
Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Results
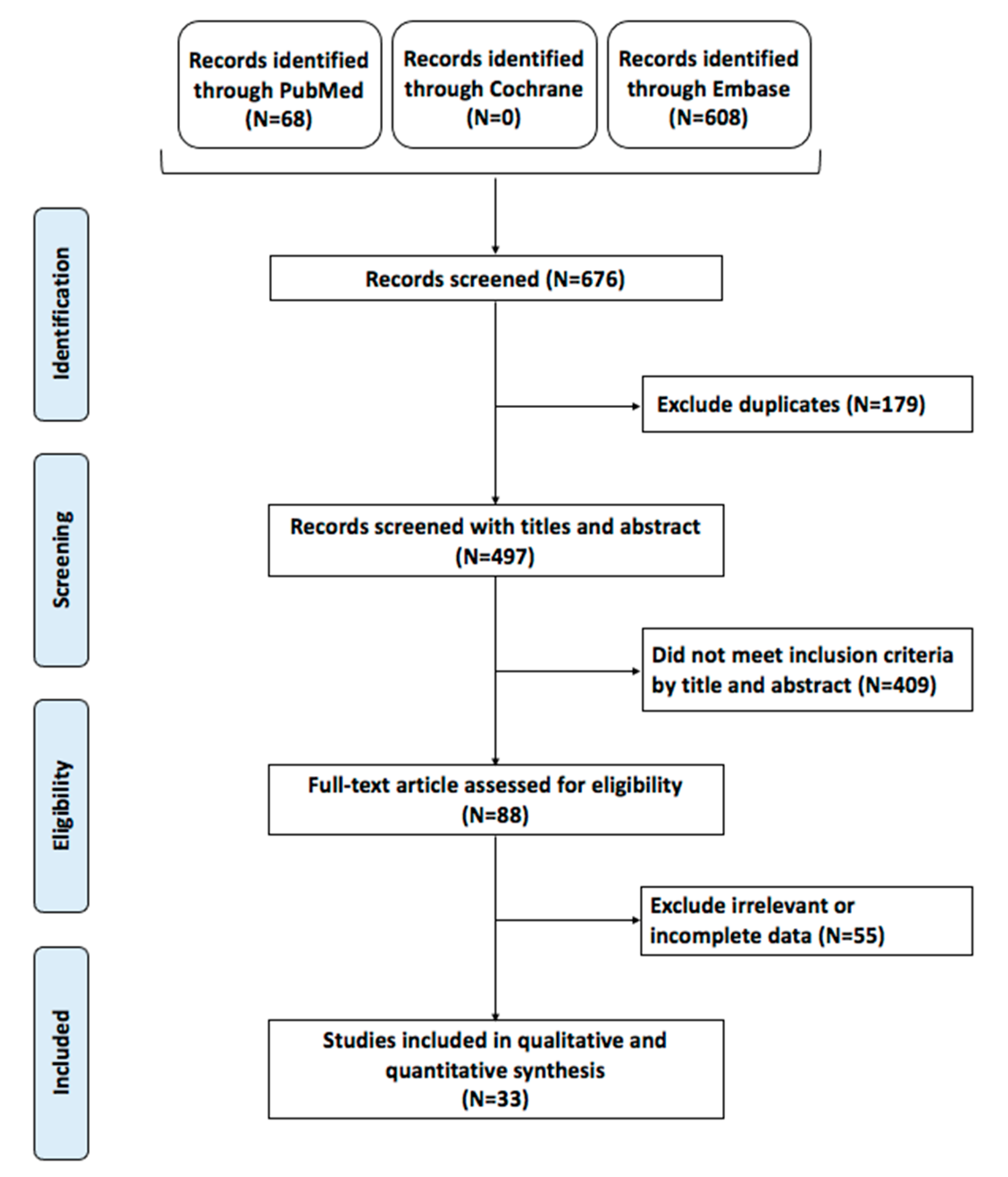
2.1. Literature Search
2.2. Study Population
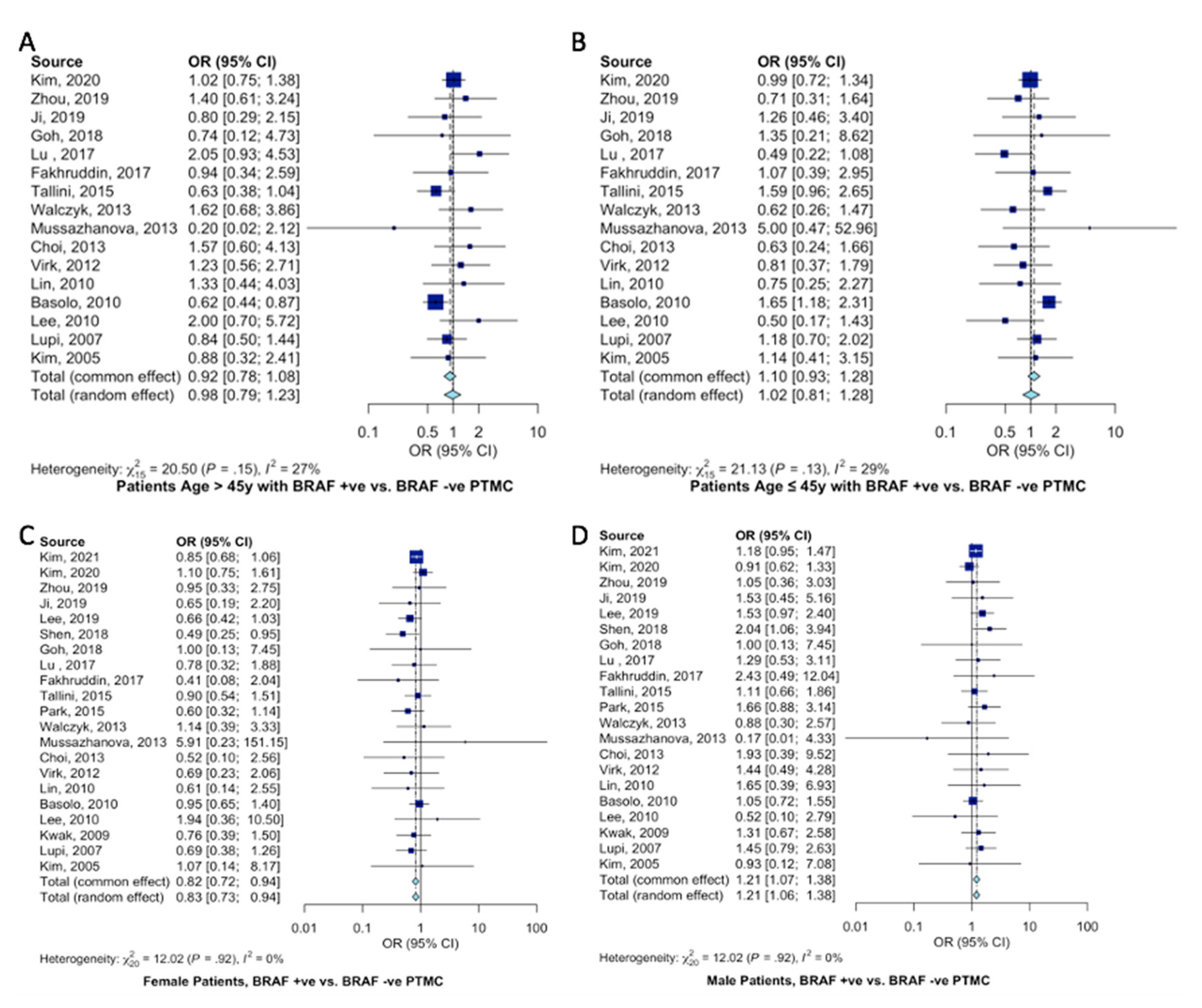
2.3. Demographic Characteristics
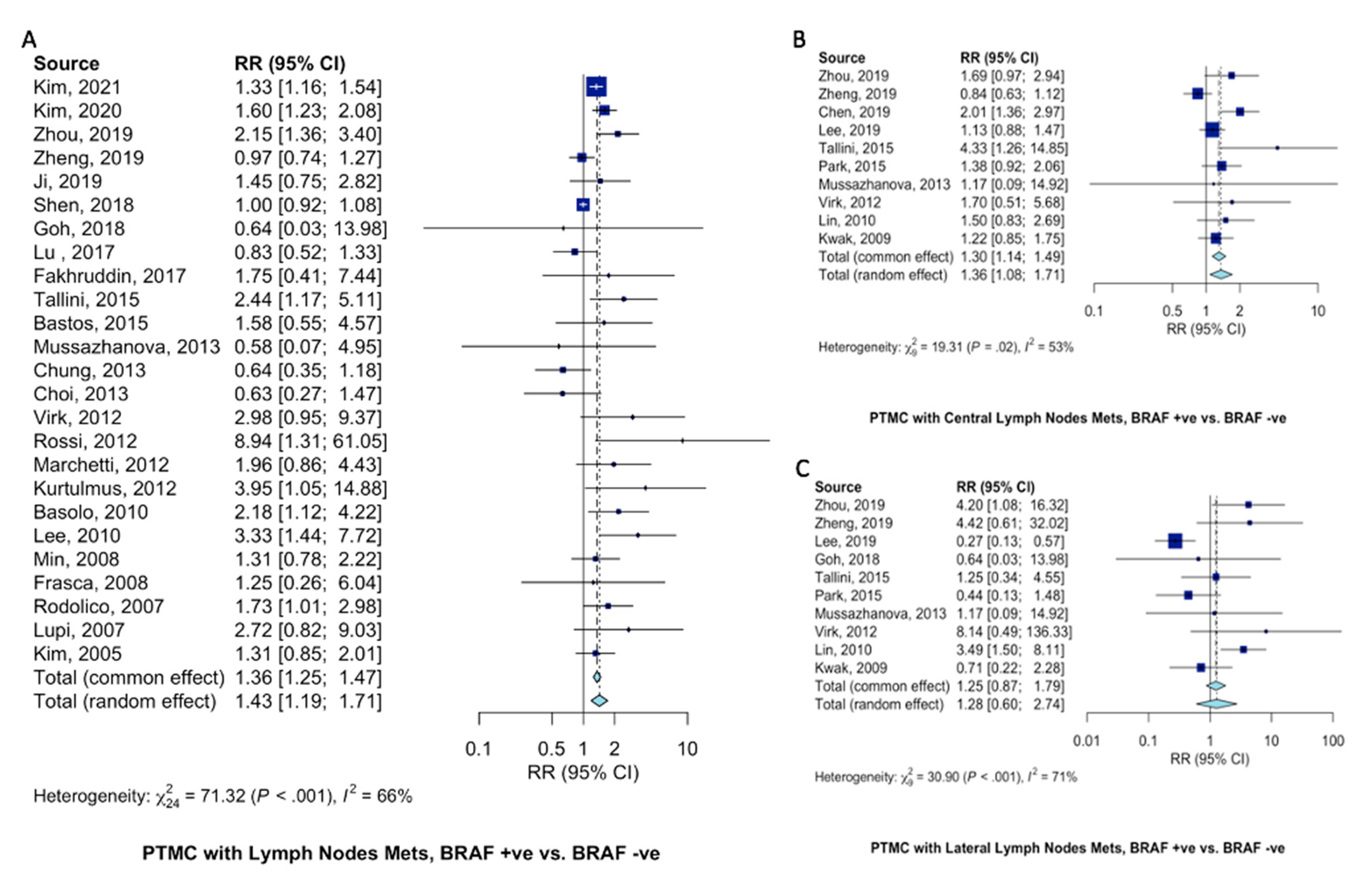
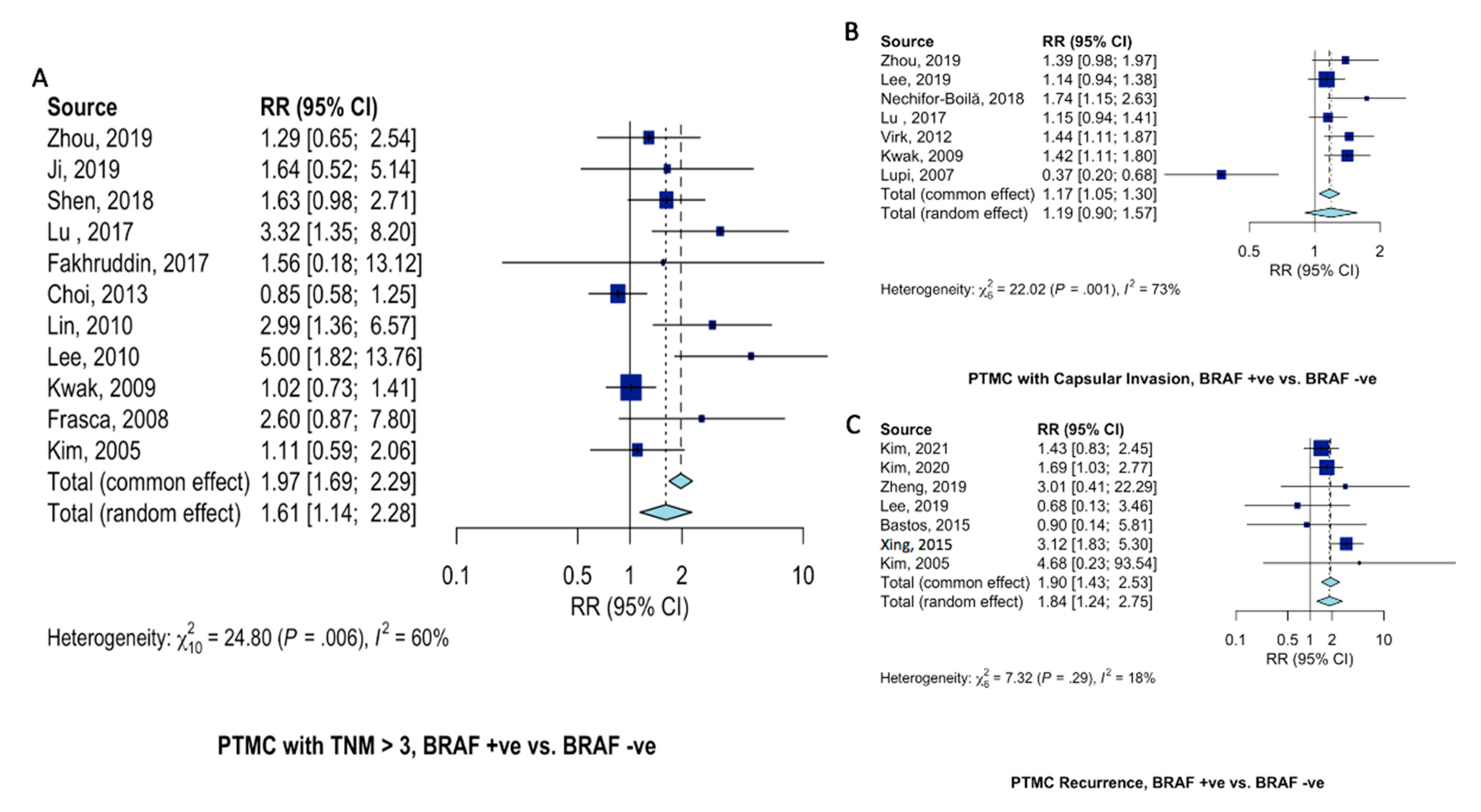
2.4. Pathological Features
3. Discussion
4. Materials and Methodology
4.1. Literature Search
4.2. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davies, L.; Welch, H.G. Increasing Incidence of Thyroid Cancer in the United States, 1973-2002. JAMA 2006, 295, 2164–2167. [Google Scholar] [CrossRef] [Green Version]
- Sun, W.; Lan, X.; Zhang, H.; Dong, W.; Wang, Z.; He, L.; Zhang, T.; Liu, S. Risk Factors for Central Lymph Node Metastasis in CN0 Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0139021. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fligor, S.C.; Lopez, B.; Uppal, N.; Lubitz, C.C.; James, B.C. Time to Surgery and Thyroid Cancer Survival in the United States. Ann. Surg. Oncol. 2021, 28, 3556–3565. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Weng, J.; Bauer, J.; Ranvier, G.; Clark, O.H.; Duh, Q.-Y.; Shibru, D.; Bastian, B.; Griffin, A. The Prevalence and Prognostic Value of BRAF Mutation in Thyroid Cancer. Ann. Surg. 2007, 246, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. BRAF Mutation in Papillary Thyroid Cancer: Pathogenic Role, Molecular Bases, and Clinical Implications. Endocr. Rev. 2007, 28, 742–762. [Google Scholar] [CrossRef] [PubMed]
- Elisei, R.; Ugolini, C.; Viola, D.; Lupi, C.; Biagini, A.; Giannini, R.; Romei, C.; Miccoli, P.; Pinchera, A.; Basolo, F. BRAFV600E Mutation and Outcome of Patients with Papillary Thyroid Carcinoma: A 15-Year Median Follow-Up Study. J. Clin. Endocrinol. Metab. 2008, 93, 3943–3949. [Google Scholar] [CrossRef] [Green Version]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Viola, D.; Elisei, R.; Bendlova, B.; Yip, L.; Mian, C.; Vianello, F.; Tuttle, R.M.; et al. Association Between BRAF V600E Mutation and Mortality in Patients With Papillary Thyroid Cancer. JAMA 2013, 309, 1493–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Kwon, H. The Impact of BRAF Mutation on the Recurrence of Papillary Thyroid Carcinoma: A Meta-Analysis. Cancers 2020, 12, 2056. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, K.J.; Bae, J.H.; Kim, J.H.; Kim, N.H.; Kim, H.Y.; Kim, H.Y.; Baek, S.-K.; Kim, S.G.; Jung, K.Y. Null Association between BRAF V600E Mutation and Tumor Recurrence in Patients with Papillary Thyroid Microcarcinoma in South Korea. Int. J. Thyroidol. 2021, 14, 135–142. [Google Scholar] [CrossRef]
- Kim, K.J.; Kim, S.G.; Tan, J.; Shen, X.; Viola, D.; Elisei, R.; Puxeddu, E.; Fugazzola, L.; Colombo, C.; Jarząb, B.; et al. BRAF V600E status may facilitate decision-making on active surveillance of low-risk papillary thyroid microcarcinoma. Eur. J. Cancer 2019, 124, 161–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Li, J.; Wang, Y.; Xue, S.; Zhang, Y. Association of BRAF gene and TSHR with cervical lymph node metastasis of papillary thyroid microcarcinoma. Oncol. Lett. 2018, 17, 183–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiangqian, Z.; Chen, P.; Ming, G.; Jingtai, Z.; Xiukun, H.; Jingzhu, Z.; Xi, W.; Jiadong, C.; Dapeng, L.; Biyun, Q. Risk factors for cervical lymph node metastasis in papillary thyroid microcarcinoma: A study of 1,587 patients. Cancer Biol. Med. 2019, 16, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.-D.; Zhang, Z.; Wang, K.-K.; Shang, M.-Y.; Zhao, S.-S.; Ding, W.-B.; Du, R.; Yu, Z.; Xu, X.-M. A multivariable model of BRAFV600E and ultrasonographic features for predicting the risk of central lymph node metastasis in cN0 papillary thyroid microcarcinoma. Cancer Manag. Res. 2019, 11, 7211–7217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, W.; Xie, H.; Wei, B.; Shen, H.; Liu, A.; Gao, Y.; Wang, L. Relationship between BRAF V600E gene mutation and the clinical and pathologic characteristics of papillary thyroid microcarcinoma. Int. J. Clin. Exp. Pathol. 2019, 12, 3492–3499. [Google Scholar]
- Lee, S.M.; Lee, C.R.; Kang, S.-W.; Lee, J.; Jeong, J.J.; Nam, K.-H.; Chung, W.Y.; Park, C.S. Association between BRAFV600E Mutations and Clinicopathological Features of Papillary Thyroid Microcarcinoma (PTMC). J. Endocr. Surg. 2019, 19, 76–84. [Google Scholar] [CrossRef]
- Nechifor-Boilă, A.C.; Szász, E.A.; Descotes, F.; Berger, N.; Zahan, A.E.; Loghin, A.; Ceteraş, D.M.; Borda, A. Morphological features predictive for BRAF(V600E) mutation in papillary thyroid microcarcinomas. Romanian J. Morphol. Embryol. 2018, 59, 747–753. [Google Scholar]
- Shen, G.; Kou, Y.; Liu, B.; Huang, R.; Kuang, A. The BRAFV600E Mutation in Papillary Thyroid Microcarcinoma with Intermediate-Risk to High-Risk Features: Does the Mutation Have an Effect on Clinical Response to Radioiodine Therapy? Nucl. Med. Commun. 2019, 40, 8. [Google Scholar] [CrossRef]
- Goh, X.; Lum, J.; Yang, S.P.; Chionh, S.B.; Koay, E.; Chiu, L.; Parameswaran, R.; Ngiam, K.Y.; Loh, T.K.S.; Nga, M.E.; et al. BRAF mutation in papillary thyroid cancer-Prevalence and clinical correlation in a South-East Asian cohort. Clin. Otolaryngol. 2018, 44, 114–123. [Google Scholar] [CrossRef]
- Lu, H.-Z.; Qiu, T.; Ying, J.-M.; Lyn, N. Association between BRAFV600E mutation and the clinicopathological features of solitary papillary thyroid microcarcinoma. Oncol. Lett. 2017, 13, 1595–1600. [Google Scholar] [CrossRef] [Green Version]
- Fakhruddin, N.; Jabbour, M.; Novy, M.; Tamim, H.; Bahmad, H.; Farhat, F.; Zaatari, G.; Aridi, T.; Kriegshauser, G.; Oberkanins, C.; et al. BRAF and NRAS Mutations in Papillary Thyroid Carcinoma and Concordance in BRAF Mutations Between Primary and Corresponding Lymph Node Metastases. Sci. Rep. 2017, 7, 4666. [Google Scholar] [CrossRef] [PubMed]
- Tallini, G.; De Biase, D.; Durante, C.; Acquaviva, G.; Bisceglia, M.; Bruno, R.; Reggiani, M.L.B.; Casadei, G.P.; Costante, G.; Cremonini, N.; et al. BRAF V600E and risk stratification of thyroid microcarcinoma: A multicenter pathological and clinical study. Mod. Pathol. 2015, 28, 1343–1359. [Google Scholar] [CrossRef] [PubMed]
- Park, V.; Kim, E.-K.; Lee, H.S.; Moon, H.J.; Yoon, J.H.; Kwak, J.Y. Real-Time PCR Cycle Threshold Values for the BRAFV600E Mutation in Papillary Thyroid Microcarcinoma May Be Associated With Central Lymph Node Metastasis. Medicine 2015, 94, e1149. [Google Scholar] [CrossRef] [PubMed]
- Bastos, A.U.; Oler, G.; Nozima, B.H.N.; Moysés, R.A.; Cerutti, J.M. BRAF V600E and decreased NIS and TPO expression are associated with aggressiveness of a subgroup of papillary thyroid microcarcinoma. Eur. J. Endocrinol. 2015, 173, 525–540. [Google Scholar] [CrossRef] [Green Version]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association Between BRAF V600E Mutation and Recurrence of Papillary Thyroid Cancer. J. Clin. Oncol. 2015, 33, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Walczyk, A.; Kowalska, A.; Kowalik, A.; Sygut, J.; Wypiórkiewicz, E.; Chodurska, R.; Pięciak, L.; Góźdź, S. The BRAFV600E mutation in papillary thyroid microcarcinoma: Does the mutation have an impact on clinical outcome? Clin. Endocrinol. 2014, 80, 899–904. [Google Scholar] [CrossRef]
- Mussazhanova, Z.; Matsuda, K.; Naruke, Y.; Mitsutake, N.; Stanojevic, B.; Rougounovitch, T.; Saenko, V.; Suzuki, K.; Nishihara, E.; Hirokawa, M.; et al. Significance of p53-binding protein 1 (53BP1) expression in thyroid papillary microcarcinoma: Association withBRAFV600Emutation status. Histopathology 2013, 63, 726–734. [Google Scholar] [CrossRef]
- Chung, S.Y.; Lee, J.S.; Lee, H.; Park, S.H.; Kim, S.J.; Ryu, H.S. Cytomorphological Factors and BRAF Mutation Predicting Risk of Lymph Node Metastasis in Preoperative Liquid-Based Fine Needle Aspirations of Papillary Thyroid Carcinoma. Acta Cytol. 2013, 57, 252–258. [Google Scholar] [CrossRef]
- Choi, S.Y.; Park, H.; Kang, M.K.; Lee, D.K.; Lee, K.D.; Lee, H.S.; Kim, S.W.; Lee, E.N.; Hong, J.C. The relationship between the BRAFV600E mutation in papillary thyroid microcarcinoma and clinicopathologic factors. World J. Surg. Oncol. 2013, 11, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virk, R.K.; Van Dyke, A.L.; Finkelstein, A.; Prasad, A.; Gibson, J.; Hui, P.; Theoharis, C.G.; Carling, T.; A Roman, S.; A Sosa, J.; et al. BRAFV600E mutation in papillary thyroid microcarcinoma: A genotype–phenotype correlation. Mod. Pathol. 2012, 26, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Rossi, E.D.; Martini, M.; Bd, S.C.; Lombardi, C.P.; Pontecorvi, A.; Vellone, V.G.; Zannoni, G.F.; Larocca, L.M.; Fadda, G. BRAF(V600E) mutation analysis on liquid-based cytology-processed aspiration biopsies predicts bilaterality and lymph node involvement in papillary thyroid microcarcinoma. Cancer Cytopathol. 2012, 121, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, I.; Iervasi, G.; Mazzanti, C.M.; Lessi, F.; Tomei, S.; Naccarato, A.G.; Aretini, P.; Alberti, B.; Di Coscio, G.; Bevilacqua, G.; et al. Detection of the BRAFV600E Mutation in Fine Needle Aspiration Cytology of Thyroid Papillary Microcarcinoma Cells Selected by Manual Macrodissection: An Easy Tool to Improve the Preoperative Diagnosis. Thyroid 2012, 22, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Kurtulmus, N.; Duren, M.; Ince, U.; Yakicier, M.C.; Peker, O.; Aydın, O.; Altiok, E.; Giray, S.; Azizlerli, H. BRAFV600E mutation in Turkish patients with papillary thyroid cancer: Strong correlation with indicators of tumor aggressiveness. Endocrine 2012, 42, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.-L.; Wang, O.-C.; Zhang, X.-H.; Dai, X.-X.; Hu, X.-Q.; Qu, J.-M. The BRAF Mutation Is Predictive of Aggressive Clinicopathological Characteristics in Papillary Thyroid Microcarcinoma. Ann. Surg. Oncol. 2010, 17, 3294–3300. [Google Scholar] [CrossRef] [PubMed]
- Basolo, F.; Torregrossa, L.; Giannini, R.; Miccoli, M.; Lupi, C.; Sensi, E.; Berti, P.; Elisei, R.; Vitti, P.; Baggiani, A. Correlation between the BRAF V600E Mutation and Tumor Invasiveness in Papillary Thyroid Carcinomas Smaller than 20 Millimeters: Analysis of 1060 Cases. J. Clin. Endocrinol. Metab. 2010, 95, 4197–4205. [Google Scholar] [CrossRef] [Green Version]
- Lee, X.; Gao, M.; Ji, Y.; Yü, Y.; Feng, Y.; Li, Y.; Zhang, Y.; Cheng, W.; Zhao, W. Analysis of Differential BRAFV600E Mutational Status in High Aggressive Papillary Thyroid Microcarcinoma. Ann. Surg. Oncol. 2008, 16, 240–245. [Google Scholar] [CrossRef]
- Kwak, J.Y.; Kim, E.-K.; Chung, W.Y.; Moon, H.J.; Kim, M.J.; Choi, J.R. Association of BRAFV600E Mutation with Poor Clinical Prognostic Factors and US Features in Korean Patients with Papillary Thyroid Microcarcinoma. Radiology 2009, 253, 854–860. [Google Scholar] [CrossRef]
- Min, H.S.; Choe, G.; Kim, S.-W.; Park, Y.J.; Park, D.J.; Youn, Y.-K.; Park, S.H.; Cho, B.Y.; Park, S.Y. S100A4 expression is associated with lymph node metastasis in papillary microcarcinoma of the thyroid. Mod. Pathol. 2008, 21, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Frasca, F.; Nucera, C.; Pellegriti, G.; Gangemi, P.; Attard, M.; Stella, M.; Loda, M.; Vella, V.; Giordano, C.; Trimarchi, F.; et al. BRAF(V600E) mutation and the biology of papillary thyroid cancer. Endocrine-Related Cancer 2008, 15, 191–205. [Google Scholar] [CrossRef]
- Rodolico, V.; Cabibi, D.; Pizzolanti, G.; Richiusa, P.; Gebbia, N.; Martorana, A.; Russo, A.; Amato, M.C.; Galluzzo, A.; Giordano, C. BRAFV600E mutation and p27kip1 expression in papillary carcinomas of the thyroid ≤1 cm and their paired lymph node metastases. Cancer 2007, 110, 1218–1226. [Google Scholar] [CrossRef] [Green Version]
- Lupi, C.; Giannini, R.; Ugolini, C.; Proietti, A.; Berti, P.; Minuto, M.; Materazzi, G.; Elisei, R.; Santoro, M.; Miccoli, P.; et al. Association of BRAF V600E Mutation with Poor Clinicopathological Outcomes in 500 Consecutive Cases of Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2007, 92, 4085–4090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.Y.; Kim, W.B.; Song, J.Y.; Rhee, Y.S.; Gong, G.; Cho, Y.M.; Kim, S.Y.; Kim, S.C.; Hong, S.J. The BRAFV600E mutation is not associated with poor prognostic factors in Korean patients with conventional papillary thyroid microcarcinoma. Clin. Endocrinol. 2005, 63, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzini, L.; Baroli, A.; Marzoli, L.; Guglielmi, R.; Papini, E. Cancer recurrence in papillary thyroid microcarcinoma: A multivariate analysis on 231 patients with a 12-year follow-up. Minerva Endocrinol. 2013, 38. [Google Scholar]
- Al-Qurayshi, Z.; Nilubol, N.; Tufano, R.P.; Kandil, E. Wolf in Sheep’s Clothing: Papillary Thyroid Microcarcinoma in the US. J. Am. Coll. Surg. 2020, 230, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. BRAF Mutation in Papillary Thyroid Microcarcinoma: The Promise of Better Risk Management. Ann. Surg. Oncol. 2009, 16, 801–803. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.C.; Choi, E.C.; Yoon, Y.-H.; Kim, E.-H.; Koo, B.S. Central lymph node metastases in unilateral papillary thyroid microcarcinoma. Br. J. Surg. 2009, 96, 253–257. [Google Scholar] [CrossRef]
- Wada, N.; Duh, Q.-Y.; Sugino, K.; Iwasaki, H.; Kameyama, K.; Mimura, T.; Ito, K.; Takami, H.; Takanashi, Y. Lymph Node Metastasis from 259 Papillary Thyroid Microcarcinomas: Frequency, Pattern of Occurrence and Recurrence, and Optimal Strategy for Neck Dissection. Ann. Surg. 2003, 237, 399. [Google Scholar] [CrossRef]
- Miccoli, P.; Minuto, M.N.; Ugolini, C.; Panicucci, E.; Berti, P.; Massi, M.; Basolo, F. Intrathyroidal Differentiated Thyroid Carcinoma: Tumor Size-Based Surgical Concepts. World J. Surg. 2007, 31, 888–894. [Google Scholar] [CrossRef]
- Lee, D.Y.; Hwang, S.M.; An, J.H.; Son, K.R.; Baek, S.-K.; Kim, S.G.; Chae, Y.S.; Jung, K.-Y. Predicting Extrathyroidal Extension in Patients With Papillary Thyroid Microcarcinoma According to a BRAF Mutation. Clin. Exp. Otorhinolaryngol. 2017, 10, 174–181. [Google Scholar] [CrossRef]
- Issa, P.P.; Omar, M.; Buti, Y.; Issa, C.P.; Chabot, B.; Carnabatu, C.J.; Munshi, R.; Hussein, M.; Aboueisha, M.; Shama, M.; et al. Hashimoto’s Thyroiditis Minimizes Lymph Node Metastasis in BRAF Mutant Papillary Thyroid Carcinomas. Biomedicines 2022, 10, 2051. [Google Scholar] [CrossRef]
- Tallini, G.; De Leo, A.; Repaci, A.; de Biase, D.; Reggiani, M.L.B.; Di Nanni, D.; Ambrosi, F.; Di Gioia, C.; Grani, G.; Rhoden, K.J.; et al. Does the Site of Origin of the Microcarcinoma with Respect to the Thyroid Surface Matter? A Multicenter Pathologic and Clinical Study for Risk Stratification. Cancers 2020, 12, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemeier, L.A.; Akatsu, H.K.; Song, C.; Carty, S.E.; Hodak, S.P.; Yip, L.; Ferris, R.L.; Tseng, G.C.; Seethala, R.R.; Lebeau, S.O.; et al. A combined molecular-pathologic score improves risk stratification of thyroid papillary microcarcinoma. Cancer 2011, 118, 2069–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apostol, D.C.; Giuşcă, S.E.; Căruntu, I.-D.; Lozneanu, L.; Andriescu, E.C.; Moscalu, M. Relationships between clinicopathological prognostic factors in papillary thyroid microcarcinoma: A refined analysis based on 428 cases. Int. J. Clin. Exp. Pathol. 2017, 10, 8944–8956. [Google Scholar]
- Tuttle, R.M.; Fagin, J.A.; Minkowitz, G.; Wong, R.J.; Roman, B.; Patel, S.; Untch, B.; Ganly, I.; Shaha, A.R.; Shah, J.P.; et al. Natural History and Tumor Volume Kinetics of Papillary Thyroid Cancers During Active Surveillance. JAMA Otolaryngol. Neck Surg. 2017, 143, 1015–1020. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Oda, H. Low-risk papillary microcarcinoma of the thyroid: A review of active surveillance trials. Eur. J. Surg. Oncol. (EJSO) 2017, 44, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Kandil, E.; Omar, M.; Aboueisha, M.; Attia, A.S.; Ali, K.M.; Abu Alhuda, R.F.; Issa, P.P.; Wolfe, S.; Omari, S.; Buti, Y.; et al. Efficacy and Safety of Radiofrequency Ablation of Thyroid Nodules: A Multi-institutional Prospective Cohort Study. Ann. Surg. 2022. [Google Scholar] [CrossRef]
- Kandil, E.; Omar, M.; Attia, A.S.; Shihabi, A.; Shaear, M.; Metz, T.; Issa, P.P.; Russell, J.O.; Tufano, R.P. Radiofrequency ablation as a novel modality in the USA for treating toxic thyroid nodules: Case series and literature review. Gland Surg. 2022, 11, 1574–1583. [Google Scholar] [CrossRef]
- Zhu, Y.; Che, Y.; Gao, S.; Ren, S.; Tong, M.; Wang, L.; Yang, F. Long-term follow-up results of PTMC treated by ultrasound-guided radiofrequency ablation: A retrospective study. Int. J. Hyperth. 2021, 38, 1225–1232. [Google Scholar] [CrossRef]
- Valcavi, R.; Riganti, F.; Bertani, A.; Formisano, D.; Pacella, C.M. Percutaneous Laser Ablation of Cold Benign Thyroid Nodules: A 3-Year Follow-Up Study in 122 Patients. Thyroid 2010, 20, 1253–1261. [Google Scholar] [CrossRef]
- Cesareo, R.; Naciu, A.; Iozzino, M.; Pasqualini, V.; Simeoni, C.; Casini, A.; Campagna, G.; Manfrini, S.; Tabacco, G.; Palermo, A. Nodule Size as Predictive Factor of Efficacy of Radiofrequency Ablation in Treating Autonomously Functioning Thyroid Nodules. Int. J. Hyperthermia 2018, 34, 617–623. [Google Scholar] [CrossRef] [Green Version]
- Greenland, S.; Robins, J.M. Estimation of a Common Effect Parameter from Sparse Follow-Up Data. Biometrics 1985, 41, 55. [Google Scholar] [CrossRef] [PubMed]
- Robins, J. A new approach to causal inference in mortality studies with a sustained exposure period—Application to control of the healthy worker survivor effect. Math. Model. 1986, 7, 1393–1512. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study Design | PTMC Total | % BRAF Mutated |
|---|---|---|---|---|---|
| Kim [10] | 2021 | South Korea | Retro | 2319 | 60.16 |
| Kim [11] | 2020 | Multicenter study | Retro | 743 | 32.44 |
| Zhou [12] | 2019 | China | Retro | 162 | 83.33 |
| Zheng [13] | 2019 | China | Retro | 299 | 83.28 |
| Chen [14] | 2019 | China | Retro | 182 | 47.80 |
| Ji [15] | 2019 | China | Retro | 89 | 75.28 |
| Lee [16] | 2019 | South Korea | Retro | 911 | 78.70 |
| Nechifor-Boilă [17] | 2018 | Romania | Retro | 25 | 36.00 |
| Shen [18] | 2018 | China | Retro | 236 | 62.29 |
| Goh [19] | 2018 | Singapore | Retro | 21 | 33.33 |
| Lu [20] | 2017 | China | Retro | 108 | 54.63 |
| Fakhruddin [21] | 2017 | Lebanon | Retro | 75 | 72.00 |
| Tallini [22] | 2015 | Italy | Retro | 264 | 50.00 |
| Park [23] | 2015 | South Korea | Retro | 460 | 79.78 |
| Bastos [24] | 2015 | Brazil | Retro | 40 | 52.50 |
| Xing [25] | 2015 | Multicenter | Retro | 534 | 41.01 |
| Walczyk [26] | 2013 | Poland | Retro | 113 | 69.03 |
| Mussazhanova [27] | 2013 | Japan | Retro | 13 | 46.15 |
| Chung [28] | 2013 | South Korea | Retro | 111 | 22.52 |
| Choi [29] | 2013 | South Korea | Retro | 101 | 71.29 |
| Virk [30] | 2012 | US | Retro | 124 | 70.16 |
| Rossi [31] | 2012 | Italy | Retro | 50 | 68.00 |
| Marchetti [32] | 2012 | Italy | Retro | 85 | 74.12 |
| Kurtulmus [33] | 2012 | Turkey | Retro | 64 | 29.69 |
| Lin [34] | 2010 | China | Retro | 61 | 34.43 |
| Basolo [35] | 2010 | Italy | Retro | 578 | 39.62 |
| Lee [36] | 2010 | China | Retro | 64 | 37.50 |
| Kwak [37] | 2009 | South Korea | Retro | 339 | 62.83 |
| Min [38] | 2008 | South Korea | Retro | 60 | 53.33 |
| Frasca [39] | 2008 | Italy | Retro | 103 | 24.27 |
| Rodolic [40] | 2007 | Italy | Retro | 214 | 41.12 |
| Lupi [41] | 2007 | Italy | Retro | 230 | 39.13 |
| Kim [42] | 2005 | South Korea | Retro | 60 | 51.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attia, A.S.; Hussein, M.; Issa, P.P.; Elnahla, A.; Farhoud, A.; Magazine, B.M.; Youssef, M.R.; Aboueisha, M.; Shama, M.; Toraih, E.; et al. Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies. Int. J. Mol. Sci. 2022, 23, 15626. https://doi.org/10.3390/ijms232415626
Attia AS, Hussein M, Issa PP, Elnahla A, Farhoud A, Magazine BM, Youssef MR, Aboueisha M, Shama M, Toraih E, et al. Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies. International Journal of Molecular Sciences. 2022; 23(24):15626. https://doi.org/10.3390/ijms232415626
Chicago/Turabian StyleAttia, Abdallah S., Mohammad Hussein, Peter P. Issa, Ahmad Elnahla, Ashraf Farhoud, Brandon M. Magazine, Mohanad R. Youssef, Mohamed Aboueisha, Mohamed Shama, Eman Toraih, and et al. 2022. "Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies" International Journal of Molecular Sciences 23, no. 24: 15626. https://doi.org/10.3390/ijms232415626
APA StyleAttia, A. S., Hussein, M., Issa, P. P., Elnahla, A., Farhoud, A., Magazine, B. M., Youssef, M. R., Aboueisha, M., Shama, M., Toraih, E., & Kandil, E. (2022). Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies. International Journal of Molecular Sciences, 23(24), 15626. https://doi.org/10.3390/ijms232415626