

In Vivo Biofilm Formation on Novel PEEK, Titanium, and Zirconia Implant Abutment Materials

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
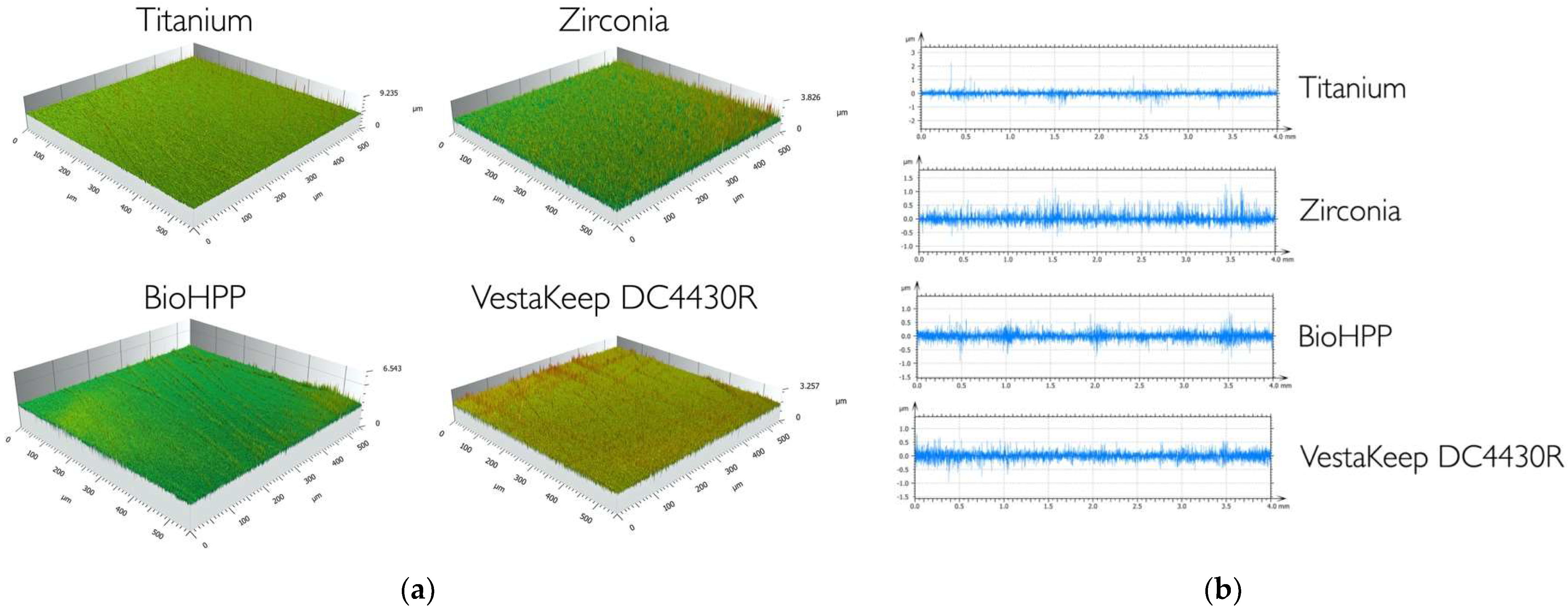
2.1. Characterization of Test Surfaces
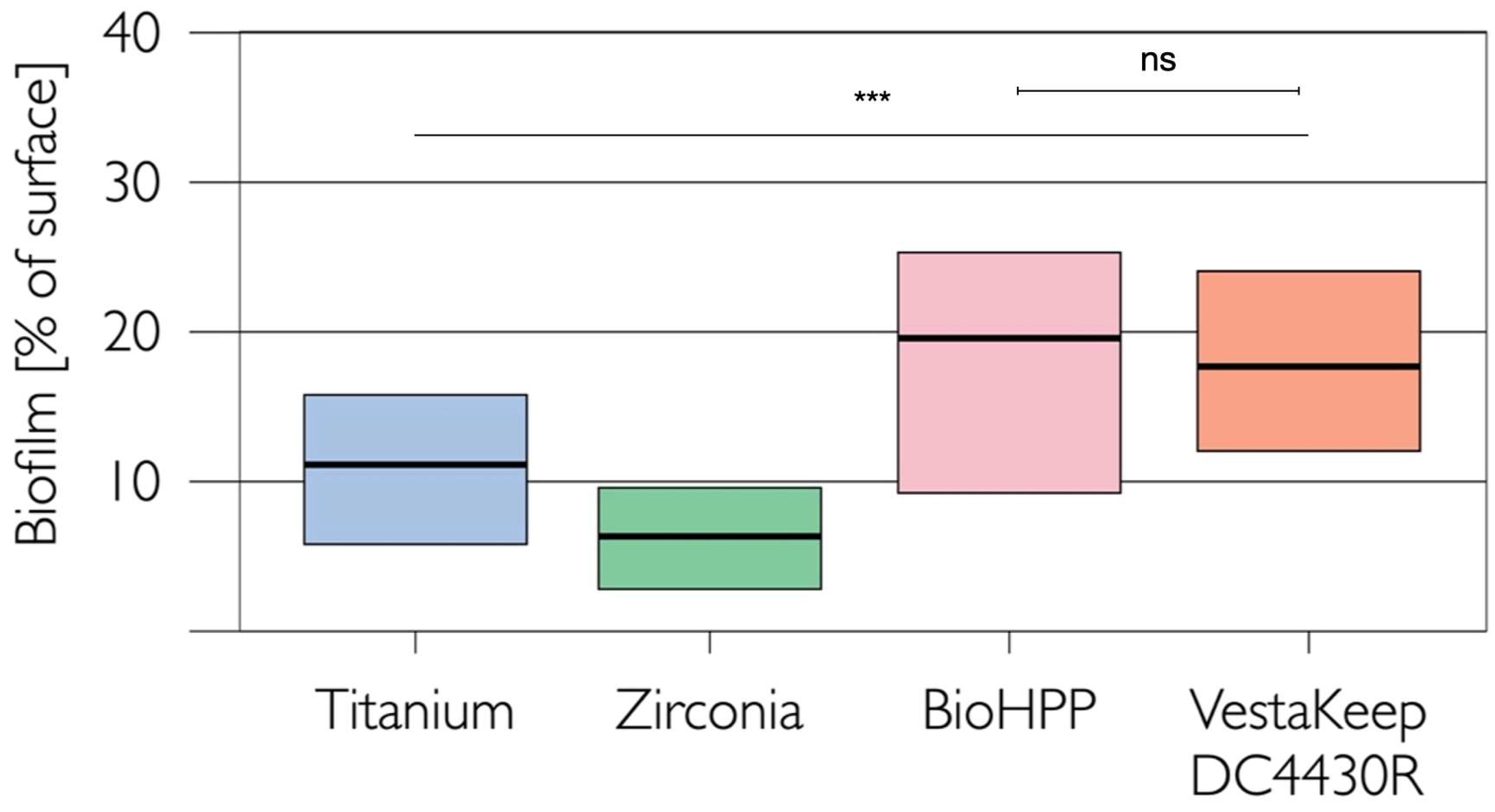
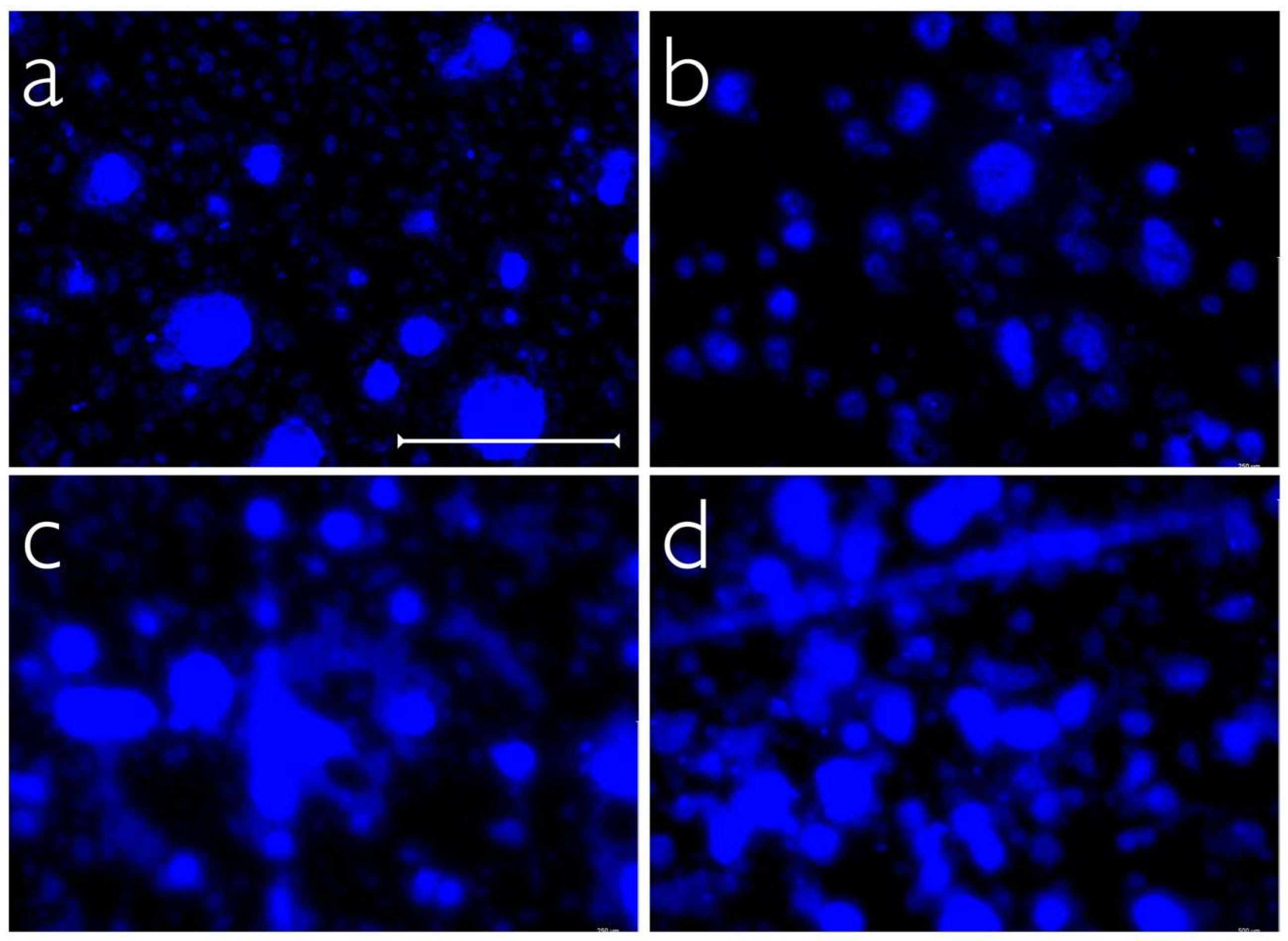
2.2. In Vivo Biofilm Formation
3. Discussion
4. Materials and Methods
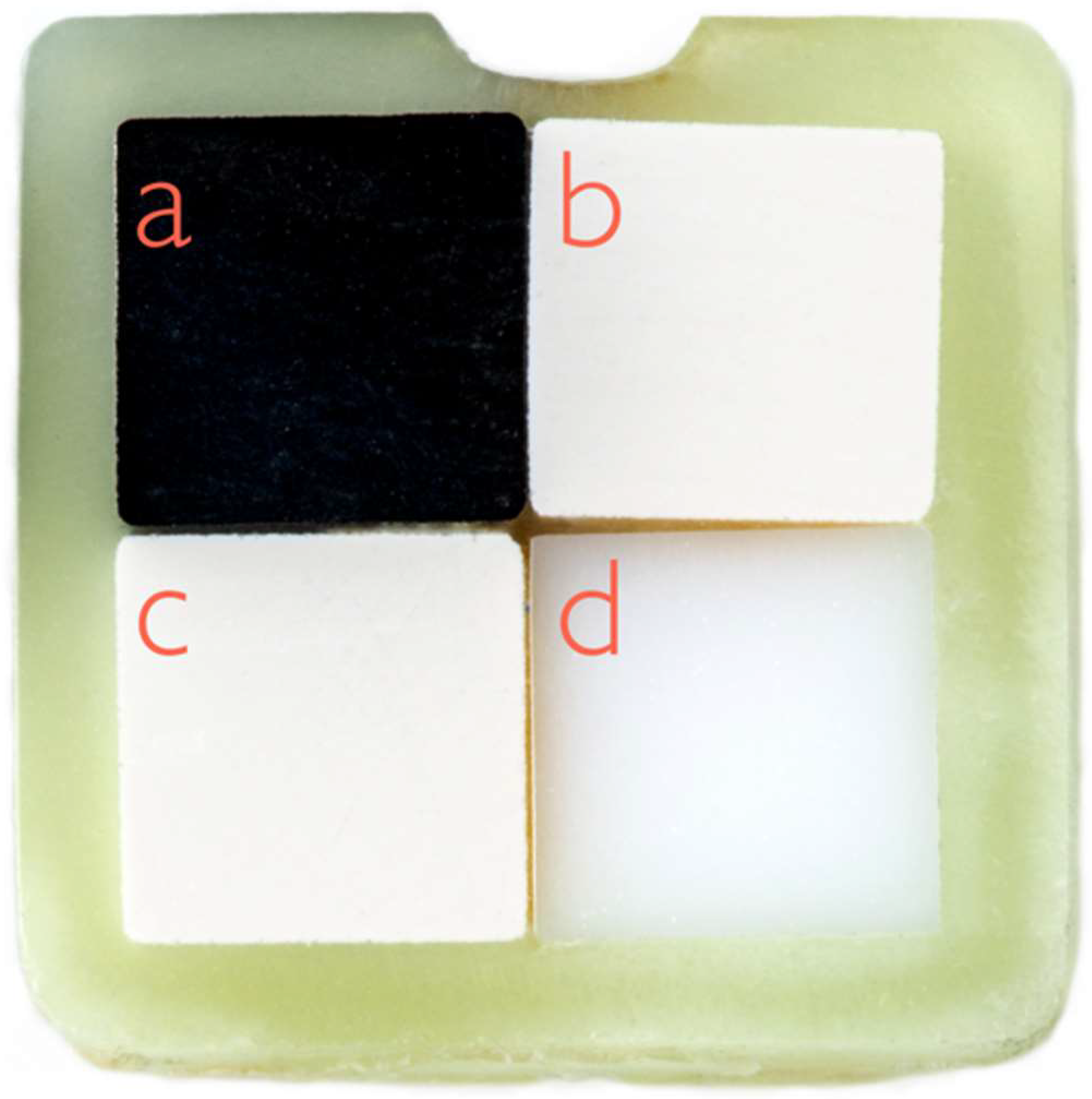
4.1. Preparation and Characterization of the Test Specimens
4.2. In Vivo Biofilm Formation
4.3. Visualization and Quantification of Adhering Biofilms
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Human Microbiome Project Consortium. Structure, Function and Diversity of the Healthy Human Microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.R.; Yu, W.-H.; Lakshmanan, A.; Wade, W.G. The Human Oral Microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samaranayake, L.; Bandara, N.; Pesee, S. Oral Biofilms: What Are They? In Oral Biofilms and Modern Dental Materials; Ionescu, A.C., Hahnel, S., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 1–7. ISBN 978-3-030-67387-1. [Google Scholar]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Scribante, A. Oral Microbiota in Patients with Peri-Implant Disease: A Narrative Review. Appl. Sci. 2022, 12, 3250. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-Implant Diseases and Conditions: Consensus Report of Workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Décaillet, F. The Characteristics of Biofilms in Peri-Implant Disease. J. Clin. Periodontol. 2011, 38, 203–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.; Wang, H.-L. Biofilm Related to Dental Implants. Implant Dent. 2010, 19, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dabdoub, S.M.; Tsigarida, A.A.; Kumar, P.S. Patient-Specific Analysis of Periodontal and Peri-Implant Microbiomes. J. Dent. Res. 2013, 92, 168S–175S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derks, J.; Tomasi, C. Peri-Implant Health and Disease. A Systematic Review of Current Epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S158–S171. [Google Scholar] [CrossRef]
- Lee, C.-T.; Huang, Y.-W.; Zhu, L.; Weltman, R. Prevalences of Peri-Implantitis and Peri-Implant Mucositis: Systematic Review and Meta-Analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Mombelli, A.; Oosten, M.A.C.; Schürch, E.; Lang, N.P. The Microbiota Associated with Successful or Failing Osseointegrated Titanium Implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Roos-Jansåker, A.-M.; Lindahl, C.; Renvert, H.; Renvert, S. Nine- to Fourteen-Year Follow-up of Implant Treatment. Part II: Presence of Peri-Implant Lesions. J. Clin. Periodontol. 2006, 33, 290–295. [Google Scholar] [CrossRef]
- Koldsland, O.C.; Scheie, A.A.; Aass, A.M. Prevalence of Peri-Implantitis Related to Severity of the Disease with Different Degrees of Bone Loss. J. Periodontol. 2010, 81, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-Implantitis—Onset and Pattern of Progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Hickok, N.J.; Shapiro, I.M.; Chen, A.F. The Impact of Incorporating Antimicrobials into Implant Surfaces. J. Dent. Res. 2018, 97, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-Implantitis. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S246–S266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramani, K.; Jung, R.E.; Molenberg, A.; Hammerle, C.H.F. Biofilm on Dental Implants: A Review of the Literature. Int. J. Oral Maxillofac. Implant. 2009, 24, 616–626. [Google Scholar]
- Belibasakis, G.N.; Charalampakis, G.; Bostanci, N.; Stadlinger, B. Peri-Implant Infections of Oral Biofilm Etiology. Adv. Exp. Med. Biol. 2015, 830, 69–84. [Google Scholar] [CrossRef]
- Shah, S.R.; Tatara, A.M.; D’Souza, R.N.; Mikos, A.G.; Kasper, F.K. Evolving Strategies for Preventing Biofilm on Implantable Materials. Mater. Today 2013, 16, 177–182. [Google Scholar] [CrossRef]
- Rimondini, L.; Cochis, A.; Varoni, E.; Azzimonti, B.; Carrassi, A. Biofilm Formation on Implants and Prosthetic Dental Materials. In Handbook of Bioceramics and Biocomposites; Antoniac, I.V., Ed.; Springer International Publishing: Cham, Switzerland, 2015; pp. 1–37. ISBN 978-3-319-09230-0. [Google Scholar]
- Heitz-Mayfield, L.J.A. Peri-Implant Diseases: Diagnosis and Risk Indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef]
- Papavasileiou, D.; Behr, M.; Gosau, M.; Gerlach, T.; Buergers, R. Peri-Implant Biofilm Formation on Luting Agents Used for Cementing Implant-Supported Fixed Restorations: A Preliminary in Vivo Study. Int. J. Prosthodont. 2015, 28, 371–373. [Google Scholar] [CrossRef] [Green Version]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary Prevention of Peri-Implantitis: Managing Peri-Implant Mucositis. J. Clin. Periodontol. 2015, 42 (Suppl. S16), S152–S157. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.C. Prevention and Treatment of Periodontal Diseases in Primary Care. Evid. Based Dent. 2014, 15, 68–69. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Eickholz, P.; Loos, B.G.; Papapanou, P.; van der Velden, U.; Armitage, G.; Bouchard, P.; Deinzer, R.; Dietrich, T.; Hughes, F.; et al. Principles in Prevention of Periodontal Diseases: Consensus Report of Group 1 of the 11th European Workshop on Periodontology on Effective Prevention of Periodontal and Peri-Implant Diseases. J. Clin. Periodontol. 2015, 42, S5–S11. [Google Scholar] [CrossRef]
- Ramburrun, P.; Pringle, N.A.; Dube, A.; Adam, R.Z.; D’Souza, S.; Aucamp, M. Recent Advances in the Development of Antimicrobial and Antifouling Biocompatible Materials for Dental Applications. Materials 2021, 14, 3167. [Google Scholar] [CrossRef]
- Tobias, R.S. Antibacterial Properties of Dental Restorative Materials: A Review. Int. Endod. J. 1988, 21, 155–160. [Google Scholar] [CrossRef]
- Brum, R.S.; Labes, L.G.; Volpato, C.Â.M.; Benfatti, C.A.M.; Pimenta, A.d.L. Strategies to Reduce Biofilm Formation in PEEK Materials Applied to Implant Dentistry-A Comprehensive Review. Antibiotics 2020, 9, 609. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Jepsen, S.; Stadlinger, B.; Terheyden, H. Peri-Implantitis and Its Prevention. Clin. Oral Implant. Res. 2019, 30, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Hisbergues, M.; Vendeville, S.; Vendeville, P. Zirconia: Established Facts and Perspectives for a Biomaterial in Dental Implantology. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 88, 519–529. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial Adhesion on Commercially Pure Titanium and Zirconium Oxide Disks: An in Vivo Human Study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef]
- Yin, L.; Nakanishi, Y.; Alao, A.-R.; Song, X.-F.; Abduo, J.; Zhang, Y. A Review of Engineered Zirconia Surfaces in Biomedical Applications. Procedia CIRP 2017, 65, 284–290. [Google Scholar] [CrossRef]
- Della Bona, A.; Pecho, O.E.; Alessandretti, R. Zirconia as a Dental Biomaterial. Materials 2015, 8, 4978–4991. [Google Scholar] [CrossRef]
- Depprich, R.; Zipprich, H.; Ommerborn, M.; Mahn, E.; Lammers, L.; Handschel, J.; Naujoks, C.; Wiesmann, H.-P.; Kübler, N.R.; Meyer, U. Osseointegration of Zirconia Implants: An SEM Observation of the Bone-Implant Interface. Head Face Med. 2008, 4, 25–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buser, D.; Sennerby, L.; de Bruyn, H. Modern Implant Dentistry Based on Osseointegration: 50 Years of Progress, Current Trends and Open Questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Roehling, S.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Braissant, O.; Woelfler, H.; Waltimo, T.; Kniha, H.; Gahlert, M. In Vitro Biofilm Formation on Titanium and Zirconia Implant Surfaces. J. Periodontol. 2017, 88, 298–307. [Google Scholar] [CrossRef]
- De Avila, E.D.; Avila-Campos, M.J.; Vergani, C.E.; Spolidório, D.M.P.; Mollo, F.d.A. Structural and Quantitative Analysis of a Mature Anaerobic Biofilm on Different Implant Abutment Surfaces. J. Prosthet. Dent. 2016, 115, 428–436. [Google Scholar] [CrossRef]
- Pellegrini, G.; Francetti, L.; Barbaro, B.; Del Fabbro, M. Novel Surfaces and Osseointegration in Implant Dentistry. J. Investig. Clin. Dent. 2018, 9, e12349. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, F.H.; Galárraga-Vinueza, M.E.; Magini, R.; Fredel, M.; Silva, F.; Souza, J.C.M.; Zhang, Y.; Henriques, B. Zirconia Surface Modifications for Implant Dentistry. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 98, 1294–1305. [Google Scholar] [CrossRef]
- Grischke, J.; Eberhard, J.; Stiesch, M. Antimicrobial Dental Implant Functionalization Strategies—A Systematic Review. Dent. Mater. J. 2016, 35, 545–558. [Google Scholar] [CrossRef] [Green Version]
- Panayotov, I.V.; Orti, V.; Cuisinier, F.; Yachouh, J. Polyetheretherketone (PEEK) for Medical Applications. J. Mater. Sci. Mater. Med. 2016, 27, 118. [Google Scholar] [CrossRef]
- Bathala, L.; Majeti, V.; Rachuri, N.; Singh, N.; Gedela, S. The Role of Polyether Ether Ketone (Peek) in Dentistry—A Review. J. Med. Life 2019, 12, 5–9. [Google Scholar] [CrossRef]
- Alexakou, E.; Damanaki, M.; Zoidis, P.; Bakiri, E.; Mouzis, N.; Smidt, G.; Kourtis, S. PEEK High Performance Polymers: A Review of Properties and Clinical Applications in Prosthodontics and Restorative Dentistry. Eur. J. Prosthodont. Restor. Dent. 2019, 27, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of Polyetheretherketone (PEEK) in Oral Implantology and Prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Zoidis, P.; Papathanasiou, I.; Polyzois, G. The Use of a Modified Poly-Ether-Ether-Ketone (PEEK) as an Alternative Framework Material for Removable Dental Prostheses. A Clinical Report. J. Prosthodont. 2016, 25, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Chowdhary, R. PEEK Materials as an Alternative to Titanium in Dental Implants: A Systematic Review. Clin. Implant Dent. Relat. Res. 2019, 21, 208–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahnel, S.; Wieser, A.; Lang, R.; Rosentritt, M. Biofilm Formation on the Surface of Modern Implant Abutment Materials. Clin. Oral Implant. Res. 2015, 26, 1297–1301. [Google Scholar] [CrossRef]
- Barkarmo, S.; Longhorn, D.; Leer, K.; Johansson, C.B.; Stenport, V.; Franco-Tabares, S.; Kuehne, S.A.; Sammons, R. Biofilm Formation on Polyetheretherketone and Titanium Surfaces. Clin. Exp. Dent. Res. 2019, 5, 427–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sissons, C.H. Artificial Dental Plaque Biofilm Model Systems. Adv. Dent. Res. 1997, 11, 110–126. [Google Scholar] [CrossRef]
- Schmalz, G. Determination of Biocompatibility. In Biocompatibility of Dental Materials; Schmalz, G., Arenholt-Bindslev, D., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2009; pp. 13–43. ISBN 978-3-540-77782-3. [Google Scholar]
- Olson, H.; Betton, G.; Robinson, D.; Thomas, K.; Monro, A.; Kolaja, G.; Lilly, P.; Sanders, J.; Sipes, G.; Bracken, W.; et al. Concordance of the Toxicity of Pharmaceuticals in Humans and in Animals. Regul. Toxicol. Pharmacol. 2000, 32, 56–67. [Google Scholar] [CrossRef]
- Anderson, J.M. Future Challenges in the in Vitro and in Vivo Evaluation of Biomaterial Biocompatibility. Regen. Biomater. 2016, 3, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Quirynen, M.; Marechal, M.; Busscher, H.J.; Weerkamp, A.H.; Darius, P.L.; van Steenberghe, D. The Influence of Surface Free Energy and Surface Roughness on Early Plaque Formation: An in Vivo Study in Man. J. Clin. Periodontol. 1990, 17, 138–144. [Google Scholar] [CrossRef]
- Bollen, C.M.; Papaioanno, W.; van Eldere, J.; Schepers, E.; Quirynen, M.; van Steenberghe, D. The Influence of Abutment Surface Roughness on Plaque Accumulation and Peri-Implant Mucositis. Clin. Oral Implant. Res. 1996, 7, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Kern, M.; Lehmann, F. Influence of Surface Conditioning on Bonding to Polyetheretherketon (PEEK). Dent. Mater. 2012, 28, 1280–1283. [Google Scholar] [CrossRef]
- Fuhrmann, G.; Steiner, M.; Freitag-Wolf, S.; Kern, M. Resin Bonding to Three Types of Polyaryletherketones (PAEKs)-Durability and Influence of Surface Conditioning. Dent. Mater. 2014, 30, 357–363. [Google Scholar] [CrossRef]
- Porojan, L.; Toma, F.R.; Vasiliu, R.D.; Topală, F.-I.; Porojan, S.D.; Matichescu, A. Optical Properties and Color Stability of Dental PEEK Related to Artificial Ageing and Staining. Polymers 2021, 13, 4102. [Google Scholar] [CrossRef] [PubMed]
- Zeller, B.; Stöckli, S.; Zaugg, L.K.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Waltimo, T.; Zitzmann, N.U. Biofilm Formation on Metal Alloys, Zirconia and Polyetherketoneketone as Implant Materials in Vivo. Clin. Oral Implant. Res. 2020, 31, 1078–1086. [Google Scholar] [CrossRef] [PubMed]
- Rimondini, L.; Cerroni, L.; Carrassi, A.; Torricelli, P. Bacterial Colonization of Zirconia Ceramic Surfaces: An in Vitro and in Vivo Study. Int. J. Oral Maxillofac. Implant. 2002, 17, 793–798. [Google Scholar]
- Al-Ahmad, A.; Wiedmann-Al-Ahmad, M.; Faust, J.; Bächle, M.; Follo, M.; Wolkewitz, M.; Hannig, C.; Hellwig, E.; Carvalho, C.; Kohal, R. Biofilm Formation and Composition on Different Implant Materials in Vivo. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 95, 101–109. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Karygianni, L.; Schulze Wartenhorst, M.; Bächle, M.; Hellwig, E.; Follo, M.; Vach, K.; Han, J.-S. Bacterial Adhesion and Biofilm Formation on Yttria-Stabilized, Tetragonal Zirconia and Titanium Oral Implant Materials with Low Surface Roughness—An in Situ Study. J. Med. Microbiol. 2016, 65, 596–604. [Google Scholar] [CrossRef] [Green Version]
- Desch, A.; Freifrau von Maltzahn, N.; Stumpp, N.; Dalton, M.; Yang, I.; Stiesch, M. Biofilm Formation on Zirconia and Titanium over Time—An in Vivo Model Study. Clin. Oral Implant. Res. 2020, 31, 865–880. [Google Scholar] [CrossRef]
- Sreenivasan, P.K.; DeVizio, W.; Prasad, K.V.V.; Patil, S.; Chhabra, K.G.; Rajesh, G.; Javali, S.B.; Kulkarni, R.D. Regional Differences within the Dentition for Plaque, Gingivitis, and Anaerobic Bacteria. J. Clin. Dent. 2010, 21, 13–19. [Google Scholar]
- Sreenivasan, P.K.; Prasad, K.V.V. Distribution of Dental Plaque and Gingivitis within the Dental Arches. J. Int. Med. Res. 2017, 45, 1585–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haffajee, A.D.; Teles, R.P.; Patel, M.R.; Song, X.; Yaskell, T.; Socransky, S.S. Factors Affecting Human Supragingival Biofilm Composition. II. Tooth Position. J. Periodontal Res. 2009, 44, 520–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palk, L.; Sneyd, J.; Shuttleworth, T.J.; Yule, D.I.; Crampin, E.J. A Dynamic Model of Saliva Secretion. J. Theor. Biol. 2010, 266, 625–640. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administration in Peri-Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Cuggia, G.; Scribante, A. Domiciliary Use of Chlorhexidine vs. Postbiotic Gels in Patients with Peri-Implant Mucositis: A Split-Mouth Randomized Clinical. Trial. Appl. Sci. 2022, 12, 2800. [Google Scholar] [CrossRef]
- Jennes, M.-E.; Naumann, M.; Peroz, S.; Beuer, F.; Schmidt, F. Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review. Antibiotics 2021, 10, 1350. [Google Scholar] [CrossRef]
- Wassmann, T.; Schubert, A.; Malinski, F.; Rosentritt, M.; Krohn, S.; Techmer, K.; Bürgers, R. The Antimicrobial and Cytotoxic Effects of a Copper-Loaded Zinc Oxide Phosphate Cement. Clin. Oral Investig. 2020, 24, 3899–3909. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surface Roughness [μm] | ||
|---|---|---|
| Material | Ra | Sa |
| PEEK-BioHPP | 0.099 (0.086/0.114) | 0.133 (0.114/0.152) |
| PEEK-VestaKeep DC4430R | 0.100 (0.085/0.121) | 0.130 (0.108/0.168) |
| Titanium | 0.114 (0.087/0.128) | 0.130 (0.111/0.150) |
| Zirconia | 0.100 (0.090/0.112) | 0.117 (0.103/0.130) |
| Intraoral Position | Gender | |||
|---|---|---|---|---|
| Canine | First Molar | Female | Male | |
| Titanium | 5.3 (1.5/12.8) a | 11.6 (6.3/24.3) a | 15.1 (10.6/20.6) | 7.7 (5.4/13.2) |
| Zirconia | 1.9 (1.1/5.6) b | 5.4 (3.5/18.0) b | 8.6 (3.2/15.1) | 3.6 (3.0/8.4) |
| PEEK-BioHPP | 14.2 (3.8/19.4) c | 19.6 (9.0/44.9) c | 21.5 (14.9/34.9) | 17.7 (9.3/23.4) |
| PEEK-VestaKeep DC4430R | 8.7 (4.2/19.3) d | 22.5 (10.7/38.8) d | 21.2 (17.0/25.3) | 15.5 (11.4/21.5) |
| Class of Material | No. | Test Material | Manufacturer |
|---|---|---|---|
| Titanium (grade 2) | 1 | Zenotec Ti pur | Wieland Dental + Technik GmbH & Co. KG, Pforzheim, Germany |
| Zirconia (zirconium dioxide) | 2 | Cercon base | Dentsply Sirona, Charlotte, NC, USA |
| PEEK (polyetheretherketone) | 3 | BioHPP | Bredent GmbH & Co. KG, Senden, Germany |
| 4 | VestaKeep DC4430R | Evonik Industries AG, Essen, Germany |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiessner, A.; Wassmann, T.; Wiessner, J.M.; Schubert, A.; Wiechens, B.; Hampe, T.; Bürgers, R. In Vivo Biofilm Formation on Novel PEEK, Titanium, and Zirconia Implant Abutment Materials. Int. J. Mol. Sci. 2023, 24, 1779. https://doi.org/10.3390/ijms24021779
Wiessner A, Wassmann T, Wiessner JM, Schubert A, Wiechens B, Hampe T, Bürgers R. In Vivo Biofilm Formation on Novel PEEK, Titanium, and Zirconia Implant Abutment Materials. International Journal of Molecular Sciences. 2023; 24(2):1779. https://doi.org/10.3390/ijms24021779
Chicago/Turabian StyleWiessner, Andreas, Torsten Wassmann, Johanna Maria Wiessner, Andrea Schubert, Bernhard Wiechens, Tristan Hampe, and Ralf Bürgers. 2023. "In Vivo Biofilm Formation on Novel PEEK, Titanium, and Zirconia Implant Abutment Materials" International Journal of Molecular Sciences 24, no. 2: 1779. https://doi.org/10.3390/ijms24021779
APA StyleWiessner, A., Wassmann, T., Wiessner, J. M., Schubert, A., Wiechens, B., Hampe, T., & Bürgers, R. (2023). In Vivo Biofilm Formation on Novel PEEK, Titanium, and Zirconia Implant Abutment Materials. International Journal of Molecular Sciences, 24(2), 1779. https://doi.org/10.3390/ijms24021779