Shoha, Z. How to define, diagnose and treat poor responders? Responses from a worldwide survey of IVF clinics. Reprod. Biomed. Online 2015, 30, 581–592. [Google Scholar] [CrossRef] [Green Version]
- Oudendijk, J.F.; Yarde, F.; Eijkemans, M.J.; Broekmans, F.J.; Broer, S.L. The poor responder in IVF: Is the prognosis always poor?: A systematic review. Hum. Reprod. Update 2012, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, N.P.; Devroey, P. A systematic review of randomized trials for the treatment of poor ovarian responders: Is there any light at the end of the tunnel? Fertil. Steril. 2011, 96, 1058.e7–1061.e7. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.J.M.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE consensus on the definition of “poor response” to ovarian stimulation for in vitro fertilization: The bologna criteria. Hum. Reprod. Oxf. Engl. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [Green Version]
- Younis, J.S.; Ben-Ami, M.; Ben-Shlomo, I. The bologna criteria for poor ovarian response: A contemporary critical appraisal. J. Ovarian Res. 2015, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- Bozdag, G.; Polat, M.; Yarali, I.; Yarali, H. Live birth rates in various subgroups of poor ovarian responders fulfilling the bologna criteria. Reprod. Biomed. Online 2017, 34, 639–644. [Google Scholar] [CrossRef] [Green Version]
- Alviggi, C.; Andersen, C.Y.; Buehler, K.; Conforti, A.; De Placido, G.; Esteves, S.C.; Fischer, R.; Galliano, D.; Polysoz, N.P.; Sunkara, S.K.; et al. A new more detailed stratification of low responders to ovarian stimulation: From a poor ovarian response to a low prognosis concept. Fertil. Steril. 2016, 105, 1452. [Google Scholar] [CrossRef] [Green Version]
- Conforti, A.; Esteves, S.C.; Picarelli, S.; Iorio, G.; Rania, E.; Zullo, F.; De Placido, G.; Alviggi, C. Novel approaches for diagnosis and management of low prognosis patients in assisted reproductive technology: The POSEIDON concept. Panminerva Med. 2019, 61, 24–29. [Google Scholar] [CrossRef]
- ACOG. Committee opinion no 671: Perinatal risks associated with assisted reproductive technology. Obs. Gynecol. 2016, 128, e61–e68. [Google Scholar] [CrossRef]
- Practice Committee of Society for Assisted Reproductive Technology; Practice Committee of American Society for Reproductive Medicine. Elective single-embryo transfer. Fertil. Steril. 2012, 97, 835–842. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; Carbone, I.F.; Borrelli, R.; de Placido, G.; Guerriero, S. Influence of cryopreservation on perinatal outcome after blastocystvs cleavage-stage embryo transfer: Systematic review and meta-analysis. Ultrasound Obs. Gynecol. 2018, 51, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Humaidan, P.; Alviggi, C.; Fischer, R.; Esteves, S.C. The novel POSEIDON stratification of “Low prognosis patients in Assisted Reproductive Technology” and its proposed marker of successful outcome. F1000Res 2016, 5, 2911. [Google Scholar] [CrossRef] [Green Version]
- Forman, E.J.; Hong, K.H.; Ferry, K.M.; Tao, X.; Taylor, D.; Levy, B.; Treff, N.R.; Scott Jr, R.T. In vitro fertilization with single euploid blastocyst transfer: A randomized controlled trial. Fertil. Steril. 2013, 100. [Google Scholar] [CrossRef] [Green Version]
- Ata, B.; Kaplan, B.; Danzer, H.; Glassner, M.; Opsahl, M.; Tan, S.L.; Munne, S. Array CGH analysis shows that aneuploidy is not related to the number of embryos generated. Reprod. Biomed. Online 2012, 24, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Esteves, S.C.; Carvalho, J.F.; Martinhago, C.D.; Melo, A.A.; Bento, F.C.; Humaidan, P.; Alviggi, C. Estimation of age-dependent decrease in blastocyst euploidy by next generation sequencing: Development of a novel prediction model. Panminerva Med. 2018, 61, 3–10. [Google Scholar] [CrossRef] [Green Version]
- La Marca, A.; Sunkara, S.K. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: From theory to practice. Hum. Reprod. Update 2014, 20, 124–140. [Google Scholar] [CrossRef] [Green Version]
- Alviggi, C.; Conforti, A.; Esteves, S.C.; Vallone, R.; Venturella, R.; Staiano, S.; Castaldo, E.; Andersen, C.Y.; De Placido, G. Understanding ovarian hypo-response to exogenous gonadotropin in ovarian stimulation and its new proposed marker—the follicle-To-Oocyte. (FOI) index. Front. Endocrinol. 2018, 9, 589. [Google Scholar] [CrossRef]
- Dosouto, C.; Haahr, T.; Humaidan, P. Advances in ovulation trigger strategies. Panminerva Med. 2019, 61, 42–51. [Google Scholar] [CrossRef]
- Haahr, T.; Dosouto, C.; Alviggi, C.; Esteves, S.C.; Humaidan, P. Management strategies for POSEIDON groups 3 and 4. Front. Endocrinol. (Lausanne) 2019, 10, 614. [Google Scholar] [CrossRef]
- Esteves, S.C.; Carvalho, J.F.; Bento, F.C.; Santos, J. A Novel Predictive Model to Estimate the Number of Mature Oocytes Required for Obtaining at Least One Euploid Blastocyst for Transfer in Couples Undergoing in vitro Fertilization/Intracytoplasmic Sperm Injection: The ART Calculator. Front. Endocrinol. 2019, 10, 99. [Google Scholar] [CrossRef] [Green Version]
- Alviggi, C.; Pettersson, K.; Longobardi, S.; Andersen, C.Y.; Conforti, A.; De Rosa, P.; Clarizia, R.; Strina, I.; Mollo, A.; De Placido, G.; et al. A common polymorphic allele of the LH beta-subunit gene is associated with higher exogenous FSH consumption during controlled ovarian stimulation for assisted reproductive technology. Reprod. Biol. Endocrinol. 2013, 11, 51. [Google Scholar] [CrossRef] [Green Version]
- Conforti, A.; Alfano, S.; De Rosa, P.; Alviggi, C.; De Placido, G. The role of gonadotropin polymorphisms and their receptors in assisted reproductive technologies and controlled ovarian stimulation: A prospective observational study. Ital. J. Gynaecol. Obs. 2017, 29, 15–21. [Google Scholar] [CrossRef]
- La Marca, A.; Papaleo, E.; Alviggi, C.; Ruvolo, G.; De Placido, G.; Candiani, M.; Cittadini, E.; De Michele, F.; Moriondo, V.; Catellani, V.; et al. The combination of genetic variants of the FSHB and FSHR genes affects serum FSH in women of reproductive age. Hum. Reprod. 2013, 28, 1369–1374. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; Esteves, S.C. Impact of mutations and polymorphisms of gonadotrophins and their receptors on the outcome of controlled ovarian stimulation. In Principles and Practice of Controlled Ovarian Stimulation in ART; Ghumman, S., Ed.; Springer: New Delhi, India, 2015; pp. 147–156. [Google Scholar]
- Alviggi, C.; Clarizia, R.; Pettersson, K.; Mollo, A.; Humaidan, P.; Strina, I.; Coppola, M.; Ranieri, A.; D’Uva, M.; De Placido, G. Suboptimal response to GnRHa long protocol is associated with a common LH polymorphism. Reprod. Biomed. Online 2011, 22 (Suppl. 1), S67–S72. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; Santi, D.; Esteves, S.C.; Andersen, C.Y.; Humaidan, P.; Chiodini, P.; De Placido, G.; Simoni, M. Clinical relevance of genetic variants of gonadotrophins and their receptors in controlled ovarian stimulation: A systematic review and meta-analysis. Hum. Reprod. Update 2018, 24, 1–16. [Google Scholar] [CrossRef]
- Alviggi, C.; Guadagni, R.; Conforti, A.; Coppola, G.; Picarelli, S.; De Rosa, P.; Vallone, R.; Strina, I.; Pagano, T.; Mollo, A.; et al. Association between intrafollicular concentration of benzene and outcome of controlled ovarian stimulation in IVF/ICSI cycles: A pilot study. J. Ovar. Res. 2014, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Mahalingaiah, S.; Missmer, S.A.; Maity, A.; Williams, P.L.; Meeker, J.D.; Berry, K.; Ehrich, S.; Perry, M.J.; Cramer, D.W.; Hauser, R. Association of hexachlorobenzene. (HCB), dichlorodiphenyltrichloroethane. (DDT), dichlorodiphenyldichloroethylene. (DDE) with in vitro fertilization. (IVF) outcomes. Environ. Health Perspect 2012, 120, 316–320. [Google Scholar] [CrossRef] [Green Version]
- Conforti, A.; Mascia, M.; Cioffi, G.; De Angelis, C.; Coppola, G.; De Rosa, P.; Pivonello, R.; Alviggi, C.; De Placido, G. Air pollution and female fertility: A systematic review of literature. Reprod. Biol. Endocrinol. 2018, 16, 117. [Google Scholar] [CrossRef]
- Bloom, M.S.; Fujimoto, V.Y.; Storm, R.; Zhang, L.; Butts, C.D.; Sollohub, D.; Jansing, R.L. Persistent organic pollutants (POPs) in human follicular fluid and in vitro fertilization outcomes, a pilot study. Reprod. Toxicol. 2017, 67, 165–173. [Google Scholar] [CrossRef]
- Agarwal, A.; Gupta, S.; Sharma, R. Oxidative stress and its implications in female infertility—A clinician’s perspective. Reprod. Biomed. Online 2005, 11, 641–650. [Google Scholar] [CrossRef]
- Velthut, A.; Zilmer, M.; Zilmer, K.; Kaart, T.; Karro, H.; Salumets, A. Elevated blood plasma antioxidant status is favourable for achieving IVF/ICSI pregnancy. Reprod. Biomed. Online 2013, 26, 345–352. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Saleh, R.A.; Bedaiwy, M.A. Role of reactive oxygen species in the pathophysiology of human reproduction. Fertil. Steril. 2003, 79, 829–843. [Google Scholar] [CrossRef] [Green Version]
- Showell, M.G.; Mackenzie-Proctor, R.; Jordan, V.; Hart, R.J. Antioxidants for female subfertility. Cochrane Database Syst. Rev. 2017, 7, Cd007807. [Google Scholar] [CrossRef]
- Devroey, P.; Pellicer, A.; Nyboe Andersen, A.; Arce, J.C. A randomized assessorblind trial comparing highly purified hMG and recombinant FSH in a GnRH antagonist cycle with compulsory single-blastocyst transfer. Fertil. Steril. 2012, 97, 561–571. [Google Scholar] [CrossRef]
- Lehert, P.; Schertz, J.C.; Ezcurra, D. Recombinant human follicle-stimulating hormone produces more oocytes with a lower total dose per cycle in assisted reproductive technologies compared with highly purified human menopausal gonadotrophin: A meta-analysis. Reprod. Biol. Endocrinol. 2010, 8, 112. [Google Scholar] [CrossRef] [Green Version]
- Hompes, P.G.; Broekmans, F.J.; Hoozemans, D.A.; Schats, R. Effectiveness of highly purified human menopausal gonadotropin vs. recombinant follicle-stimulating hormone in first-cycle in vitro fertilizationintracytoplasmic sperm injection patients. Fertil. Steril. 2008, 89, 1685–1693. [Google Scholar] [CrossRef]
- Platteau, P.; Andersen, A.N.; Balen, A.; Devroey, P.; Sorensen, P.; Helmgaard, L.; Arce, J.C. Similar ovulation rates, but different follicular development with highly purified menotrophin compared with recombinant FSH in WHO Group II anovulatory infertility: A randomized controlled study. Hum. Reprod. 2006, 21, 1798–804. [Google Scholar] [CrossRef] [Green Version]
- Drakopoulos, P.; Santos-Ribeiro, S.; Bosch, E.; Garcia-Velasco, J.; Blockeel, C.; Romito, A.; Tournaye, H.; Polyzos, N.P. The Effect of Dose Adjustments in a Subsequent Cycle of Women With Suboptimal Response Following Conventional Ovarian Stimulation. Front. Endocrinol. 2018, 9, 361. [Google Scholar] [CrossRef] [Green Version]
- Behre, H.M.; Greb, R.R.; Mempel, A.; Sonntag, B.; Kiesel, L.; Kaltwasser, P.; Seliger, E.; Ropke, F.; Gromoll, J.; Nieschlag, E.; et al. Significance of a common single nucleotide polymorphism in exon 10 of the follicle-stimulating hormone (FSH) receptor gene for the ovarian response to FSH: A pharmacogenetic approach to controlled ovarian hyperstimulation. Pharm. Genom. 2005, 15, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Lisi, F.; Rinaldi, L.; Fishel, S.; Lisi, R.; Pepe, G.P.; Picconeri, M.G.; Campbell, A. Use of recombinant LHin a group of unselected IVF patients. Reprod. Biomed. Online 2002, 5, 104–108. [Google Scholar] [CrossRef]
- Ferraretti, A.P.; Gianaroli, L.; Magli, M.C.; D’Angelo, A.; Farfalli, V.; Montanaro, N. Exogenous luteinizing hormone in controlled ovarian hyperstimulation for assisted reproduction techniques. Fertil. Steril. 2004, 82, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- De Placido, G.; Alviggi, C.; Perino, A.; Strina, I.; Lisi, F.; Fasolino, A.; De Palo, R.; Ranieri, A.; Colacurci, N.; Mollo, A. Recombinant human LH supplementation versus recombinant human FSH (rFSH) step-up protocol during controlled ovarian stimulation in normogonadotrophic women with initial inadequate ovarian response to rFSH. A multicentre, prospective, randomized controlled trial. Hum. Reprod. 2005, 20, 390–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruvolo, G.; Bosco, L.; Pane, A.; Morici, G.; Cittadini, E.; Roccheri, M.C. Lower apoptosis rate in human cumulus cells after administration of recombinant luteinizing hormone to women undergoing ovarian stimulation for in vitro fertilization procedures. Fertil. Steril. 2007, 87, 542–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alviggi, C.; Conforti, A.; Esteves, S.C.; Andersen, C.Y.; Bosch, E.; Buhler, K.; Ferraretti, A.P.; De Placido, G.; Mollo, A.; Fischer, R.; et al. Recombinant luteinizing hormone supplementation in assisted reproductive technology: A systematic review. Fertil. Steril. 2018, 109, 644–664. [Google Scholar] [CrossRef] [Green Version]
- Alviggi, C.; Mollo, A.; Clarizia, R.; De Placido, G. Exploiting LH in ovarian stimulation. Reprod. Biomed. Online 2006, 12, 221–233. [Google Scholar] [CrossRef]
- Yilmaz, F.Y.; Görkemli, H.; Çolakoglu, M.C.; Aktan, M.; Gezginç, K. The evaluation of recombinant LH supplementation in patients with suboptimal response to recombinant FSH undergoing IVF treatment with GnRH agonist down-regulation. Gynecol. Endocrinol. 2015, 31, 141–144. [Google Scholar] [CrossRef]
- De Placido, G.; Alviggi, C.; Mollo, A.; Strina, I.; Ranieri, A.; Alviggi, E.; Wilding, M.; Varricchio, M.T.; Borrelli, A.L.; Conforti, S. Effects of recombinant LH (rLH) supplementation during controlled ovarian hyperstimulation (COH) in normogonadotrophic women with an initial inadequate response to recombinant FSH (rFSH) after pituitary downregulation. Clin. Endocrinol. 2004, 60, 637–643. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; Fabozzi, F.; De Placido, G. Ovarian stimulation for IVF/ICSI cycles: A pharmacogenomic approach. Med. Therap. Med. Reprod. Gynecol. Endocrinol. 2009, 11, 271–277. [Google Scholar] [CrossRef]
- Conforti, A.; Esteves, S.C.; Di Rella, F.; Strina, I.; De Rosa, P.; Fiorenza, A.; Zullo, F.; De Placido, G.; Alviggi, C. The role of recombinant LH in women with hypo-response to controlled ovarian stimulation: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2019, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagels, H.E.; Rishworth, J.R.; Siristatidis, C.S.; Kroon, B. Androgens (dehydroepiandrosterone or testosterone) for women undergoing assisted reproduction. Cochrane Database Syst. Rev. 2015, 26, Cd009749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, S.L.; Bell, R.; Donath, S.; Montalto, J.G.; Davis, S.R. Androgen levels in adult females: Changes with age, menopause, and oophorectomy. J. Clin. Endocrinol. Metab. 2005, 90, 3847–3853. [Google Scholar] [CrossRef] [PubMed]
- Tartagni, M.; Cicinelli, M.V.; Baldini, D.; Tartagni, M.V.; Alrasheed, H.; DeSalvia, M.A.; Loverro, G.; Montagnani, M. Dehydroepiandrosterone decreases the age-related decline of the in vitro fertilization outcome in women younger than 40 years old. Reprod. Biol. Endocrinol. 2015, 13, 18. [Google Scholar] [CrossRef] [Green Version]
- Moawad, A.; Shaeer, M. Long-term androgen priming by use of dehydroepiandrosterone (DHEA) improves IVF outcome in poor-responder patients. A randomized controlled study. Middle East. Fertil. Soc. J. 2012, 17, 268–274. [Google Scholar] [CrossRef]
- Vaiarelli, A.; Cimadomo, D.; Trabucco, E.; Vallefuoco, R.; Buffo, L.; Dusi, L.; Fiorini, F.; Barnocchi, N.; Bulletti, F.M.; Rienzi, L.; et al. Double stimulation in the same ovarian cycle (DuoStim) to maximize the number of oocytes retrieved from poor prognosis patients: A multicenter experience and SWOT analysis. Front. Endocrinol. 2018, 9, 317. [Google Scholar] [CrossRef] [Green Version]
- Alsbjerg, B.; Haahr, T.; Elbaek, H.O.; Laursen, R.; Povlsen, B.B.; Humaidan, P. Dual stimulation using corifollitropin alfa in 54 Bologna criteria poor ovarian responders - a case series. Reprod. Biomed. Online 2019, 38, 677–682. [Google Scholar] [CrossRef]
- Kim, C.H.; Kim, S.R.; Cheon, Y.P.; Kim, S.H.; Chae, H.D.; Kang, B.M. Minimal stimulation using gonadotropin-releasing hormone (GnRH) antagonist and recombinant human follicle-stimulating hormone versus GnRH antagonist multiple-dose protocol in low responders undergoing in vitro fertilization/intracytoplasmic sperm injection. Fertil. Steril. 2009, 92. [Google Scholar] [CrossRef]
- Morgia, F.; Sbracia, M.; Schimberni, M.; Giallonardo, A.; Piscitelli, C.; Giannini, P.; Giannini, P.; Aragona, C. A controlled trial of natural cycle versus microdose gonadotropin-releasing hormone analog flare cycles in poor responders undergoing in vitro fertilization. Fertil. Steril. 2004, 81, 1542–1547. [Google Scholar] [CrossRef]
- Barash, O.O.; Hinckley, M.D.; Rosenbluth, E.M.; Ivani, K.A.; Weckstein, L.N. High gonadotropin dosage does not affect euploidy and pregnancy rates in IVF PGS cycles with single embryo transfer. Hum. Reprod. 2017, 32, 2209–2217. [Google Scholar] [CrossRef] [Green Version]
- Labarta, E.; Bosch, E.; Alamá, P.; Rubio, C.; Rodrigo, L.; Pellicer, A. Moderate ovarian stimulation does not increase the incidence of human embryo chromosomal abnormalities in in vitro fertilization cycles. J. Clin. Endocrinol. Metab. 2012, 97, E1987–E1994. [Google Scholar] [CrossRef] [Green Version]
- Sekhon, L.; Shaia, K.; Santistevan, A.; Cohn, K.H.; Lee, J.A.; Beim, P.Y.; Copperman, A.B. The cumulative dose of gonadotropins used for controlled ovarian stimulation does not influence the odds of embryonic aneuploidy in patients with normal ovarian response. J. Assist. Reprod. Genet. 2017, 34, 749–758. [Google Scholar] [CrossRef]
- Wu, Q.; Li, H.; Zhu, Y.; Jiang, W.; Lu, J.; Wei, D.; Yan, J.; Chen, Z.J. Dosage of exogenous gonadotropins is not associated with blastocyst aneuploidy or live-birth rates in PGS cycles in Chinese women. Hum. Reprod. 2018, 33, 1875–1882. [Google Scholar] [CrossRef] [Green Version]
- Polyzos, N.P.; Blockeel, C.; Verpoest, W.; De Vos, M.; Stoop, D.; Vloeberghs, V.; Camus, M.; Devroey, P.; Tournaye, H. Live birth rates following natural cycle IVF in women with poor ovarian response according to the Bologna criteria. Hum. Reprod. 2012, 27, 3481–3486. [Google Scholar] [CrossRef] [Green Version]
- Kedem, A.; Tsur, A.; Haas, J.; Yerushalmi, G.M.; Hourvitz, A.; Machtinger, R.; Orvieto, R. Is the modified natural in vitro fertilization cycle justified in patients with “genuine” poor response to controlled ovarian hyperstimulation? Fertil. Steril. 2014, 101, 1624–1628. [Google Scholar] [CrossRef]
- Humaidan, P.; Chin, W.; Rogoff, D.; D’Hooghe, T.; Longobardi, S.; Hubbard, J.; Schertz, J. Efficacy and safety of follitropin alfa/lutropin alfa in ART: A randomized controlled trial in poor ovarian responders. Hum. Reprod. 2017, 32, 544–55. [Google Scholar] [CrossRef]
- Sunkara, S.K.; Coomarasamy, A.; Faris, R.; Braude, P.; Khalaf, Y. Long gonadotropin-releasing hormone agonist versus short agonist versus antagonist regimens in poor responders undergoing in vitro fertilization: A randomized controlled trial. Fertil. Steril. 2014, 101, 147–153. [Google Scholar] [CrossRef]
- De Geyter, C.; Fehr, P.; Moffat, R.; Gruber, I.M.; von Wolff, M. Twenty years’ experience with the Swiss data registry for assisted reproductive medicine: Outcomes, key trends and recommendations for improved practice. Swiss Med. Wkly. 2015, 145, w14087. [Google Scholar]
- Garcia-Velasco, J.A.; Bermejo, A.; Ruiz, F.; Martinez-Salazar, J.; Requena, A.; Pellicer, A. Cycle scheduling with oral contraceptive pills in the GnRH antagonist protocol vs. the long protocol: A randomized, controlled trial. Fertil. Steril. 2011, 96, 590–593. [Google Scholar] [CrossRef]
- Hauzman, E.E.; Zapata, A.; Bermejo, A.; Iglesias, C.; Pellicer, A.; Garcia-Velasco, J.A. Cycle scheduling for in vitro fertilization with oral contraceptive pills versus oral estradiol valerate: A randomized, controlled trial. Reprod. Biol. Endocrinol. 2013, 11, 96. [Google Scholar] [CrossRef] [Green Version]
- Andersen, A.N.; Devroey, P.; Arce, J.C. Clinical outcome following stimulation with highly purified hMG or recombinant FSH in patients undergoing IVF: A randomized assessor-blind controlled trial. Hum. Reprod. 2006, 21, 3217–3227. [Google Scholar] [CrossRef] [Green Version]
- Bosch, E.; Vidal, C.; Labarta, E.; Simon, C.; Remohi, J.; Pellicer, A. Highly purified hMG versus recombinant FSH in ovarian hyperstimulation with GnRH antagonists–a randomized study. Hum. Reprod. 2008, 23, 2346–2351. [Google Scholar] [CrossRef] [Green Version]
- Berkkanoglu, M.; Ozgur, K. What is the optimum maximal gonadotropin dosage used in microdose flare-up cycles in poor responders? Fertil. Steril. 2010, 94, 662–665. [Google Scholar] [CrossRef]
- Baker, V.L.; Brown, M.B.; Luke, B.; Smith, G.W.; Ireland, J.J. Gonadotropin dose is negatively correlated with live birth rate: Analysis of more than 650,000 assisted reproductive technology cycles. Fertil. Steril. 2015, 104, 1145–1152.e1-5. [Google Scholar] [CrossRef] [Green Version]
- Fauser, B.C.J.M.; Alper, M.M.; Ledger, W.; Schoolcraft, W.B.; Zandvliet, A.; Mannaerts, B.M.J.L. Pharmacokinetics and follicular dynamics of corifollitropin alfa versus recombinant FSH during ovarian stimulation for IVF. Reprod. Biomed. Online 2011, 22 (Suppl. 1), S23–S31. [Google Scholar] [CrossRef]
- Drakopoulos, P.; Vuong, T.N.L.; Ho, N.A.V.; Vaiarelli, A.; Ho, M.T.; Blockeel, C.; Camus, M.; Lam, A.T.; van de Vijver, A.; Humaidan, P.; et al. Corifollitropin alfa followed by highly purified HMG versus recombinant FSH in young poor ovarian responders: A multicentre randomized controlled clinical trial. Hum. Reprod. 2017, 32, 2225–2233. [Google Scholar] [CrossRef]
- Zilberberg, E.; Haas, J.; Dar, S.; Kedem, A.; Machtinger, R.; Orvieto, R. Coadministration of GnRH-agonist and hCG, for final oocyte maturation (double trigger), in patients with low proportion of mature oocytes. Gynecol. Endocrinol. 2015, 31, 145–147. [Google Scholar] [CrossRef]
- Engmann, L.; DiLuigi, A.; Schmidt, D.; Nulsen, J.; Maier, D.; Benadiva, C. The use of gonadotropin-releasing hormone (GnRH) agonist to induce oocyte maturation after cotreatment with GnRH antagonist in high-risk patients undergoing in vitro fertilization prevents the risk of ovarian hyperstimulation syndrome: A prospective randomized controlled study. Fertil. Steril. 2008, 89, 84–91. [Google Scholar]
- Humaidan, P.; Ejdrup Bredkjaer, H.; Westergaard, L.G.; Andersen, C.Y. 1500 IU human chorionic gonadotropin administered at oocyte retrieval rescues the luteal phase when gonadotropin-releasing hormone agonist is used for ovulation induction: A prospective, randomized, controlled study. Fertil. Steril. 2010, 93, 847–854. [Google Scholar] [CrossRef]
- Humaidan, P.; Polyzos, N.P.; Alsbjerg, B.; Erb, K.; Mikkelsen, A.L.; Elbaek, H.O.; Papanikolaou, E.G.; Andersen, C.Y. GnRHa trigger and individualized luteal phase hCG support according to ovarian response to stimulation: Two prospective randomized controlled multi-centre studies in IVF patients. Hum. Reprod. 2013, 28, 2511–2521. [Google Scholar] [CrossRef] [Green Version]
- Pereira, N.; Kelly, A.G.; Stone, L.D.; Witzke, J.D.; Lekovich, J.P.; Elias, R.T.; Schattman, G.L.; Rosenwaks, Z. Gonadotropin-releasing hormone agonist trigger increases the number of oocytes and embryos available for cryopreservation in cancer patients undergoing ovarian stimulation for fertility preservation. Fertil. Steril. 2017, 108, 532–538. [Google Scholar] [CrossRef] [Green Version]
- Oktay, K.; Türkçüoğlu, I.; Rodriguez-Wallberg, K.A. GnRH agonist trigger for women with breast cancer undergoing fertility preservation by aromatase inhibitor/FSH stimulation. Reprod. Biomed. Online 2010, 20, 783–788. [Google Scholar] [CrossRef] [Green Version]
- Humaidan, P.; Bredkjaer, H.E.; Bungum, L.; Bungum, M.; Grøndahl, M.L.; Westergaard, L.; Andersen, C.Y. GnRH agonist (buserelin) or hCG for ovulation induction in GnRH antagonist IVF/ICSI cycles: A prospective randomized study. Hum. Reprod. 2005, 20, 1213–1220. [Google Scholar] [CrossRef] [Green Version]
- Haahr, T.; Roque, M.; Esteves, S.C.; Humaidan, P. GnRH agonist trigger and LH activity luteal phase support versus hCG trigger and conventional luteal phase support in fresh embryo transfer IVF/ICSI cycles-a systematic PRISMA review and meta-analysis. Front. Endocrinol. 2017, 8, 116. [Google Scholar] [CrossRef]
- Fauser, B.C.; de Jong, D.; Olivennes, F.; Wramsby, H.; Tay, C.; Itskovitz-Eldor, J.; van Hooren, H.G. Endocrine profiles after triggering of final oocyte maturation with GnRH agonist after cotreatment with the GnRHantagonist ganirelix during ovarian hyperstimulation for in vitro fertilization. J. Clin. Endocrinol. Metab. 2002, 87, 709–715. [Google Scholar] [CrossRef]
- Shapiro, B.S.; Daneshmand, S.T.; Garner, F.C.; Aguirre, M.; Thomas, S. Gonadotropin-releasing hormone agonist combined with a reduced dose of human chorionic gonadotropin for final oocyte maturation in fresh autologous cycles of in vitro fertilization. Fertil. Steril. 2008, 90, 231–233. [Google Scholar] [CrossRef]
- Haas, J.; Zilberberg, E.; Dar, S.; Kedem, A.; Machtinger, R.; Orvieto, R. Coadministration of GnRH-agonist and hCG for final oocyte maturation (double trigger) in patients with low number of oocytes retrieved per number of preovulatory follicles–a preliminary report. J. Ovarian Res. 2014, 7, 77. [Google Scholar] [CrossRef] [Green Version]
- Beck-Fruchter, R.; Weiss, A.; Lavee, M.; Geslevich, Y.; Shalev, E. Empty follicle syndrome: Successful treatment in a recurrent case and review of the literature. Hum. Reprod. 2012, 27, 1357–1367. [Google Scholar] [CrossRef] [Green Version]
- Meniru, G.I.; Craft, I.L. Evidence from a salvaged treatment cycle supports an aetiology for the empty follicle syndrome that is related to terminal follicular developmental events. Hum. Reprod. 1997, 12, 2385–7. [Google Scholar] [CrossRef] [Green Version]
- Weil, S.; Vendola, K.; Zhou, J.; Bondy, C.A. Androgen and follicle-stimulating hormone interactions in primate ovarian follicle development. J. Clin. Endocrinol. Metab. 1999, 84, 2951–2956. [Google Scholar] [CrossRef]
- Vendola, K.A.; Zhou, J.; Adesanya, O.O.; Weil, S.J.; Bondy, C.A. Androgens stimulate early stages of follicular growth in the primate ovary. J. Clin. Investig. 1998, 101, 2622–2629. [Google Scholar] [CrossRef] [Green Version]
- Vendola, K.; Zhou, J.; Wang, J.; Famuyiwa, O.A.; Bievre, M.; Bondy, C.A. Androgens promote oocyte insulin-like growth factor I expression and initiation of follicle development in the primate ovary. Biol. Reprod. 1999, 61, 353–357. [Google Scholar] [CrossRef]
- Erickson, G.F.; Garzo, V.G.; Magoffin, D.A. Insulin-like growth factor-I regulates aromatase activity in human granulosa and granulosa luteal cells. J. Clin. Endocrinol. Metab. 1989, 69, 716–724. [Google Scholar] [CrossRef]
- Mason, H.D.; Martikainen, H.; Beard, R.W.; Anyaoku, V.; Franks, S. Direct gonadotrophic effect of growth hormone on oestradiol production by human granulosa cells in vitro. J. Endocrinol. 1990, 126, R1–R4. [Google Scholar] [CrossRef]
- Duffy, J.M.; Ahmad, G.; Mohiyiddeen, L.; Nardo, L.G.; Watson, A. Growth hormone for in vitro fertilization. Cochrane Database Syst. Rev. 2010, 1, CD000099. [Google Scholar] [CrossRef]
- Kolibianakis, E.M.; Venetis, C.A.; Diedrich, K.; Tarlatzis, B.C.; Griesinger, G. Addition of growth hormone to gonadotrophins in ovarian stimulation of poor responders treated by in-vitro fertilization: A systematic review and meta-analysis. Hum. Reprod. Update 2009, 15, 613–622. [Google Scholar] [CrossRef] [Green Version]
- Li, X.L.; Wang, L.; Lv, F.; Huang, X.M.; Wang, L.P.; Pan, Y.; Zhang, X.M. The influence of different growth hormone addition protocols to poor ovarian responders on clinical outcomes in controlled ovary stimulation cycles: A systematic review and meta-analysis. Medicine 2017, 96, e6443. [Google Scholar] [CrossRef]
- Hart, R.J.; Rombauts, L.; Norman, R.J. Growth hormone in IVF cycles: Any hope? Curr. Opin. Obs. Gynecol. 2017, 29, 119–125. [Google Scholar] [CrossRef]
- Norman, R.J.; Alvino, H.; Hull, L.M.; Mol, B.W.; Hart, R.J.; Kelly, T.L.; Rombauts, L. LIGHT investigators. Human growth hormone for poor responders: A randomized placebo-controlled trial provide no evidence for improved live birth rate. Reprod. Biomed. Online 2019, 38, 908–915. [Google Scholar] [CrossRef]
- Xu, Y.; Nisenblat, V.; Lu, C.; Li, R.; Qiao, J.; Zhen, X.; Wang, S. Pretreatment with coenzyme Q10 improves ovarian response and embryo quality in low-prognosis young women with decreased ovarian reserve: A randomized controlled trial. Reprod. Biol. Endocrinol. 2018, 16, 29. [Google Scholar] [CrossRef]
- Zhai, J.; Yao, G.; Dong, F.; Bu, Z.; Cheng, Y.; Sato, Y.; Hu, L.; Zhang, Y.; Wang, J.; Dai, S.; et al. In vitro activation of follicles and fresh tissue auto-transplantation in primary ovarian insufficiency patients. J. Clin. Endocrinol. Metab. 2016, 101, 4405–4412. [Google Scholar] [CrossRef]
- Oktay, K.; Baltaci, V.; Sonmezer, M.; Turan, V.; Unsal, E.; Baltaci, A.; Aktuna, S.; Moy, F. Oogonial precursor cell-derived autologous mitochondria injection to improve outcomes in women with multiple IVF failures due to low oocyte quality: A clinical translation. Reprod. Sci. Thousand Oaks. Calif. 2015, 22, 1612–1617. [Google Scholar] [CrossRef]
- Morohaku, K.; Tanimoto, R.; Sasaki, K.; Kawahara-Miki, R.; Kono, T.; Hayashi, K.; Hirao, Y.; Obata, Y. Complete in vitro generation of fertile oocytes from mouse primordial germ cells. Proc. Natl. Acad. Sci. USA 2016, 113, 9021–9026. [Google Scholar] [CrossRef] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Musa, A.; Haahr, T.; Humaidan, P. Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations. Int. J. Mol. Sci. 2020, 21, 2110. https://doi.org/10.3390/ijms21062110
Abu-Musa A, Haahr T, Humaidan P. Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations. International Journal of Molecular Sciences. 2020; 21(6):2110. https://doi.org/10.3390/ijms21062110
Chicago/Turabian StyleAbu-Musa, Antoine, Thor Haahr, and Peter Humaidan. 2020. "Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations" International Journal of Molecular Sciences 21, no. 6: 2110. https://doi.org/10.3390/ijms21062110
APA StyleAbu-Musa, A., Haahr, T., & Humaidan, P. (2020). Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations. International Journal of Molecular Sciences, 21(6), 2110. https://doi.org/10.3390/ijms21062110