
Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Gestational Diabetes Mellitus
3. Periodontitis and Gestational Diabetes Mellitus: Epidemiological Studies
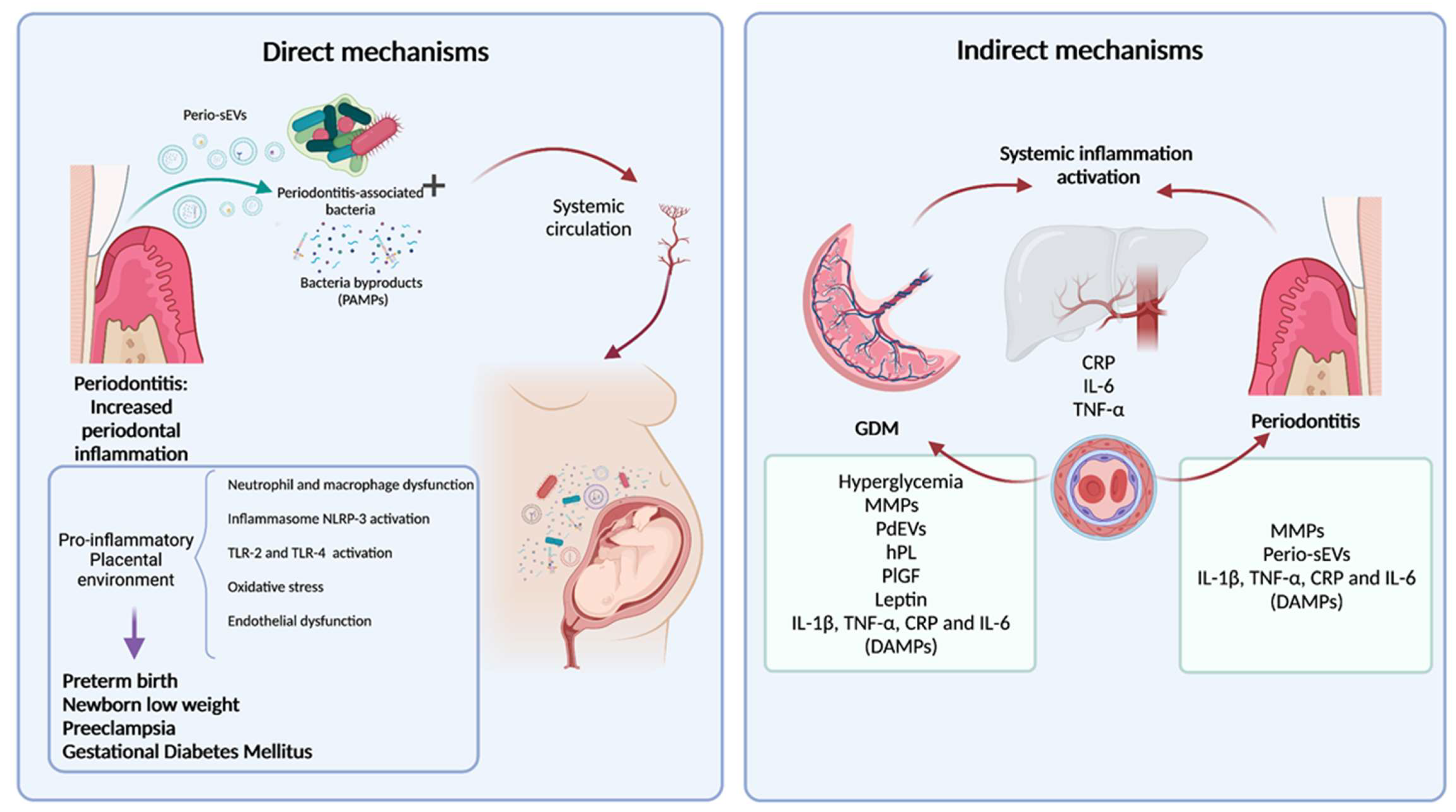
4. Periodontal Bacteria Translocation into the Maternal Fetal Unit as a Direct Mechanism of Association
5. Release of Pro-Inflammatory Molecules from Periodontal Inflamed Tissues and Systemic Inflammation as an Indirect Mechanism of Association
6. Extracellular Vesicles in the Cross-Talk between Periodontal Tissues and the Placenta
EV Release and Bioactivity in GDM
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slots, J. Periodontitis: Facts, Fallacies and the Future. Periodontol. 2000 2017, 75, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Severe Periodontitis in 1990–2010: A Systematic Review and Meta-Regression. J. Dent. Res. 2014, 93, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute and Chronic Diseases and Injuries in 188 Countries, 1990–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Eke, P.I.; Wei, L.; Borgnakke, W.S.; Thornton-Evans, G.; Zhang, X.; Lu, H.; McGuire, L.C.; Genco, R.J. Periodontitis Prevalence in Adults ≥ 65 Years of Age, in the USA. Periodontol. 2000 2016, 72, 76–95. [Google Scholar] [CrossRef]
- Graziani, F.; Tsakos, G. Patient-based Outcomes and Quality of Life. Periodontol. 2000 2020, 83, 277–294. [Google Scholar] [CrossRef]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are Periodontal Diseases Really Silent? A Systematic Review of Their Effect on Quality of Life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef]
- Suárez, L.J.; Garzón, H.; Arboleda, S.; Rodríguez, A. Oral Dysbiosis and Autoimmunity: From Local Periodontal Responses to an Imbalanced Systemic Immunity. A Review. Front. Immunol. 2020, 11, 591255. [Google Scholar] [CrossRef]
- Meyle, J.; Chapple, I. Molecular Aspects of the Pathogenesis of Periodontitis. Periodontol. 2000 2015, 69, 7–17. [Google Scholar] [CrossRef]
- Kurgan, S.; Kantarci, A. Molecular Basis for Immunohistochemical and Inflammatory Changes during Progression of Gingivitis to Periodontitis. Periodontol. 2000 2018, 76, 51–67. [Google Scholar] [CrossRef]
- Bosshardt, D.D. The Periodontal Pocket: Pathogenesis, Histopathology and Consequences. Periodontol. 2000 2018, 76, 43–50. [Google Scholar] [CrossRef]
- Sanz, M.; Kornman, K.; on behalf of working group 3 of the joint EFP/AAP workshop. Periodontitis and Adverse Pregnancy Outcomes: Consensus Report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S164–S169. [Google Scholar] [CrossRef]
- Armitage, G.C. Bi-Directional Relationship between Pregnancy and Periodontal Disease: Relationship between Pregnancy and Periodontal Disease. Periodontol. 2000 2013, 61, 160–176. [Google Scholar] [CrossRef]
- Forner, L.; Larsen, T.; Kilian, M.; Holmstrup, P. Incidence of Bacteremia after Chewing, Tooth Brushing and Scaling in Individuals with Periodontal Inflammation. J. Clin. Periodontol. 2006, 33, 401–407. [Google Scholar] [CrossRef]
- Schenkein, H.A.; Papapanou, P.N.; Genco, R.; Sanz, M. Mechanisms Underlying the Association between Periodontitis and Atherosclerotic Disease. Periodontol. 2000 2020, 83, 90–106. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Van Dyke, T.E.; on behalf of working group 1 of the joint EFP/AAP workshop. Periodontitis and Atherosclerotic Cardiovascular Disease: Consensus Report of the Joint EFP/AAPWorkshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S24–S29. [Google Scholar] [CrossRef]
- Kamer, A.R.; Craig, R.G.; Niederman, R.; Fortea, J.; de Leon, M.J. Periodontal Disease as a Possible Cause for Alzheimer’s Disease. Periodontol. 2000 2020, 83, 242–271. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Suvan, J.; Deschner, J. The Association of Periodontal Diseases with Metabolic Syndrome and Obesity. Periodontol. 2000 2020, 83, 125–153. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, M.; Graziani, F.; D’Aiuto, F. Periodontal Therapy and Cardiovascular Risk. Periodontol. 2000 2020, 83, 107–124. [Google Scholar] [CrossRef]
- Bartold, P.M.; Lopez-Oliva, I. Periodontitis and Rheumatoid Arthritis: An Update 2012–2017. Periodontol. 2000 2020, 83, 189–212. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Diabetes as a Potential Risk for Periodontitis: Association Studies. Periodontol. 2000 2020, 83, 40–45. [Google Scholar] [CrossRef]
- Bobetsis, Y.A.; Graziani, F.; Gürsoy, M.; Madianos, P.N. Periodontal Disease and Adverse Pregnancy Outcomes. Periodontol. 2000 2020, 83, 154–174. [Google Scholar] [CrossRef]
- Figuero, E.; Han, Y.W.; Furuichi, Y. Periodontal Diseases and Adverse Pregnancy Outcomes: Mechanisms. Periodontol. 2000 2020, 83, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Salomon, C.; Scholz-Romero, K.; Sarker, S.; Sweeney, E.; Kobayashi, M.; Correa, P.; Longo, S.; Duncombe, G.; Mitchell, M.D.; Rice, G.E.; et al. Gestational Diabetes Mellitus Is Associated With Changes in the Concentration and Bioactivity of Placenta-Derived Exosomes in Maternal Circulation Across Gestation. Diabetes 2016, 65, 598–609. [Google Scholar] [CrossRef] [Green Version]
- Koning, S.H.; van Zanden, J.J.; Hoogenberg, K.; Lutgers, H.L.; Klomp, A.W.; Korteweg, F.J.; van Loon, A.J.; Wolffenbuttel, B.H.R.; van den Berg, P.P. New Diagnostic Criteria for Gestational Diabetes Mellitus and Their Impact on the Number of Diagnoses and Pregnancy Outcomes. Diabetologia 2018, 61, 800–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global Estimates of Diabetes Prevalence for 2017 and Projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Lekva, T.; Norwitz, E.R.; Aukrust, P.; Ueland, T. Impact of Systemic Inflammation on the Progression of Gestational Diabetes Mellitus. Curr. Diabetes Rep. 2016, 16, 26. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41 (Suppl. S1), S13–S27. [Google Scholar] [CrossRef] [Green Version]
- Catalano, P.M.; Shankar, K. Obesity and Pregnancy: Mechanisms of Short Term and Long Term Adverse Consequences for Mother and Child. BMJ 2017, 356, j1. [Google Scholar] [CrossRef]
- Jovanovic, L.; Pettitt, D.J. Gestational Diabetes Mellitus. J. Am. Med Assoc. 2001, 286, 2516–2518. [Google Scholar] [CrossRef]
- Monteiro, L.J.; Norman, J.E.; Rice, G.E.; Illanes, S.E. Fetal Programming and Gestational Diabetes Mellitus. Placenta 2016, 48, S54–S60. [Google Scholar] [CrossRef] [Green Version]
- Escudero, C.; Gonzlez, M.; Acurio, J.; Valenzuela, F.; Sobrevi, L. The Role of Placenta in the Fetal Programming Associated to Gestational Diabetes. In Gestational Diabetes—Causes, Diagnosis and Treatment; Sobrevia, L., Ed.; InTechOpen ltd.: London, UK, 2013. [Google Scholar] [CrossRef] [Green Version]
- Glastras, S.J.; Chen, H.; Pollock, C.A.; Saad, S. Maternal Obesity Increases the Risk of Metabolic Disease and Impacts Renal Health in Offspring. Biosci. Rep. 2018, 38, BSR20180050. [Google Scholar] [CrossRef]
- Baptiste-Roberts, K.; Bronner, Y.; Nicholson, W.K. Adoption of a Healthy Lifestyle Following Gestational Diabetes Mellitus. Curr. Nutr. Rep. 2015, 4, 259–264. [Google Scholar] [CrossRef]
- Vickers, M.H. Developmental Programming and Adult Obesity: The Role of Leptin: Current Opinion in Endocrinology. Diabetes Obes. 2007, 14, 17–22. [Google Scholar] [CrossRef]
- Zhang, J.; Chi, H.; Xiao, H.; Tian, X.; Wang, Y.; Yun, X.; Xu, Y. Interleukin 6 (IL-6) and Tumor Necrosis Factor α (TNF-α) Single Nucleotide Polymorphisms (SNPs), Inflammation and Metabolism in Gestational Diabetes Mellitus in Inner Mongolia. Med. Sci. Monit. 2017, 23, 4149–4157. [Google Scholar] [CrossRef] [Green Version]
- Pantham, P.; Aye, I.L.M.H.; Powell, T.L. Inflammation in Maternal Obesity and Gestational Diabetes Mellitus. Placenta 2015, 36, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sifnaios, E.; Mastorakos, G.; Psarra, K.; Panagopoulos, N.-D.; Panoulis, K.; Vitoratos, N.; Rizos, D.; Creatsas, G. Gestational Diabetes and T-Cell (Th1/Th2/Th17/Treg) Immune Profile. In Vivo 2019, 33, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Kirbas, A. Evaluation of Inflammatory Related Markers in Gestational Diabetes Mellitus. J. Clin. Anal. Med. 2016, 7. [Google Scholar] [CrossRef]
- Wolf, M.; Sandler, L.; Hsu, K.; Vossen-Smirnakis, K.; Ecker, J.L.; Thadhani, R. First-Trimester C-Reactive Protein and Subsequent Gestational Diabetes. Diabetes Care 2003, 26, 819–824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omu, A.E. Pro-Inflammatory Cytokines, Lipid Metabolism and Inflammation in Gestational Diabetes Mellitus as Cause of Insulin Resistance. In Gestational Diabetes—Causes, Diagnosis and Treatment; Sobrevia, L., Ed.; InTechOpen ltd.: London, UK, 2013. [Google Scholar] [CrossRef] [Green Version]
- da Silva, H.E.C.; Stefani, C.M.; de Santos Melo, N.; de Almeida de Lima, A.; Rösing, C.K.; Porporatti, A.L.; Canto, G.D.L. Effect of Intra-Pregnancy Nonsurgical Periodontal Therapy on Inflammatory Biomarkers and Adverse Pregnancy Outcomes: A Systematic Review with Meta-Analysis. Syst. Rev. 2017, 6, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Chen, J.; Hu, J.; Yang, Z.; Shen, Y. Enhancement of Lipopolysaccharide-Induced Toll-like Receptor 2 Expression and Inflammatory Cytokine Secretion in HUVECs under High Glucose Conditions. Life Sci. 2013, 92, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Corrêa-Silva, S.; Alencar, A.P.; Moreli, J.B.; Borbely, A.U.; de S. Lima, L.; Scavone, C.; Damasceno, D.C.; Rudge, M.V.C.; Bevilacqua, E.; Calderon, I.M.P. Hyperglycemia Induces Inflammatory Mediators in the Human Chorionic Villous. Cytokine 2018, 111, 41–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahingur, S.E.; Xia, X.-J.; Alamgir, S.; Honma, K.; Sharma, A.; Schenkein, H.A. DNA from Porphyromonas Gingivalis and Tannerella Forsythia Induce Cytokine Production in Human Monocytic Cell Lines. Mol. Oral Microbiol. 2010, 25, 123–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahingur, S.E.; Xia, X.-J.; Schifferle, R.E. Oral Bacterial DNA Differ in Their Ability to Induce Inflammatory Responses in Human Monocytic Cell Lines. J. Periodontol. 2012, 83, 1069–1077. [Google Scholar] [CrossRef]
- Graves, D.T.; Naguib, G.; Lu, H.; Desta, T.; Amar, S. Porphyromonas Gingivalis Fimbriae Are pro-Inflammatory but Do Not Play a Prominent Role in the Innate Immune Response to P. Gingivalis. J. Endotoxin Res. 2005, 11, 13–18. [Google Scholar] [CrossRef]
- Andriankaja, O.M.; Galicia, J.; Dong, G.; Xiao, W.; Alawi, F.; Graves, D.T. Gene Expression Dynamics during Diabetic Periodontitis. J. Dent. Res. 2012, 91, 1160–1165. [Google Scholar] [CrossRef] [Green Version]
- Arimatsu, K.; Yamada, H.; Miyazawa, H.; Minagawa, T.; Nakajima, M.; Ryder, M.I.; Gotoh, K.; Motooka, D.; Nakamura, S.; Iida, T.; et al. Oral Pathobiont Induces Systemic Inflammation and Metabolic Changes Associated with Alteration of Gut Microbiota. Sci. Rep. 2015, 4, 4828. [Google Scholar] [CrossRef] [Green Version]
- Crump, K.E.; Oakley, J.C.; Xia-Juan, X.; Madu, T.C.; Devaki, S.; Mooney, E.C.; Sahingur, S.E. Interplay of Toll-Like Receptor 9, Myeloid Cells, and Deubiquitinase A20 in Periodontal Inflammation. Infect. Immun. 2017, 85, e00814-16. [Google Scholar] [CrossRef] [Green Version]
- Desoye, G.; Hauguel-de Mouzon, S. The Human Placenta in Gestational Diabetes Mellitus. The Insulin and Cytokine Network. Diabetes Care 2007, 30 (Suppl. S2), S120–S126. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Zhao, Y.H.; Chen, Y.P.; Yuan, X.L.; Wang, J.; Zhu, H.; Lu, C.M. Maternal Circulating Concentrations of Tumor Necrosis Factor-Alpha, Leptin, and Adiponectin in Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Sci. J. 2014, 2014, 926932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jawerbaum, A.; González, E. Diabetic Pregnancies: The Challenge of Developing in a pro-Inflammatory Environment. Curr. Med. Chem. 2006, 13, 2127–2138. [Google Scholar] [CrossRef]
- Sibiak, R.; Jankowski, M.; Gutaj, P.; Mozdziak, P.; Kempisty, B.; Wender-Ożegowska, E. Placental Lactogen as a Marker of Maternal Obesity, Diabetes, and Fetal Growth Abnormalities: Current Knowledge and Clinical Perspectives. JCM 2020, 9, 1142. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, A.M.; Giuffrida, D.; Moretti, L.; Re, P.; Grassi, G.; Menato, G.; Rolfo, A. Placental and Maternal SFlt1/PlGF Expression in Gestational Diabetes Mellitus. Sci. Rep. 2021, 11, 2312. [Google Scholar] [CrossRef]
- Barbour, L.A.; Shao, J.; Qiao, L.; Pulawa, L.K.; Jensen, D.R.; Bartke, A.; Garrity, M.; Draznin, B.; Friedman, J.E. Human Placental Growth Hormone Causes Severe Insulin Resistance in Transgenic Mice. Am. J. Obstet. Gynecol. 2002, 186, 512–517. [Google Scholar] [CrossRef]
- Fleenor, D.; Oden, J.; Kelly, P.A.; Mohan, S.; Alliouachene, S.; Pende, M.; Wentz, S.; Kerr, J.; Freemark, M. Roles of the Lactogens and Somatogens in Perinatal and Postnatal Metabolism and Growth: Studies of a Novel Mouse Model Combining Lactogen Resistance and Growth Hormone Deficiency. Endocrinology 2005, 146, 103–112. [Google Scholar] [CrossRef]
- Mariotti, A. Sex Steroid Hormones and Cell Dynamics in the Periodontium. Crit. Rev. Oral Biol. Med. 1994, 5, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Su, Y.; Xiong, X.; Harville, E.; Wu, H.; Jiang, Z.; Qian, X. Prevalence and Risk Factors of Periodontal Disease among Pre-Conception Chinese Women. Reprod. Health 2016, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Güncü, G.; Tözüm, T.; Çaglayan, F. Effects of Endogenous Sex Hormones on the Periodontium—Review of Literature. Aust. Dent. J. 2005, 50, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, A.J. Estrogen and Extracellular Matrix Influence Human Gingival Fibroblast Proliferation and Protein Production. J. Periodontol. 2005, 76, 1391–1397. [Google Scholar] [CrossRef]
- Yao, H.; Xu, D.; Zhu, Z.; Wang, G. Gestational Diabetes Mellitus Increases the Detection Rate and the Number of Oral Bacteria in Pregnant Women. Medicine 2019, 98, e14903. [Google Scholar] [CrossRef] [PubMed]
- Chokwiriyachit, A.; Dasanayake, A.P.; Suwannarong, W.; Hormdee, D.; Sumanonta, G.; Prasertchareonsuk, W.; Wara-Aswapati, N.; Combellick, J.; Pitiphat, W. Periodontitis and Gestational Diabetes Mellitus in Non-Smoking Females. J. Periodontol. 2013, 84, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Sharma, D.S.; Verma, M.; Lamba, A.K.; Gupta, M.M.; Sharma, S.; Perumal, V. Association between Periodontal Disease and Gestational Diabetes Mellitus-A Prospective Cohort Study. J. Clin. Periodontol. 2018, 45, 920–931. [Google Scholar] [CrossRef]
- Abariga, S.A.; Whitcomb, B.W. Periodontitis and Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Observational Studies. BMC Pregnancy Childbirth 2016, 16, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, H.; Xiong, X. Periodontitis May Be Associated with Gestational Diabetes Mellitus but Not Affirmatively. J. Evid. Based Dent. Pract. 2016, 16, 121–123. [Google Scholar] [CrossRef]
- Esteves Lima, R.P.; Cyrino, R.M.; de Carvalho Dutra, B.; Oliveira da Silveira, J.; Martins, C.C.; Miranda Cota, L.O.; Costa, F.O. Association Between Periodontitis and Gestational Diabetes Mellitus: Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 48–57. [Google Scholar] [CrossRef]
- Chaparro, A.; Zúñiga, E.; Varas-Godoy, M.; Albers, D.; Ramírez, V.; Hernández, M.; Kusanovic, J.P.; Acuña-Gallardo, S.; Rice, G.; Illanes, S.E. Periodontitis and Placental Growth Factor in Oral Fluids Are Early Pregnancy Predictors of Gestational Diabetes Mellitus. J. Periodontol. 2018, 89, 1052–1060. [Google Scholar] [CrossRef]
- Xiong, X.; Buekens, P.; Vastardis, S.; Pridjian, G. Periodontal Disease and Gestational Diabetes Mellitus. Am. J. Obstet. Gynecol. 2006, 195, 1086–1089. [Google Scholar] [CrossRef] [PubMed]
- Novak, K.F.; Taylor, G.W.; Dawson, D.R.; Ii, J.E.F.; Novak, M.J. Periodontitis and Gestational Diabetes Mellitus: Exploring the Link in NHANES III. J. Public Health Dent. 2006, 66, 163–168. [Google Scholar] [CrossRef]
- Foratori-Junior, G.A.; Jesuino, B.G.; Caracho, R.A.; Orenha, E.S.; Groppo, F.C.; Sales-Peres, S.H. de C. Association between Excessive Maternal Weight, Periodontitis during the Third Trimester of Pregnancy, and Infants’ Health at Birth. J. Appl. Oral. Sci. 2020, 28, e20190351. [Google Scholar] [CrossRef]
- Foratori-Junior, G.A.; Missio, A.L.T.; Orenha, E.S.; de Carvalho Sales-Peres, S.H. Systemic Condition, Periodontal Status, and Quality of Life in Obese Women During Pregnancy and After Delivery. Int. Dent. J. 2021, 71, 420–428. [Google Scholar] [CrossRef]
- Bi, W.G.; Emami, E.; Luo, Z.-C.; Santamaria, C.; Wei, S.Q. Effect of Periodontal Treatment in Pregnancy on Perinatal Outcomes: A Systematic Review and Meta-Analysis. J. Matern.-Fetal Neonatal Med. 2019, 34, 3259–3268. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.W.; Wang, X. Mobile Microbiome: Oral Bacteria in Extra-Oral Infections and Inflammation. J. Dent. Res. 2013, 92, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bearfield, C.; Davenport, E.S.; Sivapathasundaram, V.; Allaker, R.P. Possible Association between Amniotic Fluid Micro-Organism Infection and Microflora in the Mouth. Br. J. Obstet. Gynaecol. 2002, 109, 527–533. [Google Scholar] [CrossRef]
- Klebanoff, M.; Searle, K. The Role of Inflammation in Preterm Birth-Focus on Periodontitis. BJOG: Int. J. Obstet. Gynaecol. 2006, 113, 43–45. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, F.; Hasegawa-Nakamura, K.; Nakamura, T.; Oogai, Y.; Komatsuzawa, H.; Kawamata, K.; Douchi, T.; Hatae, M.; Noguchi, K. Detection of Fusobacterium Nucleatum in Chorionic Tissues of High-Risk Pregnant Women. J. Clin. Periodontol. 2012, 39, 417–424. [Google Scholar] [CrossRef]
- Chopra, A.; Radhakrishnan, R.; Sharma, M. Porphyromonas Gingivalis and Adverse Pregnancy Outcomes: A Review on Its Intricate Pathogenic Mechanisms. Crit. Rev. Microbiol. 2020, 46, 213–236. [Google Scholar] [CrossRef]
- Reyes, L.; Phillips, P.; Wolfe, B.; Golos, T.G.; Walkenhorst, M.; Progulske-Fox, A.; Brown, M. Porphyromonas Gingivalis and Adverse Pregnancy Outcome. J. Oral Microbiol. 2017, 9, 1374153. [Google Scholar] [CrossRef] [Green Version]
- Fan, M.; Li, X.; Gao, X.; Dong, L.; Xin, G.; Chen, L.; Qiu, J.; Xu, Y. LPS Induces Preeclampsia-Like Phenotype in Rats and HTR8/SVneo Cells Dysfunction Through TLR4/P38 MAPK Pathway. Front. Physiol. 2019, 10, 1030. [Google Scholar] [CrossRef] [Green Version]
- Ren, H.; Li, Y.; Jiang, H.; Du, M. Porphyromonas Gingivalis Induces IL-8 and IFN-Gamma Secretion and Apoptosis in Human Extravillous Trophoblast Derived HTR8/SVneo Cells via Activation of ERK1/2 and P38 Signaling Pathways. Placenta 2016, 45, 8–15. [Google Scholar] [CrossRef]
- Ganiger, K.; Sridharan, S.; Rahul, A.; Satyanarayana, A. Quantitative Analysis of Key Periodontopathic Bacteria in Gestational Diabetic and Non-Diabetic Women. J. Diabetes Metab Disord 2019, 18, 363–369. [Google Scholar] [CrossRef]
- Li, X.; Zheng, J.; Ma, X.; Zhang, B.; Zhang, J.; Wang, W.; Sun, C.; Wang, Y.; Zheng, J.; Chen, H.; et al. The Oral Microbiome of Pregnant Women Facilitates Gestational Diabetes Discrimination. J. Genet. Genom. 2021, 48, 32–39. [Google Scholar] [CrossRef]
- Balle, C.; Esra, R.; Havyarimana, E.; Jaumdally, S.Z.; Lennard, K.; Konstantinus, I.N.; Barnabas, S.L.; Happel, A.-U.; Gill, K.; Pidwell, T.; et al. Relationship between the Oral and Vaginal Microbiota of South African Adolescents with High Prevalence of Bacterial Vaginosis. Microorganisms 2020, 8, 1004. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Rajora, P.; Parihar, A.; Kaur, P.; Gandhi, P.; Gandhi, V. Evaluation of Effect of Gestational Diabetes Mellitus on Composition of the Initial Oral Microbiota of Neonates. Adv. Biomed Res. 2020, 9, 78. [Google Scholar] [CrossRef]
- Grossi, S.G.; Genco, R.J. Periodontal Disease and Diabetes Mellitus: A Two-Way Relationship. Ann. Periodontol. 1998, 3, 51–61. [Google Scholar] [CrossRef]
- Paraskevas, S.; Huizinga, J.D.; Loos, B.G. A Systematic Review and Meta-Analyses on C-Reactive Protein in Relation to Periodontitis. J. Clin. Periodontol. 2008, 35, 277–290. [Google Scholar] [CrossRef]
- Cutando, A.; López-Valverde, A.; de Diego, R.G.; de Vicente, J.; Reiter, R.; Herrero Fernández, M.; Ferrera, M.J. Effect of Topical Application of Melatonin to the Gingiva on Salivary Osteoprotegerin, RANKL and Melatonin Levels in Patients with Diabetes and Periodontal Disease. Odontology 2014, 102, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, A.; Realini, O.; Hernández, M.; Albers, D.; Weber, L.; Ramírez, V.; Param, F.; Kusanovic, J.P.; Sorsa, T.; Rice, G.E.; et al. Early Pregnancy Levels of Gingival Crevicular Fluid Matrix Metalloproteinases-8 and -9 Are Associated with the Severity of Periodontitis and the Development of Gestational Diabetes Mellitus. J. Periodontol. 2021, 92, 205–215. [Google Scholar] [CrossRef]
- Fedorova, N.V.; Ksenofontov, A.L.; Serebryakova, M.V.; Stadnichuk, V.I.; Gaponova, T.V.; Baratova, L.A.; Sud’ina, G.F.; Galkina, S.I. Neutrophils Release Metalloproteinases during Adhesion in the Presence of Insulin, but Cathepsin G in the Presence of Glucagon. Mediat. Inflamm 2018, 2018, 1574928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, M.S.; Vamsi, G.; Sripriya, R.; Sehgal, P.K. Expression of Matrix Metalloproteinases (MMP-8 and -9) in Chronic Periodontitis Patients with and without Diabetes Mellitus. J. Periodontol. 2006, 77, 1803–1808. [Google Scholar] [CrossRef]
- Théry, C.; Witwer, K.W.; Aikawa, E.; Alcaraz, M.J.; Anderson, J.D.; Andriantsitohaina, R.; Antoniou, A.; Arab, T.; Archer, F.; Atkin-Smith, G.K.; et al. Minimal Information for Studies of Extracellular Vesicles 2018 (MISEV2018): A Position Statement of the International Society for Extracellular Vesicles and Update of the MISEV2014 Guidelines. J. Extracell. Vesicles 2018, 7, 1535750. [Google Scholar] [CrossRef] [Green Version]
- Théry, C.; Ostrowski, M.; Segura, E. Membrane Vesicles as Conveyors of Immune Responses. Nat. Rev. Immunol. 2009, 9, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Yuana, Y.; Sturk, A.; Nieuwland, R. Extracellular Vesicles in Physiological and Pathological Conditions. Blood Rev. 2013, 27, 31–39. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Hassan, M.Q.; Jafferji, M.; Aqeilan, R.I.; Garzon, R.; Croce, C.M.; van Wijnen, A.J.; Stein, J.L.; Stein, G.S.; Lian, J.B. Biological Functions of MiR-29b Contribute to Positive Regulation of Osteoblast Differentiation. J. Biol. Chem. 2009, 284, 15676–15684. [Google Scholar] [CrossRef] [Green Version]
- Lian, J.B.; Stein, G.S.; van Wijnen, A.J.; Stein, J.L.; Hassan, M.Q.; Gaur, T.; Zhang, Y. MicroRNA Control of Bone Formation and Homeostasis. Nat. Rev. Endocrinol. 2012, 8, 212–227. [Google Scholar] [CrossRef] [Green Version]
- Buzas, E.I.; György, B.; Nagy, G.; Falus, A.; Gay, S. Emerging Role of Extracellular Vesicles in Inflammatory Diseases. Nat. Rev. Rheumatol. 2014, 10, 356–364. [Google Scholar] [CrossRef]
- Adam, S.; Elfeky, O.; Kinhal, V.; Dutta, S.; Lai, A.; Jayabalan, N.; Nuzhat, Z.; Palma, C.; Rice, G.E.; Salomon, C. Review: Fetal-Maternal Communication via Extracellular Vesicles—Implications for Complications of Pregnancies. Placenta 2017, 54, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Sáez, T.; de Vos, P.; Kuipers, J.; Sobrevia, L.; Faas, M.M. Fetoplacental Endothelial Exosomes Modulate High d -Glucose-Induced Endothelial Dysfunction. Placenta 2018, 66, 26–35. [Google Scholar] [CrossRef]
- Sáez, T.; de Vos, P.; Kuipers, J.; Sobrevia, L.; Faas, M.M. Exosomes Derived from Monocytes and from Endothelial Cells Mediate Monocyte and Endothelial Cell Activation under High D-Glucose Conditions. Immunobiology 2019, 224, 325–333. [Google Scholar] [CrossRef] [PubMed]
- James-Allan, L.B.; Rosario, F.J.; Barner, K.; Lai, A.; Guanzon, D.; McIntyre, H.D.; Lappas, M.; Powell, T.L.; Salomon, C.; Jansson, T. Regulation of Glucose Homeostasis by Small Extracellular Vesicles in Normal Pregnancy and in Gestational Diabetes. FASEB J. 2020, 34, 5724–5739. [Google Scholar] [CrossRef] [Green Version]
- Rice, G.E.; Scholz-Romero, K.; Sweeney, E.; Peiris, H.; Kobayashi, M.; Duncombe, G.; Mitchell, M.D.; Salomon, C. The Effect of Glucose on the Release and Bioactivity of Exosomes From First Trimester Trophoblast Cells. J. Clin. Endocrinol. Metab. 2015, 100, E1280–E1288. [Google Scholar] [CrossRef] [PubMed]
- Sarker, S.; Scholz-Romero, K.; Perez, A.; Illanes, S.E.; Mitchell, M.D.; Rice, G.E.; Salomon, C. Placenta-Derived Exosomes Continuously Increase in Maternal Circulation over the First Trimester of Pregnancy. J. Transl. Med. 2014, 12, 204. [Google Scholar] [CrossRef] [Green Version]
- Salomon, C.; Torres, M.J.; Kobayashi, M.; Scholz-Romero, K.; Sobrevia, L.; Dobierzewska, A.; Illanes, S.E.; Mitchell, M.D.; Rice, G.E. A Gestational Profile of Placental Exosomes in Maternal Plasma and Their Effects on Endothelial Cell Migration. PLoS ONE 2014, 9, e98667. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Liang, H.; Zhang, J.; Zen, K.; Zhang, C.-Y. Secreted MicroRNAs: A New Form of Intercellular Communication. Trends Cell Biol. 2012, 22, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Yáñez-Mó, M.; Siljander, P.R.-M.; Andreu, Z.; Zavec, A.B.; Borràs, F.E.; Buzas, E.I.; Buzas, K.; Casal, E.; Cappello, F.; Carvalho, J.; et al. Biological Properties of Extracellular Vesicles and Their Physiological Functions. J. Extracell. Vesicles 2015, 4, 27066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, L.J.; Varas-Godoy, M.; Monckeberg, M.; Realini, O.; Hernández, M.; Rice, G.; Romero, R.; Saavedra, J.F.; Illanes, S.E.; Chaparro, A. Oral Extracellular Vesicles in Early Pregnancy Can Identify Patients at Risk of Developing Gestational Diabetes Mellitus. PLoS ONE 2019, 14, e0218616. [Google Scholar] [CrossRef]
- Chaparro Padilla, A.; Weber Aracena, L.; Realini Fuentes, O.; Albers Busquetts, D.; Hernandez Ríos, M.R.; Ramirez Lobos, V.; Pascual La Roca, A.; Nart Molina, J.; Beltrán Varas, V.; Acuña-Gallardo, S.; et al. Molecular Signatures of Extracellular Vesicles in Oral Fluids of Periodontitis Patients. J. Oral Dis. 2020, 26, 1318–1325. [Google Scholar] [CrossRef]
- Nakahara, A. Exosome Profiles for Normal and Complicated Pregnancies. Obstet. Gynecol. 2019, 133, 162. [Google Scholar] [CrossRef]
- Nair, S.; Jayabalan, N.; Guanzon, D.; Palma, C.; Scholz-Romero, K.; Elfeky, O.; Zuñiga, F.; Ormazabal, V.; Diaz, E.; Rice, G.E.; et al. Human Placental Exosomes in Gestational Diabetes Mellitus Carry a Specific Set of MiRNAs Associated with Skeletal Muscle Insulin Sensitivity. Clin. Sci. 2018, 132, 2451–2467. [Google Scholar] [CrossRef]
- Li, J.; Song, L.; Zhou, L.; Wu, J.; Sheng, C.; Chen, H.; Liu, Y.; Gao, S.; Huang, W. A MicroRNA Signature in Gestational Diabetes Mellitus Associated with Risk of Macrosomia. Cell. Physiol. Biochem. 2015, 37, 243–252. [Google Scholar] [CrossRef]
- Rahimi, G.; Jafari, N.; Khodabakhsh, M.; Shirzad, Z.; Dogaheh, H.P. Upregulation of MicroRNA Processing Enzymes Drosha and Dicer in Gestational Diabetes Mellitus. Gynecol. Endocrinol. 2015, 31, 156–159. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Disease | Parameters | Targets | Experimental Design | Statistical Index | Value (Cases vs. Controls) | (95% CI) | p-Value | References |
|---|---|---|---|---|---|---|---|---|
| GDM | (a) GI (b) PI (c) TMD (d) PPD (e) BOP | GDM (n = 65) and euglycemic pregnant women (n = 331) | Case–control | Mean values | (a) 1.98 vs. 0.86 (b) 2.65 vs. 0.62 (c) 1.15 vs. 0.84 (d) 3.92 vs. 2.20 (e) 56% and 7% *GDM vs. controls | All parameters p < 0.001 | [62] | |
| GDM | (a) PPD (b) CAL (c) BOP (d) Periodontitis and GDM association | GDM (n = 50) and euglycemic pregnant women (n = 50) | Case–control | Mean values and aOR | (a) 2.4 v/s 2.1 (b) 1.4 v/s 0.9 (c) 83.2% v/s 60.2 %. (d) aOR: 7.92 *GDM vs. controls | aOR: 1.66–37.70 | (a)p = 0.02 (b)p = 0.003 (c) p = 0.001 (d) not reported | [63] |
| GDM and PE | (a) GDM incidence (b) Periodontitis and GDM association (c) Periodontitis and PE association (d) Periodontitis, GDM, and PE association | Periodontitis (n = 148), gingivitis (n = 184) and periodontally healthy pregnant women (n = 252) | Case–control | Mean values and aHR | (a) 19.6% v/s 4.4% (b) aHR: 4.12 (c) aHR: 2.20 (d) aHR: 18.79 *Periodontitis vs. controls | Periodontitis and GDM: 2.05–8.29 Periodontitis and PE: 0.86–5.6 Periodontitis, GDM, and PE: 7.45–47.4 | (a,b) p = 0.001 (c) p = 0.01 (d) p = 0.001 | [64] |
| GDM | (a) Periodontitis and GDM association in overall studies (b) Periodontitis and GDM association in high-quality studies | Cases (n = 624) and controls (n = 5724) in all studies Cases (n = 380) and controls (n = 1176) in high-quality studies | SR with MA | OR aOR | (a) OR: 1.66 (b.1) OR: 1.85 (b.2) aOR: 2.08 | (a) 1.17–2.36 (b.1) 1.03–3.32 (b.2) 1.21–3.58 | (a,b.1) p < 0.05 (b.2) p = 0.009 | [65] |
| GDM | (a) Periodontitis and GDM association in cross-sectional studies (b) Periodontitis and GDM association in case–control studies | (a) GDM (n = 314) and controls (n = 4344) (b) GDM (n = 193) and controls (n = 396) | SR with MA | OR | (a) 1.67 (b) 1.69 | (a) 1.2–2.32 (b) 0.68–4.21 | Not reported | [67] |
| GDM | (a) BOP (b) PPD (c) CAL (d) PISA | GDM (n = 14) and cohort healthy pregnancies (n = 198) | Nested Case–control | Mean values | (a) 85.5 vs. 60% (b) 3.05 vs. 2.7 (c) 2.5 vs. 2.05 (d) 1548.9 vs. 877 *GDM vs. healthy cohort | (a,c,d) p < 0.001 (b) p = 0.002 | [68] | |
| Periodontitis | (a) Periodontitis prevalence (b) Periodontitis and GDM association (c) Periodontitis and past GDM association | Pregnant women (n = 256) with or without GDM, and non-pregnant women (n = 4234) | Case–control | Mean prevalence and aOR | (a) 44.8% vs. 13.2% (b) OR: 2.54 and aOR: 2.00 (c) OR: 2.07 *GDM vs. healthy pregnant woman | (b) OR: 0.94–6,86 and aOR: 0.65–6.2 (c) GDM OR: 0.67–6.37 | Not reported | [69] |
| GDM | (a) Periodontitis, current DM, and past GDM association | Women who had histories of GDM (n = 113) and women without GDM histories (n = 4131) and current DM | Case–control | OR | (a) 8.7 | (a) 2.5–29.8 | Not reported | [70] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bendek, M.J.; Canedo-Marroquín, G.; Realini, O.; Retamal, I.N.; Hernández, M.; Hoare, A.; Busso, D.; Monteiro, L.J.; Illanes, S.E.; Chaparro, A. Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle. Int. J. Mol. Sci. 2021, 22, 11831. https://doi.org/10.3390/ijms222111831
Bendek MJ, Canedo-Marroquín G, Realini O, Retamal IN, Hernández M, Hoare A, Busso D, Monteiro LJ, Illanes SE, Chaparro A. Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle. International Journal of Molecular Sciences. 2021; 22(21):11831. https://doi.org/10.3390/ijms222111831
Chicago/Turabian StyleBendek, María José, Gisela Canedo-Marroquín, Ornella Realini, Ignacio N. Retamal, Marcela Hernández, Anilei Hoare, Dolores Busso, Lara J. Monteiro, Sebastián E. Illanes, and Alejandra Chaparro. 2021. "Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle" International Journal of Molecular Sciences 22, no. 21: 11831. https://doi.org/10.3390/ijms222111831
APA StyleBendek, M. J., Canedo-Marroquín, G., Realini, O., Retamal, I. N., Hernández, M., Hoare, A., Busso, D., Monteiro, L. J., Illanes, S. E., & Chaparro, A. (2021). Periodontitis and Gestational Diabetes Mellitus: A Potential Inflammatory Vicious Cycle. International Journal of Molecular Sciences, 22(21), 11831. https://doi.org/10.3390/ijms222111831