
Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Clinical Characteristics of Patients
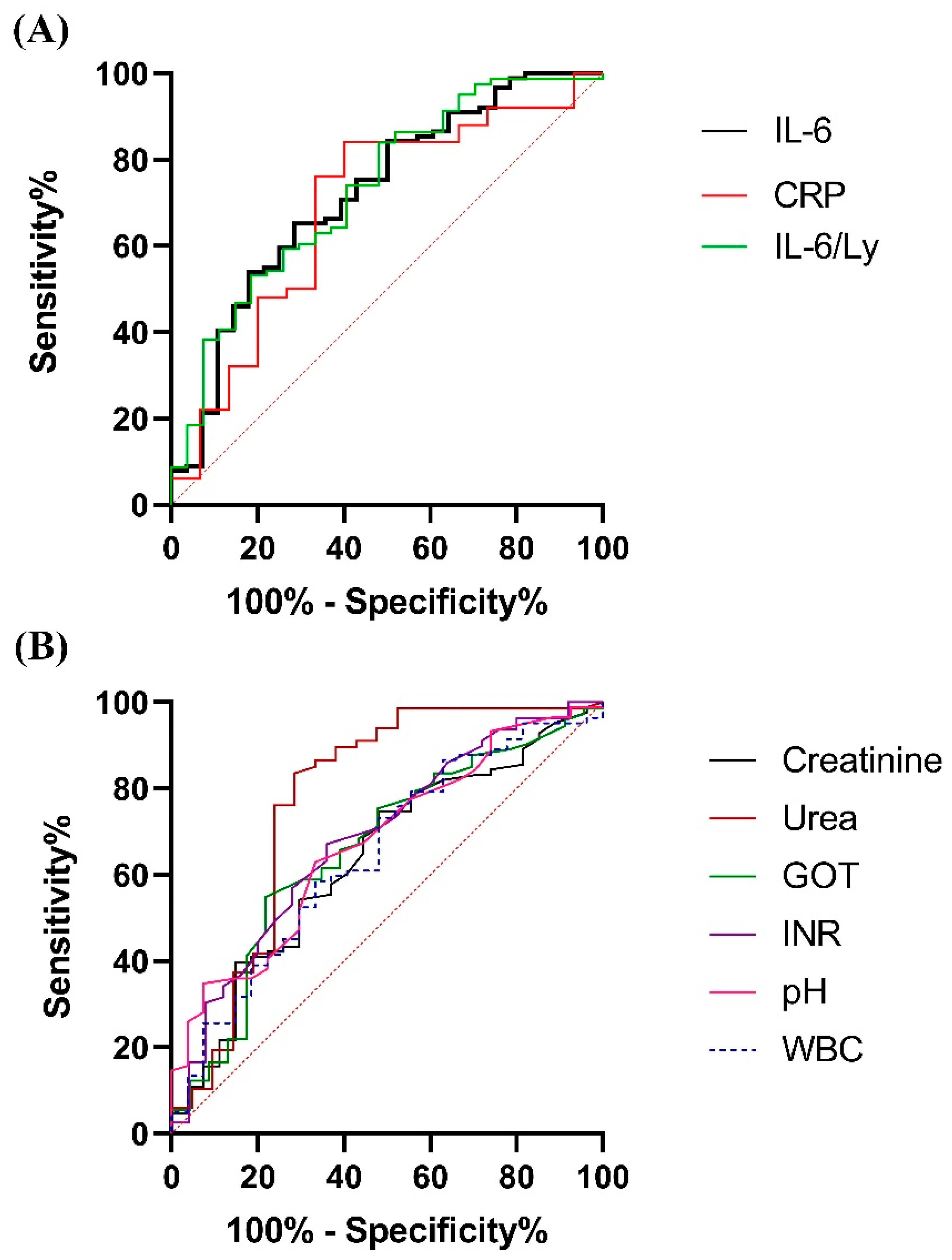
2.2. Establishing Optimal Cut-Off Levels for the Statistically Significant Biomarkers
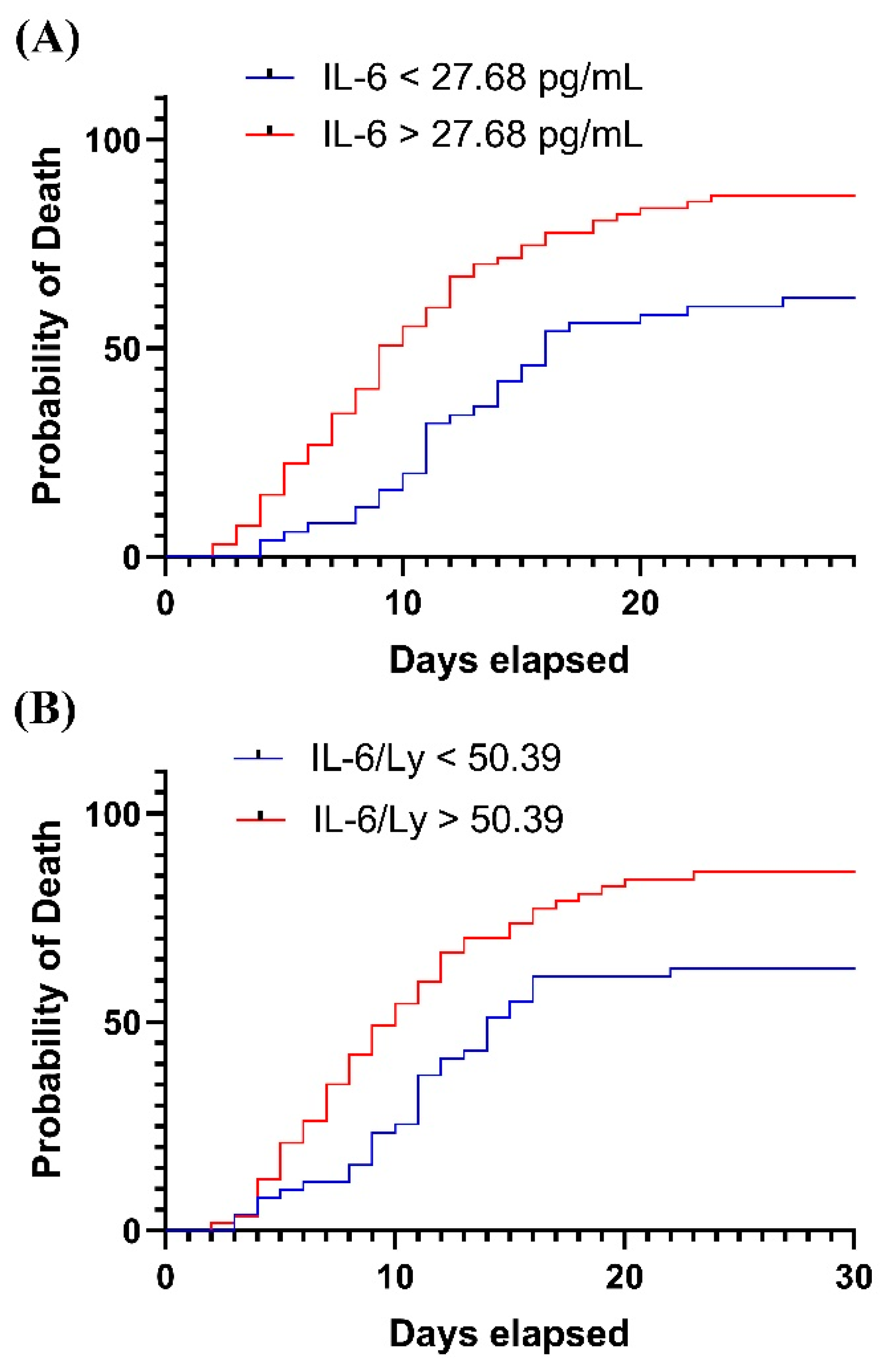
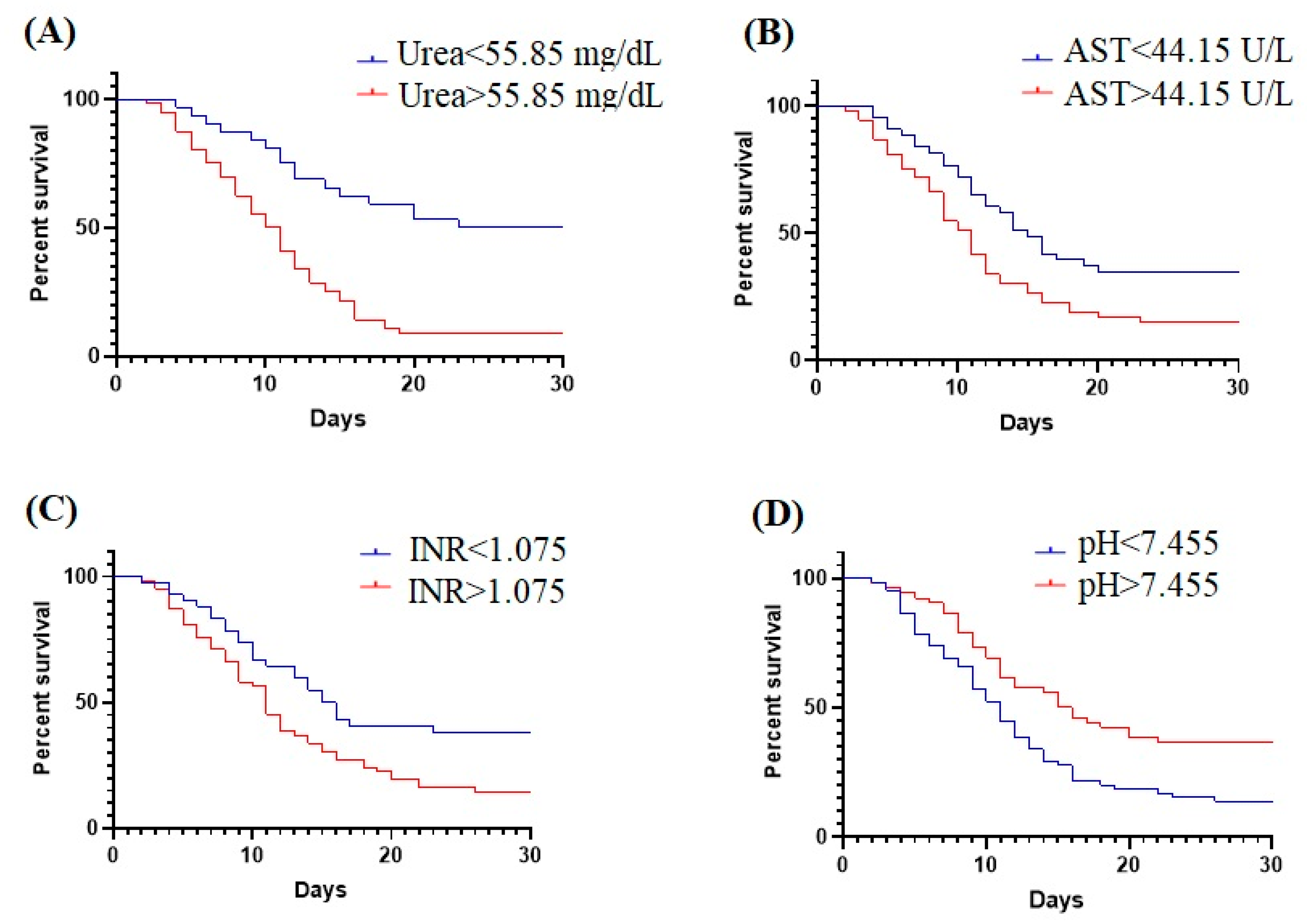
2.3. Survival Analysis
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Qian, Z.; Lu, S.; Luo, X.; Chen, Y.; Liu, L. Mortality and Clinical Interventions in Critically Ill Patient With Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 635560. [Google Scholar] [CrossRef] [PubMed]
- Chaddha, U.; Kaul, V.; Agrawal, A. What Is the True Mortality in the Critically Ill Patients with COVID-19? Indian J. Crit. Care Med. 2020, 24, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Taxbro, K.; Granath, A.; Sunnergren, O.; Seifert, S.; Jakubczyk, M.N.; Persson, M.; Hammarskjöld, A.; Alkemark, C.; Hammarskjöld, F.; RJL COVID-19 Research Group. Low Mortality Rates among Critically Ill Adults with COVID-19 at Three Non-Academic Intensive Care Units in South Sweden. Acta Anaesthesiol. Scand. 2021, 65, 1457–1465. [Google Scholar] [CrossRef] [PubMed]
- Huțanu, A.; Georgescu, A.M.; Andrejkovits, A.V.; Au, W.; Dobreanu, M. Insights into Innate Immune Response Against SARS-CoV-2 Infection. Rev. Romana De Med. De Lab. 2021, 29, 255–269. [Google Scholar] [CrossRef]
- Gustine, J.N.; Jones, D. Immunopathology of Hyperinflammation in COVID-19. Am. J. Pathol. 2021, 191, 4–17. [Google Scholar] [CrossRef]
- Wong, R.S.Y. Inflammation in COVID-19: From Pathogenesis to Treatment. Int. J. Clin. Exp. Pathol. 2021, 14, 831–844. [Google Scholar]
- Shekhawat, J.; Gauba, K.; Gupta, S.; Purohit, P.; Mitra, P.; Garg, M.; Misra, S.; Sharma, P.; Banerjee, M. Interleukin-6 Perpetrator of the COVID-19 Cytokine Storm. Ind. J. Clin. Biochem. 2021, 36, 440–450. [Google Scholar] [CrossRef]
- Montazersaheb, S.; Hosseiniyan Khatibi, S.M.; Hejazi, M.S.; Tarhriz, V.; Farjami, A.; Ghasemian Sorbeni, F.; Farahzadi, R.; Ghasemnejad, T. COVID-19 Infection: An Overview on Cytokine Storm and Related Interventions. Virol. J. 2022, 19, 92. [Google Scholar] [CrossRef]
- Li, J.; Rong, L.; Cui, R.; Feng, J.; Jin, Y.; Chen, X.; Xu, R. Dynamic Changes in Serum IL-6, IL-8, and IL-10 Predict the Outcome of ICU Patients with Severe COVID-19. Ann. Palliat. Med. 2021, 10, 3706–3714. [Google Scholar] [CrossRef]
- Gubernatorova, E.O.; Gorshkova, E.A.; Polinova, A.I.; Drutskaya, M.S. IL-6: Relevance for Immunopathology of SARS-CoV-2. Cytokine Growth Factor Rev. 2020, 53, 13–24. [Google Scholar] [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B.J.; Hellmuth, J.C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated Levels of IL-6 and CRP Predict the Need for Mechanical Ventilation in COVID-19. J. Allergy Clin. Immunol. 2020, 146, 128–136.e4. [Google Scholar] [CrossRef] [PubMed]
- Mosquera-Sulbaran, J.A.; Pedreañez, A.; Carrero, Y.; Callejas, D. C-reactive Protein as an Effector Molecule in Covid-19 Pathogenesis. Rev. Med. Virol. 2021, 31, e2221. [Google Scholar] [CrossRef] [PubMed]
- Ahnach, M.; Zbiri, S.; Nejjari, S.; Ousti, F.; Elkettani, C. C-Reactive Protein as an Early Predictor of COVID-19 Severity. J. Med. Biochem. 2020, 39, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, K.I.; Liu, S.; Yan, Z.; Xu, C.; Qiao, Z. Plasma CRP Level Is Positively Associated with the Severity of COVID-19. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 18. [Google Scholar] [CrossRef]
- Alroomi, M.; Rajan, R.; Omar, A.A.; Alsaber, A.; Pan, J.; Fatemi, M.; Zhanna, K.D.; Aboelhassan, W.; Almutairi, F.; Alotaibi, N.; et al. Ferritin Level: A Predictor of Severity and Mortality in Hospitalized COVID-19 Patients. Immun. Inflamm. Dis. 2021, 9, 1648–1655. [Google Scholar] [CrossRef]
- Deng, F.; Zhang, L.; Lyu, L.; Lu, Z.; Gao, D.; Ma, X.; Guo, Y.; Wang, R.; Gong, S.; Jiang, W. Increased Levels of Ferritin on Admission Predicts Intensive Care Unit Mortality in Patients with COVID-19. Med. Clin. 2021, 156, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.-H.; Qin, C.; Chen, M.; Wang, W.; Tian, D.-S. D-Dimer Level Is Associated with the Severity of COVID-19. Thromb Res. 2020, 195, 219–225. [Google Scholar] [CrossRef]
- Moisa, E.; Corneci, D.; Negoita, S.; Filimon, C.R.; Serbu, A.; Negutu, M.I.; Grintescu, I.M. Dynamic Changes of the Neutrophil-to-Lymphocyte Ratio, Systemic Inflammation Index, and Derived Neutrophil-to-Lymphocyte Ratio Independently Predict Invasive Mechanical Ventilation Need and Death in Critically Ill COVID-19 Patients. Biomedicines 2021, 9, 1656. [Google Scholar] [CrossRef]
- Muhammad, S.; Fischer, I.; Naderi, S.; Faghih Jouibari, M.; Abdolreza, S.; Karimialavijeh, E.; Aslzadeh, S.; Mashayekhi, M.; Zojaji, M.; Kahlert, U.D.; et al. Systemic Inflammatory Index Is a Novel Predictor of Intubation Requirement and Mortality after SARS-CoV-2 Infection. Pathogens 2021, 10, 58. [Google Scholar] [CrossRef]
- Seyit, M.; Avci, E.; Nar, R.; Senol, H.; Yilmaz, A.; Ozen, M.; Oskay, A.; Aybek, H. Neutrophil to Lymphocyte Ratio, Lymphocyte to Monocyte Ratio and Platelet to Lymphocyte Ratio to Predict the Severity of COVID-19. Am. J. Emerg. Med. 2021, 40, 110–114. [Google Scholar] [CrossRef]
- Dávila-Collado, R.; Jarquín-Durán, O.; Solís-Vallejo, A.; Nguyen, M.A.; Espinoza, J.L. Elevated Monocyte to Lymphocyte Ratio and Increased Mortality among Patients with Chronic Kidney Disease Hospitalized for COVID-19. JPM 2021, 11, 224. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chang, X.; Huang, J.; Pan, W.; Si, Z.; Zhang, C.; Li, H. The Role of IL-6/Lymphocyte Ratio in the Peripheral Blood of Severe Patients with COVID-19. Int. Immunopharmacol. 2021, 97, 107569. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Al-Ahmed, S.H.; Garout, M.A.; Al-Qaaneh, A.M.; Sule, A.A.; Tirupathi, R.; Mutair, A.A.; Alhumaid, S.; Hasan, A.; Dhawan, M.; et al. Diverse Immunological Factors Influencing Pathogenesis in Patients with COVID-19: A Review on Viral Dissemination, Immunotherapeutic Options to Counter Cytokine Storm and Inflammatory Responses. Pathogens 2021, 10, 565. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.; Fatima, R.; Assaly, R. Elevated Interleukin-6 and Severe COVID-19: A Meta-Analysis. J. Med. Virol. 2020, 92, 2283–2285. [Google Scholar] [CrossRef]
- Aykal, G.; Esen, H.; Seyman, D.; Çalışkan, T. Could IL-6 Predict the Clinical Severity of COVID-19? Turk. J. Biochem. 2021, 46, 499–507. [Google Scholar] [CrossRef]
- Liu, X.; Wang, H.; Shi, S.; Xiao, J. Association between IL-6 and Severe Disease and Mortality in COVID-19 Disease: A Systematic Review and Meta-Analysis. Postgrad. Med. J. 2021; ahead of print. [Google Scholar] [CrossRef]
- Rahayu, R.; Winarto, W.; Nasihun, T. Interleukin-6 and C-Reactive Protein on Admission as Predictor of Mortality in Severe COVID-19 Patients: A Retrospective Cohort Study. Open Access Maced. J. Med. Sci. 2022, 10, 227–231. [Google Scholar] [CrossRef]
- Smilowitz, N.R.; Kunichoff, D.; Garshick, M.; Shah, B.; Pillinger, M.; Hochman, J.S.; Berger, J.S. C-Reactive Protein and Clinical Outcomes in Patients with COVID-19. Eur. Heart J. 2021, 42, 2270–2279. [Google Scholar] [CrossRef]
- Elshazli, R.M.; Toraih, E.A.; Elgaml, A.; El-Mowafy, M.; El-Mesery, M.; Amin, M.N.; Hussein, M.H.; Killackey, M.T.; Fawzy, M.S.; Kandil, E. Diagnostic and Prognostic Value of Hematological and Immunological Markers in COVID-19 Infection: A Meta-Analysis of 6320 Patients. PLoS ONE 2020, 15, e0238160. [Google Scholar] [CrossRef]
- Gu, Y.; Wang, D.; Chen, C.; Lu, W.; Liu, H.; Lv, T.; Song, Y.; Zhang, F. PaO2/FiO2 and IL-6 Are Risk Factors of Mortality for Intensive Care COVID-19 Patients. Sci. Rep. 2021, 11, 7334. [Google Scholar] [CrossRef]
- Lavillegrand, J.-R.; Garnier, M.; Spaeth, A.; Mario, N.; Hariri, G.; Pilon, A.; Berti, E.; Fieux, F.; Thietart, S.; Urbina, T.; et al. Elevated Plasma IL-6 and CRP Levels Are Associated with Adverse Clinical Outcomes and Death in Critically Ill SARS-CoV-2 Patients: Inflammatory Response of SARS-CoV-2 Patients. Ann. Intensive Care 2021, 11, 9. [Google Scholar] [CrossRef]
- Brasen, C.L.; Christensen, H.; Olsen, D.A.; Kahns, S.; Andersen, R.F.; Madsen, J.B.; Lassen, A.; Kierkegaard, H.; Jensen, A.; Sydenham, T.V.; et al. Daily Monitoring of Viral Load Measured as SARS-CoV-2 Antigen and RNA in Blood, IL-6, CRP and Complement C3d Predicts Outcome in Patients Hospitalized with COVID-19. Clin. Chem. Lab. Med. 2021, 59, 1988–1997. [Google Scholar] [CrossRef] [PubMed]
- Laguna-Goya, R.; Utrero-Rico, A.; Talayero, P.; Lasa-Lazaro, M.; Ramirez-Fernandez, A.; Naranjo, L.; Segura-Tudela, A.; Cabrera-Marante, O.; Rodriguez de Frias, E.; Garcia-Garcia, R.; et al. IL-6–Based Mortality Risk Model for Hospitalized Patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 799–807.e9. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, M.; Hadzibegovic, A.; Kovac, M.; Jovanovic, B.; Stanisavljevic, J.; Djikic, M.; Sijan, D.; Ladjevic, N.; Palibrk, I.; Djukanovic, M.; et al. D-Dimer, CRP, PCT, and IL-6 Levels at Admission to ICU Can Predict In-Hospital Mortality in Patients with COVID-19 Pneumonia. Oxidative Med. Cell. Longev. 2022, 2022, 8997709. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; He, W.; Liang, J.; Wang, L.; Yu, X.; Bao, M.; Liu, H. Association of Interleukin-6 Levels with Morbidity and Mortality in Patients with Coronavirus Disease 2019 (COVID-19). Jpn. J. Infect. Dis. 2021, 74, 293–298. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic Value of Interleukin-6, C-Reactive Protein, and Procalcitonin in Patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Lampart, M.; Zellweger, N.; Bassetti, S.; Tschudin-Sutter, S.; Rentsch, K.M.; Siegemund, M.; Bingisser, R.; Osswald, S.; Kuster, G.M.; Twerenbold, R. Clinical Utility of Inflammatory Biomarkers in COVID-19 in Direct Comparison to Other Respiratory Infections—A Prospective Cohort Study. PLoS ONE 2022, 17, e0269005. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Kumar, S.; Talwar, D.; Raisinghani, N.; Madaan, S.; Hulkoti, V.; Akhilesh, A.; Khanna, S.; Shah, D.; Nimkar, S. Interleukin 6 and Its Correlation with COVID-19 in Terms of Outcomes in an Intensive Care Unit of a Rural Hospital: A Cross-Sectional Study. Indian J. Crit. Care Med. 2022, 26, 39–42. [Google Scholar] [CrossRef]
- Masotti, L.; Grifoni, E.; Pelagalli, G.; Cioni, E.; Mattaliano, C.; Cioffi, E.; Maggi, F.; Pinto, G.; Madonia, E.M.; Micheletti, I.; et al. Prognostic Role of Interleukin-6/Lymphocytes Ratio in SARS-CoV2 Related Pneumonia. Int. Immunopharmacol. 2022, 103, 108435. [Google Scholar] [CrossRef]
- Para, O.; Caruso, L.; Pestelli, G.; Tangianu, F.; Carrara, D.; Maddaluni, L.; Tamburello, A.; Castelnovo, L.; Fedi, G.; Guidi, S.; et al. Ferritin as Prognostic Marker in COVID-19: The FerVid Study. Postgrad. Med. 2022, 134, 58–63. [Google Scholar] [CrossRef]
- Cheng, L.; Li, H.; Li, L.; Liu, C.; Yan, S.; Chen, H.; Li, Y. Ferritin in the Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. J. Clin. Lab. Anal. 2020, 34, e23618. [Google Scholar] [CrossRef]
- Edeas, M.; Saleh, J.; Peyssonnaux, C. Iron: Innocent Bystander or Vicious Culprit in COVID-19 Pathogenesis? Int. J. Infect. Dis. 2020, 97, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Nugroho, J.; Wardhana, A.; Maghfirah, I.; Mulia, E.P.B.; Rachmi, D.A.; A’yun, M.Q.; Septianda, I. Relationship of D-Dimer with Severity and Mortality in SARS-CoV-2 Patients: A Meta-Analysis. Int. J. Lab. Hematol. 2021, 43, 110–115. [Google Scholar] [CrossRef]
- Varikasuvu, S.R.; Varshney, S.; Dutt, N.; Munikumar, M.; Asfahan, S.; Kulkarni, P.P.; Gupta, P. D-Dimer, Disease Severity, and Deaths (3D-Study) in Patients with COVID-19: A Systematic Review and Meta-Analysis of 100 Studies. Sci. Rep. 2021, 11, 21888. [Google Scholar] [CrossRef] [PubMed]
- Bloom, P.P.; Meyerowitz, E.A.; Reinus, Z.; Daidone, M.; Gustafson, J.; Kim, A.Y.; Schaefer, E.; Chung, R.T. Liver Biochemistries in Hospitalized Patients With COVID-19. Hepatology 2021, 73, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Burlea, B.; Gorun, F.; Motoc, A.; Gorun, O.M.; Malita, D.; Ratiu, A.; Margan, R.; Grigoras, M.L.; Bratosin, F.; et al. Predictive Value of Blood Coagulation Parameters in Poor Outcomes in COVID-19 Patients: A Retrospective Observational Study in Romania. J. Clin. Med. 2022, 11, 2831. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Paliogiannis, P.; Carru, C.; Mangoni, A.A. INR and COVID-19 Severity and Mortality: A Systematic Review with Meta-Analysis and Meta-Regression. Adv. Med. Sci. 2021, 66, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Li, S.; Sun, Q.; Zhu, J.; Chen, B.; Xiong, M.; Cao, G. Immune-Inflammatory Parameters in COVID-19 Cases: A Systematic Review and Meta-Analysis. Front. Med. 2020, 7, 301. [Google Scholar] [CrossRef]
- Lee, J.Y.; Nam, B.-H.; Kim, M.; Hwang, J.; Kim, J.Y.; Hyun, M.; Kim, H.A.; Cho, C.-H. A Risk Scoring System to Predict Progression to Severe Pneumonia in Patients with Covid-19. Sci. Rep. 2022, 12, 5390. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-Survivors (n = 89) | Survivors (n = 28) | p |
|---|---|---|---|
| Age (years) | 66 ± 12 | 58 ± 14 | 0.0033 * |
| Male gender | 46 (51.68%) | 20 (71.42%) | 0.0819 † |
| Tocilizumab Pharmacotherapy | 7 (7.86%) | 1 (3.57%) | 0.6779 † |
| Remdesivir Pharmacotherapy | 42 (47.19%) | 16 (57.14%) | 0.3927 † |
| ≥1 comorbidity (excluding type 2 diabetes) | 82 (94.25%) | 22 (78.57%) | 0.0781 † |
| Type 2 diabetes | 38 (42.69%) | 9 (32.14%) | 0.3808 † |
| Bacterial pulmonary infection | 12 (13.48%) | 1 (3.57%) | 0.1855 † |
| Laboratory Parameter | Non-Survivors (n = 89) | Survivors (n = 28) | p |
|---|---|---|---|
| Inflammatory biomarkers | |||
| IL-6 (pg/mL) | 49.84 (20.85–107.6) | 17.13 (7.468–37.43) | 0.0004 ‡ |
| Ferritin (ng/mL) | 1357 (711.3–2392) | 987.9 (588.2–2354) | 0.1291 ‡ |
| CRP (mg/L) | 106.6 (67.39–174.4) | 45.06 (23.81–119.6) | 0.0270 ‡ |
| D-Dimers (μg/mL) | 1132.5 (529.5–5273) | 735.25 (289–1138) | 0.0857 ‡ |
| Inflammatory indices | |||
| IL-6/Ly | 85.09 (22.74–163.3) | 16.95 (8.44–60.42) | 0.0003 ‡ |
| NLR | 14.47 (9.90–23.77) | 12.19 (9.42–23.2) | 0.0956 ‡ |
| SII | 3542 (2227–5582) | 3083 (2089–5343) | 0.3811 ‡ |
| PLR | 336 (256.8–491.7) | 354.6(264.1–516.4) | 0.9944 ‡ |
| MLR | 0.546 (0.443–0.814) | 0.783 (0.442–1.283) | 0.0587 ‡ |
| Biochemical markers and coagulation tests | |||
| AST (U/L) | 54 (34.5–75.5) | 33 (25–48) | 0.0209 ‡ |
| ALT (U/L) | 40 (27–59.5) | 53 (23–90) | 0.4222 ‡ |
| Total Bilirubin (mg/dL) | 0.45 (0.32–0.62) | 0.46 (0.36–0.67) | 0.5763 ‡ |
| Direct Bilirubin (mg/dL) | 0.61 ± 1.03 | 0.32 ± 0.17 | 0.9062 * |
| Creatinine (mg/dL) | 0.91 (0.72–1.81) | 0.73 (0.65–1.04) | 0.0306 ‡ |
| Urea (mg/dL) | 73.2 (56.1–133.8) | 34 (28.35–73.5) | 0.0002 ‡ |
| Blood Glucose (mg/dL) | 200.6 ± 73.05 | 192.1 ± 77.99 | 0.602 * |
| INR | 1.12 (1.03–1.25) | 1.05 (0.975–1.125) | 0.0055 ‡ |
| Complete blood count | |||
| RBC (×106/μL) | 4.22 ± 0.63 | 4.45 ± 0.61 | 0.0934 * |
| Hemoglobin (g/dL) | 12.23 ±1.99 | 12.97 ± 1.83 | 0.0919 * |
| Hematocrit (%) | 37.57 ± 6.09 | 39.46 ± 5.07 | 0.1486 * |
| MCV (fL) | 89.9 (86.85–94.5) | 88.1 (86.39–92.1) | 0.9134 ‡ |
| MCH (pg) | 29.3 (28.36–30.88) | 29.02 (28–30.34) | 0.4962 ‡ |
| MCHC (g/dL) | 32.52 ± 1.30 | 32.9 ± 1.41 | 0.2063 * |
| WBC (×109/L) | 12.73 (9.09–16.69) | 9.33 (7.15–13.56) | 0.0223 ‡ |
| Neutrophils (×109/L) | 10.86 (7.558–14.02) | 8.51 (5.88–12.13) | 0.0596 ‡ |
| Lymphocytes (×109/L) | 0.72 (0.42–0.99) | 0.71 (0.47–0.92) | 0.5967 ‡ |
| Monocytes (×109/L) | 0.50 (0.30–0.83) | 0.48 (0.3–0.59) | 0.3295 ‡ |
| Eosinophils (×109/L) | 0.006 (0–0.02) | 0.005 (0–0.04) | 0.9682 ‡ |
| Basophils (×109/L) | 0.020 (0.008–0.044) | 0.022 (0.011–0.035) | 0.9692 ‡ |
| Platelets (×103/μL) | 247.4 ± 104.2 | 267.6 ± 86.68 | 0.2411 * |
| Acid-base balance | |||
| pH | 7.44 (7.33–7.47) | 7.47 (7.43–7.52) | 0.0055 ‡ |
| pO2 (mmHg) | 72.55 (59.5–90.7) | 73.5 (59.25–92.23) | 0.9539 ‡ |
| Lactate (mmol/L) | 1.6 (1.1–2.1) | 1.5 (1.2–2.1) | 0.9654 ‡ |
| SO2 (%) | 92 (87.25–97) | 94 (89–97) | 0.8902 ‡ |
| Laboratory Parameter | Cut-Off Value | AUC | 95% CI | p Value | Sensitivity % | Specificity % |
|---|---|---|---|---|---|---|
| IL-6 | 27.68 pg/mL | 0.721 | 0.61–0.833 | 0.0004 | 65.17 | 67.86 |
| CRP | 68.15 mg/L | 0.689 | 0.527–0.851 | 0.027 | 76 | 66.67 |
| IL-6/Ly | 50.39 | 0.731 | 0.62–0.841 | 0.0003 | 60.49 | 70.37 |
| Creatinine | 0.83 mg/dL | 0.638 | 0.518–0.758 | 0.031 | 57.83 | 62.96 |
| Urea | 55.85 mg/dL | 0.772 | 0.631–0.91 | 0.0002 | 76.12 | 76.19 |
| AST | 44.15 U/L | 0.66 | 0.53–0.79 | 0.0209 | 61.64 | 65.22 |
| INR | 1.075 | 0.684 | 0.564–0.805 | 0.0055 | 67.09 | 64 |
| pH | 7.455 | 0.676 | 0.565–0.787 | 0.0055 | 62.92 | 66.67 |
| WBC | 11.68 × 109/L | 0.647 | 0.527–0.766 | 0.0223 | 59.76 | 62.96 |
| Laboratory Parameter | Log-Rank Test p Value | HR | 95% CI |
|---|---|---|---|
| IL-6 | 0.0002 | 2.17 | 1.43–3.29 |
| CRP | 0.1408 | 1.57 | 0.87–2.84 |
| IL-6/Ly | 0.0019 | 1.64 | 1.12–2.41 |
| Creatinine | 0.0521 | 1.36 | 0.93–1.98 |
| Urea | <0.0001 | 2.22 | 1.45–3.38 |
| AST | 0.0094 | 1.56 | 1.04–2.33 |
| INR | 0.0091 | 1.54 | 1.05–2.26 |
| pH | 0.0029 | 0.62 | 0.43–0.9 |
| WBC | 0.2438 | 1.2 | 0.82–1.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pál, K.; Molnar, A.A.; Huțanu, A.; Szederjesi, J.; Branea, I.; Timár, Á.; Dobreanu, M. Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 10423. https://doi.org/10.3390/ijms231810423
Pál K, Molnar AA, Huțanu A, Szederjesi J, Branea I, Timár Á, Dobreanu M. Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients. International Journal of Molecular Sciences. 2022; 23(18):10423. https://doi.org/10.3390/ijms231810423
Chicago/Turabian StylePál, Krisztina, Anca Alexandra Molnar, Adina Huțanu, János Szederjesi, Ionuț Branea, Ágota Timár, and Minodora Dobreanu. 2022. "Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients" International Journal of Molecular Sciences 23, no. 18: 10423. https://doi.org/10.3390/ijms231810423
APA StylePál, K., Molnar, A. A., Huțanu, A., Szederjesi, J., Branea, I., Timár, Á., & Dobreanu, M. (2022). Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients. International Journal of Molecular Sciences, 23(18), 10423. https://doi.org/10.3390/ijms231810423