

Toxicity Derived from Interaction between Natural Compounds and Cancer Therapeutic Drugs Metabolized by CYP3A4: Lessons Learned from Two Clinical Case Reports



Abstract
:1. Introduction
2. Detailed Case Description: Case Reports, Dietary Supplements, and Drug–Natural Compound Interactions
2.1. Case Report 1
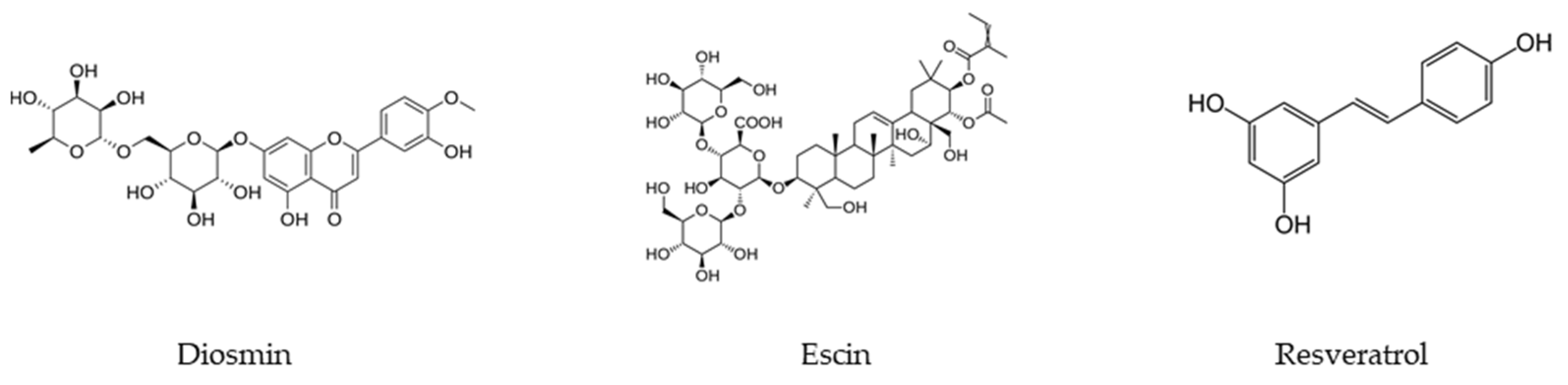
2.1.1. Dietary Supplement and Natural Compounds
2.1.2. Antineoplastic Agents and CYP3A4 Metabolism
2.1.3. Drug–Natural Compound Interactions: CYP3A4 Inhibition
2.1.4. Actions Taken
2.2. Case Report 2
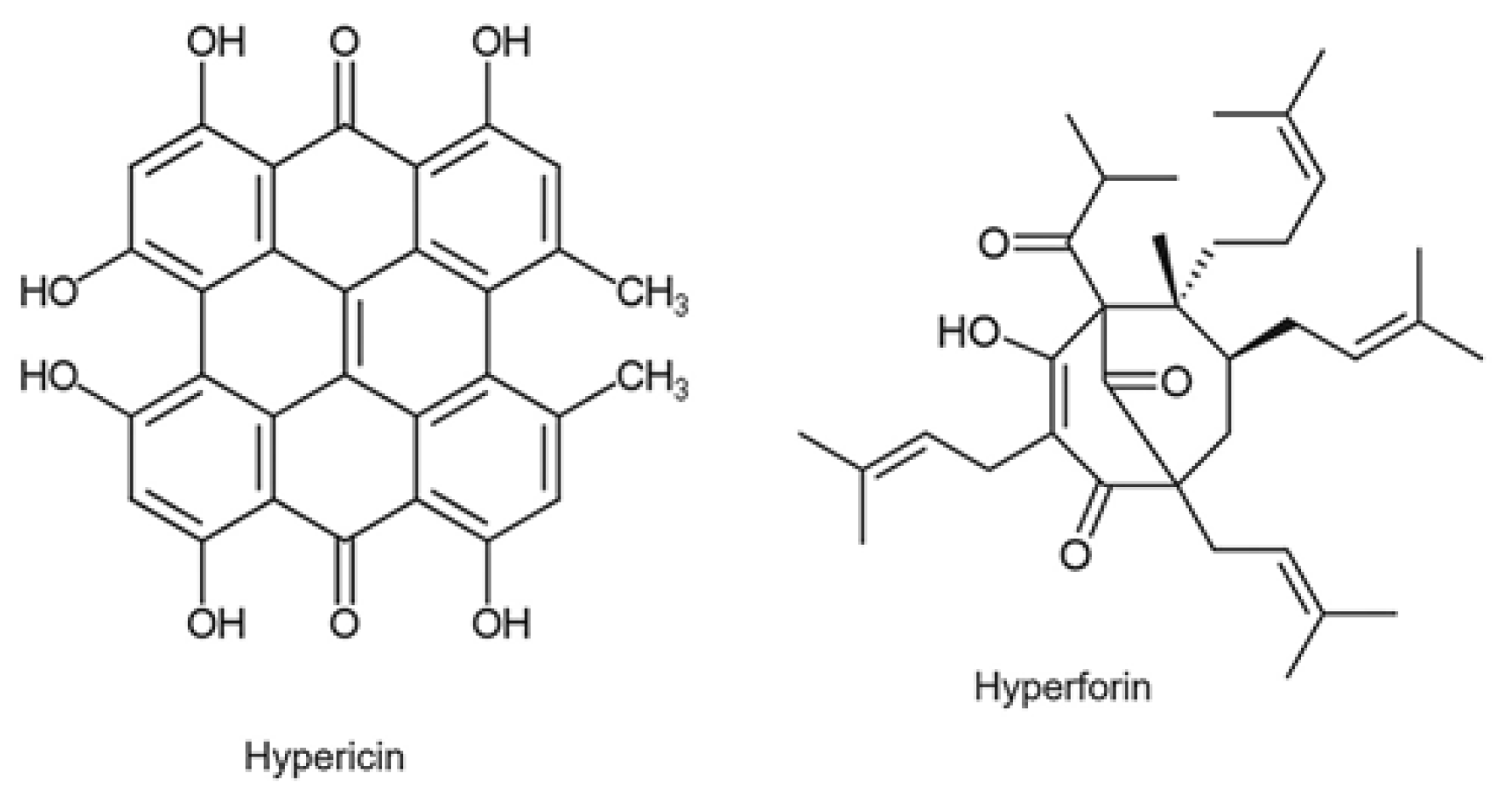
2.2.1. Dietary Supplement and Natural Compounds
2.2.2. Antineoplastic Agents and CYP3A4 Metabolism
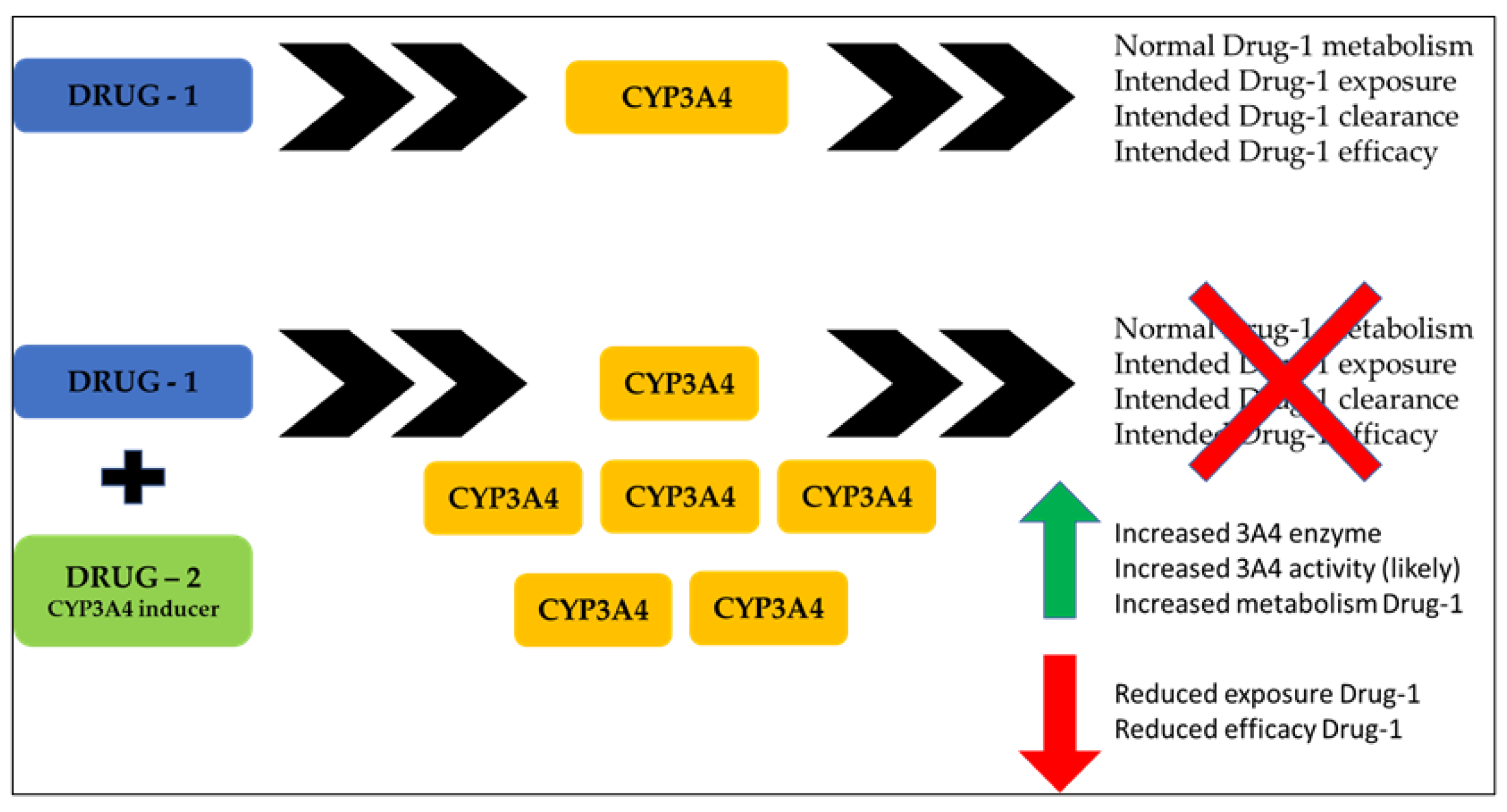
2.2.3. Drug–Natural Compound Interactions: CYP3A4 Inhibition
2.2.4. Actions Taken
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shaw, D.; Graeme, L.; Pierre, D.; Elizabeth, W.; Kelvin, C. Pharmacovigilance of herbal medicine. J. Ethnopharmacol. 2012, 140, 513–518. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [PubMed]
- Fillon, M. Clinicians need to stay current with polypharmacy concerns. CA A Cancer J. Clin. 2023, 73, 341–343. [Google Scholar] [CrossRef]
- Mohamed, M.R.; Mohile, S.G.; Juba, K.M.; Awad, H.; Wells, M.; Loh, K.P.; Flannery, M.; Culakova, E.; Tylock, R.G.; Ramsdale, E.E. Association of polypharmacy and potential drug-drug interactions with adverse treatment outcomes in older adults with advanced cancer. Cancer 2023, 129, 1096–1104. [Google Scholar] [CrossRef] [PubMed]
- Barak, R.; Waissengrin, B.; Wolf, I. Less Is More: Polypharmacy at the End of Life. Isr. Med. Assoc. J. 2021, 23, 452–453. [Google Scholar] [PubMed]
- Novak, J.; Goldberg, A.; Dharmarajan, K.; Amini, A.; Maggiore, R.J.; Presley, C.J.; Nightingale, G. Polypharmacy in older adults with cancer undergoing radiotherapy: A review. J. Geriatr. Oncol. 2022, 13, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Krečak, I.; Pivac, L.; Lucijanić, M.; Skelin, M. Polypharmacy, Potentially Inappropriate Medications, and Drug-to-Drug Interactions in Patients with Chronic Myeloproliferative Neoplasms. Biomedicines 2023, 11, 1301. [Google Scholar] [CrossRef]
- Ramsdale, E.; Mohamed, M.; Yu, V.; Otto, E.; Juba, K.; Awad, H.; Moorthi, K.; Plumb, S.; Patil, A.; Vogelzang, N.; et al. Polypharmacy, Potentially Inappropriate Medications, and Drug-Drug Interactions in Vulnerable Older Adults with Advanced Cancer Initiating Cancer Treatment. Oncologist 2022, 27, e580–e588. [Google Scholar] [CrossRef]
- Choudhury, A.; Singh, P.A.; Bajwa, N.; Dash, S.; Bisht, P. Pharmacovigilance of herbal medicines: Concerns and future prospects. J. Ethnopharmacol. 2023, 309, 116383. [Google Scholar] [CrossRef]
- Turner, J.P.; McKinnon, R.A.; Bell, J.S. The Management of Polypharmacy in People with Cancer and Chronic Conditions. In Cancer and Chronic Conditions; Koczwara, B., Ed.; Springer: Singapore, 2016. [Google Scholar] [CrossRef]
- Vrijkorte, E.; Vries, J.; Schaafsma, R.; Wymenga, M.; Munnink, T.O. Optimising pharmacotherapy in older cancer patients with polypharmacy. Eur. J. Cancer Care 2020, 29, e13185. [Google Scholar] [CrossRef]
- Griese-Mammen, N.; Hersberger, K.E.; Messerli, M.; Leikola, S.; Horvat, N.; van Mil, J.W.F.; Kos, M. PCNE definition of medication review: Reaching agreement. Pharm. Weekbl. 2018, 40, 1199–1208. [Google Scholar] [CrossRef]
- PCNE Position Paper on Medication Review. Available online: https://www.pcne.org/upload/files/149_Position_Paper_on_PCNE_Medication_Review_final.pdf (accessed on 8 September 2023).
- Zaij, S.; Maia, K.P.; Leguelinel-Blache, G.; Roux-Marson, C.; Kinowski, J.M.; Richard, H. Intervention of pharmacist included in multidisciplinary team to reduce adverse drug event: A qualitative systematic review. BMC Health Serv. Res. 2023, 23, 927. [Google Scholar] [CrossRef] [PubMed]
- Whitman, A.; Erdeljac, P.; Jones, C.; Pillarella, N.; Nightingale, G. Managing Polypharmacy in Older Adults with Cancer across Different Healthcare Settings. Drug Health Patient Saf. 2021, 13, 101–116. [Google Scholar] [CrossRef]
- Medication Review in the NHS, England. Available online: https://www.england.nhs.uk/primary-care/pharmacy/smr/ (accessed on 8 September 2023).
- Rose, O.; Cheong, V.-L.; Dhaliwall, S.; Eislage, K.; Erzkamp, S.; Jorgenson, D.; Martínez, F.; Luetsch, K. Standards in medication review: An international perspective. Can. Pharm. J. Rev. Pharm. Can. 2020, 153, 215–223. [Google Scholar] [CrossRef]
- Mackler, E.R.; Azar, M.K.; Johengen, E.; Farris, K.B.; Thompson, A.N. Feasibility of a comprehensive medication review to improve medication use for patients with cancer and comorbid conditions. Support. Care Cancer 2022, 30, 10111–10116. [Google Scholar] [CrossRef] [PubMed]
- Whitman, A.M.; DeGregory, K.A.; Morris, A.L.; Ramsdale, E.E. A Comprehensive Look at Polypharmacy and Medication Screening Tools for the Older Cancer Patient. Oncologist 2016, 21, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Kvarnström, K.; Niittynen, I.; Kallio, S.; Lindén-Lahti, C.; Airaksinen, M.; Schepel, L. Developing an In-House Comprehensive Medication Review Training Program for Clinical Pharmacists in a Finnish Hospital Pharmacy. Int. J. Environ. Res. Public Health 2023, 20, 6158. [Google Scholar] [CrossRef]
- Schöttker, B.; Chen, L.-J.; Caspari, R.; Brenner, H. Protocol of the OPTIMAL study: Optimization of polypharmacy in geriatric oncology—A randomized controlled trial. BMC Cancer 2023, 23, 357. [Google Scholar] [CrossRef]
- HDI Highlighter Opensource Software. Available online: https://github.com/ancnudde/hdi_highlighter (accessed on 30 October 2023).
- Cnudde, A.; Watrin, P.; Souard, F. HDI Highlighter, The First Intelligent Tool to Screen the Literature on Herb–Drug Interactions. Clin. Pharmacokinet. 2022, 61, 761–788. [Google Scholar] [CrossRef]
- Gougis, P.; Hilmi, M.; Geraud, A.; Mir, O.; Funck-Brentano, C. Potential cytochrome P450-mediated pharmacokinetic interactions between herbs, food, and dietary supplements and cancer treatments. Crit. Rev. Oncol. 2021, 166, 103342. [Google Scholar] [CrossRef]
- Chan, W.-J.J.; Adiwidjaja, J.; McLachlan, A.J.; Boddy, A.V.; Harnett, J.E. Interactions between natural products and cancer treatments: Underlying mechanisms and clinical importance. Cancer Chemother. Pharmacol. 2023, 91, 103–119. [Google Scholar] [CrossRef] [PubMed]
- Orzetti, S.; Tommasi, F.; Bertola, A.; Bortolin, G.; Caccin, E.; Cecco, S.; Ferrarin, E.; Giacomin, E.; Baldo, P. Genetic Therapy and Molecular Targeted Therapy in Oncology: Safety, Pharmacovigilance, and Perspectives for Research and Clinical Practice. Int. J. Mol. Sci. 2022, 23, 3012. [Google Scholar] [CrossRef]
- Huwait, E.; Mobashir, M. Potential and Therapeutic Roles of Diosmin in Human Diseases. Biomedicines 2022, 10, 1076. [Google Scholar] [CrossRef] [PubMed]
- Gerges, S.H.; Wahdan, S.A.; Elsherbiny, D.A.; El-Demerdash, E. Pharmacology of Diosmin, a Citrus Flavone Glycoside: An Updated Review. Eur. J. Drug Metab. Pharmacokinet. 2021, 47, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Enciclopedia Humanitas. Available online: https://www.humanitas-care.it/enciclopedia/integratori-alimentari/escina/ (accessed on 27 June 2023).
- Dudek-Makuch, M.; Studzińska-Sroka, E. Horse chestnut–efficacy and safety in chronic venous insufficiency: An overview. Rev. Bras. Farm. 2015, 25, 533–541. [Google Scholar] [CrossRef]
- Salehi, B.; Mishra, A.P.; Nigam, M.; Sener, B.; Kilic, M.; Sharifi-Rad, M.; Fokou, P.V.T.; Martins, N.; Sharifi-Rad, J. Resveratrol: A Double-Edged Sword in Health Benefits. Biomedicines 2018, 6, 91. [Google Scholar] [CrossRef]
- Enciclopedia Humanitas. Available online: https://www.humanitas.it/enciclopedia/integratori-alimentari/resveratrolo/#:~:text=Il%20resveratrolo%20%C3%A8%20una%20sostanza,patogeni%20come%20batteri%20o%20funghi (accessed on 27 June 2023).
- Clinical Pharmacology. School of Medicine. Available online: https://drug-interactions.medicine.iu.edu/MainTable.aspx (accessed on 27 June 2023).
- Lexicomp® Database. Available online: https://online.lexi.com/lco/action/home (accessed on 26 September 2023).
- EMA—European Medicine Agency. Available online: https://www.ema.europa.eu/en/documents/product-information/kisqali-epar-product-information_it.pdf (accessed on 26 September 2023).
- AIFA—Agenzia Italiana del Farmaco. Available online: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_003230_040233_RCP.pdf&sys=m0b1l3 (accessed on 27 June 2023).
- Burkina, V.; Zlabek, V.; Halsne, R.; Ropstad, E.; Zamaratskaia, G. In vitro effects of the citrus flavonoids diosmin, naringenin and naringin on the hepatic drug-metabolizing CYP3A enzyme in human, pig, mouse and fish. Biochem. Pharmacol. 2016, 110–111, 109–116. [Google Scholar] [CrossRef]
- Yoo, H.H.; Lee, M.; Chung, H.J.; Lee, S.K.; Kim, D.H. Effects of diosmin, a flavonoid glycoside in citrus fruits, on P-glycoprotein-mediated drug efflux in human intestinal Caco-2 cells. J. Agric. Food Chem. 2007, 55, 7620–7625. [Google Scholar] [CrossRef]
- Bedada, S.K.; Neerati, P. Modulation of CYP3A enzyme activity by diosmin and its consequence on carbamazepine pharmacokinetics in rats. Naunyn-Schmiedebergs Arch. Pharmacol. 2018, 391, 115–121. [Google Scholar] [CrossRef]
- Bedada, S.K.; Boga, P.K. Influence of diosmin on the metabolism and disposition of carbamazepine in healthy subjects. Xenobiotica 2016, 47, 879–884. [Google Scholar] [CrossRef]
- Hellum, B.H.; Nilsen, O.G. In vitro Inhibition of CYP3A4 Metabolism and P-Glycoprotein-Mediated Transport by Trade Herbal Products. Basic Clin. Pharmacol. Toxicol. 2008, 102, 466–475. [Google Scholar] [CrossRef] [PubMed]
- Spanakis, M.; Vizirianakis, I.S.; Mironidou-Tzouveleki, M.; Niopas, I. In vitro inhibition of CYP3A4 and CYP2D6 activity by the horse chestnut constituents’ aescin and aesculetin. In Proceedings of the 8th Southeast European Congress on Xenobiotic Metabolism and Toxicity—XEMET 2010, Thessaloniki, Greece, 1–5 October 2010. [Google Scholar] [CrossRef]
- Huang, Y.; Zheng, S.-L.; Zhu, H.-Y.; Xu, Z.-S.; Xu, R.-A. Effects of aescin on cytochrome P450 enzymes in rats. J. Ethnopharmacol. 2014, 151, 583–590. [Google Scholar] [CrossRef]
- Choi, J.S.; Choi, B.C.; Kang, K.W. Effect of resveratrol on the pharmacokinetics of oral and intravenous nicardipine in rats: Possible role of P-glycoprotein inhibition by resveratrol. Pharm. Int. J. Pharm. Sci. 2009, 64, 49–52. [Google Scholar]
- Hong, S.-P.; Choi, D.-H.; Choi, J.-S. Effects of Resveratrol on the Pharmacokinetics of Diltiazem and Its Major Metabolite, Desacetyldiltiazem, in Rats. Cardiovasc. Ther. 2008, 26, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Piver, B.; Berthou, F.; Dreano, Y.; Lucas, D. Inhibition of CYP3A, CYP1A and CYP2E1 activities by resveratrol and other non volatile red wine components. Toxicol. Lett. 2001, 125, 83–91. [Google Scholar] [CrossRef]
- Zhou, Z.W.; Zhou, S.F. Application of mechanism-based CYP inhibition for predicting drug-drug interactions. Expert Opin. Drug Metab. Toxicol. 2009, 5, 579–605. [Google Scholar] [CrossRef]
- Basheer, L.; Schultz, K.; Kerem, Z. Inhibition of cytochrome P450 3A by acetoxylated analogues of resveratrol in in vitro and in silico models. Sci. Rep. 2016, 6, 31557. [Google Scholar] [CrossRef] [PubMed]
- Detampel, P.; Beck, M.; Krähenbühl, S.; Huwyler, J. Drug interaction potential of resveratrol. Drug Metab. Rev. 2012, 44, 253–265. [Google Scholar] [CrossRef]
- Chow, S.; Garland, L.; Hsu, C.H.; Vining, D.R.; Chew, W.M.; Miller, J.A.; Perloff, M.; Crowell, J.A.; Alberts, D.S. Resveratrol Modulates Drug- and Carcinogen-Metabolizing Enzymes in a Healthy Volunteer Study. Cancer Prev. Res. 2010, 3, 1168–1175. [Google Scholar] [CrossRef]
- VigiErbe. Sistema di Fitovigilanza dell’Istituto Superiore di Sanità. Available online: https://www.vigierbe.it/ (accessed on 9 October 2021).
- Istikoglou, C.I.; Mavreas, V.; Geroulanos, G. History and therapeutic properties of Hypericum Perforatum from antiquity until today. Psychiatriki 2010, 21, 332–338. [Google Scholar]
- Klemow, K.M.; Bartlow, A.; Crawford, J.; Kocher, N.; Shah, J.; Ritsick, M.; Benzie, I.F.F.; Wachtel-Galor, S. Medical Attributes of St. John’s Wort (Hypericum perforatum). In Herbal Medicine: Biomolecular and Clinical Aspects; CRC Press: Boca Raton, FL, USA, 2011; Chapter 11. [Google Scholar]
- NIH—National Center for Complementary and Integrative Health. Available online: https://www.nccih.nih.gov/health/st-johns-wort (accessed on 27 October 2022).
- Mayo Clinic. Available online: https://www.mayoclinic.org/drugs-supplements-st-johns-wort/art-20362212 (accessed on 9 October 2021).
- Ghazizadeh, J.; Sadigh-Eteghad, S.; Marx, W.; Fakhari, A.; Hamedeyazdan, S.; Torbati, M.; Taheri-Tarighi, S.; Araj-Khodaei, M.; Mirghafourvand, M. The effects of lemon balm (Melissa officinalis L.) on depression and anxiety in clinical trials: A systematic review and meta-analysis. Phytother. Res. 2021, 35, 6690–6705. [Google Scholar] [CrossRef]
- Petrisor, G.; Motelica, L.; Craciun, L.N.; Oprea, O.C.; Ficai, D.; Ficai, A. Melissa officinalis: Composition, Pharmacological Effects and Derived Release Systems—A Review. Int. J. Mol. Sci. 2022, 23, 3591. [Google Scholar] [CrossRef]
- EMA/HMPC/310761/2013. Committee on Herbal Medicinal Products (HMPC). Available online: https://www.ema.europa.eu/en/documents/herbal-summary/melissa-leaf-summary-public_en.pdf (accessed on 26 February 2022).
- Lexicomp® Database. Available online: https://online.lexi.com/lco/action/doc/retrieve/docid/multinat_f/4668446?cesid=4TfUeeaoKSW&searchUrl=%2Flco%2Faction%2Fsearch%3Fq%3Dpaclitaxel%26t%3Dname%26acs%3Dtrue%26acq%3Dpacli (accessed on 26 February 2022).
- AIFA—Agenzia Italiana del Farmaco. Available online: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_000829_039399_RCP.pdf&retry=0&sys=m0b1l3 (accessed on 19 June 2023).
- Fasinu, P.S.; Rapp, G.K. Herbal Interaction with Chemotherapeutic Drugs—A Focus on Clinically Significant Findings. Front. Oncol. 2019, 9, 1356. [Google Scholar] [CrossRef] [PubMed]
- Josefson, D. St John’s wort interferes with chemotherapy, study shows. Br. Med. J. 2002, 325, 460. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, G.; Zhu, B.; Wu, J.; Wang, J.; El-Aty, A.M.A.; Li, T.; Liu, J.; Yang, T.; Wang, D.; et al. St John’s wort induces both cytochrome P450 3A4–catalyzed sulfoxidation and 2C19–dependent hydroxylation of omeprazole. Clin. Pharmacol. Ther. 2004, 75, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Mai, I.; Störmer, E.; Bauer, S.; Krüger, H.; Budde, K.; Roots, I. Impact of St John’s wort treatment on the pharmacokinetics of tacrolimus and mycophenolic acid in renal transplant patients. Nephrol. Dial. Transplant. 2003, 18, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Bilia, A.R.; Gallori, S.; Vincieri, F.F. St. John’s wort and depression: Efficacy, safety and tolerability—An update. Life Sci. 2002, 70, 3077–3096. [Google Scholar] [CrossRef]
- Baldo, P.; Fornasier, G.; Ciolfi, L.; Sartor, I.; Francescon, S. Pharmacovigilance in oncology. Pharm. Weekbl. 2018, 40, 832–841. [Google Scholar] [CrossRef]
- Zhang, T.; Zhao, M.; Pang, Y.; Zhang, W.; Liu, L.A.; Wei, D.-Q. Recent progress on bioinformatics, functional genomics, and metabolomics research of cytochrome P450 and its impact on drug discovery. Curr. Top. Med. Chem. 2012, 12, 1346–1355. [Google Scholar] [CrossRef]
- Klein, K.; Zanger, U.M. Pharmacogenomics of Cytochrome P450 3A4: Recent Progress Toward the “Missing Heritability” Problem. Front. Genet. 2013, 4, 12. [Google Scholar] [CrossRef]
- Li, G.; Yi, B.; Liu, J.; Jiang, X.; Pan, F.; Yang, W.; Liu, H.; Liu, Y.; Wang, G. Effect of CYP3A4 Inhibitors and Inducers on Pharmacokinetics and Pharmacodynamics of Saxagliptin and Active Metabolite M2 in Humans Using Physiological-Based Pharmacokinetic Combined DPP-4 Occupancy. Front. Pharmacol. 2021, 12, 746594. [Google Scholar] [CrossRef] [PubMed]
- Samuels, E.R.; Sevrioukova, I. Inhibition of Human CYP3A4 by Rationally Designed Ritonavir-Like Compounds: Impact and Interplay of the Side Group Functionalities. Mol. Pharm. 2018, 15, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.; Choi, C.; Oh, E.S.; Kim, C.O.; Park, K.; Park, M.S. Effect of Rifampicin on the Pharmacokinetics of Evogliptin in Healthy Volunteers. Drug Des. Dev. Ther. 2022, 16, 4301–4310. [Google Scholar] [CrossRef] [PubMed]
- Hukkanen, J. Induction of cytochrome P450 enzymes: A view on human in vivo findings. Expert Rev. Clin. Pharmacol. 2014, 5, 569–585. [Google Scholar] [CrossRef]
- Enciclopedia Humanitas. Available online: https://www.humanitascatania.it/enciclopedia-medica/integratori-alimentari/diosmina/ (accessed on 27 June 2023).




{kind=link}
{kind=link}
{kind=link}
| Types | Example of Agents |
|---|---|
| Inhibitors | escin (Aesculus hippocastanum), amiodarone, azole antifungals, bergamottin, bile acids, chamomile (Matricaria chamomilla L.), cimetidine, curcumin (Curcuma longa L.), cyclosporin, diltiazem. Fluoroquinolone antibiotics, green tea (Camellia sinensis), macrolide antibiotics, peppermint oil (Menta x piperita L.), pomegranate juice (citrus x paradisi), protease inhibitors, resveratrol |
| Strong inducers | carbamazepine, common valerian (Valeriana officinalis), Hyperforin (Hypericum perforatum), glucocorticoids, phenobarbital, phenytoin, rifampicin |
| Substrates | alfentanyl, amiodarone, antihistamines, azole antifungal, amprenavir, benzodiazepines, calcium channel blockers, carbamazepine, codeine, cyclosporine, cyclophosphamide, erythromycin, estradiol, exemestane, HMG-CoA reductase inhibitors, hydrocortisone, imatinib, lidocaine, midazolam, ribociclib, ritonavir, sirolimus, tacrolimus, tamoxifen, testosterone, tricyclic antidepressants |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orzetti, S.; Baldo, P. Toxicity Derived from Interaction between Natural Compounds and Cancer Therapeutic Drugs Metabolized by CYP3A4: Lessons Learned from Two Clinical Case Reports. Int. J. Mol. Sci. 2023, 24, 15976. https://doi.org/10.3390/ijms242115976
Orzetti S, Baldo P. Toxicity Derived from Interaction between Natural Compounds and Cancer Therapeutic Drugs Metabolized by CYP3A4: Lessons Learned from Two Clinical Case Reports. International Journal of Molecular Sciences. 2023; 24(21):15976. https://doi.org/10.3390/ijms242115976
Chicago/Turabian StyleOrzetti, Sabrina, and Paolo Baldo. 2023. "Toxicity Derived from Interaction between Natural Compounds and Cancer Therapeutic Drugs Metabolized by CYP3A4: Lessons Learned from Two Clinical Case Reports" International Journal of Molecular Sciences 24, no. 21: 15976. https://doi.org/10.3390/ijms242115976
APA StyleOrzetti, S., & Baldo, P. (2023). Toxicity Derived from Interaction between Natural Compounds and Cancer Therapeutic Drugs Metabolized by CYP3A4: Lessons Learned from Two Clinical Case Reports. International Journal of Molecular Sciences, 24(21), 15976. https://doi.org/10.3390/ijms242115976