

Role of Nasal Nitric Oxide in Primary Ciliary Dyskinesia and Other Respiratory Conditions in Children

 and
and
Abstract
:1. Introduction
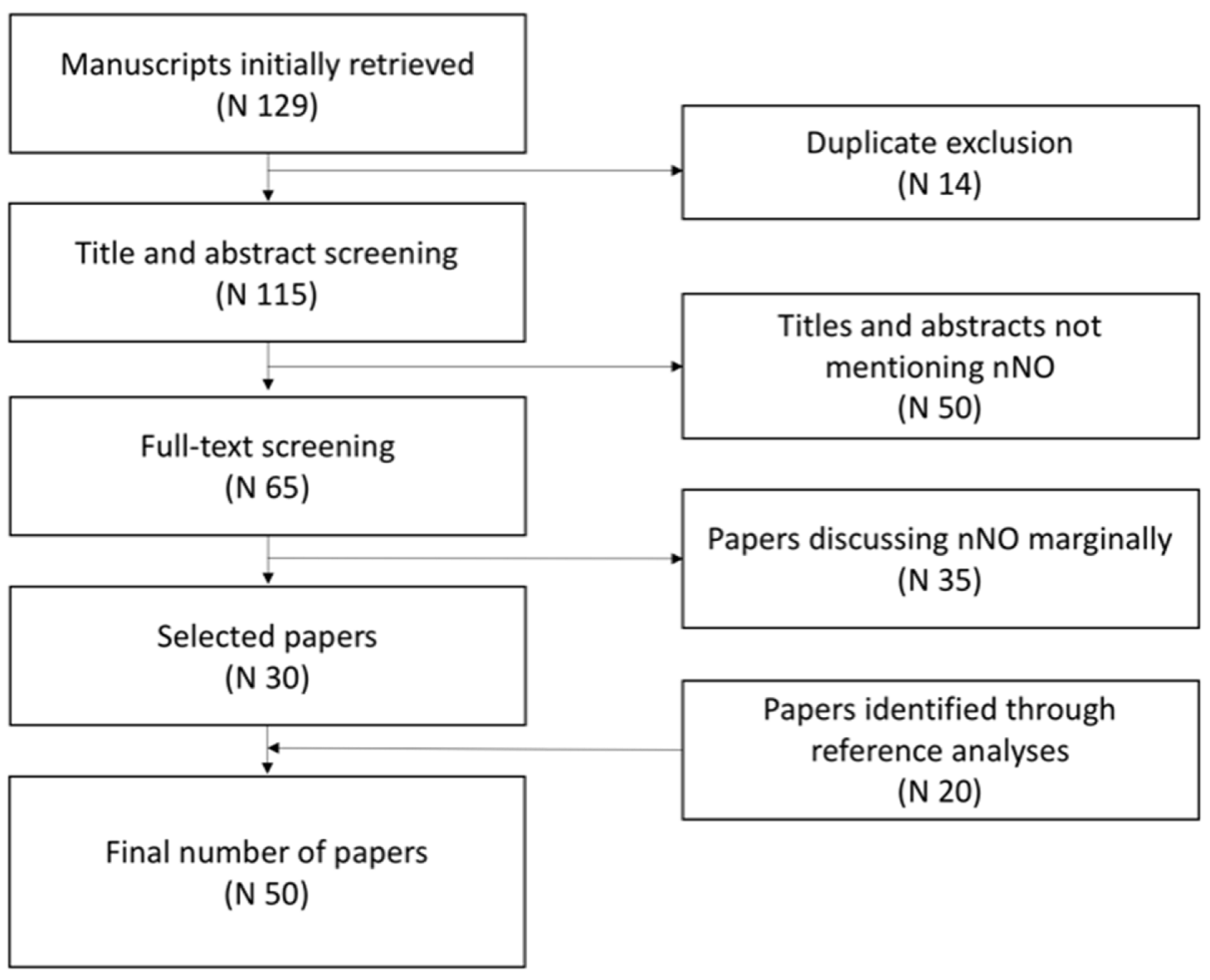
2. Materials and Methods
3. Results and Discussion
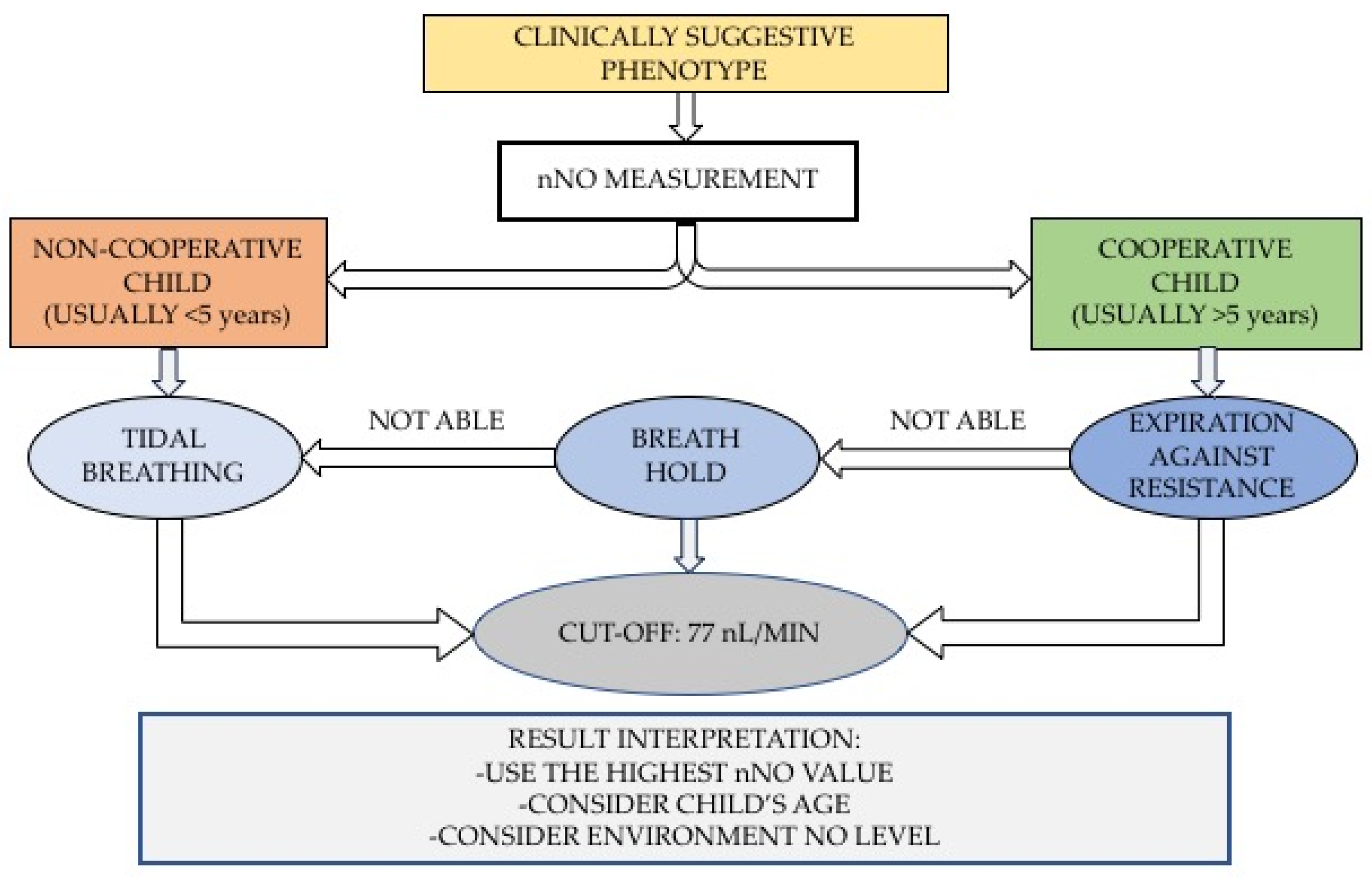
3.1. Measurement Techniques, Devices, and Age Limitations
3.2. nNO in Primary Ciliary Dyskinesia (PCD)
3.2.1. nNO Cut-Off Levels for PCD
3.2.2. Relationship between nNO, Genotypes, and Ciliary Function: A Molecular Focus
3.3. Applications of nNO in Other Respiratory Inflammatory Diseases
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manna, A.; Montella, S.; Maniscalco, M.; Maglione, M.; Santamaria, F. Clinical application of nasal nitric oxide measurement in pediatric airway diseases. Pediatr. Pulmonol. 2015, 50, 85–99. [Google Scholar] [CrossRef]
- Yoshida, K.; Takabayashi, T.; Imoto, Y.; Sakashita, M.; Narita, N.; Fujieda, S. Reduced nasal nitric oxide levels in patients with eosinophilic chronic rhinosinusitis. Allergol. Int. 2019, 68, 225–232. [Google Scholar] [CrossRef]
- American Thoracic Society, European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef]
- Beydon, N.; Kouis, P.; Marthin, J.K.; Latzin, P.; Colas, M.; Davis, S.D.; Haarman, E.; Harris, A.L.; Hogg, C.; Kilbride, E.; et al. Nasal nitric oxide measurement in children for the diagnosis of primary ciliary dyskinesia: European Respiratory Society technical standard. Eur. Respir. J. 2023, 61, 2202031. [Google Scholar] [CrossRef]
- Marthin, J.K.; Philipsen, M.C.; Rosthoj, S.; Nielsen, K.G. Infant nasal nitric oxide over time: Natural evolution and impact of respiratory tract infection. Eur. Respir. J. 2018, 51, 1702503. [Google Scholar] [CrossRef]
- Buechel, F.; Usemann, J.; Aline, A.; Salfeld, P.; Moeller, A.; Jung, A. Feasibility of nasal NO screening in healthy newborns. Pediatr. Pulmonol. 2022, 57, 231–238. [Google Scholar] [CrossRef]
- Adams, P.S.; Tian, X.; Zahid, M.; Khalifa, O.; Leatherbury, L.; Lo, C.W. Establishing normative nasal nitric oxide values in infants. Respir. Med. 2015, 109, 1126–1130. [Google Scholar] [CrossRef]
- O’Callaghan, C.; Chilvers, M.; Hogg, C.; Bush, A.; Lucas, J. Diagnosing primary ciliary dyskinesia. Thorax 2007, 62, 656–657. [Google Scholar] [CrossRef]
- Kartagener, M. Zur pathogenese der bronkiectasien: Bronkiectasien bei situs viscerum inversus. Beitr. Klin. Tuberk. 1933, 82, 489–501. [Google Scholar] [CrossRef]
- Shapiro, A.J.; Josephson, M.; Rosenfeld, M.; Yilmaz, O.; Davis, S.D.; Polineni, D.; Guadagno, E.; Leigh, M.W.; Lavergne, V. Accuracy of Nasal Nitric Oxide Measurement as a Diagnostic Test for Primary Ciliary Dyskinesia. A Systematic Review and Meta-analysis. Ann. Am. Thorac. Soc. 2017, 14, 1184–1196. [Google Scholar] [CrossRef]
- Behan, L.; Dunn Galvin, A.; Rubbo, B.; Masefield, S.; Copeland, F.; Manion, M.; Rindlisbacher, B.; Redfern, B.; Lucas, J.S. Diagnosing primary ciliary dyskinesia: An international patient perspective. Eur. Respir. J. 2016, 48, 1096–1107. [Google Scholar] [CrossRef]
- Gustafsson, L.E.; Leone, A.M.; Persson, M.G.; Wiklund, N.P.; Moncada, S. Endogenous nitric oxide is present in the exhaled air of rabbits, guinea pigs and humans. Biochem. Biophys. Res. Commun. 1991, 181, 852–857. [Google Scholar] [CrossRef]
- Lundberg, J.O.; Weitzberg, E.; Nordvall, S.L.; Kuylenstierna, R.; Lundberg, J.M.; Alving, K. Primarily nasal origin of exhaled nitric oxide and absence in Kartagener’s syndrome. Eur. Respir. J. 1994, 7, 1501–1504. [Google Scholar] [CrossRef]
- Leigh, M.W.; Ferkol, T.W.; Davis, S.D.; Lee, H.S.; Rosenfeld, M.; Dell, S.D.; Sagel, S.D.; Milla, C.; Olivier, K.N.; Sullivan, K.M.; et al. Clinical Features and Associated Likelihood of Primary Ciliary Dyskinesia in Children and Adolescents. Ann. Am. Thorac. Soc. 2016, 13, 1305–1313. [Google Scholar] [CrossRef]
- Behan, L.; Dimitrov, B.D.; Kuehni, C.E.; Hogg, C.; Carroll, M.; Evans, H.J.; Goutaki, M.; Harris, A.; Packham, S.; Walker, W.T.; et al. PICADAR: A diagnostic predictive tool for primary ciliary dyskinesia. Eur. Respir. J. 2016, 47, 1103. [Google Scholar] [CrossRef]
- Lucas, J.S.; Walker, W.T. NO way! Nasal nitric oxide measurement in infants. Eur. Respir. J. 2018, 51, 1800958. [Google Scholar] [CrossRef]
- Schultz, R.; Elenius, V.; Lukkarinen, H.; Saarela, T. Two novel mutations in the DNAH11 gene in primary ciliary dyskinesia (CILD7) with considerable variety in the clinical and beating cilia phenotype. BMC Med. Genet. 2020, 21, 237. [Google Scholar] [CrossRef]
- Leigh, M.W.; Hazucha, M.J.; Chawla, K.K.; Baker, B.R.; Shapiro, A.J.; Brown, D.E.; LaVange, L.M.; Horton, B.J.; Qaqish, B.; Carson, J.L.; et al. Standardizing nasal nitric oxide measurement as a test for primary ciliary dyskinesia. Ann. Am. Thorac. Soc. 2013, 10, 574–581. [Google Scholar] [CrossRef]
- Collins, S.A.; Gove, K.; Walker, W.; Lucas, J.S.A. Nasal nitric oxide screening for primary ciliary dyskinesia: Systematic review and meta-analysis. Eur. Respir. J. 2014, 44, 1589–1599. [Google Scholar] [CrossRef]
- Marthin, J.K.; Nielsen, K.G. Hand-held tidal breathing nasal nitric oxide measurement--a promising targeted case-finding tool for the diagnosis of primary ciliary dyskinesia. PLoS ONE 2013, 8, e57262. [Google Scholar] [CrossRef]
- Marthin, J.K.; Nielsen, K.G. Choice of nasal nitric oxide technique as first-line test for primary ciliary dyskinesia. Eur. Respir. J. 2011, 37, 559–565. [Google Scholar] [CrossRef]
- Mateos-Corral, D.; Coombs, R.; Grasemann, H.; Ratjen, F.; Dell, S.D. Diagnostic value of nasal nitric oxide measured with non-velum closure techniques for children with primary ciliary dyskinesia. J. Pediatr. 2011, 159, 420–424. [Google Scholar] [CrossRef]
- Rybnikar, T.; Senkerik, M.; Chladek, J.; Chladkova, J.; Kalfert, D.; Skoloudik, L. Adenoid hypertrophy affects screening for primary ciliary dyskinesia using nasal nitric oxide. Int. J. Pediatr. Otorhinolaryngol. 2018, 115, 6–9. [Google Scholar] [CrossRef]
- Walker, W.T.; Jackson, C.L.; Coles, J.; Lackie, P.M.; Faust, S.N.; Hall-Stoodley, L.; Lucas, J.S. Ciliated cultures from patients with primary ciliary dyskinesia produce nitric oxide in response to Haemophilus influenzae infection and proinflammatory cytokines. Chest 2014, 145, 668–669. [Google Scholar] [CrossRef]
- Walker, W.T.; Jackson, C.L.; Lackie, P.M.; Hogg, C.; Lucas, J.S. Nitric oxide in primary ciliary dyskinesia. Eur. Respir. J. 2012, 40, 1024–1032. [Google Scholar] [CrossRef]
- Legendre, M.; Thouvenin, G.; Taytard, J.; Baron, M.; Le Bourgeois, M.; Tamalet, A.; Mani, R.; Jouvion, G.; Amselem, S.; Escudier, E.; et al. High Nasal Nitric Oxide, Cilia Analyses, and Genotypes in a Retrospective Cohort of Children with Primary Ciliary Dyskinesia. Ann. Am. Thorac. Soc. 2022, 19, 1704–1712. [Google Scholar] [CrossRef]
- Knowles, M.R.; Ostrowski, L.E.; Leigh, M.W.; Sears, P.R.; Davis, S.D.; Wolf, W.E.; Hazucha, M.J.; Carson, J.L.; Olivier, K.N.; Sagel, S.D.; et al. Mutations in RSPH1 Cause Primary Ciliary Dyskinesia with a Unique Clinical and Ciliary Phenotype. Am. J. Respir. Crit. Care Med. 2014, 189, 707–717. [Google Scholar] [CrossRef]
- Pifferi, M.; Boner, A.L.; Gracci, S.; Fonnesu, R.; Maj, D.; Donzelli, G.; Michelucci, A.; Cangiotti, A.; Bertini, V.; Valetto, A.; et al. Longitudinal Nitric Oxide Levels and Infections by Ultrastructure and Genotype in Primary Ciliary Dyskinesia. Chest 2022, 162, 1265–1276. [Google Scholar] [CrossRef]
- Davis, S.D.; Rosenfeld, M.; Lee, H.S.; Ferkol, T.W.; Sagel, S.D.; Dell, S.D.; Milla, C.; Pittman, J.E.; Shapiro, A.J.; Sullivan, K.M.; et al. Primary Ciliary Dyskinesia: Longitudinal Study of Lung Disease by Ultrastructure Defect and Genotype. Am. J. Respir. Crit. Care Med. 2019, 199, 190–198. [Google Scholar] [CrossRef]
- Pifferi, M.; Bush, A.; Mariani, F.; Piras, M.; Michelucci, A.; Cangiotti, A.; Di Cicco, M.; Caligo, M.A.; Miccoli, M.; Boner, A.L.; et al. Lung Function Longitudinal Study by Phenotype and Genotype in Primary Ciliary Dyskinesia. Chest 2020, 158, 117–120. [Google Scholar] [CrossRef]
- Grasemann, H.; Tullis, E.; Ratjen, F. A randomized controlled trial of inhaled L-arginine in patients with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2013, 12, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Kouis, P.; Hadjisavvas, A.; Middleton, N.; Papatheodorou, S.I.; Kyriacou, K.; Yiallouros, P.K. The effect of l-Arginine on Ciliary Beat Frequency in PCD patients, non-PCD respiratory patients and healthy controls. Pulm. Pharmacol. Ther. 2018, 48, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Pifferi, M.; Bush, A.; Rizzo, M.; Tonacci, A.; Di Cicco, M.; Piras, M.; Maggi, F.; Paiola, G.; Michelucci, A.; Cangiotti, A.; et al. Olfactory dysfunction is worse in primary ciliary dyskinesia compared with other causes of chronic sinusitis in children. Thorax 2018, 73, 980–982. [Google Scholar] [CrossRef] [PubMed]
- Pietrobon, M.; Zamparo, I.; Maritan, M.; Franchi, S.A.; Pozzan, T.; Lodovichi, C. Interplay among cGMP, cAMP, and Ca2+ in living olfactory sensory neurons in vitro and in vivo. J. Neurosci. Off. J. Soc. Neurosci. 2011, 31, 8395–8405. [Google Scholar] [CrossRef]
- Kronenberg, G.; Gertz, K.; Baldinger, T.; Kirste, I.; Eckart, S.; Yildirim, F.; Ji, S.; Heuser, I.; Schröck, H.; Hörtnagl, H.; et al. Impact of actin filament stabilization on adult hippocampal and olfactory bulb neurogenesis. J. Neurosci. 2010, 30, 3419–3431. [Google Scholar] [CrossRef]
- Nakhleh, N.; Francis, R.; Giese, R.A.; Tian, X.; Li, Y.; Zariwala, M.A.; Yagi, H.; Khalifa, O.; Kureshi, S.; Chatterjee, B.; et al. High prevalence of respiratory ciliary dysfunction in congenital heart disease patients with heterotaxy. Circulation 2012, 125, 2232–2242. [Google Scholar] [CrossRef]
- Stewart, E.; Adams, P.S.; Tian, X.; Khalifa, O.; Wearden, P.; Zahid, M.; Lo, C.W. Airway ciliary dysfunction: Association with adverse postoperative outcomes in nonheterotaxy congenital heart disease patients. J. Thorac. Cardiovasc. Surg. 2018, 155, 755–763. [Google Scholar] [CrossRef]
- Zahid, M.; Bais, A.; Tian, X.; Devine, W.; Lee, D.M.; Yau, C.; Sonnenberg, D.; Beerman, L.; Khalifa, O.; Lo, C.W. Airway ciliary dysfunction and respiratory symptoms in patients with transposition of the great arteries. PLoS ONE 2018, 13, e0191605. [Google Scholar] [CrossRef]
- Chen, Q.B.; Chen, L.; Zheng, X.Y.; Zheng, X.; Fang, Q.; Xiao, M.; Lin, X.-T. The Clinical Significance of Nasal Nitric Oxide Concentrations in Preschool Children with Nasal Inflammatory Disease. Int. Arch. Allergy Immunol. 2020, 181, 51–55. [Google Scholar] [CrossRef]
- Liu, D.; Huang, Z.; Huang, Y.; Yi, X.; Chen, X. Measurement of nasal and fractional exhaled nitric oxide in children with upper airway inflammatory disease: Preliminary results. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 2308–2311. [Google Scholar] [CrossRef]
- Sutiratanachai, W.; Kanchongkittiphon, W.; Klangkalya, N.; Jotikasthira, W.; Kiewngam, P.; Manuyakorn, W. Airway Nitric Oxide in Children with HDM-Induced Allergic Rhinitis. Am. J. Rhinol. Allergy 2022, 36, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Antosova, M.; Bencova, A.; Mokra, D.; Plevkova, J.; Pepucha, L.; Buday, T. Exhaled and Nasal Nitric Oxide—Impact for Allergic Rhinitis. Physiol. Res. 2020, 69 (Suppl. S1), S123–S130. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Fasola, S.; Cilluffo, G.; Malizia, V.; Montalbano, L.; Landi, M.; Passalacqua, G.; La Grutta, S. Nasal budesonide efficacy for nasal nitric oxide and nasal obstruction in rhinitis. Pediatr. Allergy Immunol. 2017, 28, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Baraldi, E.; Azzolin, N.M.; Carrà, S.; Dario, C.; Marchesini, L.; Zacchello, F. Effect of topical steroids on nasal nitric oxide production in children with perennial allergic rhinitis: A pilot study. Respir. Med. 1998, 92, 558–561. [Google Scholar] [CrossRef] [PubMed]
- Occasi, F.; Duse, M.; Vittori, T.; Rugiano, A.; Tancredi, G.; De Castro, G.; Indinnimeo, L.; Zicari, A.M. Primary school children often underestimate their nasal obstruction. Rhinology 2016, 54, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.; Cheng, S.; Xie, S.; Zhang, H.; Zhang, J.; Wang, F.; Xie, S.; Xie, Z.; Jiang, W. Predictive Value of Nasal Nitric Oxide and Serum NOS2 Levels in the Efficacy of Subcutaneous Immunotherapy in Pediatric Patients with Allergic Rhinitis. Mediat. Inflamm. 2022, 2022, 1679536. [Google Scholar] [CrossRef]
- Parisi, G.F.; Manti, S.; Papale, M.; Amato, M.; Licari, A.; Marseglia, G.L.; Leonardi, S. Nasal Nitric Oxide and Nasal Cytology as Predictive Markers of Short-Term Sublingual Allergen-Specific Immunotherapy Efficacy in Children with Allergic Rhinitis. Am. J. Rhinol. Allergy 2022, 36, 323–329. [Google Scholar] [CrossRef]
- Maniscalco, M.; Sofia, M.; Pelaia, G. Nitric oxide in upper airways inflammatory diseases. Inflamm. Res. 2007, 56, 58–69. [Google Scholar] [CrossRef]
- Güney, E.; Emiralioğlu, N.; Cinel, G.; Yalçın, E.; Doğru, D.; Kiper, N.; Özçelik, H.U. Nasal nitric oxide levels in primary ciliary dyskinesia, cystic fibrosis and healthy children. Turk. J. Pediatr. 2019, 61, 20–25. [Google Scholar] [CrossRef]
- de Winter-de Groot, K.M.; van Haren Noman, S.; Speleman, L.; Schilder, A.G.M.; van der Ent, C.K. Nasal nitric oxide levels and nasal polyposis in children and adolescents with cystic fibrosis. JAMA Otolaryngol.—Head Neck Surg. 2013, 139, 931–936. [Google Scholar] [CrossRef]
- Kirihene, R.K.; Rees, G.; Wormald, P.J. The influence of the size of the maxillary sinus ostium on the nasal and sinus nitric oxide levels. Am. J. Rhinol. 2002, 16, 261–264. [Google Scholar] [CrossRef] [PubMed]
- Michl, R.K.; Hentschel, J.; Fischer, C.; Beck, J.F.; Mainz, J.G. Reduced nasal nitric oxide production in cystic fibrosis patients with elevated systemic inflammation markers. PLoS ONE 2013, 8, e79141. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Disease | nNO Levels | Suggested Mechanisms | Clinical Use |
|---|---|---|---|
| PCD | Low |
| PCD diagnosis in a clinically suggestive patient |
| Rhinosinusitis | Low |
| Possible marker of severity |
| Allergic rhinitis | High |
| Possible prognostic role in assessing immunotherapy response |
| Cystic fibrosis | Normal or low |
| Reduced levels can be associated with higher prevalence of infections |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paternò, S.; Pisani, L.; Zanconato, S.; Ferraro, V.A.; Carraro, S. Role of Nasal Nitric Oxide in Primary Ciliary Dyskinesia and Other Respiratory Conditions in Children. Int. J. Mol. Sci. 2023, 24, 16159. https://doi.org/10.3390/ijms242216159
Paternò S, Pisani L, Zanconato S, Ferraro VA, Carraro S. Role of Nasal Nitric Oxide in Primary Ciliary Dyskinesia and Other Respiratory Conditions in Children. International Journal of Molecular Sciences. 2023; 24(22):16159. https://doi.org/10.3390/ijms242216159
Chicago/Turabian StylePaternò, Salvatore, Laura Pisani, Stefania Zanconato, Valentina Agnese Ferraro, and Silvia Carraro. 2023. "Role of Nasal Nitric Oxide in Primary Ciliary Dyskinesia and Other Respiratory Conditions in Children" International Journal of Molecular Sciences 24, no. 22: 16159. https://doi.org/10.3390/ijms242216159
APA StylePaternò, S., Pisani, L., Zanconato, S., Ferraro, V. A., & Carraro, S. (2023). Role of Nasal Nitric Oxide in Primary Ciliary Dyskinesia and Other Respiratory Conditions in Children. International Journal of Molecular Sciences, 24(22), 16159. https://doi.org/10.3390/ijms242216159