
Ang–Tie Angiogenic Pathway Is Distinctively Expressed in Benign and Malignant Adrenocortical Tumors

 , and
, and
Abstract
:1. Introduction
2. Results
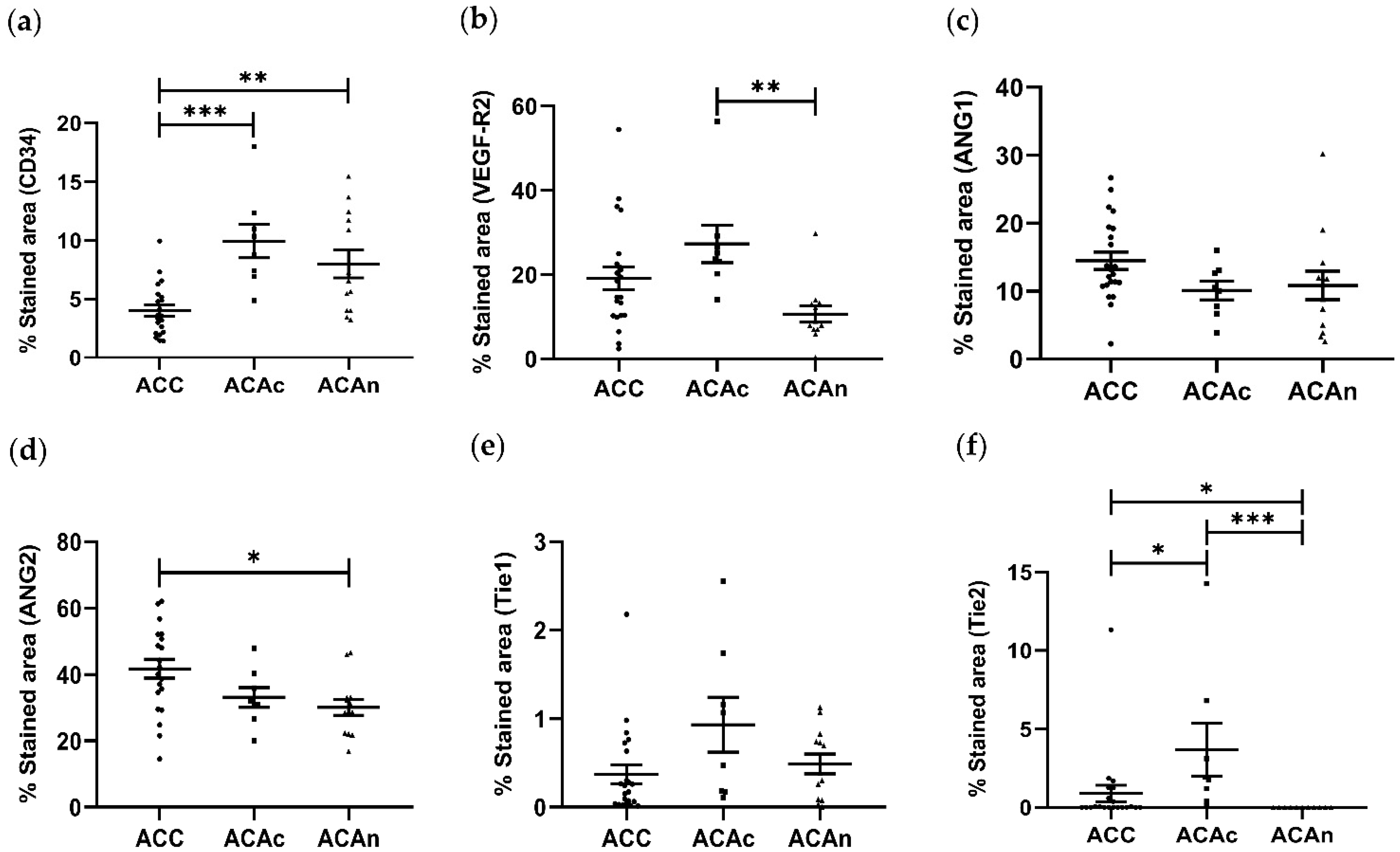
2.1. Angiogenic Proteins Expression in ACT
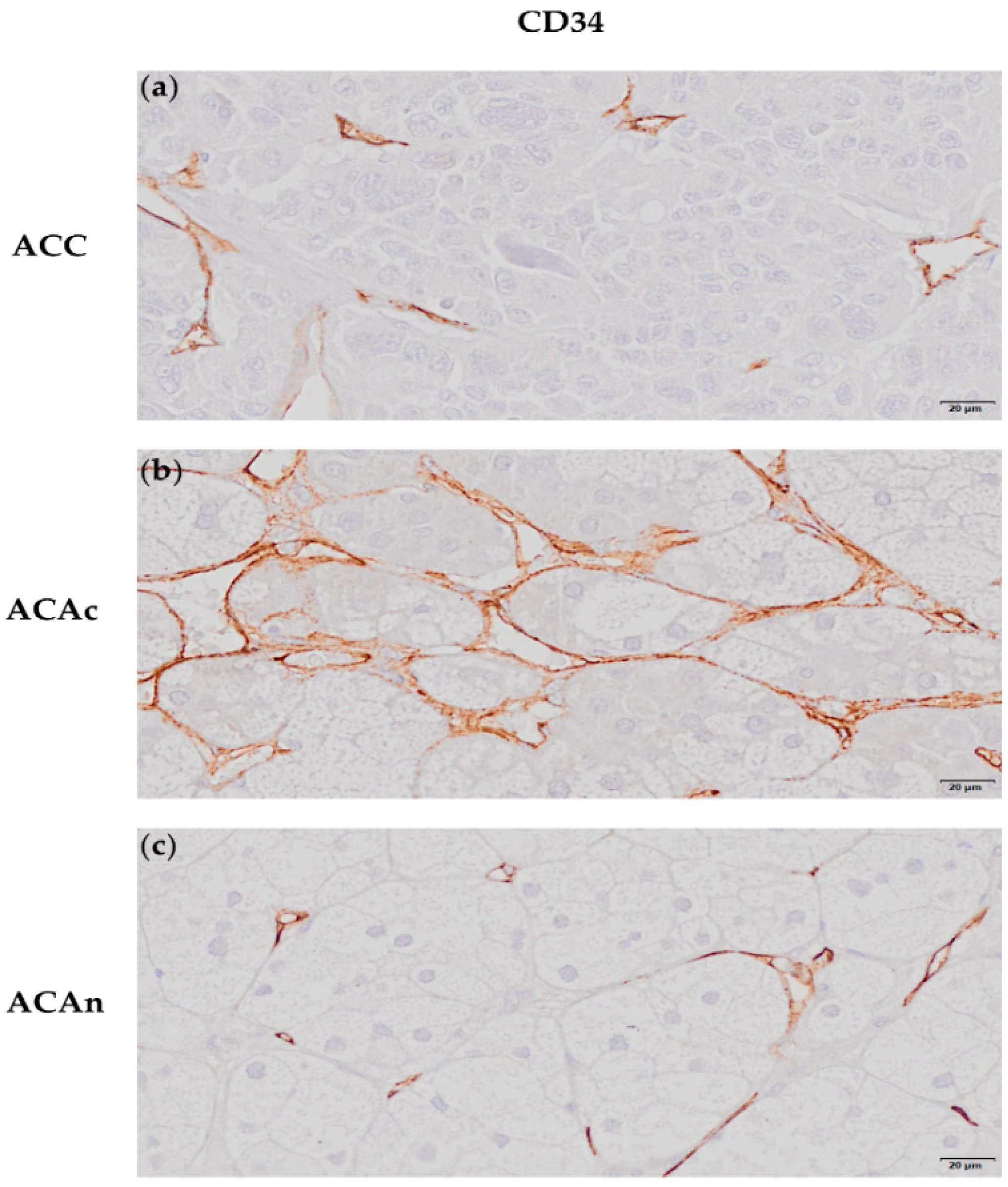
2.1.1. CD34 Expression
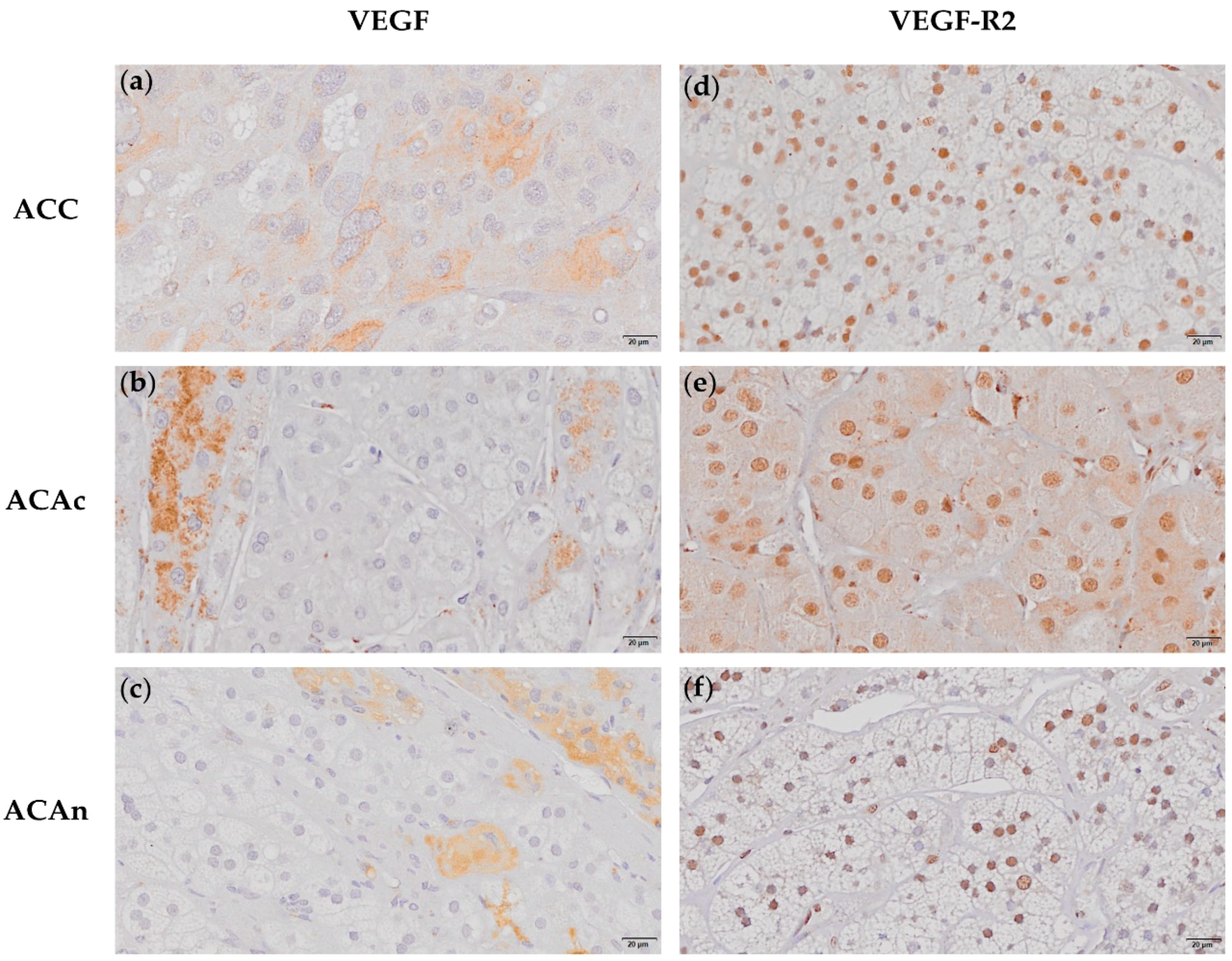
2.1.2. VEGF and VEGF-R2 Expression
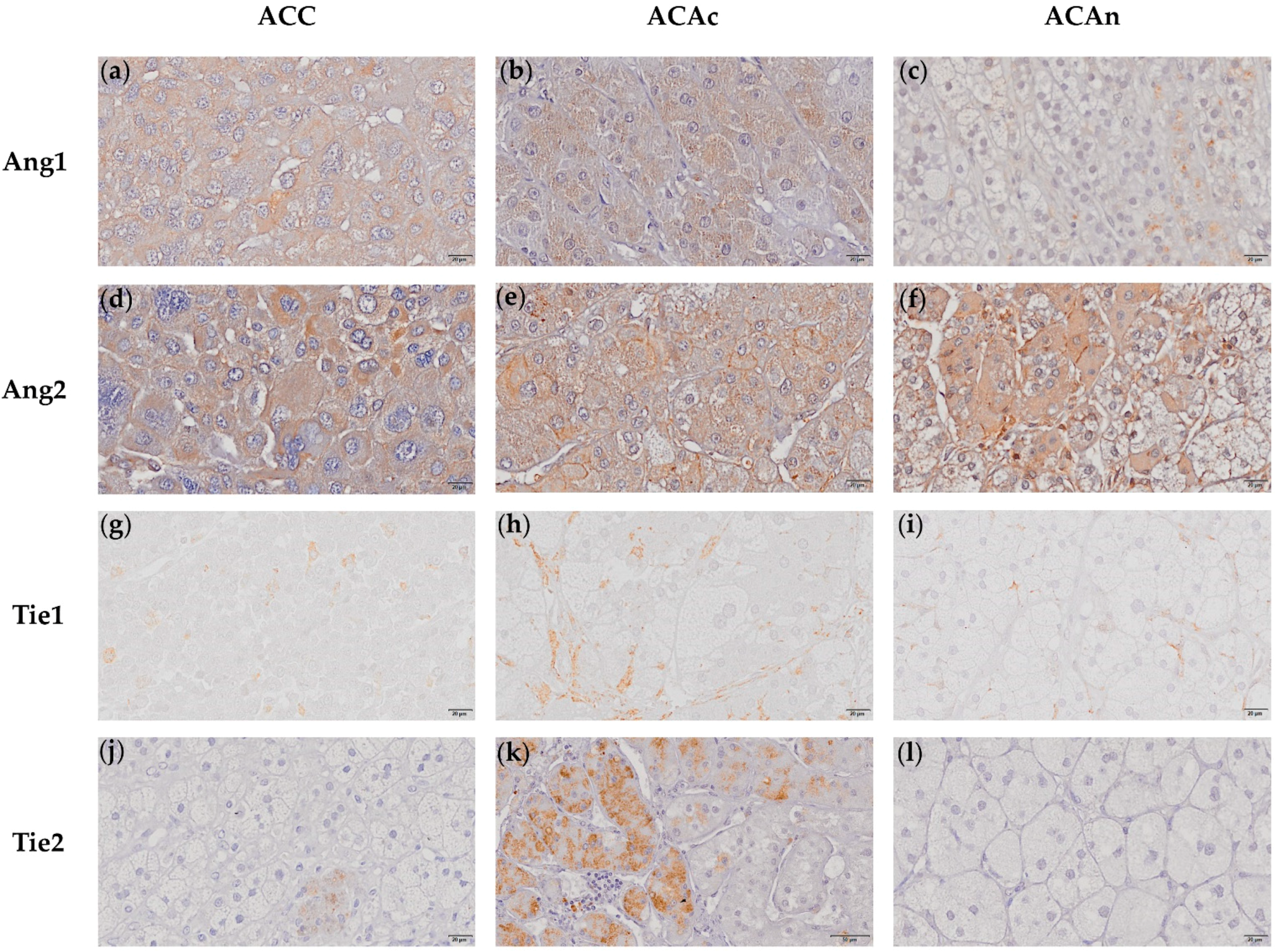
2.1.3. Ang1 and Ang2 Expression
2.1.4. Tie1 and Tie 2 Expression
2.2. Correlation between Angiogenic Biomarkers and Patients and Tumor Characteristic
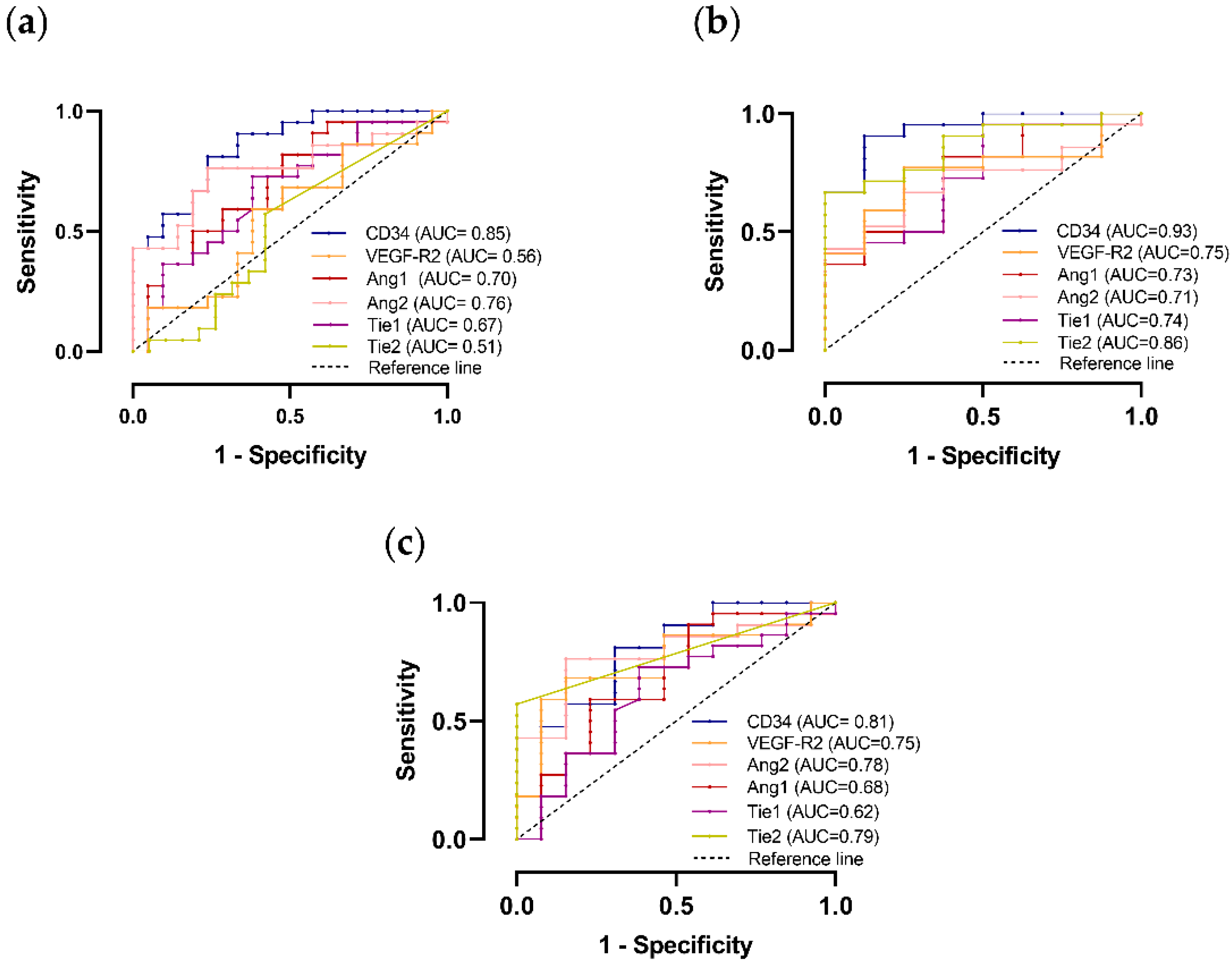
2.3. Angiogenic Markers Accuracy for Differential Diagnosis
2.4. Angiogenic Markers Accuracy to Predict ACC Prognosis
3. Discussion
4. Materials and Methods
4.1. Case Selection
4.2. Immunochemistry and Data Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lehmann, T.; Wrzesinski, T. The molecular basis of adrenocortical cancer. Cancer Genet. 2012, 205, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Pignatelli, D. Adrenal Cortex Tumors and Hyperplasias. In Contemporary Aspects of Endocrinology; IntechOpen: London, UK, 2011. [Google Scholar]
- Lau, S.K.; Weiss, L.M. The Weiss system for evaluating adrenocortical neoplasms: 25 years later. Hum. Pathol. 2009, 40, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Assié, G.; Letouzé, E.; Fassnacht, M.; Jouinot, A.; Luscap, W.; Barreau, O.; Omeiri, H.; Rodriguez, S.; Perlemoine, K.; René-Corail, F.; et al. Integrated genomic characterization of adrenocortical carcinoma. Nat. Genet. 2014, 46, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Jouinot, A.; Bertherat, J. MANAGEMENT OF ENDOCRINE DISEASE: Adrenocortical carcinoma: Differentiating the good from the poor prognosis tumors. Eur. J. Endocrinol. 2018, 178, R215–R230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lugano, R.; Ramachandran, M.; Dimberg, A. Tumor angiogenesis: Causes, consequences, challenges and opportunities. Cell. Mol. Life Sci. 2020, 77, 1745–1770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saharinen, P.; Eklund, L.; Pulkki, K.; Bono, P.; Alitalo, K. VEGF and angiopoietin signaling in tumor angiogenesis and metastasis. Trends Mol. Med. 2011, 17, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.S.; Oliveira, S.; Monteiro, M.P.; Pignatelli, D. Angiogenesis in the Normal Adrenal Fetal Cortex and Adrenocortical Tumors. Cancers 2021, 13, 1030. [Google Scholar] [CrossRef] [PubMed]
- Bernini, G.P.; Moretti, A.; Bonadio, A.G.; Menicagli, M.; Viacava, P.; Naccarato, A.G.; Iacconi, P.; Miccoli, P.; Salvetti, A. Angiogenesis in Human Normal and Pathologic Adrenal Cortex. J. Clin. Endocrinol. Metab. 2002, 87, 4961–4965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz-Cano, S.J.; de Miguel, M.; Blanes, A.; Galera, H.; Wolfe, H.J. Contribution of the microvessel network to the clonal and kinetic profiles of adrenal cortical proliferative lesions. Hum. Pathol. 2001, 32, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.S.; Costa, M.M.; Guerreiro, S.G.; Monteiro, M.P.; Pignatelli, D. Angiogenesis and Lymphangiogenesis in the Adrenocortical Tumors. Pathol. Oncol. Res. 2018, 24, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Sasano, H.; Ohashi, Y.; Suzuki, T.; Nagura, H. Vascularity in human adrenal cortex. Mod. Pathol. Off. J. United States Can. Acad. Pathol. Inc 1998, 11, 329–333. [Google Scholar]
- Xu, Y.Z.; Zhu, Y.; Shen, Z.J.; Sheng, J.Y.; He, H.C.; Ma, G.; Qi, Y.C.; Zhao, J.P.; Wu, Y.X.; Rui, W.B.; et al. Significance of heparanase-1 and vascular endothelial growth factor in adrenocortical carcinoma angiogenesis: Potential for therapy. Endocrine 2011, 40, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Xu, Y.; Chen, D.; Zhang, C.; Rui, W.; Zhao, J.; Zhu, Q.; Wu, Y.; Shen, Z.; Wang, W.; et al. Expression of STAT3 and IGF2 in adrenocortical carcinoma and its relationship with angiogenesis. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2014, 16, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, R.; Fan, F.; Wang, R.; Ye, X.; Xia, L.; Boulbes, D.; Ellis, L.M. Intracrine VEGF signalling mediates colorectal cancer cell migration and invasion. Br. J. Cancer 2017, 117, 848–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.H.; Seng, S.; Sekine, M.; Hinton, C.; Fu, Y.; Avraham, H.K.; Avraham, S. Vascular endothelial growth factor mediates intracrine survival in human breast carcinoma cells through internally expressed VEGFR1/FLT1. PLoS Med. 2007, 4, e186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feige, J.J. Angiogenesis in adrenocortical physiology and tumor development. Ann. D’endocrinologie 2009, 70, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Domingues, I.; Rino, J.; Demmers, J.A.; de Lanerolle, P.; Santos, S.C. VEGFR2 translocates to the nucleus to regulate its own transcription. PLoS ONE 2011, 6, e25668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukumura, D.; Kloepper, J.; Amoozgar, Z.; Duda, D.G.; Jain, R.K. Enhancing cancer immunotherapy using antiangiogenics: Opportunities and challenges. Nat. Rev. Clin. Oncol. 2018, 15, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Tsiamis, A.C.; Morris, P.N.; Marron, M.B.; Brindle, N.P.J. Vascular Endothelial Growth Factor Modulates the TIE-2:TIE-1 Receptor Complex. Microvasc. Res. 2002, 63, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Eklund, L.; Saharinen, P. Angiopoietin signaling in the vasculature. Exp. Cell Res. 2013, 319, 1271–1280. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | n | Expression Pattern | ||
|---|---|---|---|---|
| Nucleus + Cytoplasm | Cytoplasm | p | ||
| ACC | 21 | 8 (38%) | 13 (62%) | 0.09 |
| ACAc | 8 | 0 (0%) | 8 (100%) | |
| ACAn | 13 | 5 (38%) | 8 (62%) | |
| CD34 | VEGF-R2 | Ang1 | Ang2 | Tie1 | Tie2 | ||
|---|---|---|---|---|---|---|---|
| ENSAT score | 1–2 | 2.589 ± 0.538 | 9.676 ± 3.342 | 15.477 ± 2.278 | 44.699 ± 5.810 | 0.106 ± 0.046 | 0.284 ± 0.282 |
| 3–4 | 4.728 ± 0.944 | 15.771 ± 1.767 | 14.824 ± 1.473 | 45.449 ± 5.727 | 0.206 ± 0.111 | 0.239 ± 0.178 | |
| p | 0.051 | 0.138 | 0.945 | >0.999 | 0.731 | >0.999 | |
| Metastasis | Yes | 3.473 ± 0.533 | 17.458 ± 1.670 | 14.880 ± 2.207 | 53.200 ± 2.804 | 0.116 ± 0.058 | 0.094 ± 0.094 |
| No | 3.859 ± 0.891 | 10.958 ± 2.460 | 15.235 ± 1.889 | 41.105 ± 5.294 | 0.179 ± 0.089 | 0.333 ± 0.219 | |
| p | 0.940 | 0.106 | 0.940 | 0.283 | 0.825 | 0.471 | |
| Capsular Invasion | Yes | 3.957 ± 0.710 | 13.950 ± 1.664 | 14.030 ± 1.204 | 42.795 ± 3.700 | 0.233 ± 0.095 | 0.193 ± 0.111 |
| No | 2.478 ± 0.548 | 9.840 ± 4.857 | 14.585 ± 2.55 | 45.314 ± 16.004 | 0.155 ± 0.068 | 0.565 ± 0.564 | |
| p | 0.291 | 0.365 | 0.945 | >0.999 | 0.734 | 0.739 | |
| Venous Invasion | Yes | 3.914 ± 0.628 | 19.527 ± 2.987 | 14.099 ± 1.390 | 41.141 ± 5.186 | 0.431 ± 0.133 | 0.245 ± 0.162 |
| No | 3.474 ± 0.889 | 12.871 ± 2.633 | 14.709 ± 1.704 | 45.182 ± 3.686 | 0.099 ± 0.031 | 0.235 ± 0.187 | |
| p | 0.351 | 0.166 | 0.793 | 0.536 | 0.021 | 0.872 | |
| Sinusoidal Invasion | Yes | 4.158 ± 0.761 | 16.006 ± 2.871 | 14.245 ± 1.585 | 43.456 ± 3.733 | 0.215 ± 0.084 | 0.335 ± 0.165 |
| No | 2.808 ± 0.289 | 12.350 ±2.742 | 14.590 ± 1.639 | 43.456 ± 8.110 | 0.193 ± 0.039 | 0.014 ± 0.011 | |
| p | 0.411 | 0.446 | 0.446 | >0.999 | 0.379 | 0.850 | |
| Angiogenic Marker | HR | 95% CI | p |
|---|---|---|---|
| CD34 | 0.69 | 0.36–1.33 | 0.27 |
| VEGF | 0.60 | 0.10–3.46 | 0.59 |
| VEGF-R2 | 1.12 | 0.97–1.30 | 0.13 |
| Ang1 | 1.07 | 0.89–1.28 | 0.48 |
| Ang2 | 1.03 | 0.95–1.12 | 0.49 |
| Tie1 | 25.93 | 0.62–1087.29 | 0.09 |
| Tie2 | 1.89 | 0.42–8.45 | 0.40 |
| ACC | ACA | ||
|---|---|---|---|
| N/F | Cushing | ||
| N | 22 | 13 | 8 |
| Age at surgery | 54 ± 11 | 34 ± 8 | 59 ± 12 |
| Sex F:M | 15:7 | 9:3 | 7:1 |
| Tumor size (cm) (range) | 10 ± 5.6 (2.7–20) | 4.1 ± 2.2 (1.8–9.5) | 3.5 ± 0.98 (2.4–5) |
| Weiss score (range) | 3–8 | 0–1 | 0 |
| ENSAT score | NA | NA | |
| 1 | 15% | ||
| 2 | 31% | ||
| 3 | 31% | ||
| 4 | 23% | ||
| Functionality | |||
| N/F | 9% | 100% | |
| Cortisol | 9% | 0 | 100% |
| Aldosterone | 5% | 0 | 0 |
| Androgens | 9% | 0 | 0 |
| Cortisol + Androgens | 5% | 0 | 0 |
| Unknown | 63% | 0 | 0 |
| Antibody | CD34 (ab81289) | VEGF (ab52917) | VEGF-R2 (ab2349) | Ang1 (ab8451) | Ang2 (ab153934) | Tie1 (ab201986) | Tie2 (ab24859) |
|---|---|---|---|---|---|---|---|
| Positive control | kidney | kidney | breast | lung | placenta | kidney | lung |
| Antigen retrieval | Microwave treatment in 0.01 M citrate buffer at pH 6.0 with 0.05% Tween 20 during 15 min | Pressure-cooking boiling for 3 min in 0.01 M citrate buffer at pH 6.0 | Microwave treatment in 0.01 M citrate buffer at pH 6.0 during 15 min | Pressure cooking boiling for 3 min in 0.01 M citrate buffer at pH 6.0 with 0.05% Tween 20 | Pressure cooking boiling for 3 min in 0.01 M citrate buffer at pH 6.0 with 0.25% Triton-X | ||
| Washing solutions | PBS 0.05% Tween 20 | PBS | PBS | PBS | PBS | PBS 0.05% Tween 20 | PBS 0.05% Triton-X |
| Primary antibody dilution | 1:2000 | 1:100 | 1:100 | 1:400 | 1:400 | 1:100 | 1:100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, S.; Pereira, S.S.; Costa, M.M.; Monteiro, M.P.; Pignatelli, D. Ang–Tie Angiogenic Pathway Is Distinctively Expressed in Benign and Malignant Adrenocortical Tumors. Int. J. Mol. Sci. 2022, 23, 5579. https://doi.org/10.3390/ijms23105579
Oliveira S, Pereira SS, Costa MM, Monteiro MP, Pignatelli D. Ang–Tie Angiogenic Pathway Is Distinctively Expressed in Benign and Malignant Adrenocortical Tumors. International Journal of Molecular Sciences. 2022; 23(10):5579. https://doi.org/10.3390/ijms23105579
Chicago/Turabian StyleOliveira, Sofia, Sofia S. Pereira, Madalena M. Costa, Mariana P. Monteiro, and Duarte Pignatelli. 2022. "Ang–Tie Angiogenic Pathway Is Distinctively Expressed in Benign and Malignant Adrenocortical Tumors" International Journal of Molecular Sciences 23, no. 10: 5579. https://doi.org/10.3390/ijms23105579
APA StyleOliveira, S., Pereira, S. S., Costa, M. M., Monteiro, M. P., & Pignatelli, D. (2022). Ang–Tie Angiogenic Pathway Is Distinctively Expressed in Benign and Malignant Adrenocortical Tumors. International Journal of Molecular Sciences, 23(10), 5579. https://doi.org/10.3390/ijms23105579