


Evaluation of Human Papilloma Virus (HPV) Genotyping and Viral Load Determination as Diagnostic Biomarkers of Cervical Cancer Risk

 , , , , ,
, , , , ,  ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Study Population
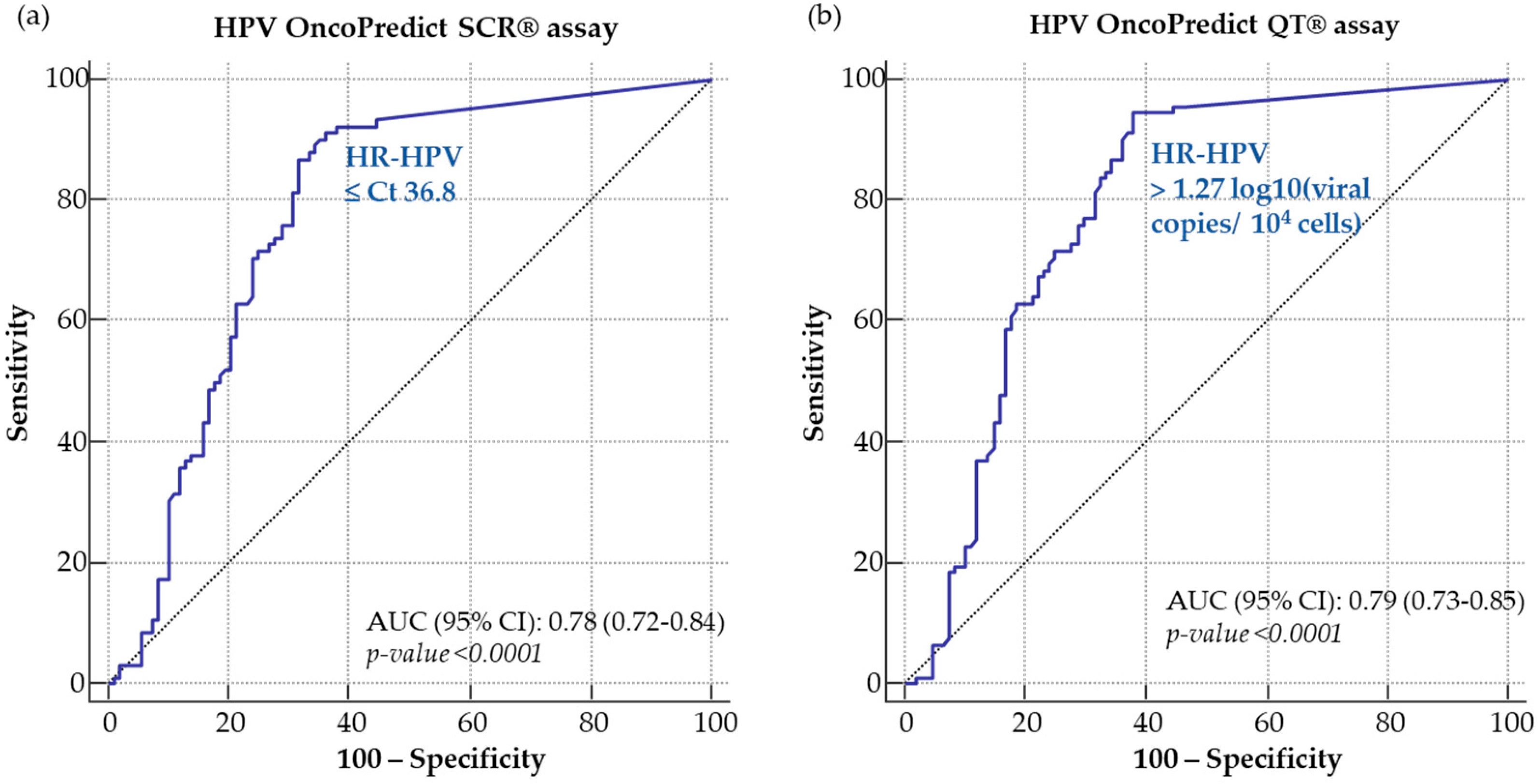
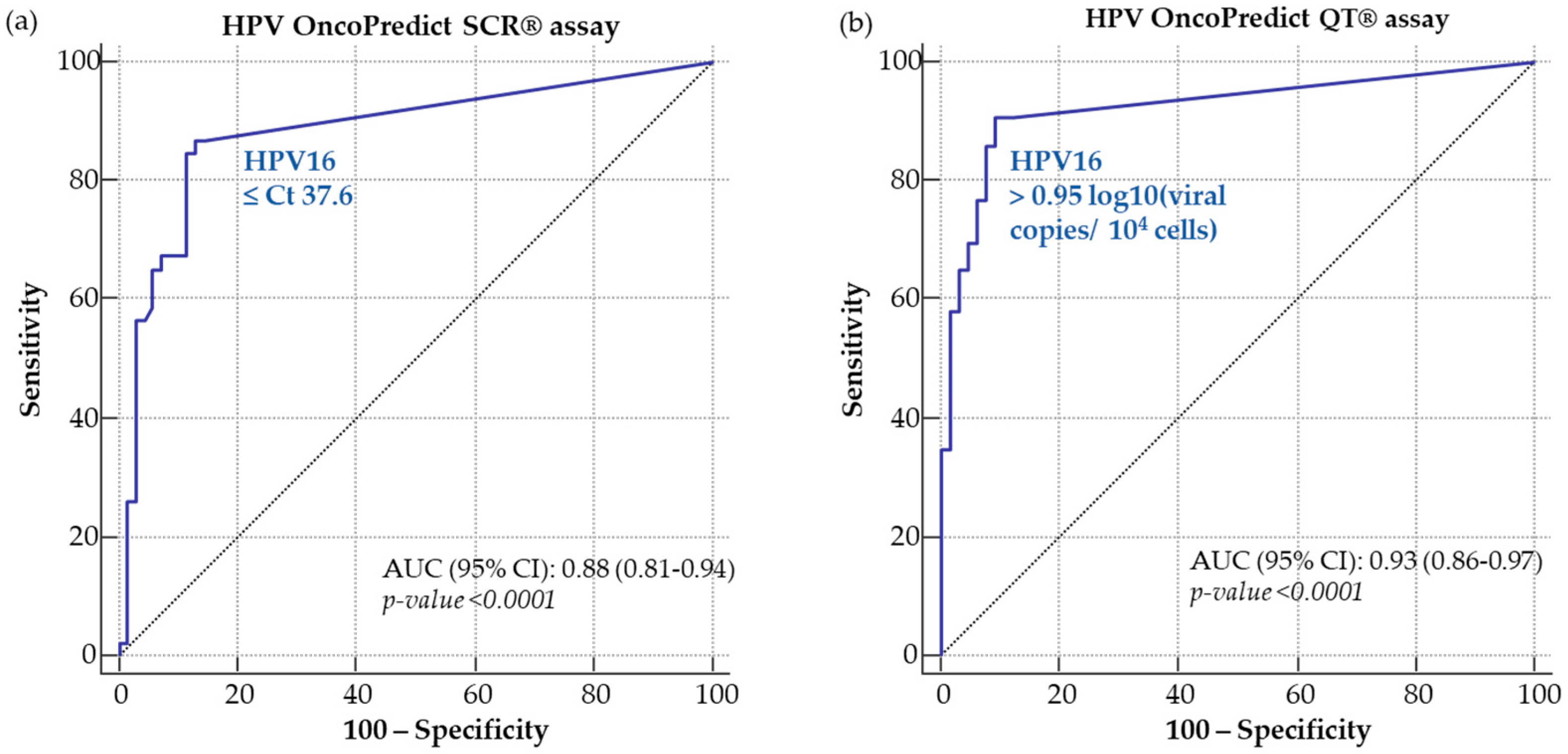
2.2. Cutoff Determination
2.3. Analytical Agreement of OncoPredict HPV® SCR and QT Assays Compared to Anyplex™ II HR-HPV
2.4. Clinical Performance of OncoPredict HPV® SCR and QT Assays
2.5. HR-HPV Prevalence and Genotype Distribution
2.6. HPV Viral Load
3. Discussion
4. Materials and Methods
4.1. Study Population and Sample Collection
4.2. Nucleic Acid Extraction, HPV Typing and Viral Load Quantification
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.M.; Muñoz, N. Human Papillomavirus Is a Necessary Cause of Invasive Cervical Cancer Worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Meijer, C.J.L.M.; Berkhof, J.; Castle, P.E.; Hesselink, A.T.; Franco, E.L.; Ronco, G.; Arbyn, M.; Bosch, F.X.; Cuzick, J.; Dillner, J.; et al. Guidelines for Human Papillomavirus DNA Test Requirements for Primary Cervical Cancer Screening in Women 30 Years and Older. Int. J. Cancer 2009, 124, 516–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkstra, M.G.; Snijders, P.J.F.; Arbyn, M.; Rijkaart, D.C.; Berkhof, J.; Meijer, C.J.L.M. Cervical Cancer Screening: On the Way to a Shift from Cytology to Full Molecular Screening. Ann. Oncol. 2014, 25, 927–935. [Google Scholar] [CrossRef]
- Dillner, J.; Rebolj, M.; Birembaut, P.; Petry, K.-U.; Szarewski, A.; Munk, C.; de Sanjose, S.; Naucler, P.; Lloveras, B.; Kjaer, S.; et al. Long Term Predictive Values of Cytology and Human Papillomavirus Testing in Cervical Cancer Screening: Joint European Cohort Study. BMJ 2008, 337, a1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GISCi. Raccomandazioni Sul Test HR HPV Come Test Di Screening Primario. 2017. Available online: https://gisci.it/documenti/documenti_gisci/Raccomandazioni_test_hr-hpv_2017.pdf (accessed on 21 September 2022).
- GISCi in Collaboration with AIO, AOGOI, SIAPEC-IAV, SICi, SICPCV, SIGO, SItI, SIV-ISV. Linee Guida Condivise per La Prevenzione Del Carcinoma Della Cervice Uterina. 2020. Available online: https://snlg.iss.it/wp-content/uploads/2020/07/LLGG-197-GISCi_et_al-vaccino-HPV-20luglio_Racc1.pdf (accessed on 9 September 2022).
- Adcock, R.; Cuzick, J.; Hunt, W.C.; McDonald, R.M.; Wheeler, C.M. Role of HPV Genotype, Multiple Infections, and Viral Load on the Risk of High-Grade Cervical Neoplasia. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1816–1824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuzick, J.; Ho, L.; Terry, G.; Kleeman, M.; Giddings, M.; Austin, J.; Cadman, L.; Ashdown-Barr, L.; Costa, M.J.; Szarewski, A. Individual Detection of 14 High Risk Human Papilloma Virus Genotypes by the PapType Test for the Prediction of High Grade Cervical Lesions. J. Clin. Virol. 2014, 60, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J.; Wheeler, C. Need for Expanded HPV Genotyping for Cervical Screening. Papillomavirus Res. 2016, 2, 112–115. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kim, B.K.; Jeon, D.; Lee, C.H.; Roh, J.-W.; Kim, J.-Y.; Park, S.-Y. Type-Specific Viral Load and Physical State of HPV Type 16, 18, and 58 as Diagnostic Biomarkers for High-Grade Squamous Intraepithelial Lesions or Cervical Cancer. Cancer Res. Treat. 2020, 52, 396–405. [Google Scholar] [CrossRef]
- Wu, Z.; Qin, Y.; Yu, L.; Lin, C.; Wang, H.; Cui, J.; Liu, B.; Liao, Y.; Warren, D.; Zhang, X.; et al. Association between Human Papillomavirus (HPV) 16, HPV18, and Other HR-HPV Viral Load and the Histological Classification of Cervical Lesions: Results from a Large-Scale Cross-Sectional Study: HR-HPV Viral Load and Cervical Lesions. J. Med. Virol. 2017, 89, 535–541. [Google Scholar] [CrossRef]
- Segondy, M.; Ngou, J.; Kelly, H.; Omar, T.; Goumbri-Lompo, O.; Doutre, S.; Mayaud, P.; Didelot, M.-N. Diagnostic Value of Human Papillomavirus (HPV) 16 and HPV18 Viral Loads for the Detection of High-Grade Cervical Intraepithelial Neoplasia (CIN2+) in a Cohort of African Women Living with HIV. J. Clin. Virol. 2018, 99, 79–83. [Google Scholar] [CrossRef]
- Dong, B.; Sun, P.; Ruan, G.; Huang, W.; Mao, X.; Kang, Y.; Pan, D.; Lin, F. Type-Specific High-Risk Human Papillomavirus Viral Load as a Viable Triage Indicator for High-Grade Squamous Intraepithelial Lesion: A Nested Case–Control Study. CMAR 2018, 10, 4839–4851. [Google Scholar] [CrossRef] [Green Version]
- Depuydt, C.E.; Jonckheere, J.; Berth, M.; Salembier, G.M.; Vereecken, A.J.; Bogers, J.J. Serial Type-Specific Human Papillomavirus (HPV) Load Measurement Allows Differentiation between Regressing Cervical Lesions and Serial Virion Productive Transient Infections. Cancer Med. 2015, 4, 1294–1302. [Google Scholar] [CrossRef] [PubMed]
- Del Mistro, A.; Adcock, R.; Carozzi, F.; Gillio-Tos, A.; De Marco, L.; Girlando, S.; Rizzolo, R.; Frayle, H.; Trevisan, M.; Sani, C.; et al. The New Technologies for Cervical CancerWorking Group. Human Papilloma Virus Genotyping for the Cross-Sectional and Longitudinal Probability of Developing Cervical Intraepithelial Neoplasia Grade 2 or More: HPV Genotyping for Risk Stratification. Int. J. Cancer 2018, 143, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oyervides-Muñoz, M.A.; Pérez-Maya, A.A.; Sánchez-Domínguez, C.N.; Berlanga-Garza, A.; Antonio-Macedo, M.; Valdéz-Chapa, L.D.; Cerda-Flores, R.M.; Trevino, V.; Barrera-Saldaña, H.A.; Garza-Rodríguez, M.L. Multiple HPV Infections and Viral Load Association in Persistent Cervical Lesions in Mexican Women. Viruses 2020, 12, 380. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, H.; Zhang, Y.; Jing, X.; Wu, N.; Hou, Y.; Hao, C. Correlation between Multi-type Human Papillomavirus Infections and Viral Loads and the Cervical Pathological Grade. Int. J. Gynecol. Obstet. 2021, 152, 96–102. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Arbyn, M.; Bergeron, C.; Bosch, F.X.; Dillner, J.; Jit, M.; Kim, J.; Poljak, M.; Nieminen, P.; Sasieni, P.; et al. Cervical Screening: ESGO-EFC Position Paper of the European Society of Gynaecologic Oncology (ESGO) and the European Federation of Colposcopy (EFC). Br. J. Cancer 2020, 123, 510–517. [Google Scholar] [CrossRef]
- Oštrbenk, A.; Xu, L.; Arbyn, M.; Poljak, M. Clinical and Analytical Evaluation of the Anyplex II HPV HR Detection Assay within the VALGENT-3 Framework. J. Clin. Microbiol. 2018, 56, e01176-18. [Google Scholar] [CrossRef] [Green Version]
- Benoy, I.; Xu, L.; Vanden Broeck, D.; Poljak, M.; Oštrbenk Valenčak, A.; Arbyn, M.; Bogers, J. Using the VALGENT-3 Framework to Assess the Clinical and Analytical Performance of the RIATOL QPCR HPV Genotyping Assay. J. Clin. Virol. 2019, 120, 57–62. [Google Scholar] [CrossRef]
- Cuschieri, K.; Geraets, D.T.; Moore, C.; Quint, W.; Duvall, E.; Arbyn, M. Clinical and Analytical Performance of the Onclarity HPV Assay Using the VALGENT Framework. J. Clin. Microbiol. 2015, 53, 3272–3279. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Dong, B.; Zhang, Q.; Mao, X.; Lin, W.; Ruan, G.; Kang, Y.; Sun, P. HR-HPV Viral Load Quality Detection Provide More Accurate Prediction for Residual Lesions after Treatment: A Prospective Cohort Study in Patients with High-Grade Squamous Lesions or Worse. Med. Oncol. 2020, 37, 37. [Google Scholar] [CrossRef]
- Arbyn, M.; Depuydt, C.; Benoy, I.; Bogers, J.; Cuschieri, K.; Schmitt, M.; Pawlita, M.; Geraets, D.; Heard, I.; Gheit, T.; et al. VALGENT: A Protocol for Clinical Validation of Human Papillomavirus Assays. J. Clin. Virol. 2016, 76, S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Chen, Y.; Li, L.; Yu, G.; Zhang, Y.; He, Y. Associations of High-Risk HPV Types and Viral Load with Cervical Cancer in China. J. Clin. Virol. 2006, 35, 264–269. [Google Scholar] [CrossRef]
- de Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human Papillomavirus Genotype Attribution in Invasive Cervical Cancer: A Retrospective Cross-Sectional Worldwide Study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Wentzensen, N.; Schiffman, M.; Dunn, T.; Zuna, R.E.; Gold, M.A.; Allen, R.A.; Zhang, R.; Sherman, M.E.; Wacholder, S.; Walker, J.; et al. Multiple Human Papillomavirus Genotype Infections in Cervical Cancer Progression in the Study to Understand Cervical Cancer Early Endpoints and Determinants. Int. J. Cancer 2009, 125, 2151–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, L.; Du, H.; Wang, C.; Huang, X.; Qu, X.; Shi, B.; Liu, Y.; Zhang, W.; Duan, X.; Wei, L.; et al. The Application of BMRT-HPV Viral Load to Secondary Screening Strategies for Cervical Cancer. PLoS ONE 2020, 15, e0232117. [Google Scholar] [CrossRef]
- Luo, H.; Du, H.; Belinson, J.L.; Wu, R. Evaluation of Alternately Combining HPV Viral Load and 16/18 Genotyping in Secondary Screening Algorithms. PLoS ONE 2019, 14, e0220200. [Google Scholar] [CrossRef]
- Manawapat-Klopfer, A.; Wang, L.; Haedicke-Jarboui, J.; Stubenrauch, F.; Munk, C.; Thomsen, L.T.; Martus, P.; Kjaer, S.K.; Iftner, T. HPV16 Viral Load and Physical State Measurement as a Potential Immediate Triage Strategy for HR-HPV-Infected Women: A Study in 644 Women with Single HPV16 Infections. Am. J. Cancer Res. 2018, 8, 715–722. [Google Scholar]
- WHO Classification of Tumours Editorial Board. World Health Organization Classification of Tumours. In Female Genital Tumours, 5th ed.; IARC Press: Lyon, France, 2020. [Google Scholar]



{kind=link}
{kind=link}
| Agreement between OncoPredict HPV® SCR and AnyplexTM II HR-HPV | Agreement between OncoPredict HPV® QT and AnyplexTM II HR-HPV | |||
|---|---|---|---|---|
| HPV16 | HR-HPV | HPV16 | HR-HPV | |
| Positive Agreement n (%) | 54/56 (96.4) | 127/141 (90.1) | 54/56 (96.4) | 131/141 (92.9) |
| Negative Agreement n (%) | 141/144 (97.9) | 53/59 (89.8) | 136/144 (94.4) | 52/59 (88.1) |
| Overall Agreement n (%) | 195/200 (97.5) | 180/200 (90.0) | 190/200 (95.0) | 182/200 (91.0) |
| Kappa (95% CI) | 0.94 (0.89–0.99) | 0.77 (0.67–0.86) | 0.88 (0.81–0.95) | 0.80 (0.71–0.89) |
| Real-Time Assay | Clinical Sensitivity (%) (95% CI) | Clinical Specificity (%) (95% CI) | Relative Sensitivity to Anyplex™ II HR-HPV (95% CI) | Relative Specificity to Anyplex™ II HR-HPV (95% CI) |
|---|---|---|---|---|
| Anyplex™ II HR-HPV | 94.6 (87.9–97.6) | 50.0 (40.7–59.2) | - | - |
| OncoPredict HPV® SCR | 87.0 (78.3–93.1) | 67.6 (57.9–76.3) | 0.92 (0.84–1.01) | 1.35 (1.08–1.70) |
| OncoPredict HPV® QT | 94.6 (87.8–98.2) | 62.0 (52.2–71.2) | 1.00 (0.93–1.07) | 1.24 (0.98–1.58) |
| Predominant Genotype | Single Infection (n = 79) | Coinfections (n = 59) | p-Value |
|---|---|---|---|
| HPV16 n (%) | 33 (41.8) | 14 (23.7) | 0.06 |
| HPV18 n (%) | 3 (3.8) | 6 (10.2) | |
| HPV31 n (%) | 18 (22.8) | 10 (17.0) | |
| HPV33 n (%) | 1 (1.3) | 3 (5.1) | |
| HPV35 n (%) | 2 (2.5) | 1 (1.7) | |
| HPV39 n (%) | 2 (2.5) | 3 (5.1) | |
| HPV45 n (%) | 4 (5.1) | 3 (5.1) | |
| HPV51 n (%) | 3 (3.8) | 7 (11.9) | |
| HPV52 n (%) | 2 (2.5) | 3 (5.1) | |
| HPV56 n (%) | 3 (3.8) | 0 (0.0) | |
| HPV58 n (%) | 7 (8.9) | 4 (6.8) | |
| HPV59 n (%) | 1 (1.3) | 5 (8.5) |
| Predominant Genotype | CIN2− HPV Positive (n = 50) | CIN2+ HPV Positive (n = 88) | p-Value |
|---|---|---|---|
| HPV16 n (%) | 8 (16.0) | 39 (44.3) | 0.009 |
| HPV18 n (%) | 4 (8.0) | 5 (5.7) | |
| HPV31 n (%) | 9 (18.0) | 19 (21.6) | |
| HPV33 n (%) | 1 (2.0) | 3 (3.4) | |
| HPV35 n (%) | 2 (4.0) | 1 (1.1) | |
| HPV39 n (%) | 4 (8.0) | 1 (1.1) | |
| HPV45 n (%) | 2 (4.0) | 5 (5.7) | |
| HPV51 n (%) | 7 (14.0) | 3 (3.4) | |
| HPV52 n (%) | 2 (4.0) | 3 (3.4) | |
| HPV56 n (%) | 2 (4.0) | 1 (1.4) | |
| HPV58 n (%) | 6 (12.0) | 5 (5.7) | |
| HPV59 n (%) | 3 (6.0) | 3 (3.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinelli, M.; Giubbi, C.; Saderi, L.; Musumeci, R.; Perdoni, F.; Leone, B.E.; Fruscio, R.; Landoni, F.; Piana, A.; Sotgiu, G.; et al. Evaluation of Human Papilloma Virus (HPV) Genotyping and Viral Load Determination as Diagnostic Biomarkers of Cervical Cancer Risk. Int. J. Mol. Sci. 2023, 24, 1320. https://doi.org/10.3390/ijms24021320
Martinelli M, Giubbi C, Saderi L, Musumeci R, Perdoni F, Leone BE, Fruscio R, Landoni F, Piana A, Sotgiu G, et al. Evaluation of Human Papilloma Virus (HPV) Genotyping and Viral Load Determination as Diagnostic Biomarkers of Cervical Cancer Risk. International Journal of Molecular Sciences. 2023; 24(2):1320. https://doi.org/10.3390/ijms24021320
Chicago/Turabian StyleMartinelli, Marianna, Chiara Giubbi, Laura Saderi, Rosario Musumeci, Federica Perdoni, Biagio Eugenio Leone, Robert Fruscio, Fabio Landoni, Andrea Piana, Giovanni Sotgiu, and et al. 2023. "Evaluation of Human Papilloma Virus (HPV) Genotyping and Viral Load Determination as Diagnostic Biomarkers of Cervical Cancer Risk" International Journal of Molecular Sciences 24, no. 2: 1320. https://doi.org/10.3390/ijms24021320
APA StyleMartinelli, M., Giubbi, C., Saderi, L., Musumeci, R., Perdoni, F., Leone, B. E., Fruscio, R., Landoni, F., Piana, A., Sotgiu, G., & Cocuzza, C. E. (2023). Evaluation of Human Papilloma Virus (HPV) Genotyping and Viral Load Determination as Diagnostic Biomarkers of Cervical Cancer Risk. International Journal of Molecular Sciences, 24(2), 1320. https://doi.org/10.3390/ijms24021320