
Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
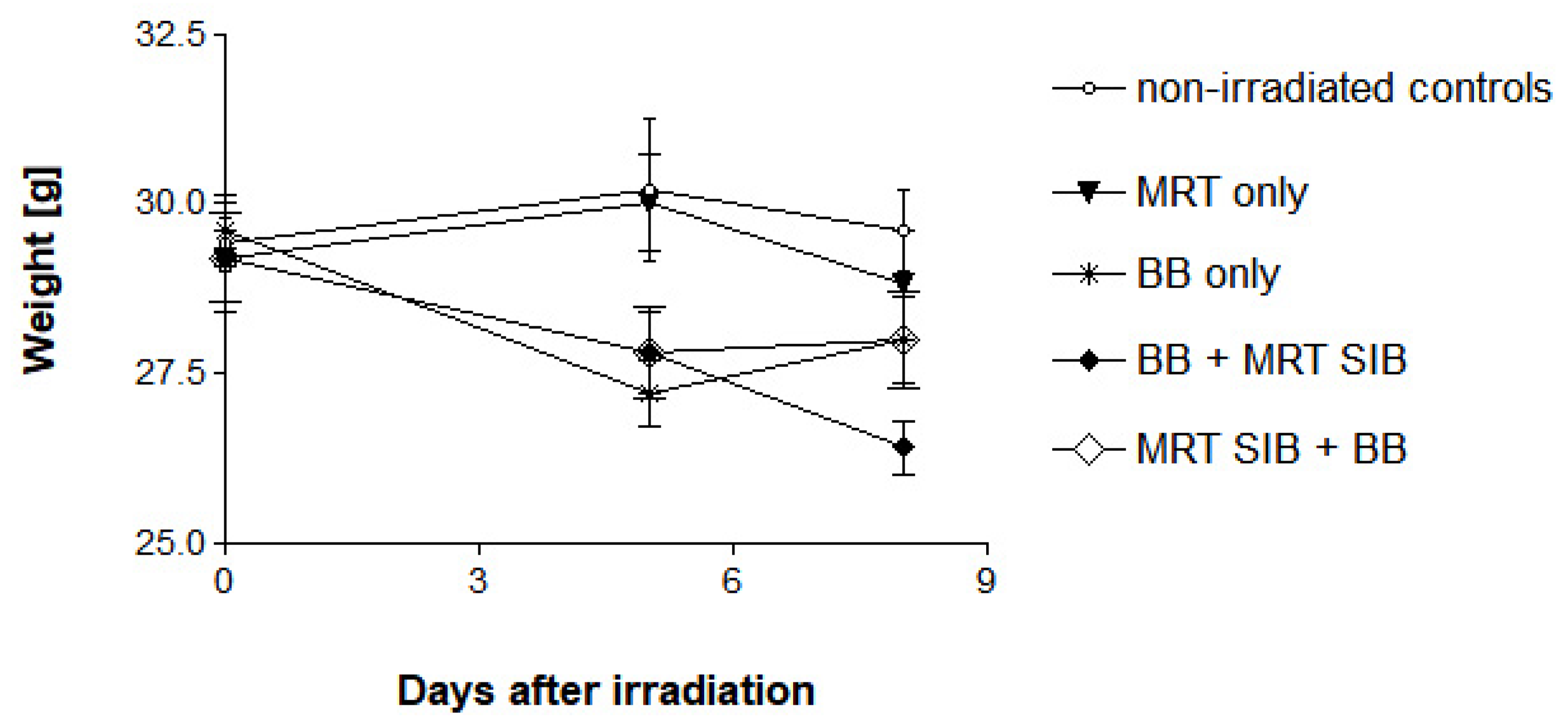
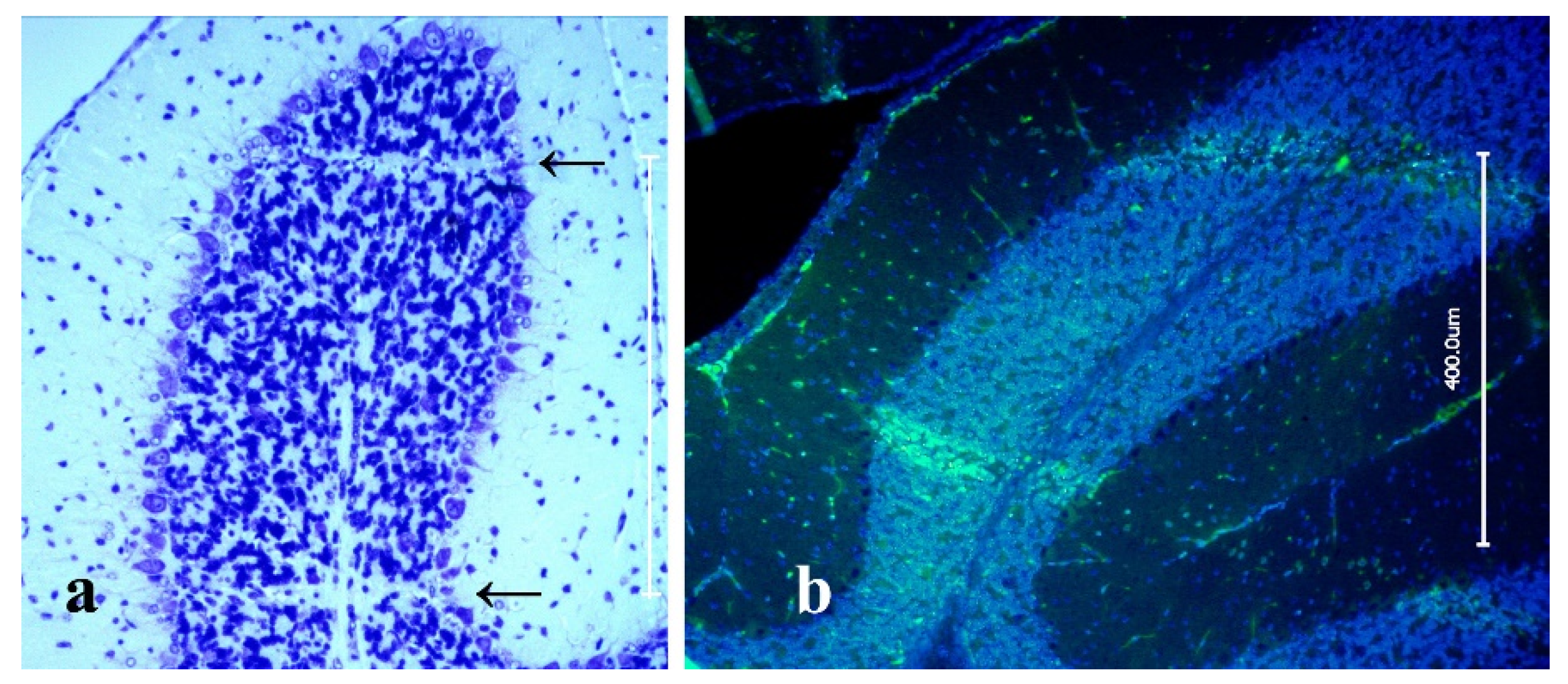
2.1. Survival, Behaviour and Normal Tissue Function
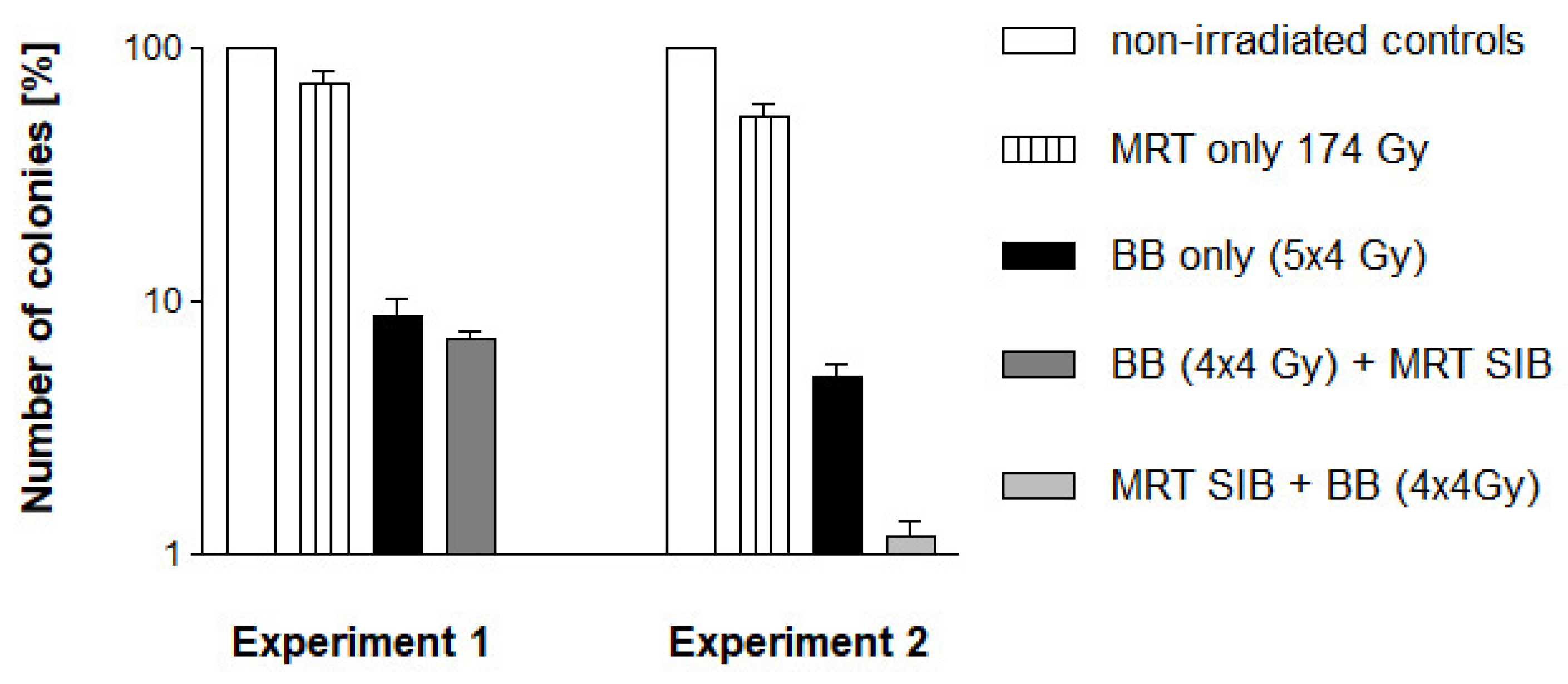
2.2. In-Vitro Study with Clonogenic Assays Using F98 Glioma Cells
3. Discussion
4. Materials and Methods
4.1. Animal Model
4.2. Irradiation Sources
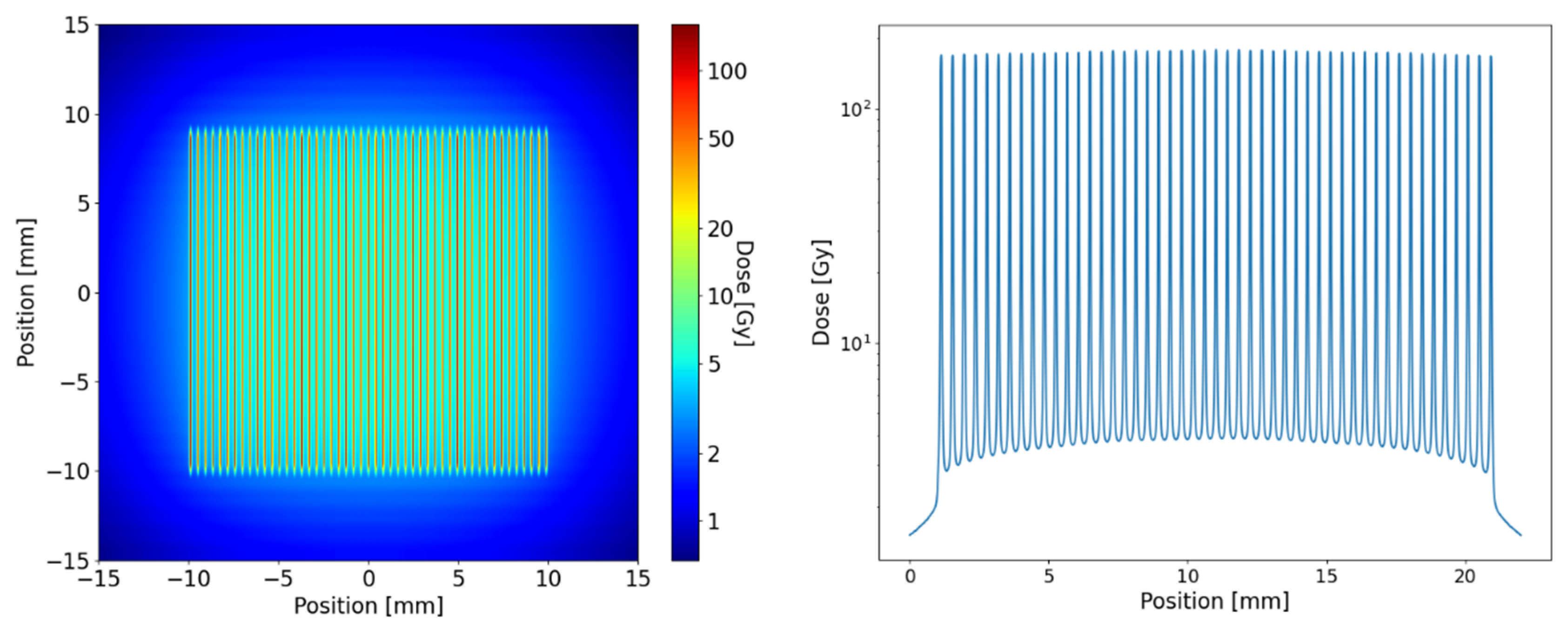
4.3. Dose Calculation and Modelling
4.4. In Vivo Model
4.5. In Vitro Model
4.6. Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Syed, M.; Liermann, J.; Verma, V.; Bernhardt, D.; Bougatf, N.; Paul, A.; Rieken, S.; Debus, J.; Adeberg, S. Survival andrecurrence patterns of multifocal glioblastoma after radiation therapy. Cancer Manag. Res. 2018, 10, 4229–4235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giese, A.; Bjerkvig, R.; Berens, M.E.; Westphal, M. Cost of migration: Invasion of malignant gliomas and implications for treatment. J. Clin. Oncol. 2003, 21, 1624–1636. [Google Scholar] [CrossRef]
- Laws, E.R., Jr.; Goldberg, W.J.; Bernstein, J.J. Migration of human malignant astrocytoma cells in the mammalian brain: Scherer revisited. Int. J. Dev. Neurosci. 1993, 11, 691–697. [Google Scholar] [CrossRef]
- Scherer, H.J. Structural development in gliomas. Am. J. Cancer 1938, 34, 333–351. [Google Scholar]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Adeberg, S.; König, L.; Bostel, T. Glioblastoma recurrence patterns after radiation therapy with regard to the subventricular zone. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R. Stupp trial (5y) 5yOS 10v2% MS 12 v 14.6mo. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Patil, N.; Somasundaram, E.; Waite, K.A.; Lathia, J.D.; Machtay, M.; Gilbert, M.R.; Connor, J.R.; Rubin, J.B.; Berens, M.E.; Buerki, R.A.; et al. Independently validated sex-specific nomograms for predicting survival in patients with newly diagnosed glioblastoma: NRG Oncology RTOG 0525 and 0825. J. Neurooncol. 2021, 155, 363–372. [Google Scholar] [CrossRef] [PubMed]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.P.; Schlegel, U.; Sabel, M.; Hau, P.; Kortmann, R.D.; Krex, D.; Grauer, O.; et al. Neurooncology Working Group of the German Cancer Society. Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA-09): A randomised, open-label, phase 3 trial. Lancet 2019, 393, 678–688. [Google Scholar] [CrossRef]
- Brandes, A.A.; Tosoni, A.; Franceschi, E.; Sotti, G.; Frezza, G.; Amistà, G.; Morandi, L.; Spagnoli, F.; Ermani, M. Recurrence pattern after temozolomide concomitant with and adjuvant to radiotherapy in newly diagnosed patients with glioblastoma: Correlation with MGMT promoter methylation status. J. Clin. Oncol. 2009, 27, 1275–1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giese, A.; Westphal, M. Treatment of malignant glioma: A problem beyond the margins of resection. J. Cancer Res. Clin. Oncol. Suppl. 2001, 127, 217–225. [Google Scholar] [CrossRef]
- Tsai, P.F.; Yang, C.C.; Chuang, C.C.; Huang, T.Y.; Wu, Y.M.; Pai, P.C.; Tseng, C.K.; Wu, T.H.; Lin, S.Y. Hippocampal dosimetry correlates with the change in neurocognitive function after hippocampal sparing during whole brain radiotherapy: A prospective study. Radiat. Oncol. 2015, 10, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, A.; Bae, K.; Gore, E.M.; Movsas, B.; Wing, S.J.; Meyers, C.A.; Bonner, J.A.; Schild SEGaspar, L.E.; Bogart, J.A.; Werner-Wasik, M.; et al. Phase III trial of prophylactic cranial irradiation compared with observation in patients with locally advanced non-small-cell lung cancer: Neurocognitive and quality-of-life analysis. J. Clin. Oncol. 2011, 29, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Eling, L.; Bouchet, A.; Ocadiz, A.; Adam, J.F.; Kershmiri, S.; Elleaume, H.; Krisch, M.; Verry, C.; Laissue, J.A.; Balosso, J.; et al. Unexpected Benefits of Multiport Synchrotron Microbeam Radiation Therapy for Brain Tumors. Cancers 2021, 13, 936. [Google Scholar] [CrossRef] [PubMed]
- Schültke, E.; Bräuer-Krisch, E.; Blattmann, H.; Requardt, H.; Laissue, J.A.; Hildebrandt, G. Survival of rats bearing advanced intracerebral F 98 tumors after glutathione depletion and microbeam radiation therapy: Conclusions from a pilot project. Radiat. Oncol. 2018, 13, 89. [Google Scholar] [CrossRef] [Green Version]
- Laissue, J.A.; Geiser, G.; Spanne, P.O.; Dilmanian, A.; Gebbers, J.A.; Geiser, M.; Wu, X.Y.; Makar, M.S.; Micca, P.L.; Nawrocky, M.M.; et al. Neuropathology of ablation of rat gliosarcomas and contiguous brain tissues using a microplanar beam of synchrotron-wiggler-generated X rays. Int. J. Cancer 1998, 78, 654–660. [Google Scholar] [CrossRef]
- Bouchet, A.; Lemasson, B.; Le Duc, G.; Maisin, C.; Bräuer-Krisch, E.; Siegbahn, E.A.; Renaud, L.; Khalil, E.; Rémy, C.; Poillot, C.; et al. Preferential effect of synchrotron microbeam radiation therapy on intracerebral 9L gliosarcoma vascular networks. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1503–1512. [Google Scholar] [CrossRef] [Green Version]
- Laissue, J.A.; Blattmann, H.; Wagner, H.P.; Grotzer, M.A.; Slatkin, D.N. Prospects for microbeam radiation therapy of brain tumours in children to reduce neurological sequelae. Dev. Med. Child Neurol. 2007, 49, 577–581. [Google Scholar] [CrossRef]
- Schültke, E.; Juurlink, B.H.J.; Ataelmannan, K.; Laissue, J.; Blattmann, H.; Bräuer-Krisch, E.; Bravin, A.; Minczewska, J.; Crosbie, J.; Taherian, H.; et al. Memory and survival after microbeam radiation therapy. Eur. J. Radiol. 2008, 68 (Suppl. S3), S142–S146. [Google Scholar] [CrossRef]
- Potez, M.; Bouchet, A.; Flaender, M.; Rome, C.; Collomb, N.; Grotzer, M.; Krisch, M.; Djonov, V.; Balosso, J.; Brun, E.; et al. Synchrotron X-Ray Boost Delivered by Microbeam Radiation Therapy After Conventional X-Ray Therapy Fractionated in Time Improves F98 Glioma Control. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 360–369. [Google Scholar] [CrossRef]
- Bouchet, A.; Bräuer-Krisch, E.; Prezado, Y. Better Efficacy of Synchrotron Spatially Microfractionated Radiation Therapy Than Uniform Radiation Therapy on Glioma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1485–1494. [Google Scholar] [CrossRef] [PubMed]
- Schültke, E.; Trippel, M.; Bräuer-Krisch, E.; Renier, M.; Bartzsch, S.; Requardt, H.; Döbrössy, M.D.; Nikkhah, G. Pencilbeam irradiation technique for whole brain radiotherapy: Technical and biological challenges in a small animal model. PLoS ONE 2013, 8, e54960. [Google Scholar] [CrossRef] [PubMed]
- José-López, R.; Quintana, R.; de la Fuente, C.; Manzanilla, E.G.; Suñol, A.; Pi Castro, D.; Añor, S.; Sánchez-Masian, D.; Fernández-Flores, F.; Ricci, E.; et al. Clinical features, diagnosis, and survival analysis of dogs with glioma. J. Vet. Intern. Med. 2021, 35, 1902–1917. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Palomo, C.; Trappetti, V.; Potez, M.; Pellicioli, P.; Krisch, M.; Laissue, J.; Djonov, V. Complete Remission of Mouse Melanoma after Temporally Fractionated Microbeam Radiotherapy. Cancers 2020, 12, 2656. [Google Scholar] [CrossRef] [PubMed]
- Trappetti, V.; Fernandez-Palomo, C.; Smyth, L.; Klein, M.; Haberthür, D.; Butler, D.; Barnes, M.; Shintani, N.; de Veer, M.; Laissue, J.A.; et al. Synchrotron Microbeam Radiation Therapy for the Treatment of Lung Carcinoma: A Preclinical Study. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 1276–1288. [Google Scholar] [CrossRef] [PubMed]
- Montay-Gruel, P.; Acharya, M.M.; Gonçalves, J.P.; Petit, B.; Petridis, I.G.; Fuchs, P.; Leavitt, R.; Petersson, K.; Gondré, M.; Ollivier, J.; et al. Hypofractionated FLASH-RT as an Effective Treatment against Glioblastoma that Reduces Neurocognitive Side Effects in Mice. Clin. Cancer Res. 2021, 27, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Crosbie, J.C.; Fournier, P.; Bartzsch, S.; Donzelli, M.; Cornelius, I.; Stevenson, A.W.; Requardt, H.; Bräuer-Krisch, E. Energy spectra considerations for synchrotron radiotherapy trials on the ID17 bio-medical beamline at the European Synchrotron Radiation Facility. J. Synchrotron. Radiat. 2015, 22, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Thomlinson, W.; Berkven, S.P.; Berruyer, G.; Bertrand, B.; Blattmann, H.; Braeuer-Krisch, E.; Brochard, T.; Charvet, A.M.; Corde, S.; DiMichiel, M.; et al. Research at the European Synchrotron Radiation Facility MedicalBeamline. Cell Mol. Biol. 2000, 46, 1053–1063. [Google Scholar]
- Bräuer-Krisch, E.; Requardt, H.; Brochard, T.; Berruyer, G.; Renier, M. New technology enables high precision multislit collimators for microbeam radiation therapy. Rev. Sci. Instr. 2009, 80, 074301. [Google Scholar] [CrossRef]
- Bouchet, A.; Serduc, R.; Laissue, J.A.; Djonov, V. Effects of microbeam radiation therapy on normal and tumoral blood vessels. Phys. Med. 2015, 31, 634–641. [Google Scholar] [CrossRef] [Green Version]
- Renier, M.; Brochard, T.; Nemoz, C.; Thomlinson, W. A white-beam fast-shutter for microbeam radiation therapy at the ESRF. Nucl. Instrum. Methods A. 2002, 479, 656–660. [Google Scholar] [CrossRef]
- Bartzsch, S.; Corde, S.; Crosbie, J.C.; Day, L.; Donzelli, M.; Krisch, M.; Lerch, M.; Pellicioli, P.; Smyth, L.M.L.; Tehei, M. Technical advances in x-ray microbeam radiation therapy. Phys. Med. Biol. 2020, 65, 02TR01. [Google Scholar] [CrossRef]
- Bartzsch, S.; Lerch, M.; Petasecca, M.; Bräuer-Krisch, E.; Oelfke, U. Influence of polarization and a source model for dose calculation in MRT. Med. Phys. 2014, 41, 041703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemierko, A. Reporting and analyzing dose distributions: A concept of equivalent uniform dose. Med. Phys. 1997, 24, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F. Rat brain tumour models in experimental neuro-oncology: The 9L, C6, T9, F98, RG2 (D74), RT-2 and CNS-1 gliomas. J. Neurooncol. 1998, 36, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Bencokova, Z.; Pauron, L.; Devic, C.; Joubert, A.; Gastaldo, J.; Massart, C.; Balosso, J.; Foray, N. Molecular and cellular response of the most extensively used rodent glioma models to radiation and/or cisplatin. J. Neurooncol. 2008, 86, 13–21. [Google Scholar] [CrossRef]
- Fernandez-Palomo, C.; Mothersill, C.; Bräuer-Krisch, E.; Laissue, J.; Seymour, C.; Schültke, E. γ-H2AX as a marker for dose deposition in the brain of wistar rats after synchrotron microbeam radiation. PLoS ONE 2015, 10, e0119924. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaekel, F.; Bräuer-Krisch, E.; Bartzsch, S.; Laissue, J.; Blattmann, H.; Scholz, M.; Soloviova, J.; Hildebrandt, G.; Schültke, E. Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol. Int. J. Mol. Sci. 2022, 23, 8319. https://doi.org/10.3390/ijms23158319
Jaekel F, Bräuer-Krisch E, Bartzsch S, Laissue J, Blattmann H, Scholz M, Soloviova J, Hildebrandt G, Schültke E. Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol. International Journal of Molecular Sciences. 2022; 23(15):8319. https://doi.org/10.3390/ijms23158319
Chicago/Turabian StyleJaekel, Felix, Elke Bräuer-Krisch, Stefan Bartzsch, Jean Laissue, Hans Blattmann, Marten Scholz, Julia Soloviova, Guido Hildebrandt, and Elisabeth Schültke. 2022. "Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol" International Journal of Molecular Sciences 23, no. 15: 8319. https://doi.org/10.3390/ijms23158319
APA StyleJaekel, F., Bräuer-Krisch, E., Bartzsch, S., Laissue, J., Blattmann, H., Scholz, M., Soloviova, J., Hildebrandt, G., & Schültke, E. (2022). Microbeam Irradiation as a Simultaneously Integrated Boost in a Conventional Whole-Brain Radiotherapy Protocol. International Journal of Molecular Sciences, 23(15), 8319. https://doi.org/10.3390/ijms23158319