Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells



Abstract
:1. Introduction
2. Results
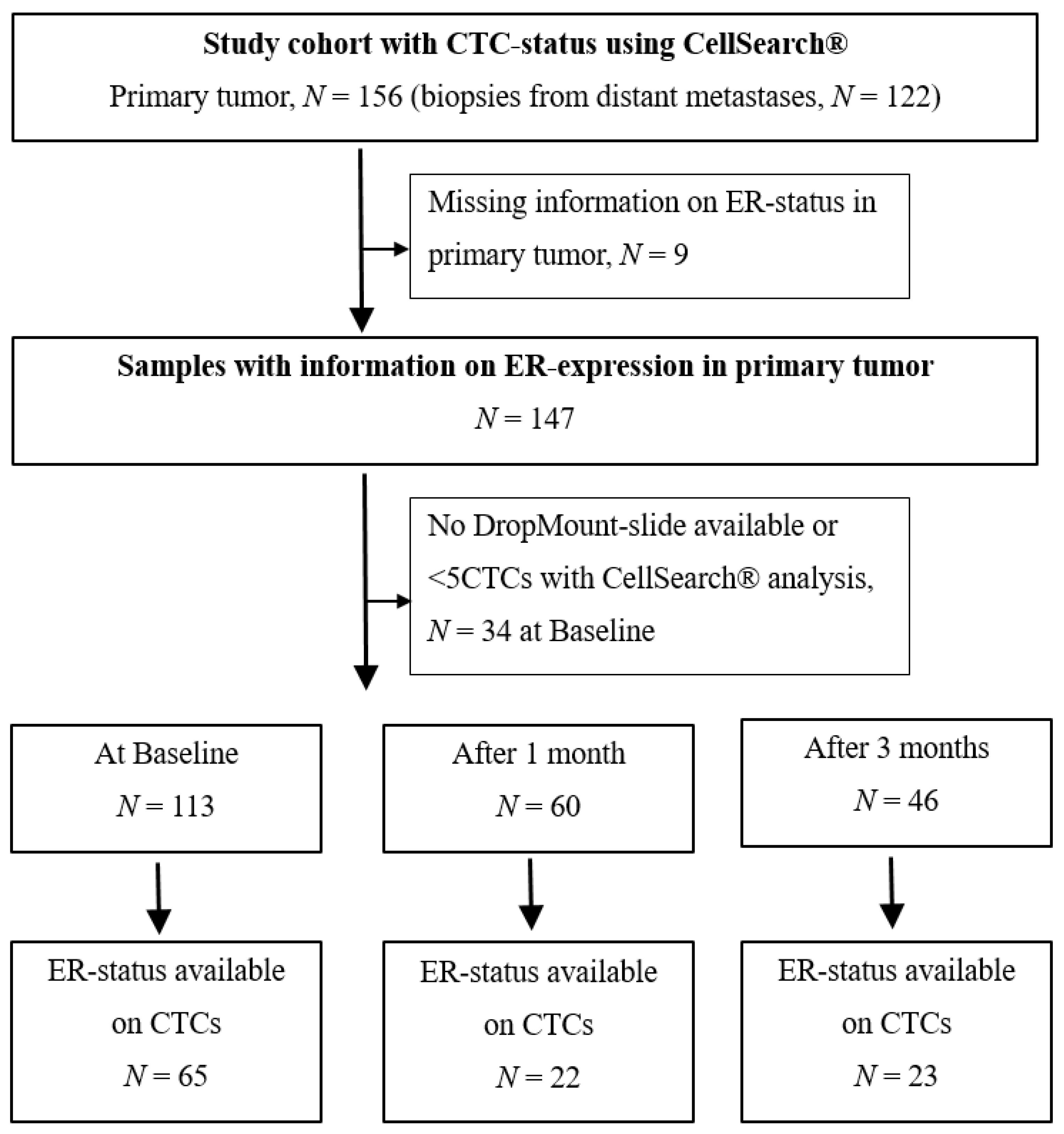
2.1. CTC Status at Baseline and During Follow-Up
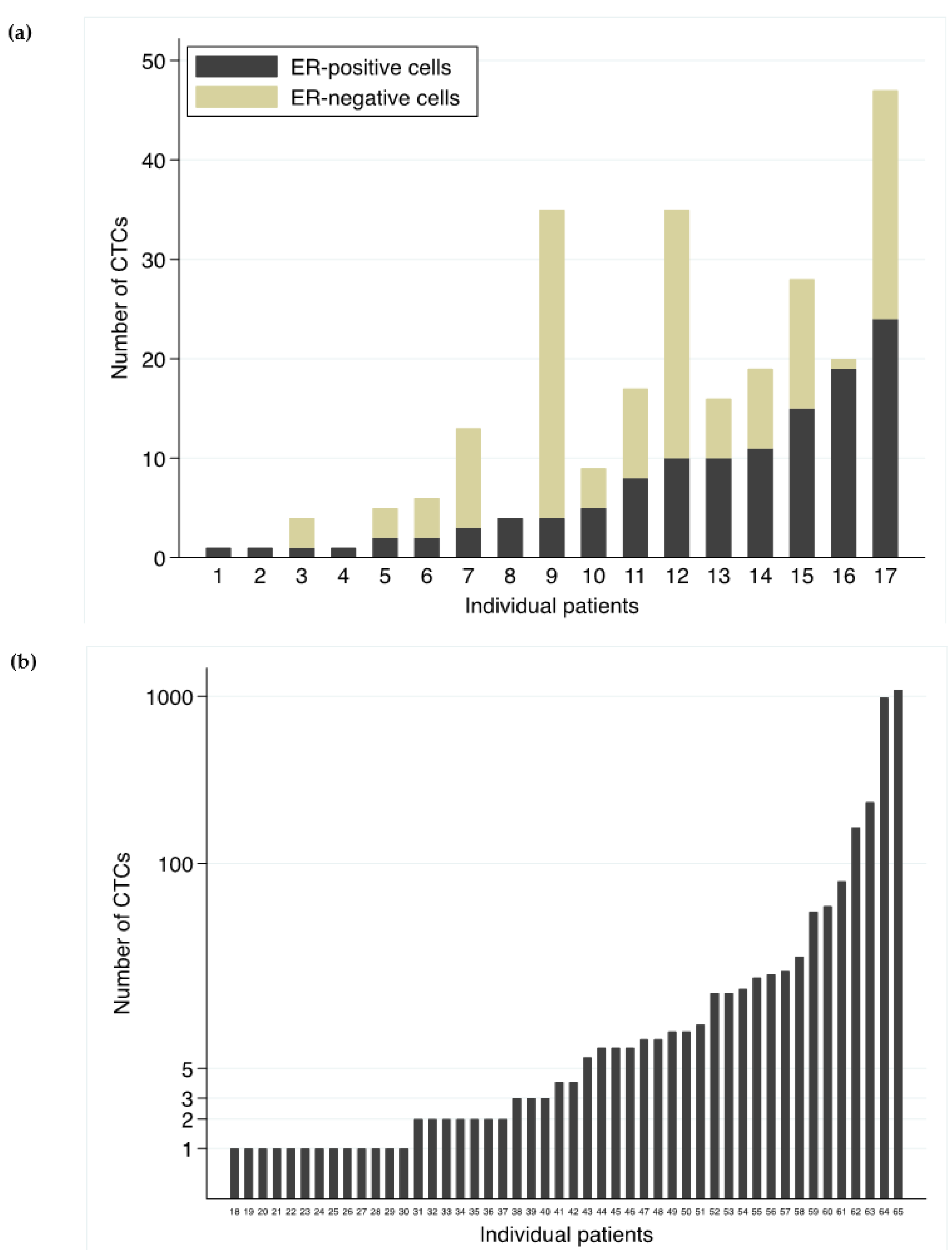
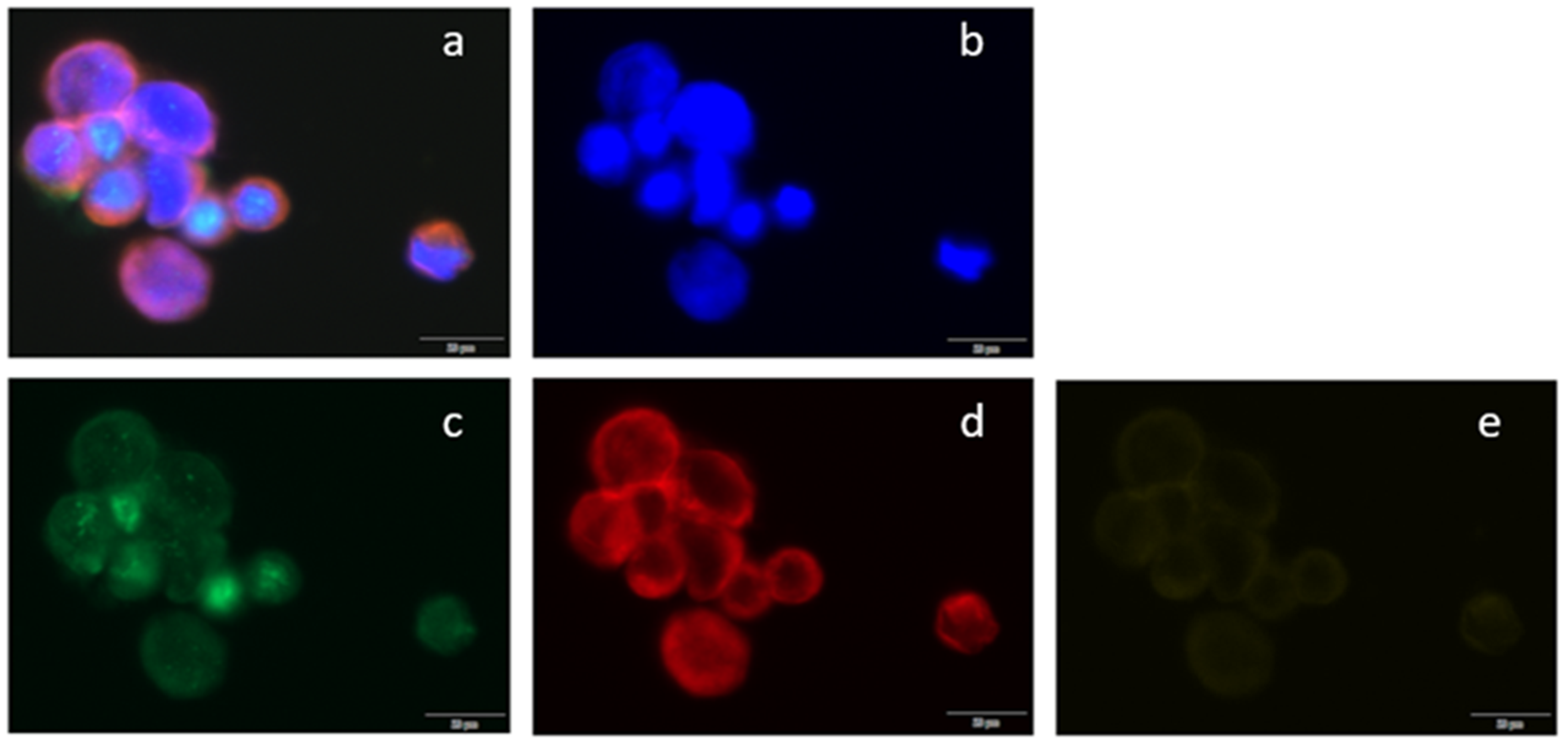
2.2. ER Status of CTCs
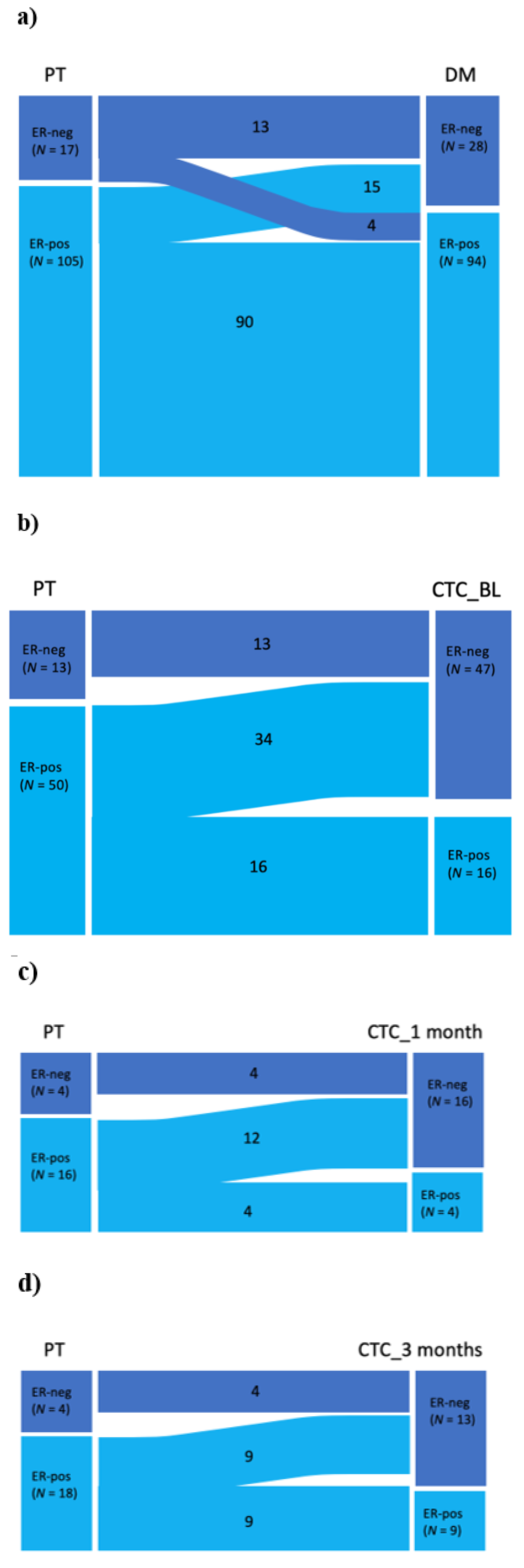
2.3. Shift in the ER Status
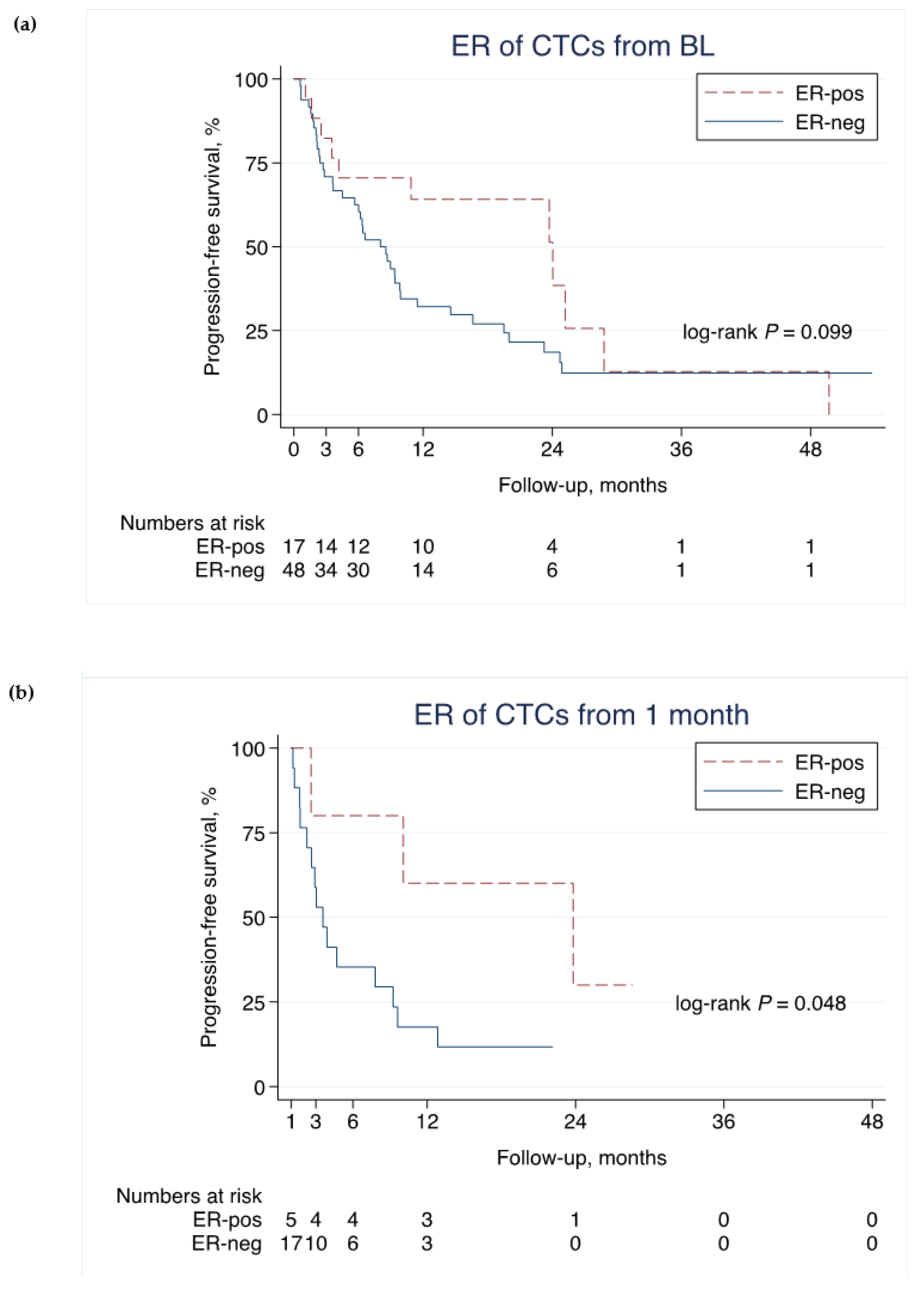
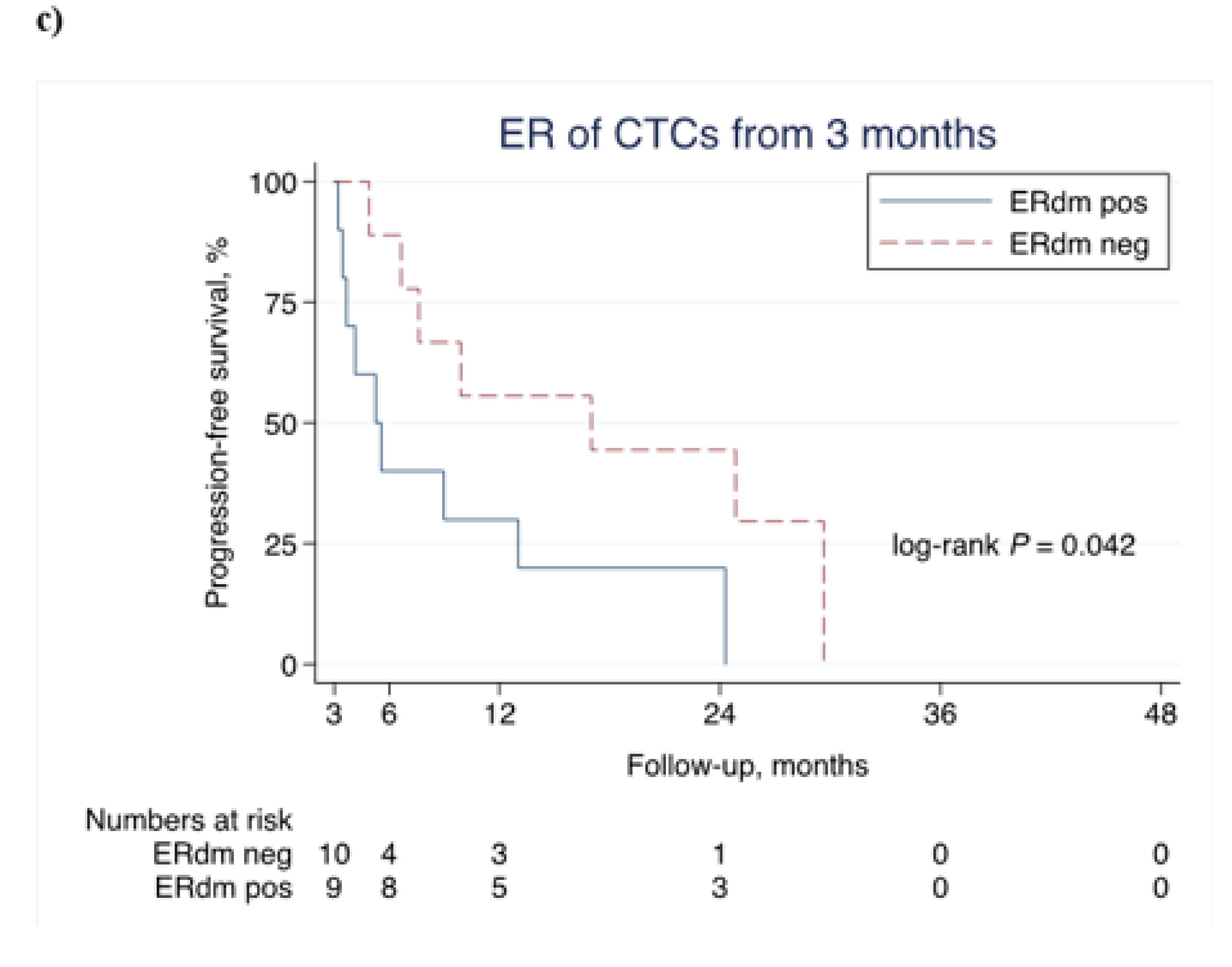
2.4. ER Status of CTCs and PFS
3. Discussion
4. Material and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brewster, A.M.; Hortobagyi, G.N.; Broglio, K.R.; Kau, S.-W.; Santa-Maria, C.A.; Arun, B.; Buzdar, A.U.; Booser, D.J.; Valero, V.; Bondy, M.; et al. Residual Risk of Breast Cancer Recurrence 5 Years After Adjuvant Therapy. J. Natl. Cancer Inst. 2008, 100, 1179–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Senkus, E.; Costa, A.; Papadopoulos, E.; Aapro, M.; Andre, F.; Harbeck, N.; Aguilar Lopez, B.; Barrios, C.H.; Bergh, J.; et al. 4th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 4) dagger. Ann. Oncol. 2018, 29, 1634–1657. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Hayes, D.F. Uses and abuses of tumor markers in the diagnosis, monitoring, and treatment of primary and metastatic breast cancer. Oncologist 2006, 11, 541–552. [Google Scholar] [CrossRef] [Green Version]
- Van Poznak, C.; Somerfield, M.R.; Bast, R.C.; Cristofanilli, M.; Goetz, M.P.; Gonzalez-Angulo, A.M.; Hicks, D.G.; Hill, E.G.; Liu, M.C.; Lucas, W.; et al. Use of Biomarkers to Guide Decisions on Systemic Therapy for Women with Metastatic Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2015, 33, 2695–2704. [Google Scholar] [CrossRef]
- Aitken, S.J.; Thomas, J.S.; Langdon, S.P.; Harrison, D.J.; Faratian, D. Quantitative analysis of changes in ER, PR and HER2 expression in primary breast cancer and paired nodal metastases. Ann. Oncol. 2010, 21, 1254–1261. [Google Scholar] [CrossRef]
- Simmons, C.; Miller, N.; Geddie, W.; Gianfelice, D.; Oldfield, M.; Dranitsaris, G.; Clemons, M. Does confirmatory tumor biopsy alter the management of breast cancer patients with distant metastases? Ann. Oncol. 2009, 20, 1499–1504. [Google Scholar] [CrossRef]
- Osborne, C.K.; Schiff, R. Mechanisms of endocrine resistance in breast cancer. Annu. Rev. Med. 2011, 62, 233–247. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, M.C.; Detre, S.; Johnston, S.; Mohsin, S.K.; Shou, J.; Allred, D.C.; Schiff, R.; Osborne, C.K.; Dowsett, M. Molecular Changes in Tamoxifen-Resistant Breast Cancer: Relationship Between Estrogen Receptor, HER-2, and p38 Mitogen-Activated Protein Kinase. J. Clin. Oncol. 2005, 23, 2469–2476. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Bidard, F.-C.; Peeters, D.; Fehm, T.; Nolè, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; García-Sáenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Scher, H.I.; Jia, X.; De Bono, J.S.; Fleisher, M.; Pienta, K.J.; Raghavan, D.; Heller, G. Circulating tumour cells as prognostic markers in progressive, castration-resistant prostate cancer: A reanalysis of IMMC38 trial data. Lancet Oncol. 2009, 10, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Hou, J.-M.; Krebs, M.; Lancashire, L.; Sloane, R.S.; Backen, A.; Swain, R.K.; Priest, L.J.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical Significance and Molecular Characteristics of Circulating Tumor Cells and Circulating Tumor Microemboli in Patients With Small-Cell Lung Cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.; Sloane, R.S.; Priest, L.; Lancashire, L.; Hou, J.-M.; Greystoke, A.; Ward, T.; Ferraldeschi, R.; Hughes, A.; Clack, G.; et al. Evaluation and Prognostic Significance of Circulating Tumor Cells in Patients With Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2011, 29, 1556–1563. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, C.; Meropol, N.J.; Punt, C.J.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.A.; Mitchell, E.; et al. Relationship among circulating tumor cells, CEA and overall survival in patients with metastatic colorectal cancer. Ann. Oncol. 2013, 24, 420–428. [Google Scholar] [CrossRef]
- Deneve, E.; Riethdorf, S.; Ramos, J.; Nocca, D.; Coffy, A.; Daures, J.P.; Maudelonde, T.; Fabre, J.M.; Pantel, K.; Alix-Panabieres, C. Capture of viable circulating tumor cells in the liver of colorectal cancer patients. Clin. Chem. 2013, 59, 1384–1392. [Google Scholar] [CrossRef] [Green Version]
- Gay, L.; Baker, A.-M.; Graham, T.A. Tumour Cell Heterogeneity. F1000Research 2016, 5, 238. [Google Scholar] [CrossRef] [Green Version]
- Smerage, J.B.; Barlow, W.E.; Hortobagyi, G.N.; Winer, E.P.; Leyland-Jones, B.; Srkalovic, G.; Tejwani, S.; Schott, A.F.; O’Rourke, M.A.; Lew, D.L.; et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J. Clin. Oncol. 2014, 32, 3483–3489. [Google Scholar] [CrossRef]
- Bock, C.; Rack, B.; Kuhn, C.; Hofmann, S.; Finkenzeller, C.; Jager, B.; Jeschke, U.; Doisneau-Sixou, S.F. Heterogeneity of ERalpha and ErbB2 Status in Cell Lines and Circulating Tumor Cells of Metastatic Breast Cancer Patients. Transl. Oncol. 2012, 5, 475–485. [Google Scholar] [CrossRef] [Green Version]
- Van De Ven, S.; Smit, V.T.H.B.M.; Dekker, T.J.A.; Nortier, J.; Kroep, J.R. Discordances in ER, PR and HER2 receptors after neoadjuvant chemotherapy in breast cancer. Cancer Treat. Rev. 2010, 37. [Google Scholar] [CrossRef]
- Curtit, E.; Nerich, V.; Mansi, L.; Chaigneau, L.; Cals, L.; Villanueva, C.; Bazan, F.; Montcuquet, P.; Meneveau, N.; Perrin, S.; et al. Discordances in Estrogen Receptor Status, Progesterone Receptor Status, and HER2 Status Between Primary Breast Cancer and Metastasis. Oncologist 2013, 18, 667–674. [Google Scholar] [CrossRef] [Green Version]
- Aktas, B.; Müller, V.; Tewes, M.; Zeitz, J.; Kasimir-Bauer, S.; Loehberg, C.R.; Rack, B.; Schneeweiss, A.; Fehm, T. Comparison of estrogen and progesterone receptor status of circulating tumor cells and the primary tumor in metastatic breast cancer patients. Gynecol. Oncol. 2011, 122, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Somlo, G.; Lau, S.K.; Frankel, P.; Ben Hsieh, H.; Liu, X.; Yang, L.; Krivacic, R.; Bruce, R.H. Multiple biomarker expression on circulating tumor cells in comparison to tumor tissues from primary and metastatic sites in patients with locally advanced/inflammatory, and stage IV breast cancer, using a novel detection technology. Breast Cancer Res. Treat. 2011, 128, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindström, L.S.; Karlsson, E.; Wilking, U.; Johansson, U.; Hartman, J.; Lidbrink, E.; Hatschek, T.; Skoog, L.; Bergh, J. Clinically Used Breast Cancer Markers Such As Estrogen Receptor, Progesterone Receptor, and Human Epidermal Growth Factor Receptor 2 Are Unstable Throughout Tumor Progression. J. Clin. Oncol. 2012, 30, 2601–2608. [Google Scholar] [CrossRef]
- Paoletti, C.; Muñiz, M.C.; Thomas, D.G.; Griffith, K.A.; Kidwell, K.M.; Tokudome, N.; Brown, M.E.; Aung, K.; Miller, M.C.; Blossom, D.L.; et al. Development of Circulating Tumor Cell-Endocrine Therapy Index in Patients with Hormone Receptor–Positive Breast Cancer. Clin. Cancer Res. 2014, 21, 2487–2498. [Google Scholar] [CrossRef] [Green Version]
- Swennenhuis, J.F.; Tibbe, A.G.; Levink, R.; Sipkema, R.C.; Terstappen, L.W. Characterization of circulating tumor cells by fluorescence in situ hybridization. Cytometry A 2009, 75, 520–527. [Google Scholar] [CrossRef]
- Babayan, A.; Hannemann, J.; Spötter, J.; Müller, V.; Pantel, K.; Joosse, S.A. Heterogeneity of Estrogen Receptor Expression in Circulating Tumor Cells from Metastatic Breast Cancer Patients. PLoS ONE 2013, 8, e75038. [Google Scholar] [CrossRef] [Green Version]
- Jansson, S.; Bendahl, P.-O.; Larsson, A.-M.; Aaltonen, K.E.; Rydén, L. Prognostic impact of circulating tumor cell apoptosis and clusters in serial blood samples from patients with metastatic breast cancer in a prospective observational cohort. BMC Cancer 2016, 16, 433. [Google Scholar] [CrossRef] [Green Version]
- Larsson, A.-M.; Jansson, S.; Bendahl, P.-O.; Jörgensen, C.L.T.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.E.; Rydén, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. 2018, 20, 48. [Google Scholar] [CrossRef]
- Molina, R.; Barak, V.; Van Dalen, A.; Duffy, M.J.; Einarsson, R.; Gion, M.; Goike, H.; Lamerz, R.; Nap, M.; Sölétormos, G.; et al. Tumor Markers in Breast Cancer—European Group on Tumor Markers Recommendations. Tumor Boil. 2005, 26, 281–293. [Google Scholar] [CrossRef] [Green Version]
- Frithiof, H.; Welinder, C.; Larsson, A.-M.; Rydén, L.; Aaltonen, K.E. A novel method for downstream characterization of breast cancer circulating tumor cells following CellSearch isolation. J. Transl. Med. 2015, 13, 126. [Google Scholar] [CrossRef] [Green Version]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. REporting recommendations for tumour MARKer prognostic studies (REMARK). Eur. J. Cancer 2005, 41, 1690–1696. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting recommendations for tumor marker prognostic studies (REMARK): Explanation and elaboration. BMC Med. 2012, 10, 51. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients, PT (n = 147) | CTC BL (n = 113) | CTC 1 Month (n = 60) | CTC 3 Months (n = 46) | DM after PT (n = 122) | |
|---|---|---|---|---|---|
| Age at diagnosis of MBC | |||||
| Median (range) in years | 65 (40–84) | 60 (34–83) | 59 (37–82) | 59 (39–77) | 59 (32–83) |
| Time from PT to DM | |||||
| Median (range) in years | 4.5 (0–36) | 4.2 (0–36) | 3.6 (0–36) | 4.7 (0–36) | 5.2 (0–36) |
| PT ER-status, n (%) | |||||
| Negative | 24 (16%) | 17 (15%) | 8 (13%) | 6 (13%) | 17 (14%) |
| Positive | 123 (84%) | 93 (85%) | 52 (87%) | 40 (87%) | 105 (86%) |
| Missing | 3 | 1 | |||
| DM ER-status, n (%) | |||||
| Negative | 28 (23%) | 22 (23%) | 13 (25%) | 7 (18%) | 28 (23%) |
| Positive | 94 (77%) | 73 (77%) | 39 (75%) | 31 (82%) | 94 (77%) |
| Missing | 25 | 18 | 8 | 8 | 25 |
| HER2-status, n (%) | |||||
| Negative | 109 (87%) | 83 (87%) | 50 (94%) | 39 (97%) | 88 (86%) |
| Positive | 17 (13%) | 11 (13%) | 3 (6%) | 1 (3%) | 14 (14%) |
| Missing | 21 | 19 | 7 | 6 | 20 |
| PT tumor size, n (%) | |||||
| T1 | 52 (37%) | 35 (34%) | 16 (27%) | 15 (35%) | 50 (42%) |
| T2 | 49 (35%) | 37 (36%) | 23 (40%) | 14 (33%) | 43 (36%) |
| T3 | 20 (14%) | 16 (16%) | 8 (14%) | 7 (16%) | 15 (13%) |
| T4 | 19 (14%) | 15 (14%) | 11 (19%) | 7 (16%) | 10 (9%) |
| Missing | 7 | 10 | 2 | 3 | 4 |
| PT Node status, n (%) | |||||
| Node negative | 41 (32%) | 27 (28%) | 13 (25%) | 10 (24%) | 39 (35%) |
| Node positive | 88 (68%) | 72 (72%) | 39 (75%) | 30 (76%) | 74 (65%) |
| Missing | 18 | 14 | 8 | 6 | 9 |
| PT NHG, n (%) | |||||
| Grade 1 | 12 (10%) | 8 (9%) | 2 (4%) | 4 (10%) | 11 (10%) |
| Grade 2 | 64 (53%) | 52 (58%) | 31 (63%) | 24 (62%) | 60 (56%) |
| Grade 3 | 45 (37%) | 29 (33%) | 16 (33%) | 11 (28%) | 37 (34%) |
| Missing | 26 | 24 | 11 | 7 | 14 |
| First-line systemic treatment, n (%) | |||||
| Endocrine only | 92 (63%) | 67 (59%) | 35 (58%) | 33 (72%) | 86 (70%) |
| Chemotherapy | 70 (48%) | 53 (47%) | 33 (53%) | 32 (70%) | 63 (52%) |
| HER2-targeted | 5 (3%) | 1 (1%) | 1 (2%) | 1 (2%) | 5 (4%) |
| CellSearch® BL CTC number | |||||
| Median (range) | 5 (0–2598) | 17 (0–2598) | 42 (0–2598) | 42 (0–2598) | 5 (0–2598) |
| Mean | 678 | 88 | 118 | 119 | 74 |
| ER Status | PT vs. DM | PT vs. BL | PT vs. 1 Month | PT vs. 3 Months | DM vs. BL | DM vs. 1 Month | DM vs. 3 Months | BL vs. 1 Month | BL vs. 3 Months | 1 Month vs. 3 Months |
|---|---|---|---|---|---|---|---|---|---|---|
| n = 122 (%) | n = 63 (%) | n = 20 (%) | n = 22 (%) | n = 55 (%) | n = 17 (%) | n = 20 (%) | n = 17 (%) | n = 19 (%) | n = 10 (%) | |
| -/- | 13 (11) | 13 (21) | 4 (20) | 4 (18) | 12 (22) | 5 (29) | 6 (30) | 10 (59) | 7 (37) | 5 (50) |
| -/+ | 4 (3) | 0 | 0 | 0 (0) | 0 | 0 | 1 (5) | 3 (17) | 6 (31) | 1 (10) |
| +/- | 15 (12) | 34 (54) | 12 (60) | 9 (41) | 29 (53) | 7 (41) | 4 (20) | 2 (12) | 3 (16) | 2 (20) |
| +/+ | 90 (74) | 16 (25) | 4 (20) | 9 (41) | 14 (25) | 5 (29) | 9 (45) | 2 (12) | 3 (16) | 2 (20) |
| p-value | 0.019 | <0.0001 | 0.0005 | 0.004 | <0.0001 | 0.016 | 0.38 | 1.0 | 0.51 | 1.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsare, C.; Bendahl, P.-O.; Moberg, E.; Levin Tykjær Jørgensen, C.; Jansson, S.; Larsson, A.-M.; Aaltonen, K.; Rydén, L. Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells. Int. J. Mol. Sci. 2020, 21, 2885. https://doi.org/10.3390/ijms21082885
Forsare C, Bendahl P-O, Moberg E, Levin Tykjær Jørgensen C, Jansson S, Larsson A-M, Aaltonen K, Rydén L. Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells. International Journal of Molecular Sciences. 2020; 21(8):2885. https://doi.org/10.3390/ijms21082885
Chicago/Turabian StyleForsare, Carina, Pär-Ola Bendahl, Eric Moberg, Charlotte Levin Tykjær Jørgensen, Sara Jansson, Anna-Maria Larsson, Kristina Aaltonen, and Lisa Rydén. 2020. "Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells" International Journal of Molecular Sciences 21, no. 8: 2885. https://doi.org/10.3390/ijms21082885
APA StyleForsare, C., Bendahl, P. -O., Moberg, E., Levin Tykjær Jørgensen, C., Jansson, S., Larsson, A. -M., Aaltonen, K., & Rydén, L. (2020). Evolution of Estrogen Receptor Status from Primary Tumors to Metastasis and Serially Collected Circulating Tumor Cells. International Journal of Molecular Sciences, 21(8), 2885. https://doi.org/10.3390/ijms21082885