

Data-Independent Acquisition Mass Spectrometry Analysis of FFPE Rectal Cancer Samples Offers In-Depth Proteomics Characterization of the Response to Neoadjuvant Chemoradiotherapy

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Study Design and Rationale
2.2. Proteomic Comparison of Responders and Non-Responders
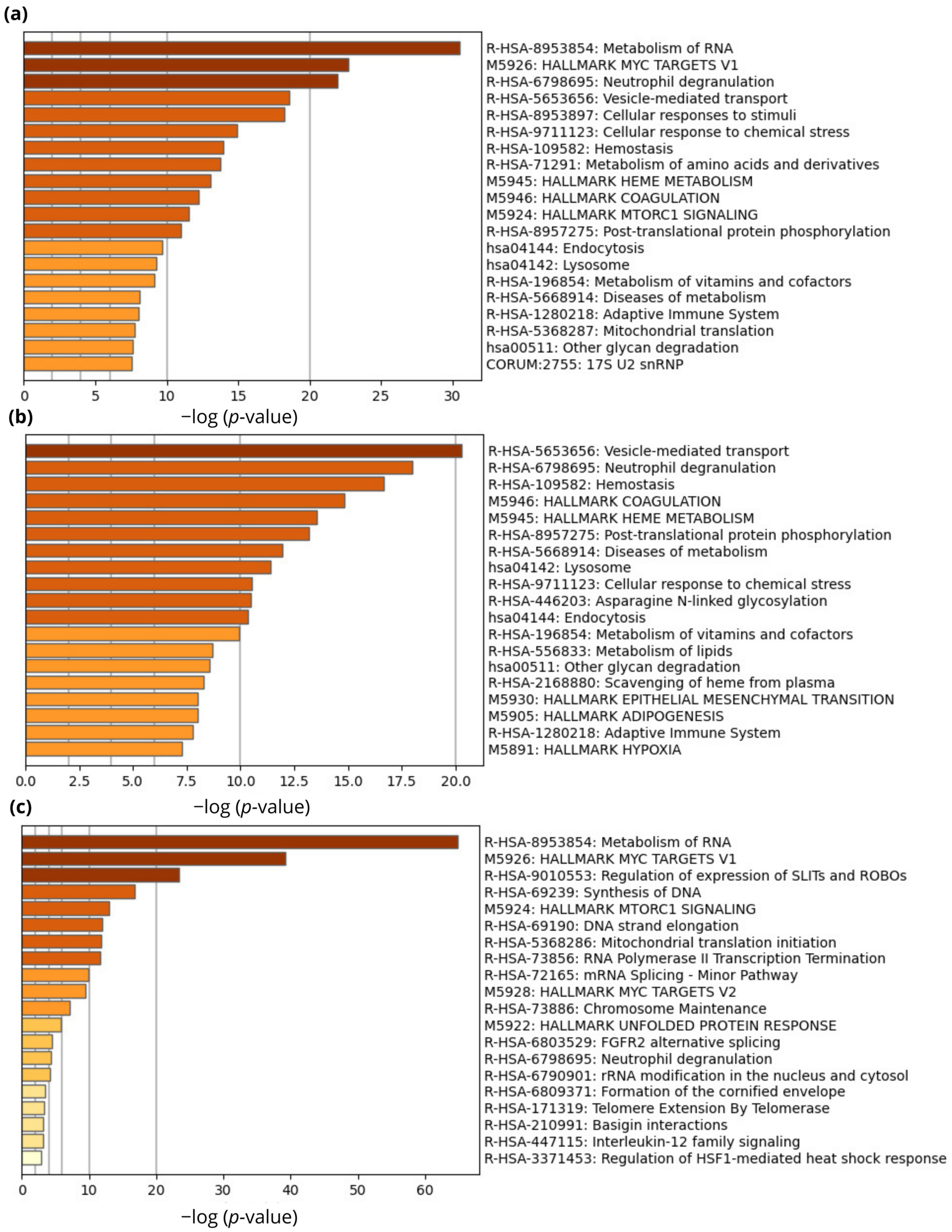
2.3. Pathway Enrichment Analysis
2.4. STRING In Silico Analysis
2.5. Shortlisting of Potential Biomarkers Based on Transcriptomics Data
2.6. Search for Drug Targets
3. Discussion
4. Materials and Methods
4.1. Patient Cohort Characteristics and Treatment
Protein Extraction from FFPE Tissue Samples
4.2. Protein Digestion and Preparation for LC-MS/MS Analysis
4.3. LC-MS/MS Analysis
4.4. MS Data Analysis
4.5. Pathway Enrichment Analysis
4.6. STRING In Silico Analysis
4.7. Shortlisting of Potential Biomarkers
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [PubMed]
- Institute of Public Health of Serbia “Dr Milan Jovanović Batut”. Malignant Tumours in Republic of Serbia; Institute of Public Health of Serbia “Dr Milan Jovanović Batut”: Belgrade, Serbia, 2022. [Google Scholar]
- Jakovljevic, K.; Malisic, E.; Cavic, M.; Krivokuca, A.; Dobricic, J.; Jankovic, R. KRAS and BRAF mutations in Serbian patients with colorectal cancer. J. BUON 2012, 17, 575–580. [Google Scholar] [PubMed]
- Brotto, K.; Malisic, E.; Cavic, M.; Krivokuca, A.; Jankovic, R. The Usability of Allele-Specific PCR and Reverse-Hybridization Assays for KRAS Genotyping in Serbian Colorectal Cancer Patients. Dig. Dis. Sci. 2013, 58, 998–1003. [Google Scholar] [PubMed]
- Čavić, M.; Krivokuća, A.; Boljević, I.; Brotto, K.; Jovanović, K.; Tanić, M.; Filipović, L.; Zec, M.; Mališić, E.; Janković, R.; et al. Pharmacogenetics in cancer therapy–8 years of experience at the Institute for Oncology and Radiology of Serbia. J. BUON 2016, 21, 1287–1295. [Google Scholar] [PubMed]
- Stojanovic-Rundic, S.; Marinkovic, M.; Cavic, M.; Karapandzic, V.P.; Gavrilovic, D.; Jankovic, R.; de Voer, R.M.; Castellvi-Bel, S.; Krivokapić, Z. The role of haematological parameters in predicting the response to radical chemoradiotherapy in patients with anal squamous cell cancer. Radiol. Oncol. 2021, 55, 449–458. [Google Scholar] [PubMed]
- Nikolic, N.; Radosavljevic, D.; Gavrilovic, D.; Nikolic, V.; Stanic, N.; Spasic, J.; Cacev, T.; Castellvi-Bel, S.; Cavic, M.; Jankovic, G. Prognostic Factors for Post-Recurrence Survival in Stage II and III Colorectal Carcinoma Patients. Medicina 2021, 57, 1108. [Google Scholar]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar]
- Stoffel, E.M.; Murphy, C.C. Epidemiology and Mechanisms of the Increasing Incidence of Colon and Rectal Cancers in Young Adults. Gastroenterology 2020, 158, 341–353. [Google Scholar]
- Brierley, D.J.; Gospodarowicz, K.M.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; Wiley: New York, NY, USA, 2017. [Google Scholar]
- Sauer, R.; Liersch, T.; Merkel, S.; Fietkau, R.; Hohenberger, W.; Hess, C.; Becker, H.; Raab, H.R.; Villanueva, M.T.; Witzigmann, H.; et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J. Clin. Oncol. 2012, 30, 1926–1933. [Google Scholar]
- Oronsky, B.; Reid, T.; Larson, C.; Knox, S.J. Locally advanced rectal cancer: The past, present, and future. Semin. Oncol. 2020, 47, 85–92. [Google Scholar]
- Petrelli, F.; Trevisan, F.; Cabiddu, M.; Sgroi, G.; Bruschieri, L.; Rausa, E.; Ghidini, M.; Turati, L. Total Neoadjuvant Therapy in Rectal Cancer: A Systematic Review and Meta-analysis of Treatment Outcomes. Ann. Surg. 2020, 271, 440–448. [Google Scholar] [PubMed]
- Loos, M.; Quentmeier, P.; Schuster, T.; Nitsche, U.; Gertler, R.; Keerl, A.; Kocher, T.; Friess, H.; Rosenberg, R. Effect of preoperative radio(chemo)therapy on long-term functional outcome in rectal cancer patients: A systematic review and meta-analysis. Ann. Surg. Oncol. 2013, 20, 1816–1828. [Google Scholar] [PubMed]
- Bernier, L.; Balyasnikova, S.; Tait, D.; Brown, G. Watch-and-Wait as a Therapeutic Strategy in Rectal Cancer. Curr. Colorectal Cancer Rep. 2018, 14, 37–55. [Google Scholar] [PubMed]
- Dossa, F.; Chesney, T.R.; Acuna, S.A.; Baxter, N.N. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 501–513. [Google Scholar]
- Smith, J.J.; Strombom, P.; Chow, O.S.; Roxburgh, C.S.; Lynn, P.; Eaton, A.; Widmar, M.; Ganesh, K.; Yaeger, R.; Cercek, A.; et al. Assessment of a Watch-and-Wait Strategy for Rectal Cancer in Patients with a Complete Response after Neoadjuvant Therapy. JAMA Oncol. 2019, 5, e185896. [Google Scholar]
- López-Campos, F.; Martín-Martín, M.; Fornell-Pérez, R.; García-Pérez, J.C.; Die-Trill, J.; Fuentes-Mateos, R.; López-Durán, S.; Domínguez-Rullán, J.; Ferreiro, R.; Riquelme-Oliveira, A.; et al. Watch and wait approach in rectal cancer: Current controversies and future directions. World J. Gastroenterol. 2020, 26, 4218–4239. [Google Scholar]
- Babic, T.; Lygirou, V.; Rosic, J.; Miladinov, M.; Djikic Rom, A.; Baira, E.; Stroggilos, R.; Pappa, E.; Zoidakis, J.; Krivokapic, Z.; et al. Pilot proteomic study of locally advanced rectal cancer before and after neoadjuvant chemoradiotherapy indicates high metabolic activity in non-responders’ tumor tissue. Proteom. Clin Appl. 2023, 17, 2100116. [Google Scholar]
- Szklarczyk, D.; Gable, A.L.; Nastou, K.C.; Lyon, D.; Kirsch, R.; Pyysalo, S.; Doncheva, N.T.; Legeay, M.; Fang, T.; Bork, P.; et al. The STRING database in 2021: Customizable protein-protein networks, and functional characterization of user-uploaded gene/measurement sets. Nucleic Acids Res. 2021, 49, D605–D612. [Google Scholar]
- Uhlen, M.; Zhang, C.; Lee, S.; Sjöstedt, E.; Fagerberg, L.; Bidkhori, G.; Benfeitas, R.; Arif, M.; Liu, Z.; Edfors, F.; et al. A pathology atlas of the human cancer transcriptome. Science 2017, 357, eaan2507. [Google Scholar] [CrossRef]
- Stelzer, G.; Rosen, N.; Plaschkes, I.; Zimmerman, S.; Twik, M.; Fishilevich, S.; Stein, T.I.; Nudel, R.; Lieder, I.; Mazor, Y.; et al. The GeneCards suite: From gene data mining to disease genome sequence analyses. Curr. Protoc. Bioinform. 2016, 2016, 1.30.1–1.30.33. [Google Scholar]
- Safran, M.; Rosen, N.; Twik, M.; BarShir, R.; Stein, T.I.; Dahary, D.; Fishilevich, S.; Lancet, D. The GeneCards Suite. Practical Guide to Life Science Databases; Springer Nature: Singapore, 2021; pp. 27–56. [Google Scholar]
- Kim, Y.J.; Sweet, S.M.M.; Egertson, J.D.; Sedgewick, A.J.; Woo, S.; Liao, W.L.; Merrihew, G.E.; Searle, B.C.; Vaske, C.; Heaton, R.; et al. Data-Independent Acquisition Mass Spectrometry to Quantify Protein Levels in FFPE Tumor Biopsies for Molecular Diagnostics. J. Proteome Res. 2019, 18, 426–435. [Google Scholar] [PubMed]
- Weke, K.; Kote, S.; Faktor, J.; Al Shboul, S.; Uwugiaren, N.; Brennan, P.M.; Goodlett, D.R.; Hupp, T.R.; Dapic, I. DIA-MS proteome analysis of formalin-fixed paraffin-embedded glioblastoma tissues. Anal. Chim. Acta 2022, 1204, 339695. [Google Scholar] [PubMed]
- Amarnani, A.; Capri, J.R.; Souda, P.; Elashoff, D.A.; Lopez, I.A.; Whitelegge, J.P.; Singh, R.R. Quantitative Proteomics Using Formalin-fixed, Paraffin-embedded Biopsy Tissues in Inflammatory Disease. J. Proteom. Bioinform. 2019, 12, 104. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.H.; Li, J.; Gong, H.F.; Yu, G.Y.; Liu, P.; Hao, L.Q.; Liu, L.J.; Bai, C.G.; Zhang, W. Comparison of Fresh Frozen Tissue With Formalin-Fixed Paraffin-Embedded Tissue for Mutation Analysis Using a Multi-Gene Panel in Patients with Colorectal Cancer. Front. Oncol. 2020, 10, 310. [Google Scholar]
- Repetto, O.; De Re, V.; De Paoli, A.; Belluco, C.; Alessandrini, L.; Canzonieri, V. Identification of Protein Clusters Predictive of Tumor Response in Rectal Cancer Patients Receiving Neoadjuvant Chemo-Radiotherapy. Oncotarget 2017, 8, 28328. Available online: www.impactjournals.com/oncotarget/ (accessed on 15 April 2022).
- Chauvin, A.; Wang, C.S.; Geha, S.; Garde-Granger, P.; Mathieu, A.A.; Lacasse, V.; Boisvert, F.M. The response to neoadjuvant chemoradiotherapy with 5-fluorouracil in locally advanced rectal cancer patients: A predictive proteomic signature. Clin. Proteom. 2018, 15, 1–16. [Google Scholar]
- Pawlik, T.M.; Keyomarsi, K. Role of cell cycle in mediating sensitivity to radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 928–942. [Google Scholar]
- Khan, S.U.; Khan, I.M.; Khan, M.U.; Ud Din, M.A.; Khan, M.Z.; Khan, N.M.; Liu, Y. Role of LGMN in tumor development and its progression and connection with the tumor microenvironment. Front. Mol. Biosci. 2023, 10, 1121964. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, S.; Wang, H.; Cui, Y.; Wang, Z.; Cheng, X.; Li, W.; Hou, J.; Ji, Y.; Liu, T. High Level of Legumain Was Correlated With Worse Prognosis and Peritoneal Metastasis in Gastric Cancer Patients. Front. Oncol. 2020, 10, 966. [Google Scholar] [CrossRef]
- Yao, Y.; Zhou, D.; Shi, D.; Zhang, H.; Zhan, S.; Shao, X.; Sun, K.; Sun, L.; Wu, G.; Tian, K.; et al. GLI1 overexpression promotes gastric cancer cell proliferation and migration and induces drug resistance by combining with the AKT-mTOR pathway. Biomed. Pharmacother. 2019, 111, 993–1004. [Google Scholar]
- Murugan, A.K. mTOR: Role in cancer, metastasis and drug resistance. Semin. Cancer Biol. 2019, 59, 92–111. [Google Scholar] [PubMed]
- Janku, F.; McConkey, D.J.; Hong, D.S.; Kurzrock, R. Autophagy as a target for anticancer therapy. Nat. Rev. Clin. Oncol. 2011, 8, 528–539. [Google Scholar] [PubMed]
- Saxton, R.A.; Sabatini, D.M. mTOR Signaling in Growth, Metabolism, and Disease. Cell 2017, 168, 960–976. [Google Scholar] [PubMed]
- Mossmann, D.; Park, S.; Hall, M.N. mTOR signalling and cellular metabolism are mutual determinants in cancer. Nat. Rev. Cancer 2018, 18, 744–757. [Google Scholar]
- Heeran, A.B.; Dunne, M.R.; Morrissey, M.E.; Buckley, C.E.; Clarke, N.; Cannon, A.; Donlon, N.E.; Nugent, T.S.; Durand, M.; Dunne, C.; et al. The protein secretome is altered in rectal cancer tissue compared to normal rectal tissue, and alterations in the secretome induce enhanced innate immune responses. Cancers 2021, 13, 1–18. [Google Scholar]
- Lee, S.Y.; Kim, C.H.; Kim, Y.J.; Kwak, H.D.; Ju, J.K.; Kim, H.R. Obesity as an independent predictive factor for pathologic complete response after neoadjuvant chemoradiation in rectal cancer. Ann. Surg. Treat Res. 2019, 96, 116–122. [Google Scholar] [CrossRef]
- Clark, W.; Siegel, E.M.; Chen, Y.A.; Zhao, X.; Parsons, C.M.; Hernandez, J.M.; Weber, J.; Thareja, S.; Choi, J.; Shibata, D. Quantitative measures of visceral adiposity and body mass index in predicting rectal cancer outcomes after neoadjuvant chemoradiation. J. Am. Coll. Surg. 2013, 216, 1070–1081. [Google Scholar] [CrossRef]
- Huminiecki, L. Magic roundabout is an endothelial-specific ohnolog of ROBO1 which neo-functionalized to an essential new role in angiogenesis. PLoS ONE 2019, 14, e0208952. [Google Scholar]
- Jones, C.A.; Nishiya, N.; London, N.R.; Zhu, W.; Sorensen, L.K.; Chan, A.C.; Lim, C.J.; Chen, H.; Zhang, Q.; Schultz, P.G.; et al. Slit2-Robo4 signalling promotes vascular stability by blocking Arf6 activity. Nat. Cell. Biol. 2009, 11, 1325–1331. [Google Scholar]
- Wu, M.F.; Liao, C.Y.; Wang, L.Y.; Chang, J.T. The role of Slit-Robo signaling in the regulation of tissue barriers. Tissue Barriers 2017, 5, e1331155. [Google Scholar]
- Marinkovic, M.; Stojanovic-Rundic, S.; Stanojevic, A.; Ostojic, M.; Gavrilovic, D.; Jankovic, R.; Maksimovic, N.; Stroggilos, R.; Zoidakis, J.; Castellví-Bel, S.; et al. Exploring novel genetic and hematological predictors of response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer. Front. Genet. 2023, 14, 1245594. [Google Scholar] [PubMed]
- Lodge, K.M.; Cowburn, A.S.; Li, W.; Condliffe, A.M. The impact of hypoxia on neutrophil degranulation and consequences for the host. Int. J. Mol. Sci. 2020, 21, 1183. [Google Scholar] [PubMed]
- Li, C.F.; He, H.L.; Wang, J.Y.; Huang, H.Y.; Wu, T.F.; Hsing, C.H.; Lee, S.W.; Lee, H.H.; Fang, J.L.; Huang, W.T.; et al. Fibroblast growth factor receptor 2 overexpression is predictive of poor prognosis in rectal cancer patients receiving neoadjuvant chemoradiotherapy. J. Clin. Pathol. 2014, 67, 1056–1061. [Google Scholar] [PubMed]
- Gillespie, M.; Jassal, B.; Stephan, R.; Milacic, M.; Rothfels, K.; Senff-Ribeiro, A.; Griss, J.; Sevilla, C.; Matthews, L.; Gong, C.; et al. The reactome pathway knowledgebase 2022. Nucleic Acids Res. 2022, 50, D687–D692. [Google Scholar] [PubMed]
- Shi, J.; Zhang, Y.; Yao, B.; Sun, P.; Hao, Y.; Piao, H.; Zhao, X. Role of exosomes in the progression, diagnosis, and treatment of gliomas. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924023-1–e924023-16. [Google Scholar] [CrossRef]
- Nobili, S.; Napoli, C.; Landini, I.; Morganti, M.; Cianchi, F.; Valanzano, R.; Tonelli, F.; Cortesini, C.; Mazzei, T.; Mini, E. Identification of potential pharmacogenomic markers of clinical efficacy of 5-fluorouracil in colorectal cancer. Int. J. Cancer 2011, 128, 1935–1945. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.H.; Iyer, V.R. Global identification of Myc target genes reveals its direct role in mitochondrial biogenesis and its E-box usage in vivo. PLoS ONE 2008, 3, e1798. [Google Scholar]
- Aviv, A.; Anderson, J.J.; Shay, J.W. Mutations, Cancer and the Telomere Length Paradox. Trends Cancer 2017, 3, 253–258. [Google Scholar]
- Gallicchio, L.; Gadalla, S.M.; Murphy, J.D.; Simonds, N.I. The Effect of Cancer Treatments on Telomere Length: A Systematic Review of the Literature. JNCI J. Natl. Cancer Inst. 2018, 110, 1048–1058. [Google Scholar]
- Zou, Z.; Tao, T.; Li, H.; Zhu, X. MTOR signaling pathway and mTOR inhibitors in cancer: Progress and challenges. Cell Biosci. 2020, 10, 1–11. [Google Scholar]
- Schieber, M.; Chandel, N.S. ROS function in redox signaling and oxidative stress. Curr. Biol. 2014, 24, R453–R462. [Google Scholar]
- Vuletić, A.; Mirjačić Martinović, K.; Tišma Miletić, N.; Zoidakis, J.; Castellvi-Bel, S.; Čavić, M. Cross-Talk Between Tumor Cells Undergoing Epithelial to Mesenchymal Transition and Natural Killer Cells in Tumor Microenvironment in Colorectal Cancer. Front. Cell. Dev. Biol. 2021, 9, 750022. [Google Scholar]
- Anufrieva, K.S.; Shender, V.O.; Arapidi, G.P.; Pavlyukov, M.S.; Shakhparonov, M.I.; Shnaider, P.V.; Butenko, I.O.; Lagarkova, M.A.; Govorun, V.M. Therapy-induced stress response is associated with downregulation of pre-mRNA splicing in cancer cells. Genome Med. 2018, 10, 49. [Google Scholar] [PubMed]
- Herskind, C.; Fleckenstein, K.; Lohr, J.; Li, C.Y.; Wenz, F.; Lohr, F. Antitumorale wirkung von interferonen und interleukinen in kombination mit strahlentherapie. Teil II: Strahlenbiologische und immunologische strategien. Strahlenther. Onkol. 2004, 180, 331. [Google Scholar]
- Gray, M.A.; Stanczak, M.A.; Mantuano, N.R.; Xiao, H.; Pijnenborg, J.F.A.; Malaker, S.A.; Miller, C.L.; Weidenbacher, P.A.; Tanzo, J.T.; Ahn, G.; et al. Targeted glycan degradation potentiates the anticancer immune response in vivo. Nat. Chem. Biol. 2020, 16, 1376–1384. [Google Scholar] [CrossRef]
- Dong, X.; Luo, Z.; Wang, Y.; Meng, L.; Duan, Q.; Qiu, L.; Peng, F.; Shen, L. Altered O-glycosylation is associated with inherent radioresistance and malignancy of human laryngeal carcinoma. Exp. Cell. Res. 2018, 362, 302–310. [Google Scholar] [CrossRef]
- Park, T. Crk and CrkL as Therapeutic Targets for Cancer Treatment. Cells 2021, 10, 739. [Google Scholar] [CrossRef]
- Xie, W.; Qu, L.; Meng, L.; Liu, C.; Wu, J.; Shou, C. PES1 regulates sensitivity of colorectal cancer cells to anticancer drugs. Biochem. Biophys. Res. Commun. 2013, 431, 460–465. [Google Scholar] [CrossRef]
- Cristóbal, I.; Manso, R.; Rincón, R.; Caramés, C.; Senin, C.; Borrero, A.; Martínez-Useros, J.; Rodriguez, M.; Zazo, S.; Aguilera, O.; et al. PP2A inhibition is a common event in colorectal cancer and its restoration using FTY720 shows promising therapeutic potential. Mol. Cancer Ther. 2014, 13, 938–947. [Google Scholar] [CrossRef]
- Masuda, H.; Baggerly, K.A.; Wang, Y.; Zhang, Y.; Gonzalez-Angulo, A.M.; Meric-Bernstam, F.; Valero, V.; Lehmann, B.D.; Pietenpol, J.A.; Hortobagyi, G.N.; et al. Differential Response to Neoadjuvant Chemotherapy among 7 Triple-Negative Breast Cancer Molecular Subtypes. Clin. Cancer Res. 2013, 19, 5533–5540. [Google Scholar] [CrossRef]
- Waitz, R.; Solomon, S.B.; Petre, E.N.; Trumble, A.E.; Fassò, M.; Norton, L.; Allison, J.P. Potent induction of tumor immunity by combining tumor cryoablation with anti-CTLA-4 therapy. Cancer Res. 2012, 72, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Cha, M.-K.; Kim, I.-H. Preferential overexpression of glutaredoxin3 in human colon and lung carcinoma. Cancer Epidemiol. 2009, 33, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Qian, L.; Lai, X.; Gu, B.; Sun, X. An Immune-Related Gene Signature for Predicting Neoadjuvant Chemoradiotherapy Efficacy in Rectal Carcinoma. Front. Immunol. 2022, 13, 784479. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Brierley, J.; Byrd, D.; Bosman, F.; Kehoe, S.; Kossary, C.; Piñeros, M.; Van Eycken, E.; Weir, H.K.; Gospodarowicz, M. The TNM classification of malignant tumours—Towards common understanding and reasonable expectations. Lancet Oncol. 2017, 18, 849–851. [Google Scholar] [CrossRef] [PubMed]
- Landberg, T.; Chavaudra, J.; Dobbs, J.; Hanks, G.; Johansson, K.A.; Möller, T. Report 50. J. Int. Comm. Radiat. Units Meas. 2016, 26. [Google Scholar] [CrossRef]
- Landberg, T.; Chavaudra, J.; Dobbs, J.; Gerard, J.P.; Hanks, G.; Horiot, J.C. Report 62. J. Int. Comm. Radiat. Units Meas. 2016, 32. [Google Scholar] [CrossRef]
- Thies, S.; Langer, R. Tumor regression grading of gastrointestinal carcinomas after neoadjuvant treatment. Front. Oncol. 2013, 3, 262. [Google Scholar] [CrossRef]
- Perez-Riverol, Y.; Bai, J.; Bandla, C.; García-Seisdedos, D.; Hewapathirana, S.; Kamatchinathan, S.; Kundu, D.J.; Prakash, A.; Frericks-Zipper, A.; Eisenacher, M.; et al. The PRIDE database resources in 2022: A hub for mass spectrometry-based proteomics evidences. Nucleic Acids Res. 2022, 50, D543–D552. [Google Scholar] [CrossRef]
- Deutsch, E.W.; Bandeira, N.; Perez-Riverol, Y.; Sharma, V.; Carver, J.J.; Mendoza, L.; Kundu, D.J.; Wang, S.; Bandla, C.; Kamatchinathan, S.; et al. The ProteomeXchange consortium at 10 years: 2023 update. Nucleic Acids Res. 2023, 51, D1539–D1548. [Google Scholar] [CrossRef]
- Fekete, J.T.; Győrffy, B. ROCplot.org: Validating predictive biomarkers of chemotherapy/hormonal therapy/anti-HER2 therapy using transcriptomic data of 3,104 breast cancer patients. Int. J. Cancer 2019, 145, 3140–3151. [Google Scholar] [CrossRef]
- El Khouli, R.H.; Macura, K.J.; Barker, P.B.; Habba, M.R.; Jacobs, M.A.; Bluemke, D.A. Relationship of temporal resolution to diagnostic performance for dynamic contrast enhanced MRI of the breast. J. Magn. Reson. Imaging 2009, 30, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Birkbak, N.J.; Gyorffy, B.; Szallasi, Z.; Eklund, A.C. Jetset: Selecting the Optimal Microarray Probe Set to Represent a Gene. 2011. Available online: http://www.biomedcentral.com/1471-2105/12/474 (accessed on 2 May 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Genes | Gene Name | Biological Function | FOLD Change | Mann–Whitney Test p-Value | AUC | ROC p-Value |
|---|---|---|---|---|---|---|
| CRKL | CRK-like Proto-Oncogene | Activate the RAS and JUN kinase signaling pathways and transform fibroblasts in a RAS-dependent fashion | 1.4 | 0.0063 | 0.748 | 8.00 × 10−4 |
| LAP3 | Leucine Aminopeptidase 3 | Predicted to enable peptidase activity; involved in proteolysis. | 1.5 | 0.0059 | 0.746 | 9.30 × 10−4 |
| THTPA | Thiamine Triphosphatase | Encodes an enzyme that catalyzes the biosynthesis of thiamine disphophate (vitamin B1) by hydrolysis of thiamine triphosphate | 1.4 | 0.0089 | 0.738 | 1.20 × 10−3 |
| PES1 | Pescadillo Ribosomal Biogenesis Factor 1 | Encodes a nuclear protein that contains a breast-cancer-associated gene 1 (BRCA1) C-terminal interaction domain | 1.2 | 0.0096 | 0.736 | 1.40 × 10−3 |
| PPP2R5E | Protein Phosphatase 2 Regulatory Subunit B’Epsilon | Protein phosphatase 2A is implicated in the negative control of cell growth and division | 1.2 | 0.01 | 0.73 | 1.60 × 10−3 |
| IFI30 | IFI30 Lysosomal Thiol Reductase | This enzyme has an important role in MHC class II-restricted antigen processing | 1.5 | 0.011 | 0.728 | 2.30 × 10−3 |
| C17orf75 | Chromosome 17 Open Reading Frame 75 | Involved in intracellular protein transport and vesicle tethering to Golgi | 1.3 | 0.015 | 0.722 | 3.00 × 10−3 |
| QDPR | Quinoid Dihydropteridine Reductase | This gene encodes the enzyme dihydropteridine reductase, which catalyzes the NADH-mediated reduction of quinonoid dihydrobiopterin | 1.3 | 0.013 | 0.719 | 4.10 × 10−3 |
| RRM2B | Ribonucleotide Reductase Regulatory TP53 Inducible Subunit M2B | This heterotetrameric enzyme catalyzes the conversion of ribonucleoside diphosphates to deoxyribonucleoside diphosphates | 1.3 | 0.016 | 0.719 | 3.60 × 10−3 |
| GLRX | Glutaredoxin | This enzyme highly contributes to the antioxidant defense system | 1.7 | 0.02 | 0.709 | 4.70 × 10−3 |
| USO1 | USO1 Vesicle Transport Factor | Peripheral membrane protein that recycles between the cytosol and the Golgi apparatus during interphase | 1.2 | 0.022 | 0.707 | 6.60 × 10−3 |
| ARAF | A-Raf Proto-Oncogene, Serine/Threonine Kinase | Involved in negative regulation of apoptotic process, regulation of TOR signaling, and regulation of cellular protein metabolic process | 1.2 | 0.024 | 0.706 | 6.80 × 10−3 |
| CTBS | Chitobiase | Lysosomal glycosidase is involved in degradation of asparagine-linked oligosaccharides on glycoproteins | 1.3 | 0.024 | 0.705 | 6.70 × 10−3 |
| SNRPD3 | Small Nuclear Ribonucleoprotein D3 Polypeptide | This gene encodes a core component of the spliceosome, which is a nuclear ribonucleoprotein complex that functions in pre-mRNA splicing | 1.2 | 0.027 | 0.7 | 8.30 × 10−3 |
| Genes | Gene Name | Biological Function | FOLD Change | Mann–Whitney Test p-Value | AUC | ROC p-Value |
|---|---|---|---|---|---|---|
| COPB1 | COPI Coat Complex Subunit Beta 1 | This gene encodes a protein subunit of the coatomer complex to mediate biosynthetic protein transport from the ER via the Golgi up to the trans-Golgi network | 1.1 | 0.0061 | 0.749 | 4.00 × 10−4 |
| MGLL | Monoglyceride Lipase | Catalyzes the conversion of monoacylglycerides to free fatty acids and glycerol, and gene expression may play a role in cancer tumorigenesis and metastasis | 1.3 | 0.0083 | 0.74 | 1.10 × 10−3 |
| HAS1 | Hyaluronan Synthase 1 | Essential to hyaluronan synthesis, it has a structural role in tissue architectures and regulates cell adhesion, migration, and differentiation. | 1.9 | 0.012 | 0.729 | 1.80 × 10−3 |
| TALDO1 | Transaldolase 1 | Transaldolase 1 is a key enzyme of the nonoxidative pentose phosphate pathway, providing ribose-5-phosphate for nucleic acid synthesis and NADPH for lipid biosynthesis. | 1.2 | 0.012 | 0.729 | 2.30 × 10−3 |
| DNAH9 | Dynein Axonemal Heavy Chain 9 | This gene encodes the heavy chain subunit of axonemal dynein, a large multi-subunit molecular motor. | 1.4 | 0.013 | 0.724 | 2.90 × 10−3 |
| KDELR3 | KDEL Endoplasmic Reticulum Protein Retention Receptor 3 | This gene encodes a member of the KDEL endoplasmic reticulum protein retention receptor family | 1.6 | 0.015 | 0.722 | 4.10 × 10−3 |
| HLA-DPB1 | Major Histocompatibility Complex, Class II, DP Beta 1 | It plays a central role in the immune system by presenting peptides derived from extracellular proteins | 1.8 | 0.02 | 0.709 | 5.20 × 10−3 |
| RBP3 | Retinol-binding Protein 3 | Interphotoreceptor retinol-binding protein is found primarily in the interphotoreceptor matrix of the retina between the retinal pigment epithelium and the photoreceptor cells * | 1.8 | 0.022 | 0.708 | 5.30 × 10−3 |
| STAP2 | Signal-transducing Adaptor Family Member 2 | This gene encodes the substrate of breast tumor kinase, an Src-type non-receptor tyrosine kinase | 1.2 | 0.025 | 0.703 | 6.90 × 10−3 |
| Gene | Protein Name Encoded by Gene | Drug | DRUGBANK ID | Drug Type | Usage | Drug Approval Status | Welch t-Test p Value |
|---|---|---|---|---|---|---|---|
| QPRT | Quinolinate Phosphoribosyltransferase | Niacin | DB00627 | B vitamin | Hyperlipidemia, dyslipidemia, hypertriglyceridemia | Approved, investigational, nutraceutical | 4.43 × 10−5 |
| CLCA4 | Chloride Channel Accessory 4 | Talniflumate | DB09295 | Small molecule, CaCC blocker, and Cl−-/HCO3−exchange inhibitor | Cystic fibrosis, chronic obstructive pulmonary disease (COPD), and asthma | Experimental | 1.11 × 10−2 |
| ATG4B | Autophagy-related 4B Cysteine Peptidase | Esomeprazole | DB00736 | Proton pump inhibitor | Gastroesophageal reflux disease (GERD) for gastric protection to prevent recurrence of stomach ulcers or gastric damage | Approved, investigational | 1.89 × 10−4 |
| ATG4B | Nimodipine | DB00393 | Calcium channel blocker | Acts primarily on vascular smooth muscle cells; improves the neurologic outcome following subarachnoid hemorrhage from ruptured intracranial aneurysm. | Approved, investigational | ||
| PTGS2 | Prostaglandin Endoperoxide Synthase 2 | Diclofenac, Acetylsalicylic acid, Ibuprofen, Rofecoxib, Acetaminophen | DB00586, DB00945, DB01050, DB00533, DB00316 | COX inhibitors, anti-inflammatory agents | Therapy for acute and chronic pain and inflammation from a variety of causes | Approved | 2.08 × 10−4 |
| Characteristics | Responders N (%) | Non-Responders N (%) | p-Value * | |
|---|---|---|---|---|
| Gender | Male | 3 (33.3) | 7 (63.6) 4 (36.4) | 0.4 |
| Female | 6 (66.7) | |||
| Age (years) | Mean (SD) | 64.0 (6.7) | 62.4 (10.3) | 1.0 |
| Median (Range) | 66.0 (50–72) | 64.0 (48–83) | ||
| UICC staging | II | 0.0 (0) | 2.0 (18.2) | 0.5 |
| III | 9.0 (100) | 9.0 (81.8) | ||
| Tumor grade | 1 | 7.0 (77.8) | 8.0 (72.7) | 0.8 |
| 2 | 2.0 (22.2) | 3.0 (27.3) | ||
| 3 | 0.0 (0.0) | 0.0 (0.0) | ||
| Tumor localization | Inferior rectum (<5 cm) | 5.0 (55.6) | 9.0 (81.8) | 0.4 |
| Mid rectum (5–10 cm) | 4.0 (44.4) | 2.0 (18.2) | ||
| Superior rectum (>10 cm) | 0.0 (0) | 0.0 (0) | ||
| Acute toxicity | without | 1.0 (12.5) | 2.0 (18.2) | 0.7 |
| with | 8.0 (87.5) | 9.0 (81.8) | ||
| Tumor Regression Grade (TRG) | 1 | 8.0 (88.89) | / | |
| 2 | 1.0 (11.11) | / | ||
| 3 | / | 2.0 (18.18) | ||
| 4 | / | 7.0 (63.64) | ||
| 5 | / | 2.0 (18.18) | ||
| Total | 9 (100) | 11 (100) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanojevic, A.; Samiotaki, M.; Lygirou, V.; Marinkovic, M.; Nikolic, V.; Stojanovic-Rundic, S.; Jankovic, R.; Vlahou, A.; Panayotou, G.; Fijneman, R.J.A.; et al. Data-Independent Acquisition Mass Spectrometry Analysis of FFPE Rectal Cancer Samples Offers In-Depth Proteomics Characterization of the Response to Neoadjuvant Chemoradiotherapy. Int. J. Mol. Sci. 2023, 24, 15412. https://doi.org/10.3390/ijms242015412
Stanojevic A, Samiotaki M, Lygirou V, Marinkovic M, Nikolic V, Stojanovic-Rundic S, Jankovic R, Vlahou A, Panayotou G, Fijneman RJA, et al. Data-Independent Acquisition Mass Spectrometry Analysis of FFPE Rectal Cancer Samples Offers In-Depth Proteomics Characterization of the Response to Neoadjuvant Chemoradiotherapy. International Journal of Molecular Sciences. 2023; 24(20):15412. https://doi.org/10.3390/ijms242015412
Chicago/Turabian StyleStanojevic, Aleksandra, Martina Samiotaki, Vasiliki Lygirou, Mladen Marinkovic, Vladimir Nikolic, Suzana Stojanovic-Rundic, Radmila Jankovic, Antonia Vlahou, George Panayotou, Remond J. A. Fijneman, and et al. 2023. "Data-Independent Acquisition Mass Spectrometry Analysis of FFPE Rectal Cancer Samples Offers In-Depth Proteomics Characterization of the Response to Neoadjuvant Chemoradiotherapy" International Journal of Molecular Sciences 24, no. 20: 15412. https://doi.org/10.3390/ijms242015412
APA StyleStanojevic, A., Samiotaki, M., Lygirou, V., Marinkovic, M., Nikolic, V., Stojanovic-Rundic, S., Jankovic, R., Vlahou, A., Panayotou, G., Fijneman, R. J. A., Castellví-Bel, S., Zoidakis, J., & Cavic, M. (2023). Data-Independent Acquisition Mass Spectrometry Analysis of FFPE Rectal Cancer Samples Offers In-Depth Proteomics Characterization of the Response to Neoadjuvant Chemoradiotherapy. International Journal of Molecular Sciences, 24(20), 15412. https://doi.org/10.3390/ijms242015412