
An Emerging Strategy for Muscle Evanescent Trauma Discrimination by Spectroscopy and Chemometrics

Abstract
:1. Introduction
2. Results and Discussion
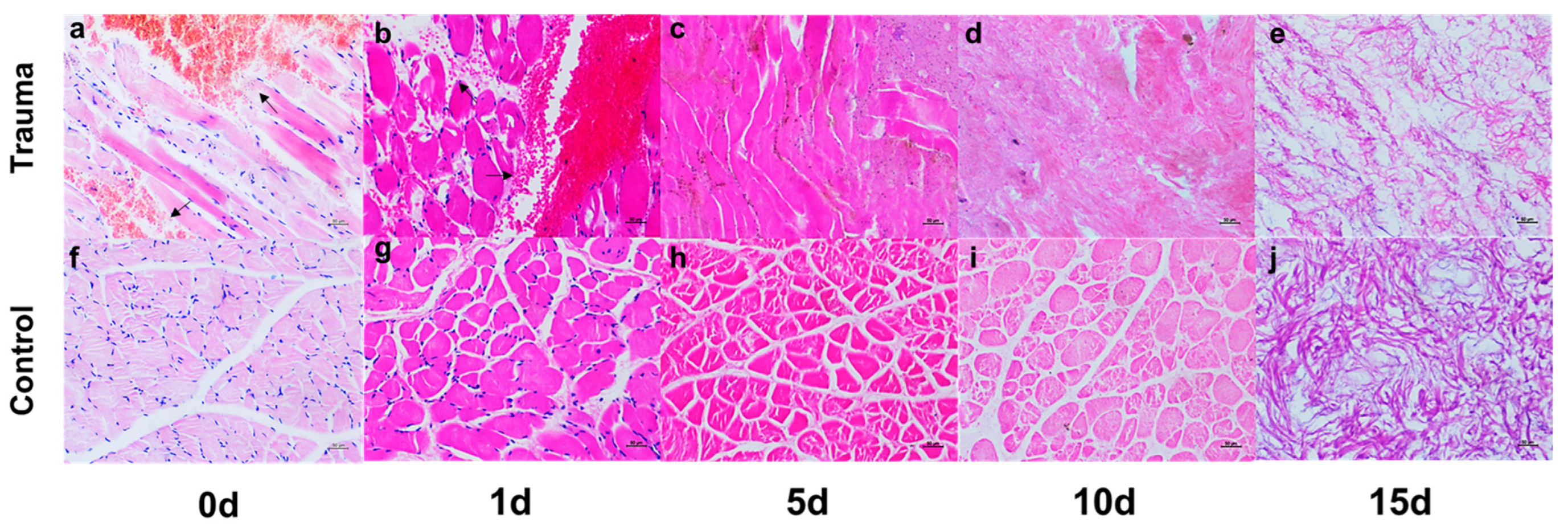
2.1. Macroscopic and Microscopic Visualization
2.2. Spectral Characteristic Peaks and Changes in Time Sequence
2.3. Classification Model of Rat Muscle Trauma Based on ATR-FTIR
2.4. Classification Model of Human Muscle Trauma Based on Micro-IR
3. Materials and Methods
3.1. Animal Model Establishment and Sample Preparation
3.2. Spectral Collection and Data Preprocessing
3.3. Multivariable Statistical Analysis and Software
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Messerer, D.A.C.; Halbgebauer, R.; Nilsson, B.; Pavenstädt, H.; Radermacher, P.; Huber-Lang, M. Immunopathophysiology of trauma-related acute kidney injury. Nat. Rev. Nephrol. 2021, 17, 91–111. [Google Scholar] [CrossRef]
- Grewal, H.S.; Dangayach, N.S.; Ahmad, U.; Ghosh, S.; Gildea, T.; Mehta, A.C. Treatment of Tracheobronchial Injuries: A Contemporary Review. Chest 2019, 155, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Simmons, J.W.; Powell, M.F. Acute traumatic coagulopathy: Pathophysiology and resuscitation. Br. J. Anaesth. 2016, 117 (Suppl. 3), iii31–iii43. [Google Scholar] [CrossRef] [Green Version]
- Stein, P.; Kaserer, A.; Sprengel, K.; Wanner, G.A.; Seifert, B.; Theusinger, O.M.; Spahn, D.R. Change of transfusion and treatment paradigm in major trauma patients. Anaesthesia 2017, 72, 1317–1326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempsey, N.; Blau, S. Evaluating the evidentiary value of the analysis of skeletal trauma in forensic research: A review of research and practice. Forensic Sci. Int. 2020, 307, 110140. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Oramary, D.; Kamin, K.; Buschmann, C.T.; Kleber, C. Synergistic Effects of Forensic Medicine and Traumatology: Comparison of Clinical Diagnosis Autopsy Findings in Trauma-Related Deaths. World J. Surg. 2020, 44, 1137–1148. [Google Scholar] [CrossRef] [Green Version]
- Leal, L.B.; Nogueira, M.S.; Canevari, R.A.; Carvalho, L.F.C.S. Vibration spectroscopy and body biofluids: Literature review for clinical applications. Photodiagnosis Photodyn. Ther. 2018, 24, 237–244. [Google Scholar] [CrossRef]
- Takamura, A.; Ozawa, T. Recent advances of vibrational spectroscopy and chemometrics for forensic biological analysis. Analyst 2021, 146, 7431–7449. [Google Scholar] [CrossRef]
- Lopes, J.; Correia, M.; Martins, I.; Henriques, A.G.; Delgadillo, I.; da Cruz ESilva, O.; Nunes, A. FTIR and Raman Spectroscopy Applied to Dementia Diagnosis Through Analysis of Biological Fluids. J. Alzheimers Dis. 2016, 52, 801–812. [Google Scholar] [CrossRef]
- Kumar, R.; Sharma, K.; Sharma, V. Bloodstain age estimation through infrared spectroscopy and Chemometric models. Sci. Justice 2020, 60, 538–546. [Google Scholar] [CrossRef]
- Lin, H.; Zhang, Y.; Wang, Q.; Li, B.; Huang, P.; Wang, Z. Estimation of the age of human bloodstains under the simulated indoor and outdoor crime scene conditions by ATR-FTIR spectroscopy. Sci. Rep. 2017, 7, 13254. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Chophi, R.; Jossan, J.K.; Singh, R. Detection of bloodstains using attenuated total reflectance-Fourier transform infrared spectroscopy supported with PCA and PCA-LDA. Med. Sci. Law 2021, 61, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Cai, W.; Wu, H.; Yang, C.; Yu, K.; Liu, R.; Wei, X.; Lin, H.; Sun, Q.; Wang, Z. Identification of human and non-human bloodstains on rough carriers based on ATR-FTIR and chemometrics. Microchem. J. 2022, 180, 107620. [Google Scholar] [CrossRef]
- Mistek-Morabito, E.; Lednev, I.K. Discrimination of menstrual and peripheral blood traces using attenuated total reflection Fourier transform-infrared (ATR FT-IR) spectroscopy and chemometrics for forensic purposes. Anal. Bioanal. Chem. 2021, 413, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- Das, T.; Harshey, A.; Srivastava, A.; Nigam, K.; Yadav, V.K.; Sharma, K.; Sharma, A. Analysis of the ex-vivo transformation of semen, saliva and urine as they dry out using ATR-FTIR spectroscopy and chemometric approach. Sci. Rep. 2021, 11, 11855. [Google Scholar] [CrossRef]
- Wei, X.; Yu, K.; Wu, D.; Huang, P.; Sun, Q.; Wang, Z. Species identification of semen stains by ATR-FTIR spectroscopy. Int. J. Legal Med. 2021, 135, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Orphanou, C.M.; Walton-Williams, L.; Mountain, H.; Cassella, J. The detection and discrimination of human body fluids using ATR FT-IR spectroscopy. Forensic Sci. Int. 2015, 252, e10–e16. [Google Scholar] [CrossRef]
- Wu, D.; Luo, Y.W.; Zhang, J.; Luo, B.; Zhang, K.; Yu, K.; Liu, R.N.; Lin, H.C.; Wei, X.; Wang, Z.Y.; et al. Fourier-transform infrared microspectroscopy of pulmonary edema fluid for postmortem diagnosis of diabetic ketoacidosis. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 258, 119882. [Google Scholar] [CrossRef]
- Lin, H.; Luo, Y.; Sun, Q.; Zhang, J.; Tuo, Y.; Zhang, Z.; Wang, L.; Deng, K.; Chen, Y.; Huang, P.; et al. Identification of Pulmonary Edema in Forensic Autopsy Cases of Sudden Cardiac Death Using Fourier Transform Infrared Microspectroscopy: A Pilot Study. Anal. Chem. 2018, 90, 2708–2715. [Google Scholar] [CrossRef]
- Lin, H.; Guo, X.; Luo, Y.; Chen, Y.; Zhao, R.; Guan, D.; Wang, Z.; Huang, P. Postmortem Diagnosis of Fatal Hypothermia by Fourier Transform Infrared Spectroscopic Analysis of Edema Fluid in Formalin-Fixed, Paraffin-Embedded Lung Tissues. J. Forensic Sci. 2020, 65, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Cuazitl, A.; Vazquez-Zapien, G.J.; Sanchez-Brito, M.; Limon-Pacheco, J.H.; Guerrero-Ruiz, M.; Garibay-Gonzalez, F.; Delgado-Macuil, R.J.; de Jesus, M.G.G.; Corona-Perezgrovas, M.A.; Pereyra-Talamantes, A.; et al. ATR-FTIR spectrum analysis of saliva samples from COVID-19 positive patients. Sci. Rep. 2021, 11, 19980. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, S.; Yadav, D.K.; Rawal, R. Saliva based noninvasive screening of Oral Submucous Fibrosis using ATR-FTIR spectroscopy. J. Pharm. Biomed. Anal. 2021, 203, 114202. [Google Scholar] [CrossRef] [PubMed]
- Bel’skaya, L.V.; Sarf, E.A.; Solomatin, D.V. Age and Gender Characteristics of the Infrared Spectra of Normal Human Saliva. Appl. Spectrosc. 2020, 74, 536–543. [Google Scholar] [CrossRef]
- Cai, W.; Wang, G.; Wu, H.; Li, H.; Shen, C.; Wei, X.; Yu, K.; Sun, Q.; Wang, Z. Identifying traumatic brain injury (TBI) by ATR-FTIR spectroscopy in a mouse model. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2022, 274, 121099. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, A.; Liu, R.; Zhang, H.; Lin, H.; Zhang, P.; Huang, P.; Wang, Z. Identifying muscle hemorrhage in rat cadavers with advanced decomposition by FT-IR microspectroscopy combined with chemometrics. Leg. Med. 2020, 47, 101748. [Google Scholar] [CrossRef] [PubMed]
- Mabwa, D.; Gajjar, K.; Furniss, D.; Schiemer, R.; Crane, R.; Fallaize, C.; Martin-Hirsch, P.L.; Martin, F.L.; Kypraios, T.; Seddon, A.B.; et al. Mid-infrared spectral classification of endometrial cancer compared to benign controls in serum or plasma samples. Analyst 2021, 146, 5631–5642. [Google Scholar] [CrossRef] [PubMed]
- Morais, C.L.M.; Lima, K.M.G.; Singh, M.; Martin, F.L. Tutorial: Multivariate classification for vibrational spectroscopy in biological samples. Nat. Protoc. 2020, 15, 2143–2162. [Google Scholar] [CrossRef]
- Rutledge, D.N. Comparison of principal components analysis, independent components analysis and common components analysis. J. Anal. Test. 2018, 2, 235–248. [Google Scholar] [CrossRef]
- Ballabio, D.; Consonni, V. Classification tools in chemistry. Part 1: Linear models. PLS-DA. Anal. Methods 2013, 5, 3790–3798. [Google Scholar] [CrossRef]
- Westerhuis, J.A.; Hoefsloot, H.C.J.; Smit, S.; Vis, D.J.; Smilde, A.K.; van Velzen, E.J.J.; van Duijnhoven, J.P.M.; van Dorsten, F.A. Assessment of PLS-DA cross validation. Metabolomics 2008, 4, 81–89. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wavenumber (cm−1) | Assignment |
|---|---|
| ~1011–1009 | Stretch C-O, carbohydrates |
| ~1100–1040 | Stretch P=O symmetric of the >PO2− groups of nucleic acids, phospholipids |
| ~1201 | PO2− asymmetric, phosphate I |
| ~1239–1238 | Asymmetric PO2− stretching |
| ~1243 | ν(PO2−) asymmetric stretching of phosphodiesters |
| ~1338–1337 | CH2 wagging |
| ~1402 | Symmetric CH3 bending modes of the methyl groups of proteins |
| ~1449 | Asymmetric CH3 bending of the methyl groups of proteins |
| ~1467–1465 | CH2 scissoring mode of the acyl chain of lipid, cholesterol-methyl band |
| ~1570–1510 | Amide II |
| ~1695–1620 | Amide Ⅰ |
| ~1714 | C=O thymine |
| ~1739–1738 | ν(C=O), polysaccharides, hemicellulose |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, G.; Wu, H.; Yang, C.; Li, Z.; Chen, R.; Liang, X.; Yu, K.; Li, H.; Shen, C.; Liu, R.; et al. An Emerging Strategy for Muscle Evanescent Trauma Discrimination by Spectroscopy and Chemometrics. Int. J. Mol. Sci. 2022, 23, 13489. https://doi.org/10.3390/ijms232113489
Wang G, Wu H, Yang C, Li Z, Chen R, Liang X, Yu K, Li H, Shen C, Liu R, et al. An Emerging Strategy for Muscle Evanescent Trauma Discrimination by Spectroscopy and Chemometrics. International Journal of Molecular Sciences. 2022; 23(21):13489. https://doi.org/10.3390/ijms232113489
Chicago/Turabian StyleWang, Gongji, Hao Wu, Canyu Yang, Zefeng Li, Run Chen, Xinggong Liang, Kai Yu, Huiyu Li, Chen Shen, Ruina Liu, and et al. 2022. "An Emerging Strategy for Muscle Evanescent Trauma Discrimination by Spectroscopy and Chemometrics" International Journal of Molecular Sciences 23, no. 21: 13489. https://doi.org/10.3390/ijms232113489
APA StyleWang, G., Wu, H., Yang, C., Li, Z., Chen, R., Liang, X., Yu, K., Li, H., Shen, C., Liu, R., Wei, X., Sun, Q., Zhang, K., & Wang, Z. (2022). An Emerging Strategy for Muscle Evanescent Trauma Discrimination by Spectroscopy and Chemometrics. International Journal of Molecular Sciences, 23(21), 13489. https://doi.org/10.3390/ijms232113489