
Salivary Immunoglobulin Gamma-3 Chain C Is a Promising Noninvasive Biomarker for Systemic Lupus Erythematosus

 ,
,  ,
, 
Abstract
:1. Introduction
2. Results
2.1. Salivary Protein Identification
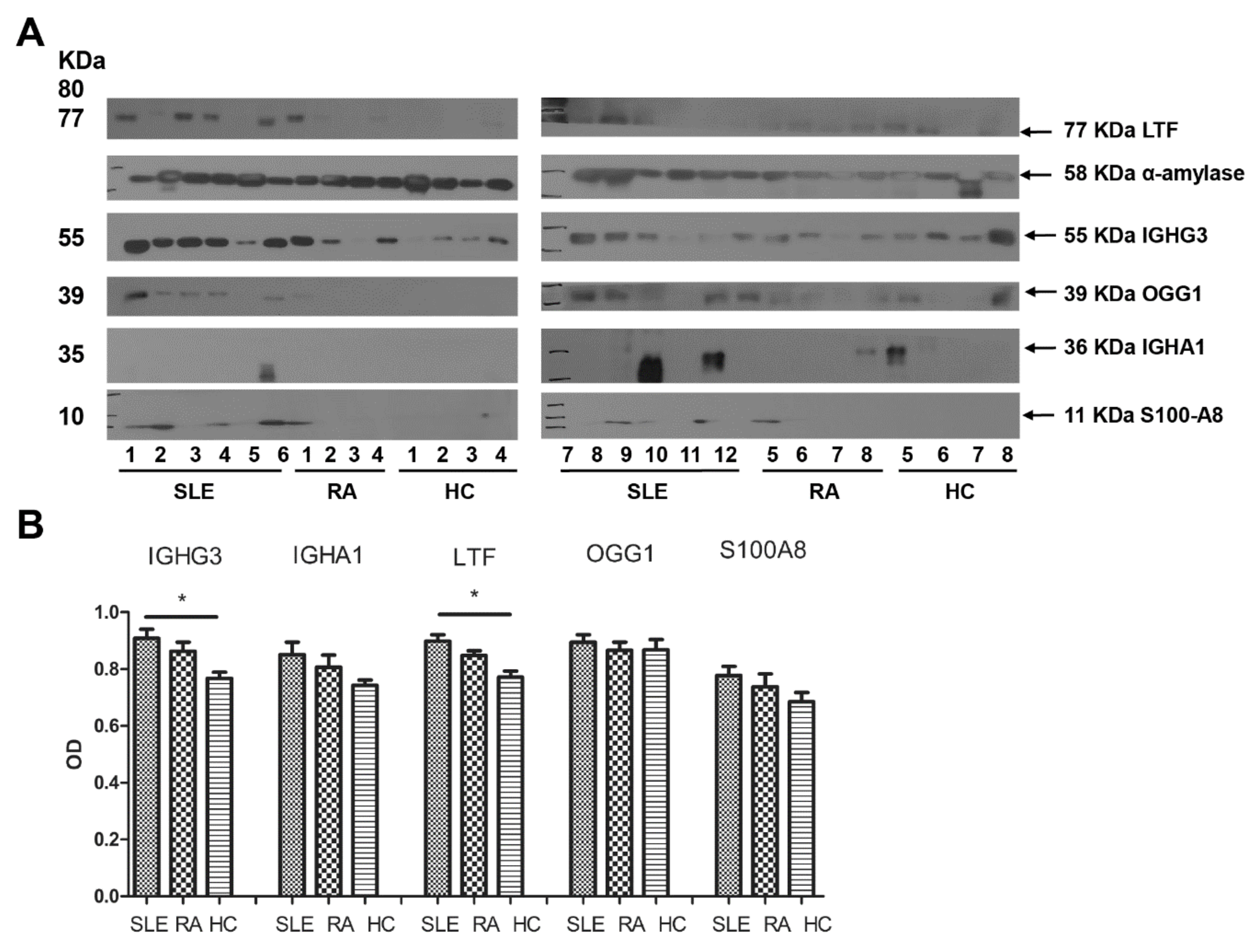
2.2. Expressions of Salivary Proteins in Patients with SLE
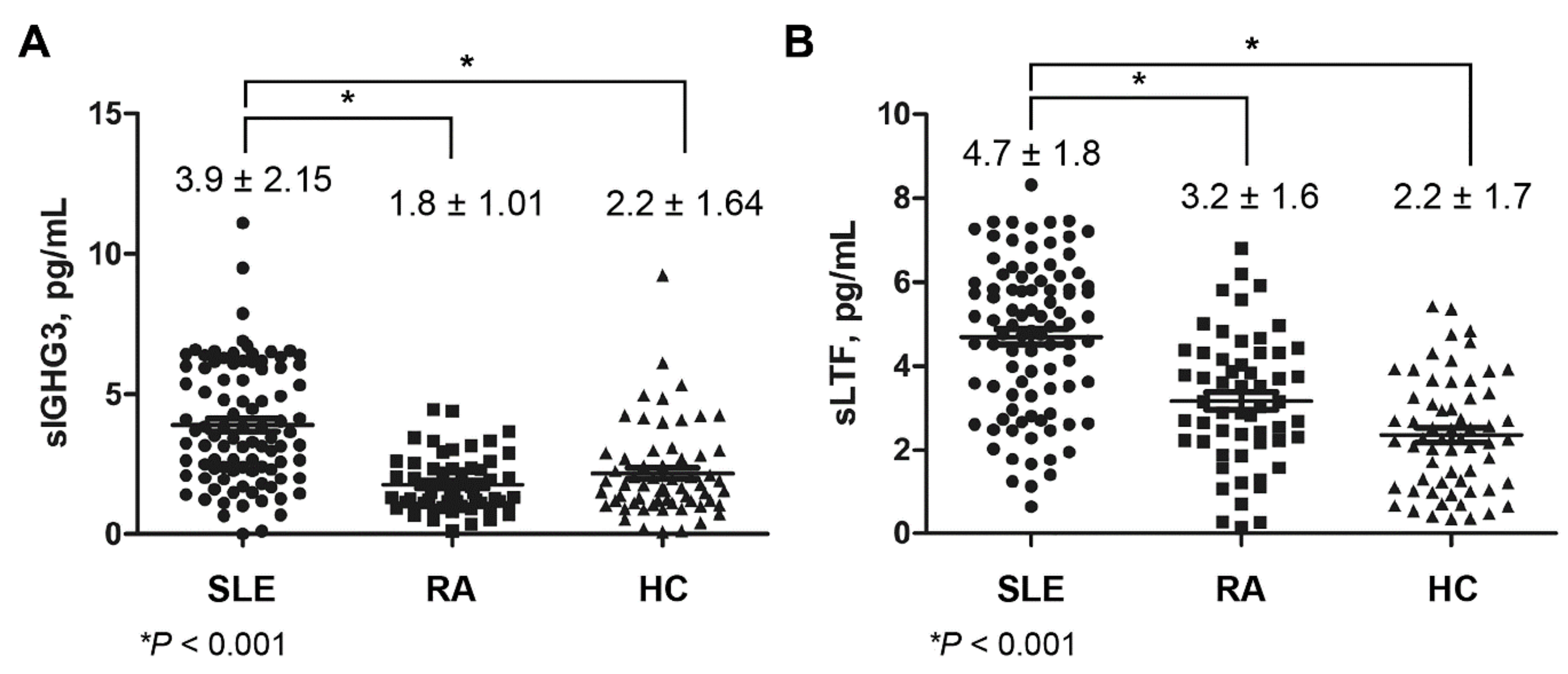
2.3. Expression of Salivary IGHG3 and Lactoferrin in SLE
2.4. Correlation of Salivary Proteins and Clinical Features in SLE
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Saliva Sample Collection
4.3. Two-Dimensional Gel Electrophoresis
4.4. Liquid Chromatography Tandem Mass Spectrometry
4.5. Western Blot Analysis
4.6. Enzyme-Linked Immunosorbent Assay
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SLE | Systemic Lupus Erythematosus |
| dsDNA | double-stranded DNA |
| 2DE | Two-Dimensional Gel Electrophoresis |
| MS | Mass Spectrometry |
| SS | Sjogren’s Syndrome |
| HCs | Healthy Controls |
| S100A8 | Protein S100-A8 |
| OGG1 | 8-oxoguanine DNA glycosylase |
| IGHG3 | Immunoglobulin gamma-3 chain c region |
| IGHA1 | Immunoglobulin alpha-1 chain c region |
| SLEDAI | Systemic Lupus Erythematosus Disease Activity Index |
| ESR | Erythrocyte Sedimentation Rate |
| LN | Lupus Nephritis |
| RA | Rheumatoid Arthritis |
| DAS28 | Disease Activity Score-28 |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under the Curve |
| CI | Confidence Interval |
| FcγR | Fcγ Receptor |
| RBC | Red Blood Cells |
| Th1 | T-helper cell type 1 |
| LC-MS | Liquid Chromatography tandem Mass Spectrometry |
| LTF | Lactoferrin |
| Ab | Antibody |
References
- Lisnevskaia, L.; Murphy, G.; Isenberg, D. Systemic lupus erythematosus. Lancet 2014, 384, 1878–1888. [Google Scholar] [CrossRef]
- Linnik, M.D.; Hu, J.Z.; Heilbrunn, K.R.; Strand, V.; Hurley, F.L.; Joh, T. LJP 394 investigator consortium. Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheumatol. 2005, 52, 1129–1137. [Google Scholar] [CrossRef]
- Pan, N.; Amigues, I.; Lyman, S.; Duculan, R.; Aziz, F.; Crow, M.K.; Kirou, K.A. A surge in anti-dsDNA titer predicts a severe lupus flare within six months. Lupus 2014, 23, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Mostoslavsky, G.; Fischel, R.; Yachimovich, N.; Yarkoni, Y.; Rosenmann, E.; Monestier, M.; Baniyash, M.; Eilat, D. Lupus anti-DNA autoantibodies cross-react with a glomerular structural protein: A case for tissue injury by molecular mimicry. Eur. J. Immunol. 2001, 31, 1221–1227. [Google Scholar] [CrossRef]
- Kavanaugh, A.F.; Solomon, D.H.; American College of Rheumatology ad hoc Committee on Immunologic Testing Guidelines. Guidelines for immunologic laboratory testing in the rheumatic diseases: Anti-DNA antibody tests. Arthritis Rheumatol. 2002, 47, 546–555. [Google Scholar] [CrossRef] [PubMed]
- ter Borg, E.J.; Horst, G.; Hummel, E.J.; Limburg, P.C.; Kallenberg, C.G. Measurement of increases in anti-double-stranded DNA antibody levels as a predictor of disease exacerbation in systemic lupus erythematosus. A long-term, prospective study. Arthritis Rheumatol. 1990, 33, 634–643. [Google Scholar]
- Ballou, S.P.; Kushner, I. Lupus patients who lack detectable anti-DNA: Clinical features and survival. Arthritis Rheumatol. 1982, 25, 1126–1129. [Google Scholar] [CrossRef]
- Truedsson, L.; Bengtsson, A.A.; Sturfelt, G. Complement deficiencies and systemic lupus erythematosus. Autoimmunity 2007, 40, 560–566. [Google Scholar] [CrossRef]
- Walport, M.J. Complement and systemic lupus erythematosus. Arthritis Res. 2002, 4 (Suppl. 3), S279–S293. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.; Shi, Y.; Cai, B.; Wang, L.; Wu, Y.; Ying, B.; Qin, L.; Hu, C.; Li, Y. MALDI-TOF MS combined with magnetic beads for detecting serum protein biomarkers and establishment of boosting decision tree model for diagnosis of systemic lupus erythematosus. Rheumatology 2009, 48, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Leitner, A.; Lindner, W. Chemical tagging strategies for mass spectrometry-based phospho-proteomics. Methods Mol. Biol. 2009, 527, 229–243. [Google Scholar] [PubMed]
- Kazemipour, N.; Qazizadeh, H.; Sepehrimanesh, M.; Salimi, S. Biomarkers identified from serum proteomic analysis for the differential diagnosis of systemic lupus erythematosus. Lupus 2015, 24, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, E.; Lamster, I.B. The diagnostic applications of saliva—A review. Crit. Rev. Oral Biol. Med. 2002, 13, 197–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamy, E.; Mau, M. Saliva proteomics as an emerging, non-invasive tool to study livestock physiology, nutrition and diseases. J. Proteom. 2012, 75, 4251–4258. [Google Scholar] [CrossRef]
- Abdul Rehman, S.; Khurshid, Z.; Hussain Niazi, F.; Naseem, M.; Al Waddani, H.; Sahibzada, H.A.; Sannam Khan, R. Role of salivary biomarkers in detection of cardiovascular diseases (CVD). Proteomes 2017, 5, 21. [Google Scholar] [CrossRef]
- Kaur, J.; Jacobs, R.; Huang, Y.; Salvo, N.; Politis, C. Salivary biomarkers for oral cancer and pre-cancer screening: A review. Clin. Oral Investig. 2018, 22, 633–640. [Google Scholar] [CrossRef]
- Navarro-Mendoza, E.P.; Aguirre-Valencia, D.; Posso-Osorio, I.; Correa-Forero, S.V.; Torres-Cutiva, D.F.; Loaiza, D.; Tobón, G.J. Cytokine markers of B lymphocytes in minor salivary gland infiltrates in Sjögren’s syndrome. Autoimmun. Rev. 2018, 17, 709–714. [Google Scholar] [CrossRef]
- Tzioufas, A.G.; Kapsogeorgou, E.K. Saliva proteomics is a promising tool to study Sjögren syndrome. Nat. Rev. Rheumatol. 2015, 11, 202–203. [Google Scholar] [CrossRef]
- Lee, J.; Baek, S.; Koh, J.H.; Kim, J.W.; Kim, S.Y.; Chung, S.H.; Choi, S.S.; Cho, M.L.; Kwok, S.K.; Ju, J.H.; et al. Soluble siglec-5 is a novel salivary biomarker for primary Sjogren’s syndrome. J. Autoimmun. 2019, 100, 114–119. [Google Scholar] [CrossRef]
- Baldini, C.; Giusti, L.; Ciregia, F.; Da Valle, Y.; Giacomelli, C.; Donadio, E.; Sernissi, F.; Bazzichi, L.; Giannaccini, G.; Bombardieri, S.; et al. Proteomic analysis of saliva: A unique tool to distinguish primary Sjögren’s syndrome from secondary Sjögren’s syndrome and other sicca syndromes. Arthritis Res. Ther. 2011, 13, R194. [Google Scholar] [CrossRef] [Green Version]
- Bave, U.; Magnusson, M.; Eloranta, M.L.; Perers, A.; Alm, G.V.; Ronnblom, L. Fc gamma RIIa is expressed on natural IFN-alpha-producing cells (plasmacytoid dendritic cells) and is required for the IFN-alpha production induced by apoptotic cells combined with lupus IgG. J. Immunol. 2003, 171, 3296–3302. [Google Scholar]
- Yap, D.Y.; Yung, S.; Zhang, Q.; Tang, C.; Chan, T.M. Serum level of proximal renal tubular epithelial cell-binding immunoglobulin G in patients with lupus nephritis. Lupus 2016, 25, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Guo, H.; Leung, J.C.; Chan, L.Y.; Chan, T.M.; Lai, K.N. The pathogenetic role of immunoglobulin G from patients with systemic lupus erythematosus in the development of lupus pleuritis. Rheumatology (Oxford) 2004, 43, 286–293. [Google Scholar] [CrossRef] [Green Version]
- Lai, M.; De Stefano, V.; Landolfi, R. Haemoglobin levels in autoimmune haemolytic anaemias at diagnosis: Relationship with immunoproteins on red blood cells. Immunol. Res. 2014, 60, 127–131. [Google Scholar]
- Kurasawa, K.; Arai, S.; Owada, T.; Maezawa, R.; Kumano, K.; Fukuda, T. Autoantibodies against platelet-derived growth factor receptor alpha in patients with systemic lupus erythematosus. Mod. Rheumatol. 2010, 20, 458–465. [Google Scholar]
- Thedsawad, A.; Taka, O.; Wanachiwanawin, W. Significances of red cell bound immunoglobulin g as detected by flow cytometry in patients with coombs-negative immune hemolysis. Transfus Med. 2016, 26, 130–137. [Google Scholar] [CrossRef]
- Manolova, I.; Dancheva, M.; Halacheva, K. Predominance of IgG1 and IgG3 subclasses of autoantibodies to neutrophil cytoplasmic antigens in patients with systemic lupus erythematosus. Rheumatol. Int. 2002, 21, 227–233. [Google Scholar] [CrossRef]
- Elenitsas, R.; Abell, E.; Lee, Y.Y.; Huang, J.; Deng, J.S. Comparison of IgG subclass autoantibodies in patients with systemic lupus erythematosus and subacute cutaneous lupus erythematosus. J. Dermatol. Sci. 1990, 1, 207–215. [Google Scholar] [CrossRef]
- Pan, Q.; Guo, L.; Wu, J.; Cai, J.; Liao, H.; Lan, Q.; Peng, Y.; He, Y.; Liu, H.F. Association between IgG4 autoantibody and complement abnormalities in systemic lupus erythematosus. Mediat. Inflamm. 2016, 2016, 2196986. [Google Scholar] [CrossRef] [Green Version]
- Bashford-Rogers, R.J.M.; Bergamaschi, L.; McKinney, E.F.; Pombal, D.C.; Mescia, F.; Lee, J.C.; Thomas, D.C.; Flint, S.M.; Kellam, P.; Jayne, D.R.W.; et al. Analysis of the b cell receptor repertoire in six immune-mediated diseases. Nature 2019, 574, 122–126. [Google Scholar] [CrossRef]
- González-Chávez, S.A.; Arévalo-Gallegos, S.; Rascón-Cruz, Q. Lactoferrin: Structure, function and applications. Int. J. Antimicrob. Agents 2009, 33, e301–e308. [Google Scholar] [CrossRef] [PubMed]
- Legrand, D.; Elass, E.; Carpentier, M.; Mazurier, J. Lactoferrin: A modulator of immune and inflammatory responses. Cell. Mol. Life Sci. 2005, 62, 2549–2559. [Google Scholar] [CrossRef]
- Legrand, D.; Elass, E.; Carpentier, M.; Mazurier, J. Interactions of lactoferrin with cells involved in immune function. Biochem. Cell Biol. 2006, 84, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Caccavo, D.; Rigon, A.; Picardi, A.; Galluzzo, S.; Vadacca, M.; Ferri, G.M.; Amoroso, A.; Afeltra, A. Anti-lactoferrin antibodies in systemic lupus erythematosus: Isotypes and clinical correlates. Clin. Rheumatol. 2005, 24, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Li, K.J.; Lu, M.C.; Hsieh, S.C.; Wu, C.H.; Yu, H.S.; Tsai, C.Y.; Yu, C.L. Release of surface-expressed lactoferrin from polymorphonuclear neutrophils after contact with CD4+ T cells and its modulation on Th1/Th2 cytokine production. J. Leukoc. Biol. 2006, 80, 350–358. [Google Scholar] [CrossRef]
- Hu, L.; Hu, X.; Long, K.; Gao, C.; Dong, H.L.; Zhong, Q.; Gao, X.M.; Gong, F.Y. Extraordinarily potent proinflammatory properties of lactoferrin-containing immunocomplexes against human monocytes and macrophages. Sci. Rep. 2017, 7, 4230. [Google Scholar] [CrossRef]
- Gao, C.H.; Dong, H.L.; Tai, L.; Gao, X.M. Lactoferrin-containing immunocomplexes drive the conversion of human macrophages from M2-into M1-like phenotype. Front. Immunol. 2018, 9, 37. [Google Scholar] [CrossRef]
- Tan, E.M.; Cohen, A.S.; Fries, J.F.; Masi, A.T.; McShane, D.J.; Rothfield, N.F.; Schaller, J.G.; Talal, N.; Winchester, R.J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982, 25, 1271–1277. [Google Scholar] [CrossRef]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Shushan, B. A review of clinical diagnostic applications of liquid chromatography-tandem mass spectrometry. Mass Spectrom. Rev. 2010, 29, 930–944. [Google Scholar] [CrossRef]
- Park, C.; Kang, D.S.; Shin, G.H.; Seo, J.; Kim, H.; Suh, P.G.; Bae, C.D.; Shin, J.H. Identification of novel phosphatidic acid-binding proteins in the rat brain. Neurosci. Lett. 2015, 595, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Hmmier, A.; Dowling, P. DIGE analysis software and protein identification approaches. Methods Mol. Biol. 2018, 1664, 41–50. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Spot | Increased Protein Name | Fold of Variation SLE vs. HC | ANOVA, p-Value |
|---|---|---|---|
| 2 | Immunoglobulin gamma-3 chain C region | 4.101 | 0.000158 |
| 3 | S100A8 | 3.894 | 0.0045 |
| 6 | 8-oxoguanine DNA glycosylase | 3.516 | 0.00637 |
| 7 | S100A8 | 2.947 | 2.48 × 10−8 |
| 8 | Lactotransferrin | 2.827 | 4.06 × 10−7 |
| 9 | 8-oxoguanine DNA glycosylase | 2.794 | 0.00653 |
| Spot | Decreased Protein Name | Fold of Variation SLE vs. HC | ANOVA, p-Value |
| 1 | Alpha-amylase 1 | −4.228 | 0.000691 |
| 4 | Alpha-amylase 1 | −3.676 | 0.0372 |
| 5 | Immunoglobulin alpha-1 chain C region | −3.532 | 0.00511 |
| 10 | Leukemia-associated protein 7 | −2.176 | 0.0178 |
| Clinical Characteristics | IGHG3, pg/mL | Lactoferrin, pg/mL | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| ESR | 0.26 | 0.01 | −0.09 | 0.4 |
| Complement 3 | −0.02 | 0.89 | 0.21 | 0.05 |
| Complement 4 | −0.02 | 0.88 | 0.2 | 0.06 |
| Anti-dsDNA Ab (+) | 0.25 | 0.01 | −0.05 | 0.63 |
| Mucocutaneous involvement | 0.15 | 0.14 | 0.08 | 0.48 |
| Arthritis | −0.1 | 0.36 | 0.01 | 0.9 |
| Nephritis | 0.28 | 0.01 | −0.01 | 0.94 |
| Serositis | 0.04 | 0.74 | −0.15 | 0.16 |
| Hematologic disease | −0.02 | 0.83 | −0.08 | 0.45 |
| SLEDAI | 0.03 | 0.74 | −0.09 | 0.42 |
| Use of glucocorticoids | 0.15 | 0.06 | −0.07 | 0.41 |
| Dose of glucocorticoids | 0.09 | 0.25 | −0.05 | 0.57 |
| Use of immunosuppressants | 0.21 | 0.04 | 0.02 | 0.85 |
| Clinical Characteristics | SLE | RA | HC |
|---|---|---|---|
| Number | 94 | 57 | 62 |
| Age, years | 39.8 ± 9.8 | 41.0 ± 7.9 | 39.5 ± 6.9 |
| Sex (F/M) | 87/7 | 50/7 | 58/4 |
| Leukocyte, µL | 5165.4 ± 2364.9 | ||
| Hemoglobin, µL | 12.2 ± 2.4 | ||
| Platelet, ×103, µL | 221.8 ± 76.1 | ||
| Lymphocyte, µL | 1454.0 ± 654.0 | ||
| ESR, mm/h | 16.4 ± 18.0 | ||
| Complement 3, mg/dL | 85.2 ± 26.9 | ||
| Complement 4, mg/dL | 18.6 ± 8.9 | ||
| Anti-dsDNA Ab (+), n (%) | 41 (43.6) | ||
| Rheumatoid factor (+), n (%) | 45 (77.6) | ||
| Mucocutaneous involvement, n (%) | 28 (29.8) | ||
| Arthritis, n (%) | 31 (33.0) | ||
| Nephritis, n (%) | 29 (30.9) | ||
| Serositis, n (%) | 4 (3.8) | ||
| Hematologic involvement, n (%) | 35 (37.6) | ||
| SLEDAI | 3.8 ± 4.2 | ||
| DAS-28 | 3.3 ± 1.15 | ||
| Use of glucocorticoids, n (%) | 69 (73.4) | 44 (77.2) | |
| Dose of glucocorticoids, mg * | 3.1 ± 3.7 | 2.3 ± 1.8 | |
| Use of immunosuppressants, n (%) | 35 (37.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-Y.; Nam, J.-Y.; Ryu, K.-S.; Son, I.-O.; Shin, J.-H.; Baek, W.-Y.; Kim, H.-A.; Suh, C.-H. Salivary Immunoglobulin Gamma-3 Chain C Is a Promising Noninvasive Biomarker for Systemic Lupus Erythematosus. Int. J. Mol. Sci. 2021, 22, 1374. https://doi.org/10.3390/ijms22031374
Jung J-Y, Nam J-Y, Ryu K-S, Son I-O, Shin J-H, Baek W-Y, Kim H-A, Suh C-H. Salivary Immunoglobulin Gamma-3 Chain C Is a Promising Noninvasive Biomarker for Systemic Lupus Erythematosus. International Journal of Molecular Sciences. 2021; 22(3):1374. https://doi.org/10.3390/ijms22031374
Chicago/Turabian StyleJung, Ju-Yang, Jin-Young Nam, Keun-Sil Ryu, In-Ok Son, Joo-Ho Shin, Wook-Young Baek, Hyoun-Ah Kim, and Chang-Hee Suh. 2021. "Salivary Immunoglobulin Gamma-3 Chain C Is a Promising Noninvasive Biomarker for Systemic Lupus Erythematosus" International Journal of Molecular Sciences 22, no. 3: 1374. https://doi.org/10.3390/ijms22031374
APA StyleJung, J. -Y., Nam, J. -Y., Ryu, K. -S., Son, I. -O., Shin, J. -H., Baek, W. -Y., Kim, H. -A., & Suh, C. -H. (2021). Salivary Immunoglobulin Gamma-3 Chain C Is a Promising Noninvasive Biomarker for Systemic Lupus Erythematosus. International Journal of Molecular Sciences, 22(3), 1374. https://doi.org/10.3390/ijms22031374