Identification of Lenalidomide Sensitivity and Resistance Mechanisms in Non-Del(5q) Myelodysplastic Syndromes



Abstract
:1. Introduction
2. Results
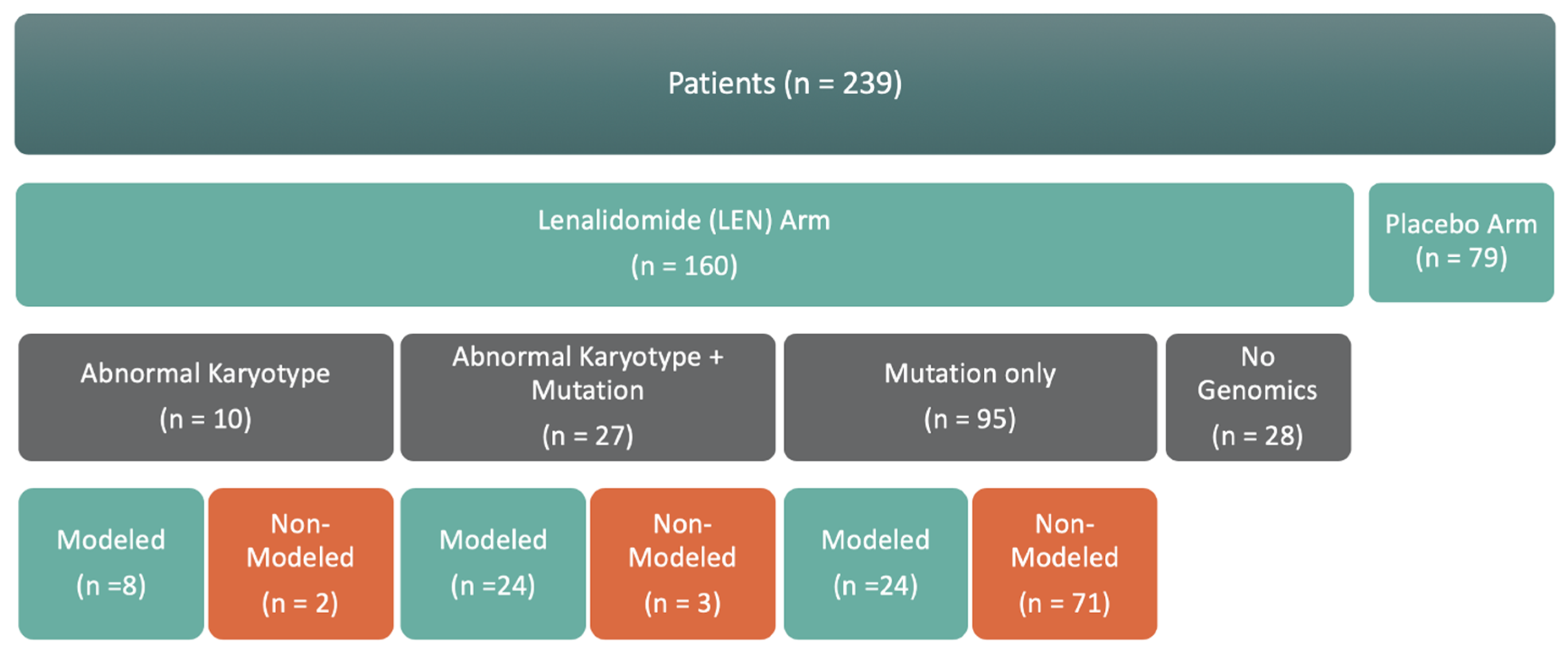
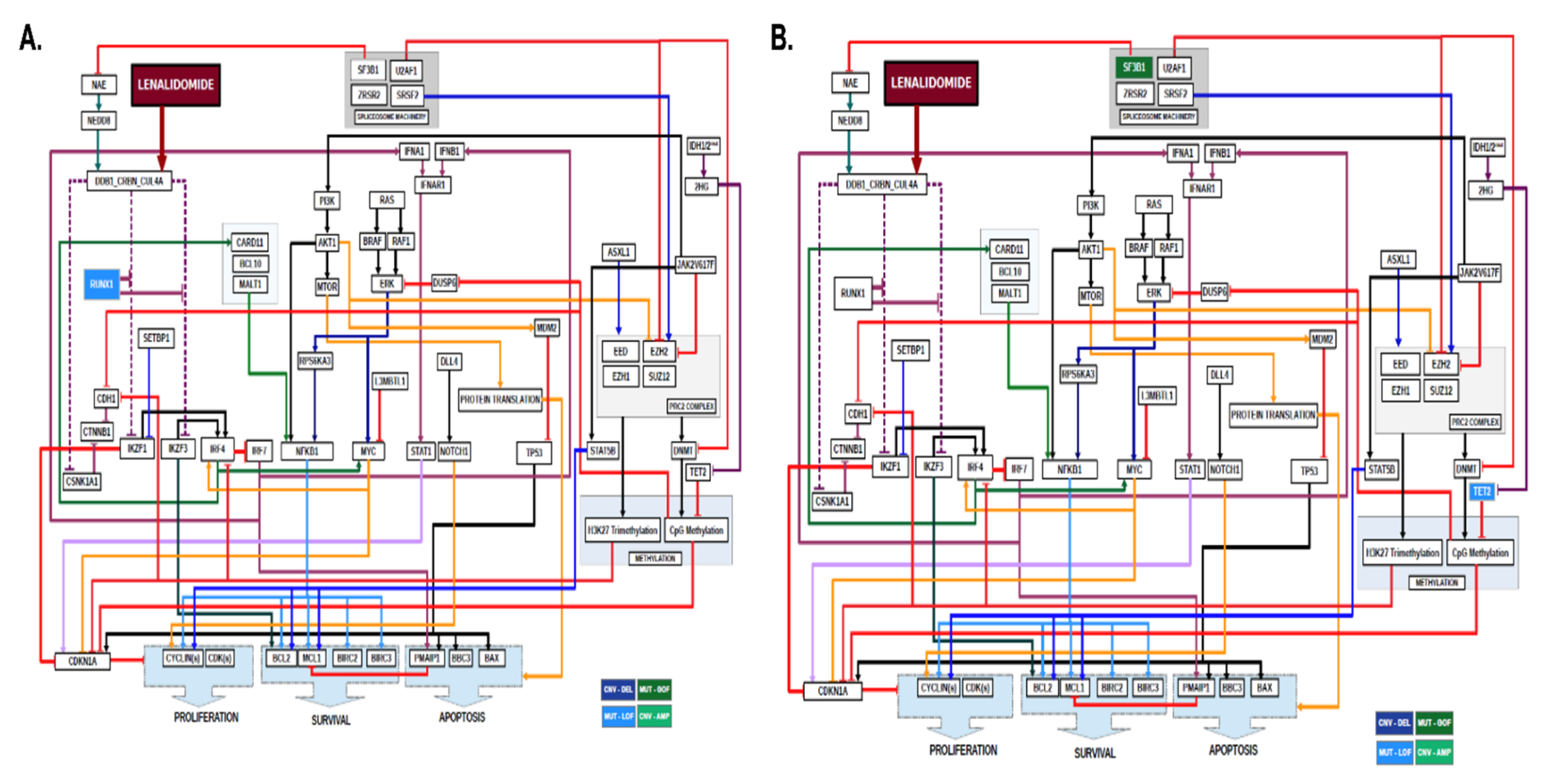
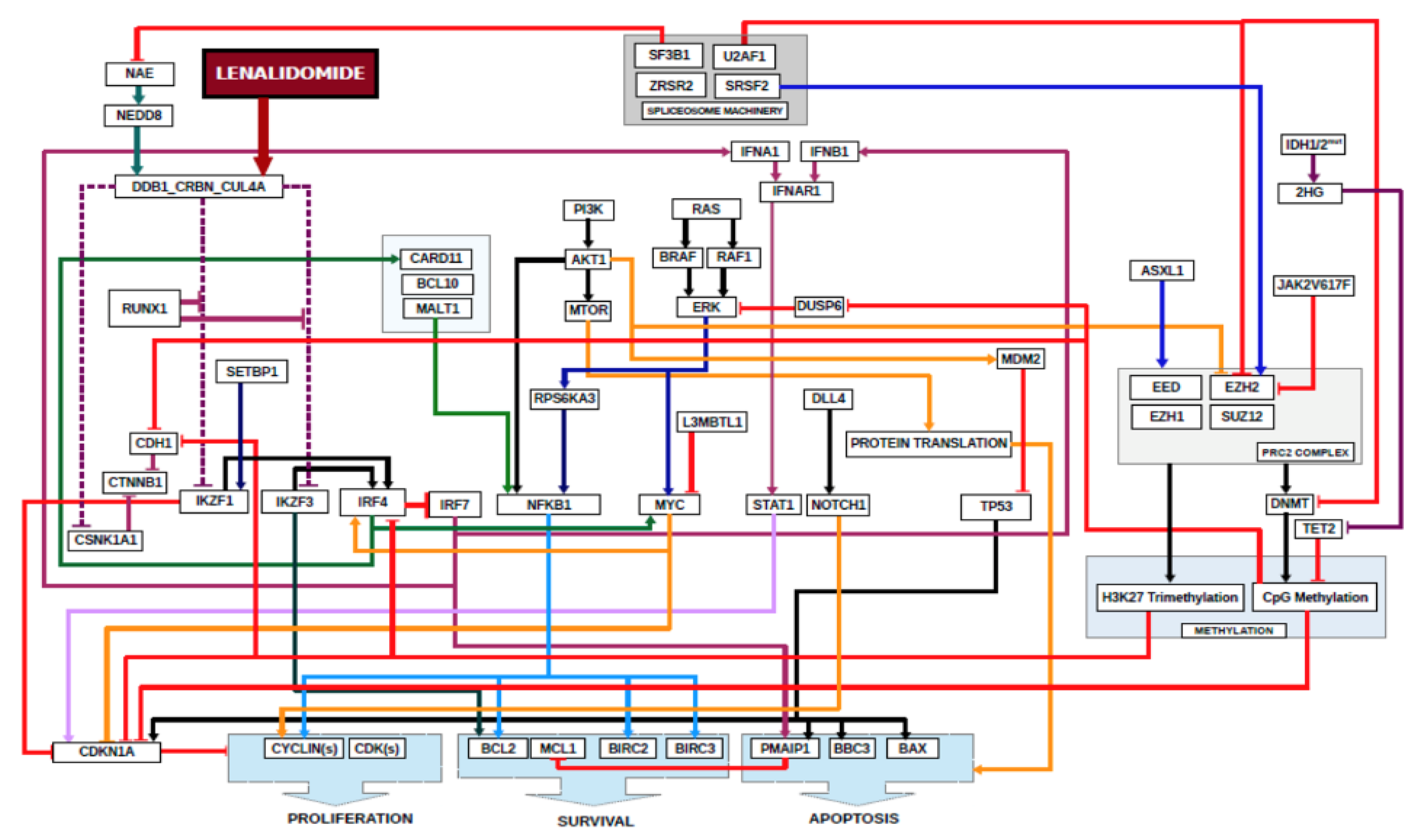
2.1. Sufficiency of Genomic Information for Computational Biology Modeling
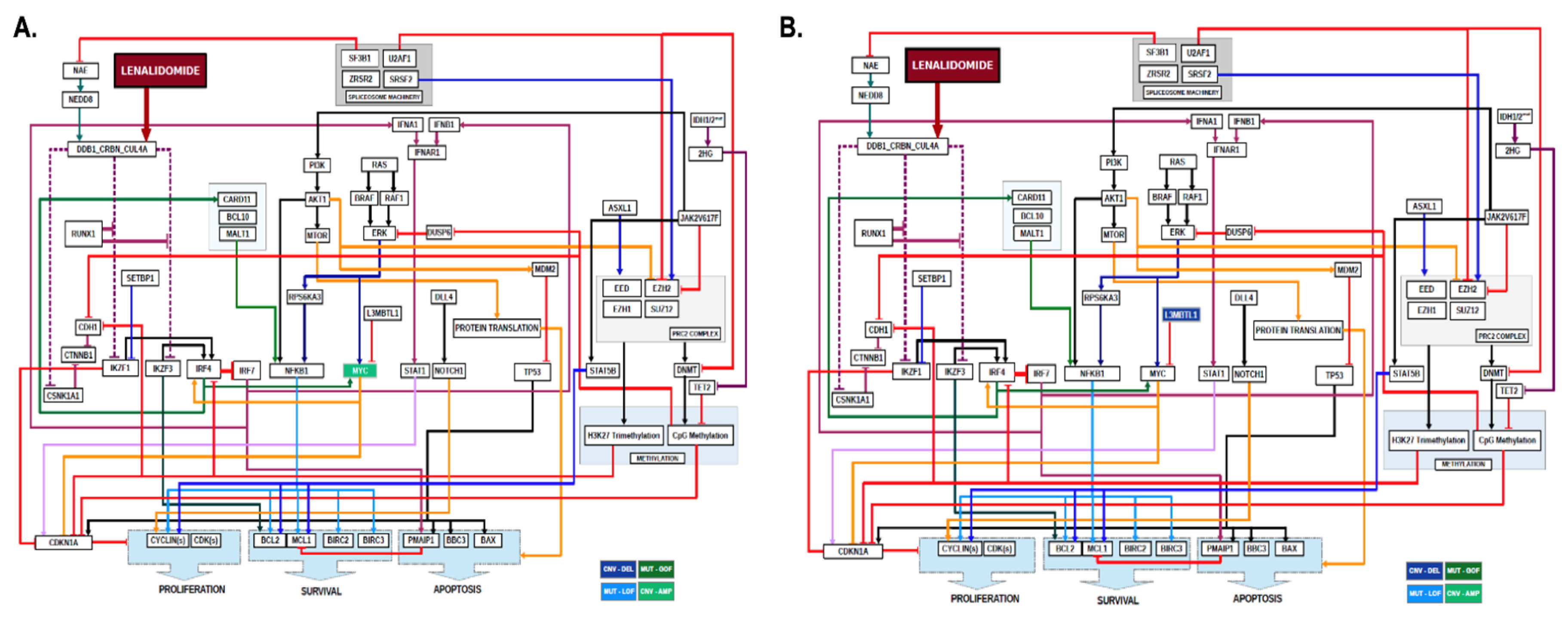
2.2. Non-Del(5q) MDS with Abnormal Karyotype
2.3. Non-Del(5q) MDS with Abnormal Karyotype and Gene Mutations
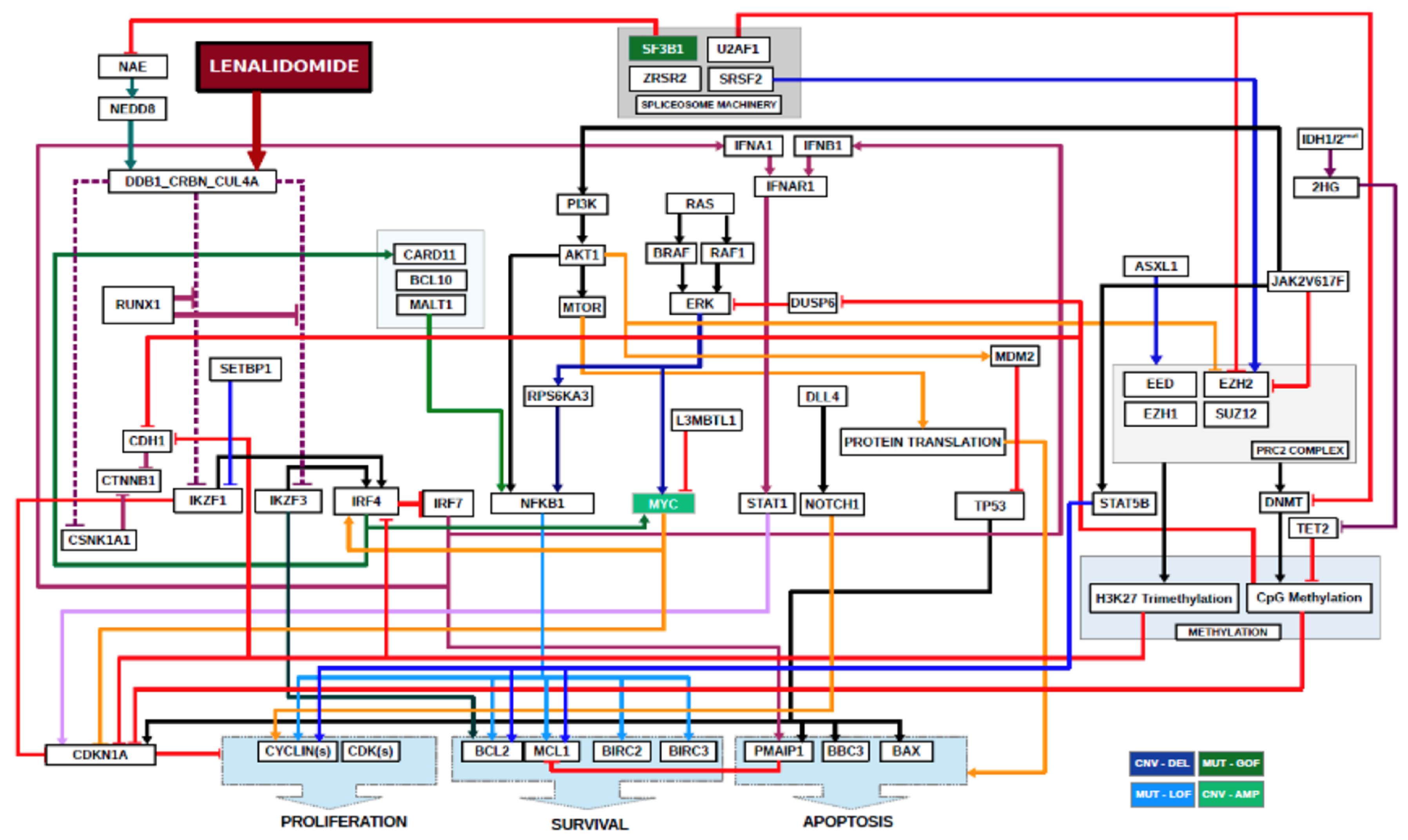
2.4. Non-Del(5q) MDS with Normal Karyotype and Gene Mutations
3. Discussion
4. Methods
4.1. Patients
4.2. Genomic Testing
4.3. Computational Biology Modeling and Digital Drug Simulation System
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- List, A.F.; Dewald, G.; Bennett, J.; Giagounidis, A.; Raza, A.; Feldman, E.; Powell, B.; Greenberg, P.; Thomas, D.; Stone, R.; et al. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N. Engl. J. Med. 2006, 355, 1456–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raza, A.; Reeves, J.A.; Feldman, E.J.; Dewald, G.W.; Bennett, J.M.; Deeg, H.J.; Dreisbach, L.; Schiffer, C.A.; Stone, R.M.; Greenberg, P.L.; et al. Phase 2 study of lenalidomide in transfusion-dependent, low-risk, and intermediate-1 risk myelodysplastic syndromes with karyotypes other than deletion 5q. Blood 2008, 111, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.L.; Stone, R.M.; Al-Kali, A.; Barta, S.K.; Bejar, R.; Bennett, J.M.; Carraway, H.; De Castro, C.M.; Deeg, H.J.; DeZern, A.E.; et al. Myelodysplastic Syndromes, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 60–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chesnais, V.; Renneville, A.; Toma, A.; Lambert, J.; Passet, M.; Dumont, F.; Chevret, S.; Lejeune, J.; Raimbault, A.; Stamatoullas, A.; et al. Effect of lenalidomide treatment on clonal architecture of myelodysplastic syndromes without 5q deletion. Blood 2016, 127, 749–760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drusbosky, L.; Medina, C.; Martuscello, R.; Hawkins, K.E.; Chang, M.; Lamba, J.K.; Vali, S.; Kumar, A.; Singh, N.K.; Abbasi, T.; et al. Computational drug treatment simulations on projections of dysregulated protein networks derived from the myelodysplastic mutanome match clinical response in patients. Leuk. Res. 2017, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Drusbosky, L.M.; Cogle, C.R. Computational Modeling and Treatment Identification in the Myelodysplastic Syndromes. Curr. Hematol. Malig. Rep. 2017, 12, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Bjorklund, C.C.; Lu, L.; Kang, J.; Hagner, P.R.; Havens, C.G.; Amatangelo, M.; Wang, M.; Ren, Y.; Couto, S.; Breider, M.; et al. Rate of CRL4(CRBN) substrate Ikaros and Aiolos degradation underlies differential activity of lenalidomide and pomalidomide in multiple myeloma cells by regulation of c-Myc and IRF4. Blood Cancer J. 2015, 5, e354. [Google Scholar] [CrossRef]
- Zhou, N.; Gutierrez-Uzquiza, A.; Zheng, X.Y.; Chang, R.; Vogl, D.T.; Garfall, A.; Bernabei, L.; Saraf, A.; Florens, L.; Washburn, M.P.; et al. RUNX proteins desensitize multiple myeloma to lenalidomide via protecting IKZFs from degradation. Leukemia 2019, 33, 2006–2021. [Google Scholar] [CrossRef] [Green Version]
- Bjorklund, C.C.; Ma, W.; Wang, Z.-Q.; Davis, R.E.; Kuhn, D.J.; Kornblau, S.M.; Wang, M.; Shah, J.J.; Orlowski, R.Z. Evidence of a role for activation of Wnt/beta-catenin signaling in the resistance of plasma cells to lenalidomide. J. Biol. Chem. 2011, 286, 11009–11020. [Google Scholar] [CrossRef] [Green Version]
- Shallis, R.M.; Zeidan, A.M. Lenalidomide in Non-Deletion 5q Lower-Risk Myelodysplastic Syndromes: A Glass Quarter Full or Three Quarters Empty? Leukemia Lymphoma 2018, 59. [Google Scholar] [CrossRef]
- Negoro, E.; Radivoyevitch, T.; Polprasert, C.; Adema, V.; Hosono, N.; Makishima, H.; Przychodzen, B.; Hirsch, C.; Clemente, M.J.; Nazha, A.; et al. Molecular Predictors of Response in Patients With Myeloid Neoplasms Treated With Lenalidomide. Leukemia 2016, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeidan, A.M.; Zahr, A.A.; Aldin, E.S.; Komrokji, R.S. Clinical Utility of Lenalidomide in the Treatment of Myelodysplastic Syndromes. J. Blood Med. 2014, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugimoto, Y.; Sekeres, M.; Makishima, H.; Traina, F.; Visconte, V.; Jankowska, A.; Jerez, A.; Szpurka, H.; O’Keefe, C.L.; Guinta, K.; et al. Cytogenetic and Molecular Predictors of Response in Patients With Myeloid Malignancies Without del[5q] Treated with Lenalidomide. J. Hematol. Oncol. 2012, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallo, M.; Del Rey, M.; Ibáñez, M.; Calasanz, M.-J.; Arenillas, L.; Larráyoz, M.J.; Pedro, C.; Jerez, A.; Maciejewski, J.; Costa, L.; et al. Response to Lenalidomide in Myelodysplastic Syndromes With del(5q): Influence of Cytogenetics and Mutations. Br. J. Haematol. 2013, 162. [Google Scholar] [CrossRef] [PubMed]
- Jonasova, A.; Neuwirtová, R.; Polackova, H.; Siskova, M.; Stopka, T.; Cmunt, E.; Belickova, M.; Moudra, A.; Minařík, L.; Fuchs, O.; et al. Lenalidomide Treatment in Lower Risk Myelodysplastic syndromes-The Experience of a Czech Hematology Center. (Positive Effect of Erythropoietin ± Prednisone Addition to Lenalidomide in Refractory or Relapsed Patients). Leuk. Res. 2018, 69. [Google Scholar] [CrossRef] [PubMed]
- Adema, V.; Palomo, L.; Toma, A.; Kosmider, O.; Fuster-Tormo, F.; Benito, R.; Salgado, R.; Such, E.; Larrayoz, M.J.; Xicoy, B.; et al. Distinct Mutational Pattern of Myelodysplastic Syndromes With and without 5q- Treated With Lenalidomide. Br. J. Haematol. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonasova, A.; Bokorová, R.; Polák, J.; Vostrý, M.; Kostečka, A.; Hájková, H.; Neuwirtová, R.; Siskova, M.; Sponerova, D.; Cermak, J.; et al. High Level of Full-Length Cereblon mRNA in Lower Risk Myelodysplastic Syndrome with Isolated 5q Deletion Is Implicated in the Efficacy of Lenalidomide. Eur. J. Haematol. 2015, 95. [Google Scholar] [CrossRef]
- Sardnal, V.; Rouquette, A.; Kaltenbach, S.; Bally, C.; Chesnais, V.; Leschi, C.; Ades, L.; Santini, V.; Park, S.; Toma, A.; et al. A G Polymorphism in the CRBN Gene Acts as a Biomarker of Response to Treatment with Lenalidomide in low/int-1 Risk MDS without del(5q). Leukemia 2013, 27. [Google Scholar] [CrossRef]
- Cluzeau, T.; McGraw, K.L.; Irvine, B.; Masala, E.; Ades, L.; Basiorka, A.A.; Maciejewski, J.; Auberger, P.; Wei, S.; Fenaux, P.; et al. Pro-inflammatory Proteins S100A9 and Tumor Necrosis Factor-α Suppress Erythropoietin Elaboration in Myelodysplastic Syndromes. Haematologica 2017, 102. [Google Scholar] [CrossRef] [Green Version]
- Kerdivel, G.; Myélodysplasies, O.B.O.T.G.F.D.; Chesnais, V.; Becht, E.; Toma, A.; Cagnard, N.; Dumont, F.; Rousseau, A.; Fenaux, P.; Chevret, S.; et al. Lenalidomide-mediated Erythroid Improvement in non-del(5q) Myelodysplastic Syndromes Is Associated with Bone Marrow Immuno-Remodeling. Leukemia 2018, 32. [Google Scholar] [CrossRef]
- Ebert, B.L.; Galili, N.; Tamayo, P.; Bosco, J.; Mak, R.; Pretz, J.; Tanguturi, S.; Ladd-Acosta, C.; Stone, R.; Golub, T.R.; et al. An Erythroid Differentiation Signature Predicts Response to Lenalidomide in Myelodysplastic Syndrome. PLoS Med. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Santini, V.; Almeida, A.; Giagounidis, A.; Gröpper, S.; Jonasova, A.; Vey, N.; Mufti, G.J.; Buckstein, R.; Mittelman, M.; Platzbecker, U.; et al. Randomized Phase III Study of Lenalidomide Versus Placebo in RBC Transfusion-Dependent Patients with Lower-Risk Non-del(5q) Myelodysplastic Syndromes and Ineligible for or Refractory to Erythropoiesis-Stimulating Agents. J. Clin. Oncol. 2016, 34, 2988–2996. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Greenberg, P.L.; Bennett, J.M.; Löwenberg, B.; Wijermans, P.W.; Nimer, S.D.; Pinto, A.; Beran, M.; De Witte, T.; Stone, R.M.; et al. Clinical application and proposal for modification of the International Working Group (IWG) response criteria in myelodysplasia. Blood 2006, 108, 419–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Signature | Biomarker | ||||
|---|---|---|---|---|---|
| Groups | Summary | Sensitive | Resistance | Sensitive | Resistance |
| Abnormal Karyotype | 88.89% of patients are Responders to Lenalidomide due to the presence of Trisomy 8 or 20q deletion. Resultant patients would have higher levels of MYC in the system, one of the factors in the sensitivity loop for Lenalidomide. | MYC (AMP), L3BMTL1 (DEL) | - | MYC | - |
| Abnormal Karyotype and Gene Mutations | 81.48% of patients are Non-Responders to Lenalidomide due to the presence of mutations in SF3B1 in combination with Trisomy 8 and 20q deletion. Also, the presence of 1q amplification in patients who are Non-Responders to Lenalidomide. | MYC (AMP), L3MBTL1 (DEL) | SF3B1-K700E, TET2 (LOF), WNT3A (AMP), MCL1 (AMP), PSEN2 (AMP) | MYC | CTNNB1, NOTCH1, MCL1, SF3B1, TET2 |
| Gene Mutations only | 91.67% of patients are Non-Responders to Lenalidomide due to presence of mutations in SF3B1 and methylation machinery. | RUNX1 (LOF) | SF3B1-K700E, TET2 (LOF) | RUNX1 | SF3B1, TET2 |
| All | 74.58% of patients were Non-Responders to Lenalidomide. | MYC (AMP), L3MBTL1 (DEL), RUNX1 (LOF) | SF3B1-700E, TET2 (LOF), WNT3A (AMP), MCL1 (AMP), PSEN2 (AMP) | MYC, RUNX1 | CTNNB1, NOTCH1, MCL1, SF3B1, TET2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drusbosky, L.M.; Cogle, C.R. Identification of Lenalidomide Sensitivity and Resistance Mechanisms in Non-Del(5q) Myelodysplastic Syndromes. Int. J. Mol. Sci. 2020, 21, 3323. https://doi.org/10.3390/ijms21093323
Drusbosky LM, Cogle CR. Identification of Lenalidomide Sensitivity and Resistance Mechanisms in Non-Del(5q) Myelodysplastic Syndromes. International Journal of Molecular Sciences. 2020; 21(9):3323. https://doi.org/10.3390/ijms21093323
Chicago/Turabian StyleDrusbosky, Leylah M., and Christopher R. Cogle. 2020. "Identification of Lenalidomide Sensitivity and Resistance Mechanisms in Non-Del(5q) Myelodysplastic Syndromes" International Journal of Molecular Sciences 21, no. 9: 3323. https://doi.org/10.3390/ijms21093323
APA StyleDrusbosky, L. M., & Cogle, C. R. (2020). Identification of Lenalidomide Sensitivity and Resistance Mechanisms in Non-Del(5q) Myelodysplastic Syndromes. International Journal of Molecular Sciences, 21(9), 3323. https://doi.org/10.3390/ijms21093323