
Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization

 ,
,  , ,
, ,  ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Radiomics
2.2. Radiomics in Prostate Cancer Management
2.3. Genomics and Molecular Tumor Characterization
2.3.1. Genomic Risk and Molecular Imaging in Prostate Cancer
Prostate Cancer Antigen 3 (PCA3)
Decipher Test®
Oncotype Dx Test®
ConfirmMDx®
Prolaris Test®
2.3.2. Radiogenomics in Prostate Cancer Management
3. Discussion
Current Challenges/Limitations and Future Perspectives
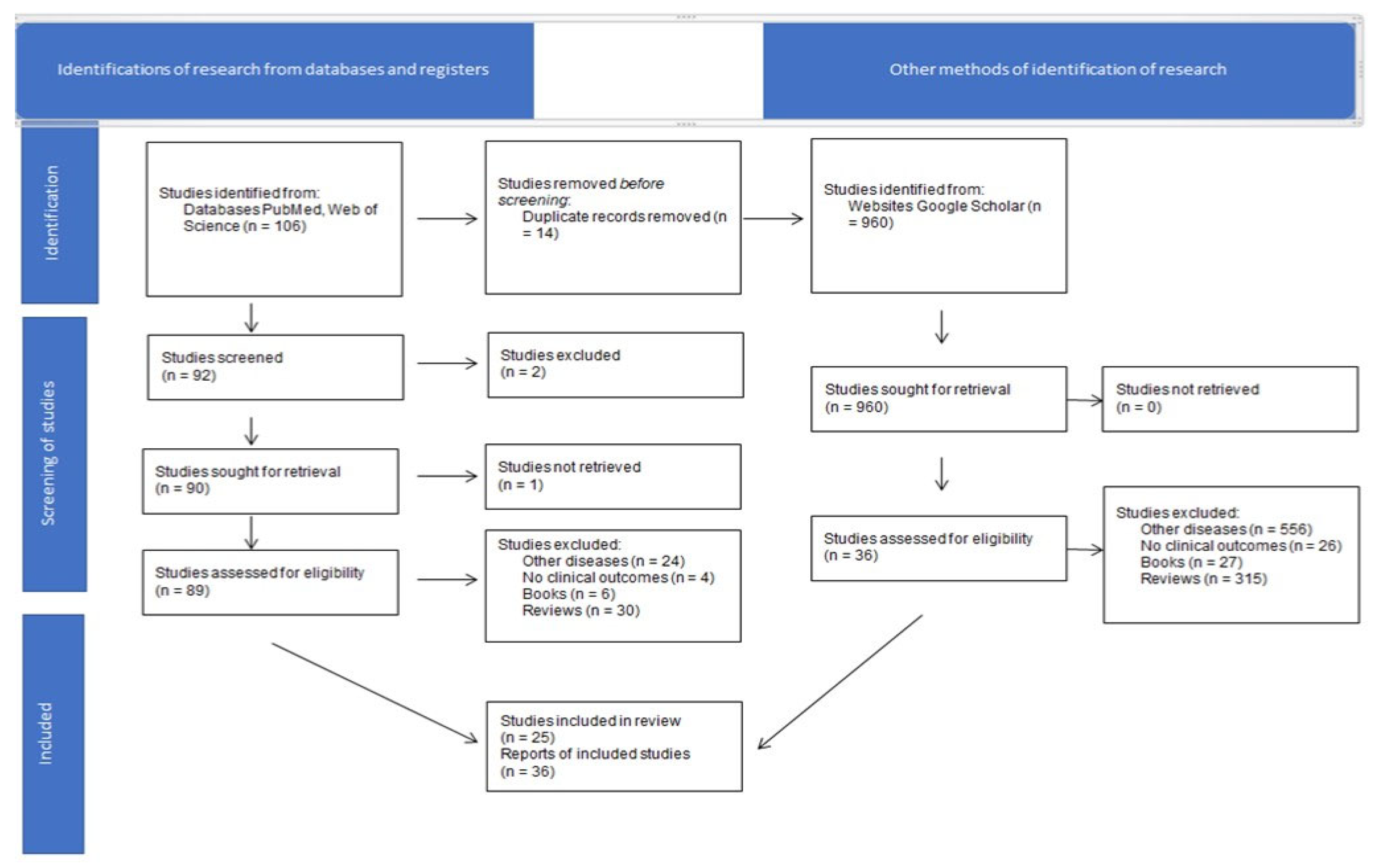
4. Material and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAN | Artificial neural network |
| ADC | Apparent diffusion coefficient |
| AI | Artificial intelligence |
| BCR | Biochemical recurrence |
| CCP | Cell cycle progression |
| CT | Computed tomography |
| DCE | Dynamic contrast-enhanced |
| DSC | Dynamic susceptibility contrast |
| DNA | Deoxyribonucleic acid |
| DRE | Digital rectal examination |
| DNN | Deep neural network |
| DWI | Diffusion-weighted imaging |
| ECE | Extracapsular extension |
| f-DWI | Full-field-of-view |
| z-DWI | Zoomed diffusion-weighted imaging |
| LASSO | Least absolute shrinkage and selection operator |
| ML | Machine learning |
| MRI | Magnetic resonance imaging |
| mpMRI | mpMRI |
| PCa | Prostate cancer |
| PIRADS | Prostate imaging reporting and data system |
| PSA | Prostate-specific antigen |
| PSMA PET-CT | Prostate-specific membrane antigen positron emission computed tomography |
| PTEN | Phosphatase and tensin homolog |
| RF | Random forest |
| RNA | Ribonucleic acid |
| ROI | Region of interest |
| RP | Radical prostatectomy |
| SAVR | Surface area-to-volume ratio |
| SVM | Support vector machine |
| T2w | T2-weighted |
| TCGA | The Cancer Genome Atlas |
| TCIA | The Cancer Imaging Archive |
| TRUS | Transrectal ultrasonography |
| VOI | Volume of interest |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; De Cobelli, O.; Lucarelli, G.; Porreca, A.; Busetto, G.M.; Cantiello, F.; Damiano, R.; Autorino, R.; Musi, G.; Vartolomei, M.D.; et al. Beyond PSA: The Role of Prostate Health Index (Phi). Int. J. Mol. Sci. 2020, 21, 1184. [Google Scholar] [CrossRef] [Green Version]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Shui, L.; Ren, H.; Yang, X.; Li, J.; Chen, Z.; Yi, C.; Zhu, H.; Shui, P. The Era of Radiogenomics in Precision Medicine: An Emerging Approach to Support Diagnosis, Treatment Decisions, and Prognostication in Oncology. Front. Oncol. 2020, 10, 570465. [Google Scholar] [CrossRef]
- Apte, A.P.; Iyer, A.; Crispin-Ortuzar, M.; Pandya, R.; van Dijk, L.V.; Spezi, E.; Thor, M.; Um, H.; Veeraraghavan, H.; Oh, J.H.; et al. Technical Note: Extension of CERR for Computational Radiomics: A Comprehensive MATLAB Platform for Reproducible Radiomics Research. Med. Phys. 2018, 45, 3713–3720. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falagario, U.G.; Jambor, I.; Ratnani, P.; Martini, A.; Treacy, P.-J.; Wajswol, E.; Lantz, A.; Papastefanou, G.; Weil, R.; Phillip, D.; et al. Performance of Prostate Multiparametric MRI for Prediction of Prostate Cancer Extra-Prostatic Extension According to NCCN Risk Categories: Implication for Surgical Planning. Minerva Urol. Nefrol. Ital. J. Urol. Nephrol. 2020, 72, 746–754. [Google Scholar] [CrossRef]
- Maggi, M.; Del Giudice, F.; Falagario, U.G.; Cocci, A.; Russo, G.I.; Di Mauro, M.; Sepe, G.S.; Galasso, F.; Leonardi, R.; Iacona, G.; et al. SelectMDx and Multiparametric Magnetic Resonance Imaging of the Prostate for Men Undergoing Primary Prostate Biopsy: A Prospective Assessment in a Multi-Institutional Study. Cancers 2021, 13, 2047. [Google Scholar] [CrossRef]
- Haffner, M.C.; Zwart, W.; Roudier, M.P.; True, L.D.; Nelson, W.G.; Epstein, J.I.; De Marzo, A.M.; Nelson, P.S.; Yegnasubramanian, S. Genomic and Phenotypic Heterogeneity in Prostate Cancer. Nat. Rev. Urol. 2021, 18, 79–92. [Google Scholar] [CrossRef]
- Erickson, A.; Hayes, A.; Rajakumar, T.; Verrill, C.; Bryant, R.J.; Hamdy, F.C.; Wedge, D.C.; Woodcock, D.J.; Mills, I.G.; Lamb, A.D. A Systematic Review of Prostate Cancer Heterogeneity: Understanding the Clonal Ancestry of Multifocal Disease. Eur. Urol. Oncol. 2021, 4, 358–369. [Google Scholar] [CrossRef]
- Panunzio, A.; Tafuri, A.; Princiotta, A.; Gentile, I.; Mazzucato, G.; Trabacchin, N.; Antonelli, A.; Cerruto, M.A. Omics in Urology: An Overview on Concepts, Current Status and Future Perspectives. Urologia 2021. [Google Scholar] [CrossRef]
- Liu, X.; Mangla, R.; Tian, W.; Qiu, X.; Li, D.; Walter, K.A.; Ekholm, S.; Johnson, M.D. The Preliminary Radiogenomics Association between MR Perfusion Imaging Parameters and Genomic Biomarkers, and Their Predictive Performance of Overall Survival in Patients with Glioblastoma. J. Neurooncol. 2017, 135, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Zinn, P.O.; Singh, S.K.; Kotrotsou, A.; Hassan, I.; Thomas, G.; Luedi, M.M.; Elakkad, A.; Elshafeey, N.; Idris, T.; Mosley, J.; et al. A Coclinical Radiogenomic Validation Study: Conserved Magnetic Resonance Radiomic Appearance of Periostin-Expressing Glioblastoma in Patients and Xenograft Models. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2018, 24, 6288–6299. [Google Scholar] [CrossRef] [Green Version]
- Hong, E.K.; Choi, S.H.; Shin, D.J.; Jo, S.W.; Yoo, R.-E.; Kang, K.M.; Yun, T.J.; Kim, J.-H.; Sohn, C.-H.; Park, S.-H.; et al. Radiogenomics Correlation between MR Imaging Features and Major Genetic Profiles in Glioblastoma. Eur. Radiol. 2018, 28, 4350–4361. [Google Scholar] [CrossRef] [PubMed]
- Kickingereder, P.; Bonekamp, D.; Nowosielski, M.; Kratz, A.; Sill, M.; Burth, S.; Wick, A.; Eidel, O.; Schlemmer, H.-P.; Radbruch, A.; et al. Radiogenomics of Glioblastoma: Machine Learning-Based Classification of Molecular Characteristics by Using Multiparametric and Multiregional MR Imaging Features. Radiology 2016, 281, 907–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Giger, M.L.; Lan, L.; Janardanan, J.; Sennett, C.A. Comparative Analysis of Image-Based Phenotypes of Mammographic Density and Parenchymal Patterns in Distinguishing between BRCA1/2 Cases, Unilateral Cancer Cases, and Controls. J. Med. Imaging Bellingham Wash 2014, 1, 031009. [Google Scholar] [CrossRef] [Green Version]
- Grimm, L.J.; Zhang, J.; Mazurowski, M.A. Computational Approach to Radiogenomics of Breast Cancer: Luminal A and Luminal B Molecular Subtypes Are Associated with Imaging Features on Routine Breast MRI Extracted Using Computer Vision Algorithms. J. Magn. Reson. Imaging 2015, 42, 902–907. [Google Scholar] [CrossRef]
- Mazurowski, M.A.; Zhang, J.; Grimm, L.J.; Yoon, S.C.; Silber, J.I. Radiogenomic Analysis of Breast Cancer: Luminal B Molecular Subtype Is Associated with Enhancement Dynamics at MR Imaging. Radiology 2014, 273, 365–372. [Google Scholar] [CrossRef]
- Zhu, Z.; Albadawy, E.; Saha, A.; Zhang, J.; Harowicz, M.R.; Mazurowski, M.A. Deep Learning for Identifying Radiogenomic Associations in Breast Cancer. Comput. Biol. Med. 2019, 109, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Karlo, C.A.; Di Paolo, P.L.; Chaim, J.; Hakimi, A.A.; Ostrovnaya, I.; Russo, P.; Hricak, H.; Motzer, R.; Hsieh, J.J.; Akin, O. Radiogenomics of Clear Cell Renal Cell Carcinoma: Associations between CT Imaging Features and Mutations. Radiology 2014, 270, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.-C.; Zhai, G.; Zhang, J.; Wang, Z.; Liu, G.; Wu, G.-Y.; Liang, D.; Zheng, H. Differentiation of Clear Cell and Non-Clear Cell Renal Cell Carcinomas by All-Relevant Radiomics Features from Multiphase CT: A VHL Mutation Perspective. Eur. Radiol. 2019, 29, 3996–4007. [Google Scholar] [CrossRef] [PubMed]
- Kocak, B.; Durmaz, E.S.; Ates, E.; Ulusan, M.B. Radiogenomics in Clear Cell Renal Cell Carcinoma: Machine Learning-Based High-Dimensional Quantitative CT Texture Analysis in Predicting PBRM1 Mutation Status. Am. J. Roentgenol. 2019, 212, W55–W63. [Google Scholar] [CrossRef] [PubMed]
- Norris, J.M.; Simpson, B.S.; Parry, M.A.; Allen, C.; Ball, R.; Freeman, A.; Kelly, D.; Kim, H.L.; Kirkham, A.; You, S.; et al. Genetic Landscape of Prostate Cancer Conspicuity on Multiparametric Magnetic Resonance Imaging: A Systematic Review and Bioinformatic Analysis. Eur. Urol. Open Sci. 2020, 20, 37–47. [Google Scholar] [CrossRef]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging Imaging and Genomics. Abdom. Radiol. 2019, 44, 1960–1984. [Google Scholar] [CrossRef] [Green Version]
- Fischer, S.; Tahoun, M.; Klaan, B.; Thierfelder, K.M.; Weber, M.-A.; Krause, B.J.; Hakenberg, O.; Fuellen, G.; Hamed, M. A Radiogenomic Approach for Decoding Molecular Mechanisms Underlying Tumor Progression in Prostate Cancer. Cancers 2019, 11, 1293. [Google Scholar] [CrossRef] [Green Version]
- Gillies, R.J.; Schabath, M.B. Radiomics Improves Cancer Screening and Early Detection. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2020, 29, 2556–2567. [Google Scholar] [CrossRef]
- Zhang, G.-M.-Y.; Han, Y.-Q.; Wei, J.-W.; Qi, Y.-F.; Gu, D.-S.; Lei, J.; Yan, W.-G.; Xiao, Y.; Xue, H.-D.; Feng, F.; et al. Radiomics Based on MRI as a Biomarker to Guide Therapy by Predicting Upgrading of Prostate Cancer From Biopsy to Radical Prostatectomy. J. Magn. Reson. Imaging 2020, 52, 1239–1248. [Google Scholar] [CrossRef] [PubMed]
- Orczyk, C.; Villers, A.; Rusinek, H.; Lepennec, V.; Bazille, C.; Giganti, F.; Mikheev, A.; Bernaudin, M.; Emberton, M.; Fohlen, A.; et al. Prostate Cancer Heterogeneity: Texture Analysis Score Based on Multiple Magnetic Resonance Imaging Sequences for Detection, Stratification and Selection of Lesions at Time of Biopsy. BJU Int. 2019, 124, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Kucharczyk, M.J.; Niazi, T. Multimodal Radiomic Features for the Predicting Gleason Score of Prostate Cancer. Cancers 2018, 10, 249. [Google Scholar] [CrossRef] [Green Version]
- Chaddad, A.; Niazi, T.; Probst, S.; Bladou, F.; Anidjar, M.; Bahoric, B. Predicting Gleason Score of Prostate Cancer Patients Using Radiomic Analysis. Front. Oncol. 2018, 8, 630. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Reynolds, H.M.; Parameswaran, B.; Wraith, D.; Finnegan, M.E.; Williams, S.; Haworth, A. Multiparametric MRI and Radiomics in Prostate Cancer: A Review. Australas. Phys. Eng. Sci. Med. 2019, 42, 3–25. [Google Scholar] [CrossRef] [PubMed]
- Bardis, M.D.; Houshyar, R.; Chang, P.D.; Ushinsky, A.; Glavis-Bloom, J.; Chahine, C.; Bui, T.-L.; Rupasinghe, M.; Filippi, C.G.; Chow, D.S. Applications of Artificial Intelligence to Prostate Multiparametric MRI (MpMRI): Current and Emerging Trends. Cancers 2020, 12, 1204. [Google Scholar] [CrossRef]
- Mortensen, M.A.; Borrelli, P.; Poulsen, M.H.; Gerke, O.; Enqvist, O.; Ulén, J.; Trägårdh, E.; Constantinescu, C.; Edenbrandt, L.; Lund, L.; et al. Artificial Intelligence-Based versus Manual Assessment of Prostate Cancer in the Prostate Gland: A Method Comparison Study. Clin. Physiol. Funct. Imaging 2019, 39, 399–406. [Google Scholar] [CrossRef]
- Ström, P.; Kartasalo, K.; Olsson, H.; Solorzano, L.; Delahunt, B.; Berney, D.M.; Bostwick, D.G.; Evans, A.J.; Grignon, D.J.; Humphrey, P.A.; et al. Artificial Intelligence for Diagnosis and Grading of Prostate Cancer in Biopsies: A Population-Based, Diagnostic Study. Lancet Oncol. 2020, 21, 222–232. [Google Scholar] [CrossRef]
- Goldenberg, S.L.; Nir, G.; Salcudean, S.E. A New Era: Artificial Intelligence and Machine Learning in Prostate Cancer. Nat. Rev. Urol. 2019, 16, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Raciti, P.; Sue, J.; Ceballos, R.; Godrich, R.; Kunz, J.D.; Kapur, S.; Reuter, V.; Grady, L.; Kanan, C.; Klimstra, D.S.; et al. Novel Artificial Intelligence System Increases the Detection of Prostate Cancer in Whole Slide Images of Core Needle Biopsies. Mod. Pathol. 2020, 33, 2058–2066. [Google Scholar] [CrossRef] [PubMed]
- Cuocolo, R.; Stanzione, A.; Ponsiglione, A.; Romeo, V.; Verde, F.; Creta, M.; La Rocca, R.; Longo, N.; Pace, L.; Imbriaco, M. Clinically Significant Prostate Cancer Detection on MRI: A Radiomic Shape Features Study. Eur. J. Radiol. 2019, 116, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Tătaru, O.S.; Vartolomei, M.D.; Rassweiler, J.J.; Virgil, O.; Lucarelli, G.; Porpiglia, F.; Amparore, D.; Manfredi, M.; Carrieri, G.; Falagario, U.; et al. Artificial Intelligence and Machine Learning in Prostate Cancer Patient Management-Current Trends and Future Perspectives. Diagnostics 2021, 11, 354. [Google Scholar] [CrossRef]
- Santone, A.; Brunese, M.C.; Donnarumma, F.; Guerriero, P.; Mercaldo, F.; Reginelli, A.; Miele, V.; Giovagnoni, A.; Brunese, L. Radiomic Features for Prostate Cancer Grade Detection through Formal Verification. Radiol. Med. 2021, 126, 688–697. [Google Scholar] [CrossRef]
- Gugliandolo, S.G.; Pepa, M.; Isaksson, L.J.; Marvaso, G.; Raimondi, S.; Botta, F.; Gandini, S.; Ciardo, D.; Volpe, S.; Riva, G.; et al. MRI-Based Radiomics Signature for Localized Prostate Cancer: A New Clinical Tool for Cancer Aggressiveness Prediction? Sub-Study of Prospective Phase II Trial on Ultra-Hypofractionated Radiotherapy (AIRC IG-13218). Eur. Radiol. 2021, 31, 716–728. [Google Scholar] [CrossRef]
- Gong, L.; Xu, M.; Fang, M.; Zou, J.; Yang, S.; Yu, X.; Xu, D.; Zhou, L.; Li, H.; He, B. Non-Invasive Prediction of Prostate Cancer Gleason Scores via Radiomics Analysis. 2019. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3411046 (accessed on 30 July 2021).
- Li, L.; Shiradkar, R.; Leo, P.; Algohary, A.; Fu, P.; Tirumani, S.H.; Mahran, A.; Buzzy, C.; Obmann, V.C.; Mansoori, B.; et al. A Novel Imaging Based Nomogram for Predicting Post-Surgical Biochemical Recurrence and Adverse Pathology of Prostate Cancer from Pre-Operative Bi-Parametric MRI. EBioMedicine 2021, 63, 103163. [Google Scholar] [CrossRef]
- Sunoqrot, M.R.S.; Selnæs, K.M.; Sandsmark, E.; Nketiah, G.A.; Zavala-Romero, O.; Stoyanova, R.; Bathen, T.F.; Elschot, M. A Quality Control System for Automated Prostate Segmentation on T2-Weighted MRI. Diagnostics 2020, 10, 714. [Google Scholar] [CrossRef]
- Hu, L.; Zhou, D.W.; Fu, C.X.; Benkert, T.; Jiang, C.Y.; Li, R.T.; Wei, L.M.; Zhao, J.G. Advanced Zoomed Diffusion-Weighted Imaging vs. Full-Field-of-View Diffusion-Weighted Imaging in Prostate Cancer Detection: A Radiomic Features Study. Eur. Radiol. 2021, 31, 1760–1769. [Google Scholar] [CrossRef] [PubMed]
- Giambelluca, D.; Cannella, R.; Vernuccio, F.; Comelli, A.; Pavone, A.; Salvaggio, L.; Galia, M.; Midiri, M.; Lagalla, R.; Salvaggio, G. PI-RADS 3 Lesions: Role of Prostate MRI Texture Analysis in the Identification of Prostate Cancer. Curr. Probl. Diagn. Radiol. 2021, 50, 175–185. [Google Scholar] [CrossRef]
- Khalvati, F.; Zhang, J.; Chung, A.G.; Shafiee, M.J.; Wong, A.; Haider, M.A. MPCaD: A Multi-Scale Radiomics-Driven Framework for Automated Prostate Cancer Localization and Detection. BMC Med. Imaging 2018, 18, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiradkar, R.; Podder, T.K.; Algohary, A.; Viswanath, S.; Ellis, R.J.; Madabhushi, A. Radiomics Based Targeted Radiotherapy Planning (Rad-TRaP): A Computational Framework for Prostate Cancer Treatment Planning with MRI. Radiat. Oncol. Lond. Engl. 2016, 11, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.L.; Lee, J.; Craig, T.; Berlin, A.; Chung, P.; Ménard, C.; Foltz, W.D. Changes in Apparent Diffusion Coefficient Radiomics Features during Dose-Painted Radiotherapy and High Dose Rate Brachytherapy for Prostate Cancer. Phys. Imaging Radiat. Oncol. 2019, 9, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Mostafaei, S.; Abdollahi, H.; Kazempour Dehkordi, S.; Shiri, I.; Razzaghdoust, A.; Zoljalali Moghaddam, S.H.; Saadipoor, A.; Koosha, F.; Cheraghi, S.; Mahdavi, S.R. CT Imaging Markers to Improve Radiation Toxicity Prediction in Prostate Cancer Radiotherapy by Stacking Regression Algorithm. Radiol. Med. 2020, 125, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Jiao, Y.; Zhang, Y.; Ren, X.; Li, P.; Yu, Q.; Zhang, Q.; Wang, Q.; Fu, S. Imaging-Based Individualized Response Prediction Of Carbon Ion Radiotherapy For Prostate Cancer Patients. Cancer Manag. Res. 2019, 11, 9121–9131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kairemo, K.; Kappadath, S.C.; Joensuu, T.; Macapinlac, H.A. A Retrospective Comparative Study of Sodium Fluoride (NaF-18)-PET/CT and Fluorocholine (F-18-CH) PET/CT in the Evaluation of Skeletal Metastases in Metastatic Prostate Cancer Using a Volumetric 3-D Radiomics Analysis. Diagnostics 2020, 11, 17. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, H.; Mofid, B.; Shiri, I.; Razzaghdoust, A.; Saadipoor, A.; Mahdavi, A.; Galandooz, H.M.; Mahdavi, S.R. Machine Learning-Based Radiomic Models to Predict Intensity-Modulated Radiation Therapy Response, Gleason Score and Stage in Prostate Cancer. Radiol. Med. 2019, 124, 555–567. [Google Scholar] [CrossRef]
- Macomber, M.W.; Phillips, M.; Tarapov, I.; Jena, R.; Nori, A.; Carter, D.; Folgoc, L.L.; Criminisi, A.; Nyflot, M.J. Autosegmentation of Prostate Anatomy for Radiation Treatment Planning Using Deep Decision Forests of Radiomic Features. Phys. Med. Biol. 2018, 63, 235002. [Google Scholar] [CrossRef] [PubMed]
- Bourbonne, V.; Vallières, M.; Lucia, F.; Doucet, L.; Visvikis, D.; Tissot, V.; Pradier, O.; Hatt, M.; Schick, U. MRI-Derived Radiomics to Guide Post-Operative Management for High-Risk Prostate Cancer. Front. Oncol. 2019, 9, 807. [Google Scholar] [CrossRef]
- Zhong, Q.-Z.; Long, L.-H.; Liu, A.; Li, C.-M.; Xiu, X.; Hou, X.-Y.; Wu, Q.-H.; Gao, H.; Xu, Y.-G.; Zhao, T.; et al. Radiomics of Multiparametric MRI to Predict Biochemical Recurrence of Localized Prostate Cancer After Radiation Therapy. Front. Oncol. 2020, 10, 731. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, D.G.; Ruinelli, L.; Piliero, M.A.; van der Gaag, L.C.; Pesce, G.A.; Valli, M.; Bosetti, M.; Presilla, S.; Richetti, A.; Deantonio, L. Cone-Beam Computed Tomography-Based Radiomics in Prostate Cancer: A Mono-Institutional Study. Strahlenther. Onkol. 2020, 196, 943–951. [Google Scholar] [CrossRef]
- Isaksson, L.J.; Pepa, M.; Zaffaroni, M.; Marvaso, G.; Alterio, D.; Volpe, S.; Corrao, G.; Augugliaro, M.; Starzyńska, A.; Leonardi, M.C.; et al. Machine Learning-Based Models for Prediction of Toxicity Outcomes in Radiotherapy. Front. Oncol. 2020, 10, 790. [Google Scholar] [CrossRef]
- Bourbonne, V.; Fournier, G.; Vallières, M.; Lucia, F.; Doucet, L.; Tissot, V.; Cuvelier, G.; Hue, S.; Le Penn Du, H.; Perdriel, L.; et al. External Validation of an MRI-Derived Radiomics Model to Predict Biochemical Recurrence after Surgery for High-Risk Prostate Cancer. Cancers 2020, 12, 814. [Google Scholar] [CrossRef] [Green Version]
- Abdollahi, H.; Mahdavi, S.R.; Mofid, B.; Bakhshandeh, M.; Razzaghdoust, A.; Saadipoor, A.; Tanha, K. Rectal Wall MRI Radiomics in Prostate Cancer Patients: Prediction of and Correlation with Early Rectal Toxicity. Int. J. Radiat. Biol. 2018, 94, 829–837. [Google Scholar] [CrossRef]
- Dinis Fernandes, C.; Dinh, C.V.; Walraven, I.; Heijmink, S.W.; Smolic, M.; van Griethuysen, J.J.M.; Simões, R.; Losnegård, A.; van der Poel, H.G.; Pos, F.J.; et al. Biochemical Recurrence Prediction after Radiotherapy for Prostate Cancer with T2w Magnetic Resonance Imaging Radiomic Features. Phys. Imaging Radiat. Oncol. 2018, 7, 9–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, H.; Tanha, K.; Mofid, B.; Razzaghdoust, A.; Saadipoor, A.; Khalafi, L.; Bakhshandeh, M.; Mahdavi, S.R. MRI Radiomic Analysis of IMRT-Induced Bladder Wall Changes in Prostate Cancer Patients: A Relationship with Radiation Dose and Toxicity. J. Med. Imaging Radiat. Sci. 2019, 50, 252–260. [Google Scholar] [CrossRef]
- Wong, J.; Fong, A.; McVicar, N.; Smith, S.; Giambattista, J.; Wells, D.; Kolbeck, C.; Giambattista, J.; Gondara, L.; Alexander, A. Comparing Deep Learning-Based Auto-Segmentation of Organs at Risk and Clinical Target Volumes to Expert Inter-Observer Variability in Radiotherapy Planning. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2020, 144, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Wildeboer, R.R.; van Sloun, R.J.G.; Wijkstra, H.; Mischi, M. Artificial Intelligence in Multiparametric Prostate Cancer Imaging with Focus on Deep-Learning Methods. Comput. Methods Programs Biomed. 2020, 189, 105316. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The Facts and the Challenges of Image Analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef]
- WHO. WHO Definitions of Genetics and Genomics. Available online: http://www.who.int/genomics/geneticsVSgenomics/en/ (accessed on 12 March 2021).
- Roth, S.C. What Is Genomic Medicine? J. Med. Libr. Assoc. 2019, 107, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Wise, A.L.; Manolio, T.A.; Mensah, G.A.; Peterson, J.F.; Roden, D.M.; Tamburro, C.; Williams, M.S.; Green, E.D. Genomic Medicine for Undiagnosed Diseases. Lancet 2019, 394, 533–540. [Google Scholar] [CrossRef]
- Visvikis, D.; Cheze Le Rest, C.; Jaouen, V.; Hatt, M. Artificial Intelligence, Machine (Deep) Learning and Radio(Geno)Mics: Definitions and Nuclear Medicine Imaging Applications. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2630–2637. [Google Scholar] [CrossRef]
- Krauss, T.; Engel, H.; Jilg, C.A.; Gratzke, C.; Bamberg, F.; Benndorf, M. MRI Phenotype of the Prostate: Transition Zone Radiomics Analysis Improves Explanation of Prostate-Specific Antigen (PSA) Serum Level Compared to Volume Measurement Alone. Eur. J. Radiol. 2020, 129, 109063. [Google Scholar] [CrossRef] [PubMed]
- Wildeboer, R.R.; Mannaerts, C.K.; van Sloun, R.J.G.; Budäus, L.; Tilki, D.; Wijkstra, H.; Salomon, G.; Mischi, M. Automated Multiparametric Localization of Prostate Cancer Based on B-Mode, Shear-Wave Elastography, and Contrast-Enhanced Ultrasound Radiomics. Eur. Radiol. 2020, 30, 806–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.; Ford, J.C.; Dogan, N.; Padgett, K.R.; Breto, A.L.; Abramowitz, M.C.; Dal Pra, A.; Pollack, A.; Stoyanova, R. Magnetic Resonance Imaging (MRI)-Based Radiomics for Prostate Cancer Radiotherapy. Transl. Androl. Urol. 2018, 7, 445–458. [Google Scholar] [CrossRef] [PubMed]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for Prostate Cancer Characterization: Combined Use of Radiomics Model with PI-RADS and Clinical Parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Zhang, S.; Wei, J.; Zhang, G.; Lei, J.; Yan, W.; Xiao, Y.; Yan, S.; Xue, H.; Feng, F.; et al. Multiparametric MRI-Based Radiomics for Prostate Cancer Screening With PSA in 4-10 Ng/ML to Reduce Unnecessary Biopsies. J. Magn. Reson. Imaging 2020, 51, 1890–1899. [Google Scholar] [CrossRef]
- Leech, M.; Osman, S.; Jain, S.; Marignol, L. Mini Review: Personalization of the Radiation Therapy Management of Prostate Cancer Using MRI-Based Radiomics. Cancer Lett. 2021, 498, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Bagher-Ebadian, H.; Janic, B.; Liu, C.; Pantelic, M.; Hearshen, D.; Elshaikh, M.; Movsas, B.; Chetty, I.J.; Wen, N. Detection of Dominant Intra-Prostatic Lesions in Patients With Prostate Cancer Using an Artificial Neural Network and MR Multi-Modal Radiomics Analysis. Front. Oncol. 2019, 9, 1313. [Google Scholar] [CrossRef]
- Dulhanty, C.; Wang, L.; Cheng, M.; Gunraj, H.; Khalvati, F.; Haider, M.A.; Wong, A. Radiomics Driven Diffusion Weighted Imaging Sensing Strategies for Zone-Level Prostate Cancer Sensing. Sensors 2020, 20, 1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Li, M.; Gu, Y.; Zhang, Y.; Yang, S.; Wei, C.; Wu, J.; Li, X.; Zhao, W.; Shen, J. Prostate Cancer Differentiation and Aggressiveness: Assessment With a Radiomic-Based Model vs. PI-RADS V2. J. Magn. Reson. Imaging 2019, 49, 875–884. [Google Scholar] [CrossRef] [Green Version]
- Algohary, A.; Shiradkar, R.; Pahwa, S.; Purysko, A.; Verma, S.; Moses, D.; Shnier, R.; Haynes, A.-M.; Delprado, W.; Thompson, J.; et al. Combination of Peri-Tumoral and Intra-Tumoral Radiomic Features on Bi-Parametric MRI Accurately Stratifies Prostate Cancer Risk: A Multi-Site Study. Cancers 2020, 12, 2200. [Google Scholar] [CrossRef]
- Lu, H.; Parra, N.A.; Qi, J.; Gage, K.; Li, Q.; Fan, S.; Feuerlein, S.; Pow-Sang, J.; Gillies, R.; Choi, J.W.; et al. Repeatability of Quantitative Imaging Features in Prostate Magnetic Resonance Imaging. Front. Oncol. 2020, 10, 551. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Formal Methods for Prostate Cancer Gleason Score and Treatment Prediction Using Radiomic Biomarkers. Magn. Reson. Imaging 2020, 66, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Schick, U.; Lucia, F.; Dissaux, G.; Visvikis, D.; Badic, B.; Masson, I.; Pradier, O.; Bourbonne, V.; Hatt, M. MRI-Derived Radiomics: Methodology and Clinical Applications in the Field of Pelvic Oncology. Br. J. Radiol. 2019, 92, 20190105. [Google Scholar] [CrossRef] [PubMed]
- Delgadillo, R.; Ford, J.C.; Abramowitz, M.C.; Dal Pra, A.; Pollack, A.; Stoyanova, R. The Role of Radiomics in Prostate Cancer Radiotherapy. Strahlenther. Onkol. 2020, 196, 900–912. [Google Scholar] [CrossRef] [PubMed]
- Khalvati, F.; Wong, A.; Haider, M.A. Automated Prostate Cancer Detection via Comprehensive Multi-Parametric Magnetic Resonance Imaging Texture Feature Models. BMC Med. Imaging 2015, 15, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madabhushi, A.; Feldman, M.D.; Metaxas, D.N.; Tomaszeweski, J.; Chute, D. Automated Detection of Prostatic Adenocarcinoma from High-Resolution Ex Vivo MRI. IEEE Trans. Med. Imaging 2005, 24, 1611–1625. [Google Scholar] [CrossRef]
- Lopes, R.; Ayache, A.; Makni, N.; Puech, P.; Villers, A.; Mordon, S.; Betrouni, N. Prostate Cancer Characterization on MR Images Using Fractal Features. Med. Phys. 2011, 38, 83–95. [Google Scholar] [CrossRef]
- Cameron, A.; Khalvati, F.; Haider, M.A.; Wong, A. MAPS: A Quantitative Radiomics Approach for Prostate Cancer Detection. IEEE Trans. Biomed. Eng. 2016, 63, 1145–1156. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, J.; Zhang, Y.-D.; Hou, Y.; Yan, X.; Wang, Y.; Zhou, M.; Yao, Y.-F.; Yang, G. FeAture Explorer (FAE): A Tool for Developing and Comparing Radiomics Models. PLoS ONE 2020, 15, e0237587. [Google Scholar] [CrossRef]
- Castillo, J.M.T.; Starmans, M.P.A.; Arif, M.; Niessen, W.J.; Klein, S.; Bangma, C.H.; Schoots, I.G.; Veenland, J.F. A Multi-Center, Multi-Vendor Study to Evaluate the Generalizability of a Radiomics Model for Classifying Prostate Cancer: High Grade vs. Low Grade. Diagnostics 2021, 11, 369. [Google Scholar] [CrossRef]
- Ma, S.; Xie, H.; Wang, H.; Yang, J.; Han, C.; Wang, X.; Zhang, X. Preoperative Prediction of Extracapsular Extension: Radiomics Signature Based on Magnetic Resonance Imaging to Stage Prostate Cancer. Mol. Imaging Biol. 2020, 22, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Xie, H.; Wang, H.; Han, C.; Yang, J.; Lin, Z.; Li, Y.; He, Q.; Wang, R.; Cui, Y.; et al. MRI-Based Radiomics Signature for the Preoperative Prediction of Extracapsular Extension of Prostate Cancer. J. Magn. Reson. Imaging 2019, 50, 1914–1925. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Wang, X.; Fu, C.; Wei, X.; Bao, J.; Ji, X.; Bai, H.; Xia, W.; Gao, X.; Huang, Y.; et al. MRI-Based Radiomics Models to Assess Prostate Cancer, Extracapsular Extension and Positive Surgical Margins. Cancer Imaging 2021, 21, 46. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Radiomics for Gleason Score Detection through Deep Learning. Sensors 2020, 20, 5411. [Google Scholar] [CrossRef]
- Wang, J.; Wu, C.-J.; Bao, M.-L.; Zhang, J.; Wang, X.-N.; Zhang, Y.-D. Machine Learning-Based Analysis of MR Radiomics Can Help to Improve the Diagnostic Performance of PI-RADS v2 in Clinically Relevant Prostate Cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef]
- Kwon, D.; Reis, I.M.; Breto, A.L.; Tschudi, Y.; Gautney, N.; Zavala-Romero, O.; Lopez, C.; Ford, J.C.; Punnen, S.; Pollack, A.; et al. Classification of Suspicious Lesions on Prostate Multiparametric MRI Using Machine Learning. J. Med. Imaging Bellingham Wash 2018, 5, 034502. [Google Scholar] [CrossRef]
- Parra, N.A.; Lu, H.; Li, Q.; Stoyanova, R.; Pollack, A.; Punnen, S.; Choi, J.; Abdalah, M.; Lopez, C.; Gage, K.; et al. Predicting Clinically Significant Prostate Cancer Using DCE-MRI Habitat Descriptors. Oncotarget 2018, 9, 37125–37136. [Google Scholar] [CrossRef]
- Penzias, G.; Singanamalli, A.; Elliott, R.; Gollamudi, J.; Shih, N.; Feldman, M.; Stricker, P.D.; Delprado, W.; Tiwari, S.; Böhm, M.; et al. Identifying the Morphologic Basis for Radiomic Features in Distinguishing Different Gleason Grades of Prostate Cancer on MRI: Preliminary Findings. PLoS ONE 2018, 13, e0200730. [Google Scholar] [CrossRef] [Green Version]
- Min, X.; Li, M.; Dong, D.; Feng, Z.; Zhang, P.; Ke, Z.; You, H.; Han, F.; Ma, H.; Tian, J.; et al. Multi-Parametric MRI-Based Radiomics Signature for Discriminating between Clinically Significant and Insignificant Prostate Cancer: Cross-Validation of a Machine Learning Method. Eur. J. Radiol. 2019, 115, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Brancato, V.; Aiello, M.; Basso, L.; Monti, S.; Palumbo, L.; Di Costanzo, G.; Salvatore, M.; Ragozzino, A.; Cavaliere, C. Evaluation of a Multiparametric MRI Radiomic-Based Approach for Stratification of Equivocal PI-RADS 3 and Upgraded PI-RADS 4 Prostatic Lesions. Sci. Rep. 2021, 11, 643. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Bao, M.-L.; Wu, C.-J.; Zhang, J.; Zhang, Y.-D.; Shi, H.-B. A Radiomics Machine Learning-Based Redefining Score Robustly Identifies Clinically Significant Prostate Cancer in Equivocal PI-RADS Score 3 Lesions. Abdom. Radiol. 2020, 45, 4223–4234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, W.; Yue, X.; Shen, J.; Gao, C.; Pang, P.; Cui, F.; Xu, M. Development of a Novel, Multi-Parametric, MRI-Based Radiomic Nomogram for Differentiating Between Clinically Significant and Insignificant Prostate Cancer. Front. Oncol. 2020, 10, 888. [Google Scholar] [CrossRef]
- Gong, L.; Xu, M.; Fang, M.; Zou, J.; Yang, S.; Yu, X.; Xu, D.; Zhou, L.; Li, H.; He, B.; et al. Noninvasive Prediction of High-Grade Prostate Cancer via Biparametric MRI Radiomics. J. Magn. Reson. Imaging 2020, 52, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Bernatz, S.; Ackermann, J.; Mandel, P.; Kaltenbach, B.; Zhdanovich, Y.; Harter, P.N.; Döring, C.; Hammerstingl, R.; Bodelle, B.; Smith, K.; et al. Comparison of Machine Learning Algorithms to Predict Clinically Significant Prostate Cancer of the Peripheral Zone with Multiparametric MRI Using Clinical Assessment Categories and Radiomic Features. Eur. Radiol. 2020, 30, 6757–6769. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, T.; Zhao, W.; Wei, C.; Li, X.; Duan, S.; Ji, L.; Lu, Z.; Shen, J. Radiomics Prediction Model for the Improved Diagnosis of Clinically Significant Prostate Cancer on Biparametric MRI. Quant. Imaging Med. Surg. 2020, 10, 368–379. [Google Scholar] [CrossRef]
- Bonekamp, D.; Kohl, S.; Wiesenfarth, M.; Schelb, P.; Radtke, J.P.; Götz, M.; Kickingereder, P.; Yaqubi, K.; Hitthaler, B.; Gählert, N.; et al. Radiomic Machine Learning for Characterization of Prostate Lesions with MRI: Comparison to ADC Values. Radiology 2018, 289, 128–137. [Google Scholar] [CrossRef]
- Bleker, J.; Kwee, T.C.; Dierckx, R.A.J.O.; de Jong, I.J.; Huisman, H.; Yakar, D. Multiparametric MRI and Auto-Fixed Volume of Interest-Based Radiomics Signature for Clinically Significant Peripheral Zone Prostate Cancer. Eur. Radiol. 2020, 30, 1313–1324. [Google Scholar] [CrossRef] [Green Version]
- Losnegård, A.; Reisæter, L.A.R.; Halvorsen, O.J.; Jurek, J.; Assmus, J.; Arnes, J.B.; Honoré, A.; Monssen, J.A.; Andersen, E.; Haldorsen, I.S.; et al. Magnetic Resonance Radiomics for Prediction of Extraprostatic Extension in Non-Favorable Intermediate- and High-Risk Prostate Cancer Patients. Acta Radiol. 2020, 61, 1570–1579. [Google Scholar] [CrossRef]
- Cysouw, M.C.F.; Jansen, B.H.E.; van de Brug, T.; Oprea-Lager, D.E.; Pfaehler, E.; de Vries, B.M.; van Moorselaar, R.J.A.; Hoekstra, O.S.; Vis, A.N.; Boellaard, R. Machine Learning-Based Analysis of [18F]DCFPyL PET Radiomics for Risk Stratification in Primary Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 340–349. [Google Scholar] [CrossRef]
- Rutman, A.M.; Kuo, M.D. Radiogenomics: Creating a Link between Molecular Diagnostics and Diagnostic Imaging. Eur. J. Radiol. 2009, 70, 232–241. [Google Scholar] [CrossRef]
- Grossi, V.; Lucarelli, G.; Forte, G.; Peserico, A.; Matrone, A.; Germani, A.; Rutigliano, M.; Stella, A.; Bagnulo, R.; Loconte, D.; et al. Loss of STK11 Expression Is an Early Event in Prostate Carcinogenesis and Predicts Therapeutic Response to Targeted Therapy against MAPK/P38. Autophagy 2015, 11, 2102–2113. [Google Scholar] [CrossRef] [Green Version]
- Clinton, T.N.; Bagrodia, A.; Lotan, Y.; Margulis, V.; Raj, G.V.; Woldu, S.L. Tissue-Based Biomarkers in Prostate Cancer. Expert Rev. Precis. Med. Drug Dev. 2017, 2, 249–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.A.; Cooperberg, M.R.; Magi-Galluzzi, C.; Simko, J.P.; Falzarano, S.M.; Maddala, T.; Chan, J.M.; Li, J.; Cowan, J.E.; Tsiatis, A.C.; et al. A 17-Gene Assay to Predict Prostate Cancer Aggressiveness in the Context of Gleason Grade Heterogeneity, Tumor Multifocality, and Biopsy Undersampling. Eur. Urol. 2014, 66, 550–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzick, J.; Berney, D.M.; Fisher, G.; Mesher, D.; Møller, H.; Reid, J.E.; Perry, M.; Park, J.; Younus, A.; Gutin, A.; et al. Prognostic Value of a Cell Cycle Progression Signature for Prostate Cancer Death in a Conservatively Managed Needle Biopsy Cohort. Br. J. Cancer 2012, 106, 1095–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzick, J.; Swanson, G.P.; Fisher, G.; Brothman, A.R.; Berney, D.M.; Reid, J.E.; Mesher, D.; Speights, V.O.; Stankiewicz, E.; Foster, C.S.; et al. Prognostic Value of an RNA Expression Signature Derived from Cell Cycle Proliferation Genes in Patients with Prostate Cancer: A Retrospective Study. Lancet Oncol. 2011, 12, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Cooperberg, M.R.; Simko, J.P.; Cowan, J.E.; Reid, J.E.; Djalilvand, A.; Bhatnagar, S.; Gutin, A.; Lanchbury, J.S.; Swanson, G.P.; Stone, S.; et al. Validation of a Cell-Cycle Progression Gene Panel to Improve Risk Stratification in a Contemporary Prostatectomy Cohort. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- Renard-Penna, R.; Cancel-Tassin, G.; Comperat, E.; Varinot, J.; Léon, P.; Roupret, M.; Mozer, P.; Vaessen, C.; Lucidarme, O.; Bitker, M.-O.; et al. Multiparametric Magnetic Resonance Imaging Predicts Postoperative Pathology but Misses Aggressive Prostate Cancers as Assessed by Cell Cycle Progression Score. J. Urol. 2015, 194, 1617–1623. [Google Scholar] [CrossRef]
- Klein, E.A.; Haddad, Z.; Yousefi, K.; Lam, L.L.C.; Wang, Q.; Choeurng, V.; Palmer-Aronsten, B.; Buerki, C.; Davicioni, E.; Li, J.; et al. Decipher Genomic Classifier Measured on Prostate Biopsy Predicts Metastasis Risk. Urology 2016, 90, 148–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klein, E.A.; Yousefi, K.; Haddad, Z.; Choeurng, V.; Buerki, C.; Stephenson, A.J.; Li, J.; Kattan, M.W.; Magi-Galluzzi, C.; Davicioni, E. A Genomic Classifier Improves Prediction of Metastatic Disease within 5 Years after Surgery in Node-Negative High-Risk Prostate Cancer Patients Managed by Radical Prostatectomy without Adjuvant Therapy. Eur. Urol. 2015, 67, 778–786. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Davicioni, E.; Crisan, A.; Jenkins, R.B.; Ghadessi, M.; Karnes, R.J. Combined Value of Validated Clinical and Genomic Risk Stratification Tools for Predicting Prostate Cancer Mortality in a High-Risk Prostatectomy Cohort. Eur. Urol. 2015, 67, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Spratt, D.E.; Zhang, J.; Santiago-Jiménez, M.; Dess, R.T.; Davis, J.W.; Den, R.B.; Dicker, A.P.; Kane, C.J.; Pollack, A.; Stoyanova, R.; et al. Development and Validation of a Novel Integrated Clinical-Genomic Risk Group Classification for Localized Prostate Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 581–590. [Google Scholar] [CrossRef]
- McCann, S.M.; Jiang, Y.; Fan, X.; Wang, J.; Antic, T.; Prior, F.; VanderWeele, D.; Oto, A. Quantitative Multiparametric MRI Features and PTEN Expression of Peripheral Zone Prostate Cancer: A Pilot Study. Am. J. Roentgenol. 2016, 206, 559–565. [Google Scholar] [CrossRef]
- Jamshidi, N.; Margolis, D.J.; Raman, S.; Huang, J.; Reiter, R.E.; Kuo, M.D. Multiregional Radiogenomic Assessment of Prostate Microenvironments with Multiparametric MR Imaging and DNA Whole-Exome Sequencing of Prostate Glands with Adenocarcinoma. Radiology 2017, 284, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Sugano, D.; Sanford, D.; Abreu, A.; Duddalwar, V.; Gill, I.; Cacciamani, G.E. Impact of Radiomics on Prostate Cancer Detection: A Systematic Review of Clinical Applications. Curr. Opin. Urol. 2020, 30, 754–781. [Google Scholar] [CrossRef]
- Schoots, I.G.; Moore, C.M.; Rouvière, O. Role of MRI in Low-Risk Prostate Cancer: Finding the Wolf in Sheep’s Clothing or the Sheep in Wolf’s Clothing? Curr. Opin. Urol. 2017, 27, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Pond, G.; Loblaw, A.; Sugar, L.; Moussa, M.; Berman, D.; Van der Kwast, T.; Vesprini, D.; Milot, L.; Kebabdjian, M.; et al. Randomized Study of Systematic Biopsy Versus Magnetic Resonance Imaging and Targeted and Systematic Biopsy in Men on Active Surveillance (ASIST): 2-Year Postbiopsy Follow-Up. Eur. Urol. 2020, 77, 311–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Houlahan, K.E.; Salmasi, A.; Sadun, T.Y.; Pooli, A.; Felker, E.R.; Livingstone, J.; Huang, V.; Raman, S.S.; Ahuja, P.; Sisk, A.E.; et al. Molecular Hallmarks of Multiparametric Magnetic Resonance Imaging Visibility in Prostate Cancer. Eur. Urol. 2019, 76, 18–23. [Google Scholar] [CrossRef]
- Fraser, M.; Sabelnykova, V.Y.; Yamaguchi, T.N.; Heisler, L.E.; Livingstone, J.; Huang, V.; Shiah, Y.-J.; Yousif, F.; Lin, X.; Masella, A.P.; et al. Genomic Hallmarks of Localized, Non-Indolent Prostate Cancer. Nature 2017, 541, 359–364. [Google Scholar] [CrossRef]
- Norris, J.M.; Simpson, B.S.; Parry, M.A.; Kasivisvanathan, V.; Allen, C.; Ball, R.; Freeman, A.; Kelly, D.; Kirkham, A.; Whitaker, H.C.; et al. Genetic Correlates of Prostate Cancer Visibility (and Invisibility) on Multiparametric Magnetic Resonance Imaging: It’s Time to Take Stock. BJU Int. 2020, 125, 340–342. [Google Scholar] [CrossRef] [Green Version]
- Parry, M.A.; Srivastava, S.; Ali, A.; Cannistraci, A.; Antonello, J.; Barros-Silva, J.D.; Ubertini, V.; Ramani, V.; Lau, M.; Shanks, J.; et al. Genomic Evaluation of Multiparametric Magnetic Resonance Imaging-Visible and -Nonvisible Lesions in Clinically Localised Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, G.; Sonpavde, G.; Pond, G.; Lucarelli, G.; Rossetti, S.; Facchini, G.; Scagliarini, S.; Cartenì, G.; Federico, P.; Daniele, B.; et al. Statin Use and Survival in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone Acetate. Eur. Urol. Focus 2018, 4, 874–879. [Google Scholar] [CrossRef]
- Gordon, J.A.; Buonerba, C.; Pond, G.; Crona, D.; Gillessen, S.; Lucarelli, G.; Rossetti, S.; Dorff, T.; Artale, S.; Locke, J.A.; et al. Statin Use and Survival in Patients with Metastatic Castration-Resistant Prostate Cancer Treated with Abiraterone or Enzalutamide after Docetaxel Failure: The International Retrospective Observational STABEN Study. Oncotarget 2018, 9, 19861–19873. [Google Scholar] [CrossRef]
- Radtke, J.P.; Takhar, M.; Bonekamp, D.; Kesch, C.; Erho, N.; du Plessis, M.; Buerki, C.; Ong, K.; Davicioni, E.; Hohenfellner, M.; et al. Transcriptome Wide Analysis of Magnetic Resonance Imaging-Targeted Biopsy and Matching Surgical Specimens from High-Risk Prostate Cancer Patients Treated with Radical Prostatectomy: The Target Must Be Hit. Eur. Urol. Focus 2018, 4, 540–546. [Google Scholar] [CrossRef]
- Porreca, A.; Del Giudice, F.; Giampaoli, M.; D’Agostino, D.; Romagnoli, D.; Corsi, P.; Del Rosso, A.; Maggi, M.; Chung, B.I.; Ferro, M.; et al. Adding Systematic Biopsy to Magnetic Resonance Ultrasound Fusion Targeted Biopsy of the Prostate in Men with Previous Negative Biopsy or Enrolled in Active Surveillance Programs: A Prospective Single Center, Randomized Study. Medicine 2020, 99, e22059. [Google Scholar] [CrossRef] [PubMed]
- De Luca, S.; Passera, R.; Cattaneo, G.; Manfredi, M.; Mele, F.; Fiori, C.; Bollito, E.; Cirillo, S.; Porpiglia, F. High Prostate Cancer Gene 3 (PCA3) Scores Are Associated with Elevated Prostate Imaging Reporting and Data System (PI-RADS) Grade and Biopsy Gleason Score, at Magnetic Resonance Imaging/Ultrasonography Fusion Software-Based Targeted Prostate Biopsy after a Previous Negative Standard Biopsy. BJU Int. 2016, 118, 723–730. [Google Scholar] [CrossRef]
- Alkasab, T.; Ahmad, A.; Rechard, P.; Mohamed, A.; Garisto, J.; Fadaak, K.; Finelli, A.; Hamilton, R.; Kulkarni, G.; Jewett, M.; et al. Mp53-12 the Role of Prostate Cancer Antigen 3 (Pca3) Test and Multi-Parametric Prostatic Magnetic Resonance Imaging (Mpmri) among Patients with Prior Negative Biopsy: Correlation with Radical Prostatectomy Pathology. J. Urol. 2016, 195, e701–e702. [Google Scholar] [CrossRef]
- Fenstermaker, M.; Mendhiratta, N.; Bjurlin, M.A.; Meng, X.; Rosenkrantz, A.B.; Huang, R.; Deng, F.-M.; Zhou, M.; Huang, W.C.; Lepor, H.; et al. Risk Stratification by Urinary Prostate Cancer Gene 3 Testing Before Magnetic Resonance Imaging-Ultrasound Fusion-Targeted Prostate Biopsy Among Men With No History of Biopsy. Urology 2017, 99, 174–179. [Google Scholar] [CrossRef]
- Perlis, N.; Al-Kasab, T.; Ahmad, A.; Goldberg, E.; Fadak, K.; Sayyid, R.; Finelli, A.; Kulkarni, G.; Hamilton, R.; Zlotta, A.; et al. Defining a Cohort That May Not Require Repeat Prostate Biopsy Based on PCA3 Score and Magnetic Resonance Imaging: The Dual Negative Effect. J. Urol. 2018, 199, 1182–1187. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.T.; Ghabili, K.; Levi, A.; Humphrey, P.A.; Sprenkle, P.C. Prostate Cancer Genomic Classifier Relates More Strongly to Gleason Grade Group Than Prostate Imaging Reporting and Data System Score in Multiparametric Prostate Magnetic Resonance Imaging-Ultrasound Fusion Targeted Biopsies. Urology 2019, 125, 64–72. [Google Scholar] [CrossRef]
- Falagario, U.G.; Beksac, A.T.; Martini, A.; Cumarasamy, S.; Gupta, A.; Prasad, S.; Thulasidass, H.; Shah, Q.N.; Jayaratna, I.; Lewis, S.; et al. Defining Prostate Cancer at Favorable Intermediate Risk: The Potential Utility of Magnetic Resonance Imaging and Genomic Tests. J. Urol. 2019, 202, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Jambor, I.; Falagario, U.; Ratnani, P.; Perez, I.M.; Demir, K.; Merisaari, H.; Sobotka, S.; Haines, G.K.; Martini, A.; Beksac, A.T.; et al. Prediction of Biochemical Recurrence in Prostate Cancer Patients Who Underwent Prostatectomy Using Routine Clinical Prostate Multiparametric MRI and Decipher Genomic Score. J. Magn. Reson. Imaging 2020, 51, 1075–1085. [Google Scholar] [CrossRef]
- Beksac, A.T.; Cumarasamy, S.; Falagario, U.; Xu, P.; Takhar, M.; Alshalalfa, M.; Gupta, A.; Prasad, S.; Martini, A.; Thulasidass, H.; et al. Multiparametric Magnetic Resonance Imaging Features Identify Aggressive Prostate Cancer at the Phenotypic and Transcriptomic Level. J. Urol. 2018, 200, 1241–1249. [Google Scholar] [CrossRef]
- Purysko, A.S.; Magi-Galluzzi, C.; Mian, O.Y.; Sittenfeld, S.; Davicioni, E.; du Plessis, M.; Buerki, C.; Bullen, J.; Li, L.; Madabhushi, A.; et al. Correlation between MRI Phenotypes and a Genomic Classifier of Prostate Cancer: Preliminary Findings. Eur. Radiol. 2019, 29, 4861–4870. [Google Scholar] [CrossRef] [PubMed]
- Leapman, M.S.; Westphalen, A.C.; Ameli, N.; Lawrence, H.J.; Febbo, P.G.; Cooperberg, M.R.; Carroll, P.R. Association between a 17-Gene Genomic Prostate Score and Multi-Parametric Prostate MRI in Men with Low and Intermediate Risk Prostate Cancer (PCa). PLoS ONE 2017, 12, e0185535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmasi, A.; Said, J.; Shindel, A.W.; Khoshnoodi, P.; Felker, E.R.; Sisk, A.E.; Grogan, T.; McCullough, D.; Bennett, J.; Bailey, H.; et al. A 17-Gene Genomic Prostate Score Assay Provides Independent Information on Adverse Pathology in the Setting of Combined Multiparametric Magnetic Resonance Imaging Fusion Targeted and Systematic Prostate Biopsy. J. Urol. 2018, 200, 564–572. [Google Scholar] [CrossRef]
- Artenstein, D.; Krug, A.; Rhee, E.; Loo, R.; Williams, S.; Reyblat, P.; Parker, R.; Finley, D. Mp24-01 Multiparametric Mri Findings in Patients with Negative Confirm Mdx Tissue Testing. J. Urol. 2019, 201, e334. [Google Scholar] [CrossRef] [Green Version]
- Wibmer, A.G.; Robertson, N.L.; Hricak, H.; Zheng, J.; Capanu, M.; Stone, S.; Ehdaie, B.; Brawer, M.K.; Vargas, H.A. Extracapsular Extension on MRI Indicates a More Aggressive Cell Cycle Progression Genotype of Prostate Cancer. Abdom. Radiol. 2019, 44, 2864–2873. [Google Scholar] [CrossRef] [PubMed]
- Bussemakers, M.J.; van Bokhoven, A.; Verhaegh, G.W.; Smit, F.P.; Karthaus, H.F.; Schalken, J.A.; Debruyne, F.M.; Ru, N.; Isaacs, W.B. DD3: A New Prostate-Specific Gene, Highly Overexpressed in Prostate Cancer. Cancer Res. 1999, 59, 5975–5979. [Google Scholar]
- Knezevic, D.; Goddard, A.D.; Natraj, N.; Cherbavaz, D.B.; Clark-Langone, K.M.; Snable, J.; Watson, D.; Falzarano, S.M.; Magi-Galluzzi, C.; Klein, E.A.; et al. Analytical Validation of the Oncotype DX Prostate Cancer Assay—A Clinical RT-PCR Assay Optimized for Prostate Needle Biopsies. BMC Genom. 2013, 14, 690. [Google Scholar] [CrossRef] [Green Version]
- Saltman, A.; Zegar, J.; Haj-Hamed, M.; Verma, S.; Sidana, A. Prostate Cancer Biomarkers and Multiparametric MRI: Is There a Role for Both in Prostate Cancer Management? Ther. Adv. Urol. 2021, 13, 1756287221997186. [Google Scholar] [CrossRef]
- Ferro, M.; Lucarelli, G.; de Cobelli, O.; Del Giudice, F.; Musi, G.; Mistretta, F.A.; Luzzago, S.; Busetto, G.M.; Buonerba, C.; Sciarra, A.; et al. The Emerging Landscape of Tumor Marker Panels for the Identification of Aggressive Prostate Cancer: The Perspective through Bibliometric Analysis of an Italian Translational Working Group in Uro-Oncology. Minerva Urol. Nephrol. 2021. [Google Scholar] [CrossRef]
- Ebell, M.H. Prolaris Test for Prostate Cancer Risk Assessment. Am. Fam. Physician 2019, 100, 311–312. [Google Scholar]
- Rajwa, P.; Syed, J.; Leapman, M.S. How Should Radiologists Incorporate Non-Imaging Prostate Cancer Biomarkers into Daily Practice? Abdom. Radiol. 2020, 45, 4031–4039. [Google Scholar] [CrossRef]
- de Cobelli, O.; Terracciano, D.; Tagliabue, E.; Raimondi, S.; Bottero, D.; Cioffi, A.; Jereczek-Fossa, B.; Petralia, G.; Cordima, G.; Almeida, G.L.; et al. Predicting Pathological Features at Radical Prostatectomy in Patients with Prostate Cancer Eligible for Active Surveillance by Multiparametric Magnetic Resonance Imaging. PLoS ONE 2015, 10, e0139696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoyanova, R.; Pollack, A.; Takhar, M.; Lynne, C.; Parra, N.; Lam, L.L.C.; Alshalalfa, M.; Buerki, C.; Castillo, R.; Jorda, M.; et al. Association of Multiparametric MRI Quantitative Imaging Features with Prostate Cancer Gene Expression in MRI-Targeted Prostate Biopsies. Oncotarget 2016, 7, 53362–53376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, P.; You, S.; Nguyen, C.; Wang, Y.; Kim, J.; Sirohi, D.; Ziembiec, A.; Luthringer, D.; Lin, S.-C.; Daskivich, T.; et al. Genes Involved in Prostate Cancer Progression Determine MRI Visibility. Theranostics 2018, 8, 1752–1765. [Google Scholar] [CrossRef]
- Eineluoto, J.T.; Sandeman, K.; Pohjonen, J.; Sopyllo, K.; Nordling, S.; Stürenberg, C.; Malén, A.; Kilpeläinen, T.P.; Santti, H.; Petas, A.; et al. Associations of PTEN and ERG with Magnetic Resonance Imaging Visibility and Assessment of Non-Organ-Confined Pathology and Biochemical Recurrence After Radical Prostatectomy. Eur. Urol. Focus 2020. [Google Scholar] [CrossRef] [PubMed]
- Hectors, S.J.; Cherny, M.; Yadav, K.K.; Beksaç, A.T.; Thulasidass, H.; Lewis, S.; Davicioni, E.; Wang, P.; Tewari, A.K.; Taouli, B. Radiomics Features Measured with Multiparametric Magnetic Resonance Imaging Predict Prostate Cancer Aggressiveness. J. Urol. 2019, 202, 498–505. [Google Scholar] [CrossRef]
- Li, L.; Shiradkar, R.; Algohary, A.; Leo, P.; Magi-Galluzzi, C.; Klein, E.; Purysko, A.; Madabhushi, A. Radiomic Features Derived from Pre-Operative Multi-Parametric MRI of Prostate Cancer Are Associated with Decipher Risk Score. In Proceedings of the Medical Imaging 2019: Computer-Aided Diagnosis; SPIE: San Diego, CA, USA, 2019; Volume 10950, pp. 996–1003. [Google Scholar]
- Sun, Y.; Williams, S.; Byrne, D.; Keam, S.; Reynolds, H.M.; Mitchell, C.; Wraith, D.; Murphy, D.; Haworth, A. Association Analysis between Quantitative MRI Features and Hypoxia-Related Genetic Profiles in Prostate Cancer: A Pilot Study. Br. J. Radiol. 2019, 92, 20190373. [Google Scholar] [CrossRef] [PubMed]
- VanderWeele, D.J.; McCann, S.; Fan, X.; Antic, T.; Jiang, Y.; Oto, A. Radiogenomics of Prostate Cancer: Association between Qunatitative Multiparametric MRI Features and PTEN. J. Clin. Oncol. 2015, 33, 126. [Google Scholar] [CrossRef]
- Switlyk, M.D.; Salberg, U.B.; Geier, O.M.; Vlatkovic, L.; Lilleby, W.; Lyng, H.; Seierstad, T. PTEN Expression in Prostate Cancer: Relationship With Clinicopathologic Features and Multiparametric MRI Findings. Am. J. Roentgenol. 2019, 212, 1206–1214. [Google Scholar] [CrossRef]
- Stoyanova, R.; Takhar, M.; Tschudi, Y.; Ford, J.C.; Solórzano, G.; Erho, N.; Balagurunathan, Y.; Punnen, S.; Davicioni, E.; Gillies, R.J.; et al. Prostate Cancer Radiomics and the Promise of Radiogenomics. Transl. Cancer Res. 2016, 5, 432–447. [Google Scholar] [CrossRef] [Green Version]
- Brastianos, H.C.; Murgic, J.; Salcedo, A.; Chua, M.L.K.; Meng, A.; Fraser, M.; Brundage, M.; Fleshner, N.E.; van der Kwast, T.; Bristow, R.G.; et al. Determining the Impact of Spatial Heterogeneity on Genomic Prognostic Biomarkers for Localized Prostate Cancer. Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lucarelli, G.; Ditonno, P.; Bettocchi, C.; Spilotros, M.; Rutigliano, M.; Vavallo, A.; Galleggiante, V.; Fanelli, M.; Larocca, A.M.V.; Germinario, C.A.; et al. Serum Sarcosine Is a Risk Factor for Progression and Survival in Patients with Metastatic Castration-Resistant Prostate Cancer. Future Oncol. 2013, 9, 899–907. [Google Scholar] [CrossRef]
- Gabriele, C.; Cantiello, F.; Nicastri, A.; Crocerossa, F.; Russo, G.I.; Cicione, A.; Vartolomei, M.D.; Ferro, M.; Morgia, G.; Lucarelli, G.; et al. High-Throughput Detection of Low Abundance Sialylated Glycoproteins in Human Serum by TiO2 Enrichment and Targeted LC-MS/MS Analysis: Application to a Prostate Cancer Sample Set. Anal. Bioanal. Chem. 2019, 411, 755–763. [Google Scholar] [CrossRef]
- Lucarelli, G.; Fanelli, M.; Larocca, A.M.V.; Germinario, C.A.; Rutigliano, M.; Vavallo, A.; Selvaggi, F.P.; Bettocchi, C.; Battaglia, M.; Ditonno, P. Serum Sarcosine Increases the Accuracy of Prostate Cancer Detection in Patients with Total Serum PSA Less than 4.0 Ng/Ml. Prostate 2012, 72, 1611–1621. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Buonerba, C.; Terracciano, D.; Lucarelli, G.; Cosimato, V.; Bottero, D.; Deliu, V.M.; Ditonno, P.; Perdonà, S.; Autorino, R.; et al. Biomarkers in Localized Prostate Cancer. Future Oncol. 2016, 12, 399–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, F.A.; Kolowitz, B.J.; Awan, O.; Aerts, H.J.; von Reden, A.; Halabi, S.; Mohiuddin, S.A.; Malik, S.; Shrestha, R.B.; Deible, C. Technical Challenges in the Clinical Application of Radiomics. JCO Clin. Cancer Inform. 2017, 1, 1–8. [Google Scholar] [CrossRef]
- Smith, C.P.; Czarniecki, M.; Mehralivand, S.; Stoyanova, R.; Choyke, P.L.; Harmon, S.; Turkbey, B. Radiomics and Radiogenomics of Prostate Cancer. Abdom. Radiol. 2019, 44, 2021–2029. [Google Scholar] [CrossRef]
- Papadimitroulas, P.; Brocki, L.; Christopher Chung, N.; Marchadour, W.; Vermet, F.; Gaubert, L.; Eleftheriadis, V.; Plachouris, D.; Visvikis, D.; Kagadis, G.C.; et al. Artificial Intelligence: Deep Learning in Oncological Radiomics and Challenges of Interpretability and Data Harmonization. Phys. Med. 2021, 83, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Pooch, E.H.; Ballester, P.L.; Barros, R.C. Can We Trust Deep Learning Models Diagnosis? The Impact of Domain Shift in Chest Radiograph Classification. arXiv 2019, arXiv:190901940. [Google Scholar]
- Yang, J.; Fang, R.; Ni, B.; Li, Y.; Xu, Y.; Li, L. Probabilistic Radiomics: Ambiguous Diagnosis with Controllable Shape Analysis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2019; pp. 658–666. [Google Scholar]
- Ackaouy, A.; Courty, N.; Vallée, E.; Commowick, O.; Barillot, C.; Galassi, F. Unsupervised Domain Adaptation with Optimal Transport in Multi-Site Segmentation of Multiple Sclerosis Lesions from MRI Data. Front. Comput. Neurosci. 2020, 14, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, S.; Takahashi, M.; Kinoshita, M.; Miyake, M.; Kawaguchi, R.; Shinojima, N.; Mukasa, A.; Saito, K.; Nagane, M.; Otani, R.; et al. Fine-Tuning Approach for Segmentation of Gliomas in Brain Magnetic Resonance Images with a Machine Learning Method to Normalize Image Differences among Facilities. Cancers 2021, 13, 1415. [Google Scholar] [CrossRef]
- Lo Gullo, R.; Daimiel, I.; Morris, E.A.; Pinker, K. Combining Molecular and Imaging Metrics in Cancer: Radiogenomics. Insights Imaging 2020, 11, 1. [Google Scholar] [CrossRef]
- Leijenaar, R.T.H.; Carvalho, S.; Velazquez, E.R.; van Elmpt, W.J.C.; Parmar, C.; Hoekstra, O.S.; Hoekstra, C.J.; Boellaard, R.; Dekker, A.L.A.J.; Gillies, R.J.; et al. Stability of FDG-PET Radiomics Features: An Integrated Analysis of Test-Retest and Inter-Observer Variability. Acta Oncol. 2013, 52, 1391–1397. [Google Scholar] [CrossRef] [Green Version]
- Ferro, M.; Terracciano, D.; Buonerba, C.; Lucarelli, G.; Bottero, D.; Perdonà, S.; Autorino, R.; Serino, A.; Cantiello, F.; Damiano, R.; et al. The Emerging Role of Obesity, Diet and Lipid Metabolism in Prostate Cancer. Future Oncol. 2017, 13, 285–293. [Google Scholar] [CrossRef] [Green Version]
- The Cancer Genome Atlas (TCGA). Available online: https://www.genome.gov/Funded-Programs-Projects/Cancer-Genome-Atlas (accessed on 4 April 2021).
- Welcome to the Cancer Imaging Archive. Available online: https://www.cancerimagingarchive.net/ (accessed on 4 April 2021).
- Angeles, A.K.; Heckmann, D.; Flosdorf, N.; Duensing, S.; Sültmann, H. The ERG-Regulated LINC00920 Promotes Prostate Cancer Cell Survival via the 14-3-3ε-FOXO Pathway. Mol. Cancer Res. 2020, 18, 1545–1559. [Google Scholar] [CrossRef]
- Christensen, G.B.; Baffoe-Bonnie, A.B.; George, A.; Powell, I.; Bailey-Wilson, J.E.; Carpten, J.D.; Giles, G.G.; Hopper, J.L.; Severi, G.; English, D.R.; et al. Genome-Wide Linkage Analysis of 1,233 Prostate Cancer Pedigrees from the International Consortium for Prostate Cancer Genetics Using Novel SumLINK and SumLOD Analyses. Prostate 2010, 70, 735–744. [Google Scholar] [CrossRef] [Green Version]
- International Cancer Genome Consortium; Hudson, T.J.; Anderson, W.; Artez, A.; Barker, A.D.; Bell, C.; Bernabé, R.R.; Bhan, M.K.; Calvo, F.; Eerola, I.; et al. International Network of Cancer Genome Projects. Nature 2010, 464, 993–998. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Wang, W.; Zhao, Y.; Liang, K.; Huang, Y. Identification of Potential Key Genes for Pathogenesis and Prognosis in Prostate Cancer by Integrated Analysis of Gene Expression Profiles and the Cancer Genome Atlas. Front. Oncol. 2020, 10, 809. [Google Scholar] [CrossRef]
- Stanzione, A.; Gambardella, M.; Cuocolo, R.; Ponsiglione, A.; Romeo, V.; Imbriaco, M. Prostate MRI Radiomics: A Systematic Review and Radiomic Quality Score Assessment. Eur. J. Radiol. 2020, 129, 109095. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.W.L. The Potential of Radiomic-Based Phenotyping in Precision Medicine: A Review. JAMA Oncol. 2016, 2, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Rundo, L.; Han, C.; Zhang, J.; Hataya, R.; Nagano, Y.; Militello, C.; Ferretti, C.; Nobile, M.S.; Tangherloni, A.; Gilardi, M.C. CNN-based prostate zonal segmentation on T2-weighted MR images: A cross-dataset study. In Neural Approaches to Dynamics of Signal Exchanges; Springer: Berlin/Heidelberg, Germany, 2020; pp. 269–280. [Google Scholar]
- Ushinsky, A.; Bardis, M.; Glavis-Bloom, J.; Uchio, E.; Chantaduly, C.; Nguyentat, M.; Chow, D.; Chang, P.D.; Houshyar, R. A 3D-2D Hybrid U-Net Convolutional Neural Network Approach to Prostate Organ Segmentation of Multiparametric MRI. Am. J. Roentgenol. 2021, 216, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Yaniv, O.; Portnoy, O.; Talmon, A.; Kiryati, N.; Konen, E.; Mayer, A. V-Net Light-Parameter-Efficient 3-D Convolutional Neural Network for Prostate MRI Segmentation. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; pp. 442–445. [Google Scholar]
- Chaddad, A.; Kucharczyk, M.J.; Cheddad, A.; Clarke, S.E.; Hassan, L.; Ding, S.; Rathore, S.; Zhang, M.; Katib, Y.; Bahoric, B.; et al. Magnetic Resonance Imaging Based Radiomic Models of Prostate Cancer: A Narrative Review. Cancers 2021, 13, 552. [Google Scholar] [CrossRef]
- Kang, J.; Rancati, T.; Lee, S.; Oh, J.H.; Kerns, S.L.; Scott, J.G.; Schwartz, R.; Kim, S.; Rosenstein, B.S. Machine Learning and Radiogenomics: Lessons Learned and Future Directions. Front. Oncol. 2018, 8, 228. [Google Scholar] [CrossRef]
- Andreassen, C.N.; Schack, L.M.H.; Laursen, L.V.; Alsner, J. Radiogenomics-Current Status, Challenges and Future Directions. Cancer Lett. 2016, 382, 127–136. [Google Scholar] [CrossRef]
- Chen, S.; Ning, Z.; He, X.; Qi, X. Radiogenomics Map: A Novel Approach for Noninvasive Identification of Molecular Properties? Radiology 2017, 285, 1060–1061. [Google Scholar] [CrossRef] [Green Version]
- Lucarelli, G.; Ferro, M.; Loizzo, D.; Bianchi, C.; Terracciano, D.; Cantiello, F.; Bell, L.N.; Battaglia, S.; Porta, C.; Gernone, A.; et al. Integration of Lipidomics and Transcriptomics Reveals Reprogramming of the Lipid Metabolism and Composition in Clear Cell Renal Cell Carcinoma. Metabolites 2020, 10, 509. [Google Scholar] [CrossRef] [PubMed]
- Lucarelli, G.; Loizzo, D.; Ferro, M.; Rutigliano, M.; Vartolomei, M.D.; Cantiello, F.; Buonerba, C.; Di Lorenzo, G.; Terracciano, D.; De Cobelli, O.; et al. Metabolomic Profiling for the Identification of Novel Diagnostic Markers and Therapeutic Targets in Prostate Cancer: An Update. Expert Rev. Mol. Diagn. 2019, 19, 377–387. [Google Scholar] [CrossRef]


{kind=link}
| Terminology | Short Definition |
|---|---|
| Radiomics | Quantitative approach to medical imaging, enhancing existing data through mathematical analysis [68]. |
| Genomics | Study of whole genomes, including elements from genetics. Genomics uses a combination of recombinant DNA, DNA sequencing methods, and bioinformatics to sequence, assemble, and analyze the structure and function of genomes [69,70,71]. |
| Radiogenomics | Genomics information that can be explained or decoded by radiomics and to develop methodology to create more-efficient predictive models [72]. |
| Author | Clinical Outcomes | Type of Image Acquisition | Results |
|---|---|---|---|
| Radiomics in diagnosis and detection of prostate cancer | |||
| Zhang et al. [29] | Upgrading Gleason score from biopsy to RP | MRI | AUC: combined clinical and radiomics model 0.910, clinical model 0.646, radiomics model 0.868 |
| Dulhanty et al. [80] | Detection of PCa | MRI | Zone-discovery radiomics model (AUC 0.86) > clinical heuristics model (AUC 0.79) |
| Bagher- Ebadian et al. [79] | Detection of dominant intraprostatic lesions and normal tissue | MRI | Comparison between conventional model and artificial neural network model, AUC model (0.94 and 0.95, respectively) |
| Qi et al. [77] | Detection of PCa through radiomics in prostate cancer patients with PSA range 4–10 ng/mL | MRI | Combined model (radiomics signature and clinical radiological risk factors) AUC 0.933, p < 0.05 |
| Chen et al. [81] | Diagnosis of intermediate-/high-grade (GS ≥ 7) tumors | MRI | Radiomics-based model > PIRADS v2 model in PCa detection vs. no PCa (AUC 0.999). Validation in differentiating high-grade from low-grade PCa (AUC 0.777) |
| Khalvati et al. [87] | Detection of PCa | MRI | Specificity used as performance evaluation criteria can maximize the results for AUC (0.90), which leads to balanced results for sensitivity and specificity; 0.84 and 0.86, respectively |
| Hu et al. [47] | Detection of PCa | MRI | Mixed model better compared with mp-MRI signatures and clinically independent risk factors alone (AUC 0.81, 0.93, and 0.94 in training sets, and 0.74, 0.92, and 0.93 in validation sets, respectively) |
| Brunese et al. [96] | Gleason score prediction | MRI | Gleason score prediction equal to 0.98473, 0.96667, 0.98780 and 0.97561 for, respectively, Gleason score 3 + 3, Gleason score 3 + 4, Gleason score 4 + 3 and Gleason score 4 + 4 prediction |
| Radiomics and detection of clinically significant prostate cancer | |||
| Wang et al. [97] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4). Lesions defined as volume > 0.5 cm3 on histopathology. | mp-MRI | PCa vs. normal PZ + TZ Combined: 0.978 (0.947–0.993) PCa vs. normal PZ Combined: 0.983 (0.960–0.995) PCa vs. normal TZ Combined: 0.968 (0.940–0.985) |
| Kwon et al. [98] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | MRI | AUC 0.82 (random forests), 0.76 (CART), and 0.76 (adaptive LASSO) |
| Parra et al. [99] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | mpMRI | The trained models had an AUC of 0.82 and an AUC of 0.82 on validation cohort |
| Penzias et al. [100] | Detection of high-grade PCa | MRI | Gabor texture features identified as most predictive of Gleason grade on MRI (AUC of 0.69) |
| Cuocolo et al. [40] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | MRI | Multivariable analysis of T2W and ADC-derived SAVR: AUC 0.78 |
| Giambelluca et al. [48] | Presence of clinically significant PCa Gleason score ≥ 7 (3 + 4) in PIRADS 3 images | MRI | AUC of 0.769 and 0.817 on T2w or 0.749 and 0.744 on ADC maps images Analysis was performed using the GLM regression. To strengthen the reliability of the results and avoid over-fitting, 10-fold cross-validation was performed |
| Min X et al. [101] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | mpMRI | Logistic regression modeling yielded AUC 0.872 in the training cohort and 0.823 in the test cohort |
| Brancato et al. [102] | Gleason Score ≥ 6 in PIRADS 3 images and in peripheral PIRADS 3 upgraded to PIRADS 4 images | MRI | PIRADS 3 images: sensitivity, specificity and accuracy (0.8, 0.51, 0.71, respectively) with AUC = 0.76. For upgraded PIRADS 4: AUC—0.89, sensitivity—0.87, specificity—0.62 and accuracy—0.82 |
| Hou et al. [103] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4)in PIRADS 3 lesions | mpMRI | AUC model one is 0.89 and higher than that of model two with AUC of 0.87 (p = 0.003) |
| Zhang et al. [104] | Differentiation between clinically significant PCa Gleason score ≥ 7 (3 + 4) from insignificant prostate cancer | MRI | Combination AUC of 0.95 (training group), 0.93 (internal validation group), and 0.84 (external validation group). p < 0.001 |
| Gong et al. [105] | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | MRI | Combined clinical and radiomics model (T2w/DWI) yielded an AUC of 0.788 |
| Woźnicki et al. [76] | Prediction of clinically significant PCa Gleason score ≥ 7 (3 + 4) | mpMRI | The model combining radiomics, PIRADS, PSA density and DRE showed a significantly better performance compared to ADC for clinically significant prostate cancer prediction (AUC = 0.571, p = 0.022) |
| Bernatz et al. [106] | Discriminating clinically significant PCa Gleason score ≥ 7 (3 + 4) versus indolent disease | mpMRI | Three classification models were trained and a subset of shape features improved the diagnostic accuracy of the clinical assessment categories (maximum increase in diagnostic accuracy ΔAUC = +0.05, p < 0.001) |
| Gugliandolo et al. [43] | Predictive of Gleason score, PIRADS v2 score, and risk class | mpMRi | Gleason score, PIRADS v2 score, and risk class; AUC 0.74 to 0.94 |
| Krauss et al. [73] | PSA level in patients with low suspicion for clinically significant PCa Gleason score ≥ 7 (3 + 4). | MRI | Five radiomic features were significantly correlated with PSA level (r: 0.53–0.69, p < 0.05). The regression model significantly improves the explanatory value for PSA level (p < 0.05) |
| Song et al. [91] | Differentiate clinical significant PCa Gleason score ≥ 7 (3 + 4) from indolent disease | mpMRI | AUC on training, validation, and test dataset achieved results of 0.838, 0.814, and 0.824, respectively |
| Castillo et al. [92] | Differentiate high-grade versus low-grade lesions | mpMRI | The three single-center models obtained a mean AUC of 0.75, outperforming expert radiologist |
| Li et al. [107] | Prediction of clinically PCa Gleason score ≥ 7 (3 + 4) | Biparametric mpMRI | Both the radiomics model (AUC: 0.98) and the clinical–radiomics combined model (AUC: 0.98) achieved greater predictive efficacy than the clinical model (AUC: 0.79) |
| Li, Q et al. | Detection of clinically significant PCa Gleason score ≥ 7 (3 + 4) | MRI | Built a linear classifier model on these semantic traits and related to pathological outcome to identify clinically significant tumors. The discriminatory ability of the predictors was tested using cross-validation method randomly repeated and ensemble values were reported |
| Bonekamp et al. [108] | Compare radiomics and mean ADC for characterization of prostate lesions (Gleason grade group ≥ 2) | MRI | Comparison of the area under the AUC for the mean ADC (AUCglobal = 0.84; AUCzone-specific ≤ 0.87) vs. the RML (AUCglobal = 0.88, p = 0.176; AUCzone-specific ≤ 0.89, p ≥ 0.493) |
| Bleker et al. [109] | Identification of clinically significant peripheral zone PCa Gleason score ≥ 7 (3 + 4) | mpMRI | Combined model T2w and DWI images through an auto fixed VOI with AUC 0.870 (95% CI 0.980–0.754) |
| Radiomics and detection of ECE | |||
| Losnegård et al. [110] | Prediction of extraprostatic extension in non-favorable intermediate- and high-risk prostate cancer patients | mpMRI | Best AUC for extraprostatic extension prediction models used in combination (MSKCC + radiology + radiomics) 0.80 |
| Ma et al. [94] | Identification of PCa ECE | mpMRI | AUC of 0.902 and 0.883 in the training and validation cohort, respectively. Outperforming the radiologists results (AUC range 0.600–0.697), (75.00% vs. 46.88–50.00%, all p < 0.05), respectively |
| Ma et al. [93] | Identification of PCa ECE | mpMRI | AUC of 0.906 and 0.821 for the training and validation datasets, respectively |
| Cysouw et al. [111] | Prediction of lymphovascular invasion nodal or distant metastasis and Gleason score | (18F)DCFPyL PET | Lymphovascular invasion (AUC 0.86 ± 0.15, p < 0.01), nodal or distant metastasis (AUC 0.86 ± 0.14, p < 0.01), Gleason score (0.81 ± 0.16, p < 0.01), and ECE (0.76 ± 0.12, p < 0.01) |
| Biomarker | Description | Test Source | Analysis | Study | Results |
|---|---|---|---|---|---|
| Prostate cancer antigen 3 | Prostate-specific mRNA quantification | Prostate biopsy | Negative prior biopsy | De Luca et al. [138] | Significant association between PCA3 score and PI-RADS grade groups 3, 4, and 5 (p = 0.006) |
| Two negative prostate biopsies | Alkasab et al. [139] | PCA3 not statistically correlated with PCa diagnosis (p = 0.128) and PCA3 associated with high-grade PCa at final pathology (p = 0.0435) | |||
| No prior biopsy | Fernstermaker et al. [140] | PCA3 associated with MRI suspicion score of 2 and 3 (p = 0.004), not 4 and 5 (p = 0.340) | |||
| Negative prior biopsy | Perlis et al. [141] | Normal PCA3 score gave a negative predictive value of 100% (p < 0.0001) | |||
| Decipher test® | 22 RNA markers for prognosis and prediction of metastasis | RP or prostate biopsy | Low and intermediate PCa | Martin et al. [142] | Decipher® biopsy genomic test was associated with Gleason grade group and it was independent of PIRADSv2 score |
| Defining the favorable intermediate-risk prostate cancer | Falagario et al. [143] | Unfavorable intermediate-risk category (p < 0.001) and Decipher® test (p = 0.012) were statistically significant predictors of adverse pathology; mpMRI did not maintain statistical significance (p = 0.059) | |||
| Prediction of BCR | Jambor et al. [144] | Decipher® genomic score and mpMRI could not improve predictive performance of biochemical recurrence compared with the individual use of these features | |||
| mpMRI could predict aggressive prostate cancer features | Beksac et al. [145] | Association of Decipher® score was significantly with lesion size (p = 0.03), PIRADS score (p = 0.02) and extraprostatic extension (p = 0.01) | |||
| Correlation between MRI phenotypes of PCa as defined by PI-RADS v2 and Decipher | Purysko et al. [146] | MRI-visible lesions had higher Decipher® scores than MRI-invisible lesions (p < 0.0001); some lesions classified as intermediate/high risk by Decipher® are invisible on MRI | |||
| BCR and adverse pathology prediction | Li et al. [45] | New imaging-based nomogram; AUC (0.71, 95% CI 0.62–0.81) better than Decipher® AUC (0.66, 95% CI 0.56–0.77) and prostate cancer risk assessment (CAPRA) score AUC (0.69, 95% CI 0.59–0.79) | |||
| Oncotype Dx test® | 5 reference genes and 12 cancer genes generating a genomic prostate score (GPS) | Prostate biopsy | Association between mpMRI and Oncotype Dx test®GPS | Leapman et al. [147] | GPS differences among MRI categories for patients with Gleason pattern 3 + 4 (p = 0.010), not in Gleason pattern 3 + 3 |
| GPS to predict adverse pathology | Salmasi et al. [148] | GPS is a significant predictor for adverse pathology (p < 0.001) | |||
| ConfirmMDx® | Alterations in DNA methylation | Prior negative biopsies | mpMRI PIRADS score lesions after ConfirmMDx® sampling | Artenstein et al. [149] | Negative ConfirmMDx® test is in accordance with negative MRI results (71.4%). ConfirmMDx® sampling may be useful as a fusion-targeted biopsy rather than systematic biopsy |
| Prolaris test® | 46-mRNA genomic test | Prostate biopsy | Associations between MRI and the expression levels of cell cycle genes | Wibmer et al. [150] | In the RP subgroup, ECE on MRI (p ≤ 0.001–0.001) and cycle genes risk scores (p = 0.049) were significantly associated with Gleason score 4 + 3 or higher, ECE and lymph node metastases |
| Reference | Molecule Studied | Imaging Performed | Results | Approach | Method |
|---|---|---|---|---|---|
| McCann et al. [124] | PTEN | MRI | Perfusion imaging contrast uptake, T2-weighted signal-intensity skewness | Classical | Radiomic |
| Stoyanova et al. [158] | General gene expression | MRI | Radiomic signatures | Classical | Radiomic |
| Renard-Penna et al. [119] | RNA expression signature derived from cell cycle proliferation genes (Prolaris®) | mpMRI | Correlation with Gleason score (r = 0.199, p = 0.04) and PIRADS sum score (r = 0.26, p = 0.007) | Classical | Radiomic |
| Jamshidi et al. [125] | Whole-exosome DNA sequencing | mpMRI | No statistically significant linear correlation between individual mutations and mpMRI imaging parameters or PIRADS scores (p = 0.3) | Classical | Radiomic |
| Houlahan et al. [130] | Small nucleolar RNAs | mpMRI | Elevated snoRNA abundance may be a novel hallmark of nimbotic tumors (AUC: 0.87; 95%CI: 0.75–0.99) | Classical | Radiomic |
| Li P et al. [159] | Differentially expressed genes | MRI | MRI visibility (AUC: 0.86), progression-free survival HR = 2.53 (1.55–4.11), p < 0.001 BCR-free survival HR = 1.3 (1.04–1.63), p = 0.021 | Classical | Radiomic |
| Eineluoto et al. [160] | PTEN and ERG | MRI | MRI-invisible lesions had less PTEN loss and ERG-positive expression compared with patients with MRI-visible lesions (17.2% vs. 43.3%, p = 0.006; 8.6% vs. 20.0%, p = 0.125) | Classical | Radiomic |
| Hectors et al. [161] | 40 gene expression signatures plus Decipher® | MRI | Prediction of Gleason score of 8 or greater (AUC 0.72) and prediction of a Decipher® score of 0.6 or greater (AUC 0.84). | Classical | Radiomic |
| Li L et al. [162] | Decipher® | MRI | Model outperformed the prediction using PIRADS v2 (AUC = 0.67), and comparable performance with Gleason grade group (AUC = 0.80) | Classical | Radiomic |
| Sun et al. [163] | Full transcriptome genetic profiles | mpMRI | Weak association of mpMRI features and hypoxia gene expression (p < 0.05). | Classical | Radiomic |
| Fischer et al. [27] | Gene and miRNA expression (Alanyl membrane aminopeptidase, microRNA-mir-217, mir-592, mir-6715b) | mpMRI | T2c and T3b prostate cancer stages being highly correlated with aggressiveness on related imaging features (average r = ± 0.75) | Classical | Radiomic |
| Wibmer et al. [150] | Prolaris® test | MRI | ECE on MRI had significantly higher mean cell cycle risk score (reader 1: 3.9 vs. 3.2, p = 0.015; reader 2: 3.6 vs. 3.2, p = 0.045) | Classical | Radiomic |
| Vander-Weele et al. [164] | PTEN | mpMRI | Imaging uptake parameters showing mathematical correlation with PTEN expression (r = 0.25, p < 0.1 and r = 0.43, p < 0.01), and T2w unevenness also showed some correlation tendency (r = −0.25, p < 0.1) | Classical | Radiomic |
| Switlyk et al. [165] | PTEN | MRI | ADC was negatively correlated with Gleason score (p = 0.001) and tumor size (p = 0.023) | Classical | Radiomic |
| Radiogenomics | Advantages | Limitations |
|---|---|---|
| Could provide accurate imaging biomarkers, substituting for genetic testing with lower cost [179] | Lack of prospective studies [6] | |
| AI and deep learning using big public databases with genomics and imaging features will be used to develop computer-aided tools for clinical practice translation [27] | Image acquisition for defining and contouring the regions of interests need expert radiologists [26] | |
| Automatic and semi-automatic computer designed software used to reduce drawbacks (lack of standardization, imaging and reporting protocols which differ significantly among institutions) [189] | Significant time used for proper manual delineation [179] | |
| Radiomics/radiogenomics biomarkers may predictrisk and outcomes and may be used to personalize treatment options [179] | High inter-observer variability in reading and segmenting regions of interest [180] | |
| Insights into the tumor genome requires biopsies, an invasive procedure that may increase patient morbidity. Radiogenomics can predict tumor genomic alterations [26] | Lack of repeatability and reproducibility—no standardization—different acquisition protocols, scanners and radiomic studies [194,195] | |
| Availability of whole-tumor information with aradiomics-based approach that can providepredictive and prognostic data [196] | Matching the data from whole-genome sequencing with imaging data is difficult due to different patient characteristics and imaging protocols [179] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. https://doi.org/10.3390/ijms22189971
Ferro M, de Cobelli O, Vartolomei MD, Lucarelli G, Crocetto F, Barone B, Sciarra A, Del Giudice F, Muto M, Maggi M, et al. Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization. International Journal of Molecular Sciences. 2021; 22(18):9971. https://doi.org/10.3390/ijms22189971
Chicago/Turabian StyleFerro, Matteo, Ottavio de Cobelli, Mihai Dorin Vartolomei, Giuseppe Lucarelli, Felice Crocetto, Biagio Barone, Alessandro Sciarra, Francesco Del Giudice, Matteo Muto, Martina Maggi, and et al. 2021. "Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization" International Journal of Molecular Sciences 22, no. 18: 9971. https://doi.org/10.3390/ijms22189971
APA StyleFerro, M., de Cobelli, O., Vartolomei, M. D., Lucarelli, G., Crocetto, F., Barone, B., Sciarra, A., Del Giudice, F., Muto, M., Maggi, M., Carrieri, G., Busetto, G. M., Falagario, U., Terracciano, D., Cormio, L., Musi, G., & Tataru, O. S. (2021). Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization. International Journal of Molecular Sciences, 22(18), 9971. https://doi.org/10.3390/ijms22189971