
Blood–Brain Barrier Transporters: Opportunities for Therapeutic Development in Ischemic Stroke

 ,
, 

Abstract
:1. Introduction
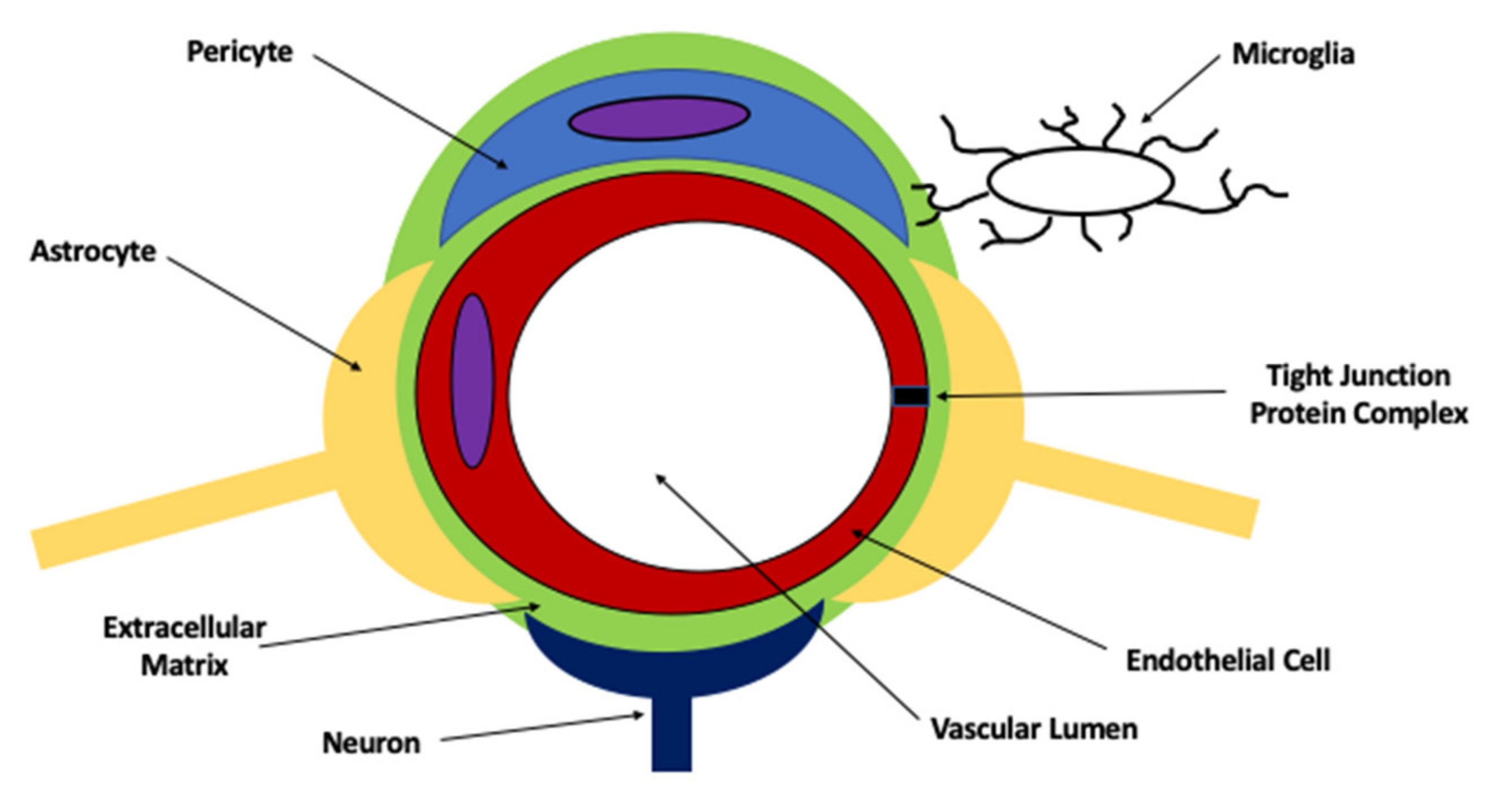
2. The Blood–Brain Barrier and the Neurovascular Unit
2.1. Blood–Brain Barrier Transport Mechanisms for Small Molecules
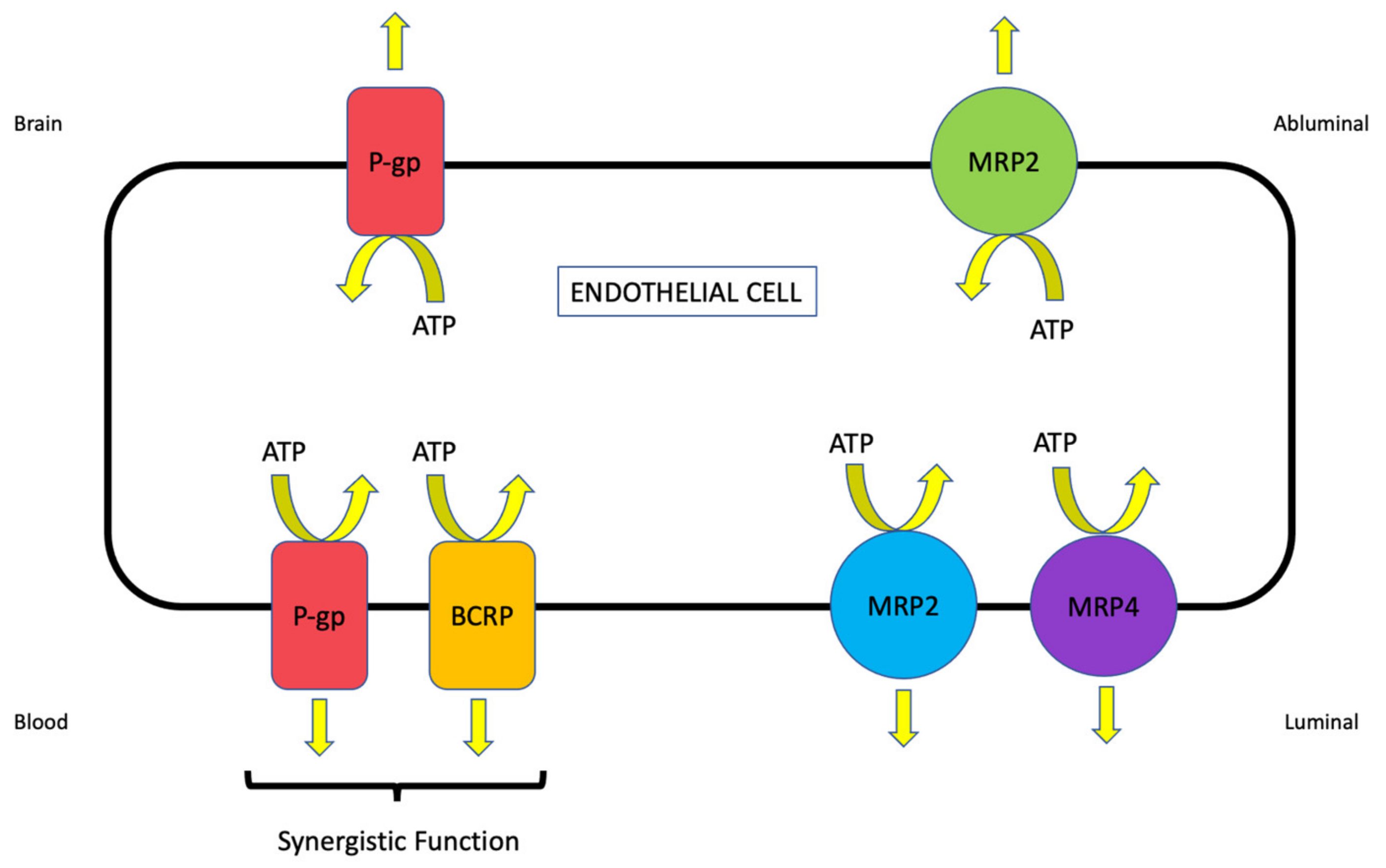
2.2. Role of Efflux Transporters in Drug Disposition to the Ischemic Brain
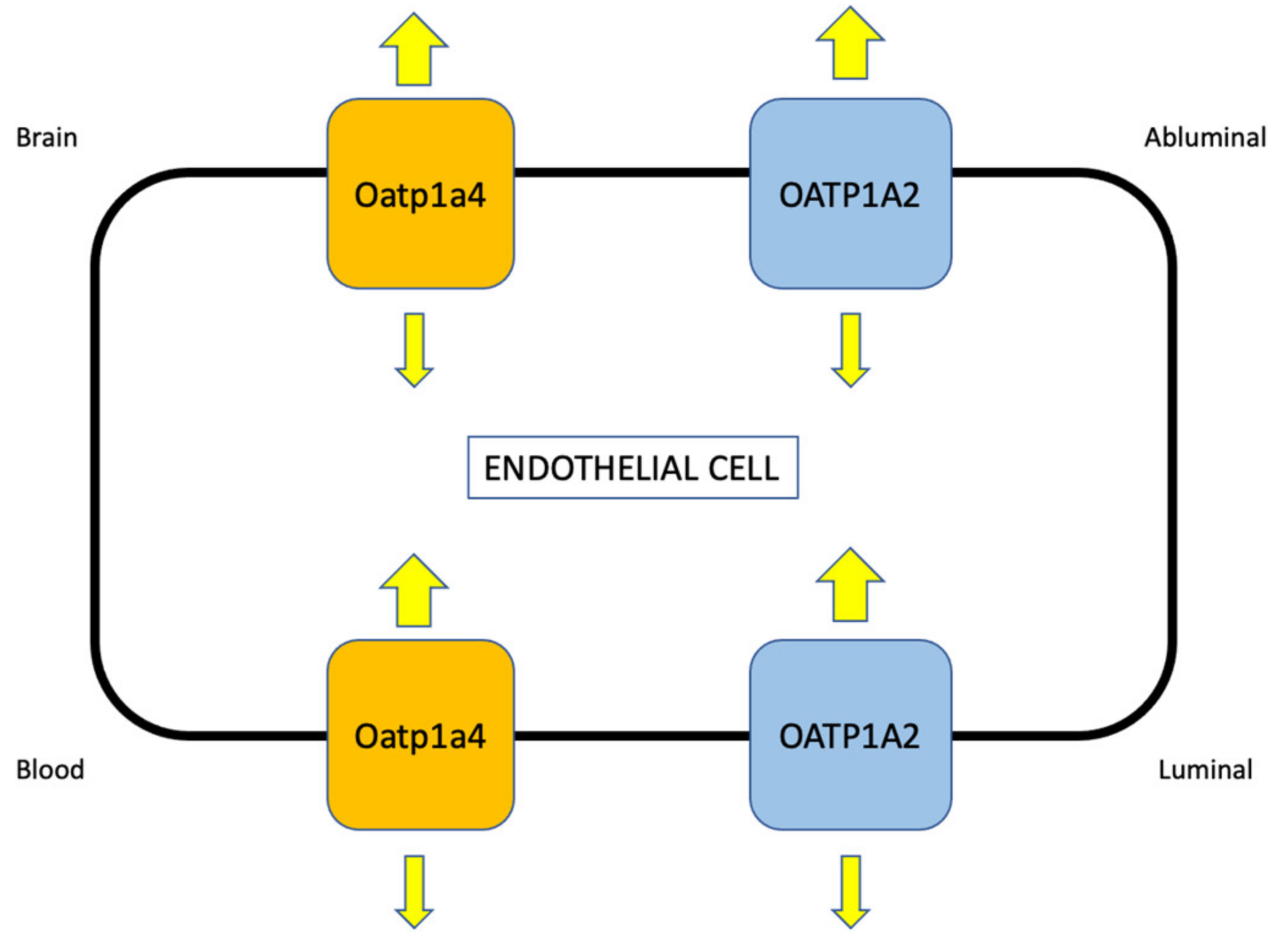
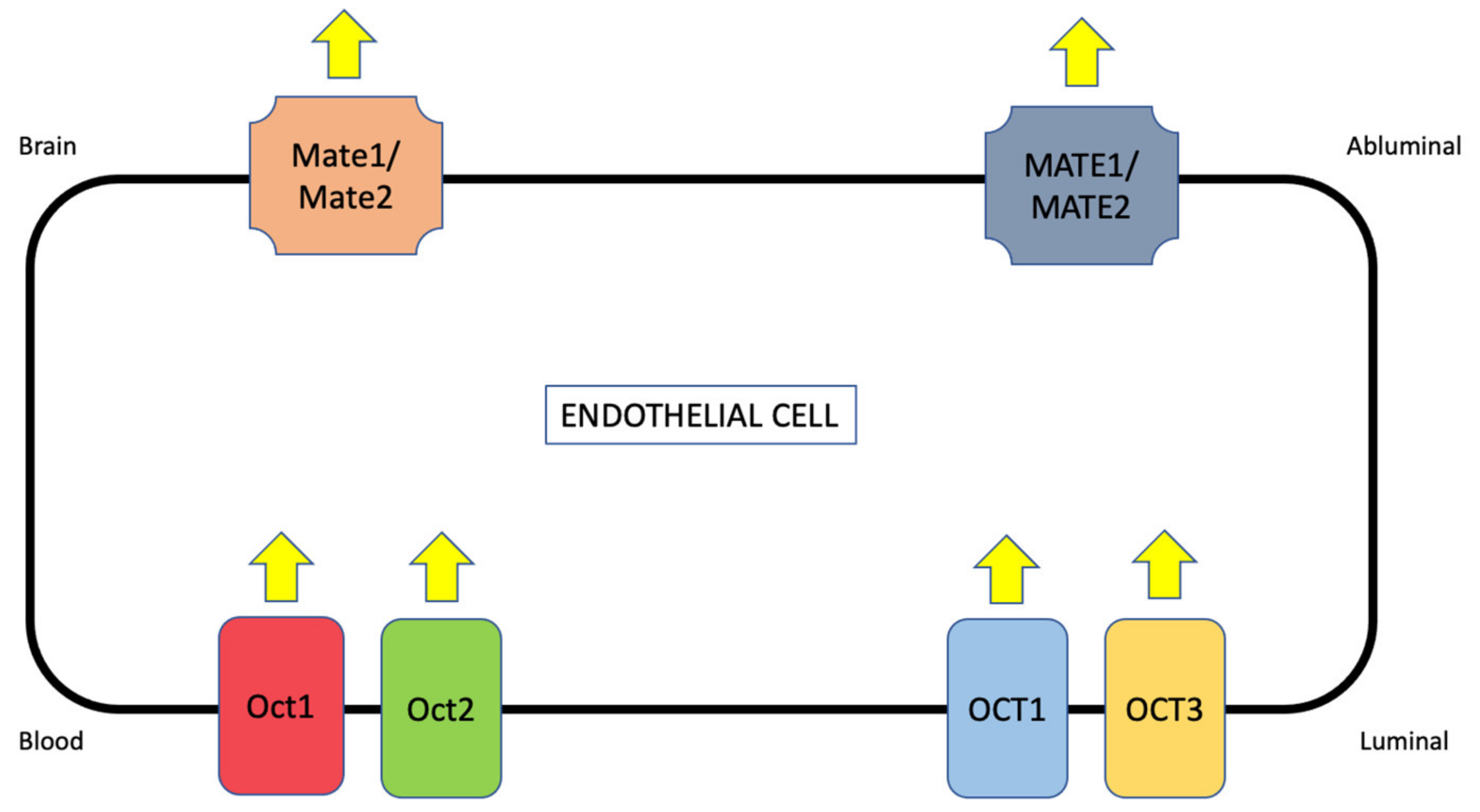
2.3. Role of Uptake Transporters in Drug Disposition to the Ischemic Brain
3. Transporter Studies for Ischemic Stroke—How to Advance the Field?
3.1. Species Selection
3.1.1. Application of Non-Human Primates to Preclinical Stroke Research
3.1.2. Application of Rodents (i.e., Mice and Rats) to Preclinical Stroke Research
3.2. Model Selection
3.2.1. Focal Cerebral Ischemia (i.e., Middle Cerebral Artery Occlusion (MCAO))
3.2.2. Embolic Stroke
3.2.3. Photothrombotic Stroke
3.2.4. Endothelin-1 Induced Stroke
4. Role of Co-Morbidities in Preclinical Transporter Studies in Stroke
4.1. Diabetes Mellitus
4.2. Tobacco Smoking
4.3. Atrial Fibrillation
4.4. Hypertension
4.5. Aging
5. Summary and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Levine, S.R.; Winn, H.R. Targeting ischemic penumbra: Part I—From pathophysiology to therapeutic strategy. J. Exp. Stroke Transl. Med. 2010, 3, 47–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manning, N.W.; Campbell, B.C.V.; Oxley, T.J.; Chapot, R. Acute ischemic stroke: Time, penumbra, and reperfusion. Stroke 2014, 45, 640–644. [Google Scholar] [CrossRef] [Green Version]
- Brzica, H.; Abdullahi, W.; Ibbotson, K.; Ronaldson, P.T. Role of Transporters in Central Nervous System Drug Delivery and Blood-Brain Barrier Protection: Relevance to Treatment of Stroke. J. Cent. Nerv. Syst. Dis. 2017, 9, 9. [Google Scholar] [CrossRef]
- Williams, E.I.; Betterton, R.D.; Davis, T.P.; Ronaldson, P.T. Transporter-Mediated Delivery of Small Molecule Drugs to the Brain: A Critical Mechanism That Can Advance Therapeutic Development for Ischemic Stroke. Pharmaceutics 2020, 12, 154. [Google Scholar] [CrossRef] [Green Version]
- The National Institute of Neurological Disorders and Stroke. rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N. Engl. J. Med. 1995, 333, 1581–1587. [Google Scholar] [CrossRef]
- O’Carroll, C.B.; Rubin, M.N.; Chong, B.W. What is the role for intra-arterial therapy in acute stroke intervention? Neurohospitalist 2015, 5, 122–132. [Google Scholar] [CrossRef] [Green Version]
- Tymianski, M. Combining neuroprotection with endovascular treatment of acute stroke: Is there hope? Stroke 2017, 48, 1700–1705. [Google Scholar] [CrossRef]
- Shi, L.; Rocha, M.; Leak, R.K.; Zhao, J.; Bhatia, T.; Mu, H.; Wei, Z.; Yu, F.; Weiner, S.L.; Ma, F.; et al. A new era for stroke therapy: Integrating neurovascular protection with optimal reperfusion. J. Cereb. Blood Flow Metab. 2018, 38, 2073–2091. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised Trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef]
- Pan, J.; Konstas, A.-A.; Bateman, B.; Ortolano, G.A.; Pile-Spellman, J. Reperfusion injury following cerebral ischemia: Patho-physiology, MR imaging, and potential therapies. Neuroradiology 2007, 49, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Candelario-Jalil, E. Injury and repair mechanisms in ischemic stroke: Considerations for the development of novel neuro-therapeutics. Curr. Opin. Investig. Drugs 2009, 10, 644–654. [Google Scholar]
- Eltzschig, H.K.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [Green Version]
- Nour, M.; Scalzo, F.; Liebeskind, D.S. Ischemia-Reperfusion Injury in Stroke. Interv. Neurol. 2012, 1, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, W.; Tripathi, D.; Ronaldson, P.T. Blood-brain barrier dysfunction in ischemic stroke: Targeting tight junctions and transporters for vascular protection. Am. J. Physiol.-Cell Physiol. 2018, 315, C343–C356. [Google Scholar] [CrossRef]
- Turner, R.C.; Lucke-Wold, B.; Lucke-Wold, N.; Elliott, A.S.; Logsdon, A.F.; Rosen, C.L.; Huber, J.D. Neuroprotection for is-chemic stroke: Moving past shortcomings and identifying promising directions. Int. J. Mol. Sci. 2013, 14, 1890–1917. [Google Scholar] [CrossRef]
- Kågedal, M.; Nilsson, D.; Huledal, G.; Reinholdsson, I.; Cheng, Y.-F.; Asenblad, N.; Pekar, D.; Borgå, O. A Study of Organic Acid Transporter-Mediated Pharmacokinetic Interaction Between NXY-059 and Cefuroxime. J. Clin. Pharmacol. 2007, 47, 1043–1048. [Google Scholar] [CrossRef]
- Sanchez-Covarrubias, L.; Slosky, L.; Thompson, B.; Davis, T.; Ronaldson, P. Transporters at CNS Barrier Sites: Obstacles or Opportunities for Drug Delivery? Curr. Pharm. Des. 2014, 20, 1422–1449. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, B.T.; Ocheltree, S.M.; Norwood, K.M.; Egleton, R.D. Decreased blood-brain barrier permeability to fluorescein in streptozotocin-treated rats. Neurosci. Lett. 2007, 411, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Okamura, T.; Okada, M.; Kikuchi, T.; Wakizaka, H.; Zhang, M.-R. Mechanisms of glutathione-conjugate efflux from the brain into blood: Involvement of multiple transporters in the course. J. Cereb. Blood Flow Metab. 2020, 40, 116–125. [Google Scholar] [CrossRef]
- Li, J.; Zheng, M.; Shimoni, O.; Banks, W.A.; Bush, A.I.; Gamble, J.R.; Shi, B. Development of Novel Therapeutics Targeting the Blood–Brain Barrier: From Barrier to Carrier. Adv. Sci. 2021, 8, 2101090. [Google Scholar] [CrossRef]
- Abdullahi, W.; Davis, T.P.; Ronaldson, P.T. Functional expression of P-glycoprotein and organic anion transporting polypep-tides at the blood-brain barrier: Understanding transport mechanisms for improved cns drug delivery? AAPS J. 2017, 19, 931–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vemula, S.; Roder, K.E.; Yang, T.; Bhat, G.J.; Thekkumkara, T.J.; Abbruscato, T.J. A Functional Role for Sodium-Dependent Glucose Transport across the Blood-Brain Barrier during Oxygen Glucose Deprivation. J. Pharmacol. Exp. Ther. 2009, 328, 487–495. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Yuen, N.; Wallace, B.K.; Wulff, H.; O’Donnell, M.E. Blood brain barrier KCa3.1 channels: Evidence for a role in brain Na uptake and edema during ischemic stroke. Stroke 2015, 46, 237–244. [Google Scholar] [CrossRef]
- O’Donnell, M.E. Blood–Brain Barrier Na Transporters in Ischemic Stroke. Adv. Pharmacol. 2014, 71, 113–146. [Google Scholar] [CrossRef]
- Shah, K.K.; Boreddy, P.R.; Abbruscato, T.J. Nicotine pre-exposure reduces stroke-induced glucose transporter-1 activity at the blood–brain barrier in mice. Fluids Barriers CNS 2015, 12, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Spudich, A.; Kilic, E.; Xing, H.; Kilic, Ü.; Rentsch, K.M.; Wunderli-Allenspach, H.; Bassetti, C.L.; Hermann, D.M. Inhibition of multidrug resistance transporter-1 facilitates neuroprotective therapies after focal cerebral ischemia. Nat. Neurosci. 2006, 9, 487–488. [Google Scholar] [CrossRef]
- Cen, J.; Liu, L.; Li, M.-S.; He, L.; Wang, L.-J.; Liu, Y.-Q.; Liu, M.; Ji, B.-S. Alteration in P-glycoprotein at the blood–brain barrier in the early period of MCAO in rats. J. Pharm. Pharmacol. 2013, 65, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Demars, K.M.; Yang, C.; Hawkins, E.K.; McCrea, A.O.; Siwarski, D.M.; Candelario-Jalil, E. Spatiotemporal Changes in P-glycoprotein Levels in Brain and Peripheral Tissues Following Ischemic Stroke in Rats. J. Exp. Neurosci. 2017, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Yemisci, M.; Caban-Toktas, S.; Gürsoy-Ozdemir, Y.; Lule, S.; Novoa-Carballal, R.; Riguera, R.; Fernandez-Megia, E.; Andrieux, K.; Couvreur, P.; Capan, Y.; et al. Systemically Administered Brain-Targeted Nanoparticles Transport Peptides across the Blood—Brain Barrier and Provide Neuroprotection. J. Cereb. Blood Flow Metab. 2015, 35, 469–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, Q.; Hu, P.; Xu, Y.; Cheng, T.; Wei, C.; Pan, L.; Shi, J. Simultaneous Blood–Brain Barrier Crossing and Protection for Stroke Treatment Based on Edaravone-Loaded Ceria Nanoparticles. ACS Nano 2018, 12, 6794–6805. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Zhang, Y.; Wang, L.; Li, G.; Gao, J.; Wang, Y. Development of L-carnosine functionalized iron oxide nanoparticles loaded with dexamethasone for simultaneous therapeutic potential of blood brain barrier crossing and ischemic stroke treatment. Drug Deliv. 2021, 28, 380–389. [Google Scholar] [CrossRef]
- Montaner, J.; Cano-Sarabia, M.; Simats, A.; Hernández-Guillamon, M.; Rosell, A.; Maspoch, D.; Campos-Martorell, M. Charge effect of a liposomal delivery system encapsulating simvastatin to treat experimental ischemic stroke in rats. Int. J. Nanomed. 2016, 11, 3035–3048. [Google Scholar] [CrossRef] [Green Version]
- Al-Ahmady, Z.S.; Jasim, D.; Ahmad, S.S.; Wong, R.; Haley, M.; Coutts, G.; Schiessl, I.; Allan, S.M.; Kostarelos, K. Selective Liposomal Transport through Blood Brain Barrier Disruption in Ischemic Stroke Reveals Two Distinct Therapeutic Opportunities. ACS Nano 2019, 13, 12470–12486. [Google Scholar] [CrossRef]
- Santos, S.D.; Xavier, M.; Leite, D.M.; Moreira, D.; Custódio, B.; Torrado, M.; Castro, R.; Leiro, V.; Rodrigues, J.; Tomás, H.; et al. PAMAM dendrimers: Blood-brain barrier transport and neuronal uptake after focal brain ischemia. J. Control. Release 2018, 291, 65–79. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Pardridge, W.M. Neuroprotection in Transient Focal Brain Ischemia After Delayed Intravenous Administration of Brain-Derived Neurotrophic Factor Conjugated to a Blood-Brain Barrier Drug Targeting System. Stroke 2001, 32, 1378–1384. [Google Scholar] [CrossRef] [Green Version]
- Daneman, R.; Prat, A. The blood-brain barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef] [Green Version]
- Iadecola, C. The Neurovascular Unit Coming of Age: A Journey through Neurovascular Coupling in Health and Disease. Neuron 2017, 96, 17–42. [Google Scholar] [CrossRef] [Green Version]
- DiNapoli, V.A.; Huber, J.D.; Houser, K.; Li, X.; Rosen, C.L. Early disruptions of the blood–brain barrier may contribute to exacerbated neuronal damage and prolonged functional recovery following stroke in aged rats. Neurobiol. Aging 2008, 29, 753–764. [Google Scholar] [CrossRef] [Green Version]
- Sakadžić, S.; Lee, J.; Boas, D.A.; Ayata, C. High-resolution in vivo optical imaging of stroke injury and repair. Brain Res. 2015, 1623, 174–192. [Google Scholar] [CrossRef] [Green Version]
- Winkler, L.; Blasig, R.; Breitkreuz-Korff, O.; Berndt, P.; Dithmer, S.; Helms, H.C.C.; Puchkov, D.; Devraj, K.; Kaya, M.; Qin, Z.; et al. Tight junctions in the blood–brain barrier promote edema formation and infarct size in stroke–Ambivalent effects of sealing proteins. J. Cereb. Blood Flow Metab. 2021, 41, 132–145. [Google Scholar] [CrossRef]
- Lochhead, J.; McCaffrey, G.; Quigley, C.E.; Finch, J.; Demarco, K.M.; Nametz, N.; Davis, T.P. Oxidative Stress Increases Blood–Brain Barrier Permeability and Induces Alterations in Occludin during Hypoxia-Reoxygenation. J. Cereb. Blood Flow Metab. 2010, 30, 1625–1636. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, Y.; Campbell, M. Tight junction modulation at the blood-brain barrier: Current and future perspectives. Biochim. Biophys. Acta (BBA)—Biomembr. 2020, 1862, 183298. [Google Scholar] [CrossRef]
- Abbott, N.J.; Patabendige, A.A.; Dolman, D.E.; Yusof, S.R.; Begley, D.J. Structure and function of the blood-brain barrier. Neurobiol. Dis. 2010, 37, 13–25. [Google Scholar] [CrossRef]
- Greene, C.; Hanley, N.; Campbell, M. Claudin-5: Gatekeeper of neurological function. Fluids Barriers CNS 2019, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Lochhead, J.J.; Yang, J.; Ronaldson, P.T.; Davis, T.P. Structure, Function, and Regulation of the Blood-Brain Barrier Tight Junction in Central Nervous System Disorders. Front. Physiol. 2020, 11, 914. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Campbell, M.; Tachibana, K.; Okada, Y.; Kondoh, M. Claudin-5: A Pharmacological Target to Modify the Permeability of the Blood–Brain Barrier. Biol. Pharm. Bull. 2021, 44, 1380–1390. [Google Scholar] [CrossRef]
- Nitta, T.; Hata, M.; Gotoh, S.; Seo, Y.; Sasaki, H.; Hashimoto, N.; Furuse, M.; Tsukita, S. Size-selective loosening of the blood-brain barrier in claudin-5-deficient mice. J. Cell Biol. 2003, 161, 653–660. [Google Scholar] [CrossRef]
- McCaffrey, G.; Seelbach, M.J.; Staatz, W.D.; Nametz, N.; Quigley, C.; Campos, C.R.; Brooks, T.A.; Davis, T.P. Occludin oli-gomeric assembly at tight junctions of the blood-brain barrier is disrupted by peripheral inflammatory hyperalgesia. J. Neuro-chem. 2008, 106, 2395–2409. [Google Scholar]
- McCaffrey, G.; Willis, C.L.; Staatz, W.D.; Nametz, N.; Quigley, C.A.; Hom, S.; Lochhead, J.J.; Davis, T.P. Occludin oligomeric assemblies at tight junctions of the blood-brain barrier are altered by hypoxia and reoxygenation stress. J. Neurochem. 2009, 110, 58–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Qu, M.; Li, Y.; Wang, L.; Zhang, L.; Wang, Y.; Tang, Y.; Tian, H.-L.; Zhang, Z.; Yang, G.-Y. MicroRNA-126-3p/-5p Overexpression Attenuates Blood-Brain Barrier Disruption in a Mouse Model of Middle Cerebral Artery Occlusion. Stroke 2020, 51, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Bhowmick, S.; D’Mello, V.; Caruso, D.; Wallerstein, A.; Abdul-Muneer, P. Impairment of pericyte-endothelium crosstalk leads to blood-brain barrier dysfunction following traumatic brain injury. Exp. Neurol. 2019, 317, 260–270. [Google Scholar] [CrossRef]
- Xia, Y.-P.; He, Q.-W.; Li, Y.-N.; Chen, S.-C.; Huang, M.; Wang, Y.; Gao, Y.; Huang, Y.; Wang, M.-D.; Mao, L.; et al. Recombinant Human Sonic Hedgehog Protein Regulates the Expression of ZO-1 and Occludin by Activating Angiopoietin-1 in Stroke Damage. PLoS ONE 2013, 8, e68891. [Google Scholar] [CrossRef] [Green Version]
- Seelbach, M.J.; Brooks, T.A.; Egleton, R.D.; Davis, T.P. Peripheral inflammatory hyperalgesia modulates morphine delivery to the brain: A role for P-glycoprotein. J. Neurochem. 2007, 102, 1677–1690. [Google Scholar] [CrossRef]
- Huber, J.D.; Witt, K.A.; Hom, S.; Egleton, R.D.; Mark, K.S.; Davis, T.P. Inflammatory pain alters blood-brain barrier permea-bility and tight junctional protein expression. Am. J. Physiol. Heart Circ. Physiol. 2001, 280, H1241–H1248. [Google Scholar] [CrossRef]
- Campos, C.R.; Ocheltree, S.M.; Hom, S.; Egleton, R.D.; Davis, T.P. Nociceptive inhibition prevents inflammatory pain induced changes in the blood–brain barrier. Brain Res. 2008, 1221, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Ronaldson, P.T.; Demarco, K.M.; Sanchez-Covarrubias, L.; Solinsky, C.M.; Davis, T.P. Transforming growth factor-beta sig-naling alters substrate permeability and tight junction protein expression at the blood-brain barrier during inflammatory pain. J. Cereb. Blood Flow Metab. 2009, 29, 1084–1098. [Google Scholar] [CrossRef] [Green Version]
- Lampugnani, M.G.; Dejana, E. Adherens junctions in endothelial cells regulate vessel maintenance and angiogenesis. Thromb. Res. 2007, 120, S1–S6. [Google Scholar] [CrossRef]
- Williams, M.J.; Lowrie, M.B.; Bennett, J.P.; Firth, J.A.; Clark, P. Cadherin-10 is a novel blood–brain barrier adhesion molecule in human and mouse. Brain Res. 2005, 1058, 62–72. [Google Scholar] [CrossRef]
- Meng, W.; Takeichi, M. Adherens Junction: Molecular Architecture and Regulation. Cold Spring Harb. Perspect. Biol. 2009, 1, a002899. [Google Scholar] [CrossRef] [Green Version]
- Artus, C. The Wnt/planar cell polarity signaling pathway contributes to the integrity of tight junctions in brain endo-thelial cells. J. Cereb. Blood Flow Metab. 2014, 34, 433–440. [Google Scholar] [CrossRef]
- Laksitorini, M.D. Modulation of Wnt/beta-catenin signaling promotes blood-brain barrier phenotype in cultured brain endothelial cells. Sci. Rep. 2019, 9, 19718. [Google Scholar] [CrossRef] [Green Version]
- Steiner, E.; Enzmann, G.U.; Lyck, R.; Lin, S.; Rüegg, M.A.; Kroger, S.; Engelhardt, B. The heparan sulfate proteoglycan agrin contributes to barrier properties of mouse brain endothelial cells by stabilizing adherens junctions. Cell Tissue Res. 2014, 358, 465–479. [Google Scholar] [CrossRef] [Green Version]
- Willis, C.L. Partial recovery of the damaged rat blood-brain barrier is mediated by adherens junction complexes, ex-tracellular matrix remodeling and macrophage infiltration following focal astrocyte loss. Neuroscience 2013, 250, 773–785. [Google Scholar] [CrossRef] [Green Version]
- Nakano-Doi, A.; Sakuma, R.; Matsuyama, T.; Nakagomi, T. Ischemic stroke activates the VE-cadherin promoter and increases VE-cadherin expression in adult mice. Histol. Histopathol. 2018, 33, 507–521. [Google Scholar]
- Oldendorf, W.H.; Cornford, M.E.; Brown, W.J. The large apparent work capability of the blood-brain barrier: A study of the mitochondrial content of capillary endothelial cells in brain and other tissues of the rat. Ann. Neurol. 1977, 1, 409–417. [Google Scholar] [CrossRef]
- Yang, J.; Reilly, B.G.; Davis, T.P.; Ronaldson, P.T. Modulation of Opioid Transport at the Blood-Brain Barrier by Altered ATP-Binding Cassette (ABC) Transporter Expression and Activity. Pharmaceutics 2018, 10, 192. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Yee, S.W.; Kim, R.B.; Giacomini, K.M. SLC transporters as therapeutic targets: Emerging opportunities. Nat. Rev. Drug Discov. 2015, 14, 543–560. [Google Scholar] [CrossRef] [Green Version]
- Ose, A.; Kusuhara, H.; Endo, C.; Tohyama, K.; Miyajima, M.; Kitamura, S.; Sugiyama, Y. Functional Characterization of Mouse Organic Anion Transporting Peptide 1a4 in the Uptake and Efflux of Drugs Across the Blood-Brain Barrier. Drug Metab. Dispos. 2010, 38, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, L.; Black, D.; Raman, C.; Woodford, K.; Zhou, M.; Haggerty, J.; Yan, A.; Cwirla, S.; Grindstaff, K. Subcellular localization of transporters along the rat blood–brain barrier and blood–cerebral-spinal fluid barrier by in vivo biotinylation. Neuroscience 2008, 155, 423–438. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; Stieger, B.; Noé, B.; Fritschy, J.-M.; Meier, P.J. Localization of the organic anion transporting polypeptide 2 (Oatp2) in capillary endothelium and choroid plexus epithelium of rat brain. J. Histochem. Cytochem. 1999, 47, 1255–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, L.M.; Woodford, K.; Zhou, M.; Black, D.S.; Haggerty, J.E.; Tate, E.H.; Grindstaff, K.K.; Mengesha, W.; Raman, C.; Zerangue, N. Expression of the Thyroid Hormone Transporters Monocarboxylate Transporter-8 (SLC16A2) and Organic Ion Transporter-14 (SLCO1C1) at the Blood-Brain Barrier. Endocrinology 2008, 149, 6251–6261. [Google Scholar] [CrossRef]
- Kubo, Y.; Ohtsuki, S.; Uchida, Y.; Terasaki, T. Quantitative Determination of Luminal and Abluminal Membrane Distributions of Transporters in Porcine Brain Capillaries by Plasma Membrane Fractionation and Quantitative Targeted Proteomics. J. Pharm. Sci. 2015, 104, 3060–3068. [Google Scholar] [CrossRef] [Green Version]
- Gao, B.; Hagenbuch, B.; Kullak-Ublick, G.A.; Benke, D.; Aguzzi, A.; Meier, P.J. Organic anion-transporting polypeptides mediate transport of opioid peptides across blood-brain barrier. J. Pharmacol. Exp. Ther. 2000, 294, 73–79. [Google Scholar]
- Kalliokoski, A.; Niemi, M. Impact of OATP transporters on pharmacokinetics. J. Cereb. Blood Flow Metab. 2009, 158, 693–705. [Google Scholar] [CrossRef] [Green Version]
- Lee, W. Polymorphisms in human organic anion-transporting polypeptide 1A2 (OATP1A2): Implications for altered drug disposition and central nervous system drug entry. J. Biol. Chem. 2005, 280, 9610–9617. [Google Scholar] [CrossRef] [Green Version]
- Bronger, H.; Koenig, J.; Kopplow, K.; Steiner, H.-H.; Ahmadi, R.; Herold-Mende, C.; Keppler, D.; Nies, A.T. ABCC Drug Efflux Pumps and Organic Anion Uptake Transporters in Human Gliomas and the Blood-Tumor Barrier. Cancer Res. 2005, 65, 11419–11428. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, G.N.; Georgian, A.R.; Sanderson, L.; Vizcay-Barrena, G.; Brown, R.C.; Muresan, P.; Fleck, R.; Thomas, S.A. Organic cation transporter 1 (OCT1) is involved in pentamidine transport at the human and mouse blood-brain barrier (BBB). PLoS ONE 2017, 12, e0173474. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-J.; Tai, Y.; Huang, M.-T.; Tsai, Y.-F.; Hsu, H.-J.; Tzen, K.-Y.; Liou, H.-H. Cellular localization of the organic cation transporters, OCT1 and OCT2, in brain microvessel endothelial cells and its implication for MPTP transport across the blood-brain barrier and MPTP-induced dopaminergic toxicity in rodents. J. Neurochem. 2010, 114, 717–727. [Google Scholar] [CrossRef]
- Soontornmalai, A.; Vlaming, M.L.; Fritschy, J.M. Differential, strain-specific cellular and subcellular distribution of multi-drug transporters in murine choroid plexus and blood-brain barrier. Neuroscience 2006, 138, 159–169. [Google Scholar] [CrossRef]
- Beaulieu, É.; Demeule, M.; Ghitescu, L.; Béliveau, R. P-glycoprotein is strongly expressed in the luminal membranes of the endothelium of blood vessels in the brain. Biochem. J. 1997, 326, 539–544. [Google Scholar] [CrossRef] [Green Version]
- Bendayan, R.; Ronaldson, P.T.; Gingras, D.; Bendayan, M. In Situ Localization of P-glycoprotein (ABCB1) in Human and Rat Brain. J. Histochem. Cytochem. 2006, 54, 1159–1167. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, A.; Terasaki, T.; Takabatake, Y.; Tenda, Y.; Tamai, I.; Yamashima, T.; Moritani, S.; Tsuruo, T.; Yamashita, J. P-glycoprotein as the drug efflux pump in primary cultured bovine brain capillary endothelial cells. Life Sci. 1992, 51, 1427–1437. [Google Scholar] [CrossRef]
- Watanabe, D. Characterization of a Primate Blood-Brain Barrier Co-Culture Model Prepared from Primary Brain En-dothelial Cells, Pericytes and Astrocytes. Pharmaceutics 2021, 13, 1484. [Google Scholar] [CrossRef]
- Virgintino, D.; Robertson, D.; Errede, M.; Benagiano, V.; Girolamo, F.; Maiorano, E.; Roncali, L.; Bertossi, M. Expression of P-Glycoprotein in Human Cerebral Cortex Microvessels. J. Histochem. Cytochem. 2002, 50, 1671–1676. [Google Scholar] [CrossRef] [Green Version]
- Bakhsheshian, J.; Wei, B.-R.; Hall, M.D.; Simpson, R.M.; Gottesman, M.M. In Vivo Bioluminescent Imaging of ATP-Binding Cassette Transporter-Mediated Efflux at the Blood–Brain Barrier. Adv. Struct. Saf. Stud. 2016, 1461, 227–239. [Google Scholar] [CrossRef]
- Hori, S. Functional expression of rat ABCG2 on the luminal side of brain capillaries and its enhancement by astro-cyte-derived soluble factor(s). J. Neurochem. 2004, 90, 526–536. [Google Scholar] [CrossRef]
- Cooray, H.C.; Blackmore, C.G.; Maskell, L.; Barrand, M.A. Localisation of breast cancer resistance protein in microvessel endothelium of human brain. NeuroReport 2002, 13, 2059–2063. [Google Scholar] [CrossRef]
- Kilic, E. ABCC1: A gateway for pharmacological compounds to the ischaemic brain. Brain 2008, 131, 2679–2689. [Google Scholar] [CrossRef] [Green Version]
- Leggas, M.; Adachi, M.; Scheffer, G.L.; Sun, D.; Wielinga, P.; Du, G.; Mercer, K.E.; Zhuang, Y.; Panetta, J.C.; Johnston, B.; et al. Mrp4 Confers Resistance to Topotecan and Protects the Brain from Chemotherapy. Mol. Cell. Biol. 2004, 24, 7612–7621. [Google Scholar] [CrossRef] [Green Version]
- Gutmann, H.; Török, M.; Fricker, G.; Huwyler, J.; Beglinger, C.; Drewe, J. Modulation of multidrug resistance protein expression in porcine brain capillary endothelial cells in vitro. Drug Metab. Dispos. 1999, 27, 937–941. [Google Scholar]
- Zhang, Y. Plasma membrane localization of multidrug resistance-associated protein homologs in brain capillary endo-thelial cells. J. Pharmacol. Exp. Ther. 2004, 311, 449–455. [Google Scholar] [CrossRef]
- Nies, A.; Jedlitschky, G.; König, J.; Herold-Mende, C.; Steiner, H.; Schmitt, H.-P.; Keppler, D. Expression and immunolocalization of the multidrug resistance proteins, MRP1–MRP6 (ABCC1–ABCC6), in human brain. Neuroscience 2004, 129, 349–360. [Google Scholar] [CrossRef]
- Klaassen, C.D.; Aleksunes, L.M. Xenobiotic, Bile Acid, and Cholesterol Transporters: Function and Regulation. Pharmacol. Rev. 2010, 62, 1–96. [Google Scholar] [CrossRef] [Green Version]
- Grube, M.; Hagen, P.; Jedlitschky, G. Neurosteroid Transport in the Brain: Role of ABC and SLC Transporters. Front. Pharmacol. 2018, 9, 354. [Google Scholar] [CrossRef]
- Sekhar, G.N.; Fleckney, A.L.; Boyanova, S.T.; Rupawala, H.; Lo, R.; Wang, H.; Farag, D.B.; Rahman, K.M.; Broadstock, M.; Reeves, S.; et al. Region-specific blood–brain barrier transporter changes leads to increased sensitivity to amisulpride in Alzheimer’s disease. Fluids Barriers CNS 2019, 16, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Sandoval, P.J.; Zorn, K.M.; Clark, A.M.; Ekins, S.; Wright, S.H. Assessment of Substrate-Dependent Ligand Interactions at the Organic Cation Transporter OCT2 Using Six Model Substrates. Mol. Pharmacol. 2018, 94, 1057–1068. [Google Scholar] [CrossRef] [Green Version]
- Ronaldson, P.T. Transport Properties of Statins by Organic Anion Transporting Polypeptide 1A2 and Regulation by Transforming Growth Factor-beta Signaling in Human Endothelial Cells. J. Pharmacol. Exp. Ther. 2021, 376, 148–160. [Google Scholar] [CrossRef]
- Amin, M.L. P-glycoprotein Inhibition for Optimal Drug Delivery. Drug Target Insights 2013, 7, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.-Y.; Tang, S.; Yang, X.-Q.; Ding, H.; Liu, X.-D.; Zeng, X.-B.; Huang, X.-P.; Deng, C.-Q. Borneol enhances the protective effect against cerebral ischemia/reperfusion injury by promoting the access of astragaloside IV and the components of Panax notoginseng saponins into the brain. Phytomedicine 2022, 94, 153822. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhou, Z.-W.; Xue, C.C.; Li, X.-X.; Zhou, S.-F. Role of P-glycoprotein in restricting the brain penetration of tanshinone IIA, a major active constituent from the root ofSalvia miltiorrhizaBunge, across the blood–brain barrier. Xenobiotica 2007, 37, 635–678. [Google Scholar] [CrossRef] [PubMed]
- Palmeira, A.; Sousa, M.E.; Vasconcelos, M.H.; Pinto, M. Three Decades of P-gp Inhibitors: Skimming Through Several Generations and Scaffolds. Curr. Med. Chem. 2012, 19, 1946–2025. [Google Scholar] [CrossRef]
- Binkhathlan, Z.; Lavasanifar, A. P-glycoprotein inhibition as a therapeutic approach for overcoming multidrug resistance in cancer: Current status and future perspectives. Curr. Cancer Drug Targets 2013, 13, 326–346. [Google Scholar] [CrossRef]
- Kalvass, J.C. Why clinical modulation of efflux transport at the human blood-brain barrier is unlikely: The ITC evi-dence-based position. Clin. Pharmacol. Ther. 2013, 94, 80–94. [Google Scholar] [CrossRef]
- Polli, J.W. An unexpected synergist role of P-glycoprotein and breast cancer resistance protein on the central nervous system penetration of the tyrosine kinase inhibitor lapatinib (N-{3-chloro-4-[(3-fluorobenzyl)oxy]phenyl}-6-[5-({[2-(methylsulfonyl)ethyl]amino }methyl)-2-furyl]-4-quinazolinamine; GW572016). Drug Metab. Dispos. 2009, 37, 439–442. [Google Scholar]
- Gomez-Zepeda, D.; Taghi, M.; Scherrmann, J.-M.; Decleves, X.; Menet, M.-C. ABC Transporters at the Blood–Brain Interfaces, Their Study Models, and Drug Delivery Implications in Gliomas. Pharmaceutics 2019, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Ohtsuki, S. Quantitative targeted absolute proteomic analysis of transporters, receptors and junction proteins for vali-dation of human cerebral microvascular endothelial cell line hCMEC/D3 as a human blood-brain barrier model. Mol. Pharm. 2013, 10, 289–296. [Google Scholar] [CrossRef]
- Billington, S.; Salphati, L.; Hop, C.E.C.A.; Chu, X.; Evers, R.; Burdette, D.; Rowbottom, C.; Lai, Y.; Xiao, G.; Humphreys, W.G.; et al. Interindividual and Regional Variability in Drug Transporter Abundance at the Human Blood–Brain Barrier Measured by Quantitative Targeted Proteomics. Clin. Pharmacol. Ther. 2019, 106, 228–237. [Google Scholar] [CrossRef]
- Robey, R.W.; To, K.K.; Polgar, O.; Dohse, M.; Fetsch, P.; Dean, M.; Bates, S.E. ABCG2: A perspective. Adv. Drug Deliv. Rev. 2009, 61, 3–13. [Google Scholar] [CrossRef]
- Breedveld, P.; Pluim, D.; Cipriani, G.; Dahlhaus, F.; Van Eijndhoven, M.A.J.; De Wolf, C.J.F.; Kuil, A.; Beijnen, J.H.; Scheffer, G.L.; Jansen, G.; et al. The Effect of Low pH on Breast Cancer Resistance Protein (ABCG2)-Mediated Transport of Methotrexate, 7-Hydroxymethotrexate, Methotrexate Diglutamate, Folic Acid, Mitoxantrone, Topotecan, and Resveratrol in In Vitro Drug Transport Models. Mol. Pharmacol. 2007, 71, 240–249. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Miao, M.; Chen, Y.; Wang, Z.; Sun, B.; Liu, X. Altered Function and Expression of ABC Transporters at the Blood–Brain Barrier and Increased Brain Distribution of Phenobarbital in Acute Liver Failure Mice. Front. Pharmacol. 2018, 9, 190. [Google Scholar] [CrossRef] [Green Version]
- Zamek-Gliszczynski, M.J. Efflux transport is an important determinant of ethinylestradiol glucuronide and ethi-nylestradiol sulfate pharmacokinetics. Drug Metab. Dispos. 2011, 39, 1794–1800. [Google Scholar] [CrossRef]
- Lee, Y.-J.; Kusuhara, H.; Jonker, J.; Schinkel, A.H.; Sugiyama, Y. Investigation of Efflux Transport of Dehydroepiandrosterone Sulfate and Mitoxantrone at the Mouse Blood-Brain Barrier: A Minor Role of Breast Cancer Resistance Protein. J. Pharmacol. Exp. Ther. 2005, 312, 44–52. [Google Scholar] [CrossRef] [Green Version]
- Tornabene, E.; Helms, H.C.C.; Pedersen, S.F.; Brodin, B. Effects of oxygen-glucose deprivation (OGD) on barrier properties and mRNA transcript levels of selected marker proteins in brain endothelial cells/astrocyte co-cultures. PLoS ONE 2019, 14, e0221103. [Google Scholar] [CrossRef]
- Ronaldson, P.T.; Finch, J.D.; DeMarco, K.M.; Quigley, C.E.; Davis, T.P. Inflammatory Pain Signals an Increase in Functional Expression of Organic Anion Transporting Polypeptide 1a4 at the Blood-Brain Barrier. J. Pharmacol. Exp. Ther. 2011, 336, 827–839. [Google Scholar] [CrossRef] [Green Version]
- Ronaldson, P.T.; Davis, T.P. Targeted Drug Delivery to Treat Pain and Cerebral Hypoxia. Pharmacol. Rev. 2013, 65, 291–314. [Google Scholar] [CrossRef] [Green Version]
- Thompson, B.J.; Sanchez-Covarrubias, L.; Slosky, L.M.; Zhang, Y.; Laracuente, M.-L.; Ronaldson, P.T. Hypoxia/Reoxygenation Stress Signals an Increase in Organic Anion Transporting polypeptide 1a4 (Oatp1a4) at the Blood–Brain Barrier: Relevance to CNS Drug Delivery. J. Cereb. Blood Flow Metab. 2014, 34, 699–707. [Google Scholar] [CrossRef]
- Abdullahi, W. Functional Expression of Organic Anion Transporting Polypeptide 1a4 Is Regulated by Transforming Growth Factor-beta/Activin Receptor-like Kinase 1 Signaling at the Blood-Brain Barrier. Mol. Pharmacol. 2018, 94, 1321–1333. [Google Scholar] [CrossRef] [Green Version]
- Abdullahi, W. Bone morphogenetic protein-9 increases the functional expression of organic anion transporting poly-peptide 1a4 at the blood-brain barrier via the activin receptor-like kinase-1 receptor. J. Cereb. Blood Flow Metab. 2017, 37, 2340–2345. [Google Scholar] [CrossRef]
- Brzica, H.; Abdullahi, W.; Reilly, B.G.; Ronaldson, P.T. Sex-specific differences in organic anion transporting polypeptide 1a4 (Oatp1a4) functional expression at the blood–brain barrier in Sprague–Dawley rats. Fluids Barriers CNS 2018, 15, 1–12. [Google Scholar] [CrossRef]
- Al-Majdoub, Z.M.; Al Feteisi, H.; Achour, B.; Warwood, S.; Neuhoff, S.; Rostami-Hodjegan, A.; Barber, J. Proteomic Quantification of Human Blood–Brain Barrier SLC and ABC Transporters in Healthy Individuals and Dementia Patients. Mol. Pharm. 2019, 16, 1220–1233. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Yu, N.; Lu, S.; Ito, S.; Zhang, X.; Prasad, B.; He, E.; Lu, X.; Li, Y.; Wang, F.; et al. Solute Carrier Family of the Organic Anion-Transporting Polypeptides 1A2– Madin-Darby Canine Kidney II: A Promising In Vitro System to Understand the Role of Organic Anion-Transporting Polypeptide 1A2 in Blood-Brain Barrier Drug Penetration. Drug Metab. Dispos. 2015, 43, 1008–1018. [Google Scholar] [CrossRef] [Green Version]
- Albekairi, T.H.; Vaidya, B.; Patel, R.; Nozohouri, S.; Villalba, H.; Zhang, Y.; Lee, Y.S.; Al-Ahmad, A.; Abbruscato, T.J. Brain Delivery of a Potent Opioid Receptor Agonist, Biphalin during Ischemic Stroke: Role of Organic Anion Transporting Polypeptide (OATP). Pharmaceutics 2019, 11, 467. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Islam, M.R.; Karamyan, V.T.; Abbruscato, T.J. In vitro and in vivo efficacy of a potent opioid receptor agonist, biphalin, compared to subtype-selective opioid receptor agonists for stroke treatment. Brain Res. 2015, 1609, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Shah, K.; Wang, H.; Karamyan, V.T.; Abbruscato, T.J. Characterization of Neuroprotective Effects of Biphalin, an Opioid Receptor Agonist, in a Model of Focal Brain Ischemia. J. Pharmacol. Exp. Ther. 2011, 339, 499–508. [Google Scholar] [CrossRef] [Green Version]
- Yang, L.; Wang, H.; Shah, K.; Karamyan, V.T.; Abbruscato, T.J. Opioid receptor agonists reduce brain edema in stroke. Brain Res. 2011, 1383, 307–316. [Google Scholar] [CrossRef]
- Islam, M.R.; Yang, L.; Lee, Y.S.; Hruby, V.J.; Karamyan, V.T.; Abbruscato, T.J. Enkephalin-Fentanyl Multifunctional Opioids as Potential Neuroprotectants for Ischemic Stroke Treatment. Curr. Pharm. Des. 2016, 22, 6459–6468. [Google Scholar] [CrossRef]
- Fang, S.; Xu, H.; Lu, J.; Zhu, Y.; Jiang, H. Neuroprotection by the Kappa-Opioid Receptor Agonist, BRL52537, is Mediated via Up-Regulating Phosphorylated Signal Transducer and Activator of Transcription-3 in Cerebral Ischemia/Reperfusion Injury in Rats. Neurochem. Res. 2013, 38, 2305–2312. [Google Scholar] [CrossRef]
- Eftekhar-Vaghefi, S.; Esmaeili-Mahani, S.; Elyasi, L.; Abbasnejad, M. Involvement of Mu Opioid Receptor Signaling in the Protective Effect of Opioid against 6-Hydroxydopamine-Induced SH-SY5Y Human Neuroblastoma Cells Apoptosis. Basic Clin. Neurosci. J. 2015, 6, 171–178. [Google Scholar]
- Sung, J.-H.; Yu, K.-H.; Park, J.-S.; Tsuruo, T.; Kim, D.-D.; Shim, C.-K.; Chung, S.-J. Saturable distribution of tacrine into the striatal extracellular fluid of the rat: Evidence of involvement of multiple organic cation transporters in the transport. Drug Metab. Dispos. 2005, 33, 440–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, K.-C.; Lu, Y.-H.; Peng, Y.-H.; Tsai, T.-F.; Kao, Y.-H.; Yang, H.-T.; Lin, C.-J. Decreased Expression of Organic Cation Transporters, Oct1 and Oct2, in Brain Microvessels and its Implication to MPTP-Induced Dopaminergic Toxicity in Aged Mice. J. Cereb. Blood Flow Metab. 2014, 35, 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betterton, R.D.; Davis, T.P.; Ronaldson, P.T. Organic Cation Transporter (OCT/OCTN) Expression at Brain Barrier Sites: Focus on CNS Drug Delivery. Handb. Exp. Pharmacol. 2021, 266, 301–328. [Google Scholar] [CrossRef]
- Hiasa, M.; Matsumoto, T.; Komatsu, T.; Moriyama, Y. Wide variety of locations for rodent MATE1, a transporter protein that mediates the final excretion step for toxic organic cations. Am. J. Physiol. Physiol. 2006, 291, C678–C686. [Google Scholar] [CrossRef]
- Chaves, C.; Campanelli, F.; Chapy, H.; Gomez-Zepeda, D.; Glacial, F.; Smirnova, M.; Taghi, M.; Pallud, J.; Perrière, N.; Declèves, X.; et al. An Interspecies Molecular and Functional Study of Organic Cation Transporters at the Blood-Brain Barrier: From Rodents to Humans. Pharmaceutics 2020, 12, 308. [Google Scholar] [CrossRef] [Green Version]
- Geier, E.G.; Chen, E.C.; Webb, A.; Papp, A.C.; Yee, S.W.; Sadee, W.; Giacomini, K.M. Profiling Solute Carrier Transporters in the Human Blood–Brain Barrier. Clin. Pharmacol. Ther. 2013, 94, 636–639. [Google Scholar] [CrossRef]
- Mehta, D.C.; Short, J.L.; Nicolazzo, J.A. Memantine Transport across the Mouse Blood–Brain Barrier Is Mediated by a Cationic Influx H+ Antiporter. Mol. Pharm. 2013, 10, 4491–4498. [Google Scholar] [CrossRef]
- Busch, A.E.; Karbach, U.; Miska, D.; Gorboulev, V.; Akhoundova, A.; Volk, C.; Arndt, P.; Ulzheimer, J.C.; Sonders, M.S.; Baumann, C.; et al. Human Neurons Express the Polyspecific Cation Transporter hOCT2, Which Translocates Monoamine Neurotransmitters, Amantadine, and Memantine. Mol. Pharmacol. 1998, 54, 342–352. [Google Scholar] [CrossRef] [Green Version]
- Graham, G.G.; Punt, J.; Arora, M.; Day, R.O.; Doogue, M.P.; Duong, J.K.; Furlong, T.J.; Greenfield, J.R.; Greenup, L.C.; Kirkpatrick, C.; et al. Clinical Pharmacokinetics of Metformin. Clin. Pharmacokinet. 2011, 50, 81–98. [Google Scholar] [CrossRef]
- Wrobel, M.P. Metformin—A new old drug. Endokrynol. Pol. 2017, 68, 482–496. [Google Scholar] [CrossRef]
- Sharma, S.; Nozohouri, S.; Vaidya, B.; Abbruscato, T. Repurposing metformin to treat age-related neurodegenerative disorders and ischemic stroke. Life Sci. 2021, 274, 119343. [Google Scholar] [CrossRef]
- Chen, Y. Antidiabetic drug metformin (GlucophageR) increases biogenesis of Alzheimer’s amyloid peptides via up-regulating BACE1 transcription. Proc. Natl. Acad. Sci. USA 2009, 106, 3907–3912. [Google Scholar] [CrossRef] [Green Version]
- Platt, S.R.; Holmes, S.P.; Howerth, E.W.; Duberstein, K.J.J.; Dove, C.R.; Kinder, H.A.; Wyatt, E.L.; Linville, A.V.; Lau, V.W.; Stice, S.L.; et al. Development and characterization of a Yucatan miniature biomedical pig permanent middle cerebral artery occlusion stroke model. Exp. Transl. Stroke Med. 2014, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Cook, D.J.; Tymianski, M. Nonhuman Primate Models of Stroke for Translational Neuroprotection Research. Neurotherapeutics 2012, 9, 371–379. [Google Scholar] [CrossRef] [Green Version]
- Narayan, S.K.; Cherian, S.G.; Phaniti, P.B.; Chidambaram, S.B.; Vasanthi, A.H.R.; Arumugam, M. Preclinical animal studies in ischemic stroke: Challenges and some solutions. Anim. Model. Exp. Med. 2021, 4, 104–115. [Google Scholar] [CrossRef]
- Debatisse, J.; Wateau, O.; Cho, T.-H.; Costes, N.; Merida, I.; Léon, C.; Langlois, J.-B.; Taborik, F.; Verset, M.; Portier, K.; et al. A non-human primate model of stroke reproducing endovascular thrombectomy and allowing long-term imaging and neurological read-outs. J. Cereb. Blood Flow Metab. 2021, 41, 745–760. [Google Scholar] [CrossRef]
- Kumar, N.; Lee, J.J.; Perlmutter, J.S.; Derdeyn, C.P. Cervical Carotid and Circle of Willis Arterial Anatomy of Macaque Monkeys: A Comparative Anatomy Study. Anat. Rec. 2009, 292, 976–984. [Google Scholar] [CrossRef] [Green Version]
- Kassel, N.F.; Langfitt, T.W. Variations in the circle of Willis in Macaca mulatta. Anat. Rec. 1965, 152, 257–263. [Google Scholar] [CrossRef]
- Hoshi, Y.; Uchida, Y.; Tachikawa, M.; Inoue, T.; Ohtsuki, S.; Terasaki, T. Quantitative Atlas of Blood–Brain Barrier Transporters, Receptors, and Tight Junction Proteins in Rats and Common Marmoset. J. Pharm. Sci. 2013, 102, 3343–3355. [Google Scholar] [CrossRef]
- Auvity, S.; Caillé, F.; Marie, S.; Wimberley, C.; Bauer, M.; Langer, O.; Buvat, I.; Goutal, S.; Tournier, N. P-Glycoprotein (ABCB1) Inhibits the Influx and Increases the Efflux of 11C-Metoclopramide Across the Blood–Brain Barrier: A PET Study on Nonhuman Primates. J. Nucl. Med. 2018, 59, 1609–1615. [Google Scholar] [CrossRef] [Green Version]
- García-Varela, L.; Arif, W.M.; García, D.V.; Kakiuchi, T.; Ohba, H.; Harada, N.; Tago, T.; Elsinga, P.H.; Tsukada, H.; Colabufo, N.A.; et al. Pharmacokinetic Modeling of [18F]MC225 for Quantification of the P-Glycoprotein Function at the Blood–Brain Barrier in Non-Human Primates with PET. Mol. Pharm. 2020, 17, 3477–3486. [Google Scholar] [CrossRef]
- Zhang, K.; Sejnowski, T.J. A universal scaling law between gray matter and white matter of cerebral cortex. Proc. Natl. Acad. Sci. USA 2000, 97, 5621–5626. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, H. MR-based statistical atlas of the Gottingen minipig brain. Neuroimage 2001, 14, 1089–1096. [Google Scholar] [CrossRef]
- Sozmen, E.G.; Hinman, J.D.; Carmichael, S.T. Models That Matter: White Matter Stroke Models. Neurotherapeutics 2012, 9, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, S.; Okuyama, J.; Tamatsu, Y.; Shimada, K.; Hoshi, H.; Iwai, J. The arterial circle of Willis of the mouse helps to decipher secrets of cerebral vascular accidents in the human. Med. Hypotheses 2004, 63, 997–1009. [Google Scholar] [CrossRef]
- McColl, B.W.; Carswell, H.V.; McCulloch, J.; Horsburgh, K. Extension of cerebral hypoperfusion and ischaemic pathology beyond MCA territory after intraluminal filament occlusion in C57Bl/6J mice. Brain Res. 2004, 997, 15–23. [Google Scholar] [CrossRef]
- Uchida, Y.; Yagi, Y.; Takao, M.; Tano, M.; Umetsu, M.; Hirano, S.; Usui, T.; Tachikawa, M.; Terasaki, T. Comparison of Absolute Protein Abundances of Transporters and Receptors among Blood–Brain Barriers at Different Cerebral Regions and the Blood–Spinal Cord Barrier in Humans and Rats. Mol. Pharm. 2020, 17, 2006–2020. [Google Scholar] [CrossRef]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke 1989, 20, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Belayev, L.; Alonso, O.F.; Busto, R.; Zhao, W.; Ginsberg, M.D. Middle Cerebral Artery Occlusion in the Rat by Intraluminal Suture. Stroke 1996, 27, 1616–1623. [Google Scholar] [CrossRef]
- Barthels, D.; Das, H. Current advances in ischemic stroke research and therapies. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2020, 1866, 165260. [Google Scholar] [CrossRef] [PubMed]
- Vital, S.A.; Gavins, F.N.E. Surgical Approach for Middle Cerebral Artery Occlusion and Reperfusion Induced Stroke in Mice. J. Vis. Exp. 2016, 2016, e54302. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.I.; Wise, P.M.; O’Donnell, M.E. Cerebral microvascular endothelial cell Na/H exchange: Evidence for the presence of NHE1 and NHE2 isoforms and regulation by arginine vasopressin. Am. J. Physiol. Cell Physiol. 2009, 297, C278–C289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.K.; Foroutan, S.; O’Donnell, M.E. Ischemia-induced stimulation of Na-K-Cl cotransport in cerebral microvas-cular endothelial cells involves AMP kinase. Am. J. Physiol. Cell Physiol. 2011, 301, C316–C326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.K.; Jelks, K.A.; O’Donnell, M.E. Ischemia-induced stimulation of cerebral microvascular endothelial cell Na-K-Cl cotransport involves p38 and JNK MAP kinases. Am. J. Physiol. Cell Physiol. 2012, 302, C505–C517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.H. Rosiglitazone attenuates hyperglycemia-enhanced hemorrhagic transformation after transient focal is-chemia in rats. Neuroscience 2013, 250, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Ismael, S.; Nasoohi, S.; Yoo, A.; Ahmed, H.A.; Ishrat, T. Tissue Plasminogen Activator Promotes TXNIP-NLRP3 Inflammasome Activation after Hyperglycemic Stroke in Mice. Mol. Neurobiol. 2020, 57, 2495–2508. [Google Scholar] [CrossRef] [PubMed]
- Steele, E.C., Jr.; Guo, Q.; Namura, S. Filamentous Middle Cerebral Artery Occlusion Causes Ischemic Damage to the Retina in Mice. Stroke 2008, 39, 2099–2104. [Google Scholar] [CrossRef] [Green Version]
- Sommer, C.J. Ischemic stroke: Experimental models and reality. Acta Neuropathol. 2017, 133, 245–261. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Chen, J.; Wang, B.; Zhang, M.; Shi, J.; Ma, Y.; Zhu, Z.; Yan, F.; He, X.; Li, S.; et al. Endovascular ischemic stroke models of adult rhesus monkeys: A comparison of two endovascular methods. Sci. Rep. 2016, 6, 31608. [Google Scholar] [CrossRef] [Green Version]
- Overgaard, K.; Sereghy, T.; Boysen, G.; Pedersen, H.; Høyer, S.; Diemer, N.H. A Rat Model of Reproducible Cerebral Infarction Using Thrombotic Blood Clot Emboli. J. Cereb. Blood Flow Metab. 1992, 12, 484–490. [Google Scholar] [CrossRef]
- Busch, E.; Krüger, K.; Hossmann, K.-A. Improved model of thromboembolic stroke and rt-PA induced reperfusion in the rat. Brain Res. 1997, 778, 16–24. [Google Scholar] [CrossRef]
- Zhang, Z.; Chopp, M.; Zhang, R.L.; Goussev, A. A Mouse Model of Embolic Focal Cerebral Ischemia. J. Cereb. Blood Flow Metab. 1997, 17, 1081–1088. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.L.; Chopp, M.; Zhang, Z.G.; Jiang, Q.; Ewing, J.R. A rat model of focal embolic cerebral ischemia. Brain Res. 1997, 766, 83–92. [Google Scholar] [CrossRef]
- Chen, Y.; Zhu, W.; Zhang, W.; Libal, N.; Murphy, S.J.; Offner, H.; Alkayed, N.J. A novel mouse model of thromboembolic stroke. J. Neurosci. Methods 2015, 256, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Ren, M.; Lin, Z.-J.; Qian, H.; Choudhury, G.R.; Liu, R.; Liu, H.; Yang, S.-H. Embolic middle cerebral artery occlusion model using thrombin and fibrinogen composed clots in rat. J. Neurosci. Methods 2012, 211, 296–304. [Google Scholar] [CrossRef] [Green Version]
- Carmichael, S.T. Rodent models of focal stroke: Size, mechanism, and purpose. NeuroRX 2005, 2, 396–409. [Google Scholar] [CrossRef] [Green Version]
- Busch, E.; Krüger, K.; Fritze, K.; Allegrini, P.R.; Hoehn-Berlage, M.; Hossmann, K.A. Blood-Brain Barrier Disturbances After rt-PA Treatment of Thromboembolic Stroke in the Rat. Acta Neurochir. Suppl. 1997, 70, 206–208. [Google Scholar] [CrossRef]
- Kleinschnitz, C.; Fluri, F.; Schuhmann, M. Animal models of ischemic stroke and their application in clinical research. Drug Des. Dev. Ther. 2015, 9, 3445–3454. [Google Scholar] [CrossRef] [Green Version]
- Lu, H.; Li, Y.; Yuan, L.; Li, H.; Lu, X.; Tong, S. Induction and imaging of photothrombotic stroke in conscious and freely moving rats. J. Biomed. Opt. 2014, 19, 096013. [Google Scholar] [CrossRef]
- Yu, C.-L.; Zhou, H.; Chai, A.-P.; Yang, Y.-X.; Mao, R.-R.; Xu, L. Whole-scale neurobehavioral assessments of photothrombotic ischemia in freely moving mice. J. Neurosci. Methods 2015, 239, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Kleinschnitz, C.; Braeuninger, S.; Pham, M.; Austinat, M.; Nölte, I.; Renné, T.; Nieswandt, B.; Bendszus, M.; Stoll, G. Blocking of Platelets or Intrinsic Coagulation Pathway–Driven Thrombosis Does Not Prevent Cerebral Infarctions Induced by Photothrombosis. Stroke 2008, 39, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Frederix, K.; Chauhan, A.K.; Kisucka, J.; Zhao, B.-Q.; Hoff, E.I.; Spronk, H.M.H.; Cate, H.T.; Wagner, D.D. Platelet adhesion receptors do not modulate infarct volume after a photochemically induced stroke in mice. Brain Res. 2007, 1185, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, W. Establishing a photothrombotic ’ring’ stroke model in adult mice with late spontaneous reperfusion: Quanti-tative measurements of cerebral blood flow and cerebral protein synthesis. J. Cereb. Blood Flow Metab. 2006, 26, 927–936. [Google Scholar] [CrossRef]
- Wester, P.; Watson, B.D.; Prado, R.; Dietrich, W.D. A Photothrombotic ‘Ring’ Model of Rat Stroke-in-Evolution Displaying Putative Penumbral Inversion. Stroke 1995, 26, 444–450. [Google Scholar] [CrossRef]
- Hu, X.; Wester, P.; Brännström, T.; Watson, B.D.; Gu, W. Progressive and reproducible focal cortical ischemia with or without late spontaneous reperfusion generated by a ring-shaped, laser-driven photothrombotic lesion in rats. Brain Res. Protoc. 2001, 7, 76–85. [Google Scholar] [CrossRef]
- Virley, D.; Hadingham, S.J.; Roberts, J.C.; Farnfield, B.; Elliott, H.; Whelan, G.; Golder, J.; David, C.; Parsons, A.A.; Hunter, A.J. A New Primate Model of Focal Stroke: Endothelin-1—Induced Middle Cerebral Artery Occlusion and Reperfusion in the Common Marmoset. J. Cereb. Blood Flow Metab. 2004, 24, 24–41. [Google Scholar] [CrossRef] [Green Version]
- Haynes, W.; Webb, D.J. Endothelin as a regulator of cardiovascular function in health and disease. J. Hypertens. 1998, 16, 1081–1098. [Google Scholar] [CrossRef]
- Abeysinghe, H.C.S.; Roulston, C.L. A Complete Guide to Using the Endothelin-1 Model of Stroke in Conscious Rats for Acute and Long-Term Recovery Studies. Program. Necrosis 2018, 1717, 115–133. [Google Scholar] [CrossRef]
- Ansari, S.; Azari, H.; Caldwell, K.J.; Regenhardt, R.W.; Hedna, V.S.; Waters, M.F.; Hoh, B.L.; Mecca, A.P. Endothelin-1 Induced Middle Cerebral Artery Occlusion Model for Ischemic Stroke with Laser Doppler Flowmetry Guidance in Rat. J. Vis. Exp. 2013, 2013, e50014. [Google Scholar] [CrossRef] [Green Version]
- Sharkey, J.; Ritchie, I.M.; Kelly, P.A. Perivascular microapplication of endothelin-1: A new model of focal cerebral ischaemia in the rat. J. Cereb. Blood Flow Metab. 1993, 13, 865–871. [Google Scholar] [CrossRef] [Green Version]
- Biernaskie, J.; Corbett, D.; Peeling, J.; Wells, J.; Lei, H. A serial MR study of cerebral blood flow changes and lesion development following endothelin-1-induced ischemia in rats. Magn. Reson. Med. 2001, 46, 827–830. [Google Scholar] [CrossRef]
- Bauer, B.; Hartz, A.M.S.; Miller, D.S. Tumor Necrosis Factor α and Endothelin-1 Increase P-Glycoprotein Expression and Transport Activity at the Blood-Brain Barrier. Mol. Pharmacol. 2007, 71, 667–675. [Google Scholar] [CrossRef] [Green Version]
- Hartz, A.M.S.; Bauer, B.; Fricker, G.; Miller, D.S. Rapid Regulation of P-Glycoprotein at the Blood-Brain Barrier by Endothelin-1. Mol. Pharmacol. 2004, 66, 387–394. [Google Scholar] [CrossRef] [Green Version]
- Harati, R.; Villégier, A.-S.; Banks, W.A.; Mabondzo, A. Susceptibility of juvenile and adult blood–brain barrier to endothelin-1: Regulation of P-glycoprotein and breast cancer resistance protein expression and transport activity. J. Neuroinflamm. 2012, 9, 273. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Ovbiagele, B.; Feng, W. Diabetes and Stroke: Epidemiology, Pathophysiology, Pharmaceuticals and Outcomes. Am. J. Med. Sci. 2016, 351, 380–386. [Google Scholar] [CrossRef] [Green Version]
- Putaala, J.; Liebkind, R.; Gordin, D.; Thorn, L.M.; Haapaniemi, E.; Forsblom, C.; Groop, P.-H.; Kaste, M.; Tatlisumak, T. Diabetes mellitus and ischemic stroke in the young: Clinical features and long-term prognosis. Neurology 2011, 76, 1831–1837. [Google Scholar] [CrossRef]
- Khoury, J.C. Diabetes mellitus: A risk factor for ischemic stroke in a large biracial population. Stroke 2013, 44, 1500–1504. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Saver, J.; Hong, K.-S.; Song, S.; Chang, K.-H.; Ovbiagele, B. Effect of pre-diabetes on future risk of stroke: Meta-analysis. BMJ 2012, 344, e3564. [Google Scholar] [CrossRef] [Green Version]
- Huber, J.D. Diabetes, Cognitive Function, and the Blood-Brain Barrier. Curr. Pharm. Des. 2008, 14, 1594–1600. [Google Scholar] [CrossRef]
- Qiao, J.; Lawson, C.; Rentrup, K.F.G.; Kulkarni, P.; Ferris, C.F. Evaluating blood–brain barrier permeability in a rat model of type 2 diabetes. J. Transl. Med. 2020, 18, 1–8. [Google Scholar] [CrossRef]
- Hawkins, B.T.; Lundeen, T.F.; Norwood, K.M.; Brooks, H.L.; Egleton, R.D. Increased blood–brain barrier permeability and altered tight junctions in experimental diabetes in the rat: Contribution of hyperglycaemia and matrix metalloproteinases. Diabetologia 2006, 50, 202–211. [Google Scholar] [CrossRef] [Green Version]
- Banks, W.A. The Blood-Brain Barrier Interface in Diabetes Mellitus: Dysfunctions, Mechanisms and Approaches to Treatment. Curr. Pharm. Des. 2020, 26, 1438–1447. [Google Scholar] [CrossRef]
- Salameh, T.S.; Mortell, W.G.; Logsdon, A.F.; Butterfield, D.A.; Banks, W.A. Disruption of the hippocampal and hypothalamic blood–brain barrier in a diet-induced obese model of type II diabetes: Prevention and treatment by the mitochondrial carbonic anhydrase inhibitor, topiramate. Fluids Barriers CNS 2019, 16, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Prasad, S. Diabetes Mellitus and Blood-Brain Barrier Dysfunction: An Overview. J. Pharmacovigil. 2014, 2, 125. [Google Scholar]
- Van Sloten, T.T. Cerebral microvascular complications of type 2 diabetes: Stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol. 2020, 8, 325–336. [Google Scholar] [CrossRef]
- Mergenthaler, P.; Lindauer, U.; Dienel, G.A.; Meisel, A. Sugar for the brain: The role of glucose in physiological and pathological brain function. Trends Neurosci. 2013, 36, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Cornford, E.M.; Hyman, S.; Pardridge, W.M. An Electron Microscopic Immunogold Analysis of Developmental Up-Regulation of the Blood—Brain Barrier GLUT1 Glucose Transporter. J. Cereb. Blood Flow Metab. 1993, 13, 841–854. [Google Scholar] [CrossRef] [Green Version]
- Farrell, C.L.; Pardridge, W.M. Blood-brain barrier glucose transporter is asymmetrically distributed on brain capillary endothelial lumenal and ablumenal membranes: An electron microscopic immunogold study. Proc. Natl. Acad. Sci. USA 1991, 88, 5779–5783. [Google Scholar] [CrossRef] [Green Version]
- Gerhart, D.Z.; Levasseur, R.J.; Broderius, M.A.; Drewes, L.R. Glucose transporter localization in brain using light and electron immunocytochemistry. J. Neurosci. Res. 1989, 22, 464–472. [Google Scholar] [CrossRef]
- Simpson, I.A.; Vannucci, S.J.; DeJoseph, M.R.; Hawkins, R.A. Glucose Transporter Asymmetries in the Bovine Blood-Brain Barrier. J. Biol. Chem. 2001, 276, 12725–12729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sogin, D.C.; Hinkle, P.C. Immunological identification of the human erythrocyte glucose transporter. Proc. Natl. Acad. Sci. USA 1980, 77, 5725–5729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, M.S.; Krizanac-Bengez, L.; Macchia, F.; Naftalin, R.; Pedley, K.C.; Mayberg, M.; Marroni, M.; Leaman, S.; Stanness, K.A.; Janigro, D. Mechanisms of glucose transport at the blood-brain barrier: An in vitro study. Brain Res. 2001, 904, 20–30. [Google Scholar] [CrossRef]
- Duelli, R.; Maurer, M.; Staudt, R.; Heiland, S.; Duembgen, L.; Kuschinsky, W. Increased cerebral glucose utilization and decreased glucose transporter Glut1 during chronic hyperglycemia in rat brain. Brain Res. 2000, 858, 338–347. [Google Scholar] [CrossRef]
- Lee, W.H.; Bondy, C.A. Ischemic injury induces brain glucose transporter gene expression. Endocrinology 1993, 133, 2540–2544. [Google Scholar] [CrossRef] [PubMed]
- Urabe, T.; Hattori, N.; Nagamatsu, S.; Sawa, H.; Mizuno, Y. Expression of Glucose Transporters in Rat Brain Following Transient Focal Ischemic Injury. J. Neurochem. 2002, 67, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Gerhart, D.Z.; Leino, R.L.; Taylor, W.E.; Borson, N.D.; Drewes, L.R. GLUT1 and GLUT3 gene expression in gerbil brain following brief ischemia: An in situ hybridization study. Mol. Brain Res. 1994, 25, 313–322. [Google Scholar] [CrossRef]
- McCall, A.L.; Van Bueren, A.M.; Nipper, V.; Moholt-Siebert, M.; Downes, H.; Lessov, N. Forebrain Ischemia Increases Glut1 Protein in Brain Microvessels and Parenchyma. J. Cereb. Blood Flow Metab. 1996, 16, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.-W.; Zhang, L.; Hou, W.-K.; Xu, Y.-X.; Xu, H.; Lou, F.-C.; Zhang, Y.; Wang, Q. Dynamic expression of glucose transporters 1 and 3 in the brain of diabetic rats with cerebral ischemia reperfusion. Chin. Med. J. 2009, 122, 1996–2001. [Google Scholar]
- Liu, H.; Liu, X.; Jia, L.; Liu, Y.; Yang, H.; Wang, G.; Xie, L. Insulin therapy restores impaired function and expression of P-glycoprotein in blood–brain barrier of experimental diabetes. Biochem. Pharmacol. 2008, 75, 1649–1658. [Google Scholar] [CrossRef]
- Maeng, H.J. Functional induction of P-glycoprotein in the blood-brain barrier of streptozotocin-induced diabetic rats: Evidence for the involvement of nuclear factor-kappaB, a nitrosative stress-sensitive transcription factor, in the regulation. Drug Metab. Dispos. 2007, 35, 1996–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, K.-C.; Pan, H.-J.; Yin, H.-S.; Chen, M.-R.; Lu, S.-C.; Lin, C.-J.; Chun-Jung, L. Change in P-glycoprotein and caveolin protein expression in brain striatum capillaries in New Zealand Obese mice with type 2 diabetes. Life Sci. 2009, 85, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, M.E.; Wang, T.W.; Jamal, A.; Loretan, C.G.; Neff, L.J. Tobacco Product Use Among Adults—United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1736–1742. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef] [Green Version]
- Markidan, J.; Cole, J.W.; Cronin, C.A.; Merino, J.G.; Phipps, M.; Wozniak, M.A.; Kittner, S.J. Smoking and Risk of Ischemic Stroke in Young Men. Stroke 2018, 49, 1276–1278. [Google Scholar] [CrossRef]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef]
- Wolf, A.P.; D’Agostino, R.B.; Kannel, W.B.; Bonita, R.; Belanger, A.J. Cigarette smoking as a risk factor for stroke. The Framingham Study. JAMA J. Am. Med. Assoc. 1988, 259, 1025–1029. [Google Scholar] [CrossRef]
- Pan, B. The relationship between smoking and stroke: A meta-analysis. Medicine 2019, 98, e14872. [Google Scholar] [CrossRef]
- Fetterman, J.L.; Weisbrod, R.M.; Feng, B.; Bastin, R.; Tuttle, S.T.; Holbrook, M.; Baker, G.; Robertson, R.M.; Conklin, D.J.; Bhatnagar, A.; et al. Flavorings in Tobacco Products Induce Endothelial Cell Dysfunction. Arter. Thromb. Vasc. Biol. 2018, 38, 1607–1615. [Google Scholar] [CrossRef]
- Malek, A.M. Secondhand Smoke Exposure and Stroke: The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Am. J. Prev. Med. 2015, 49, e89–e97. [Google Scholar] [CrossRef] [Green Version]
- Pistilli, M.; Howard, V.J.; Safford, M.M.; Lee, B.K.; Lovasi, G.S.; Cushman, M.; Malek, A.M.; McClure, L.A.; REGARDS Investigators. Association of secondhand tobacco smoke exposure during childhood on adult cardiovascular disease risk among never-smokers. Ann. Epidemiol. 2019, 32, 28–34.e1. [Google Scholar] [CrossRef]
- Howard, G.; Burke, G.L.; Szklo, M.; Tell, G.S.; Eckfeldt, J.; Evans, G.; Heiss, G. Active and passive smoking are associated with increased carotid wall thickness. The Atherosclerosis Risk in Communities Study. Arch. Intern. Med. 1994, 154, 1277–1282. [Google Scholar] [CrossRef]
- Shah, R.S.; Cole, J.W. Smoking and stroke: The more you smoke the more you stroke. Expert Rev. Cardiovasc. Ther. 2010, 8, 917–932. [Google Scholar] [CrossRef]
- Penn, A.; Snyder, C.A. 1,3 Butadiene, a Vapor Phase Component of Environmental Tobacco Smoke, Accelerates Arteriosclerotic Plaque Development. Circulation 1996, 93, 552–557. [Google Scholar] [CrossRef]
- Seo, S.-B.; Choe, E.S.; Kim, K.-S.; Shim, S.-M. The effect of tobacco smoke exposure on the generation of reactive oxygen species and cellular membrane damage using co-culture model of blood brain barrier with astrocytes. Toxicol. Ind. Health 2017, 33, 530–536. [Google Scholar] [CrossRef]
- Abbruscato, T.J.; Lopez, S.P.; Mark, K.S.; Hawkins, B.T.; Davis, T.P. Nicotine and Cotinine Modulate Cerebral Microvascular Permeability and Protein Expression of ZO-1 through Nicotinic Acetylcholine Receptors Expressed on Brain Endothelial Cells. J. Pharm. Sci. 2002, 91, 2525–2538. [Google Scholar] [CrossRef]
- Hawkins, B.; Abbruscato, T.J.; Egleton, R.D.; Brown, R.C.; Huber, J.D.; Campos, C.R.; Davis, T. Nicotine increases in vivo blood–brain barrier permeability and alters cerebral microvascular tight junction protein distribution. Brain Res. 2004, 1027, 48–58. [Google Scholar] [CrossRef]
- Kadry, H.; Noorani, B.; Bickel, U.; Abbruscato, T.J.; Cucullo, L. Comparative assessment of in vitro BBB tight junction integrity following exposure to cigarette smoke and e-cigarette vapor: A quantitative evaluation of the protective effects of metformin using small-molecular-weight paracellular markers. Fluids Barriers CNS 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Mazzone, P.; Tierney, W.; Hossain, M.; Puvenna, V.; Janigro, D.; Cucullo, L. Pathophysiological Impact of Cigarette Smoke Exposure on the Cerebrovascular System with a Focus on the Blood-brain Barrier: Expanding the Awareness of Smoking Toxicity in an Underappreciated Area. Int. J. Environ. Res. Public Health 2010, 7, 4111–4126. [Google Scholar] [CrossRef]
- Pimentel, E.; Sivalingam, K.; Doke, M.; Samikkannu, T. Effects of Drugs of Abuse on the Blood-Brain Barrier: A Brief Overview. Front. Neurosci. 2020, 14, 513. [Google Scholar] [CrossRef]
- Abbruscato, T.J.; Lopez, S.P.; Roder, K.; Paulson, J.R. Regulation of Blood-Brain Barrier Na,K,2Cl-Cotransporter through Phosphorylation during in Vitro Stroke Conditions and Nicotine Exposure. J. Pharmacol. Exp. Ther. 2004, 310, 459–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manda, V.K.; Mittapalli, R.K.; Bohn, K.A.; Adkins, C.E.; Lockman, P.R. Nicotine and cotinine increases the brain penetration of saquinavir in rat. J. Neurochem. 2010, 115, 1495–1507. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2020, 141, 139. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.M.; Del Álamo, J.C.; Akoum, N. Fibrosis, atrial fibrillation and stroke: Clinical updates and emerging mechanistic models. Heart 2021, 107, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Hayden, D.T. Rates and Determinants of 5-Year Outcomes After Atrial Fibrillation-Related Stroke: A Population Study. Stroke 2015, 46, 3488–3493. [Google Scholar] [CrossRef] [PubMed]
- Voukalis, C.; Shantsila, E.; Lip, G.Y. Clinical Stroke prevention in atrial fibrillation. J. R. Coll. Physicians Edinb. 2017, 47, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Junejo, R.T.; Braz, I.D.; Lucas, S.; Van Lieshout, J.J.; Phillips, A.A.; Lip, G.Y.; Fisher, J.P. Neurovascular coupling and cerebral autoregulation in atrial fibrillation. J. Cereb. Blood Flow Metab. 2020, 40, 1647–1657. [Google Scholar] [CrossRef]
- Girouard, H.; Iadecola, C. Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. J. Appl. Physiol. 2006, 100, 328–335. [Google Scholar] [CrossRef]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Rokita, H.; Launer, L.J.; Gudnason, V.; Arnar, D.O. Atrial fibrillation is associated with decreased total cerebral blood flow and brain perfusion. Europace 2018, 20, 1252–1258. [Google Scholar] [CrossRef]
- Petersen, P.; Kastrup, J.; Videbæk, R.; Boysen, G. Cerebral Blood Flow before and after Cardioversion of Atrial Fibrillation. J. Cereb. Blood Flow Metab. 1989, 9, 422–425. [Google Scholar] [CrossRef] [Green Version]
- Totaro, R.; Corridoni, C.; Marini, C.; Marsili, R.; Prencipe, M. Transcranial Doppler evaluation of cerebral blood flow in patients with paroxysmal atrial fibrillation. Neurol. Sci. 1993, 14, 451–454. [Google Scholar] [CrossRef]
- Aryal, R.; Patabendige, A. Blood–brain barrier disruption in atrial fibrillation: A potential contributor to the increased risk of dementia and worsening of stroke outcomes? Open Biol. 2021, 11, 200396. [Google Scholar] [CrossRef]
- Soga, Y. Clinical hypertension and vascular diseases. In Hypertension and Stroke; Aiyagari, G.P.V., Ed.; Humana Press: Totowa, NJ, USA, 2011. [Google Scholar]
- Ostwald, S.K.; Wasserman, J.; Davis, S. Medications, Comorbidities, and Medical Complications in Stroke Survivors: The CAReS Study. Rehabil. Nurs. 2006, 31, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Brown, D.W. Preeclampsia and the risk of ischemic stroke among young women: Results from the Stroke Prevention in Young Women Study. Stroke 2006, 37, 1055–1059. [Google Scholar] [CrossRef] [Green Version]
- Cipolla, M.J.; Liebeskind, D.S.; Chan, S.-L. The importance of comorbidities in ischemic stroke: Impact of hypertension on the cerebral circulation. J. Cereb. Blood Flow Metab. 2018, 38, 2129–2149. [Google Scholar] [CrossRef]
- Humphrey, J.D. Mechanisms of arterial remodeling in hypertension: Coupled roles of wall shear and intramural stress. Hypertension 2008, 52, 195–200. [Google Scholar] [CrossRef] [Green Version]
- Mohammadi, M.T.; Dehghani, G.A. Acute hypertension induces brain injury and blood–brain barrier disruption through reduction of claudins mRNA expression in rat. Pathol. Res. Pract. 2014, 210, 985–990. [Google Scholar] [CrossRef]
- Nakagawa, S.; Ohara, H.; Niwa, M.; Yamagata, K.; Nibika, T. Defective Function of the Blood-Brain Barrier in a Stroke-Prone Spontaneously Hypertensive Rat: Eval-uation in an In Vitro Cell Culture Model. Cell Mol. Neurobiol. 2022, 42, 243–253. [Google Scholar] [CrossRef]
- Hom, S.; Fleegal, M.A.; Egleton, R.D.; Campos, C.R.; Hawkins, B.T.; Davis, T.P. Comparative changes in the blood-brain barrier and cerebral infarction of SHR and WKY rats. Am. J. Physiol. Integr. Comp. Physiol. 2007, 292, R1881–R1892. [Google Scholar] [CrossRef] [Green Version]
- Yousufuddin, M.; Young, N. Aging and ischemic stroke. Aging 2019, 11, 2542–2544. [Google Scholar] [CrossRef]
- Yousufuddin, M.; Bartley, A.C.; Alsawas, M.; Sheely, H.L.; Shultz, J.; Takahashi, P.Y.; Young, N.P.; Murad, M.H. Impact of Multiple Chronic Conditions in Patients Hospitalized with Stroke and Transient Ischemic Attack. J. Stroke Cerebrovasc. Dis. 2017, 26, 1239–1248. [Google Scholar] [CrossRef]
- Suenaga, J.; Hu, X.; Pu, H.; Shi, Y.; Hassan, S.H.; Xu, M.; Leak, R.; Stetler, R.A.; Gao, Y.; Chen, J. White matter injury and microglia/macrophage polarization are strongly linked with age-related long-term deficits in neurological function after stroke. Exp. Neurol. 2015, 272, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Erdő, F.; Denes, L.; de Lange, E. Age-associated physiological and pathological changes at the blood–brain barrier: A review. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 2017, 37, 4–24. [Google Scholar] [CrossRef] [Green Version]
- Cai, W.; Zhang, K.; Li, P.; Zhu, L.; Xu, J.; Yang, B.; Hu, X.; Lu, Z.; Chen, J. Dysfunction of the neurovascular unit in ischemic stroke and neurodegenerative diseases: An aging effect. Ageing Res. Rev. 2017, 34, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, K.A.; Li, X.; Tan, Z.; VanGilder, R.L.; Rosen, C.L.; Huber, J.D. NOX2 inhibition with apocynin worsens stroke outcome in aged rats. Brain Res. 2009, 1292, 165–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lähteenvuo, J.; Rosenzweig, A. Effects of aging on angiogenesis. Circ. Res. 2012, 110, 1252–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marín, C.; Yubero-Serrano, E.M.; López-Miranda, J.; Perez-Jimenez, F. Endothelial Aging Associated with Oxidative Stress Can Be Modulated by a Healthy Mediterranean Diet. Int. J. Mol. Sci. 2013, 14, 8869–8889. [Google Scholar] [CrossRef] [PubMed]
- Zlokovic, B.V. Neurovascular pathways to neurodegeneration in Alzheimer’s disease and other disorders. Nat. Rev. Neurosci. 2011, 12, 723–738. [Google Scholar] [CrossRef]
- Wu, B.; Ueno, M.; Onodera, M.; Kusaka, T.; Huang, C.-L.; Hosomi, N.; Kanenishi, K.; Sakamoto, H. Age-related changes in P-glycoprotein expression in senescence-accelerated mouse. Curr. Aging Sci. 2009, 2, 187–192. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Transporter | Mouse | Rat | Porcine | Bovine | Non-Human Primate | Human |
|---|---|---|---|---|---|---|
| OATPs/Oatps (SLCOs/Slcos) | Oatp1a4: Luminal and Abluminal [71] | Oatp1a4: Luminal [72]; Luminal and Abluminal [73] Oatp1c1: Luminal and Abluminal [74] Oatp2b1: Abluminal [72] | Oatp3a1: Primarily Luminal [75] | Not defined | Not defined | OATP1A2: Luminal and Abluminal [76,77,78] OATP2B1: Luminal [79] |
| OCTs/Octs (SLC22A/Slc22a) | Oct1 and Oct2: Primarily Luminal [80,81] | Oct1 and Oct2: Primarily Luminal [81] | Not defined | Not defined | Not defined | OCT1 and OCT2: Primarily Luminal [80,81] |
| MATE1/Mate1 (SLC47A1/Slc47a1) | Not defined | Not defined | Not defined | Not defined | Not defined | Not defined |
| P-gp (MDR1/Mdr1) (ABCB1, Abcb1a/Abcb1b) | Luminal [82] | Luminal [83]; Luminal and Abluminal [84] | Luminal [75] | Luminal [85] | Luminal [86] | Luminal [87]; Luminal and Abluminal [84] |
| BCRP/Bcrp (ABCG2/Abcg2) | Luminal [88] | Primarily Luminal [89] | Primarily Luminal [75] | Not defined | Not defined | Primarily Luminal [90] |
| MRP1/Mrp1 (ABCC1/Abcc1) MRP4/Mrp4 (ABCC4/Abcc4) MRP5/Mrp5 (ABCC5/Abcc5) | Abluminal [82,91] Luminal [92] Luminal [82] | Abluminal [72] Luminal [72] Luminal [72] | Luminal [93] Not defined Luminal and Abluminal [75] | Luminal [94] Luminal and Abluminal [94] Luminal [94] | Not defined Not defined Not defined | Luminal [95] Luminal [79,95] Luminal [79,95] |
| Transporter | Representative Centrally Active Transport Substrates |
|---|---|
| OATPs/Oatps (SLCOs/Slcos) | HMG CoA Reductase Inhibitors (i.e., statins; atorvastatin, pravastatin, rosuvastatin) [5,96] Prostaglandin E2 [96] Estrone-3-Sulfate, Dihydroepiandrosterone Sulfate (DHEAS), Estradiol-17β-Glucuronide [97] |
| OCTs/Octs (SLC22A/Slc22a) | Memantine [5] Pramipexole, Selegiline, Varenicline [6] Amisulpride [98] Metformin [99] |
| MATE1/Mate1 (SLC47A1/Slc47a1) | Metformin, Thiamine, Topotecan [96] Amisulpride [98] |
| P-gp (MDR1/Mdr1) (ABCB1/Abcb1a/Abcb1b) | Amitriptyline, Cyclosporine A, Lapatinib, Losartan, Lovastatin, Phenytoin, Tetracycline, Verapamil [96] Atorvastatin, Rosuvastatin [100] Tacrolimus, Rifampicin [29] |
| BCRP/Bcrp (ABCG2/Abcg2) | Coumestrol, Daidzein, Dantrolene, Dipyridamole, Estradiol-17β-Glucuronide, Genistein, Glyburide, Lapatinib [96] Atorvastatin, Pravastatin, Rosuvastatin [100] Estrone-3-Sulfate, Dihydroepiandrosterone Sulfate (DHEAS), Dihydrotestosterone (DHT) [97] |
| MRPs/Mrps (ABCC/Abcc) | Glutathione (GSH), GSH Conjugates, GSSG [5] Estradiol-17β-Glucuronide [96] Estrone-3-Sulfate, Dihydroepiandrosterone Sulfate (DHEAS) [97] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nilles, K.L.; Williams, E.I.; Betterton, R.D.; Davis, T.P.; Ronaldson, P.T. Blood–Brain Barrier Transporters: Opportunities for Therapeutic Development in Ischemic Stroke. Int. J. Mol. Sci. 2022, 23, 1898. https://doi.org/10.3390/ijms23031898
Nilles KL, Williams EI, Betterton RD, Davis TP, Ronaldson PT. Blood–Brain Barrier Transporters: Opportunities for Therapeutic Development in Ischemic Stroke. International Journal of Molecular Sciences. 2022; 23(3):1898. https://doi.org/10.3390/ijms23031898
Chicago/Turabian StyleNilles, Kelsy L., Erica I. Williams, Robert D. Betterton, Thomas P. Davis, and Patrick T. Ronaldson. 2022. "Blood–Brain Barrier Transporters: Opportunities for Therapeutic Development in Ischemic Stroke" International Journal of Molecular Sciences 23, no. 3: 1898. https://doi.org/10.3390/ijms23031898
APA StyleNilles, K. L., Williams, E. I., Betterton, R. D., Davis, T. P., & Ronaldson, P. T. (2022). Blood–Brain Barrier Transporters: Opportunities for Therapeutic Development in Ischemic Stroke. International Journal of Molecular Sciences, 23(3), 1898. https://doi.org/10.3390/ijms23031898