Influence of Previous COVID-19 and Mastitis Infections on the Secretion of Brain-Derived Neurotrophic Factor and Nerve Growth Factor in Human Milk

 ,
,  ,
, 
Abstract
:
1. Introduction
2. Results
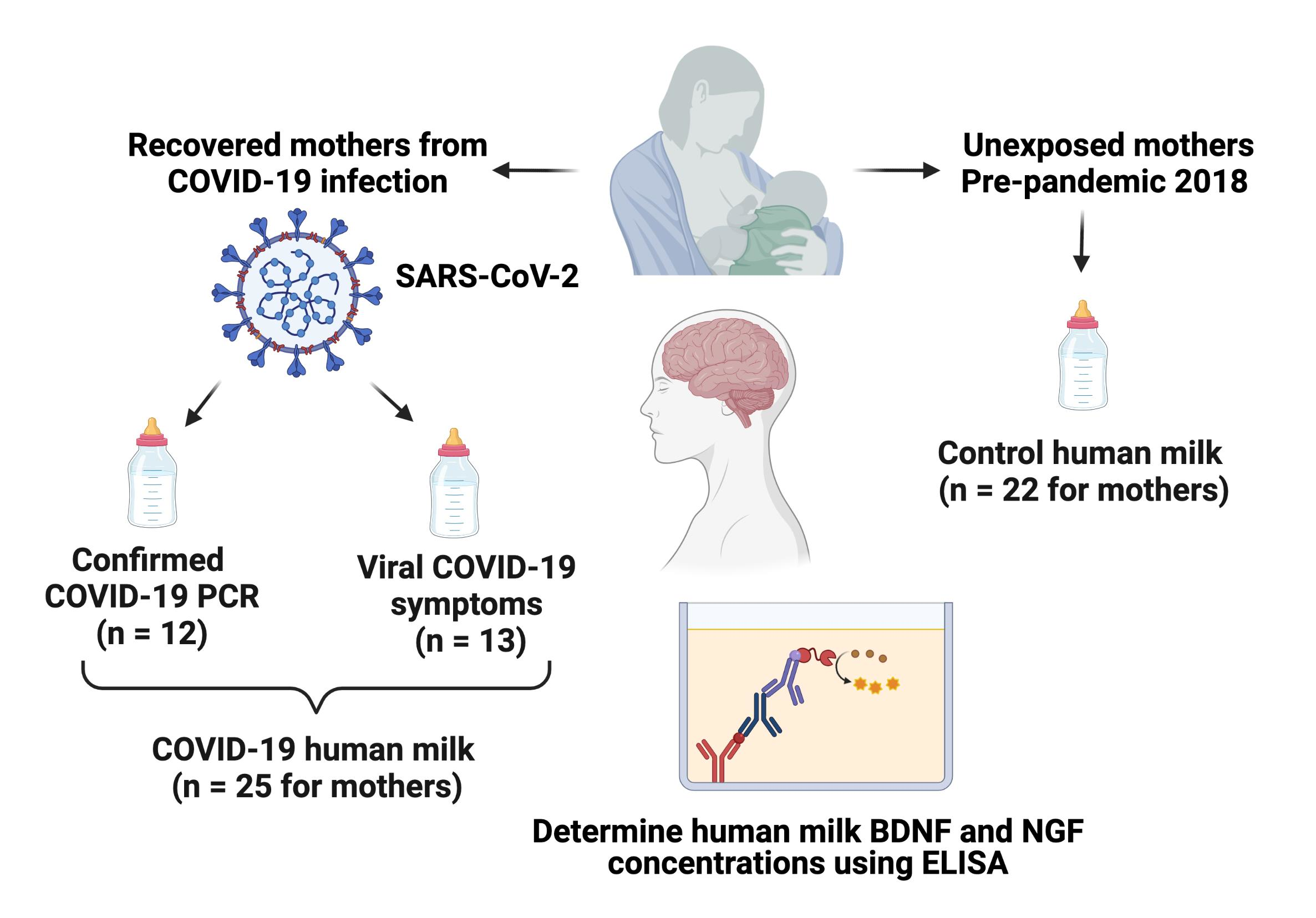
2.1. COVID-19 Study
2.1.1. Maternal Demographics
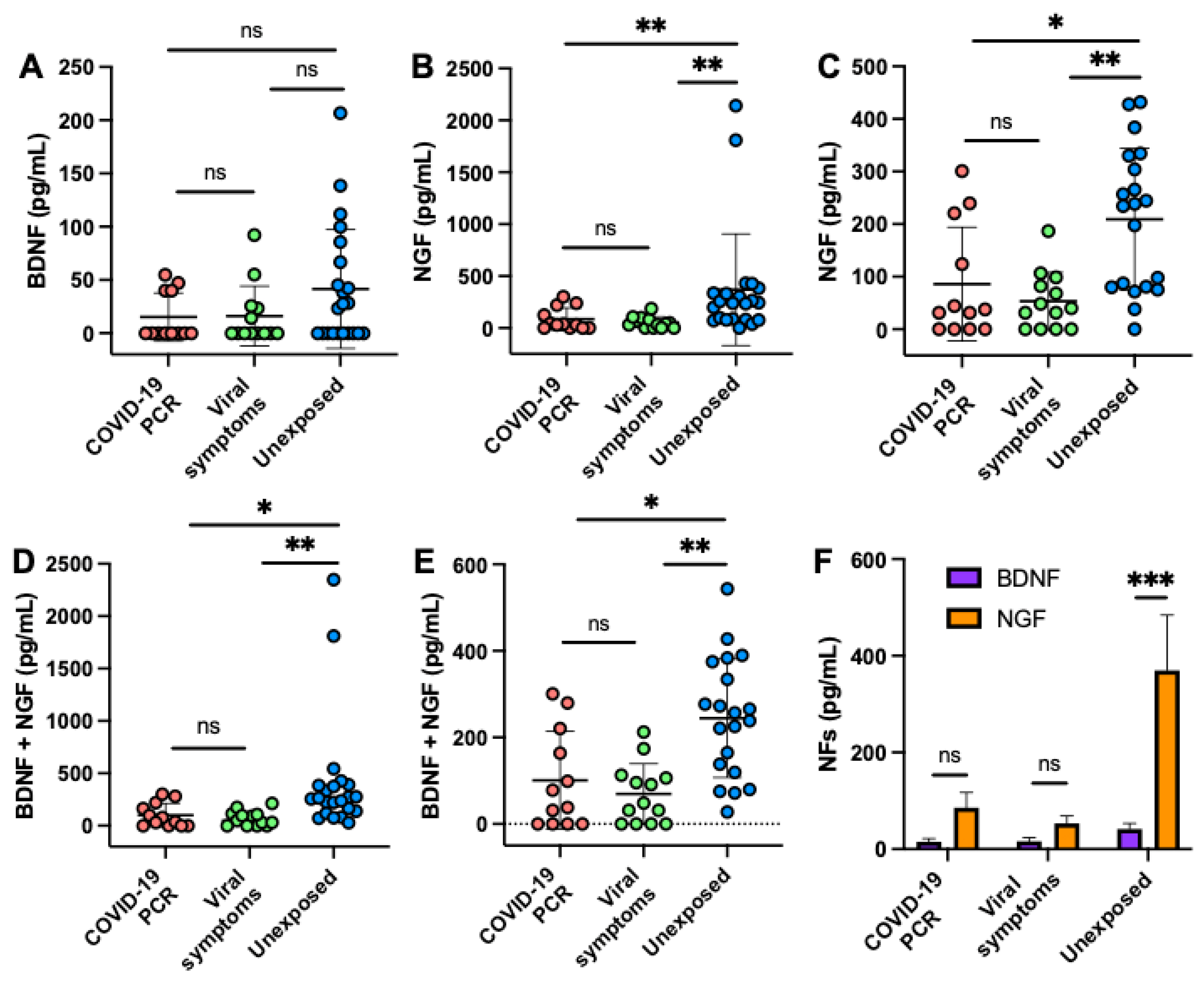
2.1.2. BDNF and NGF in Milk from COVID-19 and Unexposed Mothers
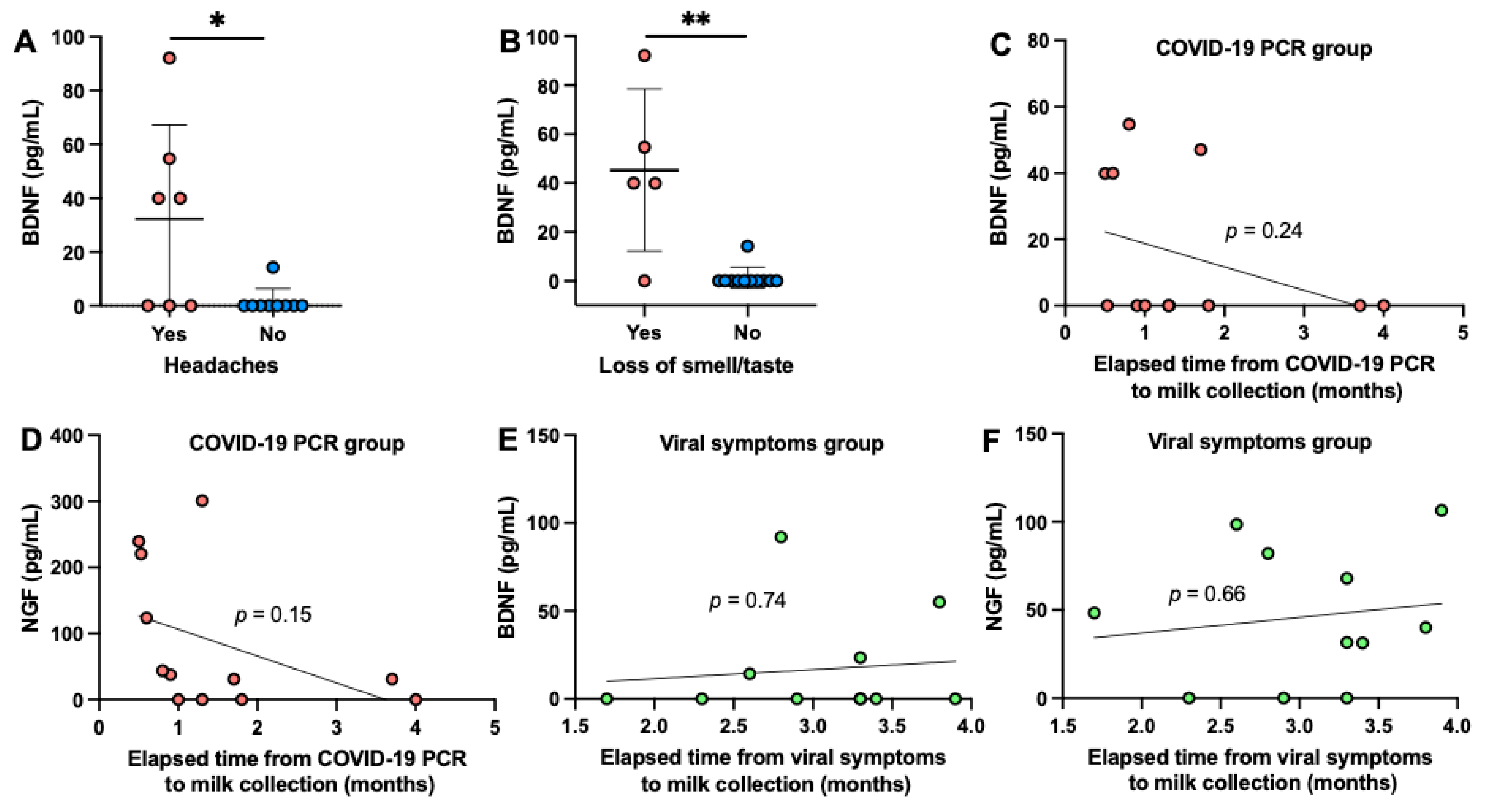
2.1.3. Effects of Maternal Factors on Human Milk BDNF and NGF
2.2. Mastitis Study
2.2.1. Maternal Demographics
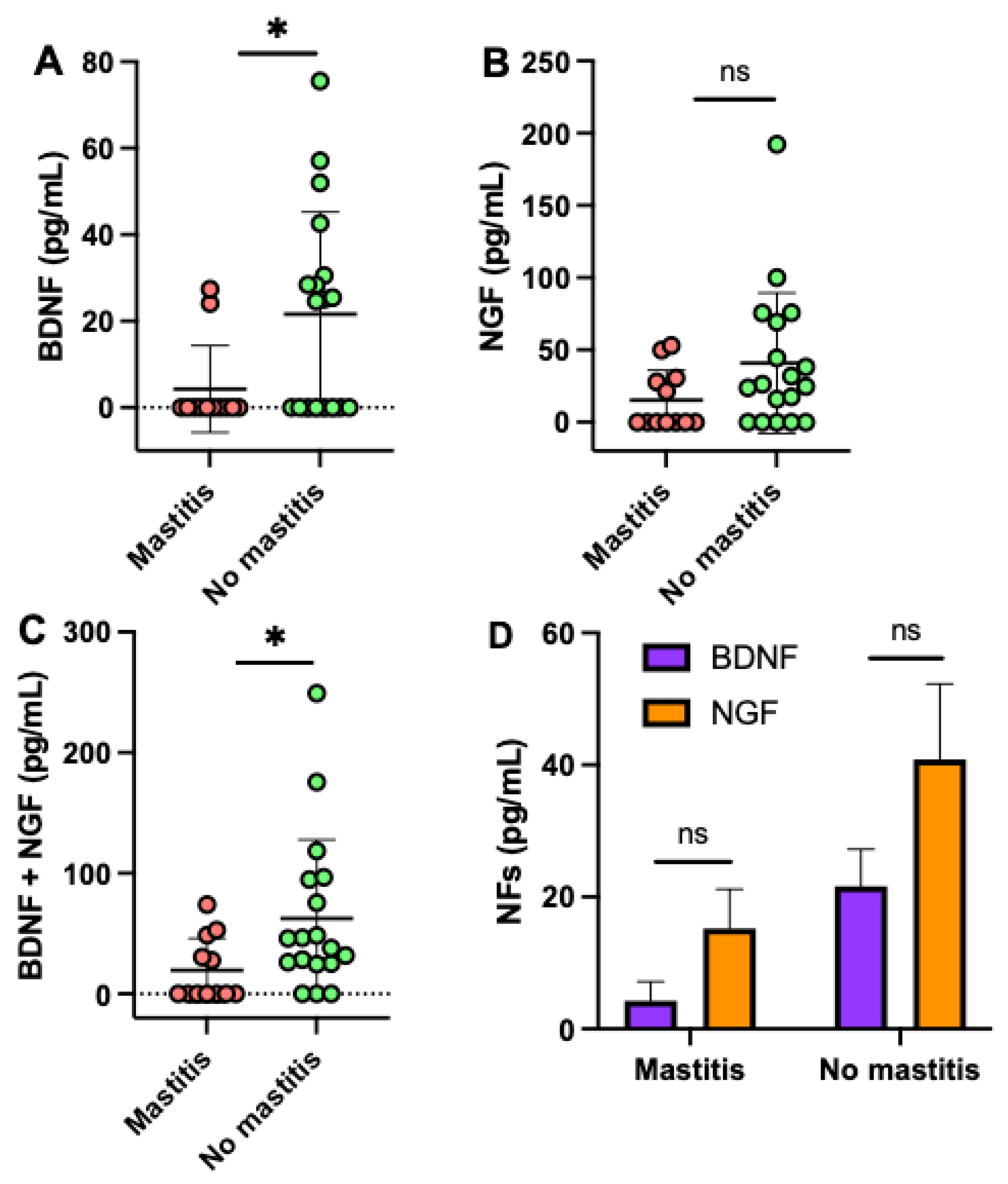
2.2.2. BDNF and NGF in Human Milk between Mastitis and No Mastitis Groups
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Human Milk Collection
4.3. BDNF and NGF Concentrations
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bondar, N.P.; Merkulova, T. Brain-derived neurotrophic factor and early-life stress: Multifaceted interplay. J. Biosci. 2016, 41, 751–758. [Google Scholar] [CrossRef]
- Boesmans, W.; Gomes, P.; Janssens, J.; Tack, J.; Berghe, P.V. Brain-derived neurotrophic factor amplifies neurotransmitter responses and promotes synaptic communication in the enteric nervous system. Gut 2008, 57, 314–322. [Google Scholar] [CrossRef]
- Mattson, M.P.; Maudsley, S.; Martin, B. BDNF and 5-HT: A dynamic duo in age-related neuronal plasticity and neurodegenerative disorders. Trends Neurosci. 2004, 27, 589–594. [Google Scholar] [CrossRef]
- Bekinschtein, P.; Cammarota, M.; Izquierdo, I.; Medina, J.H. Reviews: BDNF and memory formation and storage. Neuroscientist 2008, 14, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Barichello, T.; Lemos, J.; Generoso, J.S.; Carradore, M.M.; Moreira, A.P.; Collodel, A.; Zanatta, J.R.; Valvassori, S.S.; Quevedo, J. Evaluation of the brain-derived neurotrophic factor, nerve growth factor and memory in adult rats survivors of the neonatal meningitis by Streptococcus agalactiae. Brain Res. Bull. 2013, 92, 56–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nassar, M.F.; Younis, N.T.; El-Arab, S.E.; Fawzi, F.A. Neuro-developmental outcome and brain-derived neurotrophic factor level in relation to feeding practice in early infancy. Matern. Child. Nutr. 2011, 7, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Malamitsi-Puchner, A.; Economou, E.; Rigopoulou, O.; Boutsikou, T. Perinatal changes of brain-derived neurotrophic factor in pre-and fullterm neonates. Early Hum. Dev. 2004, 76, 17–22. [Google Scholar] [CrossRef]
- Chouthai, N.S.; Sampers, J.; Desai, N.; Smith, G.M. Changes in neurotrophin levels in umbilical cord blood from infants with different gestational ages and clinical conditions. Pediatr. Res. 2003, 53, 965–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almli, C.R.; Levy, T.; Han, B.H.; Shah, A.R.; Gidday, J.M.; Holtzman, D.M. BDNF protects against spatial memory deficits following neonatal hypoxia-ischemia. Exp. Neurol. 2000, 166, 99–114. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, P.B.; Jenkins, B.G.; Schulz, J.B.; Finkelstein, S.P.; Matthews, R.T.; Rosen, B.R.; Beal, M.F. NGF, BDNF and NT-5, but not NT-3 protect against MPP+ toxicity and oxidative stress in neonatal animals. Brain Res. 1996, 713, 178–185. [Google Scholar] [CrossRef]
- Nyárády, K.; Turai, R.; Funke, S.; Györgyi, E.; Makai, A.; Prémusz, V.; Bódis, J.; Sulyok, E. Effects of perinatal factors on sirtuin 3, 8-hydroxy-2′-deoxyguanosine, brain-derived neurotrophic factor and serotonin in cord blood and early breast milk: An observational study. Int. Breastfeed. J. 2020, 15, 1–8. [Google Scholar] [CrossRef]
- Dangat, K.; Kilari, A.; Mehendale, S.; Lalwani, S.; Joshi, S. Preeclampsia alters milk neurotrophins and long chain polyunsaturated fatty acids. Int. J. Dev. Neurosci. 2014, 33, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, E.; Hashimoto, K.; Okamura, N.; Koike, K.; Komatsu, N.; Kumakiri, C.; Nakazato, M.; Watanabe, H.; Shinoda, N.; Okada, S.I.; et al. Alterations of serum levels of brain-derived neurotrophic factor (BDNF) in depressed patients with or without antidepressants. Biol. Psychiatry 2003, 54, 70–75. [Google Scholar] [CrossRef]
- Branchi, I.; D’Andrea, I.; Fiore, M.; Di Fausto, V.; Aloe, L.; Alleva, E. Early social enrichment shapes social behavior and nerve growth factor and brain-derived neurotrophic factor levels in the adult mouse brain. Biol. Psychiatry 2006, 60, 690–696. [Google Scholar] [CrossRef]
- Torcia, M.; Bracci-Laudiero, L.; Lucibello, M.; Nencioni, L.; Labardi, D.; Rubartelli, A.; Cozzolino, F.; Aloe, L.; Garaci, E. Nerve growth factor is an autocrine survival factor for memory B lymphocytes. Cell 1996, 85, 345–356. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Laurent, S.; Onur, O.A.; Kleineberg, N.N.; Fink, G.R.; Schweitzer, F.; Warnke, C. A systematic review of neurological symptoms and complications of COVID-19. J. Neurol. 2020, 268, 392–402. [Google Scholar] [CrossRef]
- Azoulay, D.; Shehadeh, M.; Chepa, S.; Shaoul, E.; Barhom, M.; Horowitz, N.A.; Kaykov, E. Recovery from SARS-CoV-2 infection is associated with serum BDNF restoration. J. Infect. 2020, 81, e79–e81. [Google Scholar] [CrossRef]
- Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol# 4: Mastitis. Breastfeed. Med. 2008, 3, 177–180. [Google Scholar]
- Summers, A. Managing mastitis in the emergency department. Emerg. Nurse 2011, 19, 22–25. [Google Scholar] [CrossRef]
- Michie, C.; Lockie, F.; Lynn, W. The challenge of mastitis. Arch. Dis. Child. 2003, 88, 818–821. [Google Scholar] [CrossRef]
- Michie, C.A.; Gilmour, J.W. Breastfeeding and viral transmission: Risks, benefits and treatments. J. Trop. Pediatr. 2000, 46, 256–257. [Google Scholar] [CrossRef] [Green Version]
- Barichello, T.; Lemos, J.C.; Generoso, J.S.; Cipriano, A.L.; Milioli, G.L.; Marcelino, D.M.; Vuolo, F.; Petronilho, F.; Dal-Pizzol, F.; Vilela, M.C.; et al. Oxidative stress, cytokine/chemokine and disruption of blood–brain barrier in neonate rats after meningitis by Streptococcus agalactiae. Neurochem. Res. 2011, 36, 1922–1930. [Google Scholar] [CrossRef]
- Schanler, R.J.; Lau, C.; Hurst, N.M. Smith EOB. Randomized trial of donor human milk versus preterm formula as substitutes for mothers’ own milk in the feeding of extremely premature infants. Pediatrics 2018, 116, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Lanting, C.I.; Huisman, M.; Boersma, E.R.; Touwen, B.C.L.; Fidler, V. Neurological differences between 9-year-old children fed breast-milk or formula-milk as babies. Lancet 1994, 344, 1319–1922. [Google Scholar] [CrossRef]
- Lucas, A.; Morley, R.; Cole, T.J.; Lister, G.; Leeson-Payne, C. Breast milk and subsequent intelligence quotient in children born preterm. Lancet 1992, 339, 261–264. [Google Scholar] [CrossRef]
- Blesa, M.; Sullivan, G.; Anblagan, D.; Telford, E.J.; Quigley, A.J.; Sparrow, S.A.; Serag, A.; Semple, S.I.; Bastin, M.E.; Boardman, J.P. Early breast milk exposure modifies brain connectivity in preterm infants. Neuroimage 2019, 184, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Kremer, S.; Lersy, F.; de Sèze, J.; Ferré, J.C.; Maamar, A.; Carsin-Nicol, B.; Collange, O.; Bonneville, F.; Adam, G.; Martin-Blondel, G.; et al. Brain MRI findings in severe COVID-19: A retrospective observational study. Radiology 2020, 297, e242–e251. [Google Scholar] [CrossRef]
- Cardona, G.C.; Pájaro, L.D.; Marzola, I.D.; Villegas, Y.R.; Salazar, L.R. Neurotropism of SARS-CoV 2: Mechanisms and manifestations. J. Neurol. Sci. 2020, 412, 116824. [Google Scholar] [CrossRef]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Song, E.; Zhang, C.; Israelow, B.; Lu-Culligan, A.; Prado, A.V.; Skriabine, S.; Lu, P.; Weizman, O.E.; Liu, F.; Dai, Y.; et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J. Exp. Med. 2021, 218, e20202135. [Google Scholar] [CrossRef]
- Leon, A.; Buriani, A.; Dal Toso, R.; Fabris, M.; Romanello, S.; Aloe, L.; Levi-Montalcini, R. Mast cells synthesize, store, and release nerve growth factor. Proc. Natl. Acad. Sci. USA 1994, 91, 3739–3743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morichi, S.; Yamanaka, G.; Ishida, Y.; Oana, S.; Kashiwagi, Y.; Kawashima, H. Brain-derived neurotrophic factor and interleukin-6 levels in the serum and cerebrospinal fluid of children with viral infection-induced encephalopathy. Neurochem. Res. 2014, 39, 2143–2149. [Google Scholar] [CrossRef]
- Avdoshina, V.; Garzino-Demo, A.; Bachis, A.; Monaco, M.C. Human Immunodeficiency Virus-1 decreases the levels of neurotrophins in human lymphocytes. AIDS 2011, 25, 1126. [Google Scholar] [CrossRef] [Green Version]
- Caggiula, M.; Batocchi, A.; Frisullo, G.; Angelucci, F.; Patanella, A.K.; Sancricca, C.; Nociti, V.; Tonali, P.A.; Mirabella, M. Neurotrophic factors and clinical recovery in relapsing-remitting multiple sclerosis. Scand. J. Immunol. 2005, 62, 176–182. [Google Scholar] [CrossRef]
- Perrin, M.T.; Pawlak, R.; Dean, L.L.; Christis, A.; Friend, L. A cross-sectional study of fatty acids and brain-derived neurotrophic factor (BDNF) in human milk from lactating women following vegan, vegetarian, and omnivore diets. Eur. J. Nutr. 2019, 58, 2401–2410. [Google Scholar] [CrossRef]
- Dangat, K.; Kilari, A.; Mehendale, S.; Lalwani, S.; Joshi, S. Higher levels of brain derived neurotrophic factor but similar nerve growth factor in human milk in women with preeclampsia. Int. J. Dev. Neurosci. 2013, 31, 209–213. [Google Scholar] [CrossRef]
- Amir, L.H.; Forster, D.A.; Lumley, J.; McLachlan, H. A descriptive study of mastitis in Australian breastfeeding women: Incidence and determinants. BMC Public Health 2007, 7, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lumley, J.; Amir, L. Women’s experience of lactational mastitis: ‘I have never felt worse’. Aust. Fam. Phys. 2006, 35, 745. [Google Scholar]
- Abou-Dakn, M.; Fluhr, J.; Gensch, M.; Wöckel, A. Positive effect of HPA lanolin versus expressed breastmilk on painful and damaged nipples during lactation. Skin Pharmacol. Physiol. 2011, 24, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Groer, M.W.; Davis, M.; Hemphill, J. Postpartum stress: Current concepts and the possible protective role of breastfeeding. J. Obstet. Gynecol. Neonatal Nurs. 2002, 31, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Lau, C. Effects of stress on lactation. Pediatr. Clin. N. Am. 2001, 48, 221–234. [Google Scholar] [CrossRef]
- Kaufmann, R.; Foxman, B. Mastitis among lactating women: Occurrence and risk factors. Soc. Sci. Med. 1991, 33, 701–705. [Google Scholar] [CrossRef] [Green Version]
- Demers-Mathieu, V.; Huston, R.K.; Markell, A.M.; McCulley, E.A.; Martin, R.L.; Dallas, D.C. Antenatal influenza A-specific IgA, IgM, and IgG antibodies in mother’s own breast milk and donor breast milk, and gastric contents and stools from preterm infants. Nutrients 2019, 11, 1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demers-Mathieu, V.; Do, D.M.; Mathijssen, G.; Sela, D.A.; Seppo, A.; Järvinen, K.M.; Medo, E. Difference in levels of SARS-CoV-2 S1 and S2 subunits- and nucleocapsid protein-reactive SIgM/IgM, IgG and SIgA/IgA antibodies in human milk. J. Perinatol. 2020, 1–10. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Mathijssen, G.; Sela, D.A.; Järvinen, K.M.; Seppo, A.; Fels, S.; Medo, E. Human milk antibodies against S1 and S2 subunits from SARS-CoV-2, HCoV-OC43, and HCoV-229E in mothers with a confirmed COVID-19 PCR, viral symptoms, and unexposed mothers. Int. J. Mol. Sci. 2021, 22, 1749. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Mathijssen, G.; Medo, E. Previous viral symptoms and individual mothers affected the level et duration of human milk antibodies cross-reactive to S1 and S2 subunits from SARS-CoV-2, HCoV-229E, and HCoV-OC43. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Demers-Mathieu, V.; DaPra, C.; Mathijssen, G.; Medo, E. RBD SARS-CoV-2-specific antibodies in human milk from mothers with COVID-19 PCR or with symptoms suggestive of COVID-19. J. Pediatr. Gastroenterol. Nutr. 2021. accepted. [Google Scholar]
- Ismail, A.M.; Babers, G.M.; El Rehany, M.A. Brain-derived neurotrophic factor in sera of breastfed epileptic infants and in breastmilk of their mothers. Breastfeed. Med. 2015, 10, 277–282. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | COVID-19 PCR (n = 12) 2,3 | Viral Symptoms (n = 13) 3 | Unexposed (n = 22) |
|---|---|---|---|
| Postpartum time, months 1 | 5 ± 2 (4−10) | 6 ± 2 (4−9) | 6 ± 1 (5−8) |
| Infant gender, n | 6 males: 6 females | 5 males: 8 females | 3 males: 3 females |
| Maternal age, years 1 | 31 ± 4 (26−37) | 32 ± 5 (23−40) | 33 ± 4 (25−39) |
| Headaches, n | 4 | 3 | NA |
| Loss of smell and taste, n | 4 | 1 | NA |
| Fatigue, n | 3 | 2 | NA |
| Nasal congestion, n | 0 | 7 | NA |
| Date of infection | 03/29/20 to 10/13/20 | 3/08/20 to 6/25/20 | NA |
| Time from infection to collection, months 1 | 2 ± 1 (0.5−4) | 3.0 ± 0.7 (1.7−3.9) | NA |
| Demographics | Mastitis Group (n = 12) 2 | No Mastitis Group (n = 18) |
|---|---|---|
| Postpartum time, months 1 | 6 ± 2 (3−10) | 6 ± 2 (3−10) |
| Infant gender, n | 6 males: 6 females | 10 males: 8 females |
| Maternal age, years 1 | 30 ± 4 (24−35) | 33 ± 5 (23−40) |
| Stress, n | 12 | 0 |
| Fatigue, n | 12 | 0 |
| Date of mastitis(diagnosis/symptoms) | 07/12/19 to 08/17/20 | NA |
| Time from infection to collection, months 1 | 2 ± 1 (0.5−4) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demers-Mathieu, V.; Hines, D.J.; Hines, R.M.; Lavangnananda, S.; Fels, S.; Medo, E. Influence of Previous COVID-19 and Mastitis Infections on the Secretion of Brain-Derived Neurotrophic Factor and Nerve Growth Factor in Human Milk. Int. J. Mol. Sci. 2021, 22, 3846. https://doi.org/10.3390/ijms22083846
Demers-Mathieu V, Hines DJ, Hines RM, Lavangnananda S, Fels S, Medo E. Influence of Previous COVID-19 and Mastitis Infections on the Secretion of Brain-Derived Neurotrophic Factor and Nerve Growth Factor in Human Milk. International Journal of Molecular Sciences. 2021; 22(8):3846. https://doi.org/10.3390/ijms22083846
Chicago/Turabian StyleDemers-Mathieu, Veronique, Dustin J. Hines, Rochelle M. Hines, Sirima Lavangnananda, Shawn Fels, and Elena Medo. 2021. "Influence of Previous COVID-19 and Mastitis Infections on the Secretion of Brain-Derived Neurotrophic Factor and Nerve Growth Factor in Human Milk" International Journal of Molecular Sciences 22, no. 8: 3846. https://doi.org/10.3390/ijms22083846
APA StyleDemers-Mathieu, V., Hines, D. J., Hines, R. M., Lavangnananda, S., Fels, S., & Medo, E. (2021). Influence of Previous COVID-19 and Mastitis Infections on the Secretion of Brain-Derived Neurotrophic Factor and Nerve Growth Factor in Human Milk. International Journal of Molecular Sciences, 22(8), 3846. https://doi.org/10.3390/ijms22083846