
Aluminum Nanoparticles Affect Human Platelet Function In Vitro

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Characterization of Aluminium Nanoparticle
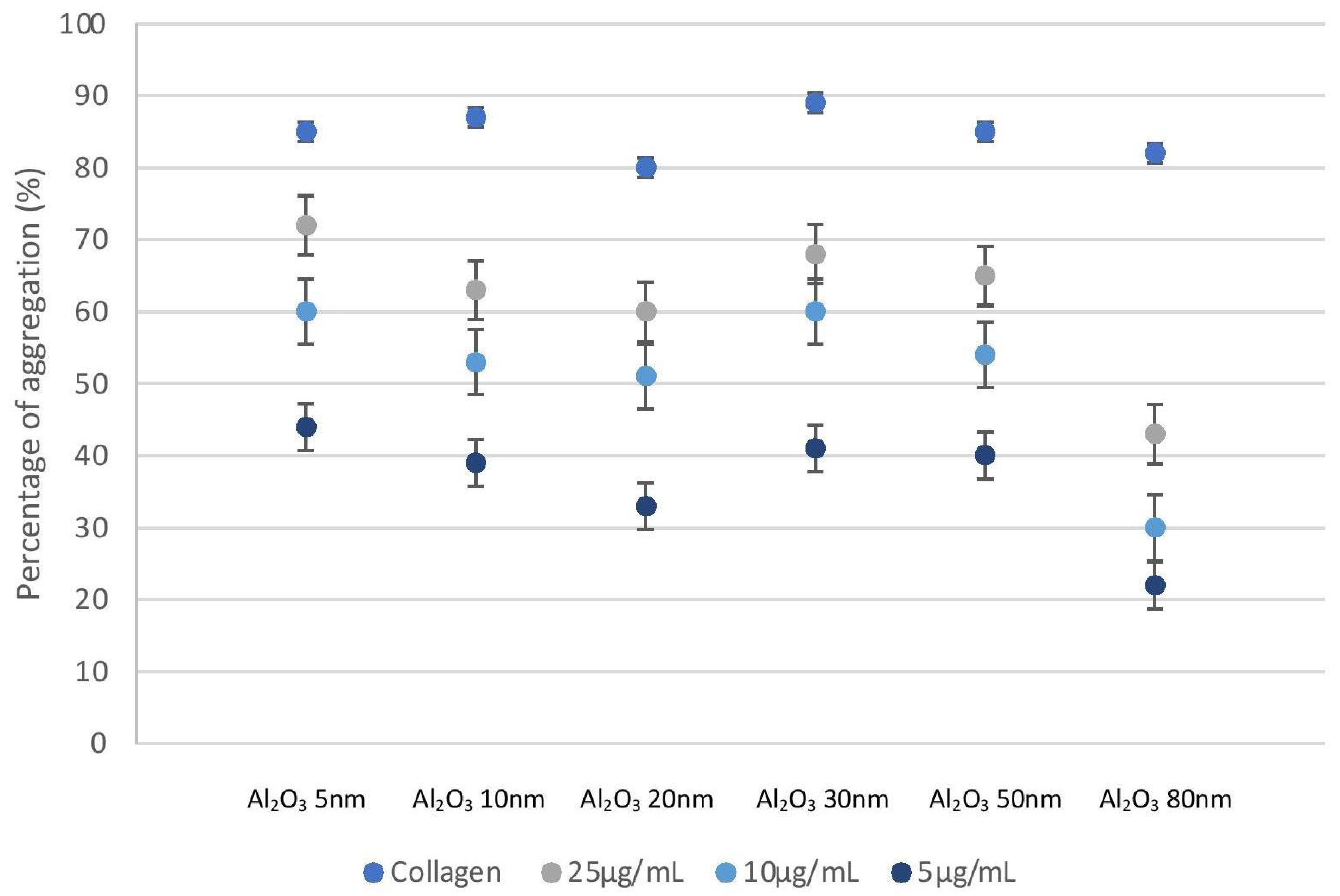
2.2. Aluminium Nanoparticles Cause Platelet Aggregation
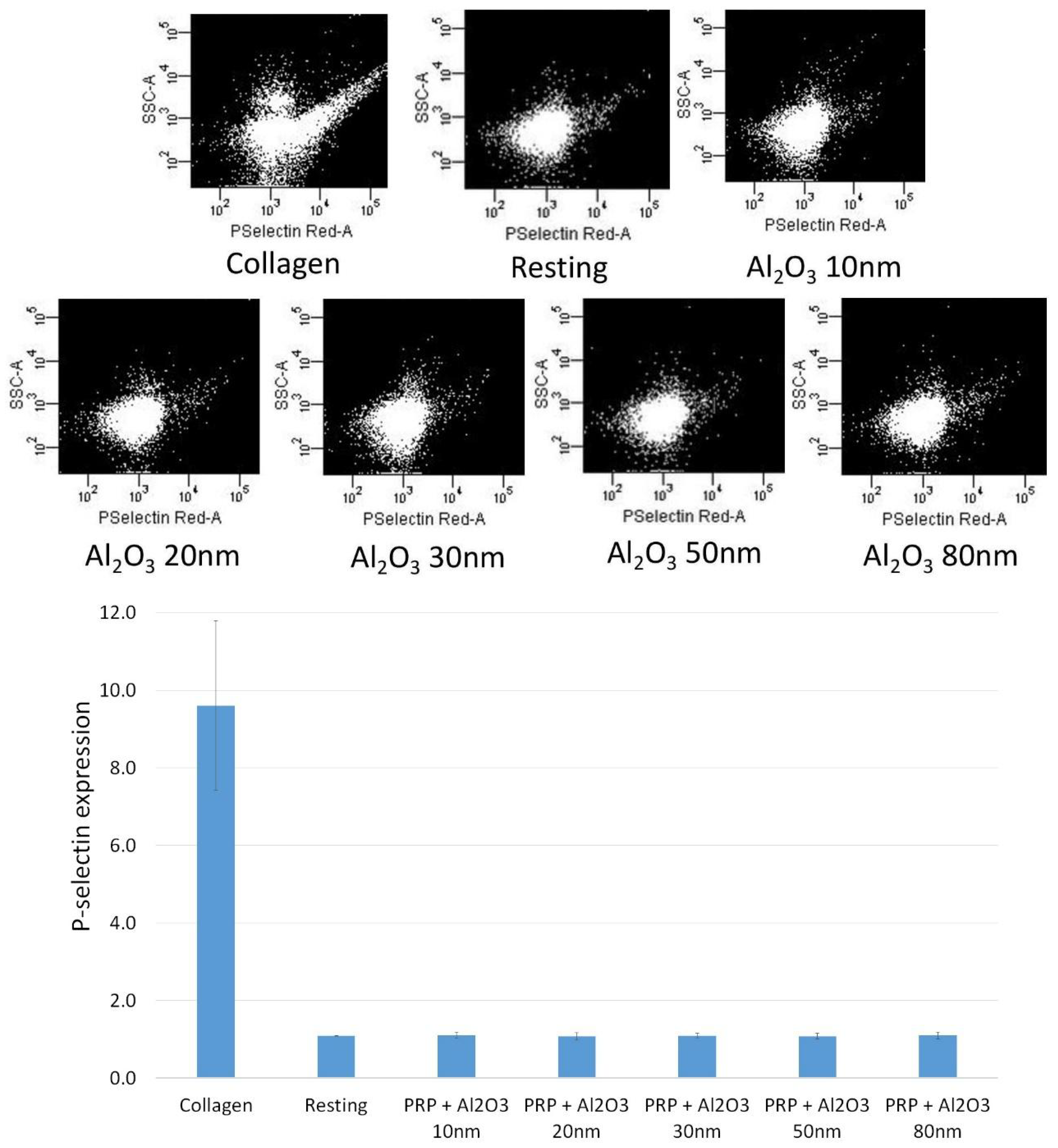
2.3. Flow Cytometry Shows No Platelet Activation in the Presence of Al Nanoparticles
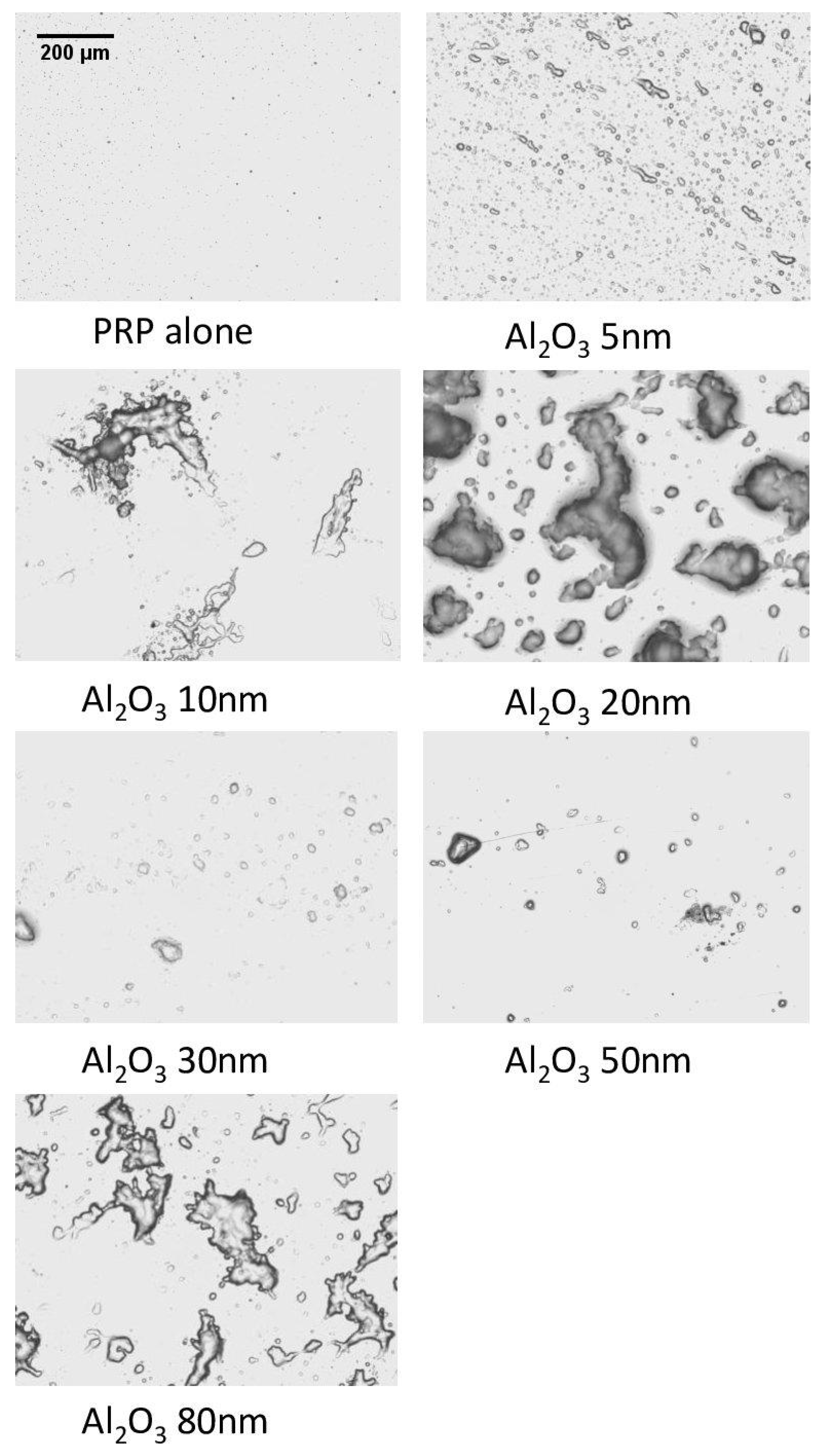
2.4. Optical Microscopy Shows Platelet Aggregates on QCM-D Crystals
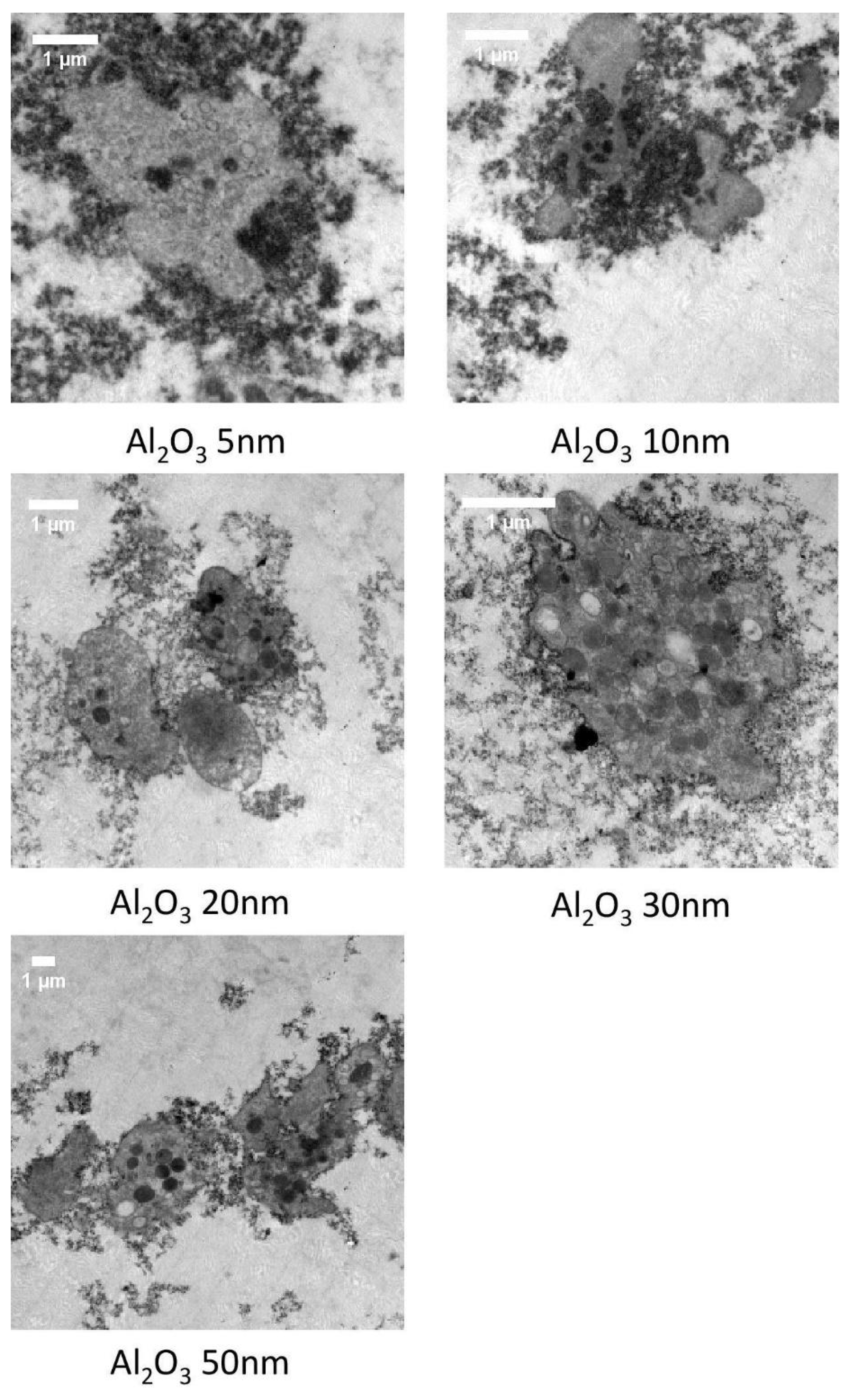
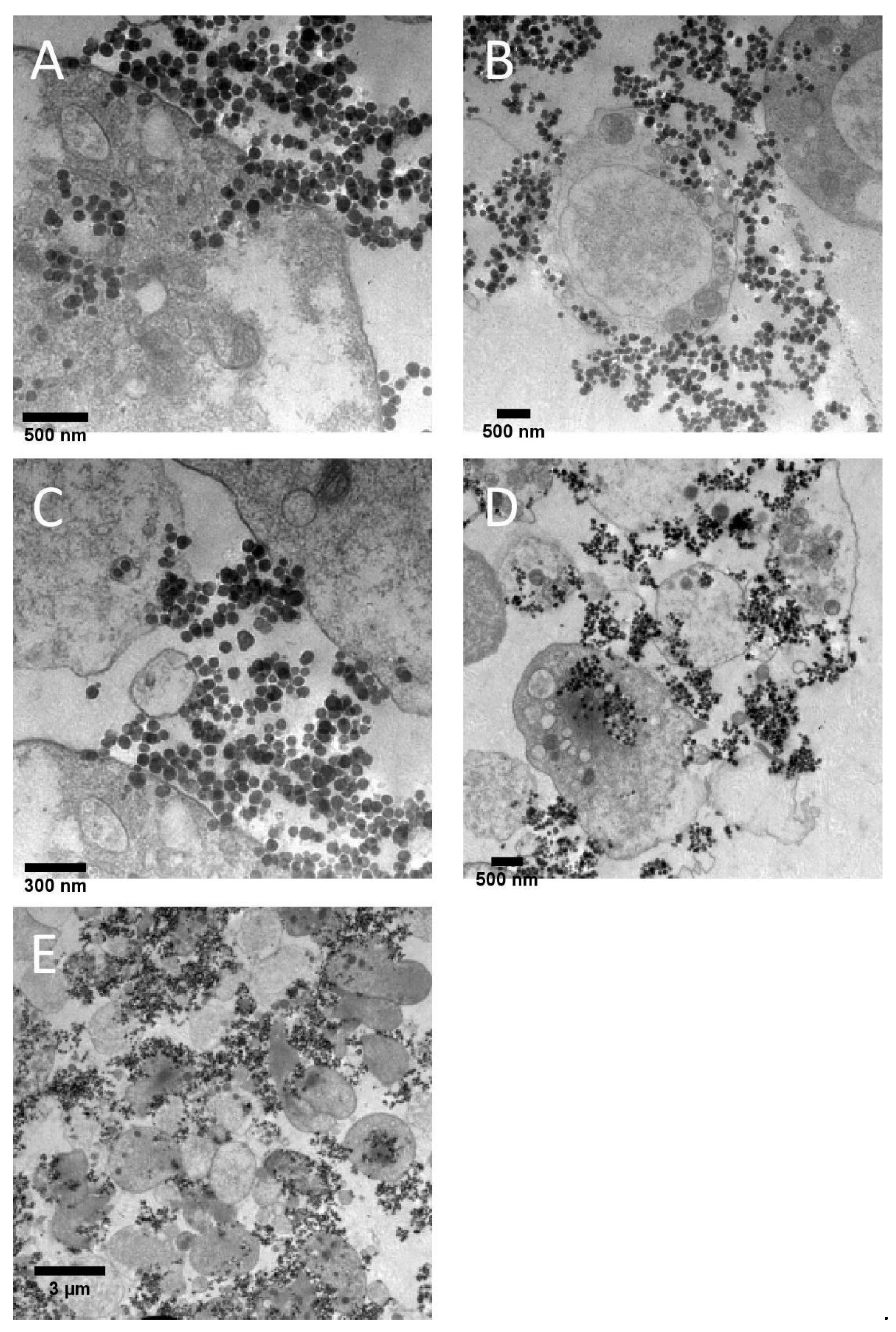
2.5. Transmission Electron Microscopy Shows Different Mechanisms of Interaction with Platelets for Small (5–50 nm) and Large (80 nm) Al Nanoparticles
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. Dispersion and Characterization of Nanoparticles
4.3. Blood Collection and Platelet Isolation
4.4. Platelet Aggregation Measured by Light Transmission Aggregometry
4.5. Platelet Activation Monitored by Flow Cytometry
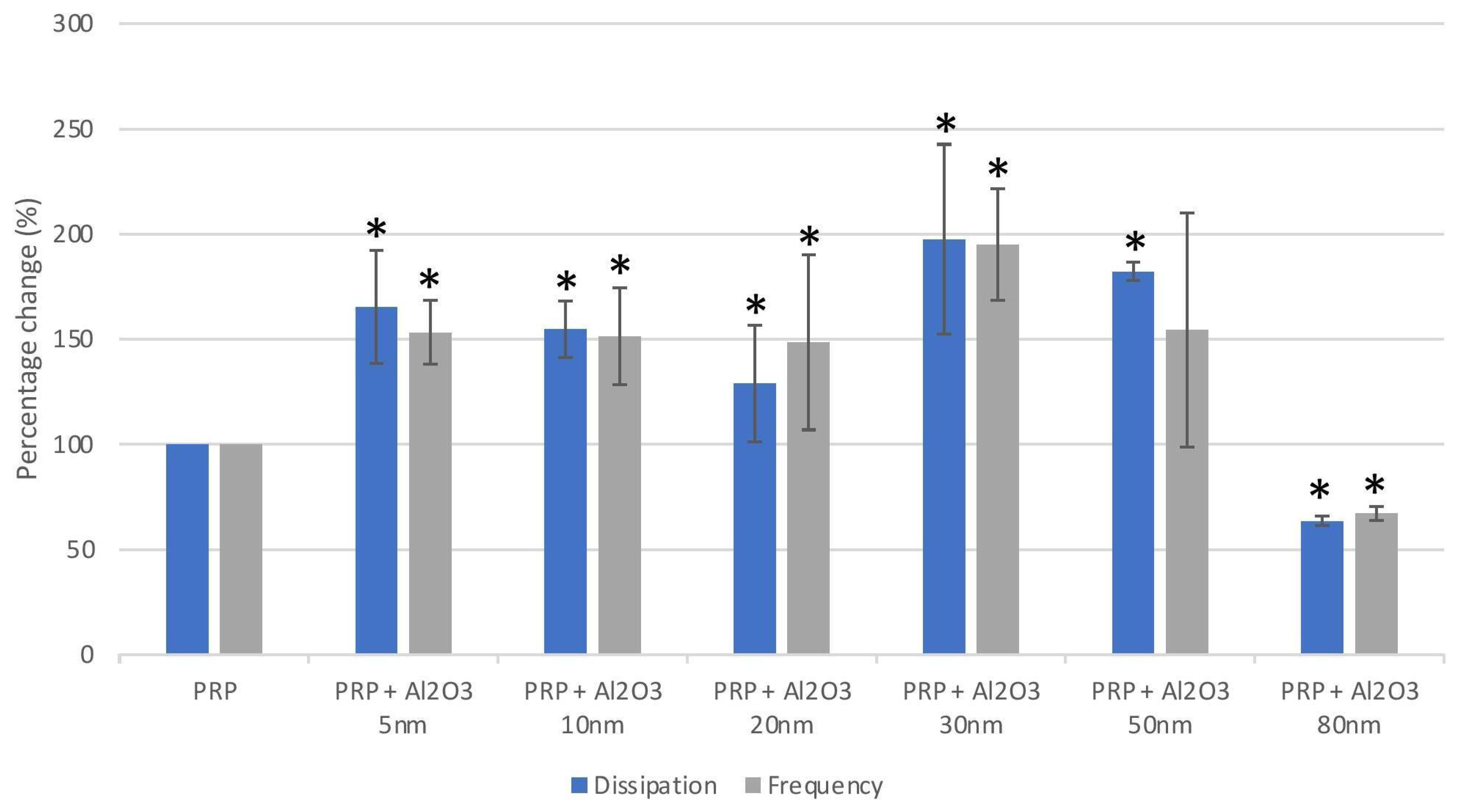
4.6. Platelet Aggregation Measured Using Quartz Crystal Microbalance with Dissipation
4.7. Optical Microscopy
4.8. Transmission Electron Microscopy
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canovas, F.; Dagneaux, L. Quality of life after total knee arthroplasty. Orthop. Traumatol. Surg. Res. 2018, 104, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Patel, A.; Pavlou, G.; Mújica-Mota, R.E.; Toms, A.D. The epidemiology of revision total knee and hip arthroplasty in England and Wales: A comparative analysis with projections for the United States. a study using the national joint registry dataset. Bone Jt. J. 2015, 97, 1076–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Kremers, H.M.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of total hip and knee replacement in the United States. J. Bone Jt. Surg. Am. Vol. 2014, 97, 1386–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, A.M.; Brock, T.M.; Heil, K.; Holmes, R.; Weusten, A. A Review on the Management of Hip and Knee Osteoarthritis. Int. J. Chronic Dis. 2013, 2013, 845015. [Google Scholar] [CrossRef] [Green Version]
- Solimeno, L.P.; Pasta, G. Knee and Ankle Arthroplasty in Hemophilia. J. Clin. Med. 2017, 6, 107. [Google Scholar] [CrossRef] [Green Version]
- Ament, J.D.; Yang, Z.; Nunley, P.; Stone, M.B.; Kim, K.D. Cost-effectiveness of cervical total disc replacement vs fusion for the treatment of 2-level symptomatic degenerative disc disease. JAMA Surg. 2014, 149, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Othman, Y.A.; Verma, R.; Qureshi, S.A. Artificial disc replacement in spine surgery. Ann. Transl. Med. 2019, 7, S170. [Google Scholar] [CrossRef]
- Xia, Z.; Ricciardi, B.F.; Liu, Z.; von Ruhland, C.; Ward, M.; Lord, A.; Hughes, L.; Goldring, S.R.; Purdue, E.; Murray, D.; et al. Nano-analyses of wear particles from metal-on-metal and non-metal-on-metal dual modular neck hip arthroplasty. Nanomed. Nanotechnol. Biol. Med. 2017, 13, 1205–1217. [Google Scholar] [CrossRef]
- Sands, D.; Schemitsch, E.H. The Role of Metal-on-Metal Bearings in Total Hip Arthroplasty and Hip Resurfacing. HSS J. 2017, 13, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Bozic, K.J.; Kurtz, S.; Lau, E.; Ong, K.; Chiu, V.; Vail, T.P.; Rubash, H.E.; Berry, D.J. The epidemiology of bearing surface usage in total hip arthroplasty in the United States. J. Bone Jt. Surg. Ser. A 2009, 91, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Matusiewicz, H. Potential release of in vivo trace metals from metallic medical implants in the human body: From ions to nanoparticles—A systematic analytical review. Acta Biomater. 2014, 10, 2379–2403. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, I.; Brown, C.; Schins, R.; Singh, S.; Newson, R.; Davis, S.; Fisher, J.; Ingham, E.; Case, C.P. The effect of nano- and micron-sized particles of cobalt-chromium alloy on human fibroblasts in vitro. Biomaterials 2007, 28, 2946–2958. [Google Scholar] [CrossRef]
- Urban, R.M.; Jacobs, J.J.; Tomlinson, M.J.; Gavrilovic, J.; Black, J.; Peoc’h, M. Dissemination of wear particles to the liver, spleen, and abdominal lymph nodes of patients with hip or knee replacement. J. Bone Jt. Surg. Ser. A 2000, 82, 457–477. [Google Scholar] [CrossRef]
- Drummond, J.; Tran, P.; Fary, C. Metal-on-Metal Hip Arthroplasty: A Review of Adverse Reactions and Patient Management. J. Funct. Biomater. 2015, 6, 486–499. [Google Scholar] [CrossRef] [Green Version]
- Onega, T.; Baron, J.; MacKenzie, T. Cancer after total joint arthroplasty: A meta-analysis. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1532–1537. [Google Scholar] [CrossRef] [Green Version]
- Gill, H.S.; Grammatopoulos, G.; Adshead, S.; Tsialogiannis, E.; Tsiridis, E. Molecular and immune toxicity of CoCr nanoparticles in MoM hip arthroplasty. Trends Mol. Med. 2012, 18, 145–155. [Google Scholar] [CrossRef]
- Jeffers, J.R.T.; Walter, W.L. Ceramic-on-ceramic bearings in hip arthroplasty: State of the art and the future. J. Bone Jt. Surg. Ser. B 2012, 94, 735–745. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.Y.; Yoon, T.R. Recent updates for biomaterials used in total hip arthroplasty. Biomater. Res. 2018, 22, 33. [Google Scholar] [CrossRef]
- Zhang, Y.F.; Zheng, Y.F.; Qin, L. A comprehensive biological evaluation of ceramic nanoparticles as wear debris. Nanomed. Nanotechnol. Biol. Med. 2011, 7, 975–982. [Google Scholar] [CrossRef]
- Wooley, P.H. How Has the Introduction of New Bearing Surfaces Altered the Biological Reactions to Byproducts of Wear and Modularity? Clin. Orthop. Relat. Res. 2014, 472, 3699–3708. [Google Scholar] [CrossRef] [Green Version]
- Bijukumar, D.R.; Segu, A.; Souza, J.C.M.; Li, X.J.; Barba, M.; Mercuri, L.G.; Jacobs, J.J.; Mathew, M.T. Systemic and local toxicity of metal debris released from hip prostheses: A review of experimental approaches. Nanomed. Nanotechnol. Biol. Med. 2018, 14, 951–963. [Google Scholar] [CrossRef]
- Behl, B.; Papageorgiou, I.; Brown, C.; Hall, R.; Tipper, J.L.; Fisher, J.; Ingham, E. Biological effects of cobalt-chromium nanoparticles and ions on dural fibroblasts and dural epithelial cells. Biomaterials 2013, 34, 3547–3558. [Google Scholar] [CrossRef] [Green Version]
- Taterra, D.; Skinningsrud, B.; Pękala, P.A.; Tomaszewska, I.M.; Marycz, K.; Radomski, M.W.; Tomaszewski, K.A. In vitro effects of cobalt and chromium nanoparticles on human platelet function. Nanotoxicology 2021, 15, 52–65. [Google Scholar] [CrossRef]
- Hassanpour, P.; Panahi, Y.; Ebrahimi-Kalan, A.; Akbarzadeh, A.; Davaran, S.; Nasibova, A.N.; Khalilov, R.; Kavetskyy, T. Biomedical applications of aluminium oxide nanoparticles. Micro Nano Lett. 2018, 13, 1227–1231. [Google Scholar] [CrossRef]
- Wang, L.; Hu, C.; Shao, L. The antimicrobial activity of nanoparticles: Present situation and prospects for the future. Int. J. Nanomed. 2017, 12, 1227–1249. [Google Scholar] [CrossRef] [Green Version]
- Ansari, M.A.; Khan, H.M.; Alzohairy, M.A.; Jalal, M.; Ali, S.G.; Pal, R.; Musarrat, J. Green synthesis of Al2O3 nanoparticles and their bactericidal potential against clinical isolates of multi-drug resistant Pseudomonas aeruginosa. World J. Microbiol. Biotechnol. 2015, 31, 153–164. [Google Scholar] [CrossRef]
- Faye, P.A.; Roualdes, O.; Rossignol, F.; Hartmann, D.J.; Desmoulière, A. Engulfment of ceramic particles by fibroblasts does not alter cell behavior. Biomed. Mater. 2017, 12, 015023. [Google Scholar] [CrossRef]
- Tsaousi, A.; Jones, E.; Case, C.P. The in vitro genotoxicity of orthopaedic ceramic (Al2O3) and metal (CoCr alloy) particles. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2010, 697, 1–9. [Google Scholar] [CrossRef]
- Yamamoto, A.; Honma, R.; Sumita, M.; Hanawa, T. Cytotoxicity evaluation of ceramic particles of different sizes and shapes. J. Biomed. Mater. Res. Part A 2004, 68, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Catelas, I.; Petit, A.; Marchand, R.; Zukor, D.J.; Yahia, L.; Huk, O.L. Cytotoxicity and macrophage cytokine release induced by ceramic and polyethylene particles in vitro. J. Bone Jt. Surg. Ser. B 1999, 81, 516–521. [Google Scholar] [CrossRef]
- Pedersen, A.B.; Mehnert, F.; Sorensen, H.T.; Emmeluth, C.; Overgaard, S.; Johnsen, S.P. The risk of venous thromboembolism, myocardial infarction, stroke, major bleeding and death in patients undergoing total hip and knee replacement: A 15-year retrospective cohort study of routine clinical practice. Bone Joint J. 2014, 96, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Radomski, A.; Jurasz, P.; Alonso-Escolano, D.; Drews, M.; Morandi, M.; Malinski, T.; Radomski, M.W. Nanoparticle-induced platelet aggregation and vascular thrombosis. Br. J. Pharmacol. 2005, 146, 882–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mills, N.L.; Törnqvist, H.; Gonzalez, M.C.; Vink, E.; Robinson, S.D.; Söderberg, S.; Boon, N.A.; Donaldson, K.; Sandström, T.; Blomberg, A.; et al. Ischemic and Thrombotic Effects of Dilute Diesel-Exhaust Inhalation in Men with Coronary Heart Disease. N. Engl. J. Med. 2007, 357, 1075–1082. [Google Scholar] [CrossRef] [Green Version]
- Santos-Martinez, M.J.; Tomaszewski, K.A.; Medina, C.; Bazou, D.; Gilmer, J.F.; Radomski, M.W. Pharmacological characterization of nanoparticle-induced platelet microaggregation using quartz crystal microbalance with dissipation: Comparison with light aggregometry. Int. J. Nanomed. 2015, 10, 5107–5119. [Google Scholar] [CrossRef] [Green Version]
- Larkin, C.M.; Breen, E.P.; Tomaszewski, K.A.; Eisele, S.; Radomski, M.W.; Ryan, T.A.; Santos-Martinez, M.-J. Platelet microaggregation in sepsis examined by quartz crystal microbalance with dissipation technology. Platelets 2018, 29, 301–304. [Google Scholar] [CrossRef]
- Mochida, Y.; Boehler, M.; Salzer, M.; Bauer, T.W. Debris from failed ceramic-on-ceramic and ceramic-on-polyethylene hip prostheses. Clin. Orthop. Relat. Res. 2001, 389, 113–125. [Google Scholar] [CrossRef]
- Santos-Martinez, M.J.; Inkielewicz-Stepniak, I.; Medina, C.; Rahme, K.; D’Arcy, D.M.; Fox, D.; Holmes, J.D.; Zhang, H.; Radomski, M.W. The use of quartz crystal microbalance with dissipation (QCM-D) for studying nanoparticle-induced platelet aggregation. Int. J. Nanomed. 2012, 7, 243–255. [Google Scholar] [CrossRef] [Green Version]
- Tonda-Turo, C.; Carmagnola, I.; Ciardelli, G. Quartz crystal microbalance with dissipation monitoring: A powerful method to predict the in vivo behavior of bioengineered surfaces. Front. Bioeng. Biotechnol. 2018, 6, 158. [Google Scholar] [CrossRef]
- Fatisson, J.; Azari, F.; Tufenkji, N. Real-time QCM-D monitoring of cellular responses to different cytomorphic agents. Biosens. Bioelectron. 2011, 26, 3207–3212. [Google Scholar] [CrossRef] [Green Version]
- Badimon, L.; Padró, T.; Vilahur, G. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease. Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 60–74. [Google Scholar] [CrossRef] [Green Version]
- Abukabda, A.B.; Stapleton, P.A.; Nurkiewicz, T.R. Metal Nanomaterial Toxicity Variations within the Vascular System. Curr. Environ. Health Rep. 2016, 3, 379–391. [Google Scholar] [CrossRef] [Green Version]
- Feng, Q.; Liu, Y.; Huang, J.; Chen, K.; Huang, J.; Xiao, K. Uptake, distribution, clearance, and toxicity of iron oxide nanoparticles with different sizes and coatings. Sci. Rep. 2018, 8, 2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Gong, Y.; Liao, W.; Luo, Y.; Wu, C.; Wang, M.; Yang, Q. A review of cardiovascular toxicity of TiO2, ZnO and Ag nanoparticles (NPs). BioMetals 2018, 31, 457–476. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, E. Action of Nanoparticles on Platelet Activation and Plasmatic Coagulation. Curr. Med. Chem. 2016, 23, 408–430. [Google Scholar] [CrossRef] [Green Version]
- Baptista, P.V.; McCusker, M.P.; Carvalho, A.; Ferreira, D.A.; Mohan, N.M.; Martins, M.; Fernandes, A.R. Nano-strategies to fight multidrug resistant bacteria—“A Battle of the Titans”. Front. Microbiol. 2018, 9, 1498. [Google Scholar] [CrossRef] [Green Version]
- Germain, M.A.; Hatton, A.; Williams, S.; Matthews, J.B.; Stone, M.H.; Fisher, J.; Ingham, E. Comparison of the cytotoxicity of clinically relevant cobalt-chromium and alumina ceramic wear particles in vitro. Biomaterials 2003, 24, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Radziun, E.; Dudkiewicz Wilczyńska, J.; Ksiazek, I.; Nowak, K.; Anuszewska, E.L.; Kunicki, A.; Olszyna, A.; Zabkowski, T. Assessment of the cytotoxicity of aluminium oxide nanoparticles on selected mammalian cells. Toxicol. Vitr. 2011, 25, 1694–1700. [Google Scholar] [CrossRef] [PubMed]
- Hannemann, F.; Hartmann, A.; Schmitt, J.; Lützner, J.; Seidler, A.; Campbell, P.; Delaunay, C.P.; Drexler, H.; Ettema, H.B.; García-Cimbrelo, E.; et al. European multidisciplinary consensus statement on the use and monitoring of metal-on-metal bearings for total hip replacement and hip resurfacing. Orthop. Traumatol. Surg. Res. 2013, 99, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Reito, A.; Berryman, F.; Young, S.; Pandit, H.G.; Lainiala, O.; Eskelinen, A.; McConnell, J.; Judge, A.; Matharu, G.S.; Murray, D.W. Blood Metal Ion Thresholds to Identify Patients with Metal-on-Metal Hip Implants at Risk of Adverse Reactions to Metal Debris. J. Bone Jt. Surg. 2017, 99, 1532–1539. [Google Scholar] [CrossRef] [Green Version]
- Grammatopoulos, G.; Munemoto, M.; Pollalis, A.; Athanasou, N.A. Correlation of serum metal ion levels with pathological changes of ARMD in failed metal-on-metal-hip-resurfacing arthroplasties. Arch. Orthop. Trauma Surg. 2017, 137, 1129–1137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissinger, M.; Grübl, A.; Pöll, G. Serum-cobalt levels with metal-on-metal bearings in the cement-free total hip arthroplasty results covering two years; prospective study. Acta Chir. Orthop. Traumatol. Cech. 2011, 78, 410–415. [Google Scholar] [PubMed]
- Savarino, L.; Padovani, G.; Ferretti, M.; Greco, M.; Cenni, E.; Perrone, G.; Greco, F.; Baldini, N.; Giunti, A. Serum ion levels after ceramic-on-ceramic and metal-on-metal total hip arthroplasty: 8-Year minimum follow-up. J. Orthop. Res. 2008, 26, 1569–1576. [Google Scholar] [CrossRef] [PubMed]
- Grübl, A.; Weissinger, M.; Brodner, W.; Gleiss, A.; Giurea, A.; Gruber, M.; Pöll, G.; Meisinger, V.; Gottsauner-Wolf, F.; Kotz, R. Serum aluminium and cobalt levels after ceramic-on-ceramic and metal-on-metal total hip replacement. J. Bone Jt. Surg. Ser. B 2006, 88, 1003–1005. [Google Scholar] [CrossRef] [Green Version]
- Montague, S.J.; Patel, P.; Martin, E.M.; Slater, A.; Quintanilla, L.G.; Perrella, G.; Kardeby, C.; Nagy, M.; Mezzano, D.; Mendes, P.M.; et al. Platelet activation by charged ligands and nanoparticles: Platelet glycoprotein receptors as pattern recognition receptors. Platelets 2021, 32, 1018–1030. [Google Scholar] [CrossRef]
- Dwivedi, M.V.; Harishchandra, R.K.; Koshkina, O.; Maskos, M.; Galla, H.-J. Size Influences the Effect of Hydrophobic Nanoparticles on Lung Surfactant Model Systems. Biophys. J. 2014, 106, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Tomaszewski, K.A.; Radomski, M.W.; Santos-Martinez, M.J. Nanodiagnostics, nanopharmacology and nanotoxicology of platelet-vessel wall interactions. Nanomedicine 2015, 10, 1451–1475. [Google Scholar] [CrossRef]
- Smyth, E.; Solomon, A.; Vydyanath, A.; Luther, P.K.; Pitchford, S.; Tetley, T.D.; Emerson, M. Induction and enhancement of platelet aggregation in vitro and in vivo by model polystyrene nanoparticles. Nanotoxicology 2015, 9, 356–364. [Google Scholar] [CrossRef]
- Van Kruchten, R.; Braun, A.; Feijge, M.A.H.; Kuijpers, M.J.E.; Rivera-Galdos, R.; Kraft, P.; Stoll, G.; Kleinschnitz, C.; Bevers, E.M.; Nieswandt, B.; et al. Antithrombotic potential of blockers of store-operated calcium channels in platelets. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 1717–1723. [Google Scholar] [CrossRef]
- Jun, E.A.; Lim, K.M.; Kim, K.; Bae, O.N.; Noh, J.Y.; Chung, K.H.; Chung, J.H. Silver nanoparticles enhance thrombus formation through increased platelet aggregation and procoagulant activity. Nanotoxicology 2011, 5, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Saikia, J.; Mohammadpour, R.; Yazdimamaghani, M.; Northrup, H.; Hlady, V.; Ghandehari, H. Silica Nanoparticle–Endothelial Interaction: Uptake and Effect on Platelet Adhesion under Flow Conditions. ACS Appl. Bio Mater. 2018, 1, 1620–1627. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.; Westein, E.; Niego, B.; Hagemeyer, C.E. Shear-Dependent Platelet Aggregation: Mechanisms and Therapeutic Opportunities. Front. Cardiovasc. Med. 2019, 6, 141. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Syed, A.M.; MacMillan, P.; Rocheleau, J.V.; Chan, W.C.W. Flow Rate Affects Nanoparticle Uptake into Endothelial Cells. Adv. Mater. 2020, 32, 1906274. [Google Scholar] [CrossRef] [PubMed]
- Michalczuk, U.; PRzekop, R.; Moskal, A. The effect of selected nanoparticles on rheological properties of human blood. Bull. Polish Acad. Sci. Tech. Sci. 2022, 70, e140437. [Google Scholar] [CrossRef]
- Gomez-Garcia, M.J.; Doiron, A.L.; Steele, R.R.M.; Labouta, H.I.; Vafadar, B.; Shepherd, R.D.; Gates, I.D.; Cramb, D.T.; Childs, S.J.; Rinker, K.D. Nanoparticle localization in blood vessels: Dependence on fluid shear stress, flow disturbances, and flow-induced changes in endothelial physiology. Nanoscale 2018, 10, 15249–15261. [Google Scholar] [CrossRef] [PubMed]
- Urban, R.M.; Tomlinson, M.J.; Hall, D.J.; Jacobs, J.J. Accumulation in liver and spleen of metal particles generated at nonbearing surfaces in hip arthroplasty. J. Arthroplast. 2004, 19, 94–101. [Google Scholar] [CrossRef]
- Radomski, M.; Moncada, S. An improved method for washing of human platelets with prostacyclin. Thromb. Res. 1983, 30, 383–389. [Google Scholar] [CrossRef]
- Shattil, S.J.; Cunningham, M.; Hoxie, J.A. Detection of activated platelets in whole blood using activation-dependent monoclonal antibodies and flow cytometry. Blood 1987, 70, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Sauerbrey, G. Verwendung von Schwingquarzen zur Wägung dünner Schichten und zur Mikrowägung. Z. Für Phys. 1959, 155, 206–222. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nanoparticles | Zeta Size (SD), nm | Polydispersity Index (SD) | Zeta Potential, mV | |||
|---|---|---|---|---|---|---|
| PPP | DDH20 | PPP | DDH20 | PPP | DDH20 | |
| Al2O3 5 nm | 239 | 680 (83.3) | 0.538 | 0.587 (0.069) | - | 62.6 |
| Al2O3 10 nm | 42.8 | 93.1 (0.98) | 0.320 | 0.219 (0.014) | - | 46.0 |
| Al2O3 20 nm | 9.51 | 39.1 (0.74) | 0.425 | 0.462 (0.052) | - | 16.8 |
| Al2O3 30 nm | 43.9 | 89.8 (0.26) | 0.447 | 0.245 (0.006) | - | 47.7 |
| Al2O3 50 nm | 113 | 152 (1.01) | 0.141 | 0.172 (0.027) | - | 50.5 |
| Al2O3 80 nm | 614 | 1158 (156.00) | 0.543 | 0.606 (0.132) | - | 1.46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taterra, D.; Skinningsrud, B.; Lauritzen, S.; Pękala, P.A.; Szwedowski, D.; Tomaszewska, I.M.; Tomaszewski, K.A. Aluminum Nanoparticles Affect Human Platelet Function In Vitro. Int. J. Mol. Sci. 2023, 24, 2547. https://doi.org/10.3390/ijms24032547
Taterra D, Skinningsrud B, Lauritzen S, Pękala PA, Szwedowski D, Tomaszewska IM, Tomaszewski KA. Aluminum Nanoparticles Affect Human Platelet Function In Vitro. International Journal of Molecular Sciences. 2023; 24(3):2547. https://doi.org/10.3390/ijms24032547
Chicago/Turabian StyleTaterra, Dominik, Bendik Skinningsrud, Sigurd Lauritzen, Przemysław A. Pękala, Dawid Szwedowski, Iwona M. Tomaszewska, and Krzysztof A. Tomaszewski. 2023. "Aluminum Nanoparticles Affect Human Platelet Function In Vitro" International Journal of Molecular Sciences 24, no. 3: 2547. https://doi.org/10.3390/ijms24032547
APA StyleTaterra, D., Skinningsrud, B., Lauritzen, S., Pękala, P. A., Szwedowski, D., Tomaszewska, I. M., & Tomaszewski, K. A. (2023). Aluminum Nanoparticles Affect Human Platelet Function In Vitro. International Journal of Molecular Sciences, 24(3), 2547. https://doi.org/10.3390/ijms24032547