
Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis

 ,
, 
Abstract
:1. Introduction
2. Results
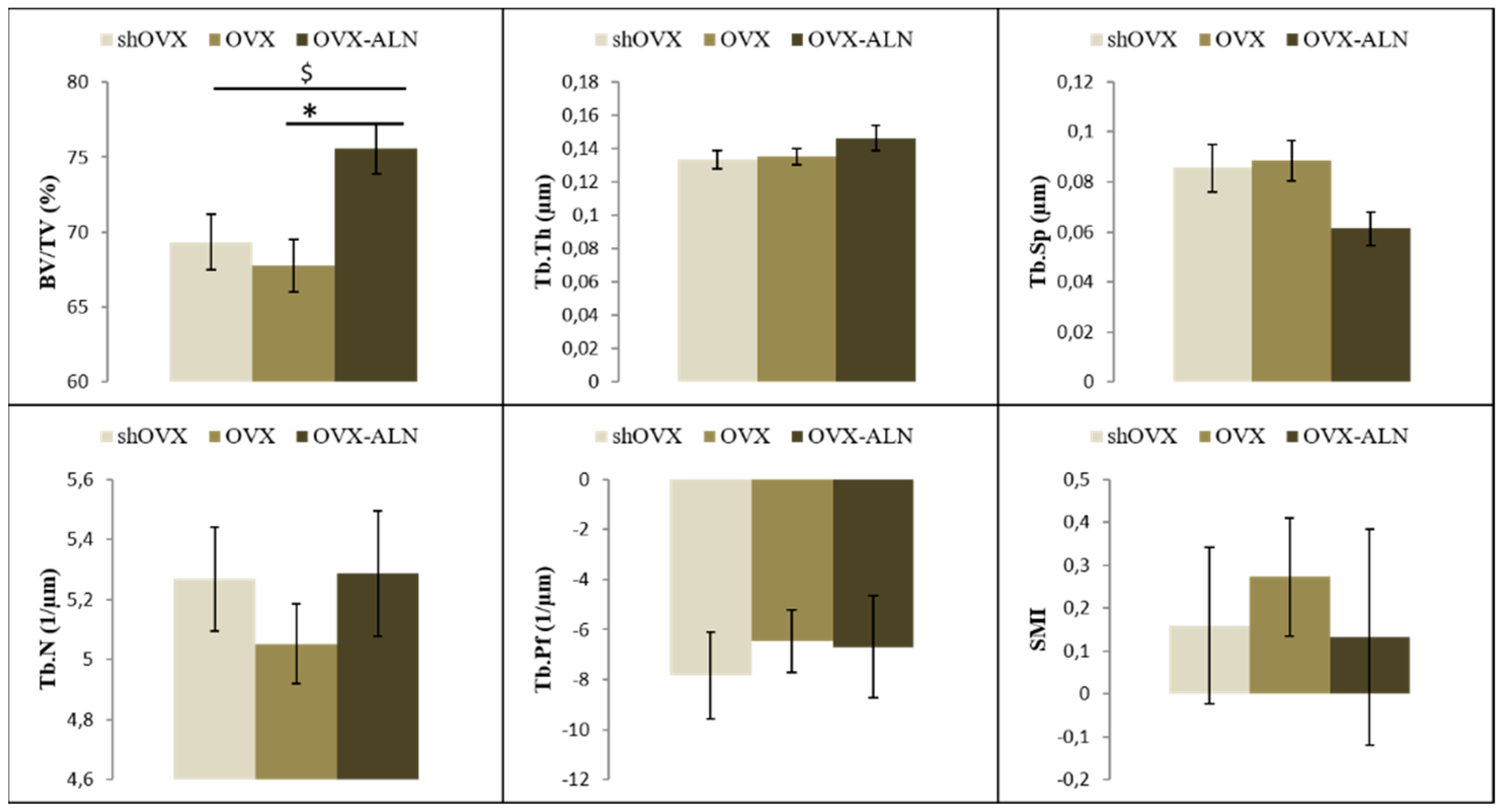
2.1. Maxilla
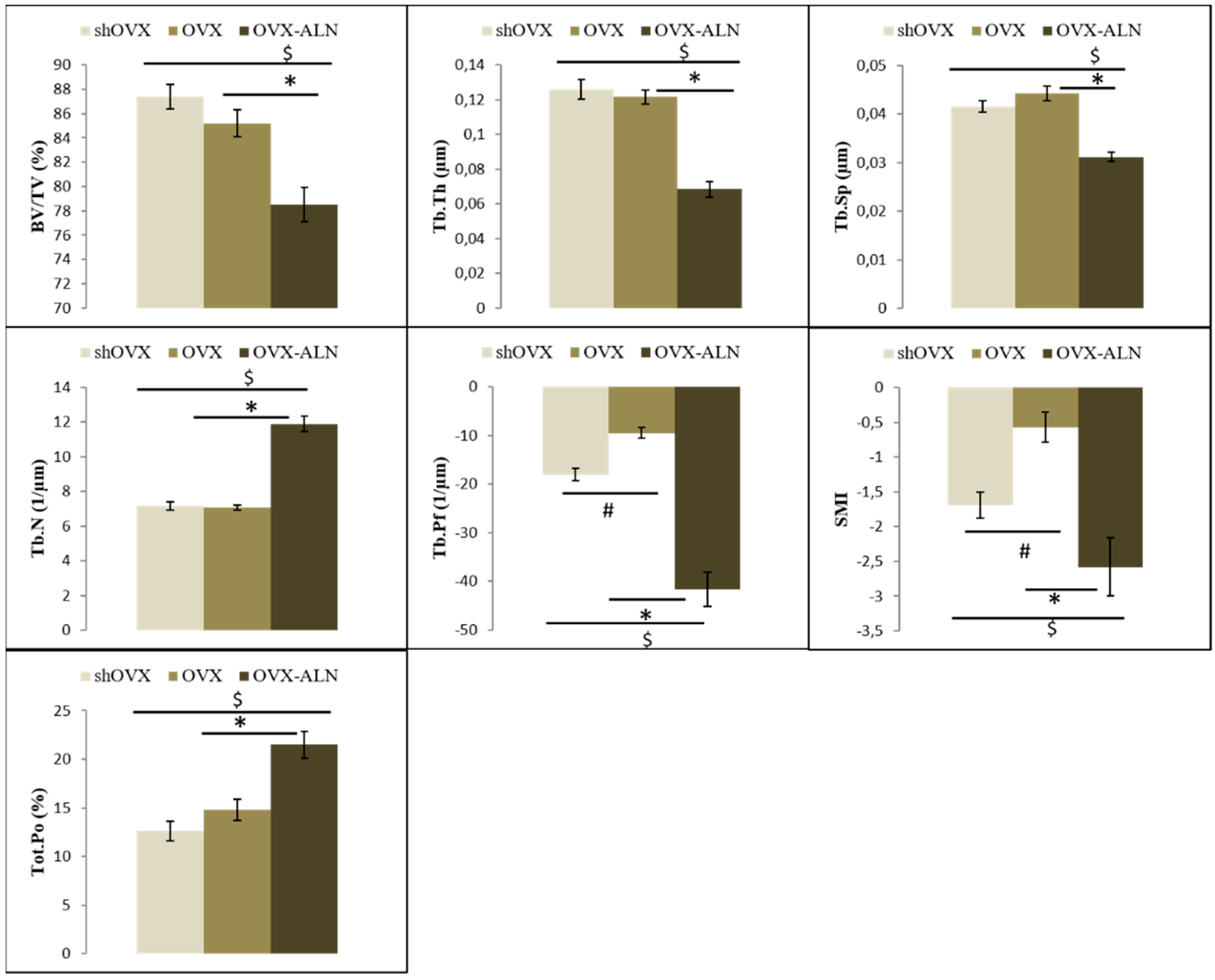
2.2. Mandible
3. Discussion
4. Materials and Methods
4.1. Animals and Experimental Design
4.2. Specimen Preparation
4.3. Micro-Computed Tomography Imaging
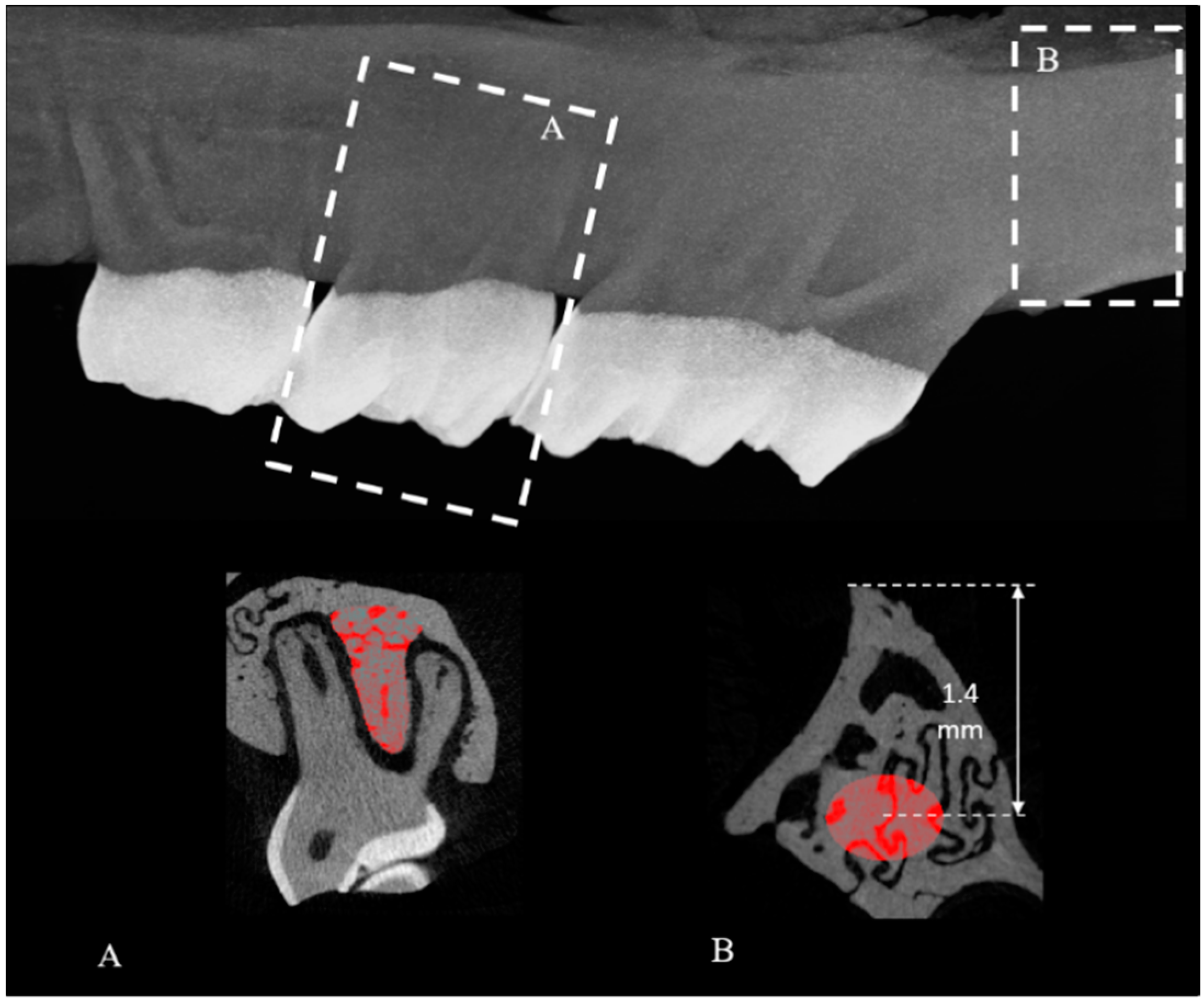
4.4. Analysis of the Maxilla
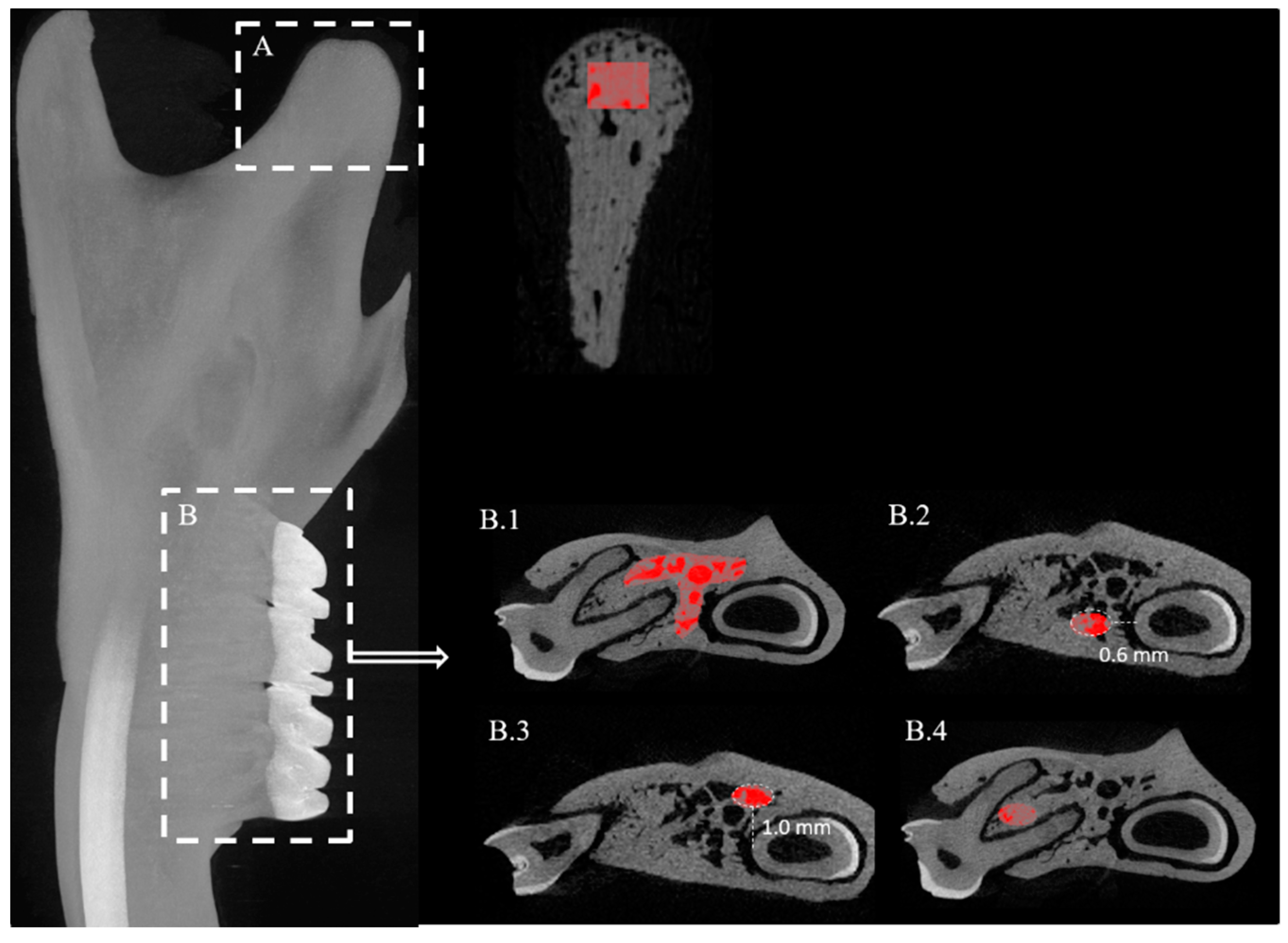
4.5. Analysis of the Mandible
4.6. Statistical Analysis
5. Conclusions
- The trabecular bone volume of the maxilla in osteoporotic rats decreases compared to control animals. Bisphosphonate treatment is able to prevent the bone loss due to ovariectomy by increasing the overall bone mass.
- The bone micro-architecture of the maxillary tuber is not affected in case of ovariectomy-induced osteoporosis.
- Deterioration of the trabecular bone morphology in response to ovariectomy can also been discerned in the mandible, in particular in the buccal area of M1 and surrounding M3.
- The mandibular condyle micro-structure is definitely affected by both ovariectomy as well as bisphosphonate treatment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALN | alendronate |
| BMD | bone mineral density |
| BV/TV | bone volume/tissue volume |
| InterRad | inter-radicular |
| M1 | first molar |
| M2 | second molar |
| M3 | third molar |
| MRONJ | medication-related osteonecrosis of the jaw |
| OVX | ovariectomized |
| ROI | region of interest |
| shOVX | sham- ovariectomized |
| SMI | structure model index |
| Tb.N | trabecular number |
| Tb.Pf | trabecular pattern factor |
| Tb.Sp | trabecular spacing |
| Tb.Th | trabecular thickness |
| Tot.Po | total porosity |
| VOI | volume of interest |
References
- McGrath, C.; Bedi, R. The importance of oral health to older people’s quality of life. Gerodontology 1999, 16, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Howson, C.P. Perspectives and needs for health in the 21st century: 20th-century paradigms in 21st-century science. J. Hum. Virol. 2000, 3, 94–103. [Google Scholar]
- Banu, J.; Bhattacharya, A.; Rahman, M.; Kang, J.X.; Fernandes, G. Endogenously produced n-3 fatty acids protect against ovariectomy induced bone loss in fat-1 transgenic mice. J. Bone Min. Metab. 2010, 28, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Pytlik, M.; Folwarczna, J.; Janiec, W. Effects of doxycycline on mechanical properties of bones in rats with ovariecto-my-induced osteopenia. Calcif. Tissue Int. 2004, 75, 225–230. [Google Scholar] [CrossRef]
- Wronski, T.J.; Pun, S.; Liang, H. Effects of age, estrogen depletion, and parathyroid hormone treatment on vertebral can-cellous wall width in female rats. Bone 1999, 25, 465–468. [Google Scholar] [CrossRef]
- Fox, J.; Miller, M.A.; Recker, R.R.; Turner, C.H.; Smith, S.Y. Effects of treatment of ovariectomized adult rhesus monkeys with parathyroid hormone 1-84 for 16 months on trabecular and cortical bone structure and biomechanical properties of the proximal femur. Calcif. Tissue Int. 2007, 81, 53–63. [Google Scholar] [CrossRef]
- Cheng, M.Z.; Zaman, G.; Rawlinson, S.C.; Pitsillides, A.A.; Suswillo, R.F.; Lanyon, L.E. Enhancement by sex hormones of the osteoregulatory effects of mechanical loading and prostaglandins in explants of rat ulnae. J. Bone Min. Res. 1997, 12, 1424–1430. [Google Scholar] [CrossRef]
- Ma, Z.; Li, S.; Sun, Y. Effect of enhanced masticatory force on OPG, RANKL and MGF in alveolar bone of ovariectomized rats. J. Appl. Oral Sci. 2020, 28, e20190409. [Google Scholar] [CrossRef] [PubMed]
- Alam, T.; AlShahrani, I.; Assiri, K.I.; Almoammar, S.; Togoo, R.A.; Luqman, M. Evaluation of clinical and radiographic parameters as dental indicators for postmenopausal osteoporosis. Oral Health Prev. Dent. 2020, 18, 499–504. [Google Scholar]
- Kribbs, P.J.; Chesnut, C.H.; Ott, S.M.; Kilcoyne, R.F. Relationships between mandibular and skeletal bone in an osteoporotic population. J. Prosthet. Dent. 1989, 62, 703–707. [Google Scholar] [CrossRef]
- Wactawski-Wende, J.; Grossi, S.G.; Trevisan, M.; Genco, R.J.; Tezal, M.; Dunford, R.G.; Ho, A.W.; Hausmann, E.; Hreshchyshyn, M.M. The role of osteopenia in oral bone loss and periodontal disease. J. Periodontol. 1996, 67, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Hildebolt, C.F. Osteoporosis and oral bone loss. Dentomaxillofac. Radiol. 1997, 26, 3–15. [Google Scholar] [CrossRef]
- Jeffcoat, M.K. Osteoporosis: A possible modifying factor in oral bone loss. Ann. Periodontol. 1998, 3, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoat, M.K.; Lewis, C.E.; Reddy, M.S.; Wang, C.Y.; Redford, M. Post-menopausal bone loss and its relationship to oral bone loss. Periodontol. 2000 2000, 23, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Khojastehpour, L.; Mogharrabi, S.; Dabbaghmanesh, M.H.; Nasrabadi, N.I. Comparison of the mandibular bone densitometry measurement between normal, osteopenic and osteoporotic postmenopausal women. J. Dent. 2013, 10, 203–209. [Google Scholar]
- Kribbs, P.J. Comparison of mandibular bone in normal and osteoporotic women. J. Prosthet. Dent. 1990, 63, 218–222. [Google Scholar] [CrossRef]
- Lee, B.D.; White, S.C. Age and trabecular features of alveolar bone associated with osteoporosis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 92–98. [Google Scholar] [CrossRef]
- Nakamoto, T.; Taguchi, A.; Ohtsuka, M.; Suei, Y.; Fujita, M.; Tanimoto, K.; Tsuda, M.; Sanada, M.; Ohama, K.; Takahashi, J.; et al. Dental panoramic radiograph as a tool to detect postmenopausal women with low bone mineral density: Untrained general dental practitioners’ diagnostic performance. Osteoporos. Int. 2003, 14, 659–664. [Google Scholar]
- Takaishi, Y.; Okamoto, Y.; Ikeo, T.; Morii, H.; Takeda, M.; Hide, K.; Arai, T.; Nonaka, K. Correlations between periodontitis and loss of mandibular bone in relation to systemic bone changes in postmenopausal Japanese women. Osteoporos. Int. 2005, 16, 1875–1882. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Han, S.S.; Lee, C.; Kim, Y.H.; Battulga, B. Microarchitectural changes in the mandibles of ovariectomized rats: A systematic review and meta-analysis. BMC Oral Health 2019, 19, 128. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Gao, K.; Lin, H.; Zhang, Y.; Li, B. Relative skeletal effects in different sites of the mandible with the proximal tibia during ovariectomy and the subsequent estrogen treatment. J. Oral Implant. 2015, 41, 386–390. [Google Scholar] [CrossRef]
- Liu, Z.; Yan, C.; Kang, C.; Zhang, B.; Li, Y. Distributional variations in trabecular architecture of the mandibular bone: An in vivo micro-CT analysis in rats. PLoS ONE 2015, 10, e0116194. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.L.; Li, C.L.; Lu, W.W.; Cai, W.X.; Zheng, L.W. Skeletal site-specific response to ovariectomy in a rat model: Change in bone density and microarchitecture. Clin. Oral Implant. Res. 2015, 26, 392–398. [Google Scholar] [CrossRef]
- Ishihara, A.; Sasaki, T.; Debari, K.; Furuya, R.; Kawawa, T.; Ramamurthy, N.S.; Golub, L.M. Effects of ovariectomy on bone morphology in maxillae of mature rats. J. Electron. Microsc. 1999, 48, 465–469. [Google Scholar] [CrossRef]
- Tanaka, M.; Ejiri, S.; Toyooka, E.; Kohno, S.; Ozawa, H. Effects of ovariectomy on trabecular structures of rat alveolar bone. J Periodontal. Res. 2002, 37, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Ejiri, S.; Tanaka, M.; Watanabe, N.; Anwar, R.B.; Yamashita, E.; Yamada, K.; Ikegame, M. Estrogen deficiency and its effect on the jaw bones. J. Bone Min. Metab. 2008, 26, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Toyooka, E.; Kohno, S.; Ozawa, H.; Ejiri, S. Long-term changes in trabecular structure of aged rat alveolar bone after ovariectomy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Moriya, Y.; Ito, K.; Murai, S. Effects of experimental osteoporosis on alveolar bone loss in rats. J. Oral Sci. 1998, 40, 171–175. [Google Scholar] [CrossRef]
- Nijenhuis, T.; van der Eerden, B.C.; Hoenderop, J.G.; Weinans, H.; van Leeuwen, J.P.; Bindels, R.J. Bone resorption inhibitor alendronate normalizes the reduced bone thickness of TRPV5(−/−) mice. J Bone Min. Res. 2008, 23, 1815–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxillofac. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef]
- Wang, H.L.; Weber, D.; McCauley, L.K. Effect of long-term oral bisphosphonates on implant wound healing: Literature review and a case report. J. Periodontol. 2007, 78, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhou, S.; Qu, R.; Yang, Y.; Gong, X.; Hong, Y.; Jin, A.; Huang, X.; Dai, Q.; Jiang, L. Icariin prevents oestrogen deficiency-induced alveolar bone loss through promoting osteogenesis via STAT3. Cell Prolif. 2020, 53, e12743. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Cheng, L.; Zhang, B.; Wang, N.; Wang, F. Tanshinone prevents alveolar bone loss in ovariectomized osteoporosis rats by up-regulating phosphoglycerate dehydrogenase. Toxicol. Appl. Pharm. 2019, 376, 9–16. [Google Scholar] [CrossRef]
- Romualdo, P.C.; Cunha, N.B.F.F.; Leoni, G.B.; Sousa-Neto, M.D.; Consolaro, A.; de Queiroz, A.M.; da Silva, R.A.B.; da Silva, L.A.B.; Nelson-Filho, P. The effect of ovariectomy and 2 antiresorptive therapeutic agents on bone response in rats: A 3-dimensional imaging analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 218–225. [Google Scholar] [CrossRef]
- Liu, H.; Li, W.; Liu, Y.S.; Zhou, Y.S. Bone micro-architectural analysis of mandible and tibia in ovariectomised rats: A quantitative structural comparison between undecalcified histological sections and micro-CT. Bone Jt. Res. 2016, 5, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Pham, S.M.; Crabbe, D.L. Effects of oestrogen deficiency on rat mandibular and tibial microarchitecture. Dentomaxillofac. Radiol. 2003, 32, 247–251. [Google Scholar] [CrossRef]
- Johnston, B.D.; Ward, W.E. The ovariectomized rat as a model for studying alveolar bone loss in postmenopausal women. Biomed. Res. Int. 2015, 2015, 635023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irie, K.; Sakakura, Y.; Tsuruga, E.; Hosokawa, Y.; Yajima, T. Three-dimensional changes of the mandible and alveolar bone in the ovariectomized rat examined by micro-focus computed tomography. J. Jpn. Soc. Periodontol. 2004, 46, 288–293. [Google Scholar] [CrossRef] [Green Version]
- Dai, Q.G.; Zhang, P.; Wu, Y.Q.; Ma, X.H.; Pang, J.; Jiang, L.Y.; Fang, B. Ovariectomy induces osteoporosis in the maxillary alveolar bone: An in vivo micro-CT and histomorphometric analysis in rats. Oral Dis. 2014, 20, 514–520. [Google Scholar] [CrossRef]
- Chatterjee, M.; Faot, F.; Correa, C.; Duyck, J.; Naert, I.; Vandamme, K. A robust methodology for the quantitative assessment of the rat jawbone microstructure. Int. J. Oral Sci. 2017, 9, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Thompson, D.D.; Simmons, H.A.; Pirie, C.M.; Ke, H.Z. FDA Guidelines and animal models for osteoporosis. Bone 1995, 17, 125S–133S. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Min. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.Y.; Tsai, M.T.; Wang, S.P.; Chen, Y.J.; Wu, J.; Hsu, J.T. Cortical bone morphological and trabecular bone microarchitectural changes in the mandible and femoral neck of ovariectomized rats. PLoS ONE 2016, 11, e0154367. [Google Scholar] [CrossRef] [PubMed]
- Bagi, C.M.; Berryman, E.; Moalli, M.R. Comparative bone anatomy of commonly used laboratory animals: Implications for drug discovery. Comp. Med. 2011, 61, 76–85. [Google Scholar] [PubMed]
- Barnsley, J.; Buckland, G.; Chan, P.E.; Ong, A.; Ramos, A.S.; Baxter, M.; Laskou, F.; Dennison, E.M.; Cooper, C.; Patel, H.P. Pathophysiology and treatment of osteoporosis: Challenges for clinical practice in older people. Aging Clin. Exp. Res. 2021, 33, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Lyu, H.; Jundi, B.; Xu, C.; Tedeschi, S.K.; Yoshida, K.; Zhao, S.; Nigwekar, S.U.; Leder, B.Z.; Solomon, D.H. Comparison of denosumab and bisphosphonates in patients with osteoporosis: A meta-analysis of randomized controlled trials. Nat. Rev. Endocrinol. 2021, 17, 31–46. [Google Scholar] [CrossRef]
- Estell, E.G.; Rosen, C.J. Emerging insights into the comparative effectiveness of anabolic therapies for osteoporosis. J Clin Endocrinol. Metab. 2019, 104, 1753–1765. [Google Scholar] [CrossRef]
- Beaudoin, C.; Jean, S.; Bessette, L.; Ste-Marie, L.-G.; Moore, L.; Brown, J.P. Denosumab compared to other treatments to prevent or treat osteoporosis in individuals at risk of fracture: A systematic review and meta-analysis. Osteoporos. Int. 2016, 27, 2835–2844. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Heide-Jørgensen, U.; Sørensen, H.T.; Prieto-Alhambra, D.; Ehrenstein, V. Comparison of risk of osteoporotic fracture in denosumab vs alendronate treatment within 3 years of initiation. JAMA Netw. Open 2019, 2, e192416. [Google Scholar] [CrossRef]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [Green Version]
- Gaudin, E.; Seidel, L.; Bacevic, M.; Rompen, E.; Lambert, F. Occurrence and risk indicators of medication-related osteonecrosis of the jaw after dental extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2015, 42, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Hallmer, F.; Bjørnland, T.; Andersson, G.; Becktor, J.P.; Kristoffersen, A.K.; Enersen, M. Bacterial diversity in medication-related osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 123, 436–444. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Wronski, T.J.; Cintrón, M.; Dann, L.M. Temporal relationship between bone loss and increased bone turnover in ovariec-tomized rats. Calcif. Tissue Int. 1988, 43, 179–183. [Google Scholar] [CrossRef]
- Kalu, D.N. The ovariectomized rat model of postmenopausal bone loss. Bone Min. 1991, 15, 175–191. [Google Scholar] [CrossRef]
- Hatori, K.; Camargos, G.V.; Chatterjee, M.; Faot, F.; Sasaki, K.; Duyck, J.; Vandamme, K. Single and combined effect of high-frequency loading and bisphosphonate treatment on the bone mi-cro-architecture of ovariectomized rats. Osteoporos. Int. 2015, 26, 303–313. [Google Scholar] [CrossRef]
- Matsumoto, K.; Amemiya, T.; Ito, M.; Hayashi, Y.; Watanabe, K.; Dezawa, K.; Arai, Y.; Honda, K. Newly developed mastication activity reduction procedure rapidly induces abnormal atrophic change of the mandibular condyle in young and elder experimental animal models. J. Oral Sci. 2020, 62, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Coutel, X.; Delattre, J.; Marchandise, P.; Falgayrac, G.; Béhal, H.; Kerckhofs, G.; Penel, G.; Olejnik, C. Mandibular bone is protected against microarchitectural alterations and bone marrow adipose conversion in ovariectomized rats. Bone 2019, 127, 343–352. [Google Scholar] [CrossRef]
- Esteves, C.M.; Moraes, R.M.; Gomes, F.C.; Marcondes, M.S.; Lima, G.M.; Anbinder, A.L. Ovariectomy-associated changes in interradicular septum and in tibia metaphysis in different observation periods in rats. Pathol. Res. Pract. 2015, 211, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Lee, J.H.; Han, S.S.; Kim, Y.H.; Choi, Y.J.; Jeon, K.J.; Jung, H.I. Site-specific and time-course changes of postmenopausal osteoporosis in rat mandible: Comparative study with femur. Sci. Rep. 2019, 9, 14155. [Google Scholar] [CrossRef]
- Watanabe, K.; Lewis, S.; Guo, X.; Ni, A.; Lee, B.S.; Deguchi, T.; Kim, D.G. Regional variations of jaw bone characteristics in an ovariectomized rat model. J. Mech. Behav. Biomed. Mater. 2020, 110, 103952. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Shen, X.; Wei, L.; Zhou, Q.; Gao, Y. Effects of bisphosphonates on mandibular condyle of ovariectomized osteoporotic rats using micro-ct and histomorphometric analysis. J. Oral Pathol. Med. 2017, 46, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Nanci, A. Structure of oral tissues. In Ten Cate’s Oral Histology: Development, Structure, and Function, 9th ed.; Nanci, A., Ten Cate, A.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 32–56. [Google Scholar]
- Owtad, P.; Park, J.H.; Shen, G.; Potres, Z.; Darendeliler, M.A. The biology of TMJ growth modification: A review. J. Dent. Res. 2013, 92, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Jung, S.Y.; Kang, J.H.; Kim, H.J.; Ko, H.M.; Jung, J.Y.; Koh, J.T.; Kim, W.J.; Kim, S.M.; Lee, E.J.; et al. Effects of bisphosphonate on the endochondral bone formation of the mandibular condyle. Anat. Histol. Embryol. 2009, 38, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Boyd, S.K.; Davison, P.; Müller, R.; Gasser, J.A. Monitoring individual morphological changes over time in ovariectomized rats by in vivo micro-computed tomography. Bone 2006, 39, 854–862. [Google Scholar] [CrossRef]
- Camargos, G.V.; Bhattacharya, P.; van Lenthe, G.H.; Del Bel Cury, A.A.; Naert, I.; Duyck, J.; Vandamme, K. Mechanical competence of ovariectomy-induced compromised bone after single or combined treatment with high-frequency loading and bisphosphonates. Sci. Rep. 2015, 5, 10795. [Google Scholar] [CrossRef] [Green Version]
- Azuma, Y.; Sato, H.; Oue, Y.; Okabe, K.; Ohta, T.; Tsuchimoto, M.; Kiyoki, M. Alendronate distributed on bone surfaces inhibits osteoclastic bone resorption in vitro and in experimental hypercalcemia models. Bone 1995, 16, 235–245. [Google Scholar] [CrossRef]
- Evans, K.D.; Lau, S.T.; Oberbauer, A.M.; Martin, R.B. Alendronate affects long bone length and growth plate morphology in the oim mouse model for Osteogenesis Imperfecta. Bone 2003, 32, 268–274. [Google Scholar] [CrossRef]
- Kimura, M.; Miyazawa, K.; Tabuchi, M.; Maeda, H.; Kameyama, Y.; Goto, S. Bisphosphonate treatment increases the size of the mandibular condyle and normalizes growth of the mandibular ramus in osteoprotegerin-deficient mice. Calcif. Tissue Int. 2008, 82, 137–147. [Google Scholar] [CrossRef]
- Gomes, C.C.; Freitas, D.Q.; Medeiros Araújo, A.M.; Ramírez-Sotelo, L.R.; Yamamoto-Silva, F.P.; de Freitas Silva, B.S.; de Melo Távora, D.; Almeida, S.M. Effect of Alendronate on Bone Microarchitecture in Irradiated Rats with Osteoporosis: Micro-CT and Histomorphometric Analysis. J. Oral Maxillofac. Surg. 2018, 76, 972–981. [Google Scholar] [CrossRef]
- Mavropoulos, A.; Rizzoli, R.; Ammann, P. Different responsiveness of alveolar and tibial bone to bone loss stimuli. J. Bone Min. Res. 2007, 22, 403–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prado, R.F.; Silveira, V.Á.; Rocha, R.F.; Vasconcellos, L.M.; Carvalho, Y.R. Effects of experimental osteoporosis and low calcium intake on postextraction sockets of rats. Int. J Exp. Pathol. 2012, 93, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mavropoulos, A.; Kiliaridis, S.; Rizzoli, R.; Ammann, P. Normal masticatory function partially protects the rat mandibular bone from estrogen-deficiency induced osteoporosis. J. Biomech. 2014, 47, 2666–2671. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | ROI | shOVX (n = 16) | OVX (n = 15) | OVX-ALN (n = 16) |
|---|---|---|---|---|
| BV/TV | M1 | 21.41 ± 0.75 | 20.56 ± 1.00 | 21.18 ± 0.66 |
| M1. Lingual | 46.87 ± 1.51 | 44.45 ± 2.54 | 44.65 ± 2.07 | |
| M1. Buccal | 42.76 ± 2.34 # | 32.31 ± 2.54 # | 37.46 ± 2.5 | |
| M2 | 18.11 ± 0.73 | 17.73 ± 0.95 | 20.73 ± 0.84 | |
| M2. InterRad | 82.02 ± 1.90 | 79.90 ± 2.70 | 80.12 ± 2.3 | |
| M3. InterRad | 81.40 ± 2.46 | 70.18 ± 5.57 | 81.37 ± 3.94 | |
| Tb.Th | M1 | 0.11 ± 0.003 | 0.10 ± 0.003 | 0.10 ± 0.002 |
| M1. Lingual | 0.14 ± 0.006 | 0.13 ± 0.006 | 0.13 ± 0.005 | |
| M1. Buccal | 0.14 ± 0.007 | 0.11 ± 0.007 | 0.11 ± 0.007 | |
| M2 | 0.10 ± 0.003 | 0.11 ± 0.003 | 0.11 ± 0.003 | |
| M2. InterRad | 0.11 ± 0.003 | 0.11 ± 0.003 | 0.10 ± 0.004 | |
| M3. InterRad | 0.10 ± 0.004 | 0.09 ± 0.006 | 0.10 ± 0.004 | |
| Tb.Sp | M1 | 0.30 ± 0.002 | 0.29 ± 0.004 | 0.3 ± 0.002 |
| M1. Lingual | 0.15 ± 0.005 | 0.15 ± 0.007 | 0.15 ± 0.007 | |
| M1. Buccal | 0.15 ± 0.006 * | 0.18 ± 0.009 * | 0.16 ± 0.009 | |
| M2 | 0.30 ± 0.005 | 0.31 ± 0.003 | 0.32 ± 0.010 | |
| M2. InterRad | 0.06 ± 0.005 | 0.06 ± 0.006 | 0.06 ± 0.007 | |
| M3. InterRad | 0.05 ± 0.003 | 0.07 ± 0.009 | 0.06 ± 0.006 | |
| Tb.N | M1 | 1.96 ± 0.06 | 2.00 ± 0.09 | 2.13 ± 0.07 |
| M1. Lingual | 3.33 ± 0.11 | 3.40 ± 0.16 | 3.30 ± 0.19 | |
| M1. Buccal | 3.06 ± 0.08 | 2.78 ± 0.13 * | 3.32 ± 0.19 * | |
| M2 | 1.71 ± 0.08 | 1.6 ± 0.07 | 1.92 ± 0.12 | |
| M2. InterRad | 7.24 ± 0.24 | 7.36 ± 0.25 | 7.87 ± 0.36 | |
| M3. InterRad | 7.91 ± 0.20 | 7.02 ± 0.35 | 7.53 ± 0.25 | |
| Tb.Pf | M1 | −9.33 ± 1.03 | −11.32 ± 1.64 | −13.08 ± 2.7 |
| M1. Lingual | −4.35 ± 0.97 | −5.70 ± 2.31 | −5.07 ± 2.17 | |
| M1. Buccal | −2.64 ± 1.15 | 0.36 ± 1.67 | −4.20 ± 2.21 | |
| M2 | −7.58 ± 1.34 | −7.68 ± 1.47 | −11.4 ± 2.04 | |
| M2. InterRad | −8.64 ± 2.00 | −8.76 ± 2.51 | −11.7 ± 3.06 | |
| M3. InterRad | −4.72 ± 1.82 # | 4.04 ± 2.81 # | 1.03 ± 1.98 | |
| SMI | M1 | −0.29 ± 0.15 | −0.36 ± 0.19 | −0.79 ± 0.34 |
| M1. Lingual | −0.39 ± 0.24 | −0.41 ± 0.41 | −0.51 ± 0.46 | |
| M1. Buccal | −0.09 ± 0.21 | 0.44 ± 0.26 | −0.34 ± 0.35 | |
| M2 | −0.05 ± 0.14 | −0.15 ± 0.21 | −0.63 ± 0.26 | |
| M2. InterRad | −0.10 ± 0.18 | −0.30 ± 0.23 | −0.30 ± 0.27 | |
| M3. InterRad | 0.32 ± 0.16 # | 1.10 ± 0.19 # | 0.79 ± 0.17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatterjee, M.; Faot, F.; Correa, C.; Kerckhofs, J.; Vandamme, K. Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis. Int. J. Mol. Sci. 2021, 22, 6559. https://doi.org/10.3390/ijms22126559
Chatterjee M, Faot F, Correa C, Kerckhofs J, Vandamme K. Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis. International Journal of Molecular Sciences. 2021; 22(12):6559. https://doi.org/10.3390/ijms22126559
Chicago/Turabian StyleChatterjee, Marissa, Fernanda Faot, Cassia Correa, Jente Kerckhofs, and Katleen Vandamme. 2021. "Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis" International Journal of Molecular Sciences 22, no. 12: 6559. https://doi.org/10.3390/ijms22126559
APA StyleChatterjee, M., Faot, F., Correa, C., Kerckhofs, J., & Vandamme, K. (2021). Is the Jaw Bone Micro-Structure Altered in Response to Osteoporosis and Bisphosphonate Treatment? A Micro-CT Analysis. International Journal of Molecular Sciences, 22(12), 6559. https://doi.org/10.3390/ijms22126559