
Metalloproteinases 1 and 3 as Potential Biomarkers in Breast Cancer Development

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Features of Patients
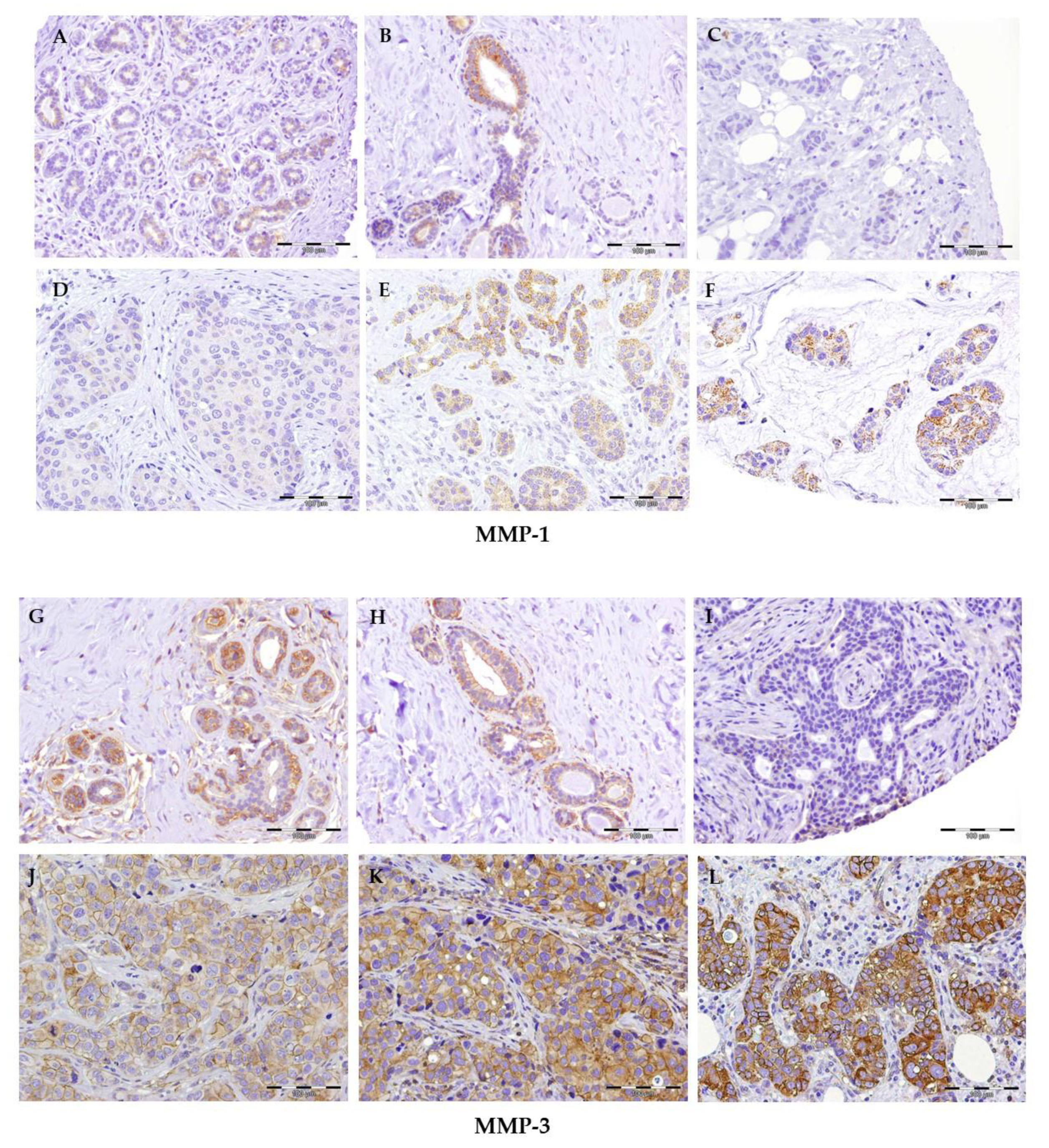
2.2. Immunohistochemical Expression of MMPs
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunocytochemical Staining
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19. Pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H. Delay in the diagnosis of breast cancer during coronavirus pandemic. EXCLI J. 2021, 20, 142–144. [Google Scholar] [PubMed]
- Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers. 2020, 12, 2237. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española de Oncología Médica. Las Cifras del Cáncer en España. 2021. Available online: http://www.seom.org (accessed on 26 June 2021).
- Lu, P.; Weaver, V.M.; Werb, Z. The extracellular matrix: A dynamic niche in cancer progression. J. Cell Biol. 2012, 196, 395–406. [Google Scholar] [CrossRef]
- Deryugina, E.I.; Quigley, J.P. Matrix metalloproteinases and tumor metastasis. Cancer Metastasis Rev. 2006, 25, 9–34. [Google Scholar]
- Belkin, A.M.; Akimov, S.S.; Zaritskaya, L.S.; Ratnikov, B.I.; Deryugina, E.I.; Strongin, A.Y. Matrix-dependent proteolysis of surface transglutaminase by membrane-type metalloproteinase regulates cancer cell adhesion and locomotion. J. Biol. Chem. 2001, 276, 18415–18422. [Google Scholar] [CrossRef] [Green Version]
- Lambert, E.; Dasse, E.; Haye, B.; Petitfrere, E. TIMPS as multifacial proteins. Crit. Rev. Oncol. Hematol. 2004, 49, 187–198. [Google Scholar] [CrossRef]
- Radisky, E.S.; Raeeszadeh-Sarmazdeh, M.; Radisky, D.C. Therapeutic Potential of Matrix Metalloproteinase Inhibition in Breast Cancer. J Cell Biochem. 2017, 118, 3531–3548. [Google Scholar] [CrossRef] [Green Version]
- Napoli, S.; Scuderi, C.; Gattuso, G.; Bella, V.D.; Candido, S.; Basile, M.S.; Libra, M.; Falzone, L. Functional Roles of Matrix Metalloproteinases and Their Inhibitors in Melanoma. Cells 2020, 9, 1151. [Google Scholar] [CrossRef]
- Tampa, M.; Georgescu, S.R.; Mitran, M.I.; Mitran, C.I.; Matei, C.; Caruntu, A.; Scheau, C.; Nicolae, I.; Matei, A.; Caruntu, C.; et al. Current Perspectives on the Role of Matrix Metalloproteinases in the Pathogenesis of Basal Cell Carcinoma. Biomolecules 2021, 11, 903. [Google Scholar] [CrossRef]
- Cascales, M.; Álvarez-Gómez, J.A. Metalloproteinasas, matriz extracelular y caáncer. An. R. Acad. Nac. Farm. 2010, 76, 59–84. [Google Scholar]
- Holmbeck, K.; Bianco, P.; Inoue, S.; Billinghurst, R.C.; Wu, W.; Chrysovergis, K.; Yamada, S.; Birkedal-Hansen, H.; Poole, A.R. The metalloproteinase MT1-MMP is required for normal development and maintenance of osteocyte processes in bone. J Cell Sci. 2005, 118, 147–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajiwara, Y.; Ueno, H.; Hashihuchi, Y.; Shinto, E.; Shimazaki, H.; Mochizuki, H.; Hase, K. Heterogeneity of metalloproteinase expression in colorectal cancer e relation of molecular findings to basic morphology. Anticancer Res. 2011, 31, 1567–1575. [Google Scholar] [PubMed]
- Sena, P.; Mariani, F.; Marzona, L.; Benincasa, M.; Ponz de Leon, M.; Palumbo, C.; Roncucciet, L. Matrix metalloproteinases 15 and 19 are stromal regulators of colorectal cancer development from the early stages. Int. J. Oncol. 2012, 41, 260–266. [Google Scholar]
- Rydlova, M.; Holubec, L.; Ludvikova, M.; Kalfert, D.; Franekova, J.; Povysil, C.; Ludvikova, M. Biological activity and clinical implications of the matrix metalloproteinases. Anticancer Res. 2008, 28, 1389–1397. [Google Scholar]
- Radisky, E.S.; Radisky, D.C. Matrix metalloproteinases as breast cancer drivers and therapeutic targets. Front. Biosci. 2015, 20, 1144–1163. [Google Scholar] [CrossRef]
- Kessenbrock, K.; Plaks, V.; Werb, Z. Matrix metalloproteinases: Regulators of the tumor microenvironment. Cell 2010, 141, 52–67. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; Wang, S.; Lu, J.; Cao, Y.; Song, N.; Yang, T.; Dong, R.; Zang, L.; Yang, Y.; Wu, T.; et al. Correlation between MMP1-PAR1 axis and clinical outcome of primary gallbladder carcinoma. Jpn. J. Clin. Oncol. 2011, 41, 1086–1093. [Google Scholar] [CrossRef]
- Grimm, M.; Lazariotou, M.; Kircher, S.; Stuermer, L.; Reiber, C.; Höfelmayr, A.; Gattenlöhner, S.; Otto, C.; Germer, C.T.; von Rahden, B.H. MMP-1 is a (pre-)invasive factor in Barrett- associated esophageal adenocarcinomas and is associated with positive lymph node status. J. Transl. Med. 2010, 8, 99. [Google Scholar] [CrossRef] [Green Version]
- Fan, S.Q.; Wei, Q.T.; Li, M.I.; Zhang, L.Q. Expression and clinical significance of MMP-2, MMp-9, Timp-1 and TIMP-2 in breast carcintoma. Ai Zheng 2003, 22, 968–973. [Google Scholar]
- Olivares-Urbano, M.A.; Griñan-Lisón, C.; Zurita, M.; del Moral, R.; Ríos-Arrabal, S.; Artacho-Cordón, F.; Arrebola, J.P.; González, A.R.; León, J.; Marchal, J.A.; et al. Matrix-metalloproteases and TIMPs as prognostic biomarkers in breast cancer patients treated with radiotherapy: A pilot study. J. Cell. Mol. Med. 2020, 24, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Ito, M.; Shiozawa, J.; Naito, S.; Kanematsu, T.; Sekine, I. Expression of the MMP-1 in human pancreatic carcinoma: Relationship with prognostic factor. Mod. Pathol. 1999, 12, 669–674. [Google Scholar]
- Egeblad, M.; Werb, Z. New functions for the matrix metalloproteinases in cancer progression. Nat. Rev. Cancer 2002, 2, 161–174. [Google Scholar] [CrossRef]
- Stetler-Stevenson, W.G. Matrix metalloproteinases in angiogenesis: A moving target for therapeutic intervention. J. Clin. Investig. 1999, 103, 1237–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eck, S.M.; Blackburn, J.S.; Schmucker, A.C.; Burrage, P.S.; Brinckerhoff, C.E. Matrix metalloproteinase and G protein coupled receptors: Co-conspirators in the pathogenesis of autoimmune disease and cancer. J Autoimmun. 2009, 33, 214–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köhrmann, A.; Kammerer, U.; Kapp, M.; Dietl, J.; Anacker, J. Expression of matrix metalloproteinases (MMPs) in primary human breast cancer and breast cancer cell lines: New findings and review of the literature. BMC Cancer 2009, 9, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, B.P.; Shah, P.M.; Rawal, U.M.; Desai, A.A.; Shah, S.V.; Rawal, R.M.; Patel, P.S. Activation of MMP-2 and MMP-9 in patients with oral squamous cell carcinoma. J. Surg. Oncol. 2005, 90, 81–88. [Google Scholar] [CrossRef]
- Pellikainen, J.M.; Ropponen, K.M.; Kataja, V.V.; Kellokoski, J.K.; Eskelinen, M.J.; Kosma, V.M. Expression of matrix metalloproteinase MMP-2 and MMP-9 in breast cancer with special reference to activator protein-2, HER-2 and prognosis. Clin. Cancer Res. 2004, 10, 7621–7628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparmann, A.; Bar-Sagi, D. Ras-induced interleukin-8 expression plays a critical role in tumor growth and angiogenesis. Cancer Cell 2004, 6, 447–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, L.R.; Camacho, D.F.; Shiozawa, Y.; Pienta, K.J.; Taichman, R.S. Mechanisms of cancer cell metastasis to the bone: A multistep process. Future Oncol. 2011, 7, 1285–1297. [Google Scholar] [CrossRef] [Green Version]
- Drabsch, Y.; Ten, D.P. TGF-b signaling in breast cancer cell invasion and bone metastasis. J. Mammary Gland Biol. Neoplasia. 2011, 16, 97–108. [Google Scholar] [CrossRef] [Green Version]
- Chabottaux, V.; Noel, A. Breast cancer progression: Insights into multifaceted matrix metalloproteinases. Clin. Exp. Metastasis 2007, 24, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Noë, V.; Fingleton, B.; Jacobs, K.; Crawford, H.C.; Vermeulen, S.; Steelant, W.; Bruyneel, E.; Matrisian, L.M.; Mareel, M. Release of an invasion promoter E-cadherin fragment by matrilysin and stromelysin-1. J. Cell Sci. 2001, 114, 111–118. [Google Scholar] [CrossRef]
- Sternlicht, M.D.; Bissett, M.J.; Werb, Z. The matrix metalloproteinase stromelysin-1 acts as a natural mammary tumor promoter. Oncogene 2000, 19, 1102–1113. [Google Scholar] [CrossRef] [Green Version]
- Sato, H.; Takino, T.; Miyamori, H. Roles of membrene-Type matrix metalloproteinase-1 in tumor invasion and metastasis. Cancer Sci. 2005, 96, 212–217. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Artacho-Cordón, F.; Ríos-Arrabal, S.; Lara, P.C.; Artacho-Cordón, A.; Calvente, I.; Núñez, M.I. Matrix metalloproteinases: Potential therapy to prevent the development of second malignancies after breast radiotherapy. Surg. Oncol. 2012, 21, 143–151. [Google Scholar]
- Bahcecioglu, G.; Basara, G.; Ellis, B.W.; Ren, X.; Zorlutuna, P. Breast cancer models: Engineering the tumor microenvironment. Acta Biomater. 2020, 106, 1–21. [Google Scholar] [CrossRef]
- Yang, J.; Bahcecioglu, G.; Zorlutuna, P. The Extracellular Matrix and Vesicles Modulate the Breast Tumor Microenvironment. Bioengineering 2020, 7, 124. [Google Scholar] [CrossRef]
- Lodewijk, I.; Nunes, S.P.; Henrique, R.; Jerónimo, C.; Dueñas, M.; Paramio, J.M. Tackling tumor microenvironment through epigenetic tools to improve cancer immunotherapy. Clin. Epigenetics 2021, 13, 63. [Google Scholar] [CrossRef]
- Falzone, L.; Salemi, R.; Travali, S.; Scalisi, A.; McCubrey, J.A.; Candido, S.; Libra, M. MMP-9 overexpression is associated with intragenic hypermethylation of MMP9 gene in melanoma. Aging 2016, 8, 933–944. [Google Scholar] [CrossRef] [Green Version]
- Simonova, O.A.; Kuznetsova, E.B.; Tanas, A.S.; Rudenko, V.V.; Poddubskaya, E.V.; Kekeeva, T.V.; Trotsenko, I.D.; Larin, S.S.; Kutsev, S.I.; Zaletaev, D.V.; et al. Abnormal Hypermethylation of CpG Dinucleotides in Promoter Regions of Matrix Metalloproteinases Genes in Breast Cancer and Its Relation to Epigenomic Subtypes and HER2 Overexpression. Biomedicines 2020, 8, 116. [Google Scholar] [CrossRef]
- Rutnam, Z.J.; Wight, T.N.; Yang, B.B. miRNAs regulate expression and function of extracellular matrix molecules. Matrix Biol. 2013, 32, 74–85. [Google Scholar] [CrossRef] [Green Version]
- Falzone, L.; Grimaldi, M.; Celentano, E.; Augustin, L.S.A.; Libra, M. Identification of Modulated MicroRNAs Associated with Breast Cancer, Diet, and Physical Activity. Cancers 2020, 12, 2555. [Google Scholar] [CrossRef]
- Rak, B.; Mehlich, D.; Garbicz, F.; Domosud, Z.; Paskal, W.; Marczewska, J.M.; Włodarski, P.K. Post-transcriptional Regulation of MMP16 and TIMP2 Expression via miR-382, miR-410 and miR-200b in Endometrial Cancer. Cancer Genom. Proteom. 2017, 14, 389–401. [Google Scholar]
- Javadian, M.; Gharibi, T.; Shekari, N.; Abdollahpour-Alitappeh, M.; Mohammadi, A.; Hossieni, A.; Mohammadi, H.; Kazemi, T. The role of microRNAs regulating the expression of matrix metalloproteinases (MMPs) in breast cancer development, progression, and metastasis. J. Cell Physiol. 2019, 234, 5399–5412. [Google Scholar] [CrossRef]
- Song, B.; Wang, C.; Liu, J.; Wang, X.; Lv, L.; Wei, L.; Xie, L.; Zheng, Y.; Song, X. MicroRNA-21 regulates breast cancer invasion partly by targeting tissue inhibitor of metalloproteinase 3 expression. J. Exp. Clin. Cancer Res. 2010, 29, 29. [Google Scholar] [CrossRef] [Green Version]
- Gumireddy, K.; Young, D.D.; Xiong, X.; Hogenesch, J.B.; Huang, Q.; Deiters, A. Small-Molecule Inhibitors of MicroRNA miR-21 Function. Angew. Chem. Int. 2008, 47, 7482–7484. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Cao, Y.D.; Ye, W.X.; Sun, Y.Y. Effect of microRNA-206 on cytoskeleton remodelling by downregulating Cdc42 in MDA-MB-231 cells. Tumori. 2010, 96, 751–755. [Google Scholar] [CrossRef]
- Martello, G.; Rosato, A.; Ferrari, F.; Manfrin, A.; Cordenonsi, M.; Dupont, S.; Enzo, E.; Guzzardo, V.; Rondina, M.; Spruce, T.; et al. A microRNA targeting dicer for metastasis control. Cell 2010, 141, 1195–1207. [Google Scholar] [CrossRef] [Green Version]
- Foekens, J.A.; Sieuwerts, A.M.; Smid, M.; Look, M.P.; De Weerd, V.; Boersma, A.W.M.; Klijn, J.G.M.; Wiemer, E.A.C.; Martens, J.W.M. Four miRNAs associated with aggressiveness of lymph node-negative, estrogen receptor-positive human breast cancer. Proc. Natl. Acad. Sci. USA 2008, 105, 13021–13026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, C.; Liu, X.; Bai, X.; Zhao, T.; Wang, M.; Xu, R.; Li, M.; Hu, Y.; Li, W.; Yang, L.; et al. MiR-519d suppresses breast cancer tumorigenesis and metastasis via targeting MMP3. Int. J. Biol. Sci. 2018, 14, 228–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niland, S.; Eble, J.A. Hold on or Cut? Integrin- and MMP-Mediated Cell-Matrix Interactions in the Tumor Microenvironment. Int. J. Mol. Sci. 2020, 22, 238. [Google Scholar] [CrossRef] [PubMed]
- Gialeli, C.; Theocharis, A.D.; Karamanos, N.K. Roles of matrix metalloproteinases in cancer progression and their pharmacological targeting. FEBS J. 2011, 278, 16–27. [Google Scholar] [CrossRef]
- Lamouille, S.; Xu, J.; Derynck, R. Molecular mechanisms of epithelial-mesenchymal transition. Nat. Rev. Mol. Cell Biol. 2014, 15, 178–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez, D.; Morrison, C.J.; Overall, C.M. Matrix metalloproteinases: What do they not do? New substrates and biological roles identified by murine models and proteomics. Biochim. Biophy. Acta. 2010, 1803, 39–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blavier, L.; Lazaryev, A.; Shi, X.H.; Dorey, F.J.; Shackleford, G.M.; DeClerk, Y.A. Stromelysin-1 (MMP-3) is a target and a regulator of Wnt1-induced epithelial-mesenchymal transition (EMT). Cancer Biol. Ther. 2010, 10, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagase, H.; Ogata, Y.; Suzuki, K.; Enghild, J.J.; Salvesen, G. Substrate specificities and activation mechanisms of matrix metalloproteinases. Biochem. Soc. Trans. 1991, 19, 715–718. [Google Scholar] [CrossRef] [Green Version]
- Fisher, C.; Gilbertson-Beadling, S.; Powers, E.A.; Petzlod, G.; Poorman, R.; Mitchell, M.A. Interstitial collagenase is required for angiogenesis in vitro. Dev. Biol. 1994, 162, 499–510. [Google Scholar] [CrossRef]
- Jezierska, A.; Motyl, T. Matrix metalloproteinase-2 involvement in breast cancer progression: A mini-review. Med. Sci. Monit. 2009, 15, 32–40. [Google Scholar]
- Van’t Veer, L.J.; Dai, H.; van de Vijver, M.J.; He, Y.D.; Hart, A.A.; Mao, M.; Peterse, H.L.; van der Kooy, K.; Marton, M.J.; Witteveen, A.T.; et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002, 415, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Roeb, E.; Arndt, M.; Jansen, B.; Schumpelick, V.; Matern, S. Simultaneous determination of matrix metalloproteinase (MMP)-7, MMP-1, -3, and -13 gene expression by multiplex PCR in colorectal carcinomas. Int. J. Colorectal. Dis. 2004, 19, 518–524. [Google Scholar] [CrossRef]
- Wieczorek, E.; Reszka, E.; Jablonowski, Z.; Jablonska, E.; Krol, M.B.; Grzegorczyk, A.; Gromadzinska, J.; Sosnowski, M.; Wasowicz, W. Genetic polymorphisms in matrix metalloproteinases (MMPs) and tissue inhibitors of MPs (TIMPs), and bladder cancer susceptibility. BJU Int. 2013, 112, 1207–1214. [Google Scholar] [CrossRef]
- Liu, H.; Kato, Y.; Erzinger, S.A.; Galena, M.K.; Qian, Y.; Palmieri, D.; Steeg, P.S.; Price, J.E. The role of MMP-1 in breast cancer growth and metastasis to the brain in a xenograft model. BMC Cancer 2012, 12, 583. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.; Mitsuhiro, T.; Yasuhiro, H.; Toshimichi, A.; Kuramae, T.; Takemoto, N.; Hamada, J.-I.; Miyamoto, M.; Hirano, S.; Kondo, S.; et al. High MMP-1 mRNA expression is a risk factor for disease-free and overall survivals in patients with invasive breast carcinoma. J. Surg. Res. 2008, 146, 104–109. [Google Scholar] [CrossRef]
- Shen, C.J.; Kuo, Y.L.; Chen, C.C.; Chen, M.J.; Cheng, Y.M. MMP1 expression is activated by Slug and enhances multi-drug resistance (MDR) in breast cancer. PLoS ONE 2017, 12, e0174487. [Google Scholar] [CrossRef] [Green Version]
- Ji, W.; Chenyang, Y.; Demin, L.; Yongxia, C.; Yunlu, J.; Xiaogang, Y.; Hanchu, X.; Wenhe, Z.; Jichun, Z.; Linbo, W. Matrix metalloproteinase-1 expression in breast carcinoma: A marker for unfavorable prognosis. Oncotarget 2017, 8, 91379–91390. [Google Scholar]
- Jones, J.L.; Walker, R.A. Control of matrix metalloproteinase activity in cancer. J. Pathol. 1997, 183, 377–379. [Google Scholar] [CrossRef]
- Alexander, C.M.; Selvarajan, S.; Mudgett, J.; Werb, Z. Stromelysin-1 regulates adipogenesis during mammary gland involution. J. Cell Biol. 2001, 152, 693–703. [Google Scholar] [CrossRef] [Green Version]
- McCawley, L.J.; Crawford, H.C.; King, L.E., Jr.; Mudgett, J.; Matrisian, L.M. A protective role for matrix metalloproteinase-3 in squamous cell carcinoma. Cancer Res. 2004, 64, 6965–6972. [Google Scholar] [CrossRef] [Green Version]
- Boström, P.; Söderström, M.; Vahlberg, T.; Söderström, K.O.; Roberts, P.J.; Carpén, O.; Hirsimäki, P. MMP-1 expression has an independent prognostic value in breast cancer. BMC Cancer 2011, 11, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.M.; Lv, L.; Tang, Y.; Zhang, L.; Wang, L.F. MMP-1 is overexpressed in triple-negative breast cancer tissues and the knockdown of MMP-1 expression inhibits tumor cell malignant behaviors in vitro. Oncol. Lett. 2019, 17, 1732–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehner, C.; Miller, E.; Nassar, A.; Bamlet, W.R.; Radisky, E.S.; Radisky, D.C. Tumor cell expression of MMP3 as a prognostic factor for poor survival in pancreatic, pulmonary, and mammary carcinoma. Genes Cancer. 2015, 6, 480–489. [Google Scholar] [CrossRef] [Green Version]
- Martins, L.M.; de Melo Escorcio Dourado, C.S.; Campos-Verdes, L.M.; Sampaio, F.A.; Revoredo, C.M.S.; Costa-Silva, D.R.; da Conceição Barros-Oliveira, M.; de Jesus Nery Junior, E.; do Rego-Medeiros, L.M.; Gebrim, L.H.; et al. Expression of matrix metalloproteinase 2 and 9 in breast cancer and breast fibroadenoma: A randomized, double-blind study. Oncotarget 2019, 10, 6879–6884. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, F.A.; Martins, L.M.; Dourado, C.S.M.E.; Revoredo, C.M.S.; Costa-Silva, D.R.; Oliveira, V.A.; Alves-Ribeiro, F.A.; Silva, B.B.D. A case-control study of Metallothionein-1 expression in breast cancer and breast fibroadenoma. Sci. Rep. 2019, 9, 7407. [Google Scholar] [CrossRef]
- Li, H.C.; Cao, D.C.; Liu, Y.; Hou, Y.F.; Wu, J.; Lu, J.S.; Di, G.H.; Liu, G.; Li, F.M.; Ou, Z.L.; et al. Prognostic value of matrix metalloproteinases (MMP-2 and MMP-9) in patients with lymph node-negative breast carcinoma. Breast Cancer Res. Treat. 2004, 88, 75–85. [Google Scholar] [CrossRef]
- Tauro, M.; Lynch, C.C. Cutting to the Chase: How Matrix Metalloproteinase-2 Activity Controls Breast-Cancer-to-Bone Metastasis. Cancers 2018, 10, 185. [Google Scholar] [CrossRef] [Green Version]
- Mook, O.R.; Frederiks, W.M.; Van Noorden, C.J. The role of gelatinases in colorectal cancer progression and metastasis. Biochim. Biophy. Acta 2004, 1705, 69–89. [Google Scholar] [CrossRef]
- Bjorklund, M.; Koivunen, E. Gelatinase-mediated migration and invasion of cancer cells. Biochim. Biophys Acta 2005, 1755, 37–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otani, Y.; Okazaki, I.; Arai, M.; Kameyama, K.; Wada, N.; Maruyama, K.; Yoshino, K.; Kitajima, M.; Hosoda, Y.; Tsuchiya, M. Gene expression of interstitial collagenase (matrix metalloproteinase 1) in gastrointestinal tract cancers. J. Gastroenterol. 1994, 29, 391–397. [Google Scholar] [CrossRef]
- Jiang, H.; Li, H. Prognostic values of tumoral MMP2 and MMP9 overexpression in breast cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 149. [Google Scholar] [CrossRef]
- Roy, R.; Yang, J.; Moses, M.A. Matrix metalloproteinases as novel biomarkers and potential therapeutic targets in human cancer. J. Clin. Oncol. 2009, 27, 5287–5297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadizadeh, F.; Bagherian-Dehkordia, M. Relationship between matrix metalloproteinase-9 and some clinicopathological prognostic factors of breast carcinoma. Am. J. Clin. Exp. Immunol. 2021, 10, 17–22. [Google Scholar] [PubMed]
- Cui, N.; Hu, M.; Khalil, R.A. Biochemical and Biological Attributes of Matrix Metalloproteinases. Prog. Mol. Biol. Transl. Sci. 2017, 147, 1–73. [Google Scholar]
- Winer, A.; Adams, S.; Mignatti, P. Matrix Metalloproteinase Inhibitors in Cancer Therapy: Turning Past Failures Into Future Successes. Mol. Cancer Ther. 2018, 17, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Fingleton, B.; Matrisian, L.M. Matrix metalloproteinase inhibitors and cancer: Trials and tribulations. Science 2002, 295, 2387–2392. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, R.E.; Libert, C. Is there new hope for therapeutic matrix metalloproteinase inhibition? Nat. Rev. Drug. Discov. 2014, 13, 904–927. [Google Scholar] [CrossRef]


{kind=link}
| Independent Variables | No. of Patients | Percentage | |
|---|---|---|---|
| Age interval | ≤50 years | 44 | 28.6 |
| 51–70 years | 53 | 34.4 | |
| >70 years | 57 | 37.0 | |
| Risk factors | First-degree family history of BC | 2 | 3.8 |
| Personal history of other tumors | 6 | 11.3 | |
| History of benign breast lesions | 4 | 7.5 | |
| Smoking | 19 | 35.8 | |
| Obesity | 16 | 30.2 | |
| More than one risk factor | 6 | 11.3 | |
| Menopause | Premenopause | 47 | 31.1 |
| Postmenopause | 104 | 68.9 | |
| Affected breast | Right breast | 39 | 30.7 |
| Left breast | 88 | 69.3 | |
| Histological type | Infiltrating ductal carcinoma | 135 | 87.7 |
| Infiltrating lobulillar carcinoma | 13 | 8.4 | |
| Other carcinomas | 6 | 3.9 | |
| Lymph node involvement | No | 70 | 45.8 |
| Yes | 83 | 54.2 | |
| Tumor stage | EI:IA-IB | 26 | 23.0 |
| EII:IIA-IIB | 52 | 46.0 | |
| EIII:IIIA-IIIB-IIIC | 30 | 26.5 | |
| EIV with any TNM | 5 | 4.4 | |
| Hormone receptors | Estrogenics and Progestogens + | 72 | 73.5 |
| Estrogenics and Progestogens − | 18 | 18.4 | |
| Treatment | Surgery + Chemotherapy + Radiotherapy | 52 | 33.8 |
| Surgery + Chemotherapy | 49 | 31.8 | |
| Surgery + Radiotherapy | 11 | 7.1 | |
| Surgery | 42 | 27.3 | |
| Tumor recurrence | No | 125 | 89.9 |
| Yes | 14 | 10.1 | |
| Tumor invasion | Bone | 5 | 20.0 |
| Lung | 4 | 16.0 | |
| Brain | 2 | 8.0 | |
| Liver | 1 | 4.0 | |
| Association with another cancer | 8 | 32.0 | |
| Metastasis to more than one organ | 5 | 20.0 | |
| Follow-up patientMortality in 2020 | Dead | 6 | 4.4 |
| Alive | 131 | 95.6 | |
| Study Variables | Group | p | |||
|---|---|---|---|---|---|
| Case | Control | Total | |||
| MMP-1 percentage | ≤50% | 29 | 9 | 38 | 0.073 |
| >50% | 117 | 16 | 133 | ||
| MMP-1 intensity | Weak | 96 | 22 | 118 | 0.043 |
| Moderate | 53 | 4 | 57 | ||
| Intense | 5 | NA | 5 | * | |
| MMP-2 percentage | ≤50% | 126 | 22 | 148 | 0.139 |
| >50% | 24 | 1 | 25 | ||
| MMP-2 intensity | Weak | 137 | 21 | 158 | 0.996 |
| Moderate | 13 | 2 | 15 | ||
| Intense | NA | NA | NA | * | |
| MMP-3 percentage | ≤50% | 57 | 16 | 73 | 0.018 |
| >50% | 90 | 9 | 99 | ||
| MMP-3 intensity | Weak | 104 | 12 | 116 | 0.025 |
| Moderate | 43 | 13 | 56 | ||
| Intense | 7 | NA | 7 | * | |
| MMP-9 percentage | ≤50% | 146 | 28 | 174 | 0.421 |
| >50% | NA | NA | NA | * | |
| MMP-9 intensity | Weak | 146 | 28 | 174 | 0.326 |
| Moderate | NA | NA | NA | * | |
| Intense | NA | NA | NA | * | |
| MMP-1 Intensity | MMP-3 Intensity | MMP-3 Percentage | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Weak | Moderate | p | Weak | Moderate | p | ≤50% | >50% | p | ||
| Age interval | ≤50 years | 32 | 10 | 0.168 | 35 | 8 | 0.177 | 12 | 31 | 0.210 |
| 51–70 years | 31 | 20 | 31 | 17 | 20 | 28 | ||||
| >70 years | 33 | 23 | 38 | 18 | 25 | 31 | ||||
| Tumor stage | EI | 19 | 7 | 0.549 | 19 | 5 | 0.766 | 10 | 14 | 0.978 |
| EII | 33 | 16 | 36 | 14 | 21 | 29 | ||||
| EIII | 19 | 10 | 18 | 9 | 10 | 17 | ||||
| EIV | 2 | 3 | 4 | 1 | 2 | 3 | ||||
| Menopause | Premenopause | 34 | 11 | 0.064 | 37 | 9 | 0.115 | 14 | 32 | 0.204 |
| Postmenopause | 60 | 41 | 65 | 33 | 41 | 57 | ||||
| Lymph node involvement | No | 42 | 25 | 0.730 | 48 | 19 | 0.856 | 26 | 41 | 0.510 |
| Yes | 54 | 27 | 55 | 24 | 30 | 49 | ||||
| Tumorrecurrence | No | 79 | 42 | 1.000 | 87 | 35/2 | 0.510 | 47 | 75 | 1.000 |
| Yes | 9 | 5 | 10 | 2 | 5 | 7 | ||||
| Affected breast | Right breast | 29 | 8 | 0.063 | 23 | 13 | 0.520 | 10 | 26 | 0.307 |
| Left breast | 51 | 34 | 62 | 25 | 33 | 54 | ||||
| Hormone receptors | Estrogenics and Progestogens + | 41 | 29 | 0.394 | 45 | 26 | 0.085 | 22 | 49 | 0.348 |
| Estrogenics and Progestogens − | 13 | 4 | 14 | 2 | 8 | 8 | ||||
| Estrogenics + | 5 | 3 | 7 | 1 | 3 | 5 | ||||
| Risk factors | First-degree family history of BC | 1 | 1 | 0.916 | 1 | 1 | 0.056 | 1 | 1 | 0.151 |
| Personal history of other tumors | 4 | 2 | 1 | 5 | 1 | 5 | ||||
| History of benign breast lesions | 3 | 1 | 3 | 1 | 1 | 3 | ||||
| Smoking | 10 | 8 | 12 | 6 | 3 | 15 | ||||
| Obesity | 10 | 6 | 14 | 2 | 9 | 7 | ||||
| More than one risk factor | 4 | 1 | 3 | 3 | 1 | 5 | ||||
| Histological type | Infiltrating ductal carcinoma | 84 | 47 | 0.748 | 91 | 38 | 0.272 | 48 | 81 | 0.502 |
| Infiltratinglobulillarcarcinoma | 8 | 5 | 8 | 5 | 6 | 7 | ||||
| Othercarcinomas | 4 | 1 | 5 | 0 | 3 | 2 | ||||
| Treatment | Surgery +Chemotherapy+ Radiotherapy | 31 | 18 | 0.984 | 36 | 15 | 0.856 | 18 | 33 | 0.863 |
| Surgery +Chemotherapy | 32 | 16 | 31 | 13 | 17 | 27 | ||||
| Surgery +Radiotherapy | 7 | 4 | 9 | 2 | 4 | 7 | ||||
| Surgery | 26 | 15 | 28 | 13 | 18 | 23 | ||||
| Tumorinvasion | Bone | 4 | 1 | 0.674 | 4 | 0 | 0.216 | 2 | 2 | 0.912 |
| Lung | 3 | 1 | 3 | 1 | 1 | 3 | ||||
| Brain | 1 | 1 | 2 | 0 | 1 | 1 | ||||
| Liver | 0 | 1 | 1 | 0 | 0 | 1 | ||||
| Association with another cancer | 6 | 2 | 3 | 5 | 3 | 5 | ||||
| Metastasis to more than one organ | 3 | 2 | 3 | 1 | 1 | 3 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argote Camacho, A.X.; González Ramírez, A.R.; Pérez Alonso, A.J.; Rejón García, J.D.; Olivares Urbano, M.A.; Torné Poyatos, P.; Ríos Arrabal, S.; Núñez, M.I. Metalloproteinases 1 and 3 as Potential Biomarkers in Breast Cancer Development. Int. J. Mol. Sci. 2021, 22, 9012. https://doi.org/10.3390/ijms22169012
Argote Camacho AX, González Ramírez AR, Pérez Alonso AJ, Rejón García JD, Olivares Urbano MA, Torné Poyatos P, Ríos Arrabal S, Núñez MI. Metalloproteinases 1 and 3 as Potential Biomarkers in Breast Cancer Development. International Journal of Molecular Sciences. 2021; 22(16):9012. https://doi.org/10.3390/ijms22169012
Chicago/Turabian StyleArgote Camacho, Angela Ximena, Amanda Rocío González Ramírez, Alejandro José Pérez Alonso, Juan David Rejón García, María Auxiliadora Olivares Urbano, Pablo Torné Poyatos, Sandra Ríos Arrabal, and María Isabel Núñez. 2021. "Metalloproteinases 1 and 3 as Potential Biomarkers in Breast Cancer Development" International Journal of Molecular Sciences 22, no. 16: 9012. https://doi.org/10.3390/ijms22169012
APA StyleArgote Camacho, A. X., González Ramírez, A. R., Pérez Alonso, A. J., Rejón García, J. D., Olivares Urbano, M. A., Torné Poyatos, P., Ríos Arrabal, S., & Núñez, M. I. (2021). Metalloproteinases 1 and 3 as Potential Biomarkers in Breast Cancer Development. International Journal of Molecular Sciences, 22(16), 9012. https://doi.org/10.3390/ijms22169012