
Comparison and Validation of Rapid Molecular Testing Methods for Theranostic Epidermal Growth Factor Receptor Alterations in Lung Cancer: Idylla versus Digital Droplet PCR

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Sample Inclusion
2.2. Limit of Blank (LoB), Positive Threshold, and Technical Validation Criteria
2.3. Material Limitations and Method Validation
2.3.1. DNA Quantity—Limit of Detection (LOD) and Limit of Quantification (LOQ)
2.3.2. Sample Tumor Content—Limit of Cellularity (LOC)
2.3.3. DNA Quality (Robustness)
2.4. Specificity
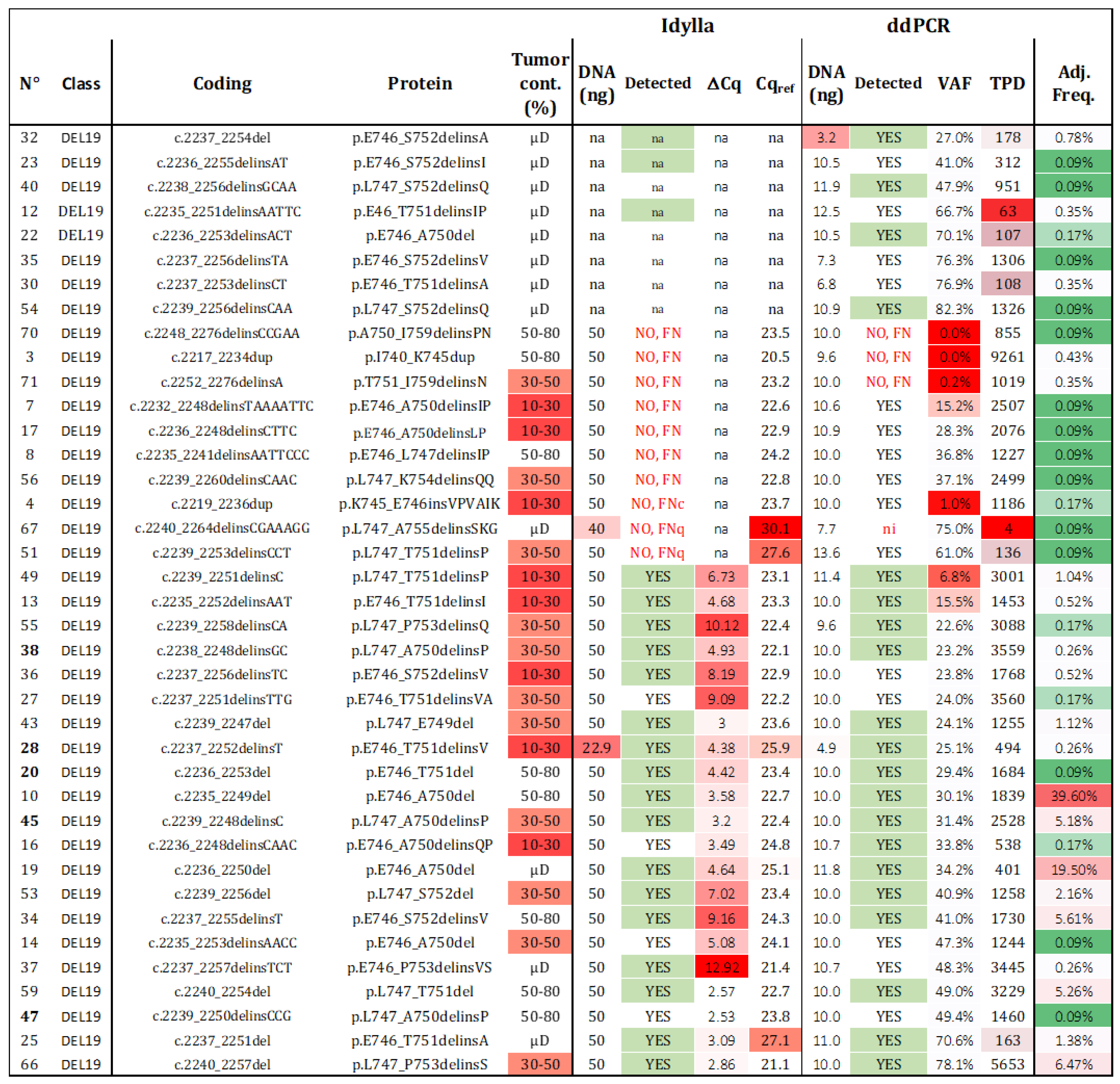
2.5. Sensitivity and Adjusted Sensitivity—Spectra of del19 Detection
3. Discussion
4. Materials and Methods
4.1. Samples
4.2. DNA Extraction and Mutation Analysis
4.3. In Silico Analysis
4.4. Graphs and Statistics
4.5. Cost and Hands-On Time
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, Methods and Major Patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Herbst, R.S.; Heymach, J.V.; Lippman, S.M. Lung Cancer. N. Engl. J. Med. 2008, 359, 1367–1380. [Google Scholar] [CrossRef] [PubMed]
- Debieuvre, D.; Molinier, O.; Falchero, L.; Locher, C.; Templement-Grangerat, D.; Meyer, N.; Morel, H.; Duval, Y.; Asselain, B.; Letierce, A.; et al. Lung Cancer Trends and Tumor Characteristic Changes over 20 Years (2000–2020): Results of Three French Consecutive Nationwide Prospective Cohorts’ Studies. Lancet Reg. Health Eur. 2022, 22, 100492. [Google Scholar] [CrossRef]
- Couraud, S.; Zalcman, G.; Milleron, B.; Morin, F.; Souquet, P.-J. Lung Cancer in Never Smokers—A Review. Eur. J. Cancer 2012, 48, 1299–1311. [Google Scholar] [CrossRef]
- Barlesi, F.; Mazieres, J.; Merlio, J.-P.; Debieuvre, D.; Mosser, J.; Lena, H.; Ouafik, L.; Besse, B.; Rouquette, I.; Westeel, V.; et al. Routine Molecular Profiling of Patients with Advanced Non-Small-Cell Lung Cancer: Results of a 1-Year Nationwide Programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet 2016, 387, 1415–1426. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Heymach, J.V. Co-Occurring Genomic Alterations in Non-Small-Cell Lung Cancer Biology and Therapy. Nat. Rev. Cancer 2019, 19, 495–509. [Google Scholar] [CrossRef]
- Rosell, R.; Karachaliou, N. Large-Scale Screening for Somatic Mutations in Lung Cancer. Lancet 2016, 387, 1354–1356. [Google Scholar] [CrossRef]
- Sharma, S.V.; Bell, D.W.; Settleman, J.; Haber, D.A. Epidermal Growth Factor Receptor Mutations in Lung Cancer. Nat. Rev. Cancer 2007, 7, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin-Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus Standard Chemotherapy as First-Line Treatment for European Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (EURTAC): A Multicentre, Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Yang, J.C.-H.; Lee, C.K.; Kurata, T.; Kim, D.-W.; John, T.; Nogami, N.; Ohe, Y.; Mann, H.; Rukazenkov, Y.; et al. Osimertinib as First-Line Treatment of EGFR Mutation-Positive Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 841–849. [Google Scholar] [CrossRef]
- Hanna, N.H.; Robinson, A.G.; Temin, S.; Baker, S.; Brahmer, J.R.; Ellis, P.M.; Gaspar, L.E.; Haddad, R.Y.; Hesketh, P.J.; Jain, D.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer with Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J. Clin. Oncol. 2021, 39, 1040–1091. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, M.; Herbst, R.S.; John, T.; Kato, T.; Majem, M.; Grohé, C.; Wang, J.; Goldman, J.W.; Lu, S.; Su, W.-C.; et al. Overall Survival with Osimertinib in Resected EGFR-Mutated NSCLC. N. Engl. J. Med. 2023, 389, 137–147. [Google Scholar] [CrossRef]
- Finall, A.; Davies, G.; Jones, T.; Emlyn, G.; Huey, P.; Mullard, A. Integration of Rapid PCR Testing as an Adjunct to NGS in Diagnostic Pathology Services within the UK: Evidence from a Case Series of Non-Squamous, Non-Small Cell Lung Cancer (NSCLC) Patients with Follow-Up. J. Clin. Pathol. 2022, 76, 391–399. [Google Scholar] [CrossRef]
- Lambros, L.; Caumont, C.; Guibourg, B.; Barel, F.; Quintin-Roué, I.; Marcorelles, P.; Merlio, J.P.; Uguen, A. Evaluation of a Fast and Fully Automated Platform to Diagnose EGFR and KRAS Mutations in Formalin-Fixed and Paraffin-Embedded Non-Small Cell Lung Cancer Samples in Less than One Day. J. Clin. Pathol. 2017, 70, 544–549. [Google Scholar] [CrossRef] [PubMed]
- D’Ardia, A.; Caputo, A.; Fumo, R.; Ciaparrone, C.; Gaeta, S.; Picariello, C.; Zeppa, P.; D’Antonio, A. Advanced Non-Small Cell Lung Cancer: Rapid Evaluation of EGFR Status on Fine-Needle Cytology Samples Using Idylla. Pathol. Res. Pract. 2021, 224, 153547. [Google Scholar] [CrossRef] [PubMed]
- Ilie, M.; Butori, C.; Lassalle, S.; Heeke, S.; Piton, N.; Sabourin, J.C.; Tanga, V.; Washetine, K.; Long-Mira, E.; Maitre, P.; et al. Optimization of EGFR Mutation Detection by the Fully-Automated qPCR-Based Idylla System on Tumor Tissue from Patients with Non-Small Cell Lung Cancer. Oncotarget 2017, 8, 103055–103062. [Google Scholar] [CrossRef]
- Sharma, S.; Satapathy, A.; Aggarwal, A.; Dewan, A.; Jain, E.; Katara, R.; Kumar, V.; Pal, R.; Pandey, S.; Naidu, M.M.; et al. Comparison of Epidermal Growth Factor Receptor Mutation Detection Turnaround Times and Concordance among Real-Time Polymerase Chain Reaction, High-Throughput next-Generation Sequencing and the Biocartis IdyllaTM Platforms in Non-Small Cell Lung Carcinomas. Pathol. Res. Pract. 2021, 220, 153394. [Google Scholar] [CrossRef]
- Van Haele, M.; Vander Borght, S.; Ceulemans, A.; Wieërs, M.; Metsu, S.; Sagaert, X.; Weynand, B. Rapid Clinical Mutational Testing of KRAS, BRAF and EGFR: A Prospective Comparative Analysis of the Idylla Technique with High-Throughput next-Generation Sequencing. J. Clin. Pathol. 2020, 73, 35–41. [Google Scholar] [CrossRef]
- Petiteau, C.; Robinet-Zimmermann, G.; Riot, A.; Dorbeau, M.; Richard, N.; Blanc-Fournier, C.; Bibeau, F.; Deshayes, S.; Bergot, E.; Gervais, R.; et al. Contribution of the Idylla(TM) System to Improving the Therapeutic Care of Patients with NSCLC through Early Screening of EGFR Mutations. Curr. Oncol. 2021, 28, 4432–4445. [Google Scholar] [CrossRef]
- Vivancos, A.; Aranda, E.; Benavides, M.; Élez, E.; Gómez-España, M.A.; Toledano, M.; Alvarez, M.; Parrado, M.R.C.; García-Barberán, V.; Diaz-Rubio, E. Comparison of the Clinical Sensitivity of the Idylla Platform and the OncoBEAM RAS CRC Assay for KRAS Mutation Detection in Liquid Biopsy Samples. Sci. Rep. 2019, 9, 8976. [Google Scholar] [CrossRef]
- Franczak, C.; Witz, A.; Geoffroy, K.; Demange, J.; Rouyer, M.; Husson, M.; Massard, V.; Gavoille, C.; Lambert, A.; Gilson, P.; et al. Evaluation of KRAS, NRAS and BRAF Mutations Detection in Plasma Using an Automated System for Patients with Metastatic Colorectal Cancer. PLoS ONE 2020, 15, e0227294. [Google Scholar] [CrossRef]
- Olmedillas-López, S.; García-Arranz, M.; García-Olmo, D. Current and Emerging Applications of Droplet Digital PCR in Oncology. Mol. Diagn. Ther. 2017, 21, 493–510. [Google Scholar] [CrossRef]
- Tsongalis, G.J.; Al Turkmani, M.R.; Suriawinata, M.; Babcock, M.J.; Mitchell, K.; Ding, Y.; Scicchitano, L.; Tira, A.; Buckingham, L.; Atkinson, S.; et al. Comparison of Tissue Molecular Biomarker Testing Turnaround Times and Concordance Between Standard of Care and the Biocartis Idylla Platform in Patients With Colorectal Cancer. Am. J. Clin. Pathol. 2020, 154, 266–276. [Google Scholar] [CrossRef]
- Khalifa, E.; Chapusot, C.; Tournier, B.; Sentis, J.; Marion, E.; Remond, A.; Aubry, M.; Pioche, C.; Bergeron, A.; Primois, C.; et al. Idylla EGFR Assay on Extracted DNA: Advantages, Limits and Place in Molecular Screening According to the Latest Guidelines for Non-Small-Cell Lung Cancer (NSCLC) Patients. J. Clin. Pathol. 2022, 76, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Vessies, D.C.L.; Greuter, M.J.E.; van Rooijen, K.L.; Linders, T.C.; Lanfermeijer, M.; Ramkisoensing, K.L.; Meijer, G.A.; Koopman, M.; Coupé, V.M.H.; Vink, G.R.; et al. Performance of Four Platforms for KRAS Mutation Detection in Plasma Cell-Free DNA: ddPCR, Idylla, COBAS Z480 and BEAMing. Sci. Rep. 2020, 10, 8122. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.; Stanley, A.; Balbi, K.; Gerrard, G.; Bennett, P. Performance Evaluation of the Biocartis Idylla EGFR Mutation Test Using Pre-Extracted DNA from a Cohort of Highly Characterised Mutation Positive Samples. J. Clin. Pathol. 2022, 75, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Kawaguchi, T.; Isa, S.-I.; Ando, M.; Tamiya, A.; Kubo, A.; Saka, H.; Takeo, S.; Adachi, H.; Tagawa, T.; et al. Multiplex Ultrasensitive Genotyping of Patients with Non-Small Cell Lung Cancer for Epidermal Growth Factor Receptor (EGFR) Mutations by Means of Picodroplet Digital PCR. eBioMedicine 2017, 21, 86–93. [Google Scholar] [CrossRef]
- Williamson, D.F.K.; Marris, S.R.N.; Rojas-Rudilla, V.; Bruce, J.L.; Paweletz, C.P.; Oxnard, G.R.; Sholl, L.M.; Dong, F. Detection of EGFR Mutations in Non-Small Cell Lung Cancer by Droplet Digital PCR. PLoS ONE 2022, 17, e0264201. [Google Scholar] [CrossRef]
- Ho, H.-L.; Wang, F.-Y.; Chiang, C.-L.; Tsai, C.-M.; Chiu, C.-H.; Chou, T.-Y. Dynamic Assessment of Tissue and Plasma EGFR-Activating and T790M Mutations with Droplet Digital PCR Assays for Monitoring Response and Resistance in Non-Small Cell Lung Cancers Treated with EGFR-TKIs. Int. J. Mol. Sci. 2022, 23, 11353. [Google Scholar] [CrossRef]
- Garcia, J.; Forestier, J.; Dusserre, E.; Wozny, A.-S.; Geiguer, F.; Merle, P.; Tissot, C.; Ferraro-Peyret, C.; Jones, F.S.; Edelstein, D.L.; et al. Cross-Platform Comparison for the Detection of RAS Mutations in cfDNA (ddPCR Biorad Detection Assay, BEAMing Assay, and NGS Strategy). Oncotarget 2018, 9, 21122–21131. [Google Scholar] [CrossRef] [PubMed]
- De Luca, C.; Gragnano, G.; Pisapia, P.; Vigliar, E.; Malapelle, U.; Bellevicine, C.; Troncone, G. EGFR Mutation Detection on Lung Cancer Cytological Specimens by the Novel Fully Automated PCR-Based Idylla EGFR Mutation Assay. J. Clin. Pathol. 2017, 70, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-S.; Park, J.-H.; Bae, Y.-K. Comparison of Two Digital PCR Methods for EGFR DNA and SARS-CoV-2 RNA Quantification. Clin. Chim. Acta Int. J. Clin. Chem. 2021, 521, 9–18. [Google Scholar] [CrossRef]
- Bocciarelli, C.; Cohen, J.; Pelletier, R.; Tran Van Nhieu, J.; Derman, J.; Favre, L.; Bourgogne, A.; Monnet, I.; Chouaid, C.; Pujals, A. Evaluation of the Idylla System to Detect the EGFR(T790M) Mutation Using Extracted DNA. Pathol. Res. Pract. 2020, 216, 152773. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Garciá, M.; Weynand, B.; Gómez-Izquierdo, L.; Hernández, M.J.; Blanco, Á.M.; Varela, M.; Matias-Guiu, X.; Nadal, E.; Márquez-Lobo, B.; Alarcaõ, A.; et al. Clinical Performance Evaluation of the IdyllaTM EGFR Mutation Test on Formalin-Fixed Paraffin-Embedded Tissue of Non-Small Cell Lung Cancer. BMC Cancer 2020, 20, 275. [Google Scholar] [CrossRef]
- Momeni-Boroujeni, A.; Salazar, P.; Zheng, T.; Mensah, N.; Rijo, I.; Dogan, S.; Yao, J.; Moung, C.; Vanderbilt, C.; Benhamida, J.; et al. Rapid EGFR Mutation Detection Using the Idylla Platform: Single-Institution Experience of 1200 Cases Analyzed by an In-House Developed Pipeline and Comparison with Concurrent Next-Generation Sequencing Results. J. Mol. Diagn. 2021, 23, 310–322. [Google Scholar] [CrossRef]
- Huang, H.; Springborn, S.; Haug, K.; Bartow, K.; Samra, H.; Menon, S.; Mackinnon, A.C. Evaluation, Validation, and Implementation of the Idylla System as Rapid Molecular Testing for Precision Medicine. J. Mol. Diagn. JMD 2019, 21, 862–872. [Google Scholar] [CrossRef]
- Evrard, S.M.; Taranchon-Clermont, E.; Rouquette, I.; Murray, S.; Dintner, S.; Nam-Apostolopoulos, Y.C.; Bellosillo, B.; Varela-Rodriguez, M.; Nadal, E.; Wiedorn, K.H.; et al. Multicenter Evaluation of the Fully Automated PCR-Based Idylla EGFR Mutation Assay on Formalin-Fixed, Paraffin-Embedded Tissue of Human Lung Cancer. J. Mol. Diagn. 2019, 21, 1010–1024. [Google Scholar] [CrossRef]
- Makutani, Y.; Sakai, K.; Yamada, M.; Wada, T.; Chikugo, T.; Satou, T.; Iwasa, Y.; Yamamoto, H.; de Velasco, M.A.; Nishio, K.; et al. Performance of Idylla(TM) RAS-BRAF Mutation Test for Formalin-Fixed Paraffin-Embedded Tissues of Colorectal Cancer. Int. J. Clin. Oncol. 2022, 27, 1180–1187. [Google Scholar] [CrossRef]
- Arcila, M.E.; Yang, S.-R.; Momeni, A.; Mata, D.A.; Salazar, P.; Chan, R.; Elezovic, D.; Benayed, R.; Zehir, A.; Buonocore, D.J.; et al. Ultrarapid EGFR Mutation Screening Followed by Comprehensive Next-Generation Sequencing: A Feasible, Informative Approach for Lung Carcinoma Cytology Specimens With a High Success Rate. JTO Clin. Res. Rep. 2020, 1, 100077. [Google Scholar] [CrossRef]
- Lee, E.; Jones, V.; Topkas, E.; Harraway, J. Reduced Sensitivity for EGFR T790M Mutations Using the Idylla EGFR Mutation Test. J. Clin. Pathol. 2021, 74, 43–47. [Google Scholar] [CrossRef]
- Holm, M.; Andersson, E.; Osterlund, E.; Ovissi, A.; Soveri, L.-M.; Anttonen, A.-K.; Kytölä, S.; Aittomäki, K.; Osterlund, P.; Ristimäki, A. Detection of KRAS Mutations in Liquid Biopsies from Metastatic Colorectal Cancer Patients Using Droplet Digital PCR, Idylla, and next Generation Sequencing. PLoS ONE 2020, 15, e0239819. [Google Scholar] [CrossRef] [PubMed]
- Offerman, S.; Prinsen, C.F.; Knol, A.; Methorst, N.; Kamphorst, J.; Niemantsverdriet, M. Short Report: Performance Evaluation of the IdyllaTM KRAS and EGFR Mutation Tests on Paraffin-Embedded Cytological NSCLC Samples. Diagn. Pathol. 2021, 16, 70. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Jänne, P.A.; Mok, T.; Peters, S. Overcoming Therapy Resistance in EGFR-Mutant Lung Cancer. Nat. Cancer 2021, 2, 377–391. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the cBioPortal. Sci. Signal 2013, 6, pl1. [Google Scholar] [CrossRef]
- De Bruijn, I.; Kundra, R.; Mastrogiacomo, B.; Tran, T.N.; Sikina, L.; Mazor, T.; Li, X.; Ochoa, A.; Zhao, G.; Lai, B.; et al. Analysis and Visualization of Longitudinal Genomic and Clinical Data from the AACR Project GENIE Biopharma Collaborative in cBioPortal. Cancer Res. 2023, online ahead of print. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ddPCR | Idylla | |||
|---|---|---|---|---|
| Technical validation threshold | ≥200 TPDs * | Cqref ≤ 26 | ||
| Limit of blank (LoB) | 1% VAF ** and ≥5 MDs | na | ||
| Limit of detection (LOD) | 0.31 ng | 5 ng | ||
| Limit of quantification (LOQ) | 1.25 ng | 25 ng | ||
| Limit of cellularity (LOC) | 2% (twice the LoB) | 10% (ΔCq unrelated to cellularity) | ||
| Recommended DNA input | 10 ng (up to 1 ng for high TC) | 50 ng (up to 10 ng for high TC) | ||
| Recommended TC input | 10% | 30% | ||
| L858R | del19 | L858R | del19 | |
| Specificity (Spe) | 100% | 100% *** | 100% | 100% |
| Sensitivity (Se) | 100% | 92.3% | 100% | 67.7% |
| Adjusted sensitivity | 100% | 92.58% | 100% | 89.91% |
| Theranostic sensitivity | 96.51% | 95.26% | ||
| Total cost for 1 to 10 analysis | €251 | €150–€114 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Léonce, C.; Guerriau, C.; Chalabreysse, L.; Duruisseaux, M.; Couraud, S.; Brevet, M.; Bringuier, P.-P.; Poncet, D.A. Comparison and Validation of Rapid Molecular Testing Methods for Theranostic Epidermal Growth Factor Receptor Alterations in Lung Cancer: Idylla versus Digital Droplet PCR. Int. J. Mol. Sci. 2023, 24, 15684. https://doi.org/10.3390/ijms242115684
Léonce C, Guerriau C, Chalabreysse L, Duruisseaux M, Couraud S, Brevet M, Bringuier P-P, Poncet DA. Comparison and Validation of Rapid Molecular Testing Methods for Theranostic Epidermal Growth Factor Receptor Alterations in Lung Cancer: Idylla versus Digital Droplet PCR. International Journal of Molecular Sciences. 2023; 24(21):15684. https://doi.org/10.3390/ijms242115684
Chicago/Turabian StyleLéonce, Camille, Clémence Guerriau, Lara Chalabreysse, Michaël Duruisseaux, Sébastien Couraud, Marie Brevet, Pierre-Paul Bringuier, and Delphine Aude Poncet. 2023. "Comparison and Validation of Rapid Molecular Testing Methods for Theranostic Epidermal Growth Factor Receptor Alterations in Lung Cancer: Idylla versus Digital Droplet PCR" International Journal of Molecular Sciences 24, no. 21: 15684. https://doi.org/10.3390/ijms242115684
APA StyleLéonce, C., Guerriau, C., Chalabreysse, L., Duruisseaux, M., Couraud, S., Brevet, M., Bringuier, P. -P., & Poncet, D. A. (2023). Comparison and Validation of Rapid Molecular Testing Methods for Theranostic Epidermal Growth Factor Receptor Alterations in Lung Cancer: Idylla versus Digital Droplet PCR. International Journal of Molecular Sciences, 24(21), 15684. https://doi.org/10.3390/ijms242115684