
Protein Plasma Levels of the IGF Signalling System Are Altered in Major Depressive Disorder

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. General Data and Subjective Scales
2.2. Correlation between Plasma IGFs Proteins and Metabolic Parameters
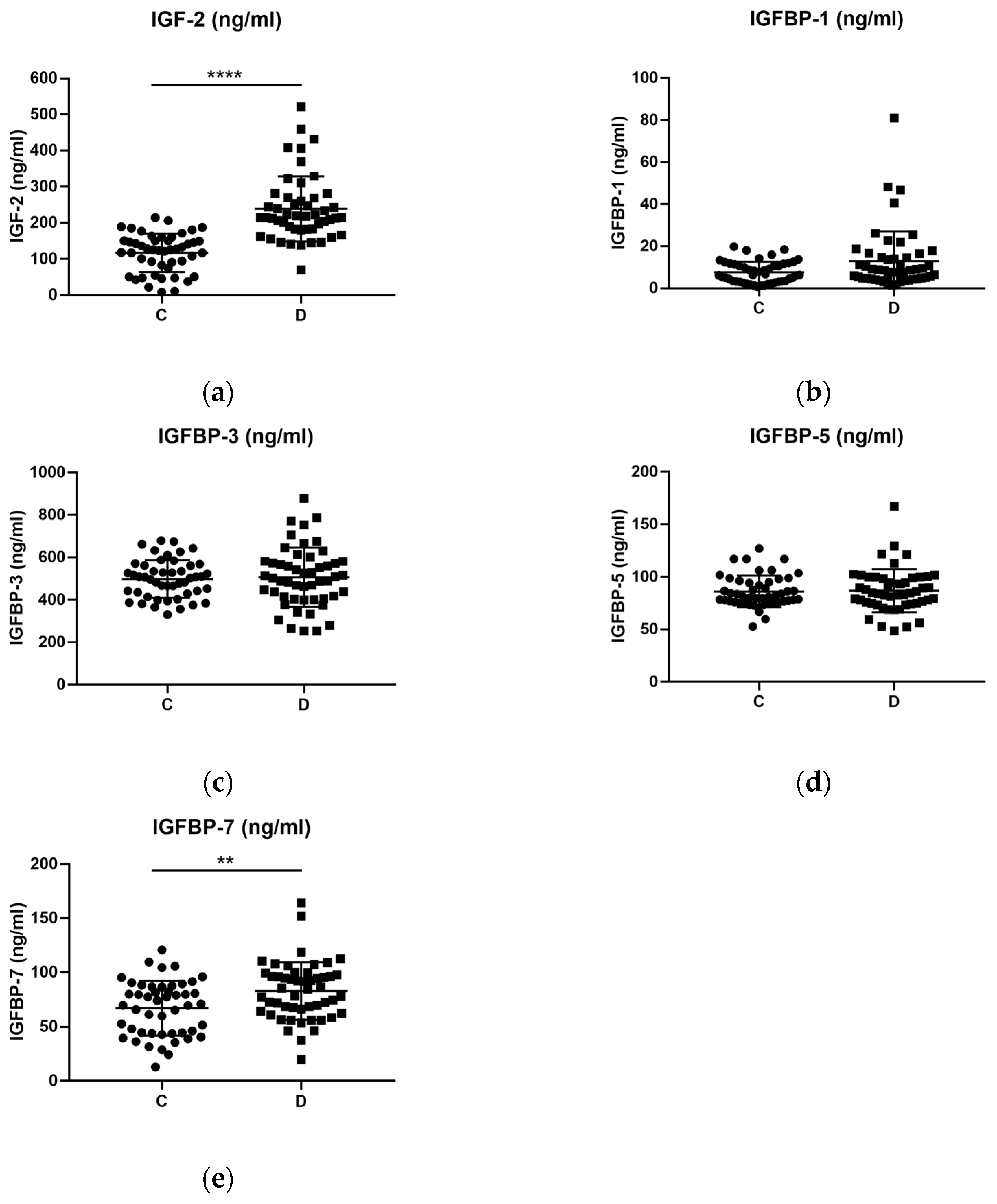
2.3. Levels of IGF Proteins in Depressed Patients and Healthy Controls
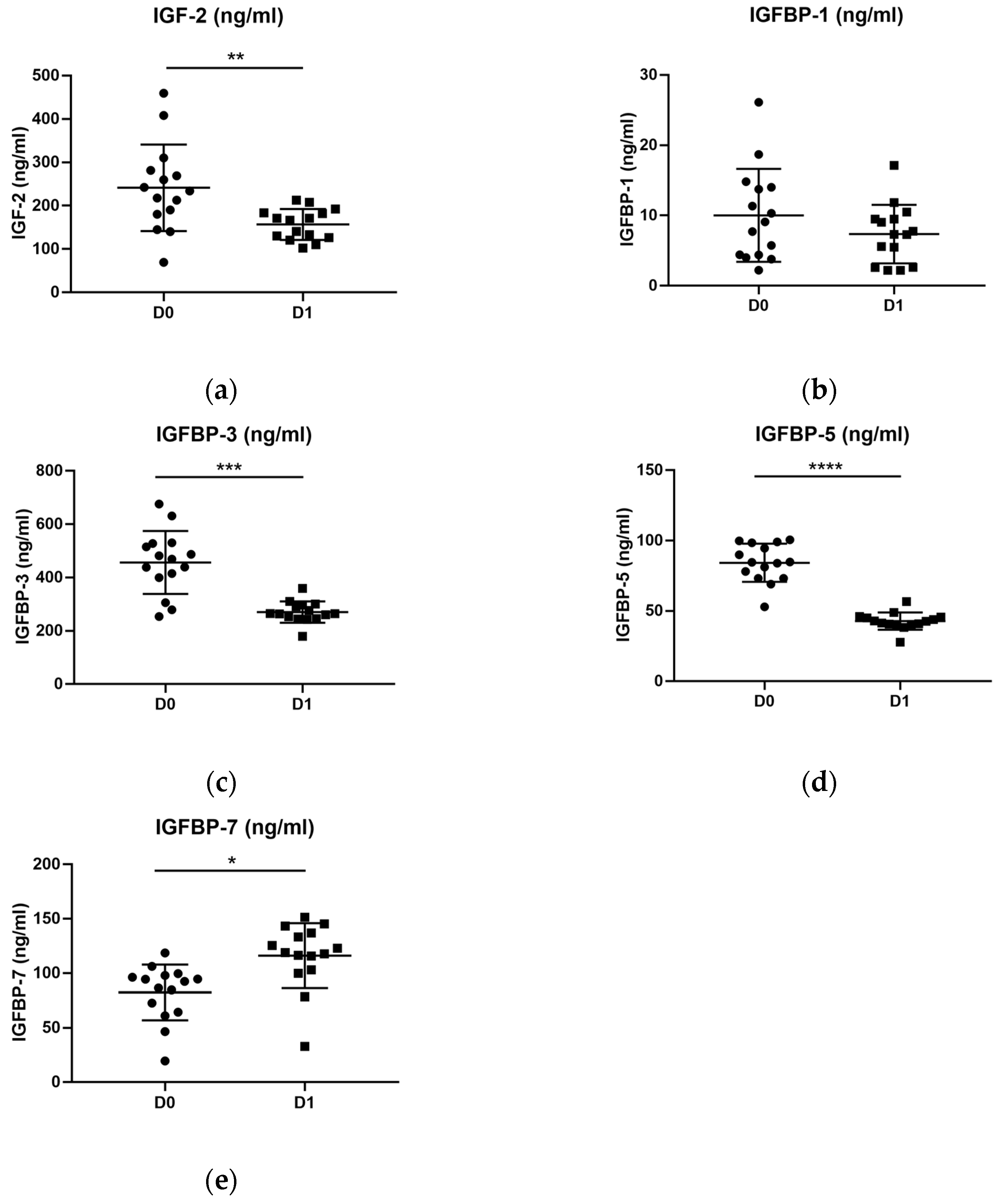
2.4. The Levels of IGF Proteins in Depressed Patients before and after Treatment
2.5. Correlation between Plasma IGFs Proteins and Subjective Scales
3. Discussion
Limitations and Future Perspectives
4. Materials and Methods
4.1. Experimental Design
4.2. Blood Collection and Plasma Obtention
4.3. Subjective Scales
4.4. Metabolic Parameters
4.5. Plasma Protein Measurement
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cui, R. Editorial: A Systematic Review of Depression. Curr. Neuropharmacol. 2015, 13, 480. [Google Scholar] [CrossRef] [PubMed]
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 4 March 2023).
- Renaud-Charest, O.; Lui, L.M.W.; Eskander, S.; Ceban, F.; Ho, R.; Di Vincenzo, J.D.; Rosenblat, J.D.; Lee, Y.; Subramaniapillai, M.; McIntyre, R.S. Onset and frequency of depression in post-COVID-19 syndrome: A systematic review. J. Psychiatr. Res. 2021, 144, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 2003, 53, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Gadad, B.S.; Jha, M.K.; Czysz, A.; Furman, J.L.; Mayes, T.L.; Emslie, M.P.; Trivedi, M.H. Peripheral biomarkers of major depression and antidepressant treatment response: Current knowledge and future outlooks. J. Affect. Disord. 2018, 233, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Forbes, B.E.; Blyth, A.J.; Wit, J.M. Disorders of IGFs and IGF-1R signaling pathways. Mol. Cell Endocrinol. 2020, 518, 111035. [Google Scholar] [CrossRef]
- Versteyhe, S.; Klaproth, B.; Borup, R.; Palsgaard, J.; Jensen, M.; Gray, S.G.; De Meyts, P. IGF-I, IGF-II, and Insulin Stimulate Dierent Gene Expression Responses through Binding to the IGF-I Receptor. Front. Endocrinol. 2013, 4, 98. [Google Scholar] [CrossRef]
- Blyth, A.J.; Kirk, N.S.; Forbes, B.E. Understanding IGF-II Action through Insights into Receptor Binding and Activation. Cells 2020, 9, 2276. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J. Insulin-Like Growth Factor Pathway and the Thyroid. Front. Endocrinol. 2021, 12, 653627. [Google Scholar] [CrossRef] [PubMed]
- Beletskiy, A.; Chesnokova, E.; Bal, N. Insulin-Like Growth Factor 2 as a Possible Neuroprotective Agent and Memory Enhancer-Its Comparative Expression, Processing and Signaling in Mammalian CNS. Int. J. Mol. Sci. 2021, 22, 1849. [Google Scholar] [CrossRef] [PubMed]
- Kelley, K.M.; Oh, Y.; Gargosky, S.E.; Gucev, Z.; Matsumoto, T.; Hwa, V.; Ng, L.; Simpson, D.M.; Rosenfeld, R.G. Insulin-like growth factor-binding proteins (IGFBPs) and their regulatory dynamics. Int. J. Biochem. Cell Biol. 1996, 28, 619–637. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Zhou, X.X.; Hu, Y.; Li, G.; Wang, Y. The Roles of Insulin-Like Growth Factor Binding Protein Family in Development and Diseases. Adv. Ther. 2021, 38, 885–903. [Google Scholar] [CrossRef] [PubMed]
- Bach, L.A. IGF-binding proteins. J. Mol. Endocrinol. 2018, 61, T11–T28. [Google Scholar] [CrossRef] [PubMed]
- Rotwein, P.; Burgess, S.K.; Milbrandt, J.D.; Krause, J.E. Differential expression of insulin-like growth factor genes in rat central nervous system. Proc. Natl. Acad. Sci. USA 1988, 85, 265–269. [Google Scholar] [CrossRef] [PubMed]
- O’Kusky, J.; Ye, P. Neurodevelopmental effects of insulin-like growth factor signaling. Front. Neuroendocrinol. 2012, 33, 230–251. [Google Scholar] [CrossRef]
- Jung, S.; Lee, Y.; Kim, G.; Son, H.; Lee, D.H.; Roh, G.S.; Kang, S.S.; Cho, G.J.; Choi, W.S.; Kim, H.J. Decreased expression of extracellular matrix proteins and trophic factors in the amygdala complex of depressed mice after chronic immobilization stress. BMC Neurosci. 2012, 13, 58. [Google Scholar] [CrossRef]
- Duan, D.; Yang, X.; Ya, T.; Chen, L. Hippocampal gene expression in a rat model of depression after electroacupuncture at the Baihui and Yintang acupoints. Neural Regen. Res. 2014, 9, 76–83. [Google Scholar] [CrossRef]
- Cline, B.H.; Steinbusch, H.W.; Malin, D.; Revishchin, A.V.; Pavlova, G.V.; Cespuglio, R.; Strekalova, T. The neuronal insulin sensitizer dicholine succinate reduces stress-induced depressive traits and memory deficit: Possible role of insulin-like growth factor 2. BMC Neurosci. 2012, 13, 110. [Google Scholar] [CrossRef]
- Luo, Y.W.; Xu, Y.; Cao, W.Y.; Zhong, X.L.; Duan, J.; Wang, X.Q.; Hu, Z.L.; Li, F.; Zhang, J.Y.; Zhou, M.; et al. Insulin-like growth factor 2 mitigates depressive behavior in a rat model of chronic stress. Neuropharmacology 2015, 89, 318–324. [Google Scholar] [CrossRef]
- Guo, D.; Xu, Y.; Liu, Z.; Wang, Y.; Xu, X.; Li, C.; Li, S.; Zhang, J.; Xiong, T.; Cao, W.; et al. IGF2 inhibits hippocampal over-activated microglia and alleviates depression-like behavior in LPS- treated male mice. Brain Res. Bull. 2023, 194, 1–12. [Google Scholar] [CrossRef]
- Chen, D.Y.; Stern, S.A.; Garcia-Osta, A.; Saunier-Rebori, B.; Pollonini, G.; Bambah-Mukku, D.; Blitzer, R.D.; Alberini, C.M. A critical role for IGF-II in memory consolidation and enhancement. Nature 2011, 469, 491–497. [Google Scholar] [CrossRef]
- Córdova-Palomera, A.; Fatjó-Vilas, M.; Gastó, C.; Navarro, V.; Krebs, M.O.; Fañanás, L. Genome-wide methylation study on depression: Differential methylation and variable methylation in monozygotic twins. Transl. Psychiatry 2015, 5, e557. [Google Scholar] [CrossRef] [PubMed]
- Mansell, T.; Novakovic, B.; Meyer, B.; Rzehak, P.; Vuillermin, P.; Ponsonby, A.L.; Collier, F.; Burgner, D.; Saffery, R.; Ryan, J.; et al. The effects of maternal anxiety during pregnancy on IGF2/H19 methylation in cord blood. Transl. Psychiatry 2016, 6, e765. [Google Scholar] [CrossRef] [PubMed]
- Vangeel, E.B.; Izzi, B.; Hompes, T.; Vansteelandt, K.; Lambrechts, D.; Freson, K.; Claes, S. DNA methylation in imprinted genes IGF2 and GNASXL is associated with prenatal maternal stress. Genes. Brain Behav. 2015, 14, 573–582. [Google Scholar] [CrossRef]
- Liu, Y.; Murphy, S.K.; Murtha, A.P.; Fuemmeler, B.F.; Schildkraut, J.; Huang, Z.; Overcash, F.; Kurtzberg, J.; Jirtle, R.; Iversen, E.S.; et al. Depression in pregnancy, infant birth weight and DNA methylation of imprint regulatory elements. Epigenetics 2012, 7, 735–746. [Google Scholar] [CrossRef] [PubMed]
- St-Pierre, J.; Hivert, M.F.; Perron, P.; Poirier, P.; Guay, S.P.; Brisson, D.; Bouchard, L. IGF2 DNA methylation is a modulator of newborn’s fetal growth and development. Epigenetics 2012, 7, 1125–1132. [Google Scholar] [CrossRef]
- Van Lieshout, R.J.; Boyle, M.H.; Favotto, L.; Krzeczkowski, J.E.; Savoy, C.; Saigal, S.; Schmidt, L.A. Impact of extremely low-birth-weight status on risk and resilience for depression and anxiety in adulthood. J. Child. Psychol. Psychiatry 2018, 59, 596–603. [Google Scholar] [CrossRef]
- Levine, S.Z. Low birth-weight and risk for major depression: A community-based longitudinal study. Psychiatry Res. 2014, 215, 618–623. [Google Scholar] [CrossRef]
- Akanji, A.O.; Ohaeri, J.U.; Al-Shammri, S.A.; Fatania, H.R. Associations of blood levels of insulin-like growth factor (IGF)-I, IGF-II and IGF binding protein (IGFBP)-3 in schizophrenic Arab subjects. Clin. Chem. Lab. Med. 2007, 45, 1229–1231. [Google Scholar] [CrossRef]
- Yang, Y.J.; Luo, T.; Zhao, Y.; Jiang, S.Z.; Xiong, J.W.; Zhan, J.Q.; Yu, B.; Yan, K.; Wei, B. Altered insulin-like growth factor-2 signaling is associated with psychopathology and cognitive deficits in patients with schizophrenia. PLoS ONE 2020, 15, e0226688. [Google Scholar] [CrossRef]
- Chao, X.L.; Jiang, S.Z.; Xiong, J.W.; Zhan, J.Q.; Wei, B.; Chen, C.N.; Yang, Y.J. Changes of Serum Insulin-like Growth Factor-2 Response to Negative Symptom Improvements in Schizophrenia Patients Treated with Atypical Antipsychotics. Curr. Med. Sci. 2020, 40, 563–569, Erratum in Curr. Med. Sci. 2020, 40, 997. [Google Scholar] [CrossRef]
- Fernández-Pereira, C.; Penedo, M.A.; Rivera-Baltanas, T.; Fernández-Martínez, R.; Ortolano, S.; Olivares, J.M.; Agís-Balboa, R.C. Insulin-like Growth Factor 2 (IGF-2) and Insulin-like Growth Factor Binding Protein 7 (IGFBP-7) Are Upregulated after Atypical Antipsychotics in Spanish Schizophrenia Patients. Int. J. Mol. Sci. 2022, 23, 9591. [Google Scholar] [CrossRef] [PubMed]
- Åberg, D.; Johansson, P.; Isgaard, J.; Wallin, A.; Johansson, J.O.; Andreasson, U.; Blennow, K.; Zetterberg, H.; Åberg, N.D.; Svensson, J. Increased Cerebrospinal Fluid Level of Insulin-like Growth Factor-II in Male Patients with Alzheimer’s Disease. J. Alzheimers Dis. 2015, 48, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Tham, A.; Nordberg, A.; Grissom, F.E.; Carlsson-Skwirut, C.; Viitanen, M.; Sara, V.R. Insulin-like growth factors and insulin-like growth factor binding proteins in cerebrospinal fluid and serum of patients with dementia of the Alzheimer type. J. Neural Transm. Park. Dis. Dement. Sect. 1993, 5, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Hertze, J.; Nägga, K.; Minthon, L.; Hansson, O. Changes in cerebrospinal fluid and blood plasma levels of IGF-II and its binding proteins in Alzheimer’s disease: An observational study. BMC Neurol. 2014, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- García-Huerta, P.; Troncoso-Escudero, P.; Wu, D.; Thiruvalluvan, A.; Cisternas-Olmedo, M.; Henríquez, D.R.; Plate, L.; Chana-Cuevas, P.; Saquel, C.; Thielen, P.; et al. Insulin-like growth factor 2 (IGF2) protects against Huntington’s disease through the extracellular disposal of protein aggregates. Acta Neuropathol. 2020, 140, 737–764. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda, D.; Grunenwald, F.; Vidal, A.; Troncoso-Escudero, P.; Cisternas-Olmedo, M.; Villagra, R.; Vergara, P.; Aguilera, C.; Nassif, M.; Vidal, R.L. Insulin-like growth factor 2 and autophagy gene expression alteration arise as potential biomarkers in Parkinson’s disease. Sci. Rep. 2022, 12, 2038. [Google Scholar] [CrossRef]
- Deuschle, M.; Blum, W.F.; Strasburger, C.J.; Schweiger, U.; Weber, B.; Körner, A.; Standhardt, H.; Gotthardt, U.; Schmider, J.; Pflaum, C.D.; et al. Insulin-like growth factor-I (IGF-I) plasma concentrations are increased in depressed patients. Psychoneuroendocrinology 1997, 22, 493–503. [Google Scholar] [CrossRef]
- Lesch, K.P.; Rupprecht, R.; Müller, U.; Pfüller, H. Comparison of GH responses after human GHRH-44 amide administration and TRH-induced TSH release in depressed patients. Biol. Psychiatry 1989, 25, 235–238. [Google Scholar] [CrossRef]
- Kopczak, A.; Stalla, G.K.; Uhr, M.; Lucae, S.; Hennings, J.; Ising, M.; Holsboer, F.; Kloiber, S. IGF-I in major depression and antidepressant treatment response. Eur. Neuropsychopharmacol. 2015, 25, 864–872. [Google Scholar] [CrossRef]
- Bot, M.; Milaneschi, Y.; Penninx, B.W.; Drent, M.L. Plasma insulin-like growth factor I levels are higher in depressive and anxiety disorders, but lower in antidepressant medication users. Psychoneuroendocrinology 2016, 68, 148–155. [Google Scholar] [CrossRef]
- Weber-Hamann, B.; Blum, W.F.; Kratzsch, J.; Gilles, M.; Heuser, I.; Deuschle, M. Insulin-like growth factor-I (IGF-I) serum concentrations in depressed patients: Relationship to saliva cortisol and changes during antidepressant treatment. Pharmacopsychiatry 2009, 42, 23–28. [Google Scholar] [CrossRef]
- Levada, O.A.; Troyan, A.S.; Pinchuk, I.Y. Serum insulin-like growth factor-1 as a potential marker for MDD diagnosis, its clinical characteristics, and treatment efficacy validation: Data from an open-label vortioxetine study. BMC Psychiatry 2020, 20, 208. [Google Scholar] [CrossRef]
- Franz, B.; Buysse, D.J.; Cherry, C.R.; Gray, N.S.; Grochocinski, V.J.; Frank, E.; Kupfer, D.J. Insulin-like growth factor 1 and growth hormone binding protein in depression: A preliminary communication. J. Psychiatr. Res. 1999, 33, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Li, S.X.; Liu, L.J.; Xu, L.Z.; Gao, L.; Wang, X.F.; Zhang, J.T.; Lu, L. Diurnal alterations in circadian genes and peptides in major depressive disorder before and after escitalopram treatment. Psychoneuroendocrinology 2013, 38, 2789–2799. [Google Scholar] [CrossRef] [PubMed]
- Rosso, G.; Zanardini, R.; Chiodelli, D.F.; Ferrari, C.; Gennarelli, M.; Bocchio-Chiavetto, L. Serum Levels of Insulin-Like Growth Factor-1 and Obsessive-Compulsive Disorder: A Case-Control Study. Neuropsychobiology 2016, 74, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Michelson, D.; Stratakis, C.; Hill, L.; Reynolds, J.; Galliven, E.; Chrousos, G.; Gold, P. Bone mineral density in women with depression. N. Engl. J. Med. 1996, 335, 1176–1181. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, R.; Rupprecht, C.; Rupprecht, M.; Noder, M.; Lesch, K.P.; Mössner, J. Effects of glucocorticoids on the regulation of the hypothalamic-pituitary-somatotropic system in depression. J. Affect. Disord. 1989, 17, 9–16. [Google Scholar] [CrossRef]
- Arinami, H.; Watanabe, Y.; Suzuki, Y.; Tajiri, M.; Tsuneyama, N.; Someya, T. Serum cortisol and insulin-like growth factor 1 levels in major depressive disorder and schizophrenia. Sci. Rep. 2023, 13, 1148. [Google Scholar] [CrossRef]
- Demirel, A.; Demirel, O.F.; Emül, M.; Duran, A.; Uğur, M. Relationships between IGF-1, schizophrenia, and treatment of metabolic syndrome. Compr. Psychiatry 2014, 55, 1391–1397. [Google Scholar] [CrossRef]
- Okamoto, N.; Yoshino, K.; Kitagawa, S.; Fujii, R.; Hamada, S.; Ikenouchi, A.; Konishi, Y.; Ueda, N.; Eto, Y.; Tsutsumi, Y.; et al. Association between Serum Insulin-like Growth Factor 1 Levels and the Clinical Symptoms of Chronic Schizophrenia: Preliminary Findings. Front. Psychiatry 2021, 12, 653802. [Google Scholar] [CrossRef]
- Chao, X.L.; Jiang, S.Z.; Xiong, J.W.; Zhan, J.Q.; Yan, K.; Yang, Y.J.; Jiang, L.P. The association between serum insulin-like growth factor 1 and cognitive impairments in patients with schizophrenia. Psychiatry Res. 2020, 285, 112731. [Google Scholar] [CrossRef] [PubMed]
- Venkatasubramanian, G.; Chittiprol, S.; Neelakantachar, N.; Naveen, M.N.; Thirthall, J.; Gangadhar, B.N.; Shetty, K.T. Insulin and insulin-like growth factor-1 abnormalities in antipsychotic-naive schizophrenia. Am. J. Psychiatry 2007, 164, 1557–1560. [Google Scholar] [CrossRef] [PubMed]
- Venkatasubramanian, G.; Chittiprol, S.; Neelakantachar, N.; Shetty, T.; Gangadhar, B.N. Effect of antipsychotic treatment on Insulin-like Growth Factor-1 and cortisol in schizophrenia: A longitudinal study. Schizophr. Res. 2010, 119, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.K.; Huang, C.Y.; Liou, Y.J.; Wang, C.K.; Lee, S.D. Glucose-insulin homeostasis, lipid profiles and GH-IGF-IGFBP axis in clozapine-treated schizophrenic obesity versus non-psychiatric obesity. Int. J. Obes. 2008, 32, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Yesilkaya, U.H.; Gica, S.; Ilnem, M.C.; Sen, M.; Ipekcioglu, D. Evaluation of IGF-1 as a novel theranostic biomarker for schizophrenia. J. Psychiatr. Res. 2021, 140, 172–179. [Google Scholar] [CrossRef]
- Chen, M.; Zhang, L.; Jiang, Q. Peripheral IGF-1 in bipolar disorder and major depressive disorder: A systematic review and meta-analysis. Ann. Palliat. Med. 2020, 9, 4044–4053. [Google Scholar] [CrossRef]
- Kim, Y.K.; Na, K.S.; Hwang, J.A.; Yoon, H.K.; Lee, H.J.; Hahn, S.W.; Lee, B.H.; Jung, H.Y. High insulin-like growth factor-1 in patients with bipolar I disorder: A trait marker? J. Affect. Disord. 2013, 151, 738–743. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, T.; He, S.; Hong, B.; Chen, Z.; Peng, D.; Wu, Y.; Wen, H.; Lin, Z.; Fang, Y.; et al. Elevated serum levels of FGF-2, NGF and IGF-1 in patients with manic episode of bipolar disorder. Psychiatry Res. 2014, 218, 54–60. [Google Scholar] [CrossRef]
- da Silva, E.G.; Pfaffenseller, B.; Walz, J.; Stertz, L.; Fries, G.; Rosa, A.R.; Magalhães, P.V. Peripheral insulin-like growth factor 1 in bipolar disorder. Psychiatry Res. 2017, 250, 30–34. [Google Scholar] [CrossRef]
- Tunçel, Ö.K.; Sarisoy, G.; Çetin, E.; Kaynar Tunçel, E.; Bilgici, B.; Karaustaoğlu, A. Neurotrophic factors in bipolar disorders patients with manic episode. Turk. J. Med. Sci. 2020, 50, 985–993. [Google Scholar] [CrossRef]
- Palomino, A.; González-Pinto, A.; Martinez-Cengotitabengoa, M.; Ruiz de Azua, S.; Alberich, S.; Mosquera, F.; Matute, C. Relationship between negative symptoms and plasma levels of insulin-like growth factor 1 in first-episode schizophrenia and bipolar disorder patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2013, 44, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Melkersson, K.I.; Hulting, A.L.; Brismar, K.E. Elevated levels of insulin, leptin, and blood lipids in olanzapine-treated patients with schizophrenia or related psychoses. J. Clin. Psychiatry 2000, 61, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Bot, M.; Jansen, R.; Chan, M.K.; Cooper, J.D.; Bahn, S.; Penninx, B.W. Serum proteomic profiles of depressive subtypes. Transl. Psychiatry 2016, 6, e851. [Google Scholar] [CrossRef] [PubMed]
- Milanesi, E.; Zanardini, R.; Rosso, G.; Maina, G.; Barbon, A.; Mora, C.; Minelli, A.; Gennarelli, M.; Bocchio-Chiavetto, L. Insulin-like growth factor binding protein 2 in bipolar disorder: An expression study in peripheral tissues. World J. Biol. Psychiatry 2018, 19, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Agis-Balboa, R.C.; Fischer, A. Generating new neurons to circumvent your fears: The role of IGF signaling. Cell Mol. Life Sci. 2014, 71, 21–42. [Google Scholar] [CrossRef]
- Agis-Balboa, R.C.; Arcos-Diaz, D.; Wittnam, J.; Govindarajan, N.; Blom, K.; Burkhardt, S.; Haladyniak, U.; Agbemenyah, H.Y.; Zovoilis, A.; Salinas-Riester, G.; et al. A hippocampal insulin-growth factor 2 pathway regulates the extinction of fear memories. EMBO J. 2011, 30, 4071–4083. [Google Scholar] [CrossRef]
- Agbemenyah, H.Y.; Agis-Balboa, R.C.; Burkhardt, S.; Delalle, I.; Fischer, A. Insulin growth factor binding protein 7 is a novel target to treat dementia. Neurobiol. Dis. 2014, 62, 135–143. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Iwamoto, T.; Ouchi, Y. Emerging evidence of insulin-like growth factor 2 as a memory enhancer: A unique animal model of cognitive dysfunction with impaired adult neurogenesis. Rev. Neurosci. 2014, 25, 559–574. [Google Scholar] [CrossRef]
- Pardo, M.; Cheng, Y.; Sitbon, Y.H.; Lowell, J.A.; Grieco, S.F.; Worthen, R.J.; Desse, S.; Barreda-Diaz, A. Insulin growth factor 2 (IGF2) as an emergent target in psychiatric and neurological disorders. Rev. Neurosci. Res. 2019, 149, 1–13. [Google Scholar] [CrossRef]
- Ranke, M.B. Insulin-like growth factor binding-protein-3 (IGFBP-3). Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 701–711. [Google Scholar] [CrossRef]
- Ricort, J.M. Insulin-like growth factor binding protein (IGFBP) signalling. Growth Horm. IGF Res. 2004, 14, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Clemmons, D.R. Insulin-like growth factor binding proteins and their role in controlling IGF actions. Cytokine Growth Factor Rev. 1997, 8, 45–62. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.C. IGF binding proteins in cancer: Mechanistic and clinical insights. Nat. Rev. Cancer 2014, 14, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Juul, A.; Dalgaard, P.; Blum, W.F.; Bang, P.; Hall, K.; Michaelsen, K.F.; Müller, J.; Skakkebaek, N.E. Serum levels of insulin-like growth factor (IGF)-binding protein-3 (IGFBP-3) in healthy infants, children, and adolescents: The relation to IGF-I, IGF-II, IGFBP-1, IGFBP-2, age, sex, body mass index, and pubertal maturation. J. Clin. Endocrinol. Metab. 1995, 80, 2534–2542. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.C.; Martin, J.L.; Beniac, V.A. High molecular weight insulin-like growth factor binding protein complex. Purification and properties of the acid-labile subunit from human serum. J. Biol. Chem. 1989, 264, 11843–11848. [Google Scholar] [CrossRef]
- Jin, L.; Shen, F.; Weinfeld, M.; Sergi, C. Insulin Growth Factor Binding Protein 7 (IGFBP7)-Related Cancer and IGFBP3 and IGFBP7 Crosstalk. Front. Oncol. 2020, 10, 727. [Google Scholar] [CrossRef]
- Armstrong, R.A. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019, 57, 87–105. [Google Scholar] [CrossRef]
- Mora, C.; Zonca, V.; Riva, M.A.; Cattaneo, A. Blood biomarkers and treatment response in major depression. Expert. Rev. Mol. Diagn. 2018, 18, 513–529. [Google Scholar] [CrossRef]
- Meana, J.J.; Mollinedo-Gajate, I. Biomarkers in Psychiatry: Between myth and clinical reality. Rev. Psiquiatr. Salud Ment. 2017, 10, 183–184. [Google Scholar] [CrossRef]
- Lozupone, M.; La Montagna, M.; D’Urso, F.; Daniele, A.; Greco, A.; Seripa, D.; Logroscino, G.; Bellomo, A.; Panza, F. The Role of Biomarkers in Psychiatry. Adv. Exp. Med. Biol. 2019, 1118, 135–162. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.J.; Pizzagalli, D.A.; Sproule, B.A.; Kennedy, S.H. Assessing anhedonia in depression: Potentials and pitfalls. Neurosci. Biobehav. Rev. 2016, 65, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Dik, M.G.; Pluijm, S.M.; Jonker, C.; Deeg, D.J.; Lomecky, M.Z.; Lips, P. Insulin-like growth factor I (IGF-I) and cognitive decline in older persons. Neurobiol. Aging 2004, 24, 573–581, Erratum in Neurobiol. Aging 2004, 25, 271. [Google Scholar] [CrossRef] [PubMed]
- Duron, E.; Funalot, B.; Brunel, N.; Coste, J.; Quinquis, L.; Viollet, C.; Belmin, J.; Jouanny, P.; Pasquier, F.; Treluyer, J.M.; et al. Insulin-like growth factor-I and insulin-like growth factor binding protein-3 in Alzheimer’s disease. J. Clin. Endocrinol. Metab. 2012, 97, 4673–4681. [Google Scholar] [CrossRef]
- Johansson, P.; Åberg, D.; Johansson, J.O.; Mattsson, N.; Hansson, O.; Ahrén, B.; Isgaard, J.; Åberg, N.D.; Blennow, K.; Zetterberg, H.; et al. Serum but not cerebrospinal fluid levels of insulin-like growth factor-I (IGF-I) and IGF-binding protein-3 (IGFBP-3) are increased in Alzheimer’s disease. Psychoneuroendocrinology 2013, 38, 1729–1737. [Google Scholar] [CrossRef]
- Salehi, Z.; Mashayekhi, F.; Naji, M. Insulin like growth factor-1 and insulin like growth factor binding proteins in the cerebrospinal fluid and serum from patients with Alzheimer’s disease. Biofactors 2008, 33, 99–106. [Google Scholar] [CrossRef]
- Vardy, E.R.; Rice, P.J.; Bowie, P.C.; Holmes, J.D.; Grant, P.J.; Hooper, N.M. Increased circulating insulin-like growth factor-1 in late-onset Alzheimer’s disease. J. Alzheimers Dis. 2007, 12, 285–290. [Google Scholar] [CrossRef]
- Vargas, T.; Martinez-Garcia, A.; Antequera, D.; Vilella, E.; Clarimon, J.; Mateo, I.; Sanchez-Juan, P.; Rodriguez-Rodriguez, E.; Frank, A.; Rosich-Estrago, M.; et al. IGF-I gene variability is associated with an increased risk for AD. Neurobiol. Aging 2011, 32, 556.e3–556.e11. [Google Scholar] [CrossRef]
- Watanabe, T.; Miyazaki, A.; Katagiri, T.; Yamamoto, H.; Idei, T.; Iguchi, T. Relationship between serum insulin-like growth factor-1 levels and Alzheimer’s disease and vascular dementia. J. Am. Geriatr. Soc. 2005, 53, 1748–1753. [Google Scholar] [CrossRef]
- Duman, R.S.; Heninger, G.R.; Nestler, E.J. A molecular and cellular theory of depression. Arch. Gen. Psychiatry 1997, 54, 597–606. [Google Scholar] [CrossRef]
- Nedic Erjavec, G.; Sagud, M.; Nikolac Perkovic, M.; Svob Strac, D.; Konjevod, M.; Tudor, L.; Uzun, S.; Pivac, N. Depression: Biological markers and treatment. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 105, 110139. [Google Scholar] [CrossRef]
- Buschke, H.; Sliwinski, M.J.; Kuslansky, G.; Lipton, R.B. Diagnosis of early dementia by the Double Memory Test: Encoding specificity improves diagnostic sensitivity and specificity. Neurology 1997, 48, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Lemos, R.; Duro, D.; Simões, M.R.; Santana, I. The free and cued selective reminding test distinguishes frontotemporal dementia from Alzheimer’s disease. Arch. Clin. Neuropsychol. 2014, 29, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Matias-Guiu, J.A.; Cabrera-Martín, M.N.; Curiel, R.E.; Valles-Salgado, M.; Rognoni, T.; Moreno-Ramos, T.; Carreras, J.L.; Loewenstein, D.A.; Matías-Guiu, J. Comparison between FCSRT and LASSI-L to Detect Early Stage Alzheimer’s Disease. J. Alzheimers Dis. 2018, 61, 103–111. [Google Scholar] [CrossRef]
- Olivares, J.M.; Berrios, G.E.; Bousoño, M. Self-Assessment Anhedonia Scale (SAAS) Neurol. Psychiatry Brain Res. 2005, 12, 121–134. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Grober, E.; Buschke, H.; Crystal, H.; Bang, S.; Dresner, R. Screening for dementia by memory testing. Neurology 1988, 38, 900–903. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Control (n = 48) | Depression (n = 51) | p-Value |
|---|---|---|---|
| Gender (F/M) | 22/26 | 30/21 | 0.230 1 |
| Age (years) | 42.58 ± 11.54 | 52.71 ± 14.57 | 0.153 2 |
| SAAS (total) | 108.17 ± 59.32 | 480.77 ± 160.62 | <0.001 3 |
| IGF-2 (ng/mL) | 116.69 ± 53.40 | 249.86 ± 119.57 | <0.001 3 |
| IGFBP-1 (ng/mL) | 7.57 ± 5.08 | 12.84 ± 14.31 | 0.061 3 |
| IGFBP-3 (ng/mL) | 498.26 ± 89.57 | 506.12 ± 139.91 | 0.809 3 |
| IGFBP-5 (ng/mL) | 86.14 ± 15.12 | 86.95 ± 20.69 | 0.904 3 |
| IGFBP-7 (ng/mL) | 67.01 ± 25.14 | 82.90 ± 26.44 | <0.01 4 |
| D | D0 (n = 15) | D1 (n = 15) | p-Value |
|---|---|---|---|
| Gender (F/M) | 7/8 | - | |
| Age (years) | 61.60 ± 10.60 | - | |
| SAAS (total) | 400.35 ± 160.41 | 370.40 ± 136.26 | 0.277 1 |
| HDRS | 24.93 ± 6.18 | 15.00 ± 4.11 | <0.001 2 |
| MMSE | 23.53 ± 4.52 | 24.80 ± 5.45 | <0.05 2 |
| FCSRT (TFR) | 27.97 ± 10.81 | 31.49 ± 10.55 | <0.01 1 |
| FCSRT (TR) | 33.91 ± 9.12 | 35.71 ± 10.90 | <0.05 1 |
| FCSRT (DFR) | 10.43 ± 3.50 | 12.13 ± 3.55 | <0.01 1 |
| FCSRT (DTR) | 12.94 ± 3.46 | 14.20 ± 2.39 | <0.01 1 |
| IGF-2 (ng/mL) | 241.29 ± 99.86 | 156.71 ± 35.64 | <0.01 |
| IGFBP-1 (ng/mL) | 10.02 ± 6.61 | 7.35 ± 4.16 | 0.258 |
| IGFBP-3 (ng/mL) | 456.49 ± 118.11 | 270.14 ± 39.86 | <0.001 |
| IGFBP-5 (ng/mL) | 84.24 ± 13.56 | 42.78 ± 6.14 | <0.001 |
| IGFBP-7 (ng/mL) | 82.36 ± 25.50 | 116.19 ± 29.85 | <0.05 |
| Metabolic Parameters | IGF Plasma Proteins | |||||
|---|---|---|---|---|---|---|
| IGF-2 (ng/mL) | IGFBP-1 (ng/mL) | IGFBP-3 (ng/mL) | IGFBP-5 (ng/mL) | IGFBP-7 (ng/mL) | ||
| Glucose (mg/dL) | r | 0.105 | 0.231 | 0.035 | −0.004 | 0.085 |
| p | 0.469 | 0.103 | 0.805 | 0.977 | 0.522 | |
| Albumin (g/dL) | r | −0.121 | 0.228 | −0.115 p | −0.216 | −0.066 p |
| p | 0.407 | 0.111 | 0.425 | 0.131 | 0.648 | |
| Cholesterol (mg/dL) | r | 0.155 | 0.190 | 0.158 p | 0.192 | 0.168 p |
| p | 0.293 | 0.195 | 0.284 | 0.190 | 0.252 | |
| Triglycerides (mg/dL) | r | 0.138 | 0.268 | −0.108 | −0.003 | 0.275 p |
| p | 0.349 | 0.065 | 0.464 | 0.983 | 0.058 | |
| Predictors | F (df1, df2) | R2 | p | β | SD | pβ |
|---|---|---|---|---|---|---|
| Model 1 | 17.35 (3, 94) | 0.36 | <0.001 | 71.96 | 36.28 | 0.05 |
| Group | 121.74 | 20.62 | <0.001 | |||
| Age | 0.83 | 0.73 | 0.258 | |||
| Gender | 20.45 | 19.33 | 0.293 | |||
| Model 2 | 25.44 (2, 95) | 0.35 | <0.001 | 86.86 | 33.45 | 0.011 |
| Group | 125.97 | 20.24 | <0.001 | |||
| Age | 0.83 | 0.73 | 0.332 | |||
| Model 3 | 49.96 (1, 96) | 0.34 | <0.001 | 116.69 | 13.45 | <0.001 |
| Group | 133.17 | 18.84 | <0.001 |
| Predictors | F (df1, df2) | R2 | p | β | SD | pβ |
|---|---|---|---|---|---|---|
| Model 1 | 9.37 (3, 95) | 0.23 | <0.001 | 31.18 | 9.29 | 0.001 |
| Group | 7.21 | 5.26 | 0.174 | |||
| Age | 0.76 | 0.19 | <0.001 | |||
| Gender | 7.92 | 4.93 | 0.112 | |||
| Model 2 | 13.00 (2, 96) | 0.21 | <0.001 | 29.61 | 9.26 | 0.002 |
| Age | 0.85 | 0.17 | <0.001 | |||
| Gender | 9.13 | 4.88 | 0.064 |
| Subjective Scales | IGF Plasma Proteins | |||||
|---|---|---|---|---|---|---|
| IGF-2 (ng/mL) | IGFBP-1 (ng/mL) | IGFBP-3 (ng/mL) | IGFBP-5 (ng/mL) | IGFBP-7 (ng/mL) | ||
| HDRS | r | −0.437 | −0.077 | −0.002 | 0.007 | −0.447 |
| p | 0.104 | 0.784 | 0.995 | 0.980 | 0.104 | |
| MMSE | r | −0.229 | <0.000 | 0.714 | 0.670 | 0.155 |
| p | 0.104 | 0.999 | 0.003 | 0.006 | 0.581 | |
| SAAS | r | −0.289 | 0.250 | −0.064 | −0.068 | −0.089 |
| p | 0.296 | 0.369 | 0.820 | 0.810 | 0.752 | |
| FCSRT_TFR | r | −0.256 | −0.066 | 0.556 | 0.456 | −0.077 |
| p | 0.358 | 0.815 | 0.031 | 0.088 | 0.785 | |
| FCSRT_TR | r | −0.298 | −0.034 | 0.754 | 0.672 | −0.005 |
| p | 0.28 | 0.904 | 0.001 | 0.006 | 0.985 | |
| FCSRT_DFR | r | −0.125 | −0.05 | 0.409 | 0.294 | 0.183 |
| p | 0.656 | 0.859 | 0.130 | 0.288 | 0.514 | |
| FCSRT_DTR | r | −0.394 | −0.027 | 0.486 | 0.452 | −0.013 |
| p | 0.146 | 0.924 | 0.066 | 0.091 | 0.964 | |
| Subjective Scales | IGF Plasma Proteins | |||||
|---|---|---|---|---|---|---|
| IGF-2 (ng/mL) | IGFBP-1 (ng/mL) | IGFBP-3 (ng/mL) | IGFBP-5 (ng/mL) | IGFBP-7 (ng/mL) | ||
| HDRS | r | −0.183 | 0.457 | −0.120 | 0.045 | 0.219 |
| p | 0.514 | 0.087 | 0.669 | 0.874 | 0.433 | |
| MMSE | r | −0.287 | 0.028 | 0.285 | 0.66 | −0.287 |
| p | 0.3 | 0.921 | 0.303 | 0.007 | 0.015 | |
| SAAS | r | −0.372 | 0.309 | −0.252 | −0.239 | −0.084 |
| p | 0.172 | 0.263 | 0.365 | 0.390 | 0.766 | |
| FCSRT_TFR | r | −0.206 | 0.068 | 0.493 | 0.608 | −0.422 |
| p | 0.461 | 0.809 | 0.062 | 0.016 | 0.188 | |
| FCSRT_TR | r | −0.251 | 0.295 | 0.410 | 0.566 | −0.380 |
| p | 0.368 | 0.286 | 0.129 | 0.028 | 0.163 | |
| FCSRT_DFR | r | −0.203 | −0.129 | 0.161 | 0.483 | −0.322 |
| p | 0.469 | 0.647 | 0.566 | 0.068 | 0.242 | |
| FCSRT_DTR | r | −0.286 | −0.162 | 0.099 | 0.429 | −0.3 |
| p | 0.302 | 0.565 | 0.726 | 0.111 | 0.277 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Pereira, C.; Penedo, M.A.; Rivera-Baltanás, T.; Pérez-Márquez, T.; Alves-Villar, M.; Fernández-Martínez, R.; Veiga, C.; Salgado-Barreira, Á.; Prieto-González, J.M.; Ortolano, S.; et al. Protein Plasma Levels of the IGF Signalling System Are Altered in Major Depressive Disorder. Int. J. Mol. Sci. 2023, 24, 15254. https://doi.org/10.3390/ijms242015254
Fernández-Pereira C, Penedo MA, Rivera-Baltanás T, Pérez-Márquez T, Alves-Villar M, Fernández-Martínez R, Veiga C, Salgado-Barreira Á, Prieto-González JM, Ortolano S, et al. Protein Plasma Levels of the IGF Signalling System Are Altered in Major Depressive Disorder. International Journal of Molecular Sciences. 2023; 24(20):15254. https://doi.org/10.3390/ijms242015254
Chicago/Turabian StyleFernández-Pereira, Carlos, Maria Aránzazu Penedo, Tania Rivera-Baltanás, Tania Pérez-Márquez, Marta Alves-Villar, Rafael Fernández-Martínez, César Veiga, Ángel Salgado-Barreira, José María Prieto-González, Saida Ortolano, and et al. 2023. "Protein Plasma Levels of the IGF Signalling System Are Altered in Major Depressive Disorder" International Journal of Molecular Sciences 24, no. 20: 15254. https://doi.org/10.3390/ijms242015254
APA StyleFernández-Pereira, C., Penedo, M. A., Rivera-Baltanás, T., Pérez-Márquez, T., Alves-Villar, M., Fernández-Martínez, R., Veiga, C., Salgado-Barreira, Á., Prieto-González, J. M., Ortolano, S., Olivares, J. M., & Agís-Balboa, R. C. (2023). Protein Plasma Levels of the IGF Signalling System Are Altered in Major Depressive Disorder. International Journal of Molecular Sciences, 24(20), 15254. https://doi.org/10.3390/ijms242015254