
Bisphosphonate-Based Conjugates and Derivatives as Potential Therapeutic Agents in Osteoporosis, Bone Cancer and Metastatic Bone Cancer


Abstract
:1. Introduction
- ✓
- In corticosteroid and postmenopausal induced osteoporosis, the most utilized BPs in these cases, which block the presence of pathological fractures, is alendronate [12].
- ✓
- They are also utilized to enhance bone morphology and decrease pain in Paget’s disease [13].
- ✓
- In hypercalcaemia of malignancy, its role is in trying to check hypercalcaemia, reducing pain, and preventing the development of osteolitic lesions and fractures [14].
- ✓
- ✓
2. Osteoporosis
Bisphosphonates Conjugates for the Treatment of Osteoporosis
3. Bone Cancer
BP Conjugates as Bone-Targeting Compounds
4. Metastatic Cancer That Spreads to the Bones
4.1. Breast Cancer
4.1.1. In Vitro Studies of BPs in Breast Cancer
4.1.2. Bisphosphonates Conjugates for the Treatment of Breast Cancer
4.2. Prostate Cancer
4.2.1. In Vitro Studies of BPs in Prostate Cancer
4.2.2. Bisphosphonates Conjugates for the Treatment of Prostate Cancer
4.3. Lung Cancer
4.3.1. In Vitro Studies of BPs in Lung Cancer
4.3.2. Bisphosphonates Conjugates for the Treatment of Lung Cancer
5. Conclusion and Future Perspective
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kuźnik, A.; Październiok-Holewa, A.; Jewula, P.; Kuźnik, N. Bisphosphonates—much more than only drugs for bone diseases. Eur. J. Pharmacol. 2020, 866, 172773. [Google Scholar] [CrossRef]
- Toussaint, N.D.; Elder, G.J.; Kerr, P.G. Bisphosphonates in chronic kidney disease; balancing potential benefits and adverse effects on bone and soft tissue. Clin. J. Am. Soc. Nephrol. 2008, 4, 221–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, R.G.G. Bisphosphonates: From bench to bedside. Ann. N. Y. Acad. Sci. 2006, 1068, 367–401. [Google Scholar] [CrossRef] [Green Version]
- Roelofs, A.J.; Thompson, K.; Ebetino, F.H.; Rogers, M.J.; Coxon, F.P. Bisphosphonates: Molecular mechanisms of action and effects on bone cells, monocytes and macrophages. Curr. Pharm. Design. 2010, 16, 2950–2960. [Google Scholar] [CrossRef] [PubMed]
- Heymann, D.; Ory, B.; Gouin, F.; Green, J.R.; Rédini, F. Bisphosphonates: New therapeutic agents for the treatment of bone tumors. Trends Mol. Med. 2004, 10, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Fernández, N.P.; Fresco, R.E.; Urizar, J.A. Bisphosphonates and oral pathology I. Gen. Prev. Asp. 2006, 11, 396–400. [Google Scholar]
- Milner, R.J.; Farese, J.; Henry, C.J.; Selting, K.; Fan, T.M.; de Lorimier, L.P. Bisphosphonates and cancer. J. Vet. Intern. Med. 2004, 18, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Bigi, A.; Boanini, E. Calcium phosphates as delivery systems for bisphosphonates. J. Funct. Biomater. 2018, 9, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocijan, R.; Klaushofer, K.; Misof, B.M. Osteoporosis therapeutics 2020. Snake Venoms 2020, 397–422. [Google Scholar] [CrossRef]
- Green, J.R.; Rogers, M.J. Pharmacologic profile of zoledronic acid: A highly potent inhibitor of bone resorption. Drug Dev. Res. 2002, 55, 210–224. [Google Scholar] [CrossRef]
- Lenz, J.-H.; Steiner-Krammer, B.; Schmidt, W.; Fietkau, R.; Mueller, P.C.; Gundlach, K.K. Does avascular necrosis of the jaws in cancer patients only occur following treatment with bisphosphonates? J. Cranio-Maxillofac. Surg. 2005, 33, 395–403. [Google Scholar] [CrossRef]
- Bagger, Y.Z.; Tankó, L.B.; Alexandersen, P.; Ravn, P.; Christiansen, C. Alendronate has a residual effect on bone mass in postmenopausal Danish women up to 7 years after treatment withdrawal. Bone 2003, 33, 301–307. [Google Scholar] [CrossRef]
- Reid, I.R.; Miller, P.; Lyles, K.; Fraser, W.; Brown, J.P.; Saidi, Y.; Mesenbrink, P.; Su, G.; Pak, J.; Zelenakas, K.; et al. Comparison of a single infusion of zoledronic acid with risedronate for paget’s disease. N. Engl. J. Med. 2005, 353, 898–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zagzag, J.; Hu, M.I.; Fisher, S.B.; Perrier, N.D. Hypercalcemia and cancer: Differential diagnosis and treatment. CA A Cancer J. Clin. 2018, 68, 377–386. [Google Scholar] [CrossRef] [Green Version]
- Michigami, T.; Hiraga, T.; Williams, P.J.; Niewolna, M.; Nishimura, R.; Mundy, G.R.; Yoneda, T. The effect of the bisphos-phonate ibandronate on breast cancer metastasis to visceral organs. Breast Cancer Res. Treat. 2002, 75, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Bauss, F.; Body, J.-J. Ibandronate in metastatic bone disease: A review of preclinical data. Anti-Cancer Drugs 2005, 16, 107–118. [Google Scholar] [CrossRef]
- Berenson, J.R.; Rosen, L.S.; Howell, A.; Porter, L.; Coleman, R.E.; Morley, W.; Dreicer, R.; Kuross, S.A.; Lipton, A.; Seaman, J.J. Zoledronic acid reduces skeletal-related events in patients with osteolytic metastases: A double-blind, randomized dose–response study. Cancer 2001, 91, 1191–1200. [Google Scholar] [CrossRef]
- Tamburrelli, F.C.; Proietti, L.; Scaramuzzo, L.; De Stefano, V.; Logroscino, C.A. Bisphosphonate therapy in multiple myeloma in preventing vertebral collapses: Preliminary report. Eur. Spine J. 2012, 21, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamsen, B. Adverse effects of bisphosphonates. Calcif. Tissue Int. 2010, 86, 421–435. [Google Scholar] [CrossRef]
- Gonen, Z.B.; Colpak, H.A.; Onger, M.E. Effects of bisphosphonate treatment on mandibular condyle tissues of temporo-mandibular joint: A stereological study. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Reyes, C.; Hitz, M.; Prieto-Alhambra, D.; Abrahamsen, B. Risks and benefits of bisphosphonate therapies. J. Cell. Biochem. 2016, 117, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, K.; Bansal, P.; Goyal, A.; Roane, D. Bisphosphonate. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470248/ (accessed on 10 April 2021).
- Li, W.; Chen, W.; Lin, Y. The efficacy of parathyroid hormone analogues in combination with bisphosphonates for the treatment of osteoporosis: A meta-analysis of randomized controlled trials. Medicine 2015, 94, e1156. [Google Scholar] [CrossRef] [PubMed]
- Kasugai, S.; Fujisawa, R.; Waki, Y.; Miyamoto, K.-I.; Ohya, K. Selective drug delivery system to bone: Small peptide (Asp)6 conjugation. J. Bone Miner. Res. 2010, 15, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Anastasilakis, A.D.; Polyzos, S.A.; Makras, P. Therapy of endocrine disease: Denosumab vs bisphosphonates for the treat-ment of postmenopausal osteoporosis. Eur. J. Endocrinol. 2018, 179, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Fleisch, H. Bisphosphonates in osteoporosis. Eur. Spine J. 2003, 12, 142–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ossipov, D.A. Bisphosphonate-modified biomaterials for drug delivery and bone tissue engineering. Expert Opin. Drug Deliv. 2015, 12, 1443–1458. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.G.; Watts, N.B.; Ebetino, F.H.; Rogers, M.J. Mechanisms of action of bisphosphonates: Similarities and differences and their potential influence on clinical efficacy. Osteoporos Int. 2008, 19, 733–759. [Google Scholar] [CrossRef]
- Kulak, C.A.; Borba, V.Z.; Kulak Júnior, J.; Shane, E. Transplantation osteoporosis. Arq. Bras. Endocrinol. Metabol. 2006, 50, 783–792. [Google Scholar] [CrossRef] [Green Version]
- Greenblatt, M.B.; Tsai, J.N.; Wein, M.N. Bone turnover markers in the diagnosis and monitoring of metabolic bone disease. Clin. Chem. 2017, 63, 464–474. [Google Scholar] [CrossRef] [Green Version]
- Kuhlmann, L.; Poulsen, J.L.; Køhler, M.; Rasmussen, H.H.; Vestergaard, P.; Drewes, A.M.; Olesen, S.S. Osteoporosis in chronic pancreatitis outpatients associates with several risk factors. Pancreas 2018, 19, 183–189. [Google Scholar]
- Chmielewska, E.; Kafarski, P. Physiologic activity of bisphosphonates—Recent advances. Open Pharm. Sci. J. 2016, 3, 56–78. [Google Scholar] [CrossRef] [Green Version]
- Steinmeyer, A.; Schwarz, K.; Haberey, M.; Langer, G.; Wiesinger, H. Synthesis and biological activities of a new series of secosteroids: Vitamin D phosphonate hybrids. Steroids 2001, 66, 257–266. [Google Scholar] [CrossRef]
- Tsushima, N.; Yabuki, M.; Harada, H.; Katsumata, T.; Kanamaru, H.; Nakatsuka, I.; Yamamoto, M.; Nakatsuka, M. Tissue distribution and pharmacological potential of SM-16896, a novel oestrogen-bisphosphonate hybrid compound. J. Pharm. Pharmacol. 2000, 52, 27–37. [Google Scholar] [CrossRef]
- Xie, Z.A.; Liu, G.; Tang, P.; Sun, X.; Chen, S.; Qin, A.; Zhu, P.; Zhang, J.; Fan, S. Bone-targeted methotrexate–alendronate conjugate inhibits osteoclastogenesis in vitro and prevents bone loss and inflammation of collagen-induced arthritis in vivo. Drug Deliv. 2018, 25, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Motaleb, H.; Ibrahim, I.T.; El-Tawoosy, M.; Mohamed, M. Synthesis, preclinical, and pharmacokinetic evaluation of a new zoledronate derivative as a promising antiosteoporotic candidate using radiolabeling technique. J. Label. Compd. Radiopharm. 2017, 60, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Farrell, K.B.; Karpeisky, A.; Thamm, D.H.; Zinnen, S. Bisphosphonate conjugation for bone specific drug targeting. Bone Rep. 2018, 9, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Svensson, E.; Christiansen, C.F.; Ulrichsen, S.P.; Rørth, M.R.; Sørensen, H.T. Survival after bone metastasis by primary cancer type: A Danish population-based cohort study. BMJ Open 2017, 7, e016022. [Google Scholar] [CrossRef] [PubMed]
- Kanakis, I.; Kousidou, O.C.; Karamanos, N.K. In vitro and in vivo antiresorptive effects of bisphosphonates in metastatic bone disease. Vivo 2005, 19, 311–318. [Google Scholar]
- Shibata, H.; Kato, S.; Sekine, I.; Abe, K.; Araki, N.; Iguchi, H.; Izumi, T.; Inaba, Y.; Osaka, I.; Kawai, A.; et al. Diagnosis and treatment of bone metastasis: Comprehensive guideline of the Japanese society of medical oncology, Japanese orthopedic association, Japanese urological association, and Japanese society for radiation oncology. ESMO Open 2016, 1, e000037. [Google Scholar] [CrossRef] [PubMed]
- Rudnick-Glick, S.; Tal, N.; Corem-Slakman, E.; Grinberg, I.; Gluz, E.; Margel, S. Synthesis and Characterization of Bisphos-phonate Nano/Micro-Particles for Bone Cancer Targeting and Therapy. 2017. Available online: http://uilis.unsyiah.ac.id/oer/files/original/063e69a06ce12330abacb6f43ad122e6.pdf (accessed on 1 October 2020).
- Marques, C.; Ferreira, J.M.; Andronescu, E.; Ficai, D.; Sonmez, M.; Ficai, A. Multifunctional materials for bone cancer treat-ment. Int. J. Nanomed. 2014, 9, 2713. [Google Scholar]
- Buchbender, C.; Heusner, T.A.; Lauenstein, T.C.; Bockisch, A.; Antoch, G. Oncologic PET/MRI, part 1: Tumors of the brain, head and neck, chest, abdomen, and pelvis. J. Nucl. Med. 2012, 53, 928–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.H.; Jin, X.; Malladi, S.; Zou, Y.; Wen, Y.H.; Brogi, E.; Smid, M.; Foekens, J.A.; Massagué, J. Selection of bone me-tastasis seeds by mesenchymal signals in the primary tumor stroma. Cell 2013, 154, 1060–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ell, B.; Mercatali, L.; Ibrahim, T.; Campbell, N.; Schwarzenbach, H.; Pantel, K.; Amadori, D.; Kang, Y. Tumor-induced osteo-clast miRNA changes as regulators and biomarkers of osteolytic bone metastasis. Cancer Cell 2013, 24, 542–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, S.J.; Prakash, P.; Salgaonkar, V.; Jones, P.D.; Cam, R.N.; Han, M.; Rieke, V.; Burdette, E.C.; Diederich, C.J. Interstitial ultrasound ablation of tumors within or adjacent to bone: Contributions of preferential heating at the bone surface. In Energy-based Treatment of Tissue and Assessment VII. Int. Soc. Opt. Photonics 2013, 8584, 85840. [Google Scholar]
- Coleman, R. Treatment of metastatic bone disease and the emerging role of radium-223. Semin. Nucl. Med. 2016, 46, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, H.-J.; Kim, K.R.; Lee, S.K.; Lee, C.K.; Park, K.-K.; Chung, W.-Y. Betulinic acid, a bioactive pentacyclic triterpenoid, inhibits skeletal-related events induced by breast cancer bone metastases and treatment. Toxicol. Appl. Pharmacol. 2014, 275, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Lee, O.L.; Horvath, N.; Lee, C.; Joshua, D.; Ho, J.; Szer, J.; Quach, H.; Spencer, A.; Harrison, S.; Mollee, P.; et al. Bisphosphonate guidelines for treatment and prevention of myeloma bone disease. Intern. Med. J. 2017, 47, 938–951. [Google Scholar] [CrossRef] [Green Version]
- Weinreich, J.; Schott, T.C.; Koenigsrainer, I.; Kueper, M.; Koenigsrainer, A.; Schott, H. Cytostatic activity of a 5-Fluoro-2′-deoxyuridine–Alendronate conjugate against gastric adenocarcinoma and non-malignant intestinal and fi-broblast cell lines. AntiCancer Res. 2012, 32, 4299–4305. [Google Scholar]
- Erez, R.; Ebner, S.; Attali, B.; Shabat, D. Chemotherapeutic bone-targeted bisphosphonate prodrugs with hydrolytic mode of activation. Bioorganic Med. Chem. Lett. 2008, 18, 816–820. [Google Scholar] [CrossRef]
- Agyin, J.K.; Santhamma, B.; Roy, S.S. Design, synthesis, and biological evaluation of bone-targeted proteasome inhibitors for multiple myeloma. Bioorganic Med. Chem. Lett. 2013, 23, 6455–6458. [Google Scholar] [CrossRef] [Green Version]
- Nakatake, H.; Ekimoto, H.; Aso, M.; Ogawa, A.; Yamaguchi, A.; Suemune, H. Dialkyl bisphosphonate platinum(II) complex as a potential drug for metastatic bone tumor. Chem. Pharm. Bull. 2011, 59, 710–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebetino, F.H.; Hogan, A.-M.L.; Sun, S.; Tsoumpra, M.K.; Duan, X.; Triffitt, J.T.; Kwaasi, A.A.; Dunford, J.E.; Barnett, B.L.; Oppermann, U.; et al. The relationship between the chemistry and biological activity of the bisphosphonates. Bone 2011, 49, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Kunda, U.M.R.; Hamada, F. Facile synthesis of bisphosphonates. Int. J. Soc. Mater. Eng. Resour. 2014, 20, 45–48. [Google Scholar] [CrossRef] [Green Version]
- El-Mabhouh, A.; Mercer, J.R. 188Re-labeled bisphosphonates as potential bifunctional agents for therapy in patients with bone metastases. Appl. Radiat. Isot. 2005, 62, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Reinholz, M.M.; Zinnen, S.P.; Dueck, A.C.; Dingli, D.; Reinholz, G.G.; Jonart, L.A.; Kitzmann, K.A.; Bruzek, A.K.; Negron, V.; Abdalla, A.K.; et al. A promising approach for treatment of tumor-induced bone diseases: Utilizing bisphos-phonate derivatives of nucleoside antimetabolites. Bone 2010, 47, 12–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roodman, G.D. Mechanisms of bone metastasis. N. Engl. J. Med. 2004, 350, 1655–1664. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, N.S.A.; Zarina, S.; Hashim, Z. Assessment of anticancer effect of alendronate in breast cancer: An in vitro study. J. Biotechnol. Biomed. Sci. 2019, 2, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Body, J.-J. Bisphosphonates for malignancy-related bone disease: Current status, future developments. Support. Care Cancer 2006, 14, 408–418. [Google Scholar] [CrossRef]
- Xu, X.-L.; Gou, W.-L.; Wang, A.-Y.; Wang, Y.; Guo, Q.-Y.; Lu, Q.; Lu, S.-B.; Peng, J. Basic research and clinical applications of bisphosphonates in bone disease: What have we learned over the last 40 years? J. Transl. Med. 2013, 11, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terpos, E.; Sezer, O.; Croucher, P.I.; García-Sanz, R.; Boccadoro, M.; San Miguel, J.; Ashcroft, J.; Bladé, J.; Cavo, M.; Delforge, M.; et al. The use of bisphosphonates in multiple myeloma: Recommendations of an expert panel on behalf of the European Myeloma Network. Ann. Oncol. 2009, 20, 1303–1317. [Google Scholar] [CrossRef] [PubMed]
- Licata, A.A. Discovery, clinical development, and therapeutic uses of bisphosphonates. Ann. Pharmacother. 2005, 39, 668–677. [Google Scholar] [CrossRef]
- Woodward, J.K.L.; Coleman, R.E.; Holen, I. Preclinical evidence for the effect of bisphosphonates and cytotoxic drugs on tumor cell invasion. Anti-Cancer Drugs 2005, 16, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Riebeling, C.; Forsea, A.-M.; Raisova, M.; Orfanos, C.E.; Geilen, C.C. The bisphosphonate pamidronate induces apoptosis in human melanoma cells in vitro. Br. J. Cancer 2002, 87, 366–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witters, L.M.; Crispino, J.; Fraterrigo, T.; Green, J.; Lipton, A. Effect of the combination of docetaxel, zoledronic acid, and a COX-2 inhibitor on the growth of human breast cancer cell lines. Am. J. Clin. Oncol. 2003, 26, S92–S97. [Google Scholar] [CrossRef]
- Matsumoto, S.; Kimura, S.; Segawa, H.; Kuroda, J.; Yuasa, T.; Sato, K.; Nogawa, M.; Tanaka, F.; Maekawa, T.; Wada, H. Efficacy of the third-generation bisphosphonate, zoledronic acid alone and combined with anti-cancer agents against small cell lung cancer cell lines. Lung Cancer 2005, 47, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Fournier, P.; Boissier, S.; Filleur, S.; Guglielmi, J.; Cabon, F.; Colombel, M.; Clézardin, P. Bisphosphonates inhibit angio-genesis in vitro and testosterone-stimulated vascular regrowth in the ventral prostate in castrated rats. Cancer Res. 2002, 62, 6538–6544. [Google Scholar] [PubMed]
- Nadar, R.A.; Margiotta, N.; Iafisco, M.; van den Beucken, J.J.; Boerman, O.C.; Leeuwenburgh, S.C. Bisphosphonate-functionalized imaging agents, anti-tumor agents and nanocarriers for the treatment of bone cancer. Adv. Healthc. Mater. 2017, 6, 1601119. [Google Scholar] [CrossRef]
- Ferretti, G.; Fabi, A.; Carlini, P.; Papaldo, P.; Fei, P.C.; Di Cosimo, S.; Salesi, N.; Giannarelli, D.; Alimonti, A.; Di Cocco, B.; et al. Zoledronic-acid-induced circulating level modifications of angiogenic factors, metalloproteinases and proin-flammatory cytokines in metastatic breast cancer patients. Oncology 2005, 69, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Dahut, W.L.; Gulley, J.L. The use of bisphosphonates in cancer patients. Acta Oncol. 2007, 46, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Fazil, M.; Baboota, S.; Sahni, J.K.; Ameeduzzafar, A.J. Bisphosphonates: Therapeutics potential and recent advances in drug delivery. Drug Deliv. 2014, 22, 1–9. [Google Scholar] [CrossRef]
- Whyte, M.P.; Wenkert, D.; Clements, K.L.; McAlister, W.H.; Mumm, S. Bisphosphonate-induced osteopetrosis. N. Engl. J. Med. 2003, 349, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Rosen, C.J.; Brown, S. Severe hypocalcemia after intravenous bisphosphonate therapy in occult Vitamin D deficiency. N. Engl. J. Med. 2003, 348, 1503–1504. [Google Scholar] [CrossRef]
- Pazianas, M.; Abrahamsen, B. Does bisphosphonate treatment reduce the risk of future cancer? Oncology 2018, 29, 1476–1485. [Google Scholar] [CrossRef]
- Clézardin, P.; Ebetino, F.H.; Fournier, P.G. Bisphosphonates and cancer-induced bone disease: Beyond their antiresorptive Activity. Cancer Res. 2005, 65, 4971–4974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ang, C.; Doyle, E.; Branch, A. Bisphosphonates as potential adjuvants for patients with cancers of the digestive system. World J. Gastroenterol. 2016, 22, 906. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R. Metastatic bone disease: Clinical features, pathophysiology and treatment strategies. Cancer Treat. Rev. 2001, 27, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, D.; Lichinitzer, M.; Lazarev, A.; MacLachlan, S.A.; Apffelstaedt, J.; Budde, M.; Bergstrom, B. Oral ibandronate for the treatment of metastatic bone disease in breast cancer: Efficacy and safety results from a randomized, double-blind, placebo-controlled trial. Ann. Oncol. 2004, 15, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Heeke, A.; Nunes, M.R.; Lynce, F. Bone-modifying agents in early-stage and advanced breast cancer. Curr. Breast Cancer Rep. 2018, 10, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennert, G.; Pinchev, M.; Gronich, N.; Saliba, W.; Flugelman, A.; Lavi, I.; Goldberg, H.; Fried, G.; Steiner, M.; Bitterman, A.; et al. Oral bisphosphonates and improved survival of breast cancer. Clin. Cancer Res. 2017, 23, 1684–1689. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.; Brufsky, A. Bisphosphonates in breast cancer. Int. J. Cancer 2014, 137, 753–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biskup, E.; Cai, F.; Vetter, M. Bone targeted therapies in advanced breast cancer. Swiss Med. Wkly. 2017, 147, 2526. [Google Scholar] [CrossRef]
- Vasikaran, S.D. Bisphosphonates: An overview with special reference to alendronate. Ann. Clin. Biochem. Int. J. Lab. Med. 2001, 38, 608–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adjei, I.M.; Temples, M.N.; Brown, S.B.; Sharma, B. Targeted nanomedicine to treat bone metastasis. Pharmaceutics 2018, 10, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schott, S.; Wallwiener, M.; Kootz, B.; Seeger, H.; Fehm, T.; Neubauer, H. Cytotoxicity of the new antimetabo-lite-bisphosphonate (5-FdU-alendronate) in comparison to standard therapeutics on breast and ovarian cancer cell lines in the ATP tumor chemosensitivity assay. Invest New Drugs 2012, 30, 1750–1755. [Google Scholar] [CrossRef] [PubMed]
- Schem, C.; Tower, R.J.; Kneissl, P.; Campbell, G.M.; Desel, C.; Damm, T.; Heilmann, T.; Fuchs, S.; Trauzold, A.; Glüer, C.C.; et al. Pharmacologically inactive bisphosphonates as an alternative strategy for targeting osteoclasts: In vivo assessment of 5-fluorodeoxyuridine-alendronate in a preclinical model of breast cancer bone metastases. J. Bone Miner. Res. 2016, 32, 536–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardinelli, F.; Iannucci, M.; Verratti, V.; Fusco, W.; Nicolai, M.; Tenaglia, R. Bisphosphonates treatment in metastatic prostate cancer. Eur. J. Inflamm. 2005, 3, 49–54. [Google Scholar] [CrossRef]
- Drudge-Coates, L. Skeletal complications and the use of bisphosphonates in metastatic prostate cancer. Int. J. Palliat. Nurs. 2006, 12, 462–468. [Google Scholar] [CrossRef]
- Kozyrakis, D.; Paridis, D.; Perikleous, S.; Malizos, K.; Zarkadas, A.; Tsagkalis, A. The current role of osteoclast inhibitors in patients with prostate cancer. Adv. Urol. 2018, 2018, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Saad, F. The role of bisphosphonates in the management of prostate cancer. Curr. Oncol. Rep. 2006, 8, 221–227. [Google Scholar] [CrossRef]
- Body, J.J.; von Moos, R.; Niepel, D.; Tombal, B. Hypocalcaemia in patients with prostate cancer treated with a bisphospho-nate or denosumab: Prevention supports treatment completion. BMC Urol. 2018, 18, 81. [Google Scholar] [CrossRef]
- Hayes, A.R.; Brungs, D.; Pavlakis, N. Osteoclast inhibitors to prevent bone metastases in men with high-risk, non-metastatic prostate cancer: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0191455. [Google Scholar] [CrossRef] [Green Version]
- Iranikhah, M.; Stricker, S.; Freeman, M.K. Future of bisphosphonates and denosumab for men with advanced prostate cancer. Cancer Manag. Res. 2014, 6, 217. [Google Scholar] [CrossRef] [Green Version]
- Saad, F.; Sternberg, C.N.; Mulders, P.F.; Niepel, D.; Tombal, B.F. The role of bisphosphonates or denosumab in light of the availability of new therapies for prostate cancer. Cancer Treat. Rev. 2018, 68, 25–37. [Google Scholar] [CrossRef]
- Macherey, S.; Monsef, I.; Jahn, F.; Jordan, K.; Yuen, K.K.; Heidenreich, A.; Skoetz, N. Bisphosphonates for advanced prostate cancer. Cochrane Database Syst. Rev. 2017, 12, CD006250. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.; Cook, L.M.; Lynch, C.C.; Basanta, D. An integrated computational model of the bone microenvironment in bone-metastatic prostate cancer. Cancer Res. 2014, 74, 2391–2401. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.A.; Partin, A.W. Bisphosphonates in metastatic prostate cancer. Rev. Urol. 2003, 5, 204–206. [Google Scholar] [PubMed]
- Pickering, L.M.; Mansi, J.L.; Colston, K.W. Adhesion of breast cancer cells to extracellular matrices is inhibited by zoledronic acid and enhanced by aberrant Ras signalling. Proc. Am. Soc. Clin. Oncol. 2003, 22, 4559–4567. [Google Scholar]
- Wood, J.; Bonjean, K.; Ruetz, S.; Bellahcène, A.; Devy, L.; Foidart, J.M.; Castronovo, V.; Green, J.R. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J. Pharmacol. Exp. Ther. 2002, 302, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Croucher, P.I.; De Raeve, H.; Perry, M.J.; Hijzen, A.; Shipman, C.M.; Lippitt, J.; Green, J.; Van Marck, E.; Van Camp, B.; Vanderkerken, K. Zoledronic acid treatment of 5T2MM-bearing mice inhibits the development of myeloma bone disease: Evidence for decreased osteolysis, tumor burden and angiogenesis, and increased survival. J. Bone Miner. Res. 2003, 18, 482–492. [Google Scholar] [CrossRef]
- Dieli, F.; Gebbia, N.; Poccia, F.; Caccamo, N.; Montesano, C.; Fulfaro, F.; Arcara, C.; Valerio, M.R.; Meraviglia, S.; Di Sano, C.; et al. Induction of γδ T-lymphocyte effector functions by bisphosphonate zoledronic acid in cancer patients in vivo. Blood 2003, 102, 2310–2311. [Google Scholar] [CrossRef]
- Marra, M.; Abbruzzese, A.; Addeo, R.; Prete, S.; Tassone, P.; Tonini, G.; Tagliaferri, P.; Santini, D.; Caraglia, M. Cutting the limits of aminobisphosphonates: New strategies for the potentiation of their anti-tumour effects. Curr. Cancer Drug Targets 2009, 9, 791–800. [Google Scholar] [CrossRef]
- Caraglia, M.; D’Alessandro, A.M.; Marra, M.; Giuberti, G.; Vitale, G.; Viscomi, C.; Colao, A.; Del Prete, S.; Tagliaferri, P.; Tassone, P.; et al. The farnesyl transferase inhibitor R115777 (Zarnestra®) synergistically enhances growth inhibition and apoptosis induced on epidermoid cancer cells by Zoledronic acid (Zometa®) and Pamidronate. Oncogene 2004, 23, 6900–6913. [Google Scholar] [CrossRef] [Green Version]
- De Rosa, G.; Misso, G.; Salzano, G.; Caraglia, M. Bisphosphonates and cancer: What opportunities from nanotechnology? J. Drug Deliv. 2013, 2013, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boissier, S.; Ferreras, M.; Peyruchaud, O.; Magnetto, S.; Ebetino, F.H.; Colombel, M.; Delmas, P.; Delaissé, J.M.; Clézardin, P. Bisphosphonates inhibit breast and prostate carcinoma cell invasion, an early event in the formation of bone metastases. Cancer Res. 2000, 60, 2949–2954. [Google Scholar] [PubMed]
- De Marinis, F.; Eberhardt, W.; Harper, P.G.; Sureda, B.M.; Nackaerts, K.; Soerensen, J.B.; Syrigos, K.; Trédaniel, J. Bisphos-phonate use in patients with lung cancer and bone metastases: Recommendations of a European expert panel. J. Thorac. Oncol. 2009, 4, 1280–1288. [Google Scholar] [CrossRef] [Green Version]
- Brodowicz, T.; Obyrne, K.J.; Manegold, C. Bone matters in lung cancer. Ann. Oncol. 2012, 23, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Akoury, E.; Luna, A.S.R.G.; Ahangar, P.; Gao, X.; Zolotarov, P.; Weber, M.H.; Rosenzweig, D.H. Anti-tumor effects of low dose zoledronate on lung cancer-induced spine metastasis. J. Clin. Med. 2019, 8, 1212. [Google Scholar] [CrossRef] [Green Version]
- Nakahara, Y.; Hosomi, Y.; Shibuya, M.; Mitsufuji, H.; Katagiri, M.; Naoki, K.; Soejima, K.; Nogami, N.; Nagase, S.; Nishikawa, M.; et al. Multicenter study of zoledronic acid administration in non-small-cell lung cancer patients with bone metastasis: Thoracic Oncology Research Group (TORG) 1017. Mol. Clin. Oncol. 2019, 11, 349–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirsh, V. Targeted treatments of bone metastases in patients with lung cancer. Front. Oncol. 2014, 4, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.; Cheng, R.; Zhang, Z.; Jiang, T.; Ren, S.; Ma, Z.; Zhao, S.; Zhou, C.; Zhang, J. Bisphosphonates enhance antitumor effect of EGFR-TKIs in patients with advanced EGFR mutant NSCLC and bone metastases. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Olivo, M.A.; Shah, N.A.; Pratt, G.; Risser, J.M.; Symanski, E.; Suarez-Almazor, M.E. Bisphosphonates in the treat-ment of patients with lung cancer and metastatic bone disease: A systematic review and meta-analysis. Support Care Cancer. 2012, 20, 2985–2998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yano, S.; Zhang, H.; Hanibuchi, M.; Miki, T.; Goto, H.; Uehara, H.; Sone, S. Combined therapy with a new bisphosphonate, minodronate (YM529), and chemotherapy for multiple organ metastases of small cell lung cancer cells in severe combined immunodeficient mice. Clin. Cancer Res. 2003, 9, 5380–5385. [Google Scholar] [PubMed]
- Koshimune, R.; Aoe, M.; Toyooka, S.; Hara, F.; Ouchida, M.; Tokumo, M.; Sano, Y.; Date, H.; Shimizu, N. Anti-tumor effect of bisphosphonate (YM529) on non-small cell lung cancer cell lines. BMC Cancer 2007, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Mabhouh, A.A.; Angelov, C.A.; Cavell, R.; Mercer, J.R. A 99mTc-labeled gemcitabine bisphosphonate drug conjugate as a probe to assess the potential for targeted chemotherapy of metastatic bone cancer. Nucl. Med. Biol. 2006, 33, 715–722. [Google Scholar] [CrossRef] [PubMed]
- El-Mabhouh, A.A.; Mercer, J.R. 188Re-labelled gemcitabine/bisphosphonate (Gem/BP): A multi-functional, bone-specific agent as a potential treatment for bone metastases. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
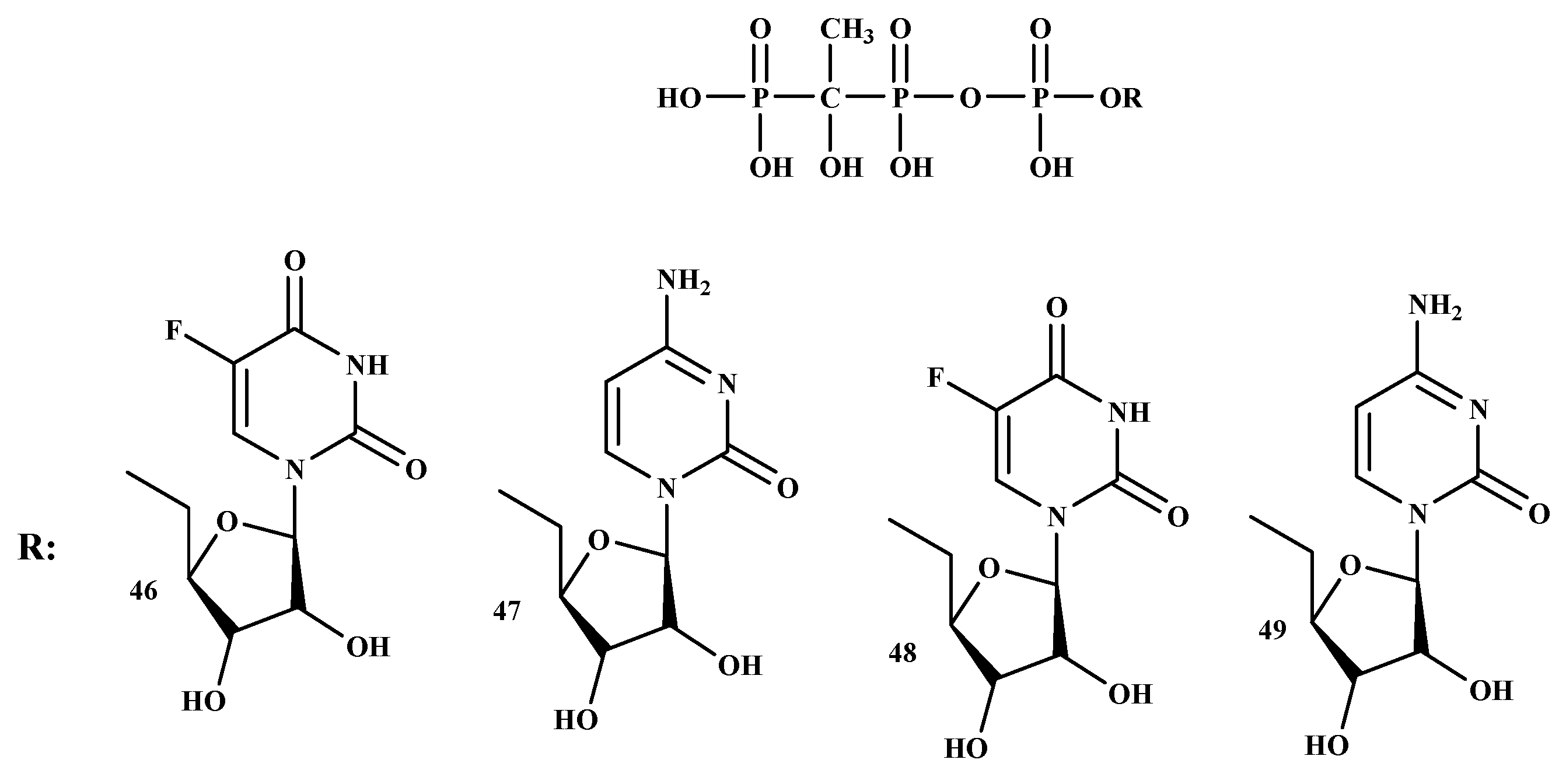
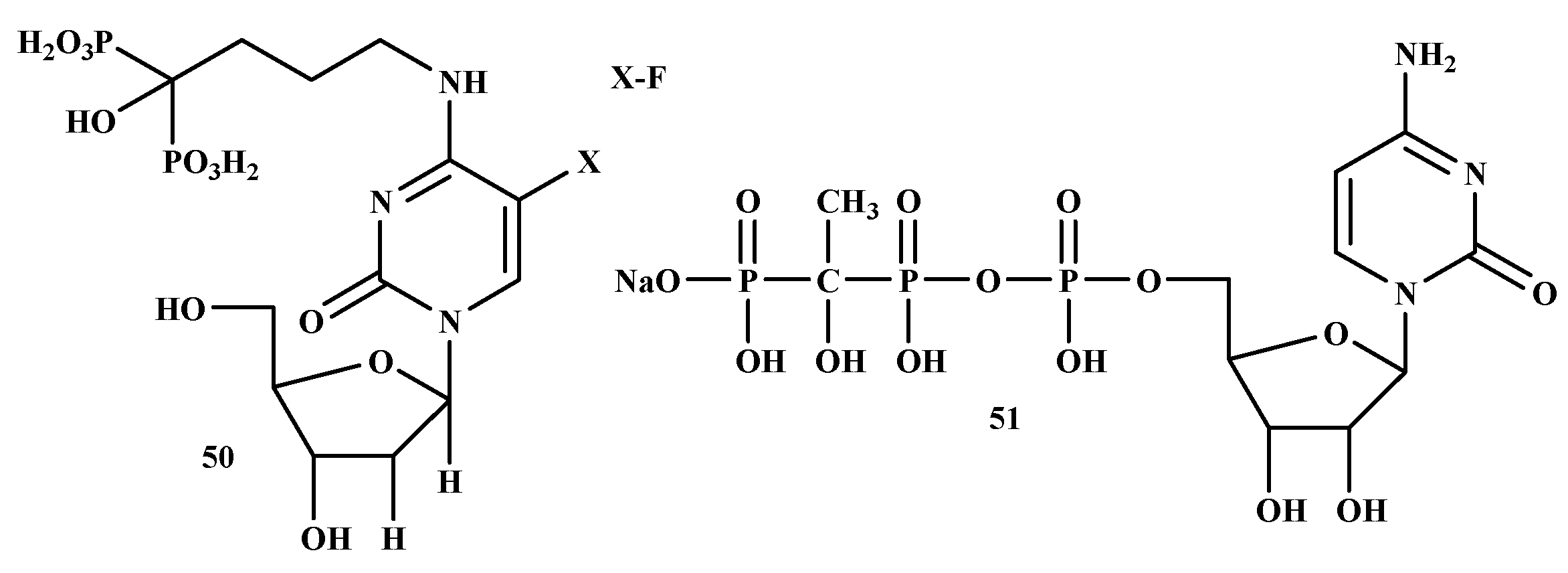
- Schott, H.; Goltz, D.; Schott, T.C.; Jauch, C.; Schwendener, R.A. N4-[Alkyl-(hydroxyphosphono) phospho-nate]-cytidine—New drugs covalently linking antimetabolites (5-FdU, araU or AZT) with bone-targeting bisphosphonates (alendronate or pamidronate). Bioorg. Med. Chem. 2011, 19, 3520–3526. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Zhang, P.; Mukthavaram, R.; Nomura, N.; Pingle, S.C.; Teng, D.; Chien, S.; Guo, F.; Kesari, S. Anti-cancer effects of nitrogen-containing bisphosphonates on human cancer cells. Oncotarget 2016, 7, 57932–57942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, R.; Pramod Kumar, S.; Arup Kumar, M.; Ajay, G. Role of Bisphosphonate (Bps) in Breast Cancer: An Update. Clin. Oncol. 2018, 1, 1–5. [Google Scholar]
- Sandholm, J.; Lehtimäki, J.; Ishizu, T.; Velu, S.E.; Clark, J.; Härkönen, P.; Jukkola-Vuorinen, A.; Schrey, A.; Harris, K.W.; Tuomela, J.M.; et al. Toll-like receptor 9 expression is associated with breast cancer sensitivity to the growth in-hibitory effects of bisphosphonates in vitro and in vivo. Oncotarget 2016, 7, 87373. [Google Scholar] [CrossRef] [Green Version]
- Gampenrieder, S.P.; Rinnerthaler, G.; Greil, R. Bone-targeted therapy in metastatic breast cancer—All well-established knowledge? Breast Care 2014, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Senaratne, S.G.; Mansi, J.L.; Colston, K.W. The bisphosphonate zoledronic acid impairs membrane localisation and induces cytochrome c release in breast cancer cells. Br. J. Cancer. 2002, 86, 1479–1486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottewell, P.; Wilson, C. Bone-targeted agents in breast cancer: Do we now have all the answers? Breast Cancer Basic Clin. Res. 2019, 13, 1178223419843501. [Google Scholar] [CrossRef] [PubMed]
- Clézardin, P. Mechanisms of action of bisphosphonates in oncology: A scientific concept evolving from antiresorptive to anticancer activities. BoneKEy Rep. 2013, 2, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ural, A.U.; Avcu, F.; Candir, M.; Guden, M.; Ozcan, M.A. In vitro synergistic cytoreductive effects of zoledronic acid and radiation on breast cancer cells. Breast Cancer Res. 2006, 8, R52. [Google Scholar] [CrossRef] [Green Version]
- Buranrat, B.; Bootha, S. Antiproliferative and antimigratory activities of bisphosphonates in human breast cancer cell line MCF-7. Oncol. Lett. 2019, 18, 1246–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragni, M.; Bonini, S.A.; Stabile, A.; Bodei, S.; Cristinelli, L.; Simeone, C.; Zani, D.; Spano, P.F.; Berruti, A.; Memo, M.; et al. Inhibition of survivin is associated with zoledronic acid-induced apoptosis of prostate cancer cells. Anticancer. Res. 2016, 36, 913–920. [Google Scholar]
- Green, J.R. Preclinical profile of zoledronic acid in prostate cancer models. Eur. Urol. Suppl. 2004, 3, 16–24. [Google Scholar] [CrossRef]
- Liu, J.; Huang, W.; Zhou, R.; Jia, S.; Tang, W.; Luo, Y.; Zhang, J. Bisphosphonates in the treatment of patients with metastatic breast, lung, and prostate cancer. Medicine 2015, 94, e2014. [Google Scholar] [CrossRef]
- Zarogoulidis, K.; Boutsikou, E.; Zarogoulidis, P.; Eleftheriadou, E.; Kontakiotis, T.; Lithoxopoulou, H.; Tzanakakis, G.; Kanakis, I.; Karamanos, N.K. The impact of zoledronic acid therapy in the survival of lung cancer patients with bone metastasis. Int. J. Cancer 2009, 125, 1705–1709. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Ouyang, X. Bone markers for monitoring efficacy in patients with bone metastases receiving zoledronic acid: A review of published data. Int. J. Biol. Markers 2013, 28, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Liu, X.; Li, X.; Guo, F.; Huang, C.; Qin, Q.; Wang, Y. Zoledronic acid increases the antitumor effect of gefitinib treatment for non-small cell lung cancer with EGFR mutations. Oncol. Rep. 2016, 35, 3460–3470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.W.; Fernandes, G.; Dziak, R. Effects of alendronate and interferon-γ on bone cancer cells in vitro. Cogent Biol. 2018, 4, 1427306. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Generation | 2nd Generation | 3rd Generation |
|---|---|---|
 |  |  |
 |  |  |
 |  |
| IC50 (nM) | |||||
|---|---|---|---|---|---|
| Cell Line | PS-341 | PS-341-BP-1 (24) | PS-341-BP-2 (25) | MG-262 | MG-262 BP (26) |
| 5TGM1 | 6.78 + 0.57 | 7.59 + 0.68 | 9.39 + 0.78 | 9.18 + 0.54 | 4.89 + 0.12 |
| RPMI 8226 | 9.50 + 0.48 | 10.18 + 0.87 | 11.51 + 0.92 | 13.76 + 0.89 | 12.47 + 0.87 |
| Cell Lines | IC50 (mol/L) |
|---|---|
| HLC-2 | 2.6 × 10−5 |
| HCC1954 | 2.8 × 10–5 |
| MCF-7 | 2.6 × 10–5 |
| K562 | 4.7 × 10–6 |
| Substance | IC50 (mol/L) |
|---|---|
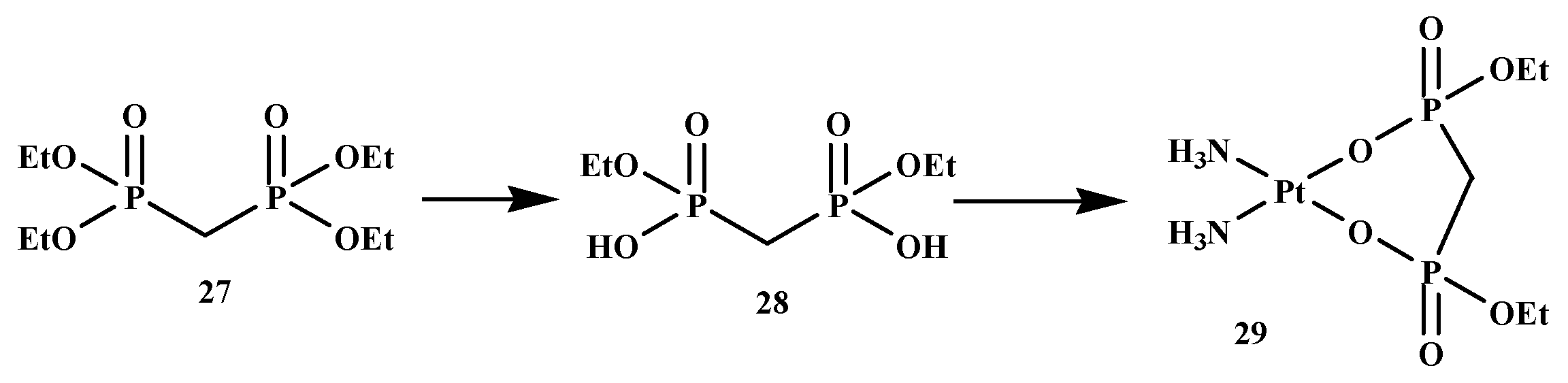
| DEBP-Pt | 2.8 × 10–−6 |
| Cisplatin | 1.1 × 10–5 |
| MCF-7 | MDA-MB 231 | OvCa-3 | OvCa-29 | |||||
|---|---|---|---|---|---|---|---|---|
| IC50 | IC90 | IC50 | IC90 | IC50 | IC90 | IC50 | IC90 | |
| 5-fluorouracil | 25.5 | 44.2 | 24.4 | 52.1 | 1.2 | 6.3 | 10.7 | 30.0 |
| Zoledronate | 8.9 | 42.9 | 6.4 | 39.1 | 1.6 | 6.0 | 3.0 | 7.2 |
| 5-Fluoro-2′-deoxyuridine-alendronate | 51.3 | 83.8 | 12.8 | 62.5 | 24.5 | 64.7 | 8.2 | 62.5 |
| Alendronate | 55.9 | 100.7 | 32.3 | 69.7 | 12.7 | 39.8 | 16.6 | 38.2 |
| 5-Fluoro-2′-deoxyuridine-alendronate-aledronate | 45.0 | 73.3 | 44.9 | 79.6 | 59.9 | 123.0 | 40.1 | 69.5 |
| Types of Cancer | Mode of Action of BPs | References |
|---|---|---|
| Breast | - Inhibits proliferation of breast cancer cells, inhibits FPPS of the mevalonate pathway and inhibits GGPPS. | [119,120] |
| Shows high affinity to bone matrix hydroxyapatite breast cancer. | [121] | |
| - Induces apoptosis by preventing ATP-dependent enzymes and prevents their absorption capacity. | [122] | |
| - Prevents breast cancer cell adhesion to the bone in vitro. - Inhibits the development and capability of cultured human breast cancer cells. - Induces loss of cell capability and DNA fragmentation in MCF-7 cells. | [123] | |
| - Prevents recurrence in postmenopausal women only. | [124] | |
| - In vitro, prevents tumor cell invasion, adhesion, migration, proliferation, and induces tumor cell apoptosis. | [125] | |
| - Improves the capability of antineoplastic agents to prevent breast cancer cell invasion. | [126] | |
| - Induces MCF-7 cell death and inhibit MCF-7 cell growth. | [127] | |
| Prostate | - Has exhibited to apply a direct cytostatic and pro-apoptotic impact on PCa cell lines in vitro. - Inhibits cell invasion and adhesion through a decrease of matrix metalloproteinase appearance. - Prevents testosterone-prompted angiogenesis in a castrated animal model. | [128] |
| - Prevents proliferation and induce apoptosis of prostate cancer cell lines in vitro. - In vitro studies of PC-3, LNCaP, and Du145 cell line, it prevents proliferation, induces apoptosis, decreases cell viability, and causes cell-cycle arrest. | [129] | |
| - Can down-regulate the expression of Bcl-2. - Induce apoptosis in prostate cancers. - Prevents proliferation markers, destroying the proliferation of tumors. | [130] | |
| Lung | - Prevents cell proliferation in SCLC and NSCLC cell lines. - Uses its anti-proliferative impact against NSCLC by the initiation of cellular apoptosis via the small GTP-binding proteins related signal transduction pathway. | [115,131] |
| - Prevents cancer cell cycle progression of NSCL carcinomas. - Induces cancer cell apoptosis in osteosarcoma, melanoma, and mesothelioma. | [125] | |
| - Improves cancer cell apoptosis, yields synergistic anticancer effects. | [132] | |
| - Prevents the action of osteoclasts and induces osteoclast apoptosis. - Exhibits prevention of the mevalonate pathway, regulation of immune response, and affects tumor signaling pathways and anti-angiogenesis. | [133] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mbese, Z.; Aderibigbe, B.A. Bisphosphonate-Based Conjugates and Derivatives as Potential Therapeutic Agents in Osteoporosis, Bone Cancer and Metastatic Bone Cancer. Int. J. Mol. Sci. 2021, 22, 6869. https://doi.org/10.3390/ijms22136869
Mbese Z, Aderibigbe BA. Bisphosphonate-Based Conjugates and Derivatives as Potential Therapeutic Agents in Osteoporosis, Bone Cancer and Metastatic Bone Cancer. International Journal of Molecular Sciences. 2021; 22(13):6869. https://doi.org/10.3390/ijms22136869
Chicago/Turabian StyleMbese, Zintle, and Blessing A. Aderibigbe. 2021. "Bisphosphonate-Based Conjugates and Derivatives as Potential Therapeutic Agents in Osteoporosis, Bone Cancer and Metastatic Bone Cancer" International Journal of Molecular Sciences 22, no. 13: 6869. https://doi.org/10.3390/ijms22136869
APA StyleMbese, Z., & Aderibigbe, B. A. (2021). Bisphosphonate-Based Conjugates and Derivatives as Potential Therapeutic Agents in Osteoporosis, Bone Cancer and Metastatic Bone Cancer. International Journal of Molecular Sciences, 22(13), 6869. https://doi.org/10.3390/ijms22136869