

Enumeration and Characterization of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Characteristics of the Study Population
2.2. Relationship between the Clinicopathological Features of the Patients and the CTC Count
2.3. Prognostic Value of CTC Count in HCC Patients Undergoing TACE
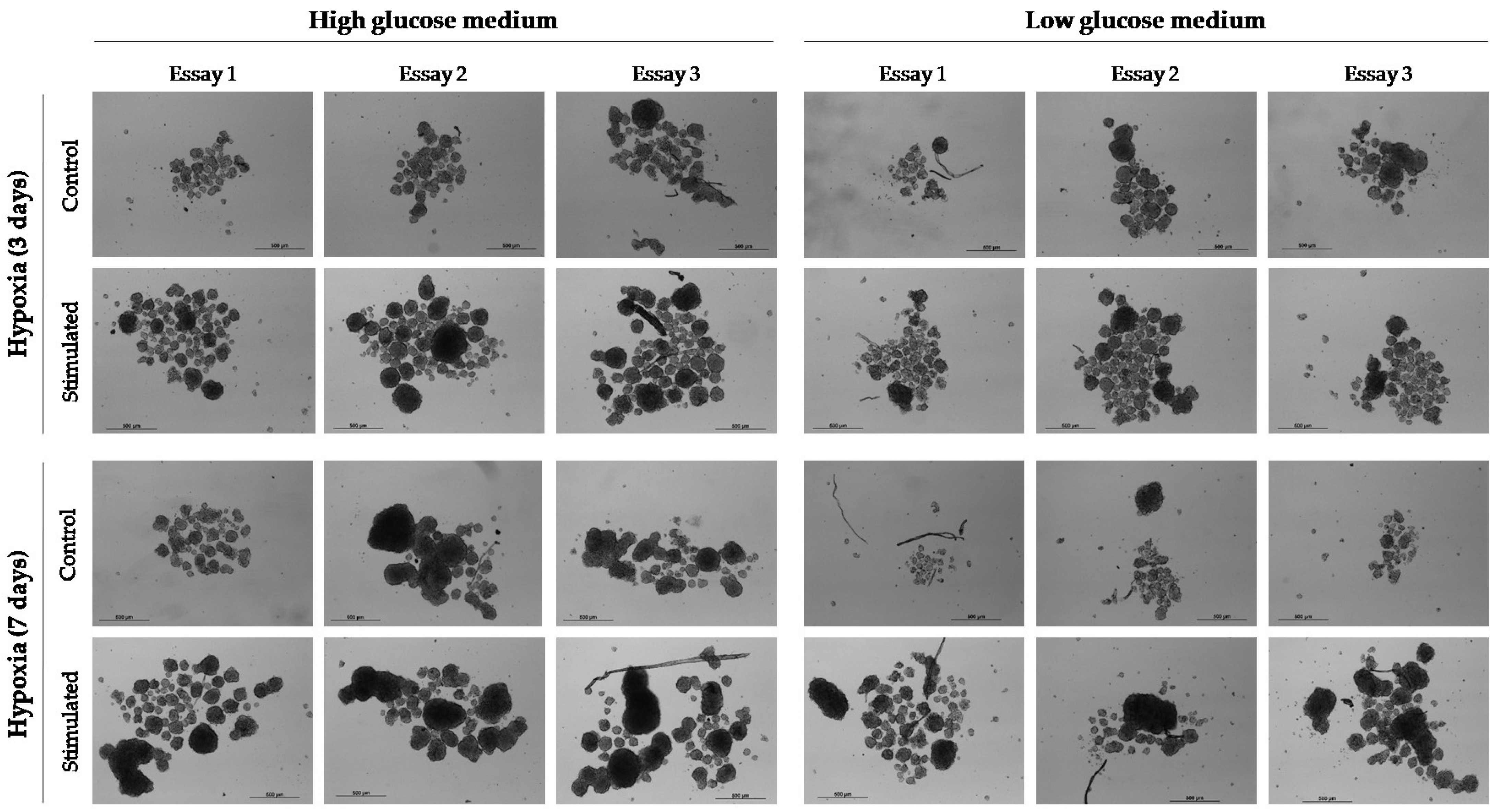
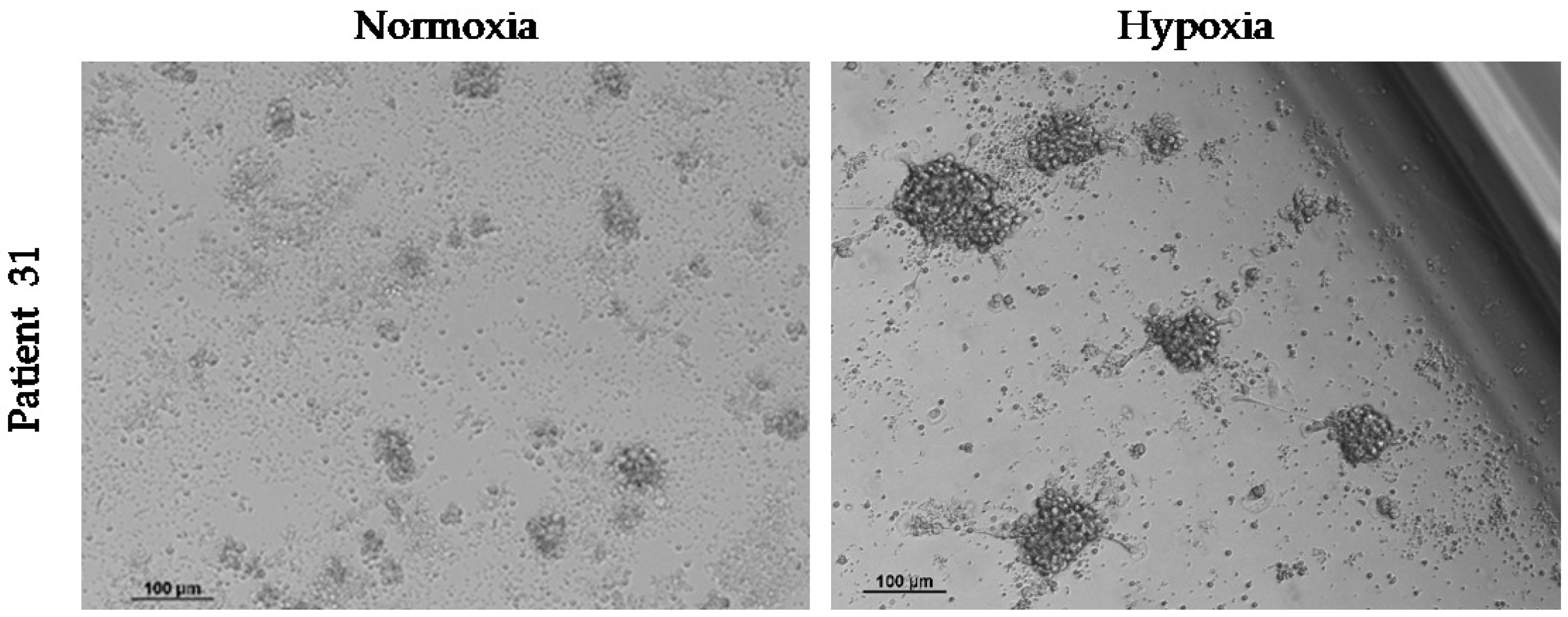
2.4. Ex Vivo Culture of CTCs
2.4.1. Culture of EpCAM+ CTCs Isolated by the IsoFlux System
2.4.2. Culture of CD45− CTCs Isolated by Negative Enrichment
3. Discussion
4. Materials and Methods
4.1. Study Design, Population, and TACE Procedure
4.2. Evaluation of Tumor Vascularity
4.3. Sample Collection and Data Management
4.4. Cell Culture
4.5. CTC Isolation from Peripheral Blood
4.5.1. Positive Enrichment of CTCs and the IsoFlux System
4.5.2. Negative Enrichment of CTCs
4.6. CTC Immunolabeling and Enumeration
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luo, Y.T.; Cheng, J.; Feng, X.; He, S.J.; Wang, Y.W.; Huang, Q. The Viable Circulating Tumor Cells with Cancer Stem Cells Feature, Where Is the Way Out? J. Exp. Clin. Cancer Res. 2018, 37, 38. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lingala, S.; Khoobyari, S.; Nolta, J.; Zern, M.A.; Wu, J. Epithelial Mesenchymal Transition and Hedgehog Signaling Activation Are Associated with Chemoresistance and Invasion of Hepatoma Subpopulations. J. Hepatol. 2011, 55, 838–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamashita, T.; Ji, J.; Budhu, A.; Forgues, M.; Yang, W.; Wang, H.-Y.; Jia, H.; Ye, Q.; Qin, L.-X.; Wauthier, E.; et al. EpCAM-Positive Hepatocellular Carcinoma Cells Are Tumor-Initiating Cells with Stem/Progenitor Cell Features. Gastroenterology 2009, 136, 1012–1024. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.-F.; Xu, Y.; Yang, X.-R.; Guo, W.; Zhang, X.; Qiu, S.-J.; Shi, R.-Y.; Hu, B.; Zhou, J.; Fan, J. Circulating Stem Cell-like Epithelial Cell Adhesion Molecule-Positive Tumor Cells Indicate Poor Prognosis of Hepatocellular Carcinoma after Curative Resection. Hepatology 2013, 57, 1458–1468. [Google Scholar] [CrossRef] [PubMed]
- Espejo-Cruz, M.L.; González-Rubio, S.; Zamora-Olaya, J.; Amado-Torres, V.; Alejandre, R.; Sánchez-Frías, M.; Ciria, R.; De la Mata, M.; Rodríguez-Perálvarez, M.; Ferrín, G. Circulating Tumor Cells in Hepatocellular Carcinoma: A Comprehensive Review and Critical Appraisal. Int. J. Mol. Sci. 2021, 22, 13073. [Google Scholar] [CrossRef]
- Yu, M.; Bardia, A.; Aceto, N.; Bersani, F.; Madden, M.W.; Donaldson, M.C.; Desai, R.; Zhu, H.; Comaills, V.; Zheng, Z.; et al. Cancer Therapy. Ex Vivo Culture of Circulating Breast Tumor Cells for Individualized Testing of Drug Susceptibility. Science 2014, 345, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Shi, L.; Zhang, X.; Sun, B.; Yang, Y.; Ge, N.; Liu, H.; Yang, X.; Chen, L.; Qian, H.; et al. PERK/PAkt Phenotyping in Circulating Tumor Cells as a Biomarker for Sorafenib Efficacy in Patients with Advanced Hepatocellular Carcinoma. Oncotarget 2015, 7, 2646–2659. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.-J.; Pan, Y.-D.; Pei, X.-Y.; Chen, H.; Nguyen, S.; Kashyap, A.; Liu, J.; Wu, J. Capturing Circulating Tumor Cells of Hepatocellular Carcinoma. Cancer Lett. 2012, 326, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, X.; Zhang, J.; Sun, B.; Zheng, L.; Li, J.; Liu, S.; Sui, G.; Yin, Z. Microfluidic Chip for Isolation of Viable Circulating Tumor Cells of Hepatocellular Carcinoma for Their Culture and Drug Sensitivity Assay. Cancer Biol. Ther. 2016, 17, 1177–1187. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Salam, I.M.; Awadein, N.E.-S.; Ashour, M. Cytotoxicity of Luffa Cylindrica (L.) M.Roem. Extract against Circulating Cancer Stem Cells in Hepatocellular Carcinoma. J. Ethnopharmacol. 2019, 229, 89–96. [Google Scholar] [CrossRef]
- Sánchez-Lorencio, M.I.; Ramirez, P.; Saenz, L.; Martínez Sánchez, M.V.; De La Orden, V.; Mediero-Valeros, B.; Veganzones-De-Castro, S.; Baroja-Mazo, A.; Revilla Nuin, B.; Gonzalez, M.R.; et al. Comparison of Two Types of Liquid Biopsies in Patients With Hepatocellular Carcinoma Awaiting Orthotopic Liver Transplantation. Transplant. Proc. 2015, 47, 2639–2642. [Google Scholar] [CrossRef] [PubMed]
- Li, T.-J.; Lin, T.-W.; Wu, S.-P.; Chu, H.-T.; Kuo, Y.-H.; Chiou, J.-F.; Lu, L.-S.; Chen, C.-C. Patient-Derived Tumor Chemosensitization of GKB202, an Antrodia Cinnamomea Mycelium-Derived Bioactive Compound. Molecules 2021, 26, 6018. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.-L.; Zhang, Y.-J.; Zhang, X.-F.; Fei, X.; Zhang, H.; Li, C.-G.; Sun, B. 3D Culture of Circulating Tumor Cells for Evaluating Early Recurrence and Metastasis in Patients with Hepatocellular Carcinoma. Onco Targets Ther. 2021, 14, 2673–2688. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Cheng, H.; Yang, X.; Liu, G. Superstable Homogeneous Iodinated Formulation Technology: Revolutionizing Transcatheter Arterial Chemoembolization. Sci. Bull. 2020, 65, 1685–1687. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, L.; Zhao, D.; Yue, S.; Sun, H.; Ni, C.; Zhong, Z. Polymersome-Stabilized Doxorubicin-Lipiodol Emulsions for High-Efficacy Chemoembolization Therapy. J. Control. Release 2022, 350, 122–131. [Google Scholar] [CrossRef]
- Llovet, J.M.; Bruix, J. Systematic Review of Randomized Trials for Unresectable Hepatocellular Carcinoma: Chemoembolization Improves Survival. Hepatology 2003, 37, 429–442. [Google Scholar] [CrossRef] [Green Version]
- Shimada, Y.; Sudo, T.; Akamatsu, S.; Sunada, T.; Myomoto, A.; Okano, K.; Shimizu, K. Cell Lines of Circulating Tumor Cells: What Is Known and What Needs to Be Resolved. J. Pers. Med. 2022, 12, 666. [Google Scholar] [CrossRef]
- Xie, W.; Yin, T.; Chen, Y.-L.; Zhu, D.-M.; Zan, M.-H.; Chen, B.; Ji, L.-W.; Chen, L.; Guo, S.-S.; Huang, H.-M.; et al. Capture and “Self-Release” of Circulating Tumor Cells Using Metal-Organic Framework Materials. Nanoscale 2019, 11, 8293–8303. [Google Scholar] [CrossRef]
- Fan, X.; Liu, S.; Su, F.; Pan, Q.; Lin, T. Effective Enrichment of Prostate Cancer Stem Cells from Spheres in a Suspension Culture System. Urol. Oncol. 2012, 30, 314–318. [Google Scholar] [CrossRef]
- De Sousa, G.R.; Vieira, G.M.; das Chagas, P.F.; Pezuk, J.A.; Brassesco, M.S. Should We Keep Rocking? Portraits from Targeting Rho Kinases in Cancer. Pharmacol. Res. 2020, 160, 105093. [Google Scholar] [CrossRef] [PubMed]
- Ohata, H.; Ishiguro, T.; Aihara, Y.; Sato, A.; Sakai, H.; Sekine, S.; Taniguchi, H.; Akasu, T.; Fujita, S.; Nakagama, H.; et al. Induction of the Stem-like Cell Regulator CD44 by Rho Kinase Inhibition Contributes to the Maintenance of Colon Cancer-Initiating Cells. Cancer Res. 2012, 72, 5101–5110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhandary, L.; Whipple, R.A.; Vitolo, M.I.; Charpentier, M.S.; Boggs, A.E.; Chakrabarti, K.R.; Thompson, K.N.; Martin, S.S. ROCK Inhibition Promotes Microtentacles That Enhance Reattachment of Breast Cancer Cells. Oncotarget 2015, 6, 6251–6266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imamura, F.; Mukai, M.; Ayaki, M.; Akedo, H. Y-27632, an Inhibitor of Rho-Associated Protein Kinase, Suppresses Tumor Cell Invasion via Regulation of Focal Adhesion and Focal Adhesion Kinase. Jpn. J. Cancer Res. 2000, 91, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-S.; Joe, Y.A. A ROCK Inhibitor Blocks the Inhibitory Effect of Chondroitin Sulfate Proteoglycan on Morphological Changes of Mesenchymal Stromal/Stem Cells into Neuron-Like Cells. Biomol. Ther. 2013, 21, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; An, J.M.; Seo, J.T.; Seo, S.R. Y-27632 Induces Neurite Outgrowth by Activating the NOX1-Mediated AKT and PAK1 Phosphorylation Cascades in PC12 Cells. Int. J. Mol. Sci. 2020, 21, 7679. [Google Scholar] [CrossRef]
- Jobling, P.; Pundavela, J.; Oliveira, S.M.R.; Roselli, S.; Walker, M.M.; Hondermarck, H. Nerve-Cancer Cell Cross-Talk: A Novel Promoter of Tumor Progression. Cancer Res. 2015, 75, 1777–1781. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Fan, C.; Shangguan, W.; Liu, Y.; Li, Y.; Shang, Y.; Yin, D.; Zhang, S.; Huang, Q.; Li, X.; et al. Neurons Generated from Carcinoma Stem Cells Support Cancer Progression. Sig. Transduct. Target Ther. 2017, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zheng, Q.; Lu, Z.; Wang, L.; Ding, L.; Xia, L.; Zhang, H.; Wang, M.; Chen, Y.; Li, G. Role of the Nervous System in Cancers: A Review. Cell Death Discov. 2021, 7, 76. [Google Scholar] [CrossRef]
- Chua, T.C.; Liauw, W.; Saxena, A.; Chu, F.; Glenn, D.; Chai, A.; Morris, D.L. Systematic Review of Neoadjuvant Transarterial Chemoembolization for Resectable Hepatocellular Carcinoma. Liver Int. 2010, 30, 166–174. [Google Scholar] [CrossRef]
- Nahm, J.H.; Rhee, H.; Kim, H.; Yoo, J.E.; San Lee, J.; Jeon, Y.; Choi, G.H.; Park, Y.N. Increased Expression of Stemness Markers and Altered Tumor Stroma in Hepatocellular Carcinoma under TACE-Induced Hypoxia: A Biopsy and Resection Matched Study. Oncotarget 2017, 8, 99359–99371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulze, K.; Gasch, C.; Staufer, K.; Nashan, B.; Lohse, A.W.; Pantel, K.; Riethdorf, S.; Wege, H. Presence of EpCAM-Positive Circulating Tumor Cells as Biomarker for Systemic Disease Strongly Correlates to Survival in Patients with Hepatocellular Carcinoma. Int. J. Cancer 2013, 133, 2165–2171. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Magbanua, M.J.M.; Butler, T.M.; Collisson, E.A.; Hwang, J.; Sidiropoulos, N.; Evason, K.; McWhirter, R.M.; Hameed, B.; Wayne, E.M.; et al. Circulating Tumor Cells in Hepatocellular Carcinoma: A Pilot Study of Detection, Enumeration, and next-Generation Sequencing in Cases and Controls. BMC Cancer 2015, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Yang, X.-R.; Sun, Y.-F.; Shen, M.-N.; Ma, X.-L.; Wu, J.; Zhang, C.-Y.; Zhou, Y.; Xu, Y.; Hu, B.; et al. Clinical Significance of EpCAM MRNA-Positive Circulating Tumor Cells in Hepatocellular Carcinoma by an Optimized Negative Enrichment and QRT-PCR–Based Platform. Clin. Cancer Res. 2014, 20, 4794–4805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, J.; Wang, W.-S.; Zhu, X.-L.; Ni, C.-F. High Epithelial Cell Adhesion Molecule-Positive Circulating Tumor Cell Count Predicts Poor Survival of Patients with Unresectable Hepatocellular Carcinoma Treated with Transcatheter Arterial Chemoembolization. J. Vasc. Interv. Radiol. 2018, 29, 1678–1684. [Google Scholar] [CrossRef]
- Wu, X.; Yang, C.; Yu, H.; Cao, F.; Shan, Y.; Zhao, W. The Predictive Values of Serum Dickkopf-1 and Circulating Tumor Cells in Evaluating the Efficacy of Transcatheter Arterial Chemoembolization Treatment on Hepatocellular Carcinoma. Medicine 2019, 98, e16579. [Google Scholar] [CrossRef]
- Deng, J.; Chen, W.; Wu, X.; Zhou, Y.; Li, J. Evaluating the Predictive Power of Circulating Tumor Cells for the Prognosis of Transarterial Chemoembolization Treatment on Patients with Advanced Hepatocellular Carcinoma. Medicine 2021, 100, e24060. [Google Scholar] [CrossRef]
- Fang, Z.-T.; Zhang, W.; Wang, G.-Z.; Zhou, B.; Yang, G.-W.; Qu, X.-D.; Liu, R.; Qian, S.; Zhu, L.; Liu, L.-X.; et al. Circulating Tumor Cells in the Central and Peripheral Venous Compartment—Assessing Hematogenous Dissemination after Transarterial Chemoembolization of Hepatocellular Carcinoma. Onco Targets Ther. 2014, 7, 1311–1318. [Google Scholar] [CrossRef] [Green Version]
- Vogl, T.J.; Riegelbauer, L.J.; Oppermann, E.; Kostantin, M.; Ackermann, H.; Trzmiel, A.; Stein, S.; Eichler, K.; Zharov, V.P.; Roy, D.; et al. Early Dynamic Changes in Circulating Tumor Cells and Prognostic Relevance Following Interventional Radiological Treatments in Patients with Hepatocellular Carcinoma. PLoS ONE 2021, 16, e0246527. [Google Scholar] [CrossRef]
- Nel, I.; Jehn, U.; Gauler, T.; Hoffmann, A.-C. Individual Profiling of Circulating Tumor Cell Composition in Patients with Non-Small Cell Lung Cancer Receiving Platinum Based Treatment. Transl. Lung Cancer Res. 2014, 3, 100–106. [Google Scholar] [CrossRef]
- Lustberg, M.B.; Balasubramanian, P.; Miller, B.; Garcia-Villa, A.; Deighan, C.; Wu, Y.; Carothers, S.; Berger, M.; Ramaswamy, B.; Macrae, E.R.; et al. Heterogeneous Atypical Cell Populations Are Present in Blood of Metastatic Breast Cancer Patients. Breast Cancer Res. 2014, 16, R23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Zhang, X.M.; Zhou, X.P.; Tang, W.; Guan, Y.S.; Zhai, Z.H.; Dong, G.L. Correlation between Tumor Perfusion and Lipiodol Deposition in Hepatocellular Carcinoma after Transarterial Chemoembolization. J. Vasc. Interv. Radiol. 2010, 21, 1841–1846. [Google Scholar] [CrossRef]
- Müller, L.; Stoehr, F.; Mähringer-Kunz, A.; Hahn, F.; Weinmann, A.; Kloeckner, R. Current Strategies to Identify Patients That Will Benefit from TACE Treatment and Future Directions a Practical Step-by-Step Guide. J. Hepatocell Carcinoma 2021, 8, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Küsters, B.; Kats, G.; Roodink, I.; Verrijp, K.; Wesseling, P.; Ruiter, D.J.; de Waal, R.M.W.; Leenders, W.P.J. Micronodular Transformation as a Novel Mechanism of VEGF-A-Induced Metastasis. Oncogene 2007, 26, 5808–5815. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, T.; Yui, Y.; Naka, N.; Wakamatsu, T.; Yoshioka, K.; Araki, N.; Yoshikawa, H.; Itoh, K. Dynamic Analysis of Lung Metastasis by Mouse Osteosarcoma LM8: VEGF Is a Candidate for Anti-Metastasis Therapy. Clin. Exp. Metastasis 2013, 30, 369–379. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Perálvarez, M. Transient Cytolysis after Transarterial Chemoembolization in Patients with Hepatocellular Carcinoma. J. Pers. Med. 2022, 12, 1663. [Google Scholar] [CrossRef] [PubMed]
- Garg, T.; Shrigiriwar, A.; Habibollahi, P.; Cristescu, M.; Liddell, R.P.; Chapiro, J.; Inglis, P.; Camacho, J.C.; Nezami, N. Intraarterial Therapies for the Management of Hepatocellular Carcinoma. Cancers 2022, 14, 3351. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J. Modified RECIST (MRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Hisai, H.; Kato, J.; Kobune, M.; Murakami, T.; Miyanishi, K.; Takahashi, M.; Yoshizaki, N.; Takimoto, R.; Terui, T.; Niitsu, Y. Increased Expression of Angiogenin in Hepatocellular Carcinoma in Correlation with Tumor Vascularity. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 4852–4859. [Google Scholar]
- Amado, V.; González-Rubio, S.; Zamora, J.; Alejandre, R.; Espejo-Cruz, M.L.; Linares, C.; Sánchez-Frías, M.; García-Jurado, G.; Montero, J.L.; Ciria, R.; et al. Clearance of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Surgical Resection or Liver Transplantation. Cancers 2021, 13, 2476. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Age (years) | 63.5 ± 7.9 |
| Sex (male), n (%) | 34 (91.9%) |
| Etiology | |
| -Hepatitis C (yes), n (%) | 14 (37.8%) |
| -Hepatitis B (yes), n (%) | 5 (13.5%) |
| -Alcohol (yes), n (%) | 27 (73.0%) |
| -NAFLD (yes), n (%) | 4 (10.8%) |
| Child–Pugh score, n (%) | |
| -A | 32 (86.5%) |
| -B | 5 (13.5%) |
| MELD score | 9.0 (IQR 8.0–11.0) |
| BCLC stage, n (%) | |
| -0 | 1 (2.7%) |
| -A | 25 (67.6%) |
| -B | 8 (21.6%) |
| -C | 3 (8.1%) |
| Portal hypertension (yes), n (%) | 31 (83.8%) |
| Number of nodules, n (%) | |
| -Single nodule | 18 (48.6%) |
| -Two nodules | 11 (29.7%) |
| -Three nodules | 3 (8.1%) |
| -Four nodules | 5 (13.5%) |
| Main nodule diameter (cm) | 3.0 (IQR 2.0–4.1) |
| Total tumor diameter (cm) | 3.8 (IQR 2.9–5.7) |
| Number of treated nodules, n (%) | |
| -Single nodule | 22 (59.5%) |
| -Two nodules | 12 (32.4%) |
| -Four nodules | 3 (8.1%) |
| AFP (ng/mL) | 10.3 (IQR 3.7–49.0) |
| AST (U/L) | 35.0 (IQR 25.5–50.0) |
| ALT (U/L) | 26.0 (IQR 16.5–36.5) |
| GGT (U/L) | 76.0 (IQR 46.5–171.0) |
| Tumor vascularity, n (%) | |
| -Hypervascularity | 23 (62.2%) |
| -Moderate vascularity | 8 (21.6%) |
| -Hypovascularity | 6 (16.2%) |
| Variable | CTC Count (n = 37; 100.0%) | Cluster Presence (n = 20; 54.1%) | |||
|---|---|---|---|---|---|
| Patients n (%) | CD45− CK+ Cells | Patients n (%) | p | ||
| Median (IQR) | p | ||||
| Age (years) | |||||
| -<65 | 18 (48.6%) | 36.5 (21.8–131.8) | 0.504 | 10 (27.0%) | 0.858 |
| -≥65 | 19 (51.4%) | 33.0 (14.0–56.0) | 10 (27.0%) | ||
| Sex (male) | 34 (91.9%) | 36.5 (21.8–95.0) | 0.824 | 18 (48.6%) | 1.000 |
| Etiology | |||||
| -Hepatitis C (yes) | 14(37.8%) | 33.5 (19.8–216.5) | 0.638 | 8 (21.6%) | 0.769 |
| -Hepatitis B (yes) | 5 (13.5%) | 49.0 (31.5–72.0) | 0.790 | 3 (8.1%) | 1.000 |
| -Alcohol (yes) | 27 (73.0%) | 39.0 (21.0–110.0) | 0.932 | 13 (35.1%) | 0.288 |
| -NAFLD (yes) | 4 (10.8%) | 36.0 (23.0–139.8) | 0.941 | 3 (8.1%) | 0.609 |
| Child–Pugh score | |||||
| -A | 32 (86.5%) | 36.5 (21.3–88.3) | 0.722 | 17 (45.9%) | 1.000 |
| -B | 5 (13.5%) | 24.0 (18.0–896.5) | 3 (8.1%) | ||
| MELD score | |||||
| -<9 | 14 (37.8%) | 36.5 (20.5–62.8) | 0.826 | 5 (13.5%) | 0.081 |
| -≥9 | 23 (62.2%) | 33.0 (21.0–119.0) | 15 (40.5%) | ||
| BCLC stage | |||||
| -0-A | 26 (70.3%) | 33.5 (21.8–111.8) | 0.842 | 12 (32.4%) | 0.169 |
| -B-C | 11 (29.7%) | 39.0 (14.0–90.0) | 8 (21.6%) | ||
| Portal hypertension (yes) | 31 (83.8%) | 34.0 (16.0–110.0) | 0.650 | 16 (43.2%) | 0.667 |
| Number of nodules | |||||
| -Single nodule | 18 (48.6%) | 32.5 (21.8–112.3) | 0.915 | 9 (24.3%) | 0.630 |
| -Multinodular | 19 (51.4%) | 39.0 (16.0–90.0) | 11 (29.7%) | ||
| Main nodule diameter (cm) | |||||
| -<3 | 17 (45.9%) | 54.0 (27.0–157.5) | 0.131 | 11(29.7%) | 0.231 |
| -≥3 | 20 (54.1%) | 25.0 (17.5–54.3) | 9 (24.3%) | ||
| Total tumor diameter (cm) | |||||
| -<5 | 24 (64.9%) | 41.5 (21.3–115.3) | 0.656 | 14 (37.8%) | 0.478 |
| -≥5 | 13 (35.1%) | 31.0 (19.5–72.0) | 6 (16.2%) | ||
| Number of treated nodules | |||||
| -Single nodule | 22 (59.5%) | 33.5 (22.8–89.8) | 0.938 | 12 (32.4%) | 0.942 |
| ->1 nodule | 15 (40.5%) | 49.0 (14.0–117.0) | 8 (21.6%) | ||
| AFP (ng/mL) | |||||
| -Normal (<9) | 17 (45.9%) | 49.0 (22.5–104.5) | 0.498 | 8 (22.9%) | 0.404 |
| -Abnormal (≥9) | 18 (48.6%) | 33.0 (15.5–68.8) | 11 (31.4%) | ||
| -Missing | 2 (5.4%) | ||||
| AST (U/L) | |||||
| -Normal (<35) | 18 (48.6%) | 44.0 (22.5–112.3) | 0.670 | 11 (29.7%) | 0.402 |
| -Abnormal (≥35) | 19 (51.4%) | 33.0 (16.0–56.0) | 9 (24.3%) | ||
| ALT (U/L) | |||||
| -Normal (<27) | 19 (51.4%) | 31.0 (14.0–110.0) | 0.637 | 13 (35.1%) | 0.072 |
| -Abnormal (≥27) | 18 (48.6%) | 41.5 (22.8–91.5) | 7 (18.9%) | ||
| GGT (U/L) | |||||
| -Normal (<75) | 17 (45.9%) | 33.0 (14.0–114.5) | 0.532 | 10 (27.0%) | 0.591 |
| -Abnormal (≥75) | 20 (54.1%) | 51.0 (23.0–88.3) | 10 (27.0%) | ||
| Tumor vascularity | |||||
| -Hypervascularity | 23 (62.2%) | 49.0 (23.0–119.0) | 0.026 | 13 (35.1%) | 0.699 |
| -Medium/hypo-vascularity | 14 (37.8%) | 23.5 (12.5–54.3) | 7 (18.9%) | ||
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Responder (n = 20; 54.1%) | Non-Responder (n = 17; 45.9%) | OR (95% CI) | p | OR (95% CI) | p | |
| Age (years) | 63.7 ±7.6 | 63.2±8.3 | 1.0 (0.9–1.1) | 0.871 | - | - |
| Etiology | ||||||
| -Hepatitis C (yes), n (%) | 8 (21.6%) | 6 (16.2%) | 0.8 (0.2–3.1) | 0.769 | - | - |
| -Hepatitis B (yes), n (%) | 2 (5.4%) | 3 (8.1%) | 1.9 (0.3–13.2) | 0.503 | - | - |
| -Alcohol (yes), n (%) | 13 (35.1%) | 14 (37.8%) | 2.5 (0.5–11.8) | 0.244 | - | - |
| -NAFLD (yes), n (%) | 3 (8.10%) | 1 (2.7%) | 0.4 (0.0–3.8) | 0.389 | - | - |
| Child–Pugh score, n (%) | ||||||
| -A | 17 (45.9%) | 15 (40.5%) | 1 (Ref.) | 0.775 | - | - |
| -B | 3 (8.1%) | 2 (5.4%) | 0.8 (0.1–5.1) | - | ||
| MELD score | 9.5 (IQR 7.3–11.0) | 9.0 (IQR 8.0–11.0) | 0.9 (0.7–1.2) | 0.428 | - | - |
| BCLC stage, n (%) | ||||||
| -0-A | 17 (45.9%) | 9 (24.3%) | 1 (Ref.) | 0.041 | - | - |
| -B-C | 3 (8.1%) | 8 (21.6%) | 5.0 (1.1–23.8) | - | ||
| Portal hypertension (yes), n (%) | 18 (48.6%) | 13 (35.1%) | 0.4 (0.1–2.3) | 0.278 | - | - |
| Number of nodules, n (%) | ||||||
| -Single nodule | 13 (35.1%) | 5 (13.5%) | 1 (Ref.) | 0.035 | - | - |
| -Multinodular | 7 (18.9%) | 12 (32.4%) | 4.5 (1.1–17.9) | - | ||
| Main nodule diameter (cm) | 2.5 (IQR 2.0–3.4) | 3.6 (IQR 2.2–4.8) | 1.8 (1.0–3.2) | 0.055 | - | - |
| Total tumor diameter (cm) | 3.3 ± 1.0 | 5.8 ± 2.5 | 2.2 (1.3–3.9) | 0.005 | 2.5 (1.3–4.8) | 0.006 |
| Number of treated nodules, n (%) | ||||||
| -Single nodule | 15 (40.5%) | 7 (18.9%) | 1 (Ref.) | 0.041 | - | - |
| ->1 nodule | 5 (13.5%) | 10 (27.0%) | 4.3 (1.1–17.4) | - | ||
| AFP (ng/mL) | 12.9 (IQR 4.9–49.0) | 6.0 (IQR 3.1–46.0) | 1.0 (1.0–1.0) | 0.956 | - | - |
| AST (U/L) | 34.0 (IQR 25.0–45.5) | 35.0 (IQR 26.5–63.5) | 1.0 (1.0–1.0) | 0.563 | - | - |
| ALT (U/L) | 28.0 (IQR 18.3–36.5) | 20.0 (IQR 16.0–38.5) | 1.0 (1.0–1.0) | 0.457 | - | - |
| GGT (U/L) | 86.5 (IQR 45.0–145.0) | 75.0 (IQR 51.5–177.5) | 1.0 (1.0–1.0) | 0.516 | - | - |
| CD45−CK+ CTC count | 49.0 (IQR 23.3–118.5) | 26.0 (IQR 14.0–55.0) | 1.0 (1.0–1.0) | 0.648 | - | - |
| CD45+CK+ cell count | 30.0 (IQR 15.3–71.5) | 26.0 (IQR 18.0–51.0) | 1.0 (1.0–1.0) | 0.386 | - | - |
| Total cell count (CD45−/+CK+) | 91.5 (IQR 45.3–154.8) | 48.0 (IQR 35.5–122.5) | 1.0 (1.0–1.0) | 0.822 | - | - |
| CTC clusters (yes), n (%) | 14 (37.8%) | 6 (16.2%) | 0.2 (0.1–0.9) | 0.039 | 0.2 (0.0–1.0) | 0.049 |
| Tumor vascularity, n (%) | ||||||
| -Hypervascularity | 12 (32.4%) | 11 (29.7) | 1 (Ref.) | 0.769 | - | - |
| -Medium/hypo-vascularity | 8 (21.6%) | 6 (16.2%) | 0.8 (0.2–3.1) | - | ||
| Variable | AUROC (95% CI) | SN (95% CI) | SP (95% CI) | PPV (95% CI) | NPV (95% CI) |
|---|---|---|---|---|---|
| Univariate analysis | |||||
| Number of nodules | 0.7 (0.5–0.9) | 72.2 (48.9–95.7) | 63.2 (38.8–87.5) | 65.0(41.6–88.4) | 70.6 (46.0–95.2) |
| Total tumor diameter | 0.8 (0.6–1.0) | 77.3 (57.5–97.1) | 80.0 (56.4–100.0) | 85.0 (66.9–100.0) | 70.6 (46.0–95.2) |
| Number of treated nodules | 0.7 (0.5–0.8) | 68.2 (46.5–89.9) | 66.7 (39.5–93.9) | 75.0 (53.5–96.5) | 58.8 (32.5–85.2) |
| CTC cluster presence | 0.7 (0.5–0.9) | 70.0 (74.4–92.6) | 64.7 (39.1–90.4) | 70.0 (47.4–92.6) | 64.7 (39.1–90.4) |
| Multivariate analysis | |||||
| Combination of total tumor diameter and presence of CTC cluster | 0.9 (0.7–1.0) | 81.8 (63.4–100.0) | 86.7 (66.1–100.0) | 90.0 (74.4–100.0) | 76.5 (53.4–99.6) |
| Overall Survival-Rates | 6 Months | 14 Months | 24 Months |
|---|---|---|---|
| ≤35 CTC (n = 19; 51.4%) | 79.6% | 69.7% | 52.3% |
| >35 CTC (n = 18; 48.6%) | 94.1% | 84.7% | 61.8% |
| CTC cluster absence (n = 17; 45.9%) | 92.9% | 81.3% | 60.9% |
| CTC cluster presence (n = 20; 54.1) | 83.2% | 83.2% | 54.6% |
| Patient Number | CSC Enrichment Method | Cell Culture Conditions | CSC Spheres |
|---|---|---|---|
| 01–11 | Positive enrichment (IsoFlux; EpCAM+ cells) | Normoxia | - |
| 12–15 | Negative enrichment (depletion of CD45+ cells) | Normoxia | - |
| 16 | √ | ||
| 17 | - | ||
| 18 | √ | ||
| 19 | - | ||
| 20 | √ | ||
| 21–23 | - | ||
| 24 | Negative enrichment (depletion of CD45+ cells) | Normoxia and Hypoxia | - |
| 25 | √ | ||
| 26–30 | - | ||
| 31 | √ | ||
| 32–33 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espejo-Cruz, M.L.; González-Rubio, S.; Espejo, J.J.; Zamora-Olaya, J.M.; Alejandre-Altamirano, R.M.; Prieto-Torre, M.; Linares, C.I.; Guerrero-Misas, M.; Barrera-Baena, P.; Poyato-González, A.; et al. Enumeration and Characterization of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. Int. J. Mol. Sci. 2023, 24, 2558. https://doi.org/10.3390/ijms24032558
Espejo-Cruz ML, González-Rubio S, Espejo JJ, Zamora-Olaya JM, Alejandre-Altamirano RM, Prieto-Torre M, Linares CI, Guerrero-Misas M, Barrera-Baena P, Poyato-González A, et al. Enumeration and Characterization of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. International Journal of Molecular Sciences. 2023; 24(3):2558. https://doi.org/10.3390/ijms24032558
Chicago/Turabian StyleEspejo-Cruz, María L., Sandra González-Rubio, Juan J. Espejo, Javier M. Zamora-Olaya, Rafael M. Alejandre-Altamirano, María Prieto-Torre, Clara I. Linares, Marta Guerrero-Misas, Pilar Barrera-Baena, Antonio Poyato-González, and et al. 2023. "Enumeration and Characterization of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization" International Journal of Molecular Sciences 24, no. 3: 2558. https://doi.org/10.3390/ijms24032558
APA StyleEspejo-Cruz, M. L., González-Rubio, S., Espejo, J. J., Zamora-Olaya, J. M., Alejandre-Altamirano, R. M., Prieto-Torre, M., Linares, C. I., Guerrero-Misas, M., Barrera-Baena, P., Poyato-González, A., Sánchez-Frías, M., Ayllón, M. D., Rodríguez-Perálvarez, M. L., de la Mata, M., & Ferrín, G. (2023). Enumeration and Characterization of Circulating Tumor Cells in Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization. International Journal of Molecular Sciences, 24(3), 2558. https://doi.org/10.3390/ijms24032558