
Omeprazole Suppresses Oxaliplatin-Induced Peripheral Neuropathy in a Rodent Model and Clinical Database

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
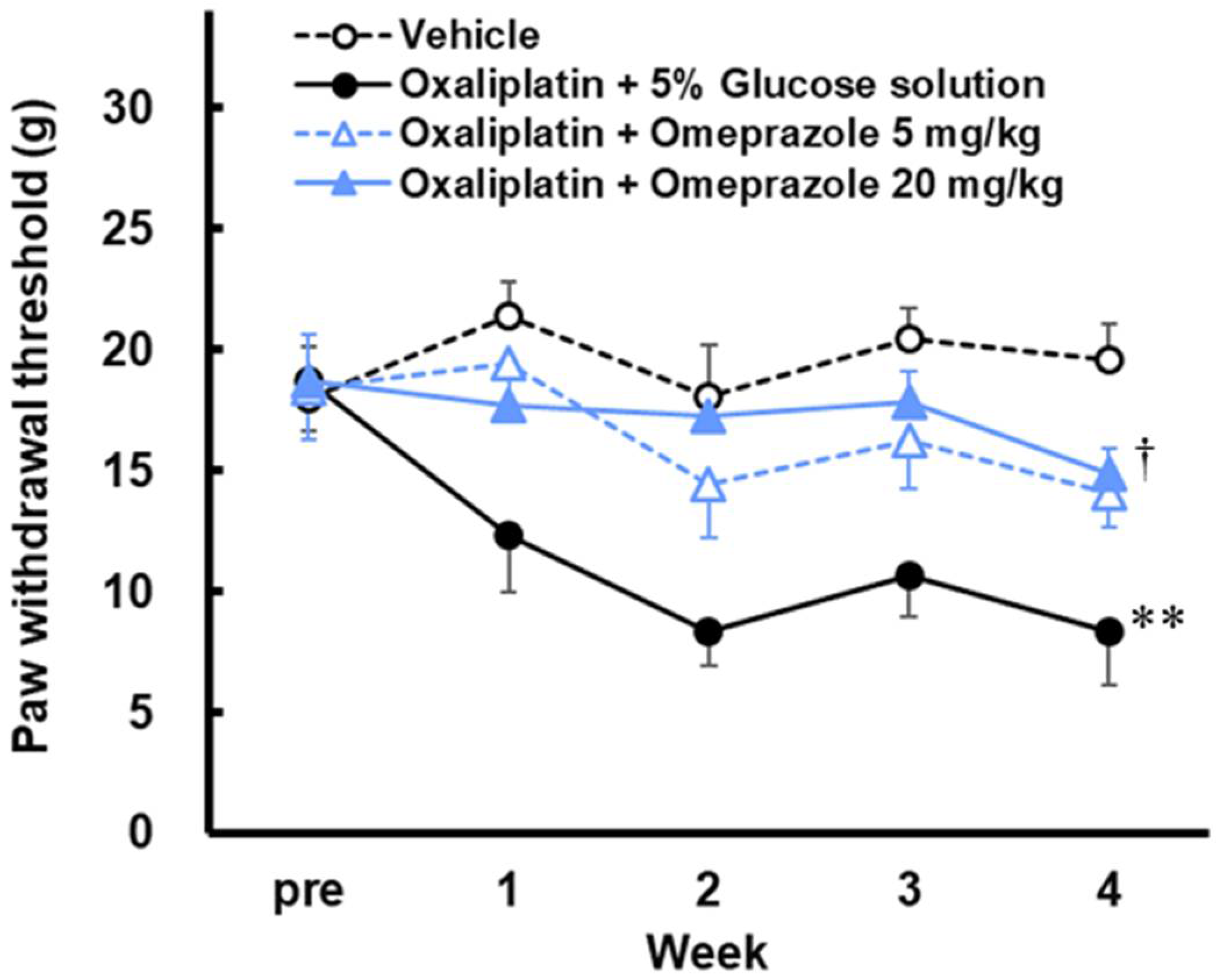
2.1. Effect of Omeprazole on Mechanical Hypersensitivity Induced by Oxaliplatin in Rats
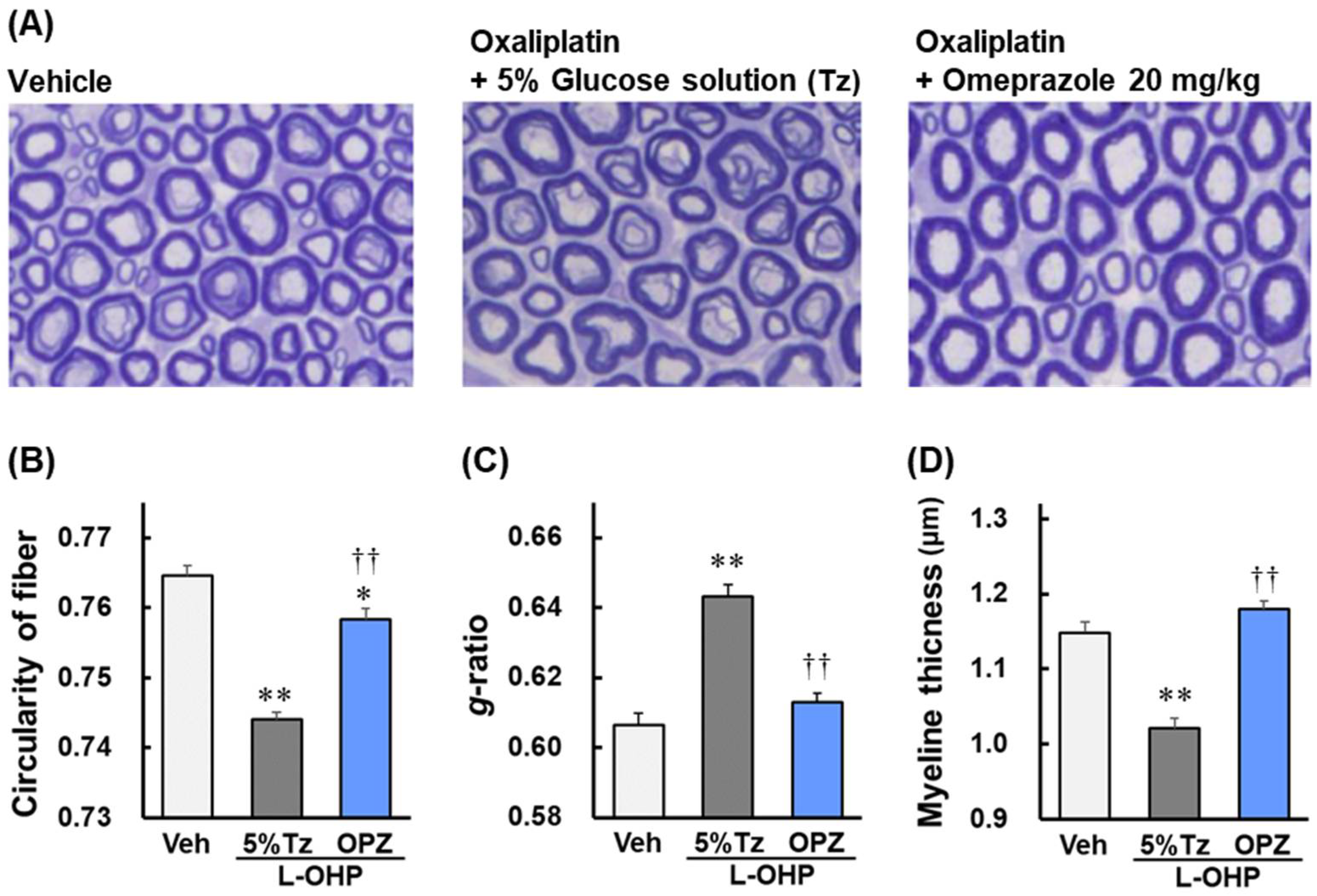
2.2. Effect of Omeprazole on Axonal Degeneration and Myelin Sheath Disorder of Sciatic Nerves Induced by Oxaliplatin in Rats
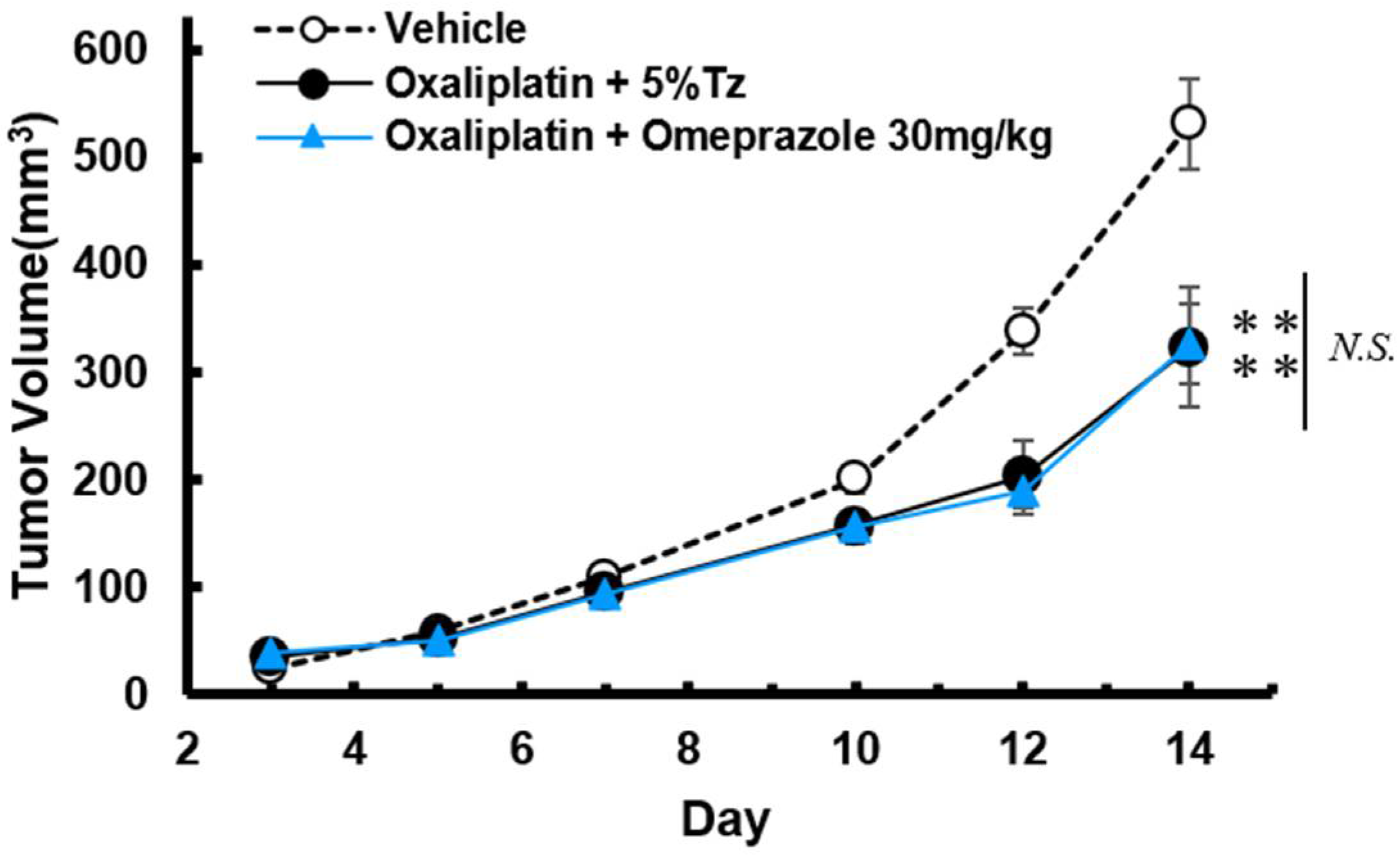
2.3. Effect of Omeprazole on the Anti-Tumor Effect of Oxaliplatin in Tumor-Bearing Mice
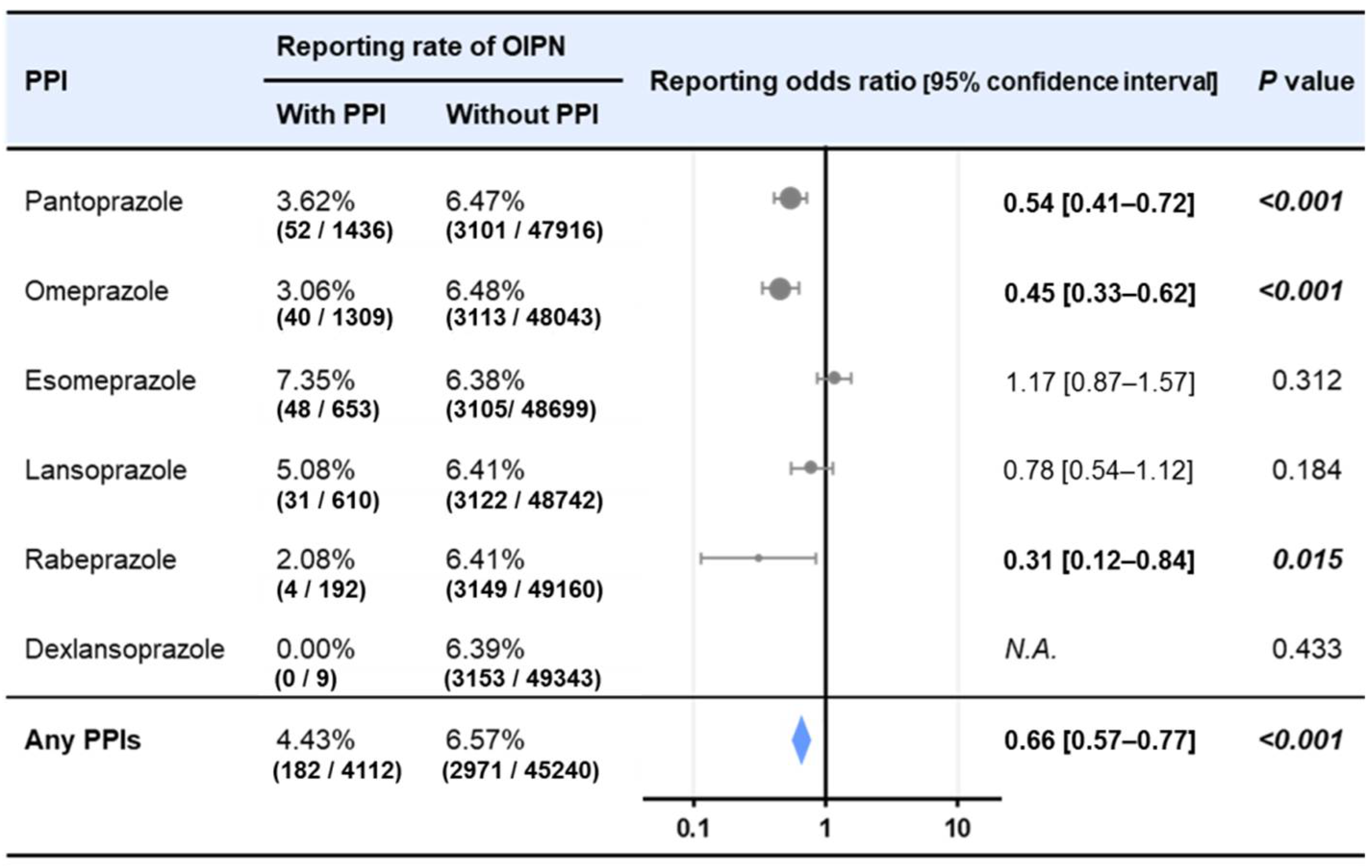
2.4. Effects of PPIs on Reporting Ratio of Peripheral Neuropathy in Oxaliplatin-Treated Patients in FAERS
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Drugs
4.3. Von Frey Test for Mechanical Hypersensitivity
4.4. Assessment of Sciatic Nerve Axonal Degeneration and Myelin Sheath Disorder
4.5. Assessment of Tumor Growth in Tumor-Bearing Mice
4.6. Analysis of FAERS Data
4.7. Sample Sizes
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Gramont, A.; Figer, A.; Seymour, M.; Homerin, M.; Hmissi, A.; Cassidy, J.; Boni, C.; Cortes-Funes, H.; Cervantes, A.; Freyer, G.; et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J. Clin. Oncol. 2000, 18, 2938–2947. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy, J.; Clarke, S.; Díaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Randomized phase III study of capecitabine plus oxaliplatin compared with fluorouracil/folinic acid plus oxaliplatin as first-line therapy for metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 2006–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmoll, H.J.; Tabernero, J.; Maroun, J.; de Braud, F.; Price, T.; Van Cutsem, E.; Hill, M.; Hoersch, S.; Rittweger, K.; Haller, D.G. Capecitabine Plus Oxaliplatin Compared with Fluorouracil/Folinic Acid As Adjuvant Therapy for Stage III Colon Cancer: Final Results of the NO16968 Randomized Controlled Phase III Trial. J. Clin. Oncol. 2015, 33, 3733–3740. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N. Engl. J. Med. 2014, 371, 1609–1618. [Google Scholar] [CrossRef] [Green Version]
- Hong, Y.S.; Park, Y.S.; Lim, H.Y.; Lee, J.; Kim, T.W.; Kim, K.P.; Kim, S.Y.; Baek, J.Y.; Kim, J.H.; Lee, K.W.; et al. S-1 plus oxaliplatin versus capecitabine plus oxaliplatin for first-line treatment of patients with metastatic colorectal cancer: A randomised, non-inferiority phase 3 trial. Lancet Oncol. 2012, 13, 1125–1132. [Google Scholar] [CrossRef]
- Wilson, R.H.; Lehky, T.; Thomas, R.R.; Quinn, M.G.; Floeter, M.K.; Grem, J.L. Acute oxaliplatin-induced peripheral nerve hyperexcitability. J. Clin. Oncol. 2002, 20, 1767–1774. [Google Scholar] [CrossRef]
- Argyriou, A.A.; Bruna, J.; Marmiroli, P.; Cavaletti, G. Chemotherapy-induced peripheral neurotoxicity (CIPN): An update. Crit. Rev. Oncol. Hematol. 2012, 82, 51–77. [Google Scholar] [CrossRef]
- Pasetto, L.M.; D’Andrea, M.R.; Rossi, E.; Monfardini, S. Oxaliplatin-related neurotoxicity: How and why? Crit. Rev. Oncol. Hematol. 2006, 59, 159–168. [Google Scholar] [CrossRef]
- Jordan, B.; Jahn, F.; Beckmann, J.; Unverzagt, S.; Müller-Tidow, C.; Jordan, K. Calcium and Magnesium Infusions for the Prevention of Oxaliplatin-Induced Peripheral Neurotoxicity: A Systematic Review. Oncology 2016, 90, 299–306. [Google Scholar] [CrossRef]
- Cascinu, S.; Catalano, V.; Cordella, L.; Labianca, R.; Giordani, P.; Baldelli, A.M.; Beretta, G.D.; Ubiali, E.; Catalano, G. Neuroprotective effect of reduced glutathione on oxaliplatin-based chemotherapy in advanced colorectal cancer: A randomized, double-blind, placebo-controlled trial. J. Clin. Oncol. 2002, 20, 3478–3483. [Google Scholar] [CrossRef] [PubMed]
- Oki, E.; Emi, Y.; Kojima, H.; Higashijima, J.; Kato, T.; Miyake, Y.; Kon, M.; Ogata, Y.; Takahashi, K.; Ishida, H.; et al. Preventive effect of Goshajinkigan on peripheral neurotoxicity of FOLFOX therapy (GENIUS trial): A placebo-controlled, double-blind, randomized phase III study. Int. J. Clin. Oncol. 2015, 20, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Egashira, N. Drug Repositioning for the Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy: A Mechanism- and Screening-Based Strategy. Front. Pharmacol. 2021, 11, 607780. [Google Scholar] [CrossRef] [PubMed]
- Kawashiri, T.; Mine, K.; Kobayashi, D.; Inoue, M.; Ushio, S.; Uchida, M.; Egashira, N.; Shimazoe, T. Therapeutic Agents for Oxaliplatin-Induced Peripheral Neuropathy; Experimental and Clinical Evidence. Int. J. Mol. Sci. 2021, 22, 1393. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, C.L.; Lacchetti, C.; Bleeker, J.; Cavaletti, G.; Chauhan, C.; Hertz, D.L.; Kelley, M.R.; Lavino, A.; Lustberg, M.B.; Paice, J.A.; et al. Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy in Survivors of Adult Cancers. J. Clin. Oncol. 2020, 38, 3325–3348. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Zhang, S.; Hu, T.; Qu, X.; Zhai, J.; Zhang, Y.; Tao, L.; Yin, J.; Song, Y. Omeprazole protects against cisplatin-induced nephrotoxicity by alleviating oxidative stress, inflammation, and transporter-mediated cisplatin accumulation in rats and HK-2 cells. Chem. Biol. Interact. 2019, 297, 130–140. [Google Scholar] [CrossRef]
- Abed, M.N.; Alassaf, F.A.; Jasim, M.H.M.; Alfahad, M.; Qazzaz, M.E. Comparison of Antioxidant Effects of the Proton Pump-Inhibiting Drugs Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole, and Rabeprazole. Pharmacology 2020, 105, 645–651. [Google Scholar] [CrossRef]
- Di Cesare Mannelli, L.; Zanardelli, M.; Failli, P.; Ghelardini, C. Oxaliplatin-induced oxidative stress in nervous system-derived cellular models: Could it correlate with in vivo neuropathy? Free Radic. Biol. Med. 2013, 64, 143–150. [Google Scholar] [CrossRef]
- Di Cesare Mannelli, L.; Zanardelli, M.; Failli, P.; Ghelardini, C. Oxaliplatin-induced neuropathy: Oxidative stress as pathological mechanism. Protective effect of silibinin. J. Pain 2012, 13, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Celik, H.; Kucukler, S.; Ozdemir, S.; Comakli, S.; Gur, C.; Kandemir, F.M.; Yardim, A. Lycopene protects against central and peripheral neuropathy by inhibiting oxaliplatin-induced ATF-6 pathway, apoptosis, inflammation and oxidative stress in brains and sciatic tissues of rats. Neurotoxicology 2020, 80, 29–40. [Google Scholar] [CrossRef]
- Tsutsumi, K.; Yamashita, Y.; Ushio, S.; Kawashiri, T.; Kaname, T.; Fujita, S.; Oishi, R.; Egashira, N. Oxaliplatin induces hypomyelination and reduced neuregulin 1 expression in the rat sciatic nerve. Neurosci. Res. 2014, 80, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Sun, J.; Kang, Z.; Zou, Z.; Wu, X.; Wang, Y.; Wu, G.; Harris, R.A.; Wang, J. Repurposing of omeprazole for oligodendrocyte differentiation and remyelination. Brain Res. 2019, 1710, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.; Gu, Z.; Gu, J.; Yu, J.; Huang, X.; Qin, F.; Li, L.; Ding, R.; Huo, J. Platinum accumulation in oxaliplatin-induced peripheral neuropathy. J. Peripher. Nerv. Syst. 2021, 26, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Cerina, M.; Narayanan, V.; Delank, A.; Meuth, P.; Graebenitz, S.; Göbel, K.; Herrmann, A.M.; Albrecht, S.; Daldrup, T.; Seidenbecher, T.; et al. Protective potential of dimethyl fumarate in a mouse model of thalamocortical demyelination. Brain Struct. Funct. 2018, 223, 3091–3106. [Google Scholar] [CrossRef]
- Miyagi, A.; Kawashiri, T.; Shimizu, S.; Shigematsu, N.; Kobayashi, D.; Shimazoe, T. Dimethyl Fumarate Attenuates Oxaliplatin-Induced Peripheral Neuropathy without Affecting the Anti-tumor Activity of Oxaliplatin in Rodents. Biol. Pharm. Bull. 2019, 42, 638–644. [Google Scholar] [CrossRef] [Green Version]
- Nawa, H.; Niimura, T.; Hamano, H.; Yagi, K.; Goda, M.; Zamami, Y.; Ishizawa, K. Evaluation of Potential Complications of Interstitial Lung Disease Associated with Antiandrogens Using Data from Databases Reporting Spontaneous Adverse Effects. Front. Pharmacol. 2021, 12, 655605. [Google Scholar] [CrossRef]
- Kawashiri, T.; Kobayashi, D.; Uchida, M.; Hiromoto, S.; Inoue, M.; Ikeda, H.; Inoue, M.; Shimazoe, T. Analysis of Secondary Leukemia and Myelodysplastic Syndrome After Chemotherapy for Solid Organ Tumors Using the Food and Drug Administration Adverse Event Reporting System (FAERS). J. Pharm. Pharm. Sci. 2021, 24, 499–508. [Google Scholar] [CrossRef]
- Hiromoto, S.; Kawashiri, T.; Yamanaka, N.; Kobayashi, D.; Mine, K.; Inoue, M.; Uchida, M.; Shimazoe, T. Use of omeprazole, the proton pump inhibitor, as a potential therapy for the capecitabine-induced hand-foot syndrome. Sci. Rep. 2021, 11, 8964. [Google Scholar] [CrossRef]
- Shimada, K.; Hasegawa, S.; Nakao, S.; Mukai, R.; Sasaoka, S.; Ueda, N.; Kato, Y.; Abe, J.; Mori, T.; Yoshimura, T.; et al. Adverse reaction profiles of hemorrhagic adverse reactions caused by direct oral anticoagulants analyzed using the Food and Drug Administration Adverse Event Reporting System (FAERS) database and the Japanese Adverse Drug Event Report (JADER) database. Int. J. Med. Sci. 2019, 16, 1295–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.X.; Lu, Z.H.; Wan, D.S.; Wu, X.J.; Ding, P.R.; Kong, L.H.; Pan, Z.Z.; Chen, G. Neuroprotective effect of neurotropin on chronic oxaliplatin-induced neurotoxicity in stage II and stage III colorectal cancer patients: Results from a prospective, randomised, single-centre, pilot clinical trial. Int. J. Colorectal. Dis. 2012, 27, 1645–1650. [Google Scholar] [CrossRef]
- Kerckhove, N.; Busserolles, J.; Stanbury, T.; Pereira, B.; Plence, V.; Bonnetain, F.; Krakowski, I.; Eschalier, A.; Pezet, D.; Balayssac, D. Effectiveness assessment of riluzole in the prevention of oxaliplatin-induced peripheral neuropathy: RILUZOX-01: Protocol of a randomised, parallel, controlled, double-blind and multicentre study by the UNICANCER-AFSOS Supportive Care intergroup. BMJ Open 2019, 9, e027770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsushima, Y.; Egashira, N.; Narishige, Y.; Fukui, S.; Kawashiri, T.; Yamauchi, Y.; Oishi, R. Calcium channel blockers reduce oxaliplatin-induced acute neuropathy: A retrospective study of 69 male patients receiving modified FOLFOX6 therapy. Biomed. Pharmacother. 2013, 67, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, N.; Kawashiri, T.; Kobayashi, D.; Shimizu, S.; Mine, K.; Hiromoto, S.; Uchida, M.; Egashira, N.; Shimazoe, T. Neuroprotective effect of alogliptin on oxaliplatin-induced peripheral neuropathy in vivo and in vitro. Sci. Rep. 2020, 10, 6734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakurai, M.; Egashira, N.; Kawashiri, T.; Yano, T.; Ikesue, H.; Oishi, R. Oxaliplatin-induced neuropathy in the rat: Involvement of oxalate in cold hyperalgesia but not mechanical allodynia. Pain 2009, 147, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, O.; Okada, Y.; Okabe, S. Effects of a proton pump inhibitor, omeprazole, on gastric secretion and gastric and duodenal ulcers or erosions in rats. Dig. Dis. Sci. 1984, 29, 394–401. [Google Scholar] [CrossRef]
- Yamamoto, S.; Kawashiri, T.; Higuchi, H.; Tsutsumi, K.; Ushio, S.; Kaname, T.; Shirahama, M.; Egashira, N. Behavioral and pharmacological characteristics of bortezomib-induced peripheral neuropathy in rats. J. Pharmacol. Sci. 2015, 129, 43–50. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mine, K.; Kawashiri, T.; Inoue, M.; Kobayashi, D.; Mori, K.; Hiromoto, S.; Kudamatsu, H.; Uchida, M.; Egashira, N.; Koyanagi, S.; et al. Omeprazole Suppresses Oxaliplatin-Induced Peripheral Neuropathy in a Rodent Model and Clinical Database. Int. J. Mol. Sci. 2022, 23, 8859. https://doi.org/10.3390/ijms23168859
Mine K, Kawashiri T, Inoue M, Kobayashi D, Mori K, Hiromoto S, Kudamatsu H, Uchida M, Egashira N, Koyanagi S, et al. Omeprazole Suppresses Oxaliplatin-Induced Peripheral Neuropathy in a Rodent Model and Clinical Database. International Journal of Molecular Sciences. 2022; 23(16):8859. https://doi.org/10.3390/ijms23168859
Chicago/Turabian StyleMine, Keisuke, Takehiro Kawashiri, Mizuki Inoue, Daisuke Kobayashi, Kohei Mori, Shiori Hiromoto, Hibiki Kudamatsu, Mayako Uchida, Nobuaki Egashira, Satoru Koyanagi, and et al. 2022. "Omeprazole Suppresses Oxaliplatin-Induced Peripheral Neuropathy in a Rodent Model and Clinical Database" International Journal of Molecular Sciences 23, no. 16: 8859. https://doi.org/10.3390/ijms23168859
APA StyleMine, K., Kawashiri, T., Inoue, M., Kobayashi, D., Mori, K., Hiromoto, S., Kudamatsu, H., Uchida, M., Egashira, N., Koyanagi, S., Ohdo, S., & Shimazoe, T. (2022). Omeprazole Suppresses Oxaliplatin-Induced Peripheral Neuropathy in a Rodent Model and Clinical Database. International Journal of Molecular Sciences, 23(16), 8859. https://doi.org/10.3390/ijms23168859