
Microcalcification and 99mTc-Pyrophosphate Uptake without Increased Bone Metabolism in Cardiac Tissue from Patients with Transthyretin Cardiac Amyloidosis

 , , and
, , and
Abstract
:1. Introduction
2. Results
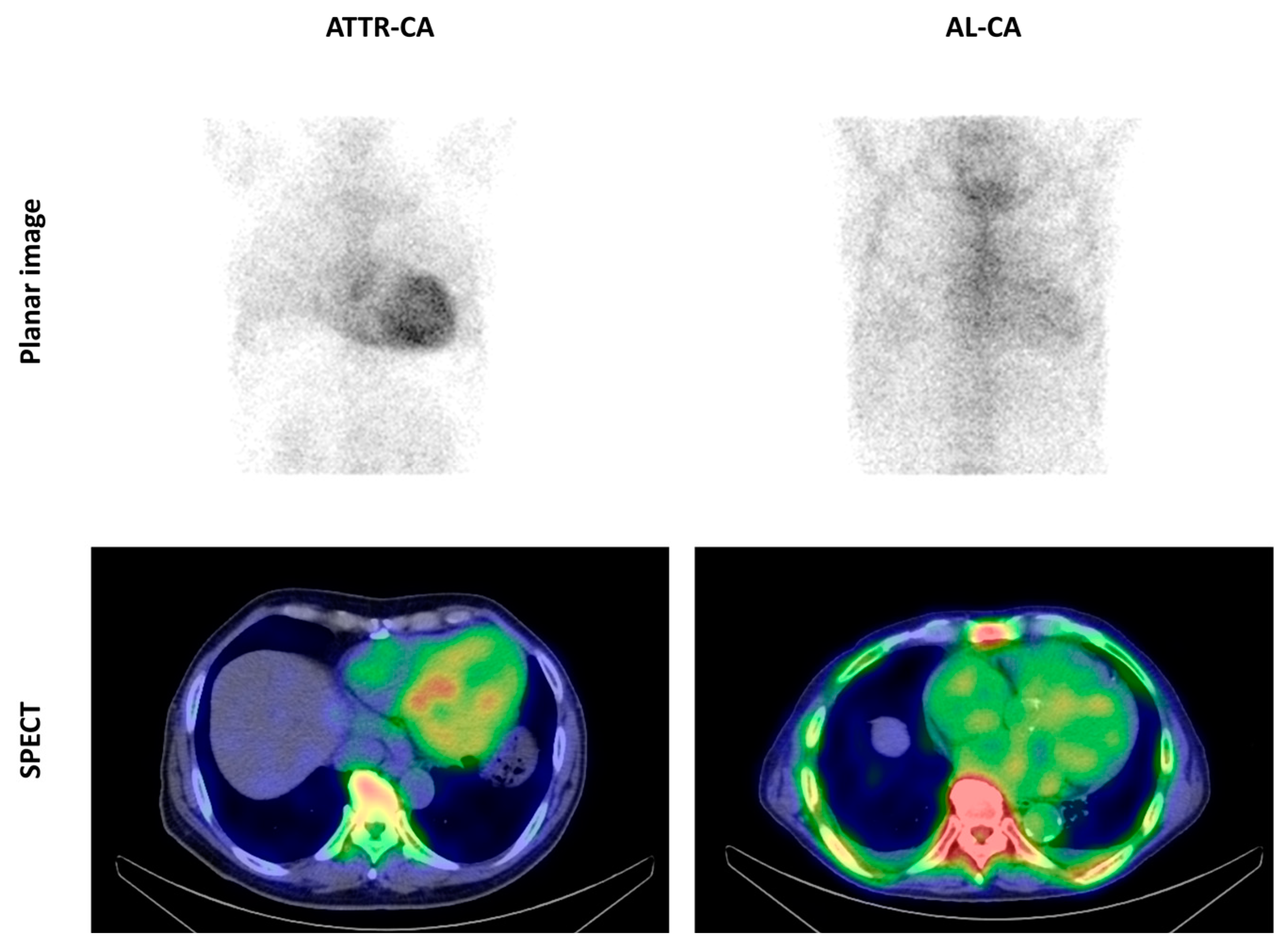
2.1. Cardiac Uptake of 99mTc-Pyrophosphate
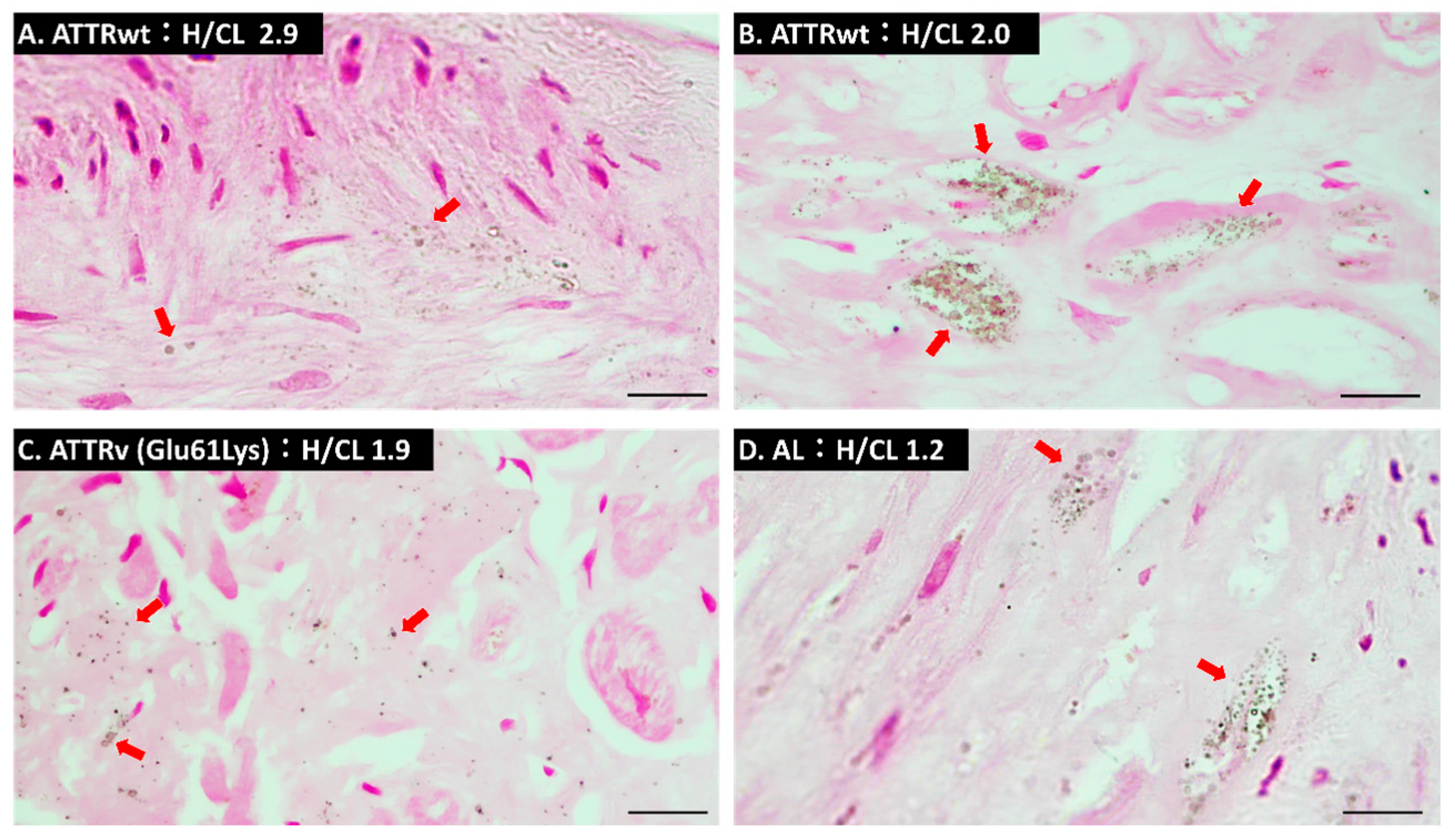
2.2. Microcalcification Detected by Von Kossa Staining
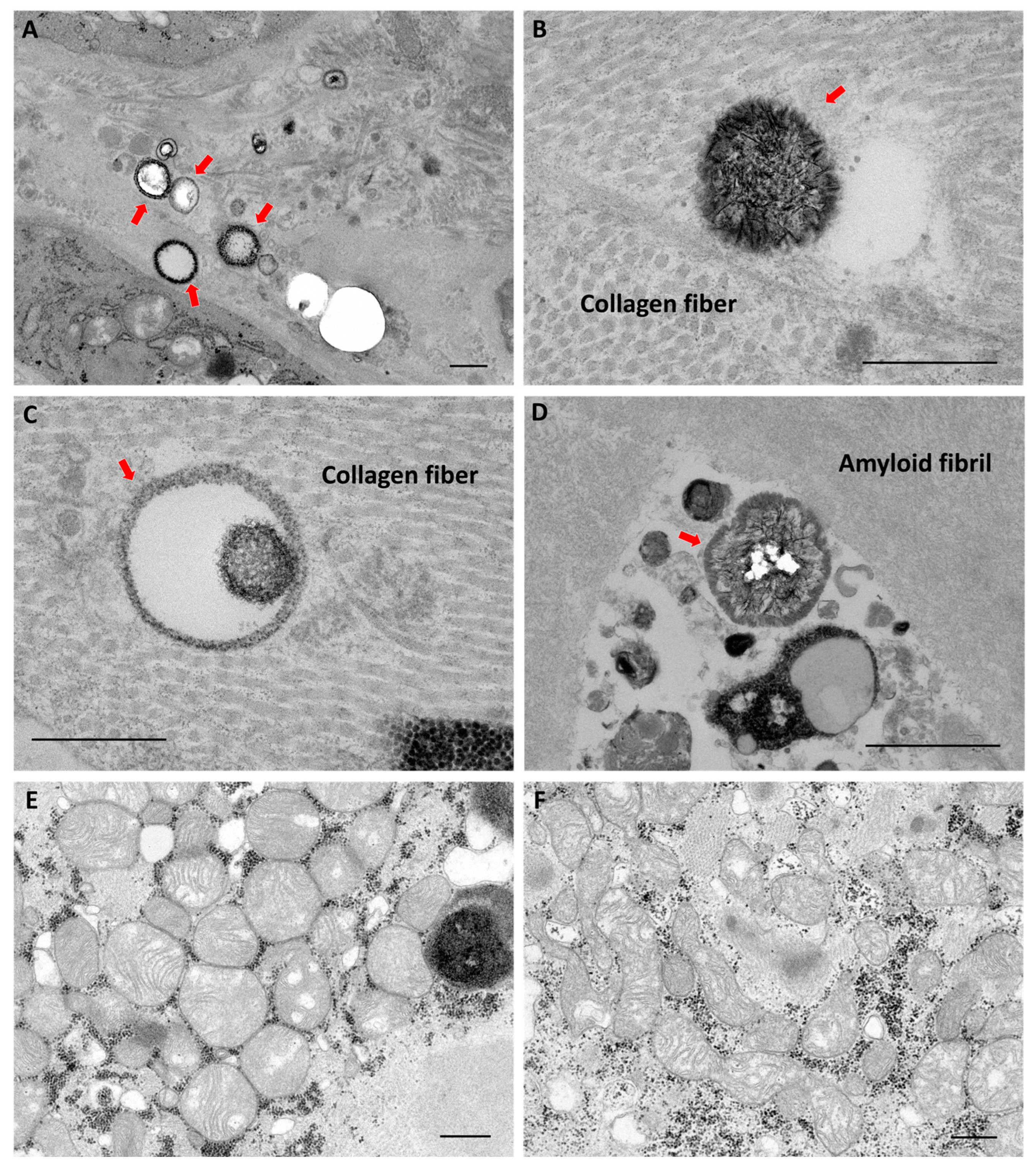
2.3. Findings of Transmission Electron Microscopy
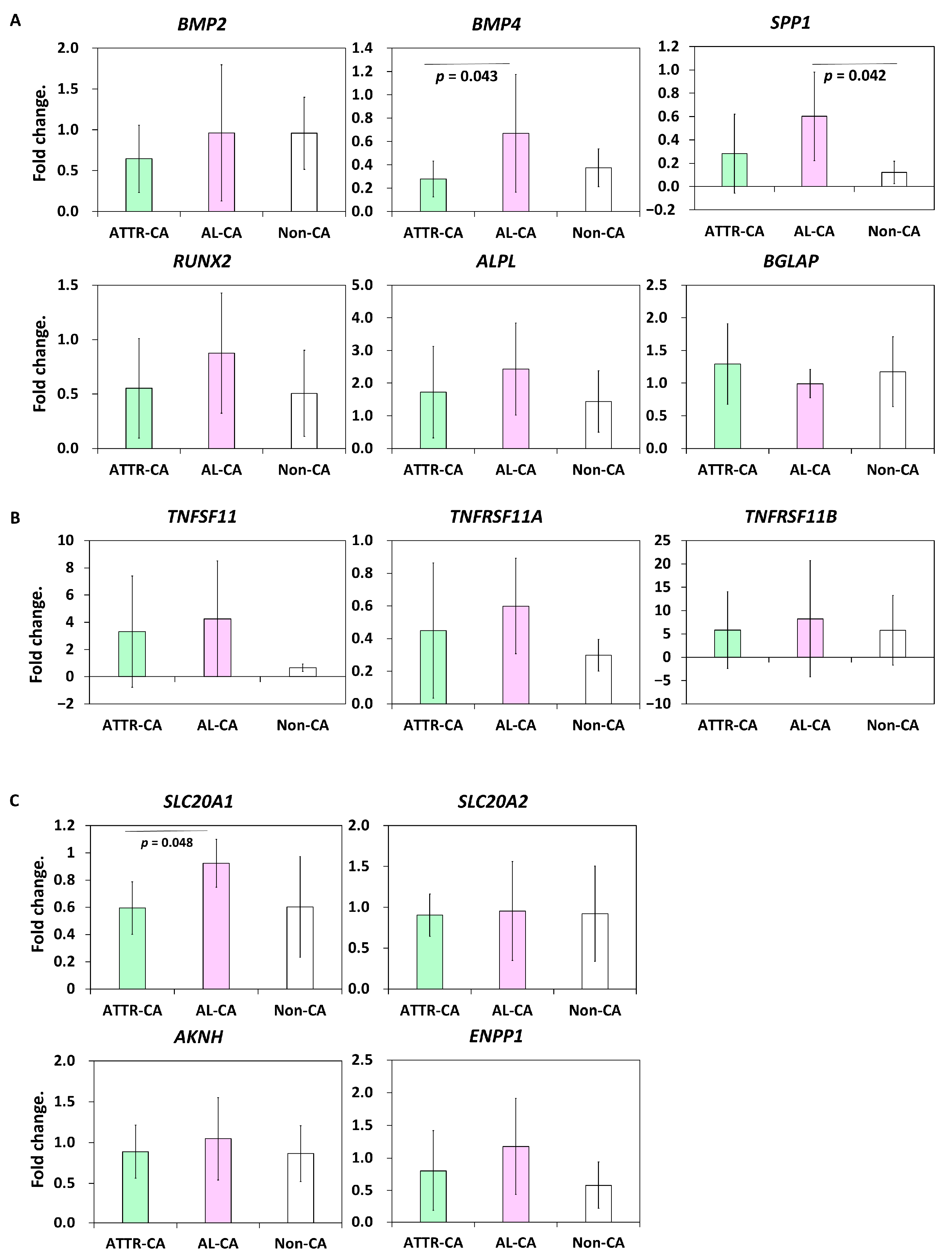
2.4. Bone Metabolism-Related Gene Expression
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. 99mTc-Pyrophosphate Scintigraphy
4.3. Right Ventricular Endomyocardial Biopsy
4.4. Von Kossa Staining
4.5. Quantitative Polymerase Chain Reaction (qPCR)
4.6. Transmission Electron Microscopy
4.7. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | analysis of variance |
| AL-CA | amyloid light-chain cardiac amyloidosis |
| ATTR-CA | transthyretin cardiac amyloidosis |
| ATTRv | hereditary transthyretin amyloidosis |
| ATTRwt | wild-type transthyretin amyloidosis |
| H/CL | heart-to-contralateral |
| 99mTc-DPD | 99mTc-dicarboxypropane diphosphonate |
| 99mTc-PYP | 99mTc-pyrophoshate |
| Non-CA | noncardiac amyloidosis |
| TEM | transmission electron microscopy |
| TTR | transthyretin |
| qPCR | quantitative polymerase chain reaction |
References
- Merlini, G.; Bellotti, V. Molecular mechanisms of amyloidosis. N. Engl. J. Med. 2003, 349, 583–596. [Google Scholar] [CrossRef] [Green Version]
- Grogan, M.; Scott, C.G.; Kyle, R.A.; Zeldenrust, S.R.; Gertz, M.A.; Lin, G.; Klarich, K.W.; Miller, W.L.; Maleszewski, J.J.; Dispenzieri, A. Natural History of Wild-Type Transthyretin Cardiac Amyloidosis and Risk Stratification Using a Novel Staging System. J. Am. Coll. Cardiol. 2016, 68, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Witteles, R.M.; Liedtke, M. AL Amyloidosis for the Cardiologist and Oncologist: Epidemiology, Diagnosis, and Management. JACC CardioOncol 2019, 1, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Foss, T.R.; Wiseman, R.L.; Kelly, J.W. The pathway by which the tetrameric protein transthyretin dissociates. Biochemistry 2005, 44, 15525–15533. [Google Scholar] [CrossRef]
- Fontana, M.; Ćorović, A.; Scully, P.; Moon, J.C. Myocardial Amyloidosis: The Exemplar Interstitial Disease. JACC Cardiovasc. Imaging 2019, 12, 2345–2356. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Adams, D.; Gonzalez-Duarte, A.; O’Riordan, W.D.; Yang, C.C.; Ueda, M.; Kristen, A.V.; Tournev, I.; Schmidt, H.H.; Coelho, T.; Berk, J.L.; et al. Patisiran, an RNAi Therapeutic, for Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 11–21. [Google Scholar] [CrossRef]
- Benson, M.D.; Waddington-Cruz, M.; Berk, J.L.; Polydefkis, M.; Dyck, P.J.; Wang, A.K.; Planté-Bordeneuve, V.; Barroso, F.A.; Merlini, G.; Obici, L.; et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 22–31. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar]
- Castano, A.; Haq, M.; Narotsky, D.L.; Goldsmith, J.; Weinberg, R.L.; Morgenstern, R.; Pozniakoff, T.; Ruberg, F.L.; Miller, E.J.; Berk, J.L.; et al. Multicenter Study of Planar Technetium 99m Pyrophosphate Cardiac Imaging: Predicting Survival for Patients with ATTR Cardiac Amyloidosis. JAMA Cardiol. 2016, 1, 880–889. [Google Scholar] [CrossRef]
- Castaño, A.; DeLuca, A.; Weinberg, R.; Pozniakoff, T.; Blaner, W.S.; Pirmohamed, A.; Bettencourt, B.; Gollob, J.; Karsten, V.; Vest, J.A.; et al. Serial scanning with technetium pyrophosphate. J. Nucl. Cardiol. 2016, 23, 1355–1363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musumeci, M.B.; Cappelli, F.; Russo, D.; Tini, G.; Canepa, M.; Milandri, A.; Bonfiglioli, R.; Di Bella, G.; My, F.; Luigetti, M.; et al. Low Sensitivity of Bone Scintigraphy in Detecting Phe64Leu Mutation-Related Transthyretin Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Van den Wyngaert, T.; Strobel, K.; Kampen, W.U.; Kuwert, T.; van der Bruggen, W.; Mohan, H.K.; Gnanasegaran, G.; Delgado-Bolton, R.; Weber, W.A.; Beheshti, M.; et al. The EANM practice guidelines for bone scintigraphy. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1723–1738. [Google Scholar] [CrossRef] [Green Version]
- Stats, M.A.; Stone, J.R. Varying levels of small microcalcifications and macrophages in ATTR and AL cardiac amyloidosis: Implications for utilizing nuclear medicine studies to subtype amyloidosis. Cardiovasc. Pathol. 2016, 25, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Thelander, U.; Westermark, G.T.; Antoni, G.; Estrada, S.; Zancanaro, A.; Ihse, E.; Westermark, P. Cardiac microcalcifications in transthyretin (ATTR) amyloidosis. Int. J. Cardiol. 2022, 352, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Porcari, A.; Fontana, M.; Gillmore, J.D. Transthyretin cardiac amyloidosis. Cardiovasc. Res. 2022; in press. [Google Scholar] [CrossRef]
- Pilebro, B.; Suhr, O.B.; Näslund, U.; Westermark, P.; Lindqvist, P.; Sundström, T. (99m)Tc-DPD uptake reflects amyloid fibril composition in hereditary transthyretin amyloidosis. Upsale J. Med. Sci. 2016, 121, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suenaga, G.; Ikeda, T.; Masuda, T.; Motokawa, H.; Yamashita, T.; Takamatsu, K.; Misumi, Y.; Ueda, M.; Matsui, H.; Senju, S.; et al. Inflammatory state exists in familial amyloid polyneuropathy that may be triggered by mutated transthyretin. Sci. Rep. 2017, 7, 1579. [Google Scholar] [CrossRef] [Green Version]
- Dittloff, K.T.; Iezzi, A.; Zhong, J.X.; Mohindra, P.; Desai, T.A.; Russell, B. Transthyretin amyloid fibrils alter primary fibroblast structure, function, and inflammatory gene expression. Am. J. Physiol. Heart Circ. Physiol. 2021, 321, H149–H160. [Google Scholar] [CrossRef]
- Saito, Y.; Nakamura, K.; Ito, H. Effects of Eicosapentaenoic Acid on Arterial Calcification. Int. J. Mol. Sci. 2020, 21, 5455. [Google Scholar] [CrossRef] [PubMed]
- Lok, Z.S.Y.; Lyle, A.N. Osteopontin in Vascular Disease. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 613–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buja, L.M.; Parkey, R.W.; Stokely, E.M.; Bonte, F.J.; Willerson, J.T. Pathophysiology of technetium-99m stannous pyrophosphate and thallium-201 scintigraphy of acute anterior myocardial infarcts in dogs. J. Clin. Investig. 1976, 57, 1508–1522. [Google Scholar] [CrossRef] [Green Version]
- Van Der Gucht, A.; Galat, A.; Rosso, J.; Guellich, A.; Garot, J.; Bodez, D.; Plante-Bordeneuve, V.; Hittinger, L.; Dubois-Randé, J.L.; Evangelista, E.; et al. [18F]-NaF PET/CT imaging in cardiac amyloidosis. J. Nucl. Cardiol. 2016, 23, 846–849. [Google Scholar] [CrossRef] [PubMed]
- Martineau, P.; Finnerty, V.; Giraldeau, G.; Authier, S.; Harel, F.; Pelletier-Galarneau, M. Examining the sensitivity of 18F-NaF PET for the imaging of cardiac amyloidosis. J. Nucl. Cardiol. 2021, 28, 209–218. [Google Scholar] [CrossRef]
- O’Sullivan, G.J.; Carty, F.L.; Cronin, C.G. Imaging of bone metastasis: An update. World J. Radiol. 2015, 7, 202–211. [Google Scholar] [CrossRef]
- Kotecha, T.; Martinez-Naharro, A.; Treibel, T.A.; Francis, R.; Nordin, S.; Abdel-Gadir, A.; Knight, D.S.; Zumbo, G.; Rosmini, S.; Maestrini, V.; et al. Myocardial Edema and Prognosis in Amyloidosis. J. Am. Coll. Cardiol. 2018, 71, 2919–2931. [Google Scholar] [CrossRef]
- Okuda, K.; Nohara, R.; Fujita, M.; Tamaki, N.; Konishi, J.; Sasayama, S. Technetium-99m-pyrophosphate uptake as an indicator of myocardial injury without infarct. J. Nucl. Med. 1994, 35, 1366–1370. [Google Scholar]
- Chien, K.R.; Reeves, J.P.; Buja, L.M.; Bonte, F.; Parkey, R.W.; Willerson, J.T. Phospholipid alterations in canine ischemic myocardium. Temporal and topographical correlations with Tc-99m-PPi accumulation and an in vitro sarcolemmal Ca2+ permeability defect. Circ. Res. 1981, 48, 711–719. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y.; Nakamura, K.; Ito, H. Molecular Mechanisms of Cardiac Amyloidosis. Int. J. Mol. Sci. 2021, 23, 25. [Google Scholar] [CrossRef]
- Bergström, J.; Gustavsson, A.; Hellman, U.; Sletten, K.; Murphy, C.L.; Weiss, D.T.; Solomon, A.; Olofsson, B.O.; Westermark, P. Amyloid deposits in transthyretin-derived amyloidosis: Cleaved transthyretin is associated with distinct amyloid morphology. J. Pathol. 2005, 206, 224–232. [Google Scholar] [CrossRef]
- Ihse, E.; Rapezzi, C.; Merlini, G.; Benson, M.D.; Ando, Y.; Suhr, O.B.; Ikeda, S.; Lavatelli, F.; Obici, L.; Quarta, C.C.; et al. Amyloid fibrils containing fragmented ATTR may be the standard fibril composition in ATTR amyloidosis. Amyloid 2013, 20, 142–150. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Rappaport, M.; Shimoni, S.; Goland, S.; Voldarsky, I.; Fabricant, Y.; Edri, O.; Cuciuc, V.; Lifshitz, S.; Tshori, S.; et al. A novel monoclonal antibody targeting aggregated transthyretin facilitates its removal and functional recovery in an experimental model. Eur. Heart J. 2020, 41, 1260–1270. [Google Scholar] [CrossRef] [Green Version]
- Wieczorek, E.; Kędracka-Krok, S.; Bystranowska, D.; Ptak, M.; Wiak, K.; Wygralak, Z.; Jankowska, U.; Ożyhar, A. Destabilisation of the structure of transthyretin is driven by Ca. Int. J. Biol. Macromol. 2021, 166, 409–423. [Google Scholar] [CrossRef] [PubMed]
- Cantarutti, C.; Mimmi, M.C.; Verona, G.; Mandaliti, W.; Taylor, G.W.; Mangione, P.P.; Giorgetti, S.; Bellotti, V.; Corazza, A. Calcium Binds to Transthyretin with Low Affinity. Biomolecules 2022, 12, 1066. [Google Scholar] [CrossRef]
- Dewanjee, M.K.; Kahn, P.C. Mechanism of localization of 99mTc-labeled pyrophosphate and tetracycline in infarcted myocardium. J. Nucl. Med. 1976, 17, 639–646. [Google Scholar] [PubMed]
- Moñivas Palomero, V.; Durante-Lopez, A.; Sanabria, M.T.; Cubero, J.S.; González-Mirelis, J.; Lopez-Ibor, J.V.; Navarro Rico, S.M.; Krsnik, I.; Dominguez, F.; Mingo, A.M.; et al. Role of Right Ventricular Strain Measured by Two-Dimensional Echocardiography in the Diagnosis of Cardiac Amyloidosis. J. Am. Soc. Echocardiogr. 2019, 32, 845–853.e1. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2−ΔΔCT Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Perugini Grading Score | |||
|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |
| ATTR-CA (N = 26) | 0 (0) | 0/26 | 1 (4) | 25 (96) |
| AL-CA (N = 6) | 3 (50) | 2 (33) | 1 (17) | 0 (0) |
| non-CA (N = 11) | 10 (91) | 0 (0) | 1 (9) | 0 (0) |
| Type | Von Kossa-Positive |
|---|---|
| ATTR-CA (N = 13) | 8 (62) a |
| AL-CA (N = 6) | 2 (33) a,b |
| non-CA (N = 6) | 0 (0) b |
| ATTR-CA | AL-CA | Non-CA | p Value | |
|---|---|---|---|---|
| serum creatinine (mg/dL) | 1.3 ± 0.6 | 1.3 ± 0.6 | 1.5 ± 1.3 | 0.794 |
| estimated glomerular filtration rate (mL/min/1.73 m2) | 49.1 ± 17.4 | 48.6 ± 22.6 | 51.6 ± 18.4 | 0.930 |
| serum calcium (mg/dL) | 9.1 ± 0.4 | 9.3 ± 0.7 | 9.2 ± 0.5 | 0.640 |
| Gene Symbol | Sequence | Product Size (bp) | |
|---|---|---|---|
| AKNH | F | CGATTTTGACAGCCACATACCC | 100 |
| R | GTTGCTGGGGTTATTCTTGTCG | ||
| ALPL | F | CAAAGGCTTCTTCTTGCTGGTG | 70 |
| R | CTGCTTGGCTTTTCCTTCATGG | ||
| BGLAP | F | CAGCCTTTGTGTCCAAGCAG | 136 |
| R | TCCGGATTGAGCTCACACAC | ||
| BMP2 | F | GCAGCTTCCACCATGAAGAATC | 144 |
| R | GCATCTGTTCTCGGAAAACCTG | ||
| BMP4 | F | ATCTTTACCGGCTTCAGTCTGG | 129 |
| R | TCTCCAGATGTTCTTCGTGGTG | ||
| ENPP1 | F | CCTGTGTTGAGCTTGGAAACTG | 135 |
| R | AGTCATCTGAACAGGCACAGAG | ||
| GAPDH | F | CAACGACCACTTTGTCAAGCTC | 144 |
| R | TCTCTTCCTCTTGTGCTCTTGC | ||
| RUNX2 | F | TCACAAATCCTCCCCAAGTAGC | 127 |
| R | AGGCGGTCAGAGAACAAACTAG | ||
| SLC20A1 | F | GCGTGGACTTGAAAGAGGAAAC | 88 |
| R | TGACTGAACTGGACAAGGTTCC | ||
| SLC20A2 | F | CGTGGATGCGGAGGAAAATAAC | 75 |
| R | TGAGGCTTTCGTCAGATACTCG | ||
| SPP1 | F | ACAGACCCTTCCAAGTAAGTCC | 119 |
| R | CATCATCAGAGTCGTTCGAGTC | ||
| TNFRSF11A | F | TGGACCAACTGTACCTTCCTTG | 95 |
| R | GGTTTTCTAGCTGGCAGAGAAG | ||
| TNFRSF11B | F | GGGACCACAATGAACAACTTGC | 75 |
| R | TTCCTGGGTGGTCCACTTAATG | ||
| TNFSF11 | F | ATCACAGCACATCAGAGCAGAG | 78 |
| R | GCTTCAAGCTTGCTCCTCTTG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, A.; Saito, Y.; Nakamura, K.; Iida, T.; Akagi, S.; Yoshida, M.; Taniyama, M.; Miyoshi, T.; Ito, H. Microcalcification and 99mTc-Pyrophosphate Uptake without Increased Bone Metabolism in Cardiac Tissue from Patients with Transthyretin Cardiac Amyloidosis. Int. J. Mol. Sci. 2023, 24, 1921. https://doi.org/10.3390/ijms24031921
Mori A, Saito Y, Nakamura K, Iida T, Akagi S, Yoshida M, Taniyama M, Miyoshi T, Ito H. Microcalcification and 99mTc-Pyrophosphate Uptake without Increased Bone Metabolism in Cardiac Tissue from Patients with Transthyretin Cardiac Amyloidosis. International Journal of Molecular Sciences. 2023; 24(3):1921. https://doi.org/10.3390/ijms24031921
Chicago/Turabian StyleMori, Atsushi, Yukihiro Saito, Kazufumi Nakamura, Toshihiro Iida, Satoshi Akagi, Masashi Yoshida, Makiko Taniyama, Toru Miyoshi, and Hiroshi Ito. 2023. "Microcalcification and 99mTc-Pyrophosphate Uptake without Increased Bone Metabolism in Cardiac Tissue from Patients with Transthyretin Cardiac Amyloidosis" International Journal of Molecular Sciences 24, no. 3: 1921. https://doi.org/10.3390/ijms24031921
APA StyleMori, A., Saito, Y., Nakamura, K., Iida, T., Akagi, S., Yoshida, M., Taniyama, M., Miyoshi, T., & Ito, H. (2023). Microcalcification and 99mTc-Pyrophosphate Uptake without Increased Bone Metabolism in Cardiac Tissue from Patients with Transthyretin Cardiac Amyloidosis. International Journal of Molecular Sciences, 24(3), 1921. https://doi.org/10.3390/ijms24031921