
One-Sided Chronic Intervillositis of Unknown Etiology in Dizygotic Twins: A Description of 3 Cases

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Placental Characteristics
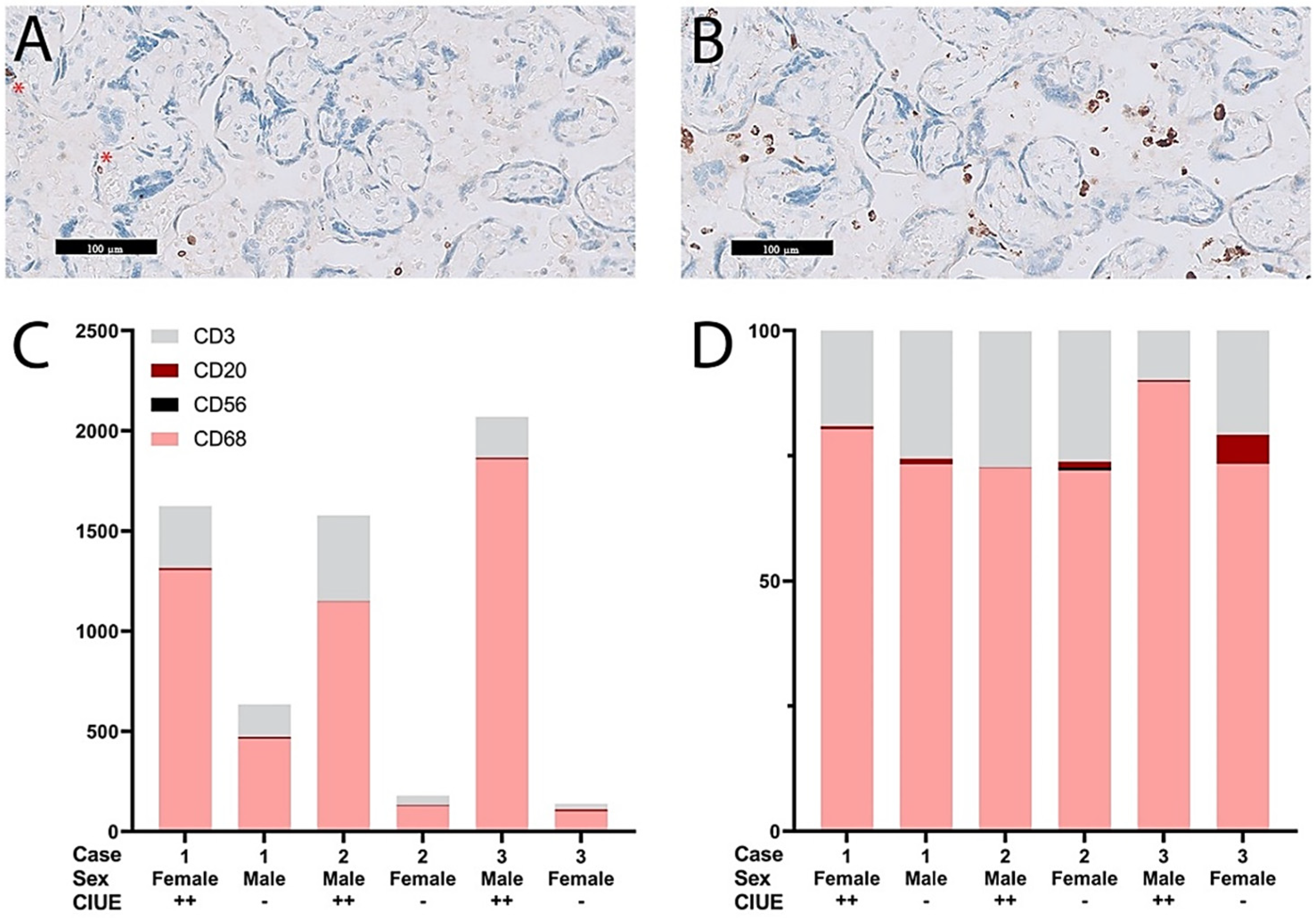
2.3. Quantification of the Intervillous Infiltrate
2.4. Intervillous Cells in Relation to Clinical Outcomes
3. Discussion
4. Materials and Methods
4.1. Case Selection
4.2. Clinical Definitions
4.3. Histology and Immunohistochemistry
4.4. Quantification of the Intervillous Infiltrate
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Labarrere, C.; Mullen, E. Fibrinoid and Trophoblastic Necrosis with Massive Chronic Intervillositis: An Extreme Variant of Villitis of Unknown Etiology. Am. J. Reprod. Immunol. 1987, 15, 85–91. [Google Scholar] [CrossRef]
- Mooney, E.E. Chronic Histiocytic Intervillositis. In Pathology of the Placenta; Khong, T., Mooney, E., Nikkels, P., Morgan, T., Gordijn, S., Eds.; Springer: Cham, Switzerland, 2019; pp. 207–211. [Google Scholar]
- Bos, M.; Nikkels, P.; Cohen, D.; Schoones, J.; Bloemenkamp, K.; Bruijn, J.; Baelde, H.; Van Der Hoorn, M.; Turner, R. Towards standardized criteria for diagnosing chronic intervillositis of unknown etiology: A systematic review. Placenta 2018, 61, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Parant, O.; Capdet, J.; Kessler, S.; Aziza, J.; Berrebi, A. Chronic intervillositis of unknown etiology (CIUE): Relation between placental lesions and perinatal outcome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 143, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Contro, E.; DeSouza, R.; Bhide, A. Chronic intervillositis of the placenta: A systematic review. Placenta 2010, 31, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Bendon, R.W.; Coventry, S.; Thompson, M.; Rudzinski, E.R.; Williams, E.M.; Oron, A.P. Significance of C4d Immunostaining in Placental Chronic Intervillositis. Pediatr. Dev. Pathol. 2015, 18, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Capuani, C.; Meggetto, F.; Duga, I.; Danjoux, M.; March, M.; Parant, O.; Brousset, P.; Aziza, J. Specific infiltration pattern of FOXP3+ regulatory T cells in chronic histiocytic intervillositis of unknown etiology. Placenta 2013, 34, 149–154. [Google Scholar] [CrossRef]
- Reus, A.D.; Van Besouw, N.M.; Molenaar, N.M.; Steegers, E.A.; Visser, W.; De Kuiper, R.P.; De Krijger, R.R.; Roelen, D.L.; Exalto, N. An Immunological Basis for Chronic Histiocytic Intervillositis in Recurrent Fetal Loss. Am. J. Reprod. Immunol. 2013, 70, 230–237. [Google Scholar] [CrossRef]
- Mekinian, A.; Costedoat-Chalumeau, N.; Masseau, A.; Botta, A.; Chudzinski, A.; Theulin, A.; Emmanuelli, V.; Hachulla, E.; De Carolis, S.; Revaux, A.; et al. Chronic histiocytic intervillositis: Outcome, associated diseases and treatment in a multicenter prospective study. Autoimmunity 2015, 48, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Hubinont, C.; Lewi, L.; Bernard, P.; Marbaix, E.; Debiève, F.; Jauniaux, E. Anomalies of the placenta and umbilical cord in twin gestations. Am. J. Obstet. Gynecol. 2015, 213, S91–S102. [Google Scholar] [CrossRef]
- Lewi, L.; Devlieger, R.; De Catte, L.; Deprest, J. Growth discordance. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 295–303. [Google Scholar] [CrossRef]
- Silver, R.M. Examining the link between placental pathology, growth restriction, and stillbirth. Best Pr. Res. Clin. Obstet. Gynaecol. 2018, 49, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.M.; Qureshi, F. Chronic villitis of unknown etiology in twin gestations. Pediatr. Pathol. 1994, 14, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Eberle, A.M.; Levesque, D.; Vintzileos, A.M.; Egan, J.F.; Tsapanos, V.; Salafia, C.M. Placental pathology in discordant twins. Am. J. Obstet. Gynecol. 1993, 169, 931–935. [Google Scholar] [CrossRef]
- Yusuf, K.; Kliman, H.J. The fetus, not the mother, elicits maternal immunologic rejection: Lessons from discordant dizygotic twin placentas. J. Perinat. Med. 2008, 36, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Faye-Petersen, O.; Sauder, A.; Estrella, Y.; Heller, D.S. Dichorionic Twins Discordant for Massive Perivillous Fibrinoid Deposition: Report of a Case and Review of the Literature. Int. J. Surg. Pathol. 2017, 26, 41–46. [Google Scholar] [CrossRef]
- Gupta, N.; Sebire, N.; Miskry, T.; Rees, H. Massive perivillous fibrin deposition associated with discordant fetal growth in a dichorionic twin pregnancy. J. Obstet. Gynaecol. 2004, 24, 579–580. [Google Scholar] [CrossRef]
- Redline, R.W.; Jiang, J.-G.; Shah, D. Discordancy for maternal floor infarction in dizygotic twin placentas. Hum. Pathol. 2003, 34, 822–824. [Google Scholar] [CrossRef]
- Bane, A.L.; E Gillan, J. Massive perivillous fibrinoid causing recurrent placental failure. BJOG Int. J. Obstet. Gynaecol. 2003, 110, 292–295. [Google Scholar] [CrossRef]
- Tchakarov, A.; Coffey, A.; Tatevian, N. Neonatal Alloimmune Thrombocytopenia Associated with Massive Chronic Intervillositis: A Case Report and Review of the Literature. Pediatr. Dev. Pathol. 2013, 16, 32–34. [Google Scholar] [CrossRef]
- Dubruc, E.; Lebreton, F.; Giannoli, C.; Rabilloud, M.; Huissoud, C.; Devouassoux-Shisheboran, M.; Allias, F. Placental histological lesions in fetal and neonatal alloimmune thrombocytopenia: A retrospective cohort study of 21 cases. Placenta 2016, 48, 104–109. [Google Scholar] [CrossRef]
- Boyd, T.K.; Redline, R.W. Chronic histiocytic intervillositis: A placental lesion associated with recurrent reproductive loss. Hum. Pathol. 2000, 31, 1389–1396. [Google Scholar] [CrossRef]
- Tsuda, S.; Zhang, X.; Hamana, H.; Shima, T.; Ushijima, A.; Tsuda, K.; Muraguchi, A.; Kishi, H.; Saito, S. Clonally Expanded Decidual Effector Regulatory T Cells Increase in Late Gestation of Normal Pregnancy, but Not in Preeclampsia, in Humans. Front. Immunol. 2018, 9, 1934. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; Tsuda, S.; Kobayashi, E.; Hamana, H.; Tsuda, K.; Shima, T.; Nakashima, A.; Ushijima, A.; Kishi, H.; Saito, S. Analysis of TCR Repertoire and PD-1 Expression in Decidual and Peripheral CD8+ T Cells Reveals Distinct Immune Mechanisms in Miscarriage and Preeclampsia. Front. Immunol. 2020, 11, 1082. [Google Scholar] [CrossRef]
- Man, J.; Hutchinson, J.C.; Heazell, A.E.; Ashworth, M.; Jeffrey, I.; Sebire, N.J. Stillbirth and intrauterine fetal death: Role of routine histopathological placental findings to determine cause of death. Ultrasound Obstet. Gynecol. 2016, 48, 579–584. [Google Scholar] [CrossRef] [Green Version]
- Bos, M.; Harris-Mostert, E.; van der Meeren, L.; Baelde, J.; Williams, D.; Nikkels, P.; Bloemenkamp, K.; van der Hoorn, M. Clinical outcomes in chronic intervillositis of unknown etiology. Placenta 2020, 91, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.M.; Boyd, T.K.; Brundler, M.-A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [Green Version]
- Benirschke, K.; Burton, G.; Baergen, R. Pathology of the Human Placenta; Springer: Berlin/Heidelberg, Germany; London, UK, 2012. [Google Scholar]


{kind=link}
| Case | 1 | 2 | 3 | |||
|---|---|---|---|---|---|---|
| Maternal characteristics | ||||||
| Gravidity | 3 | 1 | 1 | |||
| Parity | 2 | 0 | 0 | |||
| Outcome previous pregnancy | FGR without complications | NA | NA | |||
| Previous miscarriages | 0 | NA | NA | |||
| Obstetric characteristics | ||||||
| Artificial reproductive techniques | Ovulation-induction | |||||
| Gestational age (weeks) | 37 | 40 | 35 | |||
| Mode of delivery | Spontaneous | Primary caesarean section | Induction | |||
| Indication for delivery | Twin 1 in breech presentation | Severe fetal growth restriction | ||||
| Fetal characteristics | ||||||
| Sex | Female | Male | Male | Female | Male | Female |
| Birthweight percentile | p < 3 | p10–50 | p10–50 | p50–90 | p < 3 | p50–90 |
| Birthweight discordancy | 1280 g, 47% | 290 g, 9% | 1370 g, 50% | |||
| Apgar score at 5 min | 8 | 10 | 10 | 10 | 9 | 9 |
| Neonatal admission | NMCU | NICU | NMCU | |||
| Placenta characteristics | ||||||
| Fetal Membranes | Dichorionic Diamniotic | Dichorionic Diamniotic | Dichorionic Diamniotic | |||
| Placenta weight percentile | 1 p10–25 | p75–90 | p90 | p10–25 | p75–90 | |
| Chronic intervillositis of unknown etiology | Moderate | Absent | Moderate | Absent | Moderate | Absent |
| Villitis of unknown etiology | Moderate | Absent | Severe | Moderate | Absent | Absent |
| Peri-villous fibrin deposits | Absent | Absent | Moderate | Absent | Absent | Absent |
| Fetal thrombosis | Absent | Absent | Present, focal | Absent | Absent | Absent |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Meeren, L.E.; Krop, J.; Dijkstra, K.L.; Bloemenkamp, K.W.M.; Cornish, E.F.; Nikkels, P.G.J.; van der Hoorn, M.-L.P.; Bos, M. One-Sided Chronic Intervillositis of Unknown Etiology in Dizygotic Twins: A Description of 3 Cases. Int. J. Mol. Sci. 2021, 22, 4786. https://doi.org/10.3390/ijms22094786
van der Meeren LE, Krop J, Dijkstra KL, Bloemenkamp KWM, Cornish EF, Nikkels PGJ, van der Hoorn M-LP, Bos M. One-Sided Chronic Intervillositis of Unknown Etiology in Dizygotic Twins: A Description of 3 Cases. International Journal of Molecular Sciences. 2021; 22(9):4786. https://doi.org/10.3390/ijms22094786
Chicago/Turabian Stylevan der Meeren, Lotte E., Juliette Krop, Kyra L. Dijkstra, Kitty W. M. Bloemenkamp, Emily F. Cornish, Peter G. J. Nikkels, Marie-Louise P. van der Hoorn, and Manon Bos. 2021. "One-Sided Chronic Intervillositis of Unknown Etiology in Dizygotic Twins: A Description of 3 Cases" International Journal of Molecular Sciences 22, no. 9: 4786. https://doi.org/10.3390/ijms22094786
APA Stylevan der Meeren, L. E., Krop, J., Dijkstra, K. L., Bloemenkamp, K. W. M., Cornish, E. F., Nikkels, P. G. J., van der Hoorn, M. -L. P., & Bos, M. (2021). One-Sided Chronic Intervillositis of Unknown Etiology in Dizygotic Twins: A Description of 3 Cases. International Journal of Molecular Sciences, 22(9), 4786. https://doi.org/10.3390/ijms22094786