

Probiotics and Commensal Gut Microbiota as the Effective Alternative Therapy for Multiple Sclerosis Patients Treatment


Abstract
:1. Introduction
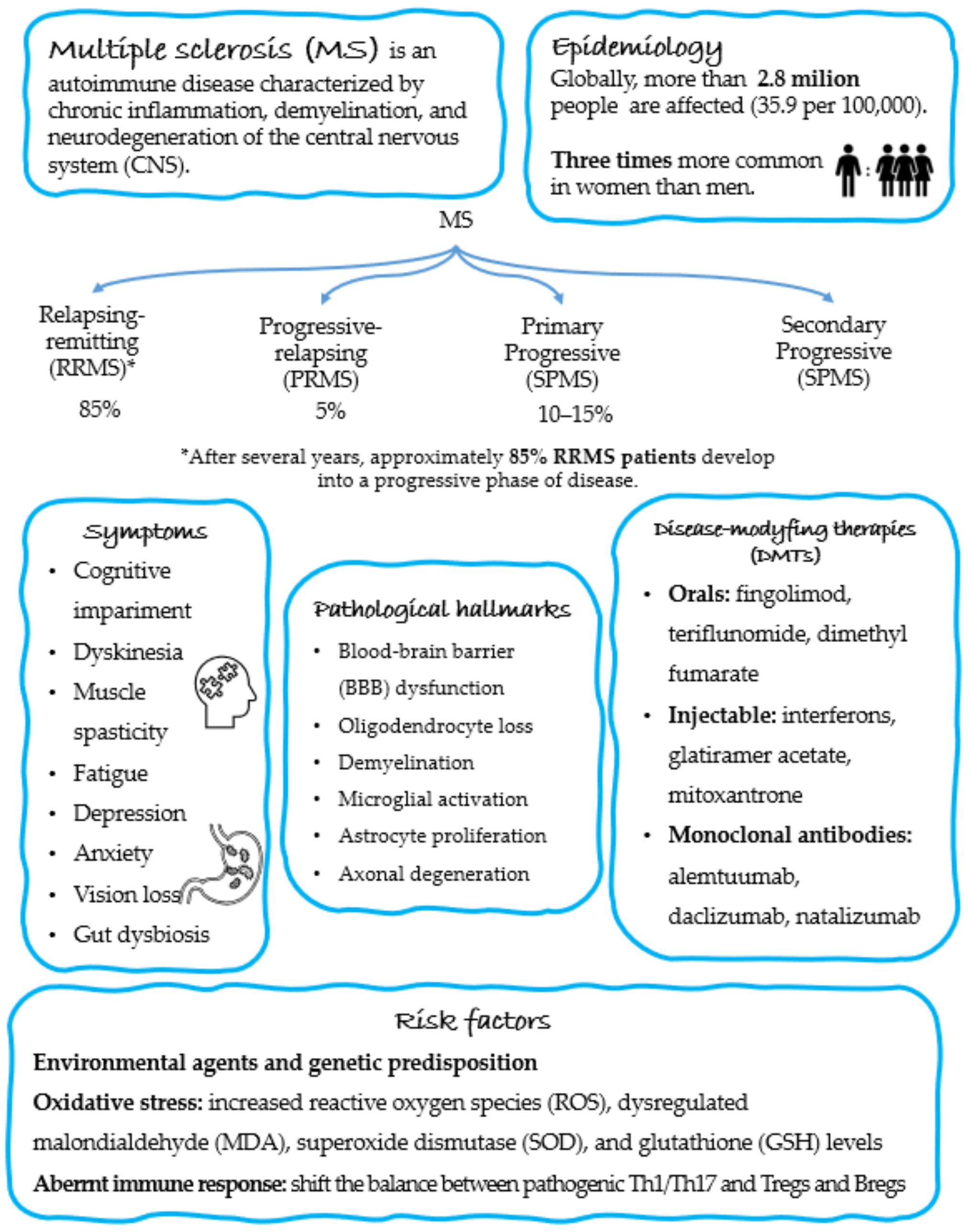
2. Epidemiology and Pathogenesis of MS
3. Gut Dysbiosis in MS
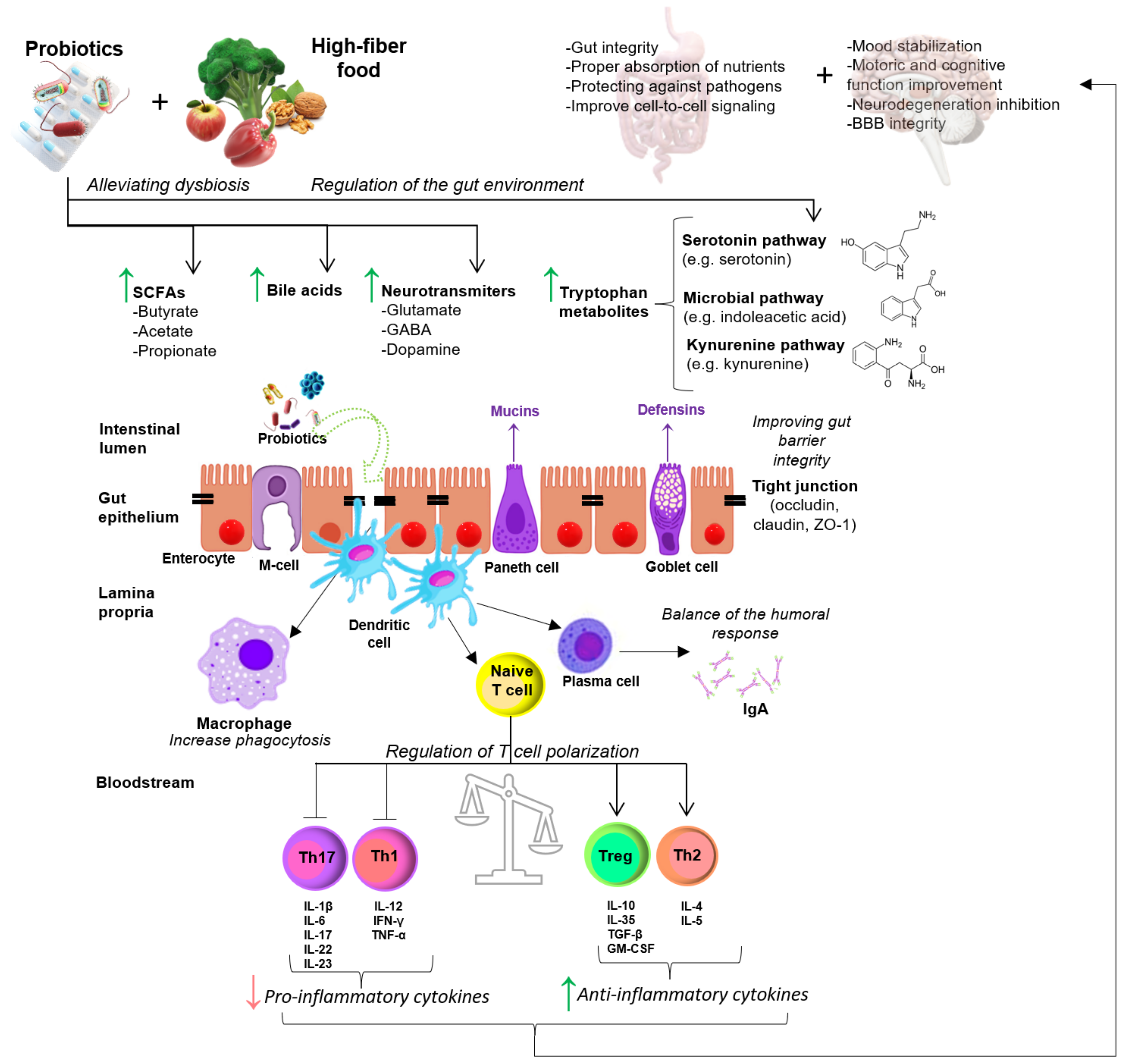
4. Effect of Probiotic Supplementation on EAE/MS
4.1. Animal Studies
4.2. Human Studies
5. Concluding Remarks and Future Perspectives
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Turnbaugh, P.J.; Ley, R.E.; Hamady, M.; Fraser-Liggett, C.M.; Knight, R.; Gordon, J.I. The Human Microbiome Project. Nature 2007, 449, 804–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gill, S.R.; Pop, M.; Deboy, R.T.; Eckburg, P.B.; Turnbaugh, P.J.; Samuel, B.S.; Gordon, J.I.; Relman, D.A.; Fraser-Liggett, C.M.; Nelson, K.E. Metagenomic analysis of the human distal gut microbiome. Science 2006, 312, 1355–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Human Microbiome Project Consortium. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Jia, H.; Cai, X.; Zhong, H.; Feng, Q.; Sunagawa, S.; Arumugam, M.; Kultima, J.R.; Prifti, E.; Nielsen, T.; et al. An integrated catalog of reference genes in the human gut microbiome. Nat. Biotechnol. 2014, 32, 834–841. [Google Scholar] [CrossRef]
- Qin, J.; Li, R.; Raes, J.; Arumugam, M.; Burgdorf, K.S.; Manichanh, C.; Nielsen, T.; Pons, N.; Levenez, F.; Yamada, T.; et al. A human gut microbial gene catalogue established by metagenomic sequencing. Nature 2010, 464, 59–65. [Google Scholar] [CrossRef] [Green Version]
- Nelson, K.E.; Weinstock, G.M.; Highlander, S.K.; Worley, K.C.; Creasy, H.H.; Wortman, J.R.; Rusch, D.B.; Mitreva, M.; Sodergren, E.; Chinwalla, A.T.; et al. A catalog of reference genomes from the human microbiome. Science 2010, 328, 994–999. [Google Scholar] [CrossRef] [Green Version]
- Arumugam, M.; Raes, J.; Pelletier, E.; Le Paslier, D.; Yamada, T.; Mende, D.R.; Fernandes, G.R.; Tap, J.; Bruls, T.; Batto, J.M.; et al. Enterotypes of the human gut microbiome. Nature 2011, 473, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Pandey, K.R.; Naik, S.R.; Vakil, B.V. Probiotics, prebiotics and synbiotics—A review. J. Food Sci. Technol. 2015, 52, 7577–7587. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Alookaran, J.J.; Rhoads, J.M. Probiotics in Autoimmune and Inflammatory Disorders. Nutrients 2018, 10, 1537. [Google Scholar] [CrossRef] [Green Version]
- Giri, P.; Shah, F.; Dwivedi, M. Probiotics and Prebiotics in the Suppression of Autoimmune Diseases; Academic Press: Cambridge, MA, USA, 2022; pp. 161–186. [Google Scholar]
- Yousefi, B.; Eslami, M.; Ghasemian, A.; Kokhaei, P.; Sadeghnejad, A. Probiotics can really cure an autoimmune disease? Gene Rep. 2019, 15, 100364. [Google Scholar] [CrossRef]
- Wang, Y.; Jiang, Y.; Deng, Y.; Yi, C.; Ding, M.; Liu, J.; Jin, X.; Shen, L.; He, Y.; Wu, X.; et al. Probiotic Supplements: Hope or Hype? Front Microbiol. 2020, 11, 160. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Syed, Y.A.; Khan, M.R. Understanding the Role of the Gut Microbiome in Brain Development and Its Association with Neurodevelopmental Psychiatric Disorders. Front. Cell Dev. Biol. 2022, 10, 880544. [Google Scholar] [CrossRef]
- Kim, C.S.; Cha, L.; Sim, M.; Jung, S.; Chun, W.Y.; Baik, H.W.; Shin, D.M. Probiotic Supplementation Improves Cognitive Function and Mood with Changes in Gut Microbiota in Community-Dwelling Older Adults: A Randomized, Double-Blind, Placebo-Controlled, Multicenter Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2021, 76, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Dinan, T.G.; Stanton, C.; Cryan, J.F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry 2013, 74, 720–726. [Google Scholar] [CrossRef]
- Tran, S.M.; Mohajeri, M.H. The Role of Gut Bacterial Metabolites in Brain Development, Aging and Disease. Nutrients 2021, 13, 732. [Google Scholar] [CrossRef]
- Zhou, L.; Foster, J.A. Psychobiotics and the gut-brain axis: In the pursuit of happiness. Neuropsychiatr. Dis. Treat. 2015, 11, 715–723. [Google Scholar] [CrossRef] [Green Version]
- Magalhães-Guedes, K.T. Psychobiotic Therapy: Method to Reinforce the Immune System. Clin. Psychopharmacol. Neurosci. 2022, 20, 17–25. [Google Scholar] [CrossRef]
- Carabotti, M.; Scirocco, A.; Maselli, M.A.; Severi, C. The gut-brain axis: Interactions between enteric microbiota, central and enteric nervous systems. Ann. Gastroenterol. 2015, 28, 203–209. [Google Scholar]
- Skonieczna-Żydecka, K.; Marlicz, W.; Misera, A.; Koulaouzidis, A.; Łoniewski, I. Microbiome-The Missing Link in the Gut-Brain Axis: Focus on Its Role in Gastrointestinal and Mental Health. J. Clin. Med. 2018, 7, 521. [Google Scholar] [CrossRef] [Green Version]
- Morais, L.H.; Schreiber, H.L.T.; Mazmanian, S.K. The gut microbiota-brain axis in behaviour and brain disorders. Nat. Rev. Microbiol. 2021, 19, 241–255. [Google Scholar] [CrossRef]
- Breit, S.; Kupferberg, A.; Rogler, G.; Hasler, G. Vagus Nerve as Modulator of the Brain-Gut Axis in Psychiatric and Inflammatory Disorders. Front. Psychiatry 2018, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Toledo, A.R.; Monroy, G.R.; Salazar, F.E.; Lee, J.-Y.; Jain, S.; Yadav, H.; Borlongan, C.V. Gut–Brain Axis as a Pathological and Therapeutic Target for Neurodegenerative Disorders. Int. J. Mol. Sci. 2022, 23, 1184. [Google Scholar] [CrossRef] [PubMed]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids from Gut Microbiota in Gut-Brain Communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Noto, D.; Hoshino, Y.; Mizuno, M.; Miyake, S. Butyrate suppresses demyelination and enhances remyelination. J. Neuroinflamm. 2019, 16, 165. [Google Scholar] [CrossRef] [Green Version]
- Codagnone, M.G.; Spichak, S.; O’Mahony, S.M.; O’Leary, O.F.; Clarke, G.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Programming Bugs: Microbiota and the Developmental Origins of Brain Health and Disease. Biol. Psychiatry 2019, 85, 150–163. [Google Scholar] [CrossRef]
- Wang, Y.; Kasper, L.H. The role of microbiome in central nervous system disorders. Brain Behav. Immun. 2014, 38, 1–12. [Google Scholar] [CrossRef] [Green Version]
- O’Sullivan, E.; Barrett, E.; Grenham, S.; Fitzgerald, P.; Stanton, C.; Ross, R.P.; Quigley, E.M.; Cryan, J.F.; Dinan, T.G. BDNF expression in the hippocampus of maternally separated rats: Does Bifidobacterium breve 6330 alter BDNF levels? Benef. Microbes 2011, 2, 199–207. [Google Scholar] [CrossRef]
- Bercik, P.; Park, A.J.; Sinclair, D.; Khoshdel, A.; Lu, J.; Huang, X.; Deng, Y.; Blennerhassett, P.A.; Fahnestock, M.; Moine, D.; et al. The anxiolytic effect of Bifidobacterium longum NCC3001 involves vagal pathways for gut-brain communication. Neurogastroenterol. Motil. 2011, 23, 1132–1139. [Google Scholar] [CrossRef] [Green Version]
- Bravo, J.A.; Forsythe, P.; Chew, M.V.; Escaravage, E.; Savignac, H.M.; Dinan, T.G.; Bienenstock, J.; Cryan, J.F. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc. Natl. Acad. Sci. USA 2011, 108, 16050–16055. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.W.; Liu, W.H.; Wu, C.C.; Juan, Y.C.; Wu, Y.C.; Tsai, H.P.; Wang, S.; Tsai, Y.C. Psychotropic effects of Lactobacillus plantarum PS128 in early life-stressed and naïve adult mice. Brain Res. 2016, 1631, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.H.; Chuang, H.L.; Huang, Y.T.; Wu, C.C.; Chou, G.T.; Wang, S.; Tsai, Y.C. Alteration of behavior and monoamine levels attributable to Lactobacillus plantarum PS128 in germ-free mice. Behav. Brain Res. 2016, 298, 202–209. [Google Scholar] [CrossRef]
- Erny, D.; Hrabě de Angelis, A.L.; Jaitin, D.; Wieghofer, P.; Staszewski, O.; David, E.; Keren-Shaul, H.; Mahlakoiv, T.; Jakobshagen, K.; Buch, T.; et al. Host microbiota constantly control maturation and function of microglia in the CNS. Nat. Neurosci. 2015, 18, 965–977. [Google Scholar] [CrossRef]
- Sarubbo, F.; Cavallucci, V.; Pani, G. The Influence of Gut Microbiota on Neurogenesis: Evidence and Hopes. Cells 2022, 11, 382. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Golden, L.C.; Voskuhl, R. The importance of studying sex differences in disease: The example of multiple sclerosis. J. Neurosci. Res. 2017, 95, 633–643. [Google Scholar] [CrossRef] [Green Version]
- Cree, B.A.C.; Arnold, D.L.; Chataway, J.; Chitnis, T.; Fox, R.J.; Pozo Ramajo, A.; Murphy, N.; Lassmann, H. Secondary Progressive Multiple Sclerosis: New Insights. Neurology 2021, 97, 378–388. [Google Scholar] [CrossRef]
- Silveira, C.; Guedes, R.; Maia, D.; Curral, R.; Coelho, R. Neuropsychiatric Symptoms of Multiple Sclerosis: State of the Art. Psychiatry Investig. 2019, 16, 877–888. [Google Scholar] [CrossRef]
- Ruggieri, S.; Petracca, M.; De Giglio, L.; De Luca, F.; Giannì, C.; Gurreri, F.; Petsas, N.; Tommasin, S.; Pozzilli, C.; Pantano, P. A matter of atrophy: Differential impact of brain and spine damage on disability worsening in multiple sclerosis. J. Neurol. 2021, 268, 4698–4706. [Google Scholar] [CrossRef]
- Gelfand, J.M. Multiple sclerosis: Diagnosis, differential diagnosis, and clinical presentation. Handb. Clin. Neurol. 2014, 122, 269–290. [Google Scholar] [CrossRef]
- Pucak, M.L.; Carroll, K.A.; Kerr, D.A.; Kaplin, A.I. Neuropsychiatric manifestations of depression in multiple sclerosis: Neuroinflammatory, neuroendocrine, and neurotrophic mechanisms in the pathogenesis of immune-mediated depression. Dialogues Clin. Neurosci. 2007, 9, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.D.; Motl, R.; Sandroff, B.M. Depression in multiple sclerosis: Is one approach for its management enough? Mult. Scler. Relat. Disord. 2021, 51, 102904. [Google Scholar] [CrossRef] [PubMed]
- Moore, S. Major depression and multiple sclerosis—A case report. J. Med. Life 2013, 6, 290–291. [Google Scholar] [PubMed]
- Claflin, S.B.; Broadley, S.; Taylor, B.V. The Effect of Disease Modifying Therapies on Disability Progression in Multiple Sclerosis: A Systematic Overview of Meta-Analyses. Front. Neurol. 2018, 9, 1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baecher-Allan, C.; Kaskow, B.J.; Weiner, H.L. Multiple Sclerosis: Mechanisms and Immunotherapy. Neuron 2018, 97, 742–768. [Google Scholar] [CrossRef] [Green Version]
- Chastain, E.M.; Miller, S.D. Molecular mimicry as an inducing trigger for CNS autoimmune demyelinating disease. Immunol. Rev. 2012, 245, 227–238. [Google Scholar] [CrossRef]
- Schreibelt, G.; van Horssen, J.; van Rossum, S.; Dijkstra, C.D.; Drukarch, B.; de Vries, H.E. Therapeutic potential and biological role of endogenous antioxidant enzymes in multiple sclerosis pathology. Brain Res. Rev. 2007, 56, 322–330. [Google Scholar] [CrossRef]
- Acar, G.; Idiman, F.; Idiman, E.; Kirkali, G.; Cakmakçi, H.; Ozakbaş, S. Nitric oxide as an activity marker in multiple sclerosis. J. Neurol. 2003, 250, 588–592. [Google Scholar] [CrossRef]
- Ghonimi, N.A.M.; Elsharkawi, K.A.; Khyal, D.S.M.; Abdelghani, A.A. Serum malondialdehyde as a lipid peroxidation marker in multiple sclerosis patients and its relation to disease characteristics. Mult. Scler. Relat. Disord. 2021, 51, 102941. [Google Scholar] [CrossRef]
- Obradovic, D.; Andjelic, T.; Ninkovic, M.; Dejanovic, B.; Kotur-Stevuljevic, J. Superoxide dismutase (SOD), advanced oxidation protein products (AOPP), and disease-modifying treatment are related to better relapse recovery after corticosteroid treatment in multiple sclerosis. Neurol. Sci. 2021, 42, 3241–3247. [Google Scholar] [CrossRef]
- Choi, I.Y.; Lee, S.P.; Denney, D.R.; Lynch, S.G. Lower levels of glutathione in the brains of secondary progressive multiple sclerosis patients measured by 1H magnetic resonance chemical shift imaging at 3 T. Mult. Scler. 2011, 17, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Dendrou, C.A.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.M.; Lalor, S.J.; Sweeney, C.M.; Tubridy, N.; Mills, K.H. T cells in multiple sclerosis and experimental autoimmune encephalomyelitis. Clin. Exp. Immunol. 2010, 162, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hirota, K.; Duarte, J.H.; Veldhoen, M.; Hornsby, E.; Li, Y.; Cua, D.J.; Ahlfors, H.; Wilhelm, C.; Tolaini, M.; Menzel, U.; et al. Fate mapping of IL-17-producing T cells in inflammatory responses. Nat. Immunol. 2011, 12, 255–263. [Google Scholar] [CrossRef]
- El-Behi, M.; Ciric, B.; Dai, H.; Yan, Y.; Cullimore, M.; Safavi, F.; Zhang, G.X.; Dittel, B.N.; Rostami, A. The encephalitogenicity of T(H)17 cells is dependent on IL-1- and IL-23-induced production of the cytokine GM-CSF. Nat. Immunol. 2011, 12, 568–575. [Google Scholar] [CrossRef] [Green Version]
- Constantinescu, C.S.; Farooqi, N.; O’Brien, K.; Gran, B. Experimental autoimmune encephalomyelitis (EAE) as a model for multiple sclerosis (MS). Br. J. Pharmacol. 2011, 164, 1079–1106. [Google Scholar] [CrossRef] [Green Version]
- Monney, L.; Sabatos, C.A.; Gaglia, J.L.; Ryu, A.; Waldner, H.; Chernova, T.; Manning, S.; Greenfield, E.A.; Coyle, A.J.; Sobel, R.A.; et al. Th1-specific cell surface protein Tim-3 regulates macrophage activation and severity of an autoimmune disease. Nature 2002, 415, 536–541. [Google Scholar] [CrossRef]
- Cua, D.J.; Sherlock, J.; Chen, Y.; Murphy, C.A.; Joyce, B.; Seymour, B.; Lucian, L.; To, W.; Kwan, S.; Churakova, T.; et al. Interleukin-23 rather than interleukin-12 is the critical cytokine for autoimmune inflammation of the brain. Nature 2003, 421, 744–748. [Google Scholar] [CrossRef]
- Jäger, A.; Dardalhon, V.; Sobel, R.A.; Bettelli, E.; Kuchroo, V.K. Th1, Th17, and Th9 effector cells induce experimental autoimmune encephalomyelitis with different pathological phenotypes. J. Immunol. 2009, 183, 7169–7177. [Google Scholar] [CrossRef] [Green Version]
- Komiyama, Y.; Nakae, S.; Matsuki, T.; Nambu, A.; Ishigame, H.; Kakuta, S.; Sudo, K.; Iwakura, Y. IL-17 Plays an Important Role in the Development of Experimental Autoimmune Encephalomyelitis. J. Immunol. 2006, 177, 566. [Google Scholar] [CrossRef] [Green Version]
- Zozulya, A.L.; Wiendl, H. The role of regulatory T cells in multiple sclerosis. Nat. Clin. Pract. Neurol. 2008, 4, 384–398. [Google Scholar] [CrossRef]
- Kleinewietfeld, M.; Hafler, D.A. Regulatory T cells in autoimmune neuroinflammation. Immunol. Rev. 2014, 259, 231–244. [Google Scholar] [CrossRef]
- Chen, J.; Chia, N.; Kalari, K.R.; Yao, J.Z.; Novotna, M.; Paz Soldan, M.M.; Luckey, D.H.; Marietta, E.V.; Jeraldo, P.R.; Chen, X.; et al. Multiple sclerosis patients have a distinct gut microbiota compared to healthy controls. Sci. Rep. 2016, 6, 28484. [Google Scholar] [CrossRef] [Green Version]
- Tremlett, H.; Fadrosh, D.W.; Faruqi, A.A.; Zhu, F.; Hart, J.; Roalstad, S.; Graves, J.; Lynch, S.; Waubant, E. Gut microbiota in early pediatric multiple sclerosis: A case-control study. Eur. J. Neurol. 2016, 23, 1308–1321. [Google Scholar] [CrossRef] [Green Version]
- Miyake, S.; Kim, S.; Suda, W.; Oshima, K.; Nakamura, M.; Matsuoka, T.; Chihara, N.; Tomita, A.; Sato, W.; Kim, S.W.; et al. Dysbiosis in the Gut Microbiota of Patients with Multiple Sclerosis, with a Striking Depletion of Species Belonging to Clostridia XIVa and IV Clusters. PLoS ONE 2015, 10, e0137429. [Google Scholar] [CrossRef] [Green Version]
- Bhargava, P.; Smith, M.D.; Mische, L.; Harrington, E.; Fitzgerald, K.C.; Martin, K.; Kim, S.; Reyes, A.A.; Gonzalez-Cardona, J.; Volsko, C.; et al. Bile acid metabolism is altered in multiple sclerosis and supplementation ameliorates neuroinflammation. J. Clin. Invest. 2020, 130, 3467–3482. [Google Scholar] [CrossRef] [Green Version]
- Duscha, A.; Gisevius, B.; Hirschberg, S.; Yissachar, N.; Stangl, G.I.; Eilers, E.; Bader, V.; Haase, S.; Kaisler, J.; David, C.; et al. Propionic Acid Shapes the Multiple Sclerosis Disease Course by an Immunomodulatory Mechanism. Cell 2020, 180, 1067.e1016–1080.e1016. [Google Scholar] [CrossRef]
- Saresella, M.; Marventano, I.; Barone, M.; La Rosa, F.; Piancone, F.; Mendozzi, L.; d’Arma, A.; Rossi, V.; Pugnetti, L.; Roda, G.; et al. Alterations in Circulating Fatty Acid Are Associated with Gut Microbiota Dysbiosis and Inflammation in Multiple Sclerosis. Front. Immunol. 2020, 11, 1390. [Google Scholar] [CrossRef]
- Camara-Lemarroy, C.R.; Silva, C.; Greenfield, J.; Liu, W.-Q.; Metz, L.M.; Yong, V.W. Biomarkers of intestinal barrier function in multiple sclerosis are associated with disease activity. Mult. Scler. J. 2019, 26, 1340–1350. [Google Scholar] [CrossRef]
- Olsson, A.; Gustavsen, S.; Langkilde, A.R.; Hansen, T.H.; Sellebjerg, F.; Bach Søndergaard, H.; Oturai, A.B. Circulating levels of tight junction proteins in multiple sclerosis: Association with inflammation and disease activity before and after disease modifying therapy. Mult. Scler. Relat. Disord. 2021, 54, 103136. [Google Scholar] [CrossRef]
- Wunsch, M.; Jabari, S.; Voussen, B.; Enders, M.; Srinivasan, S.; Cossais, F.; Wedel, T.; Boettner, M.; Schwarz, A.; Weyer, L.; et al. The enteric nervous system is a potential autoimmune target in multiple sclerosis. Acta Neuropathol. 2017, 134, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Nouri, M.; Bredberg, A.; Weström, B.; Lavasani, S. Intestinal barrier dysfunction develops at the onset of experimental autoimmune encephalomyelitis, and can be induced by adoptive transfer of auto-reactive T cells. PLoS ONE 2014, 9, e106335. [Google Scholar] [CrossRef] [PubMed]
- Secher, T.; Kassem, S.; Benamar, M.; Bernard, I.; Boury, M.; Barreau, F.; Oswald, E.; Saoudi, A. Oral Administration of the Probiotic Strain Escherichia coli Nissle 1917 Reduces Susceptibility to Neuroinflammation and Repairs Experimental Autoimmune Encephalomyelitis-Induced Intestinal Barrier Dysfunction. Front. Immunol. 2017, 8, 1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jangi, S.; Gandhi, R.; Cox, L.M.; Li, N.; von Glehn, F.; Yan, R.; Patel, B.; Mazzola, M.A.; Liu, S.; Glanz, B.L.; et al. Alterations of the human gut microbiome in multiple sclerosis. Nat. Commun. 2016, 7, 12015. [Google Scholar] [CrossRef] [Green Version]
- Kozhieva, M.; Naumova, N.; Alikina, T.; Boyko, A.; Vlassov, V.; Kabilov, M.R. Primary progressive multiple sclerosis in a Russian cohort: Relationship with gut bacterial diversity. BMC Microbiol. 2019, 19, 309. [Google Scholar] [CrossRef]
- Cekanaviciute, E.; Yoo, B.B.; Runia, T.F.; Debelius, J.W.; Singh, S.; Nelson, C.A.; Kanner, R.; Bencosme, Y.; Lee, Y.K.; Hauser, S.L.; et al. Gut bacteria from multiple sclerosis patients modulate human T cells and exacerbate symptoms in mouse models. Proc. Natl. Acad. Sci. USA 2017, 114, 10713–10718. [Google Scholar] [CrossRef] [Green Version]
- Tankou, S.K.; Regev, K.; Healy, B.C.; Tjon, E.; Laghi, L.; Cox, L.M.; Kivisäkk, P.; Pierre, I.V.; Hrishikesh, L.; Gandhi, R.; et al. A probiotic modulates the microbiome and immunity in multiple sclerosis. Ann. Neurol. 2018, 83, 1147–1161. [Google Scholar] [CrossRef]
- Abdurasulova, I.N.; Tarasova, E.A.; Nikiforova, I.G.; Il’ves, A.G.; Ivashkova, E.V.; Matsulevich, A.V.; Tatarinov, A.E.; Shangina, L.V.; Ermolenko, E.I.; Klimenko, V.M.; et al. The intestinal microbiota composition in patients with multiple sclerosis receiving different disease-modifying therapies DMT. Zh. Nevrol. Psikhiatr. Im. Korsakova 2018, 118, 62–69. [Google Scholar] [CrossRef]
- Forbes, J.D.; Chen, C.-y.; Knox, N.C.; Marrie, R.-A.; El-Gabalawy, H.; de Kievit, T.; Alfa, M.; Bernstein, C.N.; Van Domselaar, G. A comparative study of the gut microbiota in immune-mediated inflammatory diseases—Does a common dysbiosis exist? Microbiome 2018, 6, 221. [Google Scholar] [CrossRef] [Green Version]
- Oezguen, N.; Yalcinkaya, N.; Kücükali, C.I.; Dahdouli, M.; Hollister, E.B.; Luna, R.A.; Türkoglu, R.; Kürtüncü, M.; Eraksoy, M.; Savidge, T.C.; et al. Microbiota stratification identifies disease-specific alterations in neuro-Behçet’s disease and multiple sclerosis. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S121), 58–66. [Google Scholar]
- Choileáin, S.N.; Kleinewietfeld, M.; Raddassi, K.; Hafler, D.A.; Ruff, W.E.; Longbrake, E.E. CXCR3+ T cells in multiple sclerosis correlate with reduced diversity of the gut microbiome. J. Transl. Autoimmun. 2020, 3, 100032. [Google Scholar] [CrossRef] [PubMed]
- Levi, I.; Gurevich, M.; Perlman, G.; Magalashvili, D.; Menascu, S.; Bar, N.; Godneva, A.; Zahavi, L.; Chermon, D.; Kosower, N.; et al. Potential role of indolelactate and butyrate in multiple sclerosis revealed by integrated microbiome-metabolome analysis. Cell Rep. Med. 2021, 2, 100246. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.M.; Maghzi, A.H.; Liu, S.; Tankou, S.K.; Dhang, F.H.; Willocq, V.; Song, A.; Wasén, C.; Tauhid, S.; Chu, R.; et al. Gut Microbiome in Progressive Multiple Sclerosis. Ann. Neurol. 2021, 89, 1195–1211. [Google Scholar] [CrossRef] [PubMed]
- Luczynski, P.; Whelan, S.O.; O’Sullivan, C.; Clarke, G.; Shanahan, F.; Dinan, T.G.; Cryan, J.F. Adult microbiota-deficient mice have distinct dendritic morphological changes: Differential effects in the amygdala and hippocampus. Eur. J. Neurosci. 2016, 44, 2654–2666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogbonnaya, E.S.; Clarke, G.; Shanahan, F.; Dinan, T.G.; Cryan, J.F.; O’Leary, O.F. Adult Hippocampal Neurogenesis Is Regulated by the Microbiome. Biol. Psychiatry 2015, 78, e7–e9. [Google Scholar] [CrossRef]
- El Aidy, S.; Dinan, T.G.; Cryan, J.F. Gut Microbiota: The Conductor in the Orchestra of Immune-Neuroendocrine Communication. Clin. Ther. 2015, 37, 954–967. [Google Scholar] [CrossRef]
- Hoban, A.E.; Stilling, R.M.; Ryan, F.J.; Shanahan, F.; Dinan, T.G.; Claesson, M.J.; Clarke, G.; Cryan, J.F. Regulation of prefrontal cortex myelination by the microbiota. Transl. Psychiatry 2016, 6, e774. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.K.; Menezes, J.S.; Umesaki, Y.; Mazmanian, S.K. Proinflammatory T-cell responses to gut microbiota promote experimental autoimmune encephalomyelitis. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4615–4622. [Google Scholar] [CrossRef] [Green Version]
- Ochoa-Repáraz, J.; Mielcarz, D.W.; Ditrio, L.E.; Burroughs, A.R.; Foureau, D.M.; Haque-Begum, S.; Kasper, L.H. Role of gut commensal microflora in the development of experimental autoimmune encephalomyelitis. J. Immunol. 2009, 183, 6041–6050. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, M.; Ukibe, K.; Matsubara, Y.; Hosoya, T.; Sakai, F.; Kon, S.; Arima, Y.; Murakami, M.; Nakagawa, H.; Miyazaki, T. Lactobacillus helveticus SBT2171 Attenuates Experimental Autoimmune Encephalomyelitis in Mice. Front. Microbiol. 2017, 8, 2596. [Google Scholar] [CrossRef]
- Ochoa-Repáraz, J.; Mielcarz, D.W.; Ditrio, L.E.; Burroughs, A.R.; Begum-Haque, S.; Dasgupta, S.; Kasper, D.L.; Kasper, L.H. Central nervous system demyelinating disease protection by the human commensal Bacteroides fragilis depends on polysaccharide A expression. J. Immunol. 2010, 185, 4101–4108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahi, S.K.; Freedman, S.N.; Murra, A.C.; Zarei, K.; Sompallae, R.; Gibson-Corley, K.N.; Karandikar, N.J.; Murray, J.A.; Mangalam, A.K. Prevotella histicola, A Human Gut Commensal, Is as Potent as COPAXONE® in an Animal Model of Multiple Sclerosis. Front. Immunol. 2019, 10, 462. [Google Scholar] [CrossRef] [PubMed]
- Lavasani, S.; Dzhambazov, B.; Nouri, M.; Fåk, F.; Buske, S.; Molin, G.; Thorlacius, H.; Alenfall, J.; Jeppsson, B.; Weström, B. A novel probiotic mixture exerts a therapeutic effect on experimental autoimmune encephalomyelitis mediated by IL-10 producing regulatory T cells. PLoS ONE 2010, 5, e9009. [Google Scholar] [CrossRef] [Green Version]
- He, B.; Hoang, T.K.; Tian, X.; Taylor, C.M.; Blanchard, E.; Luo, M.; Bhattacharjee, M.B.; Freeborn, J.; Park, S.; Couturier, J.; et al. Lactobacillus reuteri Reduces the Severity of Experimental Autoimmune Encephalomyelitis in Mice by Modulating Gut Microbiota. Front. Immunol. 2019, 10, 385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, H.K.; Kim, G.C.; Kim, Y.; Hwang, W.; Jash, A.; Sahoo, A.; Kim, J.E.; Nam, J.H.; Im, S.H. Amelioration of experimental autoimmune encephalomyelitis by probiotic mixture is mediated by a shift in T helper cell immune response. Clin. Immunol. 2013, 146, 217–227. [Google Scholar] [CrossRef]
- Mestre, L.; Carrillo-Salinas, F.J.; Feliú, A.; Mecha, M.; Alonso, G.; Espejo, C.; Calvo-Barreiro, L.; Luque-García, J.L.; Estevez, H.; Villar, L.M.; et al. How oral probiotics affect the severity of an experimental model of progressive multiple sclerosis? Bringing commensal bacteria into the neurodegenerative process. Gut Microbes 2020, 12, 1813532. [Google Scholar] [CrossRef]
- Raheem, A.; Liang, L.; Zhang, G.; Cui, S. Modulatory Effects of Probiotics During Pathogenic Infections With Emphasis on Immune Regulation. Front. Immunol. 2021, 12, 616713. [Google Scholar] [CrossRef]
- Yokote, H.; Miyake, S.; Croxford, J.L.; Oki, S.; Mizusawa, H.; Yamamura, T. NKT cell-dependent amelioration of a mouse model of multiple sclerosis by altering gut flora. Am. J. Pathol. 2008, 173, 1714–1723. [Google Scholar] [CrossRef] [Green Version]
- Dargahi, N.; Matsoukas, J.; Apostolopoulos, V. Streptococcus thermophilus ST285 Alters Pro-Inflammatory to Anti-Inflammatory Cytokine Secretion against Multiple Sclerosis Peptide in Mice. Brain Sci. 2020, 10, 126. [Google Scholar] [CrossRef] [Green Version]
- Salehipour, Z.; Haghmorad, D.; Sankian, M.; Rastin, M.; Nosratabadi, R.; Soltan Dallal, M.M.; Tabasi, N.; Khazaee, M.; Nasiraii, L.R.; Mahmoudi, M. Bifidobacterium animalis in combination with human origin of Lactobacillus plantarum ameliorate neuroinflammation in experimental model of multiple sclerosis by altering CD4+ T cell subset balance. Biomed. Pharmacother. 2017, 95, 1535–1548. [Google Scholar] [CrossRef]
- Sokovic, S.; Mihajlovic, S.; Radojevic, D.; Popović, D.; Djokic, J.; Stanisavljević, S.; Lazarević, M.; Miljković, D.; Ruas-Madiedo, P.; Golić, N.; et al. Characterization of pH resistance and the proteolytic activity of GABA producing Lactobacillus brevis BGZLS10-17 in preparation of fermented milk beverage and the effects on the symptoms of the experimental autoimmune encephalomyelitis. J. Serb. Chem. Soc. 2019, 85, 94. [Google Scholar] [CrossRef] [Green Version]
- Abdurasulova, I.N.; Matsulevich, A.V.; Tarasova, E.A.; Kudryavtsev, I.V.; Serebrjakova, M.K.; Ermolenko, E.I.; Bisaga, G.N.; Klimenko, V.M.; Suvorov, A.N. Enterococcus faecium strain L-3 and glatiramer acetate ameliorate experimental allergic encephalomyelitis in rats by affecting different populations of immune cells. Benef. Microbes 2016, 7, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Suzuki, T.; Kaji, R.; Serata, M.; Nagata, T.; Ando, M.; Iizuka, R.; Tsujibe, S.; Murakami, J.; Kiyoshima-Shibata, J.; et al. Probiotic upregulation of peripheral IL-17 responses does not exacerbate neurological symptoms in experimental autoimmune encephalomyelitis mouse models. Immunopharmacol. Immunotoxicol. 2012, 34, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Gharehkhani Digehsara, S.; Name, N.; Esfandiari, B.; Karim, E.; Taheri, S.; Tajabadi-Ebrahimi, M.; Arasteh, J. Effects of Lactobacillus casei Strain T2 (IBRC-M10783) on the Modulation of Th17/Treg and Evaluation of miR-155, miR-25, and IDO-1 Expression in a Cuprizone-Induced C57BL/6 Mouse Model of Demyelination. Inflammation 2021, 44, 334–343. [Google Scholar] [CrossRef]
- Tankou, S.K.; Regev, K.; Healy, B.C.; Cox, L.M.; Tjon, E.; Kivisakk, P.; Vanande, I.P.; Cook, S.; Gandhi, R.; Glanz, B.; et al. Investigation of probiotics in multiple sclerosis. Mult. Scler. 2018, 24, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Cristofori, F.; Dargenio, V.N.; Dargenio, C.; Miniello, V.L.; Barone, M.; Francavilla, R. Anti-Inflammatory and Immunomodulatory Effects of Probiotics in Gut Inflammation: A Door to the Body. Front. Immunol. 2021, 12, 578386. [Google Scholar] [CrossRef]
- Li, H.; Wang, P.; Huang, L.; Li, P.; Zhang, D. Effects of regulating gut microbiota on the serotonin metabolism in the chronic unpredictable mild stress rat model. Neurogastroenterol. Motil. 2019, 31, e13677. [Google Scholar] [CrossRef] [Green Version]
- Kouchaki, E.; Tamtaji, O.R.; Salami, M.; Bahmani, F.; Daneshvar Kakhaki, R.; Akbari, E.; Tajabadi-Ebrahimi, M.; Jafari, P.; Asemi, Z. Clinical and metabolic response to probiotic supplementation in patients with multiple sclerosis: A randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2017, 36, 1245–1249. [Google Scholar] [CrossRef]
- Mohammadi, A.A.; Jazayeri, S.; Khosravi-Darani, K.; Solati, Z.; Mohammadpour, N.; Asemi, Z.; Adab, Z.; Djalali, M.; Tehrani-Doost, M.; Hosseini, M.; et al. The effects of probiotics on mental health and hypothalamic–pituitary–adrenal axis: A randomized, double-blind, placebo-controlled trial in petrochemical workers. Nutritional. Neurosci. 2016, 19, 387–395. [Google Scholar] [CrossRef]
- Salami, M.; Kouchaki, E.; Asemi, Z.; Tamtaji, O.R. How probiotic bacteria influence the motor and mental behaviors as well as immunological and oxidative biomarkers in multiple sclerosis? A double blind clinical trial. J. Funct. Foods 2019, 52, 8–13. [Google Scholar] [CrossRef]
- Rahimlou, M.; Hosseini, S.A.; Majdinasab, N.; Haghighizadeh, M.H.; Husain, D. Effects of long-term administration of Multi-Strain Probiotic on circulating levels of BDNF, NGF, IL-6 and mental health in patients with multiple sclerosis: A randomized, double-blind, placebo-controlled trial. Nutr. Neurosci. 2022, 25, 411–422. [Google Scholar] [CrossRef]
- Tamtaji, O.R.; Kouchaki, E.; Salami, M.; Aghadavod, E.; Akbari, E.; Tajabadi-Ebrahimi, M.; Asemi, Z. The Effects of Probiotic Supplementation on Gene Expression Related to Inflammation, Insulin, and Lipids in Patients with Multiple Sclerosis: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Am. Coll. Nutr. 2017, 36, 660–665. [Google Scholar] [CrossRef]
- Gilgun-Sherki, Y.; Melamed, E.; Offen, D. The role of oxidative stress in the pathogenesis of multiple sclerosis: The need for effective antioxidant therapy. J. Neurol. 2004, 251, 261–268. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Subjects | Altered Genera in MS | Study |
|---|---|---|
| RRMS (n = 20) CTR (n = 40) | ↑: Streptococcus, Eggerthella ↓: Faecalibacterium, Prevotella, Anaerostipes | Miyake et al., Japan (2015) [66] |
| RRMS (n = 60) CTR (n = 43) | ↑: Akkermansia, Methanobrevibacter ↓: Butyricimonas, Collinsella, Slackia, Prevotella | Jangi et al., USA (2016) [75] |
| RRMS (n = 71) CTR (n = 71) | ↑: Akkermansia, Acinetobacter, Calcoaceticus ↓: Parabacteroides | Cekanaviciute et al., USA (2017) [77] |
| RRMS (n = 9) CTR (n = 13) | ↑: Lactobacillus ↓: Akkermansia, Blautia | Tankou et al., USA (2018) [78] |
| RRMS (n = 17) CTR (n = 17) | ↑: atypical E coli, Enterobacter sp. ↓: E. coli | Abdurasulva et al., Russia (2018) [79] |
| RRMS (n = 19) CTR (n = 23) | ↑: Actinomyces, Eggerthella, Anaerofustis, Clostridia XIII, Clostridium III, Faecalicoccus, Streptococcus ↓: Butyricicoccus, Faecalibacterium, Dialister, Gemmiger, Lachnospiraceae, Subdolibacterium | Forbes et al., Canada (2018) [80] |
| RRMS (n = 13) CTR (n = 14) | ↑: None ↓: Prevotella | Oezguen et al., USA (2019) [81] |
| RRMS (n = 26) CTR (n = 39) | ↑: Bacteroidetes ↓: Coprococcus, Firmicutes, Paraprevotella, Ruminococcaceae | Choileáin et al., USA (2020) [82] |
| RRMS (n = 26) SPMS (n = 12) CTR (n = 38) | ↑: Akkermansia in SPMS, Streptococcus in RRMS, Collinsella in RRMS and SPMS ↓: Coprococcus, Roseburia in RRMS and SPMS, Lachnospira in RRMS | Saresella et al., Italy (2020) [69] |
| RRMS (n = 129) CTR (n = 58) | ↑: Lawsonella ↓: Faecalibacterium prausnitzii, Bacteroides fragiils, Eubacterium rectale, Butyrivibrio, Clostridium, Coprococcus, Roseburia | Levi et al., Israel (2021) [83] |
| RRMS (n = 199) Progressive MS (n = 44) CTR (n = 40) | ↑: Clostridium, Bacteroides, Gemella, Akkermansia in RRMS and progressive MS ↓: Prevotella and Dorea in RRMS and progressive MS | Cox et al., USA (2021) [84] |
| Model | Intervention | Duration | Measurements | Major Findings | Study |
|---|---|---|---|---|---|
| PLP-induced EAE in SJL/J female mice; MOG-induced EAE in C57BL/6 female mice (7 weeks old, n = 15 per group) | Administration groups (G): G1: Control (saline/peptone, orally) G2: L. casei strain Shirota (orally, once daily, 0.6–1.2 × 109 CFU) | 50 days | -Evaluation of neurological symptoms; -Histopathological changes in the spinal cord; -mRNA and protein level: IL-10, IL-17A, and IFN-γ; -Cytometric analysis of cell surface antigens: anti-CD3, anti-CD4, anti-CD8, and anti-CD25. Material: inguinal lymph nodes (ILN) and spleen. | -Improved neurological symptoms in the PLP model; -Slightly increased IL-10 level in ILN; -The enhanced percentage of CD4+/CD25+ (Tregs) in ILN and spleen; -Increased level of CD3+/CD8+ (Tcyt) in the spleen; -Elevated concentration of IL-17A and IL-10 in ILN. | Kobayashi et al., (2012) Japan [104] |
| MOG-induced EAE in C57BL/6 female mice (6–8 weeks old, n = 10 per group) | G1: Control (PBS, orally) G2: IRT5 probiotics powder: L. casei, L. acidophilus, L. reuteni, B. bifidum, and S. thermophilus (orally, once daily, 1 × 108 CFU of each strain, final 5 × 108 CFU) | 30 days | -Clinical condition and symptoms using hematoxylin and eosin test staining; -mRNA level: IL-1β, IL-2, IL-4, IL-6, IL-10, IL-12, IL-17A, and TGF-β; -Cytometric analysis of cell surface antigens: anti-B220, anti-Gr1, anti-CD11b, anti-CD11c, and anti-CD4; intracellular cytokines: anti-IL-12, anti-IL-10, anti-IL-17, anti-IFN-γ, anti-Foxp3, and anti-TNF-α. Material: spinal cord. | -Inhibited development and progression of EAE; -Delayed onset of EAE; -Suppressed EAE incidence; -Decreased the clinical symptoms of EAE; -Reduced lymphocyte infiltration in the spinal cord; -Decreased levels of Gr1+ or/and CD11b+ monocyte and CD4+ T cells in the spinal cord; -Suppressed expression levels of pathogenic cytokines: IL-1β, IL-2, IFN-γ, TNF-α, and IL-17; -Enhanced production of IL-10 in CD4+ T cells and CD11c+ dendritic cells; -Slightly increased level of B220+ B cells; -Mitigated Th1/Th17 polarization while inducing IL-10+ producing CD4+ T cells in draining lymph nodes; -Down-regulated expression levels of IL-6, IFN-γ and TNF-α at mRNA level by CD4+ T cells; -Enhanced generation of CD4+/FoxP3+ Tregs at the site of inflammation. | Kwon et al., (2013) Republic of Korea [96] |
| EGM-induced EAE in male Wistar rats (3 months old, total n = 122 per 4 groups) | G1: Control (saline, subcutaneously) G2: Control (saline, intragastric) G3: Glatiramer acetate (GA) (subcutaneously, 4 mg/kg/day) G4: E. faecium L3 (intragastrically, 8 CFU/mL) | 28 days | -Blood cell phenotyping by flow cytometry: anti-CD3, anti-CD4, anti-CD8, anti-CD16, anti-CD25, anti-FoxP3, anti-CD45RA; -Evaluation of neurological symptoms. Material: spinal cord and whole blood | -Decreased severity and disease duration of EAE animals; -Reduced number of (CD4+/CD25+/FoxP3+) Tregs and NK cells. | Abdurasulova et al., (2016) Russia [103] |
| MOG-induced EAE in C57BL/6 female mice (8–10 weeks old, n = 8 per group) | G1: Control (saline, orally) G2: L. plantarum (intragastric, once daily, 1 × 109 CFU) G3: B. animalis (intragastric, once daily, 1 × 109 CFU) G4: both probiotics | 22 days | -Clinical score evaluation; -Body weight control; -Histopathology of the spinal cord; -Evaluate the proliferative activity of isolated splenic T cells using a Brdu assay; -Determination of Tregs by flow cytometry using anti-CD4, anti-CD25, and anti-FoxP3; -Protein level: IL-4, IL-6, IL-10, IL-17, IFN-γ, TGF-β; -mRNA level: FoxP3, T-bet, GATA3, and RORγt. Material: spinal cord, spleen, brain, and peripheral lymph nodes. | -Induced polarization of CD4+ T cells toward anti-inflammatory Tregs (CD4+/CD25+/Foxp3+); -Suppressed autoreactive T cells proliferation; -Inhibited leukocyte infiltration into CNS; -Ameliorated EAE condition by favoring Th2 and Treg differentiation; -Inhibited differentiation of Th1 and Th17 cells; -Increased level of IL-6, IL-17, IFN-γ, and diminished concentration of IL-4, IL10 and TGF-β in splenocytes and lymph nodes. | Salehipour et al., (2017) Iran [101] |
| MOG-induced EAE in C57BL/6 female mice (8–12 weeks old, n = 30–40 per group) | G1: Control (PBS, orally) G2: E.coli Nissle 1917 (ECN) (orally, one daily, 1 × 108 CFU) G3: archetypal E.coli strain MG1655 (orally, one daily, 1 × 108 CFU) | 30 days | -In vivo and ex vivo intestinal permeability assessment; -mRNA level: ZO-1, claudin-8, IL-6, Reg3β, and Reg3γ; -Protein level: IFN-β, IL-17, GM-CSF. Material: serum, ileum, colon, brain, spinal cord, and lymph nodes. | -ECN reduced the severity of EAE; -ECN treatment protects from EAE-mediated alteration of the intestinal barrier function; -Reduced migration of CD4+ T cells from the periphery to the CNS during the acute phase; -Increased production of IL-10 by MOG-specific CD4+ T cells. | Secher et al., (2017) France [74] |
| PLP-induced EAE in HLA-DR3.DQ8 double transgenic and C57BL/6, both male and female mice (8–12 weeks old, n = 4–8 mice per group) | G1: Control (PBS, orally) G2: TSB media (orally) G3: P. histicola (orally, one daily, 108 CFU) G4: Copaxone® (GA) (subcutaneously, 100 μg every day) G5: Copaxone®+ P. histicola | 14 days | -Evaluation of clinical EAE scores; -Clinical condition and symptoms using hematoxylin and eosin test staining; -Evaluation of gut microbiota composition; -Cytometric analysis of cell surface antigens: anti-CD4 and anti-CD25, intracellular expression of FoxP3+ and IL-10; Material: fecal pellets, brain, and spinal cord. | -Significantly reduced severity score and delayed onset of disease; -Increased number of CD4+/FoxP3+ Tregs in periphery and gut; -Reduced frequency of IFN-y and IL-17-producing CD4+ T cells in the CNS; -P. histicola, together with Copaxone®, more effectively suppressed disease compared to either treatment alone. | Shahi et al., (2019) USA [93] |
| SCH-induced EAE in female Dark Agouti (DA) rats (8–10 weeks old, n = 5 per group) | G1:Control (MRS Broth, orally, medium for Lactobacillus spp.) G2: L. brevis BGZLS10-17 (high GABA-producing strain) (subcutaneously, one daily, 1 × 108 CFU) | 30 days | -Neurological symptoms assessment. Material: spinal cord. | -Ameliorated severity score of EAE model (G2) after L. brevis intake. | Sokovic Bajic et al., (2019) Serbia [102] |
| MBP-induced EAE in female SJL/J mice (6–9 weeks old, n = 3 per group) | G1: Control (medium, orally) G2: S. thermophilus 285 (orally, one daily, 1 × 108 CFU) | 14 days | -Cytokine level analysis: IL-1β, IL-2, IL-4, IL-5, IL-6, IL-10, GM-CSF, TNF-α, and IFN-γ using Bioplex system. Material: spleen. | -Increased level of IL-4, IL-5 and IL-10 cytokines and diminished levels of IL-1β and IFN-y. | Dargahi et al., (2020) Australia [100] |
| TMEV-infected susceptible female SJL/J mice (6–8 weeks old, n = 5–10 per group) | G1: Sham mice G2: Sham mice + Vivomixx (orally, 3 × 108 CFU) G3: TMEV-mice G4: TMEV-mice + Vivomixx Vivomixx (L. paracasei, L. plantarum, L. acidophilus, L. delbruckeii subspecies bulgaricus, B. longum, B. infantis, B. breve, and S. thermophilus). | 15 days | -Assessment of the motor functions; -Measurement of bacteria-derived SCFAs; -mRNA level: IL-1β, IL-6, TNF-α, IL-4 and IL-10 in spinal cord; -Estimation of the level of Tregs and Bregs population; -Microglial morphology; -Cytometric analysis of cell surface antigens: anti-CD4, anti-CD8, and anti-CD39; -Identification of the gut microbiota community changes. Material: plasma, brain, spinal cord, spleen, and mesenteric lymph nodes. | -The increased abundance of Bcteroidetes, Actinobacteria, and Tenericutes; -Improved motor disability; -Reduced microgliosis, astrogliosis, and leukocyte infiltration; -The enhanced presence of Bregs (CD19+/CD5+/CD1dhigh) in the CNS; -Diminished IL-1b and IL-6 gene expression in spinal cord; -Promoted IL-10 gene expression; -Increased plasma level of butyrate and acetate levels; -Restricted IL-17 production by Th17-polarized CD4+ T cells from mesenteric lymph nodes. | Mestre et al., (2020) Spain [97] |
| Cuprizone-induced mouse model of demyelination in C57BL/6 female mice (8–10 weeks old) | G1: Control G2: Cuprizone control G3: Probiotic control G4: L. casei (oral administration, 1 × 109 CFU) for 4 weeks, then cuprizone for 4 weeks G5: Cuprizone for 4 weeks, then L. casei for 4 weeks G6: Cuprizone for 4 weeks, then L. casei for 4 weeks with vitamin D3 (20 IU per day) | 28 days | -Assessment of the motor behaviors; -Y-maze test for spatial memory and learning; -mRNA expression: IDO-1, miR-155, and miR-25; -Protein level: IL-17 and TGF-β. Material: brain, blood. | -L. casei ameliorated the CPZ-induced motor impairment; -Decreased the mRNA expression of IFN-γ, IDO-1, and miR-155; -Increased serum level of TGF-β and miR-25; -L. casei can shift responses from Th17 to Tregs; -Reduced pro-inflammatory cytokines; -Diminished demyelinating symptoms. | Gharehkhani Digehsara et al., (2020) Iran [105] |
| Subjects | Sex Ratio (M/F) | BMI (kg × m−2) | Average Age ± SD | Probiotic Bacteria | Dosage (CFU g−1) | Administration | Major Findings | Limitations | Study |
|---|---|---|---|---|---|---|---|---|---|
| RRMS (n = 40) (EDSS ≤ 4.5) Including: Placebo group (n = 20) and probiotic group (n = 20) | No data. | Placebo group: 24.7 ± 3.7 Probiotic group: 25.6 ± 4.6 | Placebo group: 34.9 ± 8.9 Probiotic group: 32.8 ± 9.2 | L. acidophilus, L. casei, B. bifidum, and L. fermentum Placebo group: starch | 2 × 109 | Orally, once a day for 3 months | -Down-regulated gene expression of IL-8 and TNF-α in PBMCs compared with the placebo group. | -Lack of information about microbiota changes; -Small sample size; -No confirmation of changes in the proteins level of studied molecules (only gene expression results); -Lack of diet control. | Double-blind RCT Tamtaji et al., (2017) Iran [113] |
| RRMS (n = 60) (EDSS ≤ 4.5) Including: Placebo group (n = 30) and probiotic group (n = 30) | Placebo group: 5/25 Probiotic group: 5/25 | Placebo group: 24.7 ± 3.3 Probiotic group: 25.4 ± 4.0 | Placebo group: 33.8 ± 8.9 Probiotic group: 34.4 ± 9.2 | L. acidophilus, L. casei, B. bifidum, and L. fermentum Placebo group: starch | 2 × 109 | Orally, once a day for 3 months | -Improved EDSS, BDI, GHQ-28, and DASS scales; -Decreased serum insulin level; -Increased quantitative insulin sensitivity check index and HDL-cholesterol levels; -Diminished levels of hs CRP, plasma NO metabolites, and MDA. | Double-blind RCT Kouchaki et al., (2017) Iran [109] | |
| Control group (CTR) (n = 13) RRMS on GA (n = 7) or untreated (n = 2) | No data. | CTR: 25.8 ± 4.1 MS: 31.1 ± 5.6 | CTR: 35 ± 14 MS: 50 ± 10 | VSL3 probiotics powder consisting of Lactobacillus (L. paracasei, L. plantarum, L. acidophilus, and L. delbruckeii subspecies bulgaricus), Bifidobacterium (B. longum, B. infantis, and B. breve) and S. thermophilus Brand name: Visbiome (USA) or Vivomixx (Europe). | 3 × 1011 | Orally, twice daily for 2 months. | -Diminished level of CD14+CD16+ and enhanced frequency of CD8+ T cells in MS patients; -Decreased MFI of HLA-DR on CD45+/LIN−/CD11c+ in MS patients; -The relative level of Th1 and Th17 cells were trending down in both controls and MS patients. | -Very small study and control group; -RRMS subjects (n = 2) were treated with glatiramer acetate during supplementation; -The subjects enrolled in this study were not on a dietary restriction; -No information about the gender of the subjects. | Clinical Trial Tankou et al., (2018) USA [106] |
| RRMS (n = 48) (EDSS ≤ 4.5) Including: Placebo group (n = 24) and probiotic group (n = 24) | Placebo group: 8/18 Probiotic group: 6/18 | Placebo group: 24.5 ± 0.63 Probiotic group: 24.7 ± 0.55 | Placebo group: 36.5 ± 1.44 Probiotic group: 34.8 ± 1.06 | B. infantis, B. lactis, L. reuteri, L. casei, L. plantarum and L. fermentum Placebo group: maltodextrin | 2 × 109 | Orally, once daily for 4 months. | -Markedly improves mental health parameters: BDI, GHQ-28, and DASS; -Reduced levels of hs-CRP, NO, and MDA; -Improved insulin resistance and lipid metabolism. -Decreased EDSS parameter. | -There is no information about the potential changes in bacterial strains. | Double-blind RCT Salami et al., (2019) Iran [111] |
| RRMS (n = 70) (EDSS ≤ 4.5) Including: Placebo group (n = 35) and probiotic group (n = 35) | Placebo group: 12/21 Probiotic group: 6/26 | Placebo group: 24.55 ± 3.51 Probiotic group: 25.48 ± 4.54 | Placebo group: 39.9 ± 8.76 Probiotic group: 42.15 ± 11.98 | Protein probiotics powder consisting of the following: B. subtilis, B. bifidum, B. breve, B. infantis, B. longum, L. acidophilus, L. bulgaricus, L. casei, L. plantarum, L. rhamnosus, L. helveticus, L. salivarius, L. lactis, and 0S. thermophilus. Placebo group: maltodextrin | 2 × 109 | Orally, twice daily for 6 months. | -Greater improvement in mental health parameters: GHQ-28, BDI, FSS, PRI. | Double-blind RCT Rahimlou et al., (2020) Iran [112] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziedzic, A.; Saluk, J. Probiotics and Commensal Gut Microbiota as the Effective Alternative Therapy for Multiple Sclerosis Patients Treatment. Int. J. Mol. Sci. 2022, 23, 14478. https://doi.org/10.3390/ijms232214478
Dziedzic A, Saluk J. Probiotics and Commensal Gut Microbiota as the Effective Alternative Therapy for Multiple Sclerosis Patients Treatment. International Journal of Molecular Sciences. 2022; 23(22):14478. https://doi.org/10.3390/ijms232214478
Chicago/Turabian StyleDziedzic, Angela, and Joanna Saluk. 2022. "Probiotics and Commensal Gut Microbiota as the Effective Alternative Therapy for Multiple Sclerosis Patients Treatment" International Journal of Molecular Sciences 23, no. 22: 14478. https://doi.org/10.3390/ijms232214478
APA StyleDziedzic, A., & Saluk, J. (2022). Probiotics and Commensal Gut Microbiota as the Effective Alternative Therapy for Multiple Sclerosis Patients Treatment. International Journal of Molecular Sciences, 23(22), 14478. https://doi.org/10.3390/ijms232214478