
Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events

 , , ,
, , ,  , and
, and 
Abstract
:1. Background
2. Results
2.1. Patients’ Characteristics
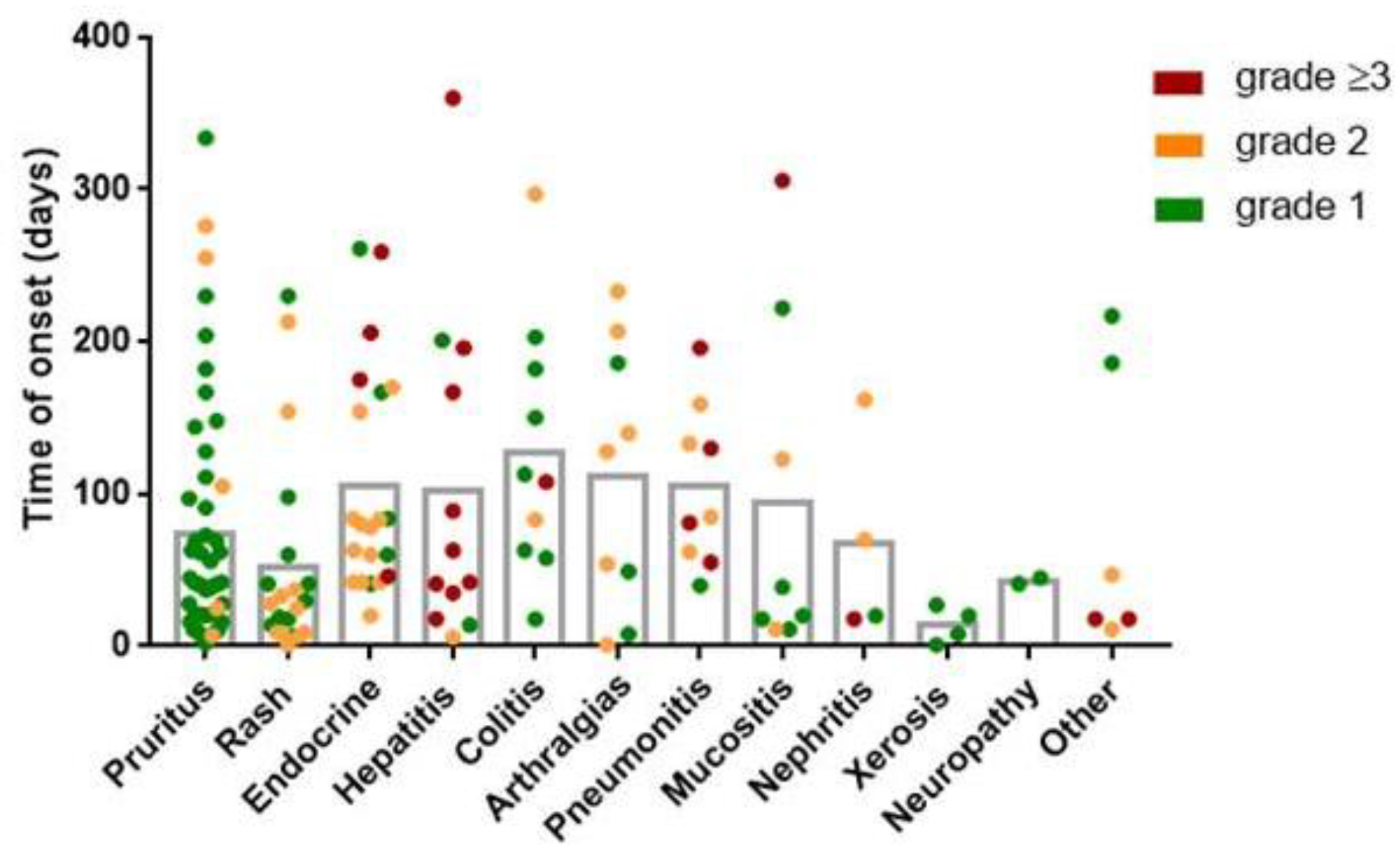
2.2. IrAE Characteristics
2.3. ANA Pattern Appearance during ICI Therapy
2.4. Association between ANA Development and IrAEs
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Sample Collection
4.3. Detection of Antinuclear Antibodies
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naidoo, J.; Page, D.B.; Wolchok, J.D. Immune Checkpoint Blockade. Hematol. Oncol. Clin. N. Am. 2014, 28, 585–600. [Google Scholar] [CrossRef]
- Stucci, S.; Palmirotta, R.; Passarelli, A.; Silvestris, E.; Argentiero, A.; Lanotte, L.; Acquafredda, S.; Todisco, A.; Silvestris, F. Immune-related adverse events during anticancer immunotherapy: Pathogenesis and management. Oncol. Lett. 2017, 14, 5671–5680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darvin, P.; Toor, S.M.; Sasidharan Nair, V.; Elkord, E. Immune checkpoint inhibitors: Recent progress and potential biomarkers. Exp. Mol. Med. 2018, 50, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, R.; Zhu, J.; Liu, Y.; Xin, Y.; Wang, Y.; Niu, K.; Wei, H. Efficacy of immune checkpoint inhibitors in the treatment of non-small cell lung cancer patients with different genes mutation: A meta-analysis. Medicine 2021, 100, e19713. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller, W.H., Jr.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall survival in patients with advanced melanoma who received nivolumab versus investigator’s choice chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef]
- Weinmann, S.C.; Pisetsky, D.S. Mechanisms of immune-related adverse events during the treatment of cancer with immune checkpoint inhibitors. Rheumatology 2019, 58 (Suppl. S7), vii59–vii67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Gerber, D.E. Autoimmunity, checkpoint inhibitor therapy and immune-related adverse events: A review. Semin. Cancer Biol. 2019, 64, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Gremese, E.; Alivernini, S.; Ferraccioli, E.S.; Ferraccioli, G. Checkpoint inhibitors (CPI) and autoimmune chronic inflammatory diseases (ACIDs): Tolerance and loss of tolerance in the occurrence of immuno-rheumatologic manifestations. Clin. Immunol. 2020, 214, 108395. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, R.J.; Vanhoorelbeke, K.; Leypoldt, F.; Kaya, Z.; Bieber, K.; McLachlan, S.M.; Komorowski, L.; Luo, J.; Marques, O.C.; Hammers, C.; et al. Mechanisms of Autoantibody-Induced Pathology. Front. Immunol. 2017, 8, 603. [Google Scholar] [CrossRef] [Green Version]
- Tahir, S.A.; Gao, J.; Miura, Y.; Blando, J.; Tidwell, R.S.S.; Zhao, H.; Subudhi, S.K.; Tawbi, H.; Keung, E.; Wargo, J.; et al. Autoimmune antibodies correlate with immune checkpoint therapy-induced toxicities. Proc. Natl. Acad. Sci. USA 2019, 116, 22246–22251. [Google Scholar] [CrossRef] [PubMed]
- Das, R.; Bar, N.; Ferreira, M.; Newman, A.M.; Zhang, L.; Bailur, J.K.; Bacchiocchi, A.; Kluger, H.; Wei, W.; Halaban, R.; et al. Early B cell changes predict autoimmunity following combination immune checkpoint blockade. J. Clin. Investig. 2018, 128, 715–720. [Google Scholar] [CrossRef] [Green Version]
- Kang, E.H.; Ha, Y.-J.; Lee, Y.J. Autoantibody Biomarkers in Rheumatic Diseases. Int. J. Mol. Sci. 2020, 21, 1382. [Google Scholar] [CrossRef] [Green Version]
- Pisetsky, D.S. Antinuclear antibodies in healthy people: The tip of autoimmunity’s iceberg? Arthritis Res. Ther. 2011, 13, 109. [Google Scholar] [CrossRef] [Green Version]
- Grygiel-Górniak, B.; Rogacka, N.; Puszczewicz, M. Antinuclear antibodies in healthy people and non-rheumatic diseases—Diagnostic and clinical implications. Reumatologia 2018, 56, 243–248. [Google Scholar] [CrossRef]
- Coureau, M.; Meert, A.-P.; Berghmans, T.; Grigoriu, B. Efficacy and Toxicity of Immune -Checkpoint Inhibitors in Patients With Preexisting Autoimmune Disorders. Front. Med. 2020, 7, 137. [Google Scholar] [CrossRef]
- Halle, B.R.; Warner, A.B.; Zaman, F.Y.; Haydon, A.; Bhave, P.; Dewan, A.K.; Ye, F.; Irlmeier, R.; Mehta, P.; Kurtansky, N.R.; et al. Immune checkpoint inhibitors in patients with pre-existing psoriasis: Safety and efficacy. J. Immunother. Cancer 2021, 9, e003066. [Google Scholar] [CrossRef]
- Gutzmer, R.; Koop, A.; Meier, F.; Hassel, J.C.; Terheyden, P.; Zimmer, L.; Heinzerling, L.; Ugurel, S.; Pföhler, C.; Gesierich, A.; et al. Programmed cell death protein-1 (PD-1) inhibitor therapy in patients with advanced melanoma and preexisting autoimmunity or ipilimumab-triggered autoimmunity. Eur. J. Cancer 2017, 75, 24–32. [Google Scholar] [CrossRef]
- Kennedy, L.C.; Bhatia, S.; Thompson, J.A.; Grivas, P. Preexisting Autoimmune Disease: Implications for Immune Checkpoint Inhibitor Therapy in Solid Tumors. J. Natl. Compr. Cancer Netw. 2019, 17, 750–757. [Google Scholar] [CrossRef]
- Bossuyt, X.; De Langhe, E.; Borghi, M.O.; Meroni, P.L. Understanding and interpreting antinuclear antibody tests in systemic rheumatic diseases. Nat. Rev. Rheumatol. 2020, 16, 715–726. [Google Scholar] [CrossRef] [PubMed]
- Kumar, Y.; Bhatia, A.; Minz, R.W. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases: A journey revisited. Diagn. Pathol. 2009, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sur, L.M.; Floca, E.; Sur, D.G.; Colceriu, M.C.; Samasca, G.; Sur, G. Antinuclear Antibodies: Marker of Diagnosis and Evolution in Autoimmune Diseases. Lab. Med. 2018, 49, 316–322. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.M.; Feltkamp, T.E.W.; Smolen, J.S.; Butcher, B.; Dawkins, R.; Fritzler, M.J.; Gordon, T.; Hardin, J.A.; Kalden, J.R.; Lahita, R.G.; et al. Range of antinuclear antibodies in ‘healthy’ individuals. Arthritis Rheum. 1997, 40, 1601–1611. [Google Scholar] [CrossRef] [PubMed]
- Mouri, A.; Kaira, K.; Yamaguchi, O.; Hashimoto, K.; Miura, Y.; Shiono, A.; Shinomiya, S.; Akagami, T.; Imai, H.; Kobayashi, K.; et al. Efficacy and Feasibility of Programmed Death-1/Programmed Death Ligand-1 Blockade Therapy in Non-Small Cell Lung Cancer Patients with High Antinuclear Antibody Titers. Front. Oncol. 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sakakida, T.; Ishikawa, T.; Chihara, Y.; Harita, S.; Uchino, J.; Tabuchi, Y.; Komori, S.; Asai, J.; Narukawa, T.; Arai, A.; et al. Safety and efficacy of PD1/PD-L1 blockade in patients with preexisasting antinuclear antibodies. Clin. Transl. Oncol. 2020, 22, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Barth, D.A.; Stanzer, S.; Spiegelberg, J.; Bauernhofer, T.; Absenger, G.; Posch, F.; Lipp, R.; Halm, M.; Szkandera, J.; Balic, M.; et al. Evaluation of autoantibodies as predictors of treatment response and immune-related adverse events during the treatment with immune checkpoint inhibitors: A prospective longitudinal pan-cancer study. Cancer Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Giannicola, R.; D’Arrigo, G.; Botta, C.; Agostino, R.; Del Medico, P.; Falzea, A.C.; Barbieri, V.; Staropoli, N.; Del Giudice, T.; Pastina, P.; et al. Early blood rise in auto-antibodies to nuclear and smooth muscle antigens is predictive of prolonged survival and autoimmunity in metastatic-non-small cell lung cancer patients treated with PD-1 immune-check point blockade by nivolumab. Mol. Clin. Oncol. 2019, 11, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Yoneshima, Y.; Tanaka, K.; Shiraishi, Y.; Hata, K.; Watanabe, H.; Harada, T.; Otsubo, K.; Iwama, E.; Inoue, H.; Masuda, S.; et al. Safety and efficacy of PD-1 inhibitors in non–small cell lung cancer patients positive for antinuclear antibodies. Lung Cancer 2019, 130, 5–9. [Google Scholar] [CrossRef]
- De Moel, E.C.; Rozeman, E.A.; Kapiteijn, E.H.; Verdegaal, E.M.E.; Grummels, A.; Bakker, J.A.; Huizinga, T.W.J.; Haanen, J.B.; Toes, R.E.M.; van Der Woude, D. Autoantibody Development under Treatment with Immune-Checkpoint Inhibitors. Cancer Immunol. Res. 2019, 7, 6–11. [Google Scholar] [CrossRef]
- Da Gama Duarte, J.; Parakh, S.; Andrews, M.C.; Woods, K.; Pasam, A.; Tutuka, C.; Ostrouska, S.; Blackburn, J.M.; Behren, A.; Cebon, J. Autoantibodies May Predict Immune-Related Toxicity: Results from a Phase I Study of Intralesional Bacillus Calmette–Guérin followed by Ipilimumab in Patients with Advanced Metastatic Melanoma. Front. Immunol. 2018, 9, 411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaenker, P.; Gray, E.; Ziman, M. Autoantibody Production in Cancer—The Humoral Immune Response toward Autologous Antigens in Cancer Patients. Autoimmun. Rev. 2016, 15, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauderon, A.; Roux-Lombard, P.; Spoerl, D. Antinuclear Antibodies With a Homogeneous and Speckled Immunofluorescence Pattern Are Associated With Lack of Cancer While Those With a Nucleolar Pattern With the Presence of Cancer. Front. Med. 2020, 7, 165. [Google Scholar] [CrossRef]
- Vlagea, A.; Falagan, S.; Gutiérrez-Gutiérrez, G.; Moreno-Rubio, J.; Merino, M.; Zambrana, F.; Casado, E.; Sereno, M. Antinuclear antibodies and cancer: A literature review. Crit. Rev. Oncol. 2018, 127, 42–49. [Google Scholar] [CrossRef]
- Gillissen, G.; Pusztai-Markos, Z. Cell mediated immune regulation in autoimmunity. Allergol. Immunopathol. 1979, 7, 153–168. [Google Scholar]
- Les, I.; Martínez, M.; Narro, A.; Pérez, I.; Sánchez, C.; Puntí, L.; Anaut, P.; Eguiluz, S.; Herrera, A.; Domínguez, S. Association of immune-related adverse events induced by nivolumab with a battery of autoantibodies. Ann. Med. 2021, 53, 762–769. [Google Scholar] [CrossRef]
- Toi, Y.; Sugawara, S.; Sugisaka, J.; Ono, H.; Kawashima, Y.; Aiba, T.; Kawana, S.; Saito, R.; Aso, M.; Tsurumi, K.; et al. Profiling Preexisting Antibodies in Patients Treated With Anti–PD-1 Therapy for Advanced Non–Small Cell Lung Cancer. JAMA Oncol. 2019, 5, 376–383. [Google Scholar] [CrossRef]
- Shafqat, H.; Gourdin, T.; Sion, A. Immune-related adverse events are linked with improved progression-free survival in patients receiving anti-PD-1/PD-L1 therapy. Semin. Oncol. 2018, 45, 156–163. [Google Scholar] [CrossRef]
- Ghosh, N.; Postow, M.; Zhu, C.; Jannat-Khah, D.; Li, Q.-Z.; Vitone, G.; Chan, K.K.; Bass, A.R. Lower baseline autoantibody levels are associated with immune-related adverse events from immune checkpoint inhibition. J. Immunother. Cancer 2022, 10, e004008. [Google Scholar] [CrossRef]
- Ghosh, N.; Chan, K.K.; Jivanelli, B.; Bass, A.R. Autoantibodies in Patients With Immune-Related Adverse Events from Checkpoint Inhibitors a Systematic Literature Review. J. Clin. Rheumatol. 2022, 28, 498–505. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE); U.S. Department of Health and Human Services: Atlanta, GA, USA, 2017.
- Damoiseaux, J.; Andrade, L.E.C.; Carballo, O.G.; Conrad, K.; Francescantonio, P.L.C.; Fritzler, M.J.; LA Torre, I.G.-D.; Herold, M.; Klotz, W.; Cruvinel, W.D.M.; et al. Clinical relevance of HEp-2 indirect immunofluorescent patterns: The International Consensus on ANA patterns (ICAP) perspective. Ann. Rheum. Dis. 2019, 78, 879–889. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ANA De Novo (n = 22) | ANA (n = 37) | Non-ANA (n = 75) | p | |
|---|---|---|---|---|
| Sex male, n (%) | 17 (77.3) | 22 (59.4) | 56 (74.7) | 0.19 |
| Age, median (IQR) | 65 (60–76) | 71 (63–74.5) | 67 (58–77) | 0.62 |
| Tumor type, n (%) | ||||
| NSCLC | 17 (77.3) | 27 (72.9) | 47 (62.7) | 0.32 |
| Melanoma | 2 (9.1) | 4 (10.8) | 14 (18.7) | 0.38 |
| Renal | 1 (4.5) | 4 (10.8) | 5 (6.7) | 0.62 |
| Head and Neck | 2 (9.1) | 0 (0) | 7 (9.3) | 0.15 |
| Urothelial | 0 (0) | 2 (5.4) | 2 (2.7) | 0.48 |
| ICI schedule, n (%) | ||||
| Anti PD-(L)1 in monotheraphy | 17 (77.3) | 29 (78.4) | 58 (77.3) | 0.99 |
| Nivolumab | 4 (18.2) | 4 (10.8) | 17 (22.7) | 0.31 |
| Pembrolizumab | 9 (40.9) | 10 (27) | 18 (24) | 0.29 |
| Atezolizumab | 1 (4.5) | 11 (29.7) | 12 (16) | 0.04 |
| Durvalumab | 3 (13.6) | 4 (10.8) | 6 (8) | 0.70 |
| Avelumab | 0 (0) | 0 (0) | 1 (1.3) | 0.67 |
| Retifanlimab | 0 (0) | 0 (0) | 4 (5.3) | 0.19 |
| Anti PD-(L)1 in combination with immunotherapy | 4 (18.2) | 5 (13.5) | 10 (13.3) | 0.84 |
| Anti-CTLA4 (Ipilimumab, Tremelimumab) | 0 (0) | 3 (8.1) | 5 (6.7) | 0.41 |
| Anti-LAG3 (Eftilagimod) | 3 (13.6) | 1 (2.7) | 4 (5.3) | 0.21 |
| Anti-NKG2A (Monalizumab) | 0 (0) | 1 (2.7) | 1 (1.3) | 0.69 |
| Anti-CD73 (Oclelumab) | 1 (4.5) | 0 (0) | 0 (0) | 0.07 |
| Anti PD-(L)1 in combination with chemotherapy | 1 (4.5) | 3 (8.1) | 7 (9.3) | 0.77 |
| Line of treatment, n (%) | ||||
| 1st line | 11 (50) | 17 (45.9) | 36 (48) | 0.95 |
| ≥2nd line | 7 (31.8) | 17 (45.9) | 33 (44) | 0.52 |
| Adjuvant | 1 (4.5) | 1 (2.7) | 3 (4) | 0.92 |
| Maintenance | 3 (13.6) | 2 (5.4) | 3 (4) | 0.24 |
| PD-L1 expression *, n (%) | ||||
| Negative (0–1%) | 2 (9.1) | 2 (5.4) | 8 (10.7) | 0.65 |
| Low (1–49%) | 2 (9.1) | 9 (24.3) | 12 (16) | 0.29 |
| High (≥50%) | 10 (45.5) | 9 (24.3) | 10 (13.3) | 0.005 |
| Patient | Sex | Age | Tumor | Treatment | Line of Treatment | Pre-Treatment ANA Patterns a (Titer) | Post-Treatment ANA Patterns a (Titer) | ANA Development (Days) | irAEs | Grade of Severity b | irAEs Onset b (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 60 | NSCLC | Pembrolizumab + Chemotherapy | Adjuvant | Negative | Cytoplasmic speckled (1:320) | 6 | Rash, pruritus, hepatotoxicity | 1, 1, 2 | 230, 230, 6 |
| 2 | M | 83 | NSCLC | Pembrolizumab | 1st | Negative | Nuclear speckled (1:160), Cytoplasmic fibrillar (1:160) | 41 | Hepatotoxicity | 3 | 41 |
| 3 | M | 58 | NSCLC | Pembrolizumab | 1st | Negative | Nuclear speckled (1:320), Cytoplasmic fibrillar (1:160), Intercellular Bridge (1:160) | 39 | Hypertiroidism | 1 | 60 |
| 4 | F | 63 | Melanoma | Pembrolizumab | 1st | Negative | Nuclear speckled (1:320) | 41 | Diabetes Mellitus | 1 | 41 |
| 5 | M | 67 | NSCLC | Pembrolizumab | 2nd | Negative | Nuclear speckled (1:640) | 18 | Hypophisitis, arthitis | 3, 2 | 259, 207 |
| 6 | F | 66 | NSCLC | Durvalumab | Maintenance | Negative | Cytoplasmic fibrillar (1:640), NuMa-like (1:640) | 113 | No | _ | _ |
| 7 | F | 73 | NSCLC | Pembrolizumab + Eftilagimod | 1st | Negative | Cytoplasmic dots (1:160) | 41 | No | _ | _ |
| 8 | M | 61 | NSCLC | Durvalumab | Maintenance | Negative | Nuclear speckled (1:160), Spindle fibers (1:160) | 35 | Pruritus, mucositis | 1,1 | 91, 11 |
| 9 | M | 62 | Neck and Head Carcinoma | Nivolumab | 3rd | Negative | Nuclear speckled (1:160) | 53 | No | _ | _ |
| 10 | M | 64 | NSCLC | Pembrolizumab | 1st | Negative | Nuclear speckled (1:160) | 70 | No | _ | _ |
| 11 | M | 76 | NSCLC | Durvalumab + Oleclumab | Maintenance | Negative | Cytoplasmic fibrillar (1:1280) | 27 | Pneumonitis | 3 | 55 |
| 12 | M | 39 | NSCLC | Durvalumab | 2nd | Negative | Cytoplasmic fibrillar (1:1280) | 53 | Pruritus | 1 | 9 |
| 13 | F | 64 | NSCLC | Atezolizumab | 3rd | Negative | Nuclear speckled (1:160) | 41 | Colitis | 3 | 108 |
| 14 | M | 76 | Renal Cancer | Nivolumab | 2nd | Negative | Cytoplasmic speckled (1:160) | 111 | No | _ | _ |
| 15 | M | 76 | NSCLC | Pembrolizumab | 2nd | Cytoplasmic speckled (1:320) | Cytoplasmic speckled (1:160), Rods & Rings (1:1280) | 49 | Pneumonitis, hepatotoxicity | 4,4 | 196, 196 |
| 16 | M | 60 | NSCLC | Pembrolizumab | 1st | Nuclear speckled (1:160) | Nuclear speckled (1:160), Nucleolar (1:160) | 126 | No | _ | _ |
| 17 | F | 84 | Melanoma | Nivolumab | 1st | Nuclear speckled (1:160) | Nuclear speckled (1:320), Cytoplasmic speckled (1:320) | 68 | Pruritus, hypothiroidism | 1,2 | 40, 83 |
| 18 | M | 78 | NSCLC | Pembrolizumab | 1st | Nuclear speckled (1:160) | Nuclear speckled (1:160), Nucleolar (1:160) | 121 | No | _ | _ |
| 19 | M | 60 | NSCLC | Nivolumab | 1st | Cytoplasmic reticular (1:640) | Cytoplasmic reticular (1:160), Nuclear speckled (1:320) | 118 | Hepatotoxicity | 3 | 167 |
| 20 | M | 59 | Neck and Head Carcinoma | Pembrolizumab | 2nd | PCNA-like (1:640), Nucleolar (1:640) | PCNA-like (1:640), Nucleolar (1:640), Intercellular bridge (1:320) | 167 | No | _ | _ |
| 21 | M | 73 | NSCLC | Pembrolizumab + Eftilagimod | 1st | Nuclear coarse speckled (1:640) | Nuclear fine dense speckled (1:320) | 43 | Rash, pruritus, colitis | 2, 1, 1 | 7, 7, 203 |
| 22 | M | 67 | NSCLC | Pembrolizumab + Eftilagimod | 1st | Nuclear speckled (1:320), Centromeric CENP-F-like (1:160) | Nuclear speckled (1:320), Centromeric CENP-F-like (1:160), Nucleolar (1:320) | 105 | Rash, pruritus, psoriasis | 2, 2, 2 | 33, 105, 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alserawan, L.; Anguera, G.; Zamora Atenza, C.; Serra López, J.; Martínez-Martínez, L.; Riudavets Melià, M.; Sullivan, I.; Barba Joaquin, A.; Majem Tarruella, M.; Vidal, S. Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events. Int. J. Mol. Sci. 2022, 23, 12641. https://doi.org/10.3390/ijms232012641
Alserawan L, Anguera G, Zamora Atenza C, Serra López J, Martínez-Martínez L, Riudavets Melià M, Sullivan I, Barba Joaquin A, Majem Tarruella M, Vidal S. Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events. International Journal of Molecular Sciences. 2022; 23(20):12641. https://doi.org/10.3390/ijms232012641
Chicago/Turabian StyleAlserawan, Leticia, Geòrgia Anguera, Carlos Zamora Atenza, Jorgina Serra López, Laura Martínez-Martínez, Mariona Riudavets Melià, Ivana Sullivan, Andrés Barba Joaquin, Margarita Majem Tarruella, and Silvia Vidal. 2022. "Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events" International Journal of Molecular Sciences 23, no. 20: 12641. https://doi.org/10.3390/ijms232012641
APA StyleAlserawan, L., Anguera, G., Zamora Atenza, C., Serra López, J., Martínez-Martínez, L., Riudavets Melià, M., Sullivan, I., Barba Joaquin, A., Majem Tarruella, M., & Vidal, S. (2022). Association between Changes in the Patterns of Antinuclear Autoantibodies during Immune Checkpoint Inhibition Therapy and the Development of Severe Immune Related Adverse Events. International Journal of Molecular Sciences, 23(20), 12641. https://doi.org/10.3390/ijms232012641