
90K/Mac-2 BP Is a New Predictive Biomarker of Response to Infliximab Therapy in IBD Patients

 , , ,
, , , 
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Analysis of Serological and Fecal Parameters across Follow-Up Time
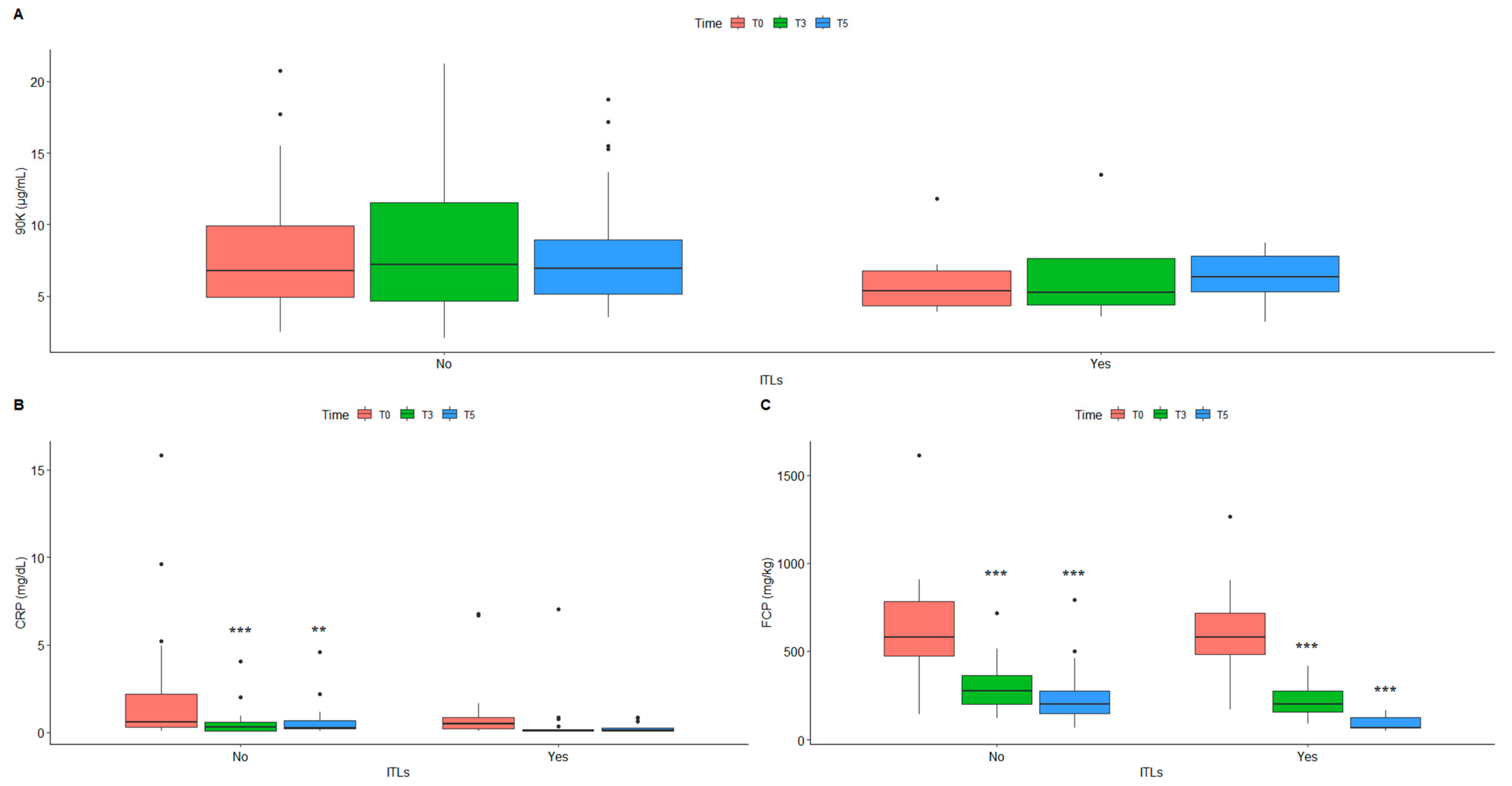
2.3. Effect of Circulating Infliximab across Follow-Up Time
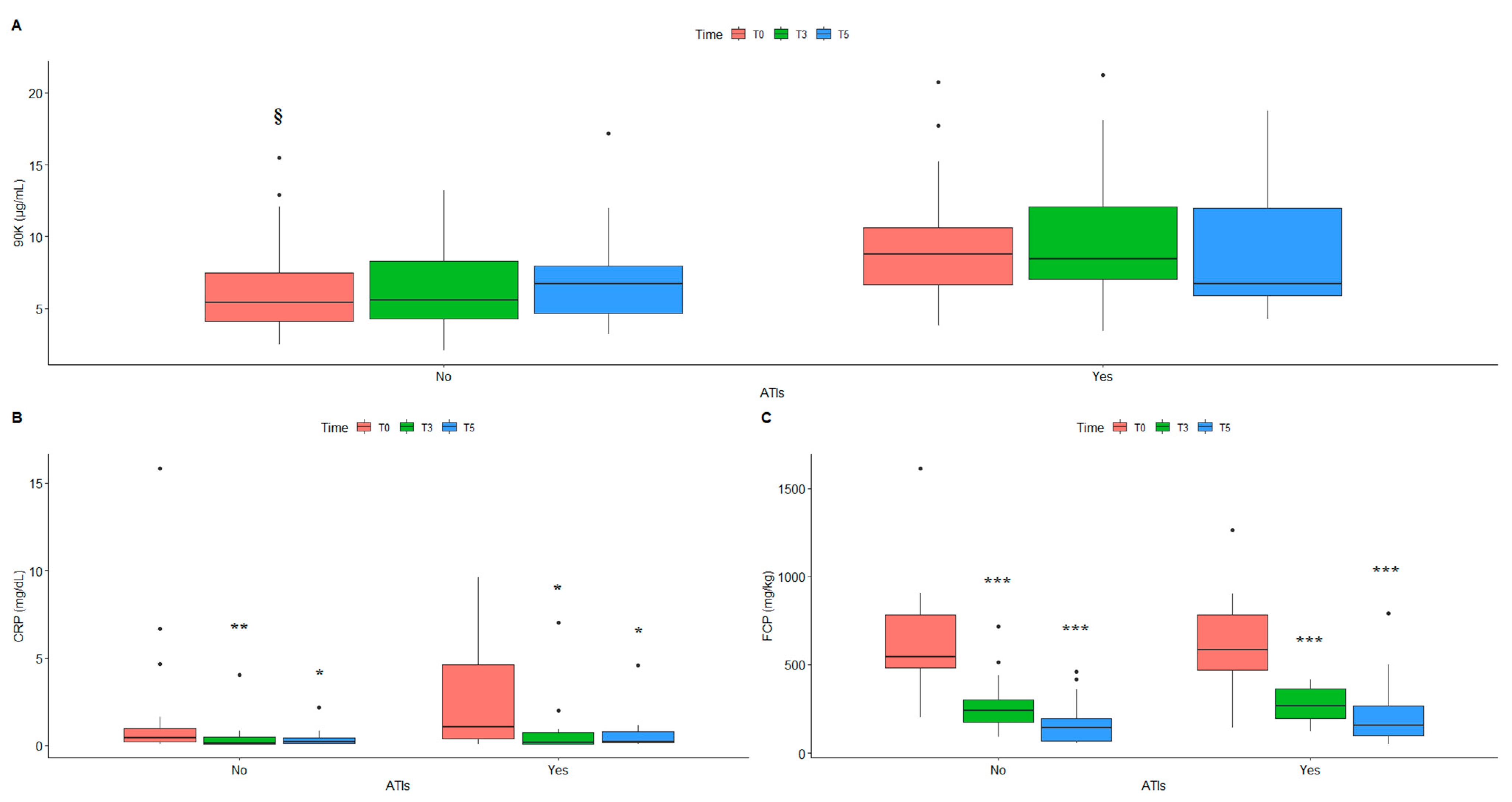
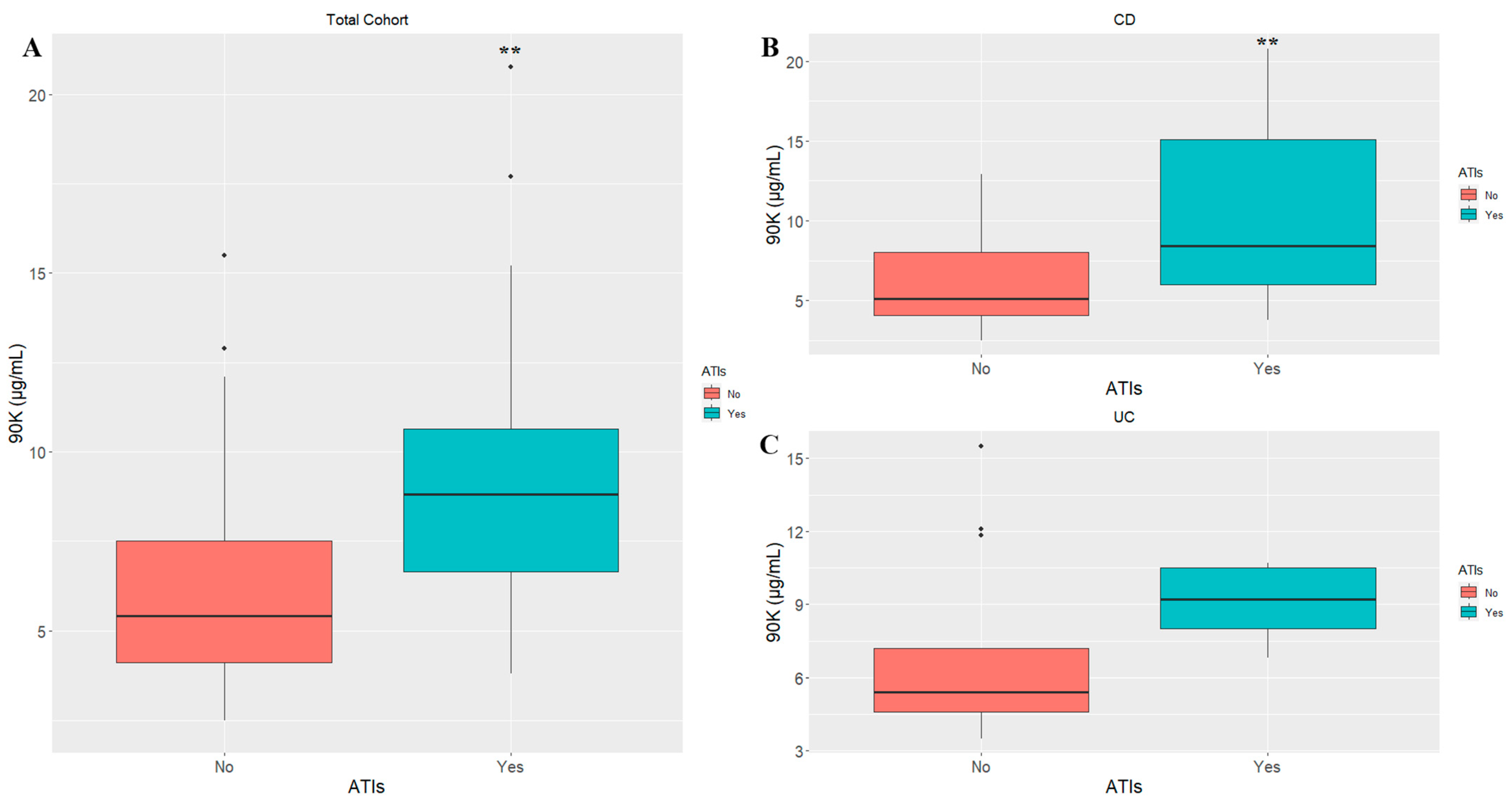
2.4. Circulating Antibodies to Infliximab Affect Serum Levels of Inflammatory Markers
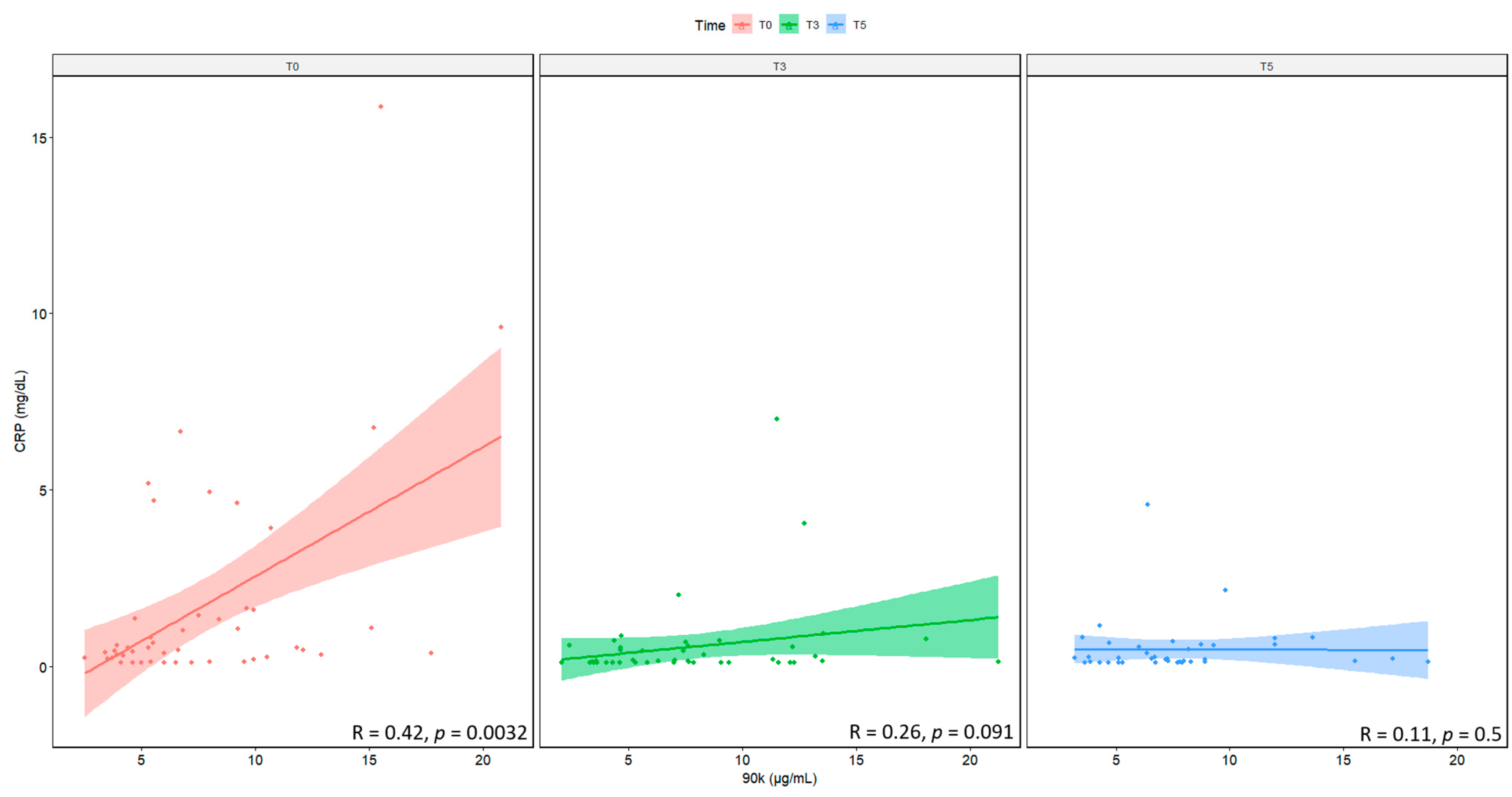
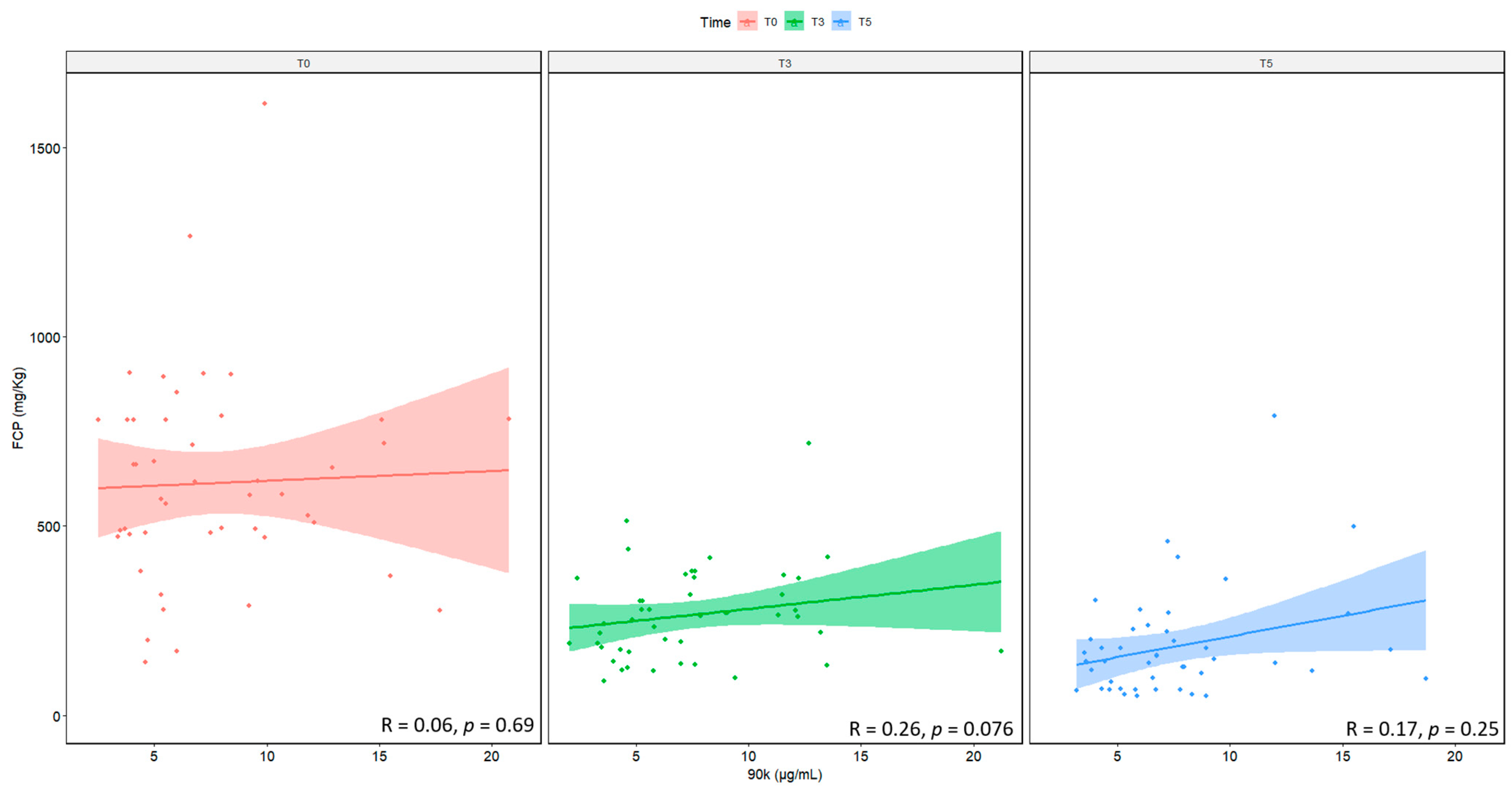
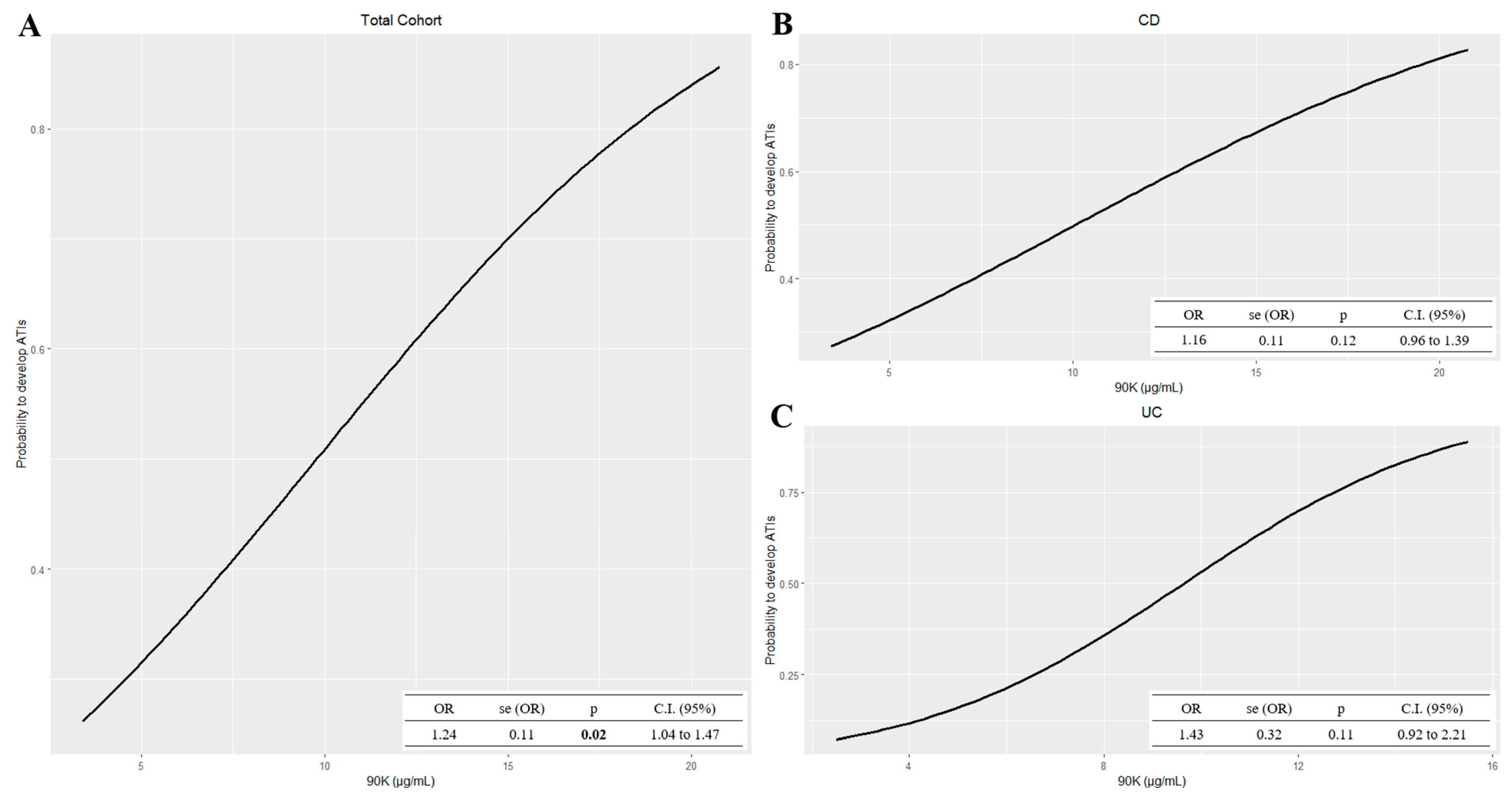
2.5. Correlation and Association between 90K and Classical Inflammatory Markers
3. Discussions
4. Materials and Methods
4.1. Ethical Considerations
4.2. Study Population
4.3. Serological Tests
4.4. Quantification of Fecal Calprotectin (FCP)
4.5. ELISA Assays
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L.; Colombel, J.F. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Sartor, R.B. Mechanisms of disease: Pathogenesis of Crohn’s disease and ulcerative colitis. Nat. Clin. Pract. Gastroenterol. Hepatol. 2006, 3, 390–407. [Google Scholar] [CrossRef]
- Saez, A.; Herrero-Fernandez, B.; Gomez-Bris, R.; Sánchez-Martinez, H.; Gonzalez-Granado, J.M. Pathophysiology of Inflammatory Bowel Disease: Innate Immune System. Int. J. Mol. Sci. 2023, 24, 1526. [Google Scholar] [CrossRef]
- Saez, A.; Gomez-Bris, R.; Herrero-Fernandez, B.; Mingorance, C.; Rius, C.; Gonzalez-Granado, J.M. Innate Lymphoid Cells in Intestinal Homeostasis and Inflammatory Bowel Disease. Int. J. Mol. Sci. 2021, 22, 7618. [Google Scholar] [CrossRef]
- Jacenik, D.; Fichna, J.; Małecka-Wojciesko, E.; Mokrowiecka, A. Protease-Activated Receptors—Key Regulators of Inflammatory Bowel Diseases Progression. J. Inflamm. Res. 2021, 14, 7487–7497. [Google Scholar] [CrossRef] [PubMed]
- Curciarello, R.; Canziani, K.E.; Docena, G.H.; Muglia, C.I. Contribution of Non-immune Cells to Activation and Modulation of the Intestinal Inflammation. Front. Immunol. 2019, 10, 647. [Google Scholar] [CrossRef] [Green Version]
- Kałużna, A.; Olczyk, P.; Komosińska-Vassev, K. The Role of Innate and Adaptive Immune Cells in the Pathogenesis and Development of the Inflammatory Response in Ulcerative Colitis. J. Clin. Med. 2022, 11, 400. [Google Scholar] [CrossRef]
- Wan, Z.; Zheng, J.; Zhu, Z.; Sang, L.; Zhu, J.; Luo, S.; Zhao, Y.; Wang, R.; Zhang, Y.; Hao, K.; et al. Intermediate role of gut microbiota in vitamin B nutrition and its influences on human health. Front. Nutr. 2022, 9, 1031502. [Google Scholar] [CrossRef]
- Jarmakiewicz-Czaja, S.; Zielińska, M.; Sokal, A.; Filip, R. Genetic and Epigenetic Etiology of Inflammatory Bowel Disease: An Update. Genes 2022, 13, 2388. [Google Scholar] [CrossRef]
- Hu, Y.; Chen, Z.; Xu, C.; Kan, S.; Chen, D. Disturbances of the Gut Microbiota and Microbiota-Derived Metabolites in Inflammatory Bowel Disease. Nutrients 2022, 14, 5140. [Google Scholar] [CrossRef]
- Berns, M.; Hommes, D.W. Anti-TNF-α therapies for the treatment of Crohn’s disease: The past, present and future. Expert Opin. Investig. Drugs 2016, 25, 129–143. [Google Scholar] [CrossRef]
- Bar-Yoseph, H.; Levhar, N.; Selinger, L.; Manor, U.; Yavzori, M.; Picard, O.; Fudim, E.; Kopylov, U.; Eliakim, R.; Ben-Horin, S.; et al. Early Drug and Anti-Infliximab Antibody Levels for Prediction of Primary Nonresponse to Infliximab Therapy. Aliment. Pharm. Ther. 2018, 47, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ungar, B.; Levy, I.; Yavne, Y.; Yavzori, M.; Picard, O.; Fudium, E.; Loebstein, R.; Chowers, Y.; Eliakim, R.; Kopylov, U.; et al. Optimizing antiTNFalpha therapy: Serum levels of infliximab and adalimumab associate with mucosal healing in patients with inflammatory bowel diseases. Clin. Gastroenterol. Hepatol. 2015, 14, 550–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neurath, M. Current and emerging therapeutic targets for IBD. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González, M.R.D.; Ballester, M.P.; Romero-González, E.; Sánchez-Pardo, A.M.; Marti-Aguado, D.; Tosca, J.; Suria, C.; Antón Ausejo, R.; Pascual Moreno, I.; Silvestre, M.D.P.; et al. Biological treatment interruption in inflammatory bowel disease: Motivation and predictive factors. Gastroenterol. Hepatol. 2022, in press. [Google Scholar] [CrossRef]
- Barrau, M.; Duprat, M.; Veyrard, P.; Tournier, Q.; Williet, N.; Phelip, J.M.; Waeckel, L.; Cheifetz, A.S.; Papamichael, K.; Roblin, X.; et al. A Systematic Review on the interest of Drug Tolerant assay in the monitoring of Inflammatory Bowel Disease. J. Crohn’s Colitis 2022, jjac164. [Google Scholar] [CrossRef]
- Mahmoud, R.; Schultheiss, H.P.; Louwers, J.; van der Kaaij, M.; van Hellemondt, B.; Mahmmod, N.; van Boeckel, P.; Jharap, B.; Fidder, H.; Oldenburg, B. Immunomodulator Withdrawal From Anti-TNF Therapy Is Not Associated With Loss of Response in Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2022, 20, 2577–2587. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Lichtenstein, L.; Assa, A.; Mazor, Y.; Weiss, B.; Levine, A.; Ron, Y.; Kopylov, U.; Bujanover, Y.; Rosenbach, Y.; et al. Levels of drug and antidrug antibodies are associated with outcome of interventions after loss of response to infliximab or adalimumab. Clin. Gastroenterol. Hepatol. 2015, 13, 522–530. [Google Scholar] [CrossRef]
- Chang, S.; Malter, L.; Hudesman, D. Disease monitoring in inflammatory bowel disease. World J. Gastroenterol. 2015, 21, 11246–11259. [Google Scholar] [CrossRef]
- Veisman, I.; Yablecovitch, D.; Kopylov, U.; Eliakim, R.; Ben-Horin, S.; Ungar, B. Predictors of Immunogenicity to Infliximab among Patients with Inflammatory Bowel Disease: Does Ethnicity Matter? Isr. Med. Assoc. J. 2021, 23, 788–793. [Google Scholar] [PubMed]
- Sasson, A.N.; Ananthakrishnan, A.N. High Anti-Infliximab Antibody Titers Do Not Impact Response to Subsequent Adalimumab Treatment in Inflammatory Bowel Diseases. Dig. Dis. Sci. 2022, 67, 3124–3128. [Google Scholar] [CrossRef] [PubMed]
- Villemonteix, J.; Guérin-El Khourouj, V.; Hugot, J.P.; Giardini, C.; Carcelain, G.; Martinez-Vinson, C. Comparison of three immunoassays for infliximab trough level monitoring in paediatric inflammatory bowel diseases. Biologicals 2021, 70, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Truta, B. Therapeutic drug monitoring in inflammatory bowel disease: At the right time in the right place. World J. Gastroenterol. 2022, 28, 1380–1383. [Google Scholar] [CrossRef]
- Bjørlykke, K.H.; Jahnsen, J.; Brynskov, J.; Molander, P.; Eberhardson, M.; Davidsdottir, L.G.; Sipponen, T.; Hjortswang, H.; Goll, G.L.; Syversen, S.W.; et al. Therapeutic drug monitoring in inflammatory bowel disease: Implementation, utilization, and barriers in clinical practice in Scandinavia. Scand. J. Gastroenterol. 2023, 58, 25–33. [Google Scholar] [CrossRef]
- Marquez-Megias, S.; Nalda-Molina, R.; Sanz-Valero, J.; Más-Serrano, P.; Diaz-Gonzalez, M.; Candela-Boix, M.R.; Ramon-Lopez, A. Cost-Effectiveness of Therapeutic Drug Monitoring of Anti-TNF Therapy in Inflammatory Bowel Disease: A Systematic Review. Pharmaceutics 2022, 14, 1009. [Google Scholar] [CrossRef]
- Cogan, R.C.; El-Matary, B.W.; El-Matary, W.M. Therapeutic drug monitoring for biological medications in inflammatory bowel disease. Saudi. J. Gastroenterol. 2022, 28, 322–331. [Google Scholar] [CrossRef]
- Irving, P.M.; Gecse, K.B. Optimizing Therapies Using Therapeutic Drug Monitoring: Current Strategies and Future Perspectives. Gastroenterology 2022, 162, 1512–1524. [Google Scholar] [CrossRef]
- Sethi, S.; Dias, S.; Kumar, A.; Blackwell, J.; Brookes, M.J.; Segal, J.P. Meta-analysis: The efficacy of therapeutic drug monitoring of anti-TNF-therapy in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2022. [Google Scholar] [CrossRef]
- Shmais, M.; Regueiro, M.; Hashash, J.G. Proactive versus Reactive Therapeutic Drug Monitoring: Why, When, and How? Inflamm. Intest. Dis. 2021, 7, 50–58. [Google Scholar] [CrossRef]
- Grossberg, L.B.; Cheifetz, A.S.; Papamichael, K. Therapeutic Drug Monitoring of Biologics in Crohn’s Disease. Gastroenterol. Clin. N. Am. 2022, 51, 299–317. [Google Scholar] [CrossRef]
- Desai, D.C.; Dherai, A.J.; Strik, A.; Mould, D.R. Personalized Dosing of Infliximab in Patients With Inflammatory Bowel Disease Using a Bayesian Approach: A Next Step in Therapeutic Drug Monitoring. J. Clin. Pharmacol. 2022. [Google Scholar] [CrossRef]
- Primas, C.; Reinisch, W.; Panetta, J.C.; Eser, A.; Mould, D.R.; Dervieux, T. Model Informed Precision Dosing Tool Forecasts Trough Infliximab and Associates with Disease Status and Tumor Necrosis Factor-Alpha Levels of Inflammatory Bowel Diseases. J. Clin. Med. 2022, 11, 3316. [Google Scholar] [CrossRef] [PubMed]
- Buczyńska, A.; Grzybowska-Chlebowczyk, U. Prognostic Factors of Biologic Therapy in Pediatric IBD. Children 2022, 9, 1558. [Google Scholar] [CrossRef]
- Atia, O.; Pujol-Muncunill, G.; Navas-López, V.M.; Orlanski-Meyer, E.; Ledder, O.; Lev-Tzion, R.; Focht, G.; Shteyer, E.; Stein, R.; Aloi, M.; et al. Children included in randomised controlled trials of biologics in inflammatory bowel diseases do not represent the real-world patient mix. Aliment. Pharmacol. Ther. 2022, 56, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Lontai, L.; Gonczi, L.; Balogh, F.; Komlodi, N.; Resal, T.; Farkas, K.; Molnar, T.; Miheller, P.; Golovics, P.A.; Schafer, E.; et al. Non-medical switch from the originator to biosimilar and between biosimilars of adalimumab in inflammatory bowel disease—a prospective, multicentre study. Dig. Liver Dis. 2022, 54, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Critchley, L.; Storey, D.; Gregg, B.; Stenson, J.; Kneebone, A.; Rimmer, T.; Burke, S.; Hussain, S.; Teoh, W.Y.; et al. Efficacy and Safety of Elective Switching from Intravenous to Subcutaneous Infliximab [CT-P13]: A Multicentre Cohort Study. J. Crohn’s Colitis 2022, 16, 1436–1446. [Google Scholar] [CrossRef]
- Liso, M.; Verna, G.; Cavalcanti, E.; De Santis, S.; Armentano, R.; Tafaro, A.; Lippolis, A.; Campiglia, P.; Gasbarrini, A.; Mastronardi, M.; et al. Interleukin 1β Blockade Reduces Intestinal Inflammation in a Murine Model of Tumor Necrosis Factor-Independent Ulcerative Colitis. Cell. Mol. Gastroenterol. Hepatol. 2022, 14, 151–171. [Google Scholar] [CrossRef]
- Iacobelli, S.; Arnò, E.; D’Orazio, A.; Coletti, G. Detection of antigens recognized by a novel monoclonal antibody in tissue and serum from patients with breast cancer. Cancer Res. 1986, 46, 3005–3010. [Google Scholar]
- Loimaranta, V.; Hepojoki, J.; Laaksoaho, O.; Pulliainen, A.T. Galectin-3-binding protein: A multitask glycoprotein with innate immunity functions in viral and bacterial infections. J. Leukoc. Biol. 2018, 104, 777–786. [Google Scholar] [CrossRef]
- Iacovazzi, P.A.; Trisolini, A.; Barletta, D.; Elba, S.; Manghisi, O.G.; Correale, M. Serum 90K/Mac-2BP glycoprotein in patients with liver cirrhosis and hepatocellular carcinoma: A comparison with alpha-fetoprotein. Clin. Chem. Lab. Med. 2001, 39, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Iacovazzi, P.A.; Guerra, V.; Elba, S.; Sportelli, F.; Manghisi, O.G.; Correale, M. Are 90K/MAC-2BP serum levels correlated with poor prognosis in HCC patients? Preliminary results. Int. J. Biol. Markers 2003, 18, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Grassadonia, A.; Graziano, V.; Pagotto, S.; Veronese, A.; Giuliani, C.; Marchisio, M.; Lanuti, P.; De Tursi, M.; D’Egidio, M.; Di Marino, P.; et al. Tgf-β1 transcriptionally promotes 90K expression: Possible implications for cancer progression. Cell Death Discov. 2021, 7, 86. [Google Scholar] [CrossRef] [PubMed]
- Bor, R.; Farkas, K.; Fabian, A.; Balint, A.; Milassin, A.; Rutka, M.; Matuz, M.; Nagy, F.; Szepes, Z.; Molnar, T. Clinical role, optimal timing and frequency of serum infliximab and anti-infliximab antibody level measurements in patients with inflammatory bowel disease. PLoS ONE. 2017, 12, e0172916. [Google Scholar] [CrossRef] [Green Version]
- Cibor, D.; Szczeklik, K.; Brzozowski, B.; Mach, T.; Owczarek, D. Serum Galectin 3, Galectin 9 and Galectin 3-Binding Proteins In Patients With Active And Inactive Inflammatory Bowel Disease. J. Physiol. Pharmacol. 2019, 70, 95–104. [Google Scholar]
- Gang, X.; Xia, Z.; Deng, F.; Liu, L.; Wang, Q.; Yu, Y.; Wang, F.; Zhu, C.; Liu, W.; Cheng, Z.; et al. Inducible LGALS3BP/90K activates antiviral innate immune responses by targeting TRAF6 and TRAF3 complex. PLoS Pathog. 2019, 15, e1008002. [Google Scholar] [CrossRef] [Green Version]
- Gallo, V.; Arienzo, A.; Iacobelli, S.; Iacobelli, V.; Antonini, G. Gal-3BP in Viral Infections: An Emerging Role in Severe Acute Respiratory Syndrome Coronavirus 2. Int. J. Mol. Sci. 2022, 23, 7314. [Google Scholar] [CrossRef]
- Cho, S.H.; Shim, H.J.; Park, M.R.; Choi, J.N.; Akanda, M.R.; Hwang, J.E.; Bae, W.K.; Lee, K.H.; Sun, E.G.; Chung, I.J. Lgals3bp suppresses colon inflammation and tumorigenesis through the downregulation of TAK1-NF-κB signaling. Cell Death Discov. 2021, 7, 65. [Google Scholar] [CrossRef]
- Drobne, D.; Kurent, T.; Golob, S.; Svegl, P.; Rajar, P.; Terzic, S.; Kozelj, M.; Novak, G.; Smrekar, N.; Plut, S.; et al. Success and safety of high infliximab trough levels in inflammatory bowel disease. Scand. J. Gastroenterol. 2018, 53, 940–946. [Google Scholar] [CrossRef]
- Roblin, X.; Boschetti, G.; Duru, G.; Williet, N.; Deltedesco, E.; Phelip, J.M.; Peyrin-Biroulet, L.; Nancey, S.; Flourié, B.; Paul, S. Distinct Thresholds of Infliximab Trough Level Are Associated with Different Therapeutic Outcomes in Patients with Inflammatory Bowel Disease: A Prospective Observational Study. Inflamm. Bowel. Dis. 2017, 23, 2048–2053. [Google Scholar] [CrossRef]
- Roblin, X.; Duru, G.; Williet, N.; Del Tedesco, E.; Cuilleron, M.; Jarlot, C.; Phelip, J.M.; Boschetti, G.; Flourié, B.; Nancey, S.; et al. Development and Internal Validation of a Model Using Fecal Calprotectin in Combination with Infliximab Trough Levels to Predict Clinical Relapse in Crohn’s Disease. Inflamm. Bowel. Dis. 2017, 23, 126–132. [Google Scholar] [CrossRef]
- Orfanoudaki, E.; Gazouli, M.; Foteinogiannopoulou, K.; Theodoraki, E.; Legaki, E.; Romanos, I.; Mouzas, I.; Koutroubakis, I.E. Infliximab trough levels are decreasing over time in patients with inflammatory bowel disease on maintenance treatment with infliximab. Eur. J. Gastroenterol. Hepatol. 2019, 31, 187–191. [Google Scholar] [CrossRef]
- Wagatsuma, K.; Yokoyama, Y.; Nakase, H. Role of Biomarkers in the Diagnosis and Treatment of Inflammatory Bowel Disease. Life 2021, 11, 1375. [Google Scholar] [CrossRef] [PubMed]
- Colman, R.J.; Tsai, Y.T.; Jackson, K.; Boyle, B.M.; Noe, J.D.; Hyams, J.S.; D’Haens, G.R.A.M.; van Limbergen, J.; Rosen, M.J.; Denson, L.A.; et al. Achieving Target Infliximab Drug Concentrations Improves Blood and Fecal Neutrophil Biomarkers in Crohn’s Disease. Inflamm. Bowel Dis. 2021, 27, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Huang, V.W.; Prosser, C.; Kroeker, K.I.; Wang, H.; Shalapay, C.; Dhami, N.; Fedorak, D.K.; Halloran, B.; Dieleman, L.A.; Goodman, K.J.; et al. Knowledge of Fecal Calprotectin and Infliximab Trough Levels Alters Clinical Decision-making for IBD Outpatients on Maintenance Infliximab Therapy. Inflamm. Bowel Dis. 2015, 21, 1359–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.J.; Kang, S.W.; Song, J.K.; Park, J.J.; Bae, Y.D.; Lee, E.Y.; Lee, E.B.; Song, Y.W. Serum galectin-3 and galectin-3 binding protein levels in Behçet’s disease and their association with disease activity. Clin. Exp. Rheumatol. 2007, 25, S41-5. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters † | Total Cohort Mean ± SD (N = 48) | CD Mean ± SD (N = 30) | UC Mean ± SD (N = 18) |
|---|---|---|---|
| Gender N (%) | |||
| Male | 30 (62.50) | 15 (50.0) | 15 (83.33) |
| Female | 18 (37.50) | 15 (50.0) | 3 (16.67) |
| Age (years) | 45.87 ± 21.74 | 41.44 ± 17.09 | 53.78 ± 27.14 |
| Smokers N (%) | 5 (16.13) | 5 (23.81) | 0 (0.00) |
| Mayo Full score (UC) (%) | |||
| 1-Mild disease | -- | 0.00 | |
| 2-Moderate disease | -- | 17.65 | |
| 3-Severe disease | -- | 82.35 | |
| Location of UC disease patients—Montreal Classification (%) | |||
| E1-Ulcerative (proctitis) | -- | 0.00 | |
| E2-Left sided UC (distal UC) | -- | 26.32 | |
| E3-Extensive UC (pancolitis) | -- | 73.68 | |
| Disease Behavior (B)—Montreal Classification (%) | |||
| B1-Inflammatory (non stricturing-non penetrating) | 81.48 | -- | |
| B2-Stricturing | 14.81 | -- | |
| B3-Penetrating | 3.70 | -- | |
| Perianal CD | 0.00 | -- | |
| Location of CD disease patients (L)—Montreal Classification (%) | |||
| L1-Ileal | -- | 33.33 | -- |
| L2-Colic | -- | 11.11 | -- |
| L3-Ileocolic | -- | 55.56 | -- |
| L4-Upper GI | -- | 0.00 | -- |
| HBI (Harvey–Bradshaw Index) | 15.52 ± 4.40 | -- | |
| Serological and fecal data at baseline | |||
| 25OH-Vitamin D (ng/mL) | 25.03 ± 11.12 | 24.08 ± 9.72 | 26.70 ± 13.39 |
| 90K (µg/mL) | 7.71 ± 4.11 | 7.78 ± 4.56 | 7.59 ± 3.36 |
| CRP (mg/dL) | 1.72 ± 2.99 | 1.55 ± 2.31 | 2.01 ± 3.93 |
| Iron (µg%) | 57.03 ± 55.86 | 62.82 ± 66.67 | 46.82 ± 27.17 |
| Ferritin (ng/mL) | 62.12 ± 57.95 | 64.95 ± 61.96 | 57.13 ± 51.53 |
| FCP (mg/kg) | 613.67 ± 272.75 | 622.34 ± 303.66 | 598.88 ± 217.95 |
| Parameters † | Infusion Cycles ‡ | |||||
|---|---|---|---|---|---|---|
| T0 (a) | T3 (b) | p § (b vs. a) | T5 (c) | p § (c vs. a) | p for Trend ¶ | |
| 25OH-vitamin D (ng/mL) | 25.03 ± 11.12 | 25.36 ± 12.08 | 0.99 | 24.32 ± 9.60 | 0.62 | 0.79 |
| 90K (µg/mL) | 7.71 ± 4.11 | 7.81 ± 4.13 | 0.11 | 7.61 ± 3.66 | 0.55 | 0.90 |
| CRP (mg/dL) | 1.72 ± 2.99 | 0.56 ± 1.18 | 0.001 | 0.48 ± 0.78 | <0.0001 | 0.04 |
| Iron (µg%) | 57.03 ± 55.86 | 73.57 ± 62.81 | 0.001 | 80.92 ± 49.32 | 0.01 | 0.05 |
| Ferritin (ng/mL) | 62.12 ± 57.95 | 45.77 ± 52.93 | 0.01 | 74.17 ± 118.95 | 0.87 | 0.55 |
| FCP(mg/kg) | 613.67 ± 272.75 | 265.50 ± 122.82 | <0.0001 | 181.11 ± 140.95 | <0.0001 | <0.0001 |
| Parameters † | Infusion Cycles ‡ | Effects p § | Contrasts p ¶ vs. (a) | |||||
|---|---|---|---|---|---|---|---|---|
| ITLs | T0 (a) | T3 (b) | T5 (c) | ITLs | Time | (b) | (c) | |
| 90K (µg/mL) | -- | 7.71 ± 4.11 | 7.81 ± 4.13 | 7.61 ± 3.66 | 0.45 | 0.98 | -- | -- |
| No | 8.14 ± 4.06 | 8.11 ± 4.04 | 7.86 ± 3.62 | -- | -- | 0.96 | 0.93 | |
| Yes | 7.22 ± 4.30 | 7.37 ± 4.46 | 7.25 ± 3.78 | -- | -- | 0.82 | 0.96 | |
| p-value ¥ | 0.45 | |||||||
| CRP (mg/dL) | -- | 1.72 ± 2.99 | 0.56 ± 1.18 | 0.48 ± 0.78 | 0.34 | 0.001 | -- | -- |
| No | 2.16 ± 3.51 | 0.55 ± 0.84 | 0.65 ± 0.99 | -- | -- | <0.001 | 0.003 | |
| Yes | 1.15 ± 2.00 | 0.57 ± 1.57 | 0.27 ± 0.26 | -- | -- | 0.09 | 0.98 | |
| p-value ¥ | 0.09 | |||||||
| FCP (mg/kg) | -- | 613.67 ± 272.75 | 265.50 ± 122.82 | 181.11 ± 140.95 | 0.02 | <0.0001 | -- | -- |
| No | 628.92 ± 292.87 | 293.50 ± 135.19 | 246.23 ± 156.43 | -- | -- | <0.001 | <0.001 | |
| Yes | 589.79 ± 256.38 | 221.10 ± 91.50 | 94.89 ± 39.20 | -- | -- | <0.001 | <0.001 | |
| p-value ¥ | 0.45 | |||||||
| Parameters † | Infusion Cycles ‡ | Effects p § | Contrasts p ¶ vs. (a) | |||||
|---|---|---|---|---|---|---|---|---|
| ATIs | T0 (a) | T3 (b) | T5 (c) | ATIs | Time | (b) | (c) | |
| 90K (µg/mL) | -- | 7.71 ± 4.11 | 7.81 ± 4.13 | 7.61 ± 3.66 | 0.007 | 0.91 | -- | -- |
| Yes | 9.76 ± 4.65 | 9.80 ± 4.80 | 8.88 ± 4.45 | -- | -- | 0.96 | 0.37 | |
| No | 6.53 ± 3.29 | 6.58 ± 3.26 | 6.86 ± 2.93 | -- | -- | 0.92 | 0.53 | |
| p-value ¥ | 0.005 | |||||||
| CRP (mg/dL) | -- | 1.72 ± 2.99 | 0.56 ± 1.18 | 0.48 ± 0.78 | 0.21 | 0.0005 | -- | -- |
| Yes | 2.33 ± 2.81 | 0.80 ± 1.67 | 0.74 ± 1.20 | -- | -- | 0.007 | 0.02 | |
| No | 1.40 ± 3.13 | 0.41 ± 0.76 | 0.36 ± 0.43 | -- | -- | 0.02 | 0.02 | |
| p-value ¥ | 0.12 | |||||||
| FCP (mg/kg) | -- | 613.67 ± 272.75 | 265.50 ± 122.82 | 181.11 ± 140.95 | 0.75 | <0.0001 | -- | -- |
| Yes | 600.65 ± 285.97 | 267.35 ± 96.72 | 213.70 ± 184.64 | -- | -- | <0.001 | <0.001 | |
| No | 619.53 ± 274.34 | 260.25 ± 138.10 | 163.28 ± 108.61 | -- | -- | <0.001 | <0.001 | |
| p-value ¥ | 0.75 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pesole, P.L.; Liso, M.; Donghia, R.; Guerra, V.; Lippolis, A.; Mastronardi, M.; Iacovazzi, P.A. 90K/Mac-2 BP Is a New Predictive Biomarker of Response to Infliximab Therapy in IBD Patients. Int. J. Mol. Sci. 2023, 24, 3955. https://doi.org/10.3390/ijms24043955
Pesole PL, Liso M, Donghia R, Guerra V, Lippolis A, Mastronardi M, Iacovazzi PA. 90K/Mac-2 BP Is a New Predictive Biomarker of Response to Infliximab Therapy in IBD Patients. International Journal of Molecular Sciences. 2023; 24(4):3955. https://doi.org/10.3390/ijms24043955
Chicago/Turabian StylePesole, Pasqua Letizia, Marina Liso, Rossella Donghia, Vito Guerra, Antonio Lippolis, Mauro Mastronardi, and Palma Aurelia Iacovazzi. 2023. "90K/Mac-2 BP Is a New Predictive Biomarker of Response to Infliximab Therapy in IBD Patients" International Journal of Molecular Sciences 24, no. 4: 3955. https://doi.org/10.3390/ijms24043955
APA StylePesole, P. L., Liso, M., Donghia, R., Guerra, V., Lippolis, A., Mastronardi, M., & Iacovazzi, P. A. (2023). 90K/Mac-2 BP Is a New Predictive Biomarker of Response to Infliximab Therapy in IBD Patients. International Journal of Molecular Sciences, 24(4), 3955. https://doi.org/10.3390/ijms24043955