
Tissue Biomarkers Predicting Lymph Node Status in Cutaneous Melanoma

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Tissue Biomarkers
2.1. Lymphovascular Invasion (LVI)
2.2. VEGF
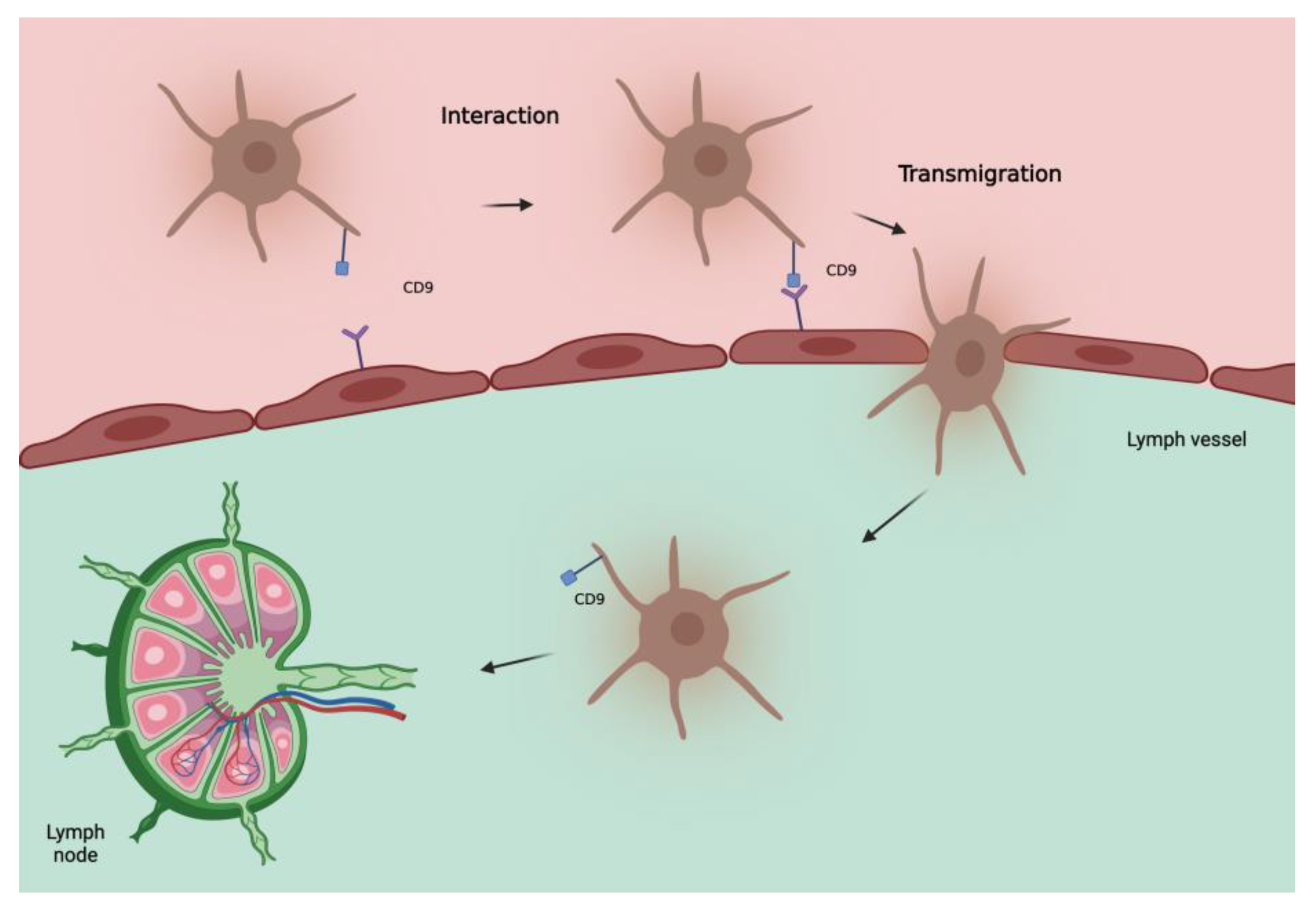
2.3. Tetraspanin CD9
2.4. LYVE-1 and D2-40
2.5. Gene Expression Profile Test (31-GEP)
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GEP | Gene expression profile |
| LVD | Lymphatic vessel density |
| LVI | Lymph vascular invasion |
| LYVE 1 | Lymphatic vessel endothelial hyaluronan receptor-1 |
| MEV | Melanoma extracellular vesicle |
| SLN | Sentinel lymph node |
References
- Strashilov, S.; Yordanov, A. Aetiology and Pathogenesis of Cutaneous Melanoma: Current Concepts and Advances. Int. J. Mol. Sci. 2021, 22, 6395. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, O.; Lucarini, G.; Rubini, C.; Lazzarini, R.; Di Primio, R.; Offidani, A. Clinical and prognostic significance of survivin, AKT and VEGF in primary mucosal oral melanoma. Anticancer Res. 2015, 35, 2113–2120. [Google Scholar] [PubMed]
- Simonetti, O.; Lucarini, G.; Rubini, C.; Goteri, G.; Zizzi, A.; Staibano, S.; Campanati, A.; Ganzetti, G.; di Primio, R.; Offidani, A. Microvessel density and VEGF, HIF-1α expression in primary oral melanoma: Correlation with prognosis. Oral Dis. 2012, 19, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Mazer, B.L.; Adamson, A.S. The Rapid Rise in Cutaneous Melanoma Diagnoses. N. Engl. J. Med. 2021, 384, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: Diagnostics—Update 2019. Eur. J. Cancer 2020, 126, 141–158. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Sacchetto, L.; Rosso, S.; Comber, H.; Bouchardy, C.; Broganelli, P.; Galceran, J.; Hackl, M.; Katalinic, A.; Louwman, M.; Robsahm, T.E.; et al. Skin melanoma deaths within 1 or 3 years from diagnosis in Europe. Int. J. Cancer 2021, 148, 2898–2905. [Google Scholar] [CrossRef]
- Prado, G.; Svoboda, R.M.; Rigel, D.S. What’s New in Melanoma. Dermatol. Clin. 2019, 37, 159–168. [Google Scholar] [CrossRef]
- Lucarini, G.; Simonetti, O.; Lazzarini, R.; Giantomassi, F.; Goteri, G.; Offidani, A. Vascular endothelial growth factor/semaphorin-3A ratio and SEMA3A expression in cutaneous malignant melanoma. Melanoma Res. 2020, 30, 433–442. [Google Scholar] [CrossRef]
- Simonetti, O.; Goteri, G.; Lucarini, G.; Rubini, C.; Stramazzotti, D.; Muzio, L.L.; Biagini, G.; Offidani, A. In Melanoma Changes of Immature and Mature Dendritic Cell Expression Correlate with Tumor Thickness: An Immunohistochemical Study. Int. J. Immunopathol. Pharmacol. 2007, 20, 325–333. [Google Scholar] [CrossRef]
- Prokopi, A.; Tripp, C.H.; Tummers, B.; Hornsteiner, F.; Spoeck, S.; Crawford, J.C.; Clements, D.R.; Efremova, M.; Hutter, K.; Bellmann, L.; et al. Skin dendritic cells in melanoma are key for successful checkpoint blockade therapy. J. Immunother. Cancer 2021, 9, e000832. [Google Scholar] [CrossRef] [PubMed]
- D’Aguanno, S.; Mallone, F.; Marenco, M.; Del Bufalo, D.; Moramarco, A. Hypoxia-dependent drivers of melanoma progression. J. Exp. Clin. Cancer Res. 2021, 40, 159. [Google Scholar] [CrossRef]
- Ribero, S.; Glass, D.; Bataille, V. Genetic epidemiology of melanoma. Eur. J. Dermatol. 2016, 26, 335–339. [Google Scholar] [CrossRef] [PubMed]
- García-López, M.A.; Barreiro, O.; García-Díez, A.; Sánchez-Madrid, F.; Peñas, P.F. Role of Tetraspanins CD9 and CD151 in Primary Melanocyte Motility. J. Investig. Dermatol. 2005, 125, 1001–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swetter, S.M.; Thompson, J.A.; Albertini, M.R.; Barker, C.A.; Baumgartner, J.; Boland, G.; Chmielowski, B.; DiMaio, D.; Durham, A.; Fields, R.C.; et al. NCCN Guidelines® Insights: Melanoma: Cutaneous, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 364–376. [Google Scholar] [CrossRef]
- AIOM Guidelines. Available online: https://snlg.iss.it/wp-content/uploads/2021/10/LG-127_Melanoma_agg2021.pdf (accessed on 22 October 2022).
- Scoggins, C.R.; Ross, M.I.; Reintgen, D.S.; Noyes, R.D.; Goydos, J.S.; Beitsch, P.D.; Urist, M.M.; Ariyan, S.; Davidson, B.S.; Sussman, J.J.; et al. Prospective Multi-Institutional Study of Reverse Transcriptase Polymerase Chain Reaction for Molecular Staging of Melanoma. J. Clin. Oncol. 2006, 24, 2849–2857. [Google Scholar] [CrossRef]
- Ji, R.-C. Lymphatic endothelial cells, tumor lymphangiogenesis and metastasis: New insights into intratumoral and peritumoral lymphatics. Cancer Metastasis Rev. 2006, 25, 677–694. [Google Scholar] [CrossRef]
- Xu, X.; Gimotty, P.A.; Guerry, D.; Karakousis, G.; Van Belle, P.; Liang, H.; Montone, K.; Pasha, T.; Ming, M.E.; Acs, G.; et al. Lymphatic invasion revealed by multispectral imaging is common in primary melanomas and associates with prognosis. Hum. Pathol. 2008, 39, 901–909. [Google Scholar] [CrossRef] [Green Version]
- Petersson, F.; Diwan, A.H.; Ivan, D.; Gershenwald, J.E.; Johnson, M.M.; Harrell, R.; Prieto, V.G. Immunohistochemical detection of lymphovascular invasion with D2-40 in melanoma correlates with sentinel lymph node status, metastasis and survival. J. Cutan. Pathol. 2009, 36, 1157–1163. [Google Scholar] [CrossRef]
- Petitt, M.; Allison, A.; Shimoni, T.; Uchida, T.; Raimer, S.; Kelly, B. Lymphatic invasion detected by D2-40/S-100 dual immunohistochemistry does not predict sentinel lymph node status in melanoma. J. Am. Acad. Dermatol. 2009, 61, 819–828. [Google Scholar] [CrossRef]
- Rose, A.E.; Christos, P.J.; Lackaye, D.; Shapiro, R.L.; Berman, R.; Mazumdar, M.; Kamino, H.; Osman, I.; Darvishian, F. Clinical Relevance of Detection of Lymphovascular Invasion in Primary Melanoma Using Endothelial Markers D2-40 and CD34. Am. J. Surg. Pathol. 2011, 35, 1441–1449. [Google Scholar] [CrossRef] [Green Version]
- Dadras, S.S.; Paul, T.; Bertoncini, J.; Brown, L.F.; Muzikansky, A.; Jackson, D.G.; Ellwanger, U.; Garbe, C.; Mihm, M.C.; Detmar, M. Tumor lymphangiogenesis: A novel prognostic indicator for cutaneous melanoma metastasis and survival. Am. J. Pathol. 2003, 162, 1951–1960. [Google Scholar] [CrossRef] [PubMed]
- Huber, G.F.; Fritzsche, F.R.; Züllig, L.; Storz, M.; Graf, N.; Haerle, S.K.; Jochum, W.; Stoeckli, S.J.; Moch, H. Podoplanin expression correlates with sentinel lymph node metastasis in early squamous cell carcinomas of the oral cavity and oropharynx. Int. J. Cancer 2010, 129, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Kilvaer, T.K.; Valkov, A.; Sorbye, S.; Smeland, E.; Bremnes, R.M.; Busund, L.-T.; Donnem, T. Profiling of VEGFs and VEGFRs as Prognostic Factors in Soft Tissue Sarcoma: VEGFR-3 Is an Independent Predictor of Poor Prognosis. PLoS ONE 2010, 5, e15368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Ma, J.; Wang, X.; Su, F.; Li, X.; Yang, S.; Ma, W.; Zhang, Y. Lymphangiogenesis and Its Relationship With Lymphatic Metastasis and Prognosis in Malignant Melanoma. Anat. Rec. 2008, 291, 1227–1235. [Google Scholar] [CrossRef]
- Buzrla, P.; Dvorackova, J.; Motyka, O. Lymphangiogenesis and Its Correlation with the VEGF Expression and the Sentinel Lymph Node in Cutaneous Melanomas. BioMed Res. Int. 2014, 2014, 372979. [Google Scholar] [CrossRef] [Green Version]
- Johnson, K.E.; Wilgus, T.A. Multiple Roles for VEGF in Non-Melanoma Skin Cancer: Angiogenesis and Beyond. J. Ski. Cancer 2012, 2012, 483439. [Google Scholar] [CrossRef] [Green Version]
- Gallego, E.; Vicioso, L.; Alvarez, M.; Hierro, I.; Perez-Villa, L.; Blanes, A.; Matilla, A. Stromal expression of vascular endo- thelial growth factor C is relevant to predict sentinel lymph node status in melanomas. Virchows Arch. 2011, 458, 621–630. [Google Scholar] [CrossRef]
- Boone, B.; Blokx, W.; De Bacquer, D.; Lambert, J.; Ruiter, D.; Brochez, L. The role of VEGF-C staining in predicting regional metastasis in melanoma. Virchows Arch. 2008, 453, 257–265. [Google Scholar] [CrossRef]
- Brychtova, S.; Bezdekova, M.; Brychta, T.; Tichy, M. The role of vascular endothelial growth factors and their receptors in malignant melanomas. Neoplasma 2008, 55, 273–279. [Google Scholar]
- Dadras, S.S.; Lange-Asschenfeldt, B.; Velasco, P.; Nguyen, L.; Vora, A.; Muzikansky, A.; Jahnke, K.; Hauschild, A.; Hirakawa, S.; Mihm, M.C.; et al. Tumor lymphangiogenesis predicts melanoma metastasis to sentinel lymph nodes. Mod. Pathol. 2005, 18, 1232–1242. [Google Scholar] [CrossRef] [PubMed]
- Toberer, F.; Haenssle, H.; Laimer, M.; Heinzel-Gutenbrunner, M.; Enk, A.; Hartschuh, W.; Helmbold, P.; Kutzner, H. Vascular Endothelial Growth Factor Receptor-3 Expression Predicts Sentinel Node Status in Primary Cutaneous Melanoma. Acta Derm. Venereol. 2020, 100, adv00235. [Google Scholar] [CrossRef] [PubMed]
- Hemler, M.E. Tetraspanin proteins promote multiple cancer stages. Nat. Rev. Cancer 2013, 14, 49–60. [Google Scholar] [CrossRef]
- Fan, J.; Zhu, G.-Z.; Niles, R.M. Expression and function of CD9 in melanoma cells. Mol. Carcinog. 2009, 49, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Powner, D.; Kopp, P.M.; Monkley, S.J.; Critchley, D.R.; Berditchevski, F. Tetraspanin CD9 in cell migration. Biochem. Soc. Trans. 2011, 39, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Lucarini, G.; Molinelli, E.; Licini, C.; Rizzetto, G.; Radi, G.; Goteri, G.; Mattioli-Belmonte, M.; Offidani, A.; Simonetti, O. Tetraspanin CD9 Expression Predicts Sentinel Node Status in Patients with Cutaneous Melanoma. Int. J. Mol. Sci. 2022, 23, 4775. [Google Scholar] [CrossRef]
- Liang, P.; Miao, M.; Liu, Z.; Wang, H.; Jiang, W.; Ma, S.; Li, C.; Hu, R. CD9 expression indicates a poor outcome in acute lymphoblastic leukemia. Cancer Biomark. 2018, 21, 781–786. [Google Scholar] [CrossRef]
- Huan, J.; Gao, Y.; Xu, J.; Sheng, W.; Zhu, W.; Zhang, S.; Cao, J.; Ji, J.; Zhang, L.; Tian, Y. Overexpression of CD9 correlates with tumor stage and lymph node metastasis in esophageal squamous cell carcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 3054–3061. [Google Scholar]
- Tasdemir, A.; Soyuer, I.; Unal, D.; Artis, T. Prognostic value of NF-κB, CD9, and VEGF in gastrointestinal stromal tumors. Contemp. Oncol. 2013, 17, 493–498. [Google Scholar] [CrossRef] [Green Version]
- Miki, Y.; Yashiro, M.; Okuno, T.; Kitayama, K.; Masuda, G.; Hirakawa, K.; Ohira, M. CD9-positive exosomes from cancer-associated fibroblasts stimulate the migration ability of scirrhous-type gastric cancer cells. Br. J. Cancer 2018, 118, 867–877. [Google Scholar] [CrossRef] [Green Version]
- Lu, W.; Fei, A.; Jiang, Y.; Chen, L.; Wang, Y. Tetraspanin CD9 interacts with α-secretase to enhance its oncogenic function in pancreatic cancer. Am. J. Transl. Res. 2020, 12, 5525–5537. [Google Scholar] [PubMed]
- Nagare, R.P.; Sneha, S.; Krishnapriya, S.; Ramachandran, B.; Murhekar, K.; Vasudevan, S.; Shabna, A.; Ganesan, T.S. ALDH1A1+ ovarian cancer stem cells co-expressing surface markers CD24, EPHA1 and CD9 form tumours in vivo. Exp. Cell Res. 2020, 392, 112009. [Google Scholar] [CrossRef] [PubMed]
- Logozzi, M.; Di Raimo, R.; Mizzoni, D.; Fais, S. Immunocapture-based ELISA to characterize and quantify exosomes in both cell culture supernatants and body fluids. Methods Enzymol. 2020, 645, 155–180. [Google Scholar] [CrossRef] [PubMed]
- Longo, N.; Yáñez-Mó, M.; Mittelbrunn, M.; De La Rosa, G.; Muňoz, M.-L.; Sánchez-Madrid, F.; Sánchez-Mateos, P. Regulatory role of tetraspanin CD9 in tumor–endothelial cell interaction during transendothelial invasion of melanoma cells. Blood 2001, 98, 3717–3726. [Google Scholar] [CrossRef] [Green Version]
- Erovic, B.M.; Neuchrist, C.; Kandutsch, S.; Woegerbauer, M.; Pammer, J. CD9 Expression on Lymphatic Vessels in Head and Neck Mucosa. Mod. Pathol. 2003, 16, 1028–1034. [Google Scholar] [CrossRef] [Green Version]
- Doeden, K.; Ma, Z.; Narasimhan, B.; Swetter, S.M.; Detmar, M.; Dadras, S.S. Lymphatic invasion in cutaneous melanoma is associated with sentinel lymph node metastasis. J. Cutan. Pathol. 2009, 36, 772–780. [Google Scholar] [CrossRef]
- Fohn, L.E.; Rodriguez, A.; Kelley, M.C.; Ye, F.; Shyr, Y.; Stricklin, G.; Robbins, J.B. D2-40 lymphatic marker for detecting lymphatic invasion in thin to intermediate thickness melanomas: Association with sentinel lymph node status and prognostic value—A retrospective case study. J. Am. Acad. Dermatol. 2011, 64, 336–345. [Google Scholar] [CrossRef]
- Gerami, P.; Cook, R.W.; Russell, M.C.; Wilkinson, J.; Amaria, R.N.; Gonzalez, R.; Lyle, S.; Jackson, G.L.; Greisinger, A.J.; Johnson, C.E.; et al. Gene expression profiling for molecular staging of cutaneous melanoma in patients undergoing sentinel lymph node biopsy. J. Am. Acad. Dermatol. 2015, 72, 780–785.e3. [Google Scholar] [CrossRef]
- Cook, R.W.; Middlebrook, B.; Wilkinson, J.; Covington, K.R.; Oelschlager, K.; Monzon, F.A.; Stone, J.F. Analytic validity of DecisionDx-Melanoma, a gene expression profile test for determining metastatic risk in melanoma patients. Diagn. Pathol. 2018, 13, 13. [Google Scholar] [CrossRef] [Green Version]
- Keller, J.; Schwartz, T.L.; Lizalek, J.M.; Chang, E.; Patel, A.D.; Hurley, M.Y.; Hsueh, E.C. Prospective validation of the prognostic 31-gene expression profiling test in primary cutaneous melanoma. Cancer Med. 2019, 8, 2205–2212. [Google Scholar] [CrossRef] [Green Version]
- Podlipnik, S.; Carrera, C.; Boada, A.; Richarz, N.A.; López-Estebaranz, J.; Pinedo-Moraleda, F.; Elosua-González, M.; Martín-González, M.; Carrillo-Gijón, R.; Redondo, P.; et al. Early outcome of a 31-gene expression profile test in 86 AJCC stage IB–II melanoma patients. A prospective multicentre cohort study. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Greenhaw, B.N.; Zitelli, J.A.; Brodland, D.G. Estimation of Prognosis in Invasive Cutaneous Melanoma: An Independent Study of the Accuracy of a Gene Expression Profile Test. Dermatol. Surg. 2018, 44, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, E.C.; DeBloom, J.R.; Lee, J.; Sussman, J.J.; Covington, K.R.; Middlebrook, B.; Johnson, C.; Cook, R.W.; Slingluff, C.L., Jr.; McMasters, K.M. Interim analysis of survival in a prospective, multi-center registry cohort of cutaneous melanoma tested with a prognostic 31-gene expression profile test. J. Hematol. Oncol. 2017, 10, 152. [Google Scholar] [CrossRef] [PubMed]
- Vetto, J.T.; Hsueh, E.C.; Gastman, B.R.; Dillon, L.D.; Monzon, F.A.; Cook, R.W.; Keller, J.; Huang, X.; Fleming, A.; Hewgley, P.; et al. Guidance of sentinel lymph node biopsy decisions in patients with T1–T2 melanoma using gene expression profiling. Futur. Oncol. 2019, 15, 1207–1217. [Google Scholar] [CrossRef] [Green Version]
- Gastman, B.R.; Gerami, P.; Kurley, S.J.; Cook, R.W.; Leachman, S.; Vetto, J.T. Identification of patients at risk of metastasis using a prognostic 31-gene expression profile in subpopulations of melanoma patients with favorable outcomes by standard criteria. J. Am. Acad. Dermatol. 2018, 80, 149–157.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, M.J.; Monzon, F.A.; Zager, J.S. Sentinel lymph node biopsy in melanoma: Beyond histologic factors. Clin. Exp. Metastasis 2021, 39, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Pingault, V.; Bondurand, N.; Kuhlbrodt, K.; Goerich, D.E.; Préhu, M.-O.; Puliti, A.; Herbarth, B.; Hermans-Borgmeyer, I.; Legius, E.; Matthijs, G.; et al. SOX10 mutations in patients with Waardenburg-Hirschsprung disease. Nat. Genet. 1998, 18, 171–173. [Google Scholar] [CrossRef]
- Ludwig, A.; Rehberg, S.; Wegner, M. Melanocyte-specific expression of dopachrome tautomerase is dependent on synergistic gene activation by the Sox10 and Mitf transcription factors. FEBS Lett. 2003, 556, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Ramos-Herberth, F.I.; Karamchandani, J.; Kim, J.; Dadras, S.S. SOX10 immunostaining distinguishes desmoplastic melanoma from excision scar. J. Cutan. Pathol. 2010, 37, 944–952. [Google Scholar] [CrossRef]
- Blochin, E.; Nonaka, D. Diagnostic value of Sox10 immunohistochemical staining for the detection of metastatic melanoma in sentinel lymph nodes. Histopathology 2009, 55, 626–628. [Google Scholar] [CrossRef]
- Manninen, A.; Gardberg, M.; Juteau, S.; Ilmonen, S.; Jukonen, J.; Andersson, N.; Carpén, O. BRAF immunohistochemistry predicts sentinel lymph node involvement in intermediate thickness melanomas. PLoS ONE 2019, 14, e0216043. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; López-Beltrán, A.; Massari, F.; MacLennan, G.T.; Montironi, R. Molecular testing for BRAF mutations to inform melanoma treatment decisions: A move toward precision medicine. Mod. Pathol. 2017, 31, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, E.; Gervais, M.-K.; Shah, P.S.; Hong, N.J.L.; Wright, F.C. Sentinel Lymph Node Biopsy in Thin Cutaneous Melanoma: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2016, 23, 4178–4188. [Google Scholar] [CrossRef] [PubMed]
- Tejera-Vaquerizo, A.; Ribero, S.; Puig, S.; Boada, A.; Paradela, S.; Moreno-Ramírez, D.; Cañueto, J.; de Unamuno, B.; Brinca, A.; Descalzo-Gallego, M.A.; et al. Survival analysis and sentinel lymph node status in thin cutaneous melanoma: A multicenter observational study. Cancer Med. 2019, 8, 4235–4244. [Google Scholar] [CrossRef] [Green Version]
- Murtha, T.D.; Han, G.; Han, D. Predictors for Use of Sentinel Node Biopsy and the Association with Improved Survival in Melanoma Patients Who Have Nodal Staging. Ann. Surg. Oncol. 2018, 25, 903–911. [Google Scholar] [CrossRef]
- Smith, N.R.; Baker, D.; James, N.H.; Ratcliffe, K.; Jenkins, M.; Ashton, S.E.; Sproat, G.; Swann, R.; Gray, N.; Ryan, A.; et al. Vascular Endothelial Growth Factor Receptors VEGFR-2 and VEGFR-3 Are Localized Primarily to the Vasculature in Human Primary Solid Cancers. Clin. Cancer Res. 2010, 16, 3548–3561. [Google Scholar] [CrossRef] [Green Version]
- Mehnert, J.M.; McCarthy, M.M.; Jilaveanu, L.; Flaherty, K.T.; Aziz, S.; Camp, R.L.; Rimm, D.L.; Kluger, H.M. Quantitative expression of VEGF, VEGF-R1, VEGF-R2, and VEGF-R3 in melanoma tissue microarrays. Hum. Pathol. 2010, 41, 375–384. [Google Scholar] [CrossRef] [Green Version]
- Murali, R.; Haydu, L.E.; Quinn, M.J.; Saw, R.P.M.; Shannon, K.; Spillane, A.J.; Stretch, J.R.; Thompson, J.F.; Scolyer, R.A. Sentinel Lymph Node Biopsy in Patients With Thin Primary Cutaneous Melanoma. Ann. Surg. 2012, 255, 128–133. [Google Scholar] [CrossRef]
- Bertolli, E.; de Macedo, M.P.; Pinto, C.A.L.; Damascena, A.S.; Molina, A.S.; Ueno, P.S.; Neto, J.P.D. Evaluation of Melanoma Features and Their Relationship with Nodal Disease: The Importance of the Pathological Report. Tumori J. 2015, 101, 501–505. [Google Scholar] [CrossRef]
- Egger, M.E.; Stevenson, M.; Bhutiani, N.; Jordan, A.C.; Scoggins, C.R.; Philips, P.; Martin, R.C.G.; McMasters, K.M. Age and Lymphovascular Invasion Accurately Predict Sentinel Lymph Node Metastasis in T2 Melanoma Patients. Ann. Surg. Oncol. 2019, 26, 3955–3961. [Google Scholar] [CrossRef]
- Namikawa, K.; Aung, P.P.; Gershenwald, J.E.; Milton, D.R.; Prieto, V.G. Clinical impact of ulceration width, lymphovascular invasion, microscopic satellitosis, perineural invasion, and mitotic rate in patients undergoing sentinel lymph node biopsy for cutaneous melanoma: A retrospective observational study at a comprehensive. Cancer Med. 2018, 7, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, E.K.; Gupta, M.; Datta, J.; Gimotty, P.A.; Guerry, D.; Xu, X.; Elder, D.E.; Czerniecki, B.J.; Fraker, U.L.; Karakousis, G.C. Prognosis of patients with melanoma and microsatellitosis undergoing sentinel lymph node biopsy. Ann. Surg. Oncol. 2013, 21, 1016–1023. [Google Scholar] [CrossRef] [PubMed]
- Burton, A.L.; Gilbert, J.; Farmer, R.W.; Stromberg, A.J.; Hagendoorn, L.; Ross, M.I.; Martin, I.R.C.G.; Mcmasters, K.M.; Scoggins, C.R.; Callender, G.G. Regression Does Not Predict Nodal Metastasis or Survival in Patients with Cutaneous Melanoma. Am. Surg. 2011, 77, 1009–1013. [Google Scholar] [CrossRef]
- Balch, C.M.; Thompson, J.F.; Gershenwald, J.E.; Soong, S.-J.; Ding, S.; McMasters, K.M.; Coit, D.G.; Eggermont, A.M.M.; Gimotty, P.A.; Johnson, T.M.; et al. Age as a Predictor of Sentinel Node Metastasis among Patients with Localized Melanoma: An Inverse Correlation of Melanoma Mortality and Incidence of Sentinel Node Metastasis Among Young and Old Patients. Ann. Surg. Oncol. 2014, 21, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Fayne, R.A.; Macedo, F.I.; Rodgers, S.E.; Möller, M.G. Evolving management of positive regional lymph nodes in melanoma: Past, present and future directions. Oncol. Rev. 2019, 13, 433. [Google Scholar] [CrossRef] [Green Version]
- Dillon, L.D.; McPhee, M.; Davidson, R.S.; Quick, A.P.; Martin, B.; Covington, K.R.; Zolochevska, O.; Cook, R.W.; Vetto, J.T.; Jarell, A.D.; et al. Expanded evidence that the 31-gene expression profile test provides clinical utility for melanoma management in a multicenter study. Curr. Med. Res. Opin. 2022, 38, 1267–1274. [Google Scholar] [CrossRef]
- Leary, N.; Walser, S.; He, Y.; Cousin, N.; Pereira, P.; Gallo, A.; Collado-Diaz, V.; Halin, C.; Garcia-Silva, S.; Peinado, H.; et al. Melanoma-derived extracellular vesicles mediate lymphatic remodelling and impair tumour immunity in draining lymph nodes. J. Extracell. Vesicles 2022, 11, e12197. [Google Scholar] [CrossRef]
- Maus, R.L.; Jakub, J.W.; Hieken, T.J.; Nevala, W.K.; Christensen, T.A.; Sutor, S.L.; Flotte, T.J.; Markovic, S.N. Identification of novel, immune-mediating extracellular vesicles in human lymphatic effluent draining primary cutaneous melanoma. OncoImmunology 2019, 8, e1667742. [Google Scholar] [CrossRef] [Green Version]
- Surman, M.; Stępień, E.; Przybyło, M. Melanoma-Derived Extracellular Vesicles: Focus on Their Proteome. Proteomes 2019, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Moosavian, S.A.; Hashemi, M.; Etemad, L.; Daneshmand, S.; Salmasi, Z. Melanoma-derived exosomes: Versatile extracellular vesicles for diagnosis, metastasis, immune modulation, and treatment of melanoma. Int. Immunopharmacol. 2022, 113, 109320. [Google Scholar] [CrossRef]


{kind=link}
|
| Biomarker | Rationale | Sample | Results |
|---|---|---|---|
| VEGFR-3 Toberer et al. [33] | Involved in the stimulation of lymphangiogenesis | 58 patients |
|
| Tetraspanin CD9 Lucarini et al. [37] | Transmembrane protein, key role in tumor progression Both suppressor and promoter of metastases, depending on the status of the cell membrane and vesicular structures | 140 patients Melanocytic nevus 20 Primary melanoma 120
|
|
| LYVE-1 Doeden et al. [47] | LYVE-1 selective marker of lymphatic vessels | 94 patients |
|
| D2-40 Fohn et al. [48] | D2-40 endothelial marker (podoplanin) In combination, better histological definition of LVI | 158 patients Primary melanomas ≤ 2.0 mm |
|
| 31-GEP Vetto et al. [55] | Gene expression profile test, (markers for cell migration/chemotaxis/metastasis, secretory molecules, adhesion, lymphocyte invasion, transcription factors, differentiation/proliferation structural proteins and surface receptors) Identifies high-risk (>5%) patients, candidates for SLN | 690 patients (total validation cohort, retrospective) staged I–III follow-up median 7 years 1421 patients (prospectively-tested) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzetto, G.; Lucarini, G.; De Simoni, E.; Molinelli, E.; Mattioli-Belmonte, M.; Offidani, A.; Simonetti, O. Tissue Biomarkers Predicting Lymph Node Status in Cutaneous Melanoma. Int. J. Mol. Sci. 2023, 24, 144. https://doi.org/10.3390/ijms24010144
Rizzetto G, Lucarini G, De Simoni E, Molinelli E, Mattioli-Belmonte M, Offidani A, Simonetti O. Tissue Biomarkers Predicting Lymph Node Status in Cutaneous Melanoma. International Journal of Molecular Sciences. 2023; 24(1):144. https://doi.org/10.3390/ijms24010144
Chicago/Turabian StyleRizzetto, Giulio, Guendalina Lucarini, Edoardo De Simoni, Elisa Molinelli, Monica Mattioli-Belmonte, Annamaria Offidani, and Oriana Simonetti. 2023. "Tissue Biomarkers Predicting Lymph Node Status in Cutaneous Melanoma" International Journal of Molecular Sciences 24, no. 1: 144. https://doi.org/10.3390/ijms24010144
APA StyleRizzetto, G., Lucarini, G., De Simoni, E., Molinelli, E., Mattioli-Belmonte, M., Offidani, A., & Simonetti, O. (2023). Tissue Biomarkers Predicting Lymph Node Status in Cutaneous Melanoma. International Journal of Molecular Sciences, 24(1), 144. https://doi.org/10.3390/ijms24010144